Embed Size (px)
Citation preview

Carcinoma Tongue- YUVARAJ KARTHICK R

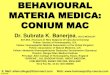
RELEVANT ANATOMY Divided into anterior 2/3rd and posterior 1/3rd
Only anterior 2/3rd is the visible part. Posterior 1/3rd can only be palpated.
Sulcus terminalis: V – shaped area that separates anterior and posterior parts.
Lined by larger papillae just anterior to the sulcus. On the midline is the foramen ceacum where the
thyroid develops from and then during development reaches the neck.

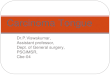
Muscles of the tongue:Intrinsic muscles:
Superior and inferior Longitudinal Transverse Vertical
Extrinsic Muscles:GenioglossusHyoglossusStyologlossusPalatoglossus

Muscles of the tongue

Intrinsic muscles ActionsSuperior longitudinal Shortens tongue and makes
dorsum concaveInferior longitudinal Shortens tongue and makes
dorsum convexTransverse Makes tongue narrow &
elongatedVertical Makes tongue broad and
flattenedExtrinsic muscles ActionsGenioglossus Protrudes Hyoglossus Depresses Styloglossus RetractsPalatoglossus Elevates

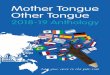
Lymphatic Drainage Tip of the tongue: Drains bilaterally to submental
nodes
Rt and Lt halves of anterior 2/3rd: Drain respectively to the Submandibular nodes. Centrally located region may drain bilaterally to deep cervical nodes.
Posterior 1/3rd: Drains to upper deep cervical nodes bilaterally (jugulodigastric)
The whole network finally drains into jugulo-omohyoid.


Blood supply of tongue Arterial Supply Lingual artery branch of
External artery. Root of tongue is supplied by tonsillar artery branch of
facial artery & ascending pharyngeal branch of external carotid
Venous supply Venae comitantes accompany lingual artery and one accompanying hypoglossal nerve
Deep lingual vein: 2 in number seen on posterior aspect and unite posteriorly to form lingual vein which later drains into internal jugular vein

Nerve Supply: Motor supply
All muscles except palatoglossus is supplied by Hypoglossal nerve.Palatoglossus is supplied by accessory nerve.
Sensory supplyLingual nerve general sensationChorda Tympani Taste sensation for anterior 2/3rd
Glossopharyngeal Nerve Both general sensation and taste of posterior 1/3rd Vagus posterior most part of the tongue through internal laryngeal nerve


Introduction to Oropharyngeal Carcinoma
In the western world it is a rare condition (2-4%) Whereas in India, very high incidence – 40% of
all cancers
Reason for above is Smoking, tobacco chewing, betel nut chewing etc.,
Most common malignancy is Squamous cell Carcinoma

Risk Factors Smoking & tobacco related products Spirit Sepsis Sharp tooth Spices
Virus: HPV, EBV Plumer Vinson syndrome

Pathology Anatomy of the oropharynx is complex Fascial planes act as barriers for the spread of
the tumor but contribute to spread of malignant cells to the lymph nodes.
Perineural spread leads to direct spread intra cranially
Angioinvasion Distant mets

Malignancies of the oral cavity SQUAMOUS CELL CA:
Most common Chronic exposure to Carcinogens Dysplasia
multiple sites of subclinical malignant sites Synchronous/ metachronous lesions
ADENOCARCINOMA: Those arising from minor salivary glands.
LYMPHOMA: Posterior most part of the tongue. Particularly around the Waldeyer’s ring

Premalignant lesions High Risk Lesions:
Erythroplakia/ Speckled erythroplakia Chronic Hyperplastic Candidiasis
Moderate Risk Lesions: Oral submucous fibrosis Syphilitic glossitis Sideropenic dysphagia (Paterson – Kelly Syndrome)
Low Risk/Equivocal Risk lesion: Oral lichen planus Discoid lupus erythematosus Discoid keratosis congenita

Leukoplakia: Defined as any white patch or
plaquethat cannot be characterized clinically or pathologically.
Varies from a well circumscribed lesion to extensive lesion involving large areas.
Speckled Leukoplakia: Variant of Leukoplakia arising
from an erythematous base Higher incidence of malignant
transformation.

