Embed Size (px)
Citation preview
Case based learning
Triangles of neck region
By
Dr. Abdul Waheed Ansari
Chairperson & Prof. Anatomy,
RAK COLLEGE OF MEDICAL SCIENCES
RAKMHSU.
12/18/2014 1
The learning outcomes for this CBL are
• The effects of compression of the neurovascular bundle of neck is usually involved in masses arising from the triangles of neck.
• The effects of injuries to hypoglossal, accessory, vagus, glossopharyngeal, lingual branch of trigeminal.
• The involvement of cervical groups of lymph nodes during infections and inflammations of salivary glands, oral cavity and tongue.
12/18/2014 2
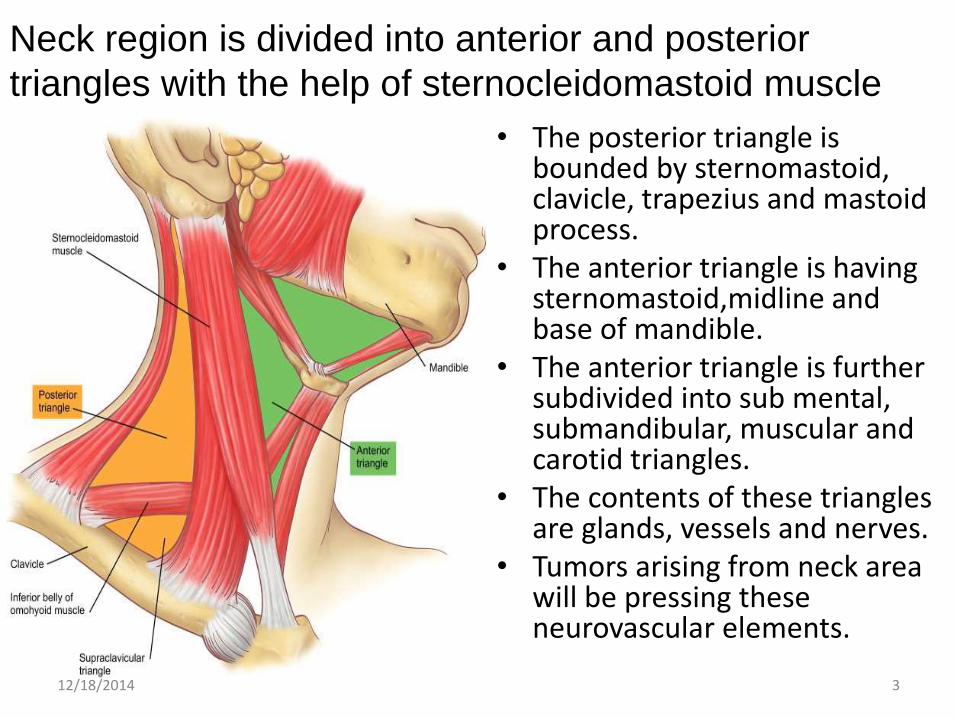
Neck region is divided into anterior and posterior
triangles with the help of sternocleidomastoid muscle
• The posterior triangle is bounded by sternomastoid, clavicle, trapezius and mastoid process.
• The anterior triangle is having sternomastoid,midline and base of mandible.
• The anterior triangle is further subdivided into sub mental, submandibular, muscular and carotid triangles.
• The contents of these triangles are glands, vessels and nerves.
• Tumors arising from neck area will be pressing these neurovascular elements.
12/18/2014 3

A Clinical case of inflamed palatine tonsil
• A 5 year old girl was taken to the primary health care physician with complaints of sore throat, running nose and high temperature.
• Her mother also complained that she had difficulty in swallowing.
• Physician examined her throat and found that the tonsils were enlarged and congested.
• Which groups of lymph nodes often becomes easily palpable when palatine tonsils are inflamed?
12/18/2014 4

Cervical groups of lymph nodes• The head and neck areas are drained by superficial and deep cervical
groups of lymph nodes.• These lymph nodes are situated in superficial and deep fascia in a cervical
collar distribution.• The head area above the parotid gland is drained into preauricular or
parotid group of lymph nodes.• Below this the lymphatic's reach the submandibular group of lymph
nodes.• From the central area of face and tongue the lymph is drained in to sub
mental group of nodes.• The palatine tonsils lymphatic reach the deep cervical-jugulo-digastric
group of lymph node.• From the posterior aspect of scalp it reaches, mastoid group, occipital
group or posterior auricular group.• The supraclavicular group of lymph nodes receive lymph from various
abdominal organs- malignancy arising from stomach & uterus may have supraclavicular lymph nodes enlargements.
12/18/2014 5

