Embed Size (px)
DESCRIPTION
cariac anatomy and physiology review
Citation preview

Cardiovascular Physiology

Objectives
• Review the basic anatomy and
physiology of the cardiovascular
system.
• Describe the electrical and mechanical
events involved in the cardiac cycle.

Objectives
• Discuss the factors that alter or impact the
electrical and mechanical events of the
cardiac cycle.
• Explain the physiology of circulation and
perfusion.

Anatomy

Did you know???Your heart is about the size of your clenched fist
It beats about 4000 times an hour and about 100,000 times a day
It will beat over 2 billion times in a lifetime
Each heartbeat pumps half a cup of blood
The force of your heartbeat is sufficient to shoot blood 30 feet into the air

Anatomy Review - The Heart
Right atrium
• Incoming blood supply
• Tricuspid valve
• Chordae tendinae and
papillary muscles
• Right Ventricle
• Pulmonary artery

Anatomy Review - The Heart
Left atrium
• Receives supply
from the pulmonary
vein
• Left ventricle
• Bicuspid (mitral) valve
• Aorta

Anatomy Review - The Heart
Heart wall
• Endocardium
• Myocardium
• EpicardiumSplits into another
outside layer – the
pericardium

The Pericardium
• Fixates the heart to thethoracic cavity
• Relatively inflexible tissue• Pericardial sac holds
30-50mL of serousfluid between thepericardium andepicardium,prevents friction during contraction

Valves of The Heart
Pulmonic
Aortic
Mitral
Tricuspid

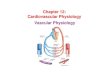
Circulation through HeartCirculation through Heart
Pulmonary
Right side of the heart
Blood from the body, low O2 high CO2, right atriumright ventriclelungs via pulmonary trunk.
Unloading of CO2 pick up O2 to left side of the heart.
Arteries carry De-Oxygenated blood
Veins carry oxygen rich blood
Systemic
Left side of heart
Oxygen rich blood - lungs- left atrium- left vent. - aorta
Blood transported via systemic arteries to body tissues, gas and nutrient exchange across capillary walls
Blood is then returned to the right side of the heart through superior and inferior venae cavae.


Circulation through HeartCirculation through Heart
Although equal volumes of blood are flowing in the pulmonary and systemic circuits, the two ventricles have uneven workloads.
Pulmonary Circuit: right, short low pressure circulation.
Systemic Circuit: left, long pathway, five times as much resistance to blood flow, high pressure

Coronary CirculationCoronary Circulation
The functional supply of the heart, is the shortest circulation in the body.
The arterial supply of coronary circulation is provided by the right and left coronary arteries arising from the base of the aorta, and encircle the heart in the atrioventricular groove.

Coronary ArteriesCoronary Arteries
• The coronary arteries provide an intermittent, pulsating blood flow to the myocardium.
• Actively deliver blood when the heart is relaxed, ineffective when the ventricles are contracting because:– compressed by contracting myocardium– entrances to the coronary arteries is
blocked by the open Aortic valve.

Coronary Artery SuppliesRight C.A.
Right atrium andventricle
Inferior portion ofthe left ventricle
Interventricularseptum
Conductionsystem

Coronary Artery Supplies
Left Main C.A.
Left atrium
Nearly all of theleft ventricle
Circumflex and LAD Branch
AV node in halfof the population

Cardiac Physiology
• Electrical components
• Electrophysiology
• The Cardiac Cycle
• Mechanical Events of the Cardiac Cycle
• Influences of Electrical and Mechanical
• Heart Function

Electrical Conduction System

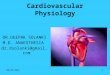
Action Potential
Upstroke depolarisation
Early repolarisation
Notch Plateau
Late rapid Repolarisation
Resting potential
Intracellular
Extracellular
Ref: Woods et al (2005) Cardiac Nursing 5th ed Lippincott, Wilkins & Williams: Philadelphia p 23

Cardiac Cell Types
Electrical cells• Generate andconduct impulsesrapidly• SA and AV nodes• Nodal pathways• Interventricularseptum• No contractileproperties

Cardiac Cell Types
Muscle (myocardial) cells• Main function iscontraction• Atrial muscle• Ventricular muscle• Able to conductelectrical impulses• May generate its ownimpulses with certaintypes of stimuli

Unique Properties of Cardiac Cells
• Automaticity
SA and AV nodes
• Excitability (all cells)
Points of stimulation
• Nervous system
• Physical cell damage
• Ischemia
• Electrolytes
• Conductivity (all cells)
Points of stimulation• Nervous system
• Electrolytes
Slowing of conductivity• Ischemia
• Calcification of nodal
pathways
Contraction• Muscle cells

Mechanical Functionof the Heart

The Cardiac Cycle
2 components
Diastole Filling of the chamber
Systole Contraction of the chamber and ejection of
blood