Premalignant lesions… Erythroplakia:
Any lesion of the oral mucosa that presents as a bright red plaque which cannot be characterized clinically or pathologically
Lesions are irregular in outline and separated from normal mucosa

Premalignant conditions Chronic Hyperplastic candidiasis:
Produces dense plaques of leukoplakia High incidence of malignant transformation Believed to be invasion of Candida Albicans Sometimes associated with immunodeficiency
Rx: Prolonged antifungals either topical or systemic
Persistent lesions should undergo laser ablation or surgical excision.


Oral submucous fibrosis: Progressive disease with fibrous bands beneath
the mucosa contracture limited mouth opening restricted tongue movement.
Almost entirely confined to Asian population Epithelium also shows dysplasia
Rx: Intralesional steroid/surgical excision and placement of grafts
Mainly associated with areca nut usage than tobacco.


Sideropenic dysplasia A.k.a Plummer – Vincent and Paterson – Kelly
Syndrome. There is a well known relationship b/w the
condition & oral cancers. Common in Scandinavian women Leads to Epithelial atrophy mucosa velnerable
to carcinogens malignancy
Rx: Correction of sideropenia with Fe supplements decreases incidence of malignancy


Clinical Features Painless long standing ulcer Later becomes painful d/t
infection or nerve involvement Readily bleeds to touch Induration present more than the ulcer area Edge may be raised and everted.
Excessive salivation Dysphagia d/t fixation of tongue by involvement of
genioglossus or d/t posterior third growth. Halitosis Change in voice Neck nodes Aspiration bronchopneumonia

Classification and Staging



Investigations Patient presents with a chronic ulcer Edge
biopsy
Neck nodes palpable FNAC
Indirect laryngoscope posterior lesions
CT or MRI For the extent of the lesions
CXR to r/o pneumonia

Treatment: Principle treatment modality Surgery and RT
Smaller lesions Either RT or Surgical excision
Larger lesion Combination of both
If neck nodes are involved MRND

Treatment options T1 or T2 lesion with no nodes surgery RT RT is usually Brachy or EBRT
T3 or T4 without nodes or lesion N2 Surgery + Post op RT Chemo
N3 disease or M1 disease Palliative Therapy

Surgery Advantages:
Short term treatment Specimen available for Histopath Can plan on adjuvant No radiation sequelae
Disadvantages: Tissue and functional loss Disfigurement Bleeding & infection


Radiotherapy Can primarily treat T1 or T2 disease Disadvantages are altered taste, xerostomia Long term treatment (at least 6 weeks)
Osteonecrosis of the mandible. Newer techniques like IMRT reduce the above
complications.


Chemotherapy Curative
Neoadjuvant Adjuvant Concurrent (to treat micromets)
Palliative Recurrence Metastatic disease
Drugs: Cisplatin, MTX,5FU

Management of neck nodes: Clinically node negative disease:
Cervical nodes may have occult mets upto 30% even if clinically node negative
Hence Selective Node dissection is suggested “Supraomohyoid dissection”
Especially in Ca Tongue micromets can extend upto level IV Hence extended supraomohyoid dissection is suggested

Clinically node positive disease: N1 disease Supra omohyoid dissection
N2a & N2b MRND + post op RT
N2c disease B/l MRND Postop RT
N3 Extensive neck involvement Possible try EBRT



Thank You











![Metachronous Carcinoma of the Trachea and Lung after a ... · in tongue and rest of that in oral cavity and oropharynx [6]. The most common cause of oropharyngeal carcinoma in the](https://img.pdfslide.net/doc/110x75/5ed44ec04e1aa219885a91c7/metachronous-carcinoma-of-the-trachea-and-lung-after-a-in-tongue-and-rest-of.jpg)