Cardiac Output
• The amount of blood ejected from the
ventricle in one minute
• Elements of cardiac output
Stroke volume CO = SV x HR• Amount of blood ejected from the
ventricle in one contraction
Heart rate
• The number of cardiac cycles in one minute

Determination of Stroke Volume
PreloadAmount of blood delivered to the chamber.Depends upon venous return to the heart.Also dependent upon the amount of blood
delivered to the ventricle by the atrium.Contractility
The efficiency and strength of contractionFrank Starling’s Law
AfterloadResistance to forward blood flow by the vessel
walls

Cardiac Feedback Loops
• Master controller: the medullaIncoming input
• ChemoreceptorsSense changes in pH, PaCO2 and PaO2
• BaroreceptorsSense changes in arterial pressure
Response of the medulla• Stimulate the autonomic nervous system

Autonomic Nervous System
Sympathetic Nervous System
Extensively innervates the SA node and ventricular cells
• Increase in heart rate
• Increase in conduction and contractility in the ventricles
Parasympathetic Nervous System
Innervates the SA and AV nodes
• Decreases heart rate
• Decreases conduction times through the AV node

Chemical Factors
• Hormones
Adrenaline
• Stimulation of beta receptors in the
myocardium
• Increase in contractility of the ventricles
• Increase in conduction throughout the
ventricles

Chemical Factors
Electrolyte Concentrations
Calcium
• Impacts the strength of contractions
• High calcium may cause irritability of electrical cells

Chemical Factors
PotassiumImpacts the rates of firing and recovery of thecardiac cells
• High potassium• Irregular firing of cardiac cells• Dysrhythmias and ventricular fibrillation potentials
• Low potassium• Longer delays in the firing of cardiac cells• May be caused by diuretic use• Bradycardia• Hypotension (systemic complication)• Poor cardiac output results

The Vascular System

The Vascular System
• The vascular system is composed of the systemic and pulmonary circulation.
• Both systems consist of arteries, capillaries and veins.
• Arterial system: away from the heart
• Venous system: capillary beds to heart
• Anatomical differences of arteries and veins

Factors Contributing to Arterial Blood Pressure
BP = CO x TPR• Cardiac Pump
• Blood Volume
• Peripheral Resistance
• Elasticity of Arterial Walls
• Viscosity of Blood

Factors Aiding Venous Return
1) Cardiac Pump
2) Respiratory Pump
3) Muscular Pump

Control Of Blood Pressure
• Cardioacceleratory & Cardioinhibitory centres in the Medulla.
• Chemicals, Temperature, Sex, Emotions and age, effect heart rate
• Vasomotor centre, pressoreceptors (baroreceptors), chemoreceptors - chemical and autoregulation

Pathophysiology
When it all goes wrong

Pathophysiology – Pericardial, Myocardial and Endocardial
Disease • Pericarditis – inflammation of the pericardium
• Effusion – excess fluid/blood/pus in the pericardial sac
• Tamponade – significant compression of the heart due to pericardial effusion
• Myocarditis – inflammation of the myocardium
• Cardiomyopathies – dilatation, hypertrophy or non-compliance of the myocardium
• Infective Endocarditis – infective organisms invade the endothelial lining of the heart involving the valves, causing vegetation

Pathophysiology - Valvular Heart Disease
• Stenotic – unable to open fully restricting forward blood flow afterload and cause hypertrophy (enlarged muscle)
• Regurgitant, incompetent or insufficient– Unable to close fully permit backward blood flow– volume load and cause dilation of chambers
• Rheumatic Heart Disease – extensive inflammatory changes scarring of the
valves
• Infective Endocarditis– Endovascular infection vegetation on a heart valve
• Degenerative Changes

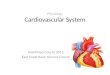
Physiology of Ischaemia
Atherosclerosis – HardeningAtheroma (plaque) builds up in the coronary arteries and reduces blood flow and O2 supply to the heart muscle, resulting in angina pain. Prolonged ischaemia or plaque rupture leads to myocardial infarction and loss of myocardial function (heart failure). The extent of damage depends on which artery is affected and time to treatment.

References
• Darovic, G. (2002). Hemodynamic Monitoring invasive and noninvasive clinical application 3rd ed. W.B. Saunders Company.
• Marieb, E.N. (2001). Human Anatomy and Physiology 2nd ed. The Benjamin/Cummings Publishing Company: California.
• Stinson Kidd, P.& Dorman, Wagner, K. (2001). High Acuity Nursing 3rd ed. Prentice Hall: New Jersey.
• Thelan, L.A., Urden, L.D., Lough, M.E. & Stacy, K.M. (1998). Critical Care Nursing Diagnosis and Management 3rd ed. Mosby: St Louis.
• Tortora, G.J. & Grabowski, S.R. (1993). Principles of Anatomy & Physiology 7th Ed. Harper Collins: New York