Lymph nodes of head and neck
12/18/2014 6
A clinical case of spinal accessory nerve injury
• An abscess was surgically removed from the middle of the posterior triangle on the right side.
• During recovery the patient noticed that her shoulder drooped and she could no longer raise her right hand above her head to brush her hair.
• Which nerve has been cut?
12/18/2014 7
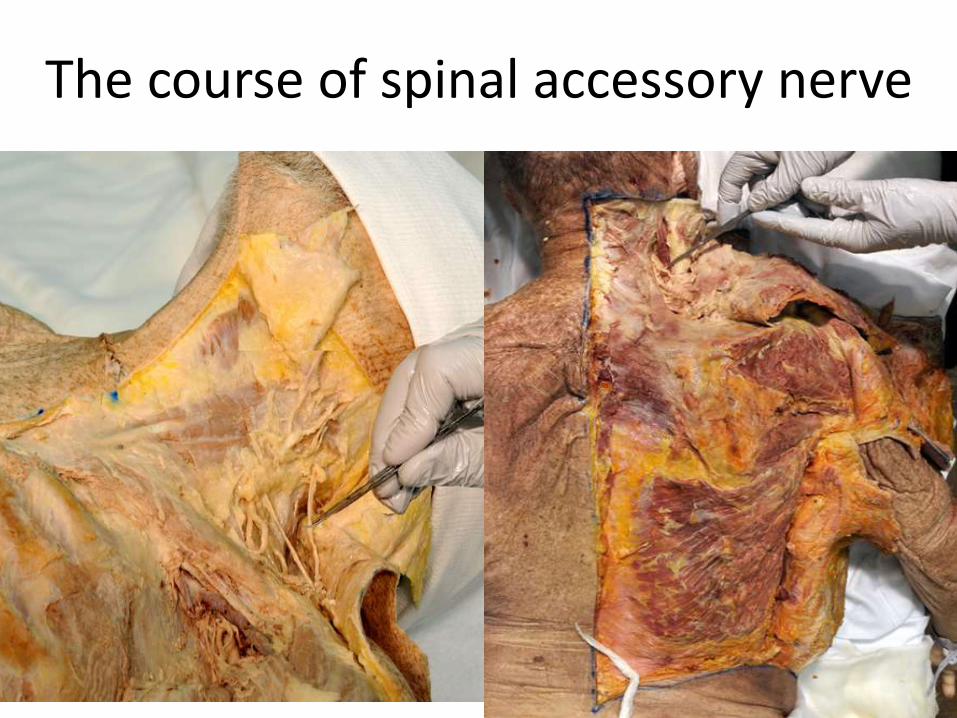
The course of spinal accessory nerve
12/18/2014 8

The accessory nerve is the XI cranial nerve
• It arises from its nucleus in brain stem- the nucleus ambiguous.
• The accessory nerve has two roots, a cranial root and a spinal root.
• The spinal accessory enters the cranial cavity through foramen magnum and joins the cranial root and leave the cranial cavity through the foramen rotundum.
• In the neck it supplies the sternomastoid and trapezius muscles.
• It runs in the posterior triangle of neck.
• Injury to this nerve leads to drooping of the shoulder.12/18/2014 9

Congenital torticollis is wry neck- a clinical condition due to tumor of sternomastoid
• Spasmodic Torticollis (ST) is a painful and debilitating neurological movement disorder.
• Approximately 3 in every 10,000 people – about 90,000 people in the United States – are known to suffer from ST.
12/18/2014 10

The cervical plexus are formed under the posterior triangle
• The following nerves arise from the cervical plexus:-
1.Lesser occipital nerve
2.Great auricular nerve
3. Transverse cervical nerve
4. Supraclavicular nerves
• The lesser occipital nerve carry sensations from the occipital area of scalp.
• The great auricular nerve carries sensation from areas around parotid gland.
• The transverse cervical nerve carries sensation from midline to the sternal notch/jugular notch.
• The supraclavicular nerves carry sensation from chest wall until the sternal angle.12/18/2014 11

Superficial cervical plexus is seen emerging behind the posterior border of the sternocleidomastoid muscle at the intersection of the muscle with the external jugular
vein
• 1. transverse cervical nerve
• 2. lesser occipital nerve
• 3.supraclavicular nerves
• 4. external jugular vein.
• 5. Greater auricular nerve.
12/18/2014 12

A clinical case of mumps
• A mother brings her 5 year old son to pediatric hospital with complains of her son having fever and swelling around his neck.
• The pediatrician informed her that her son is having mumps infection.
12/18/2014 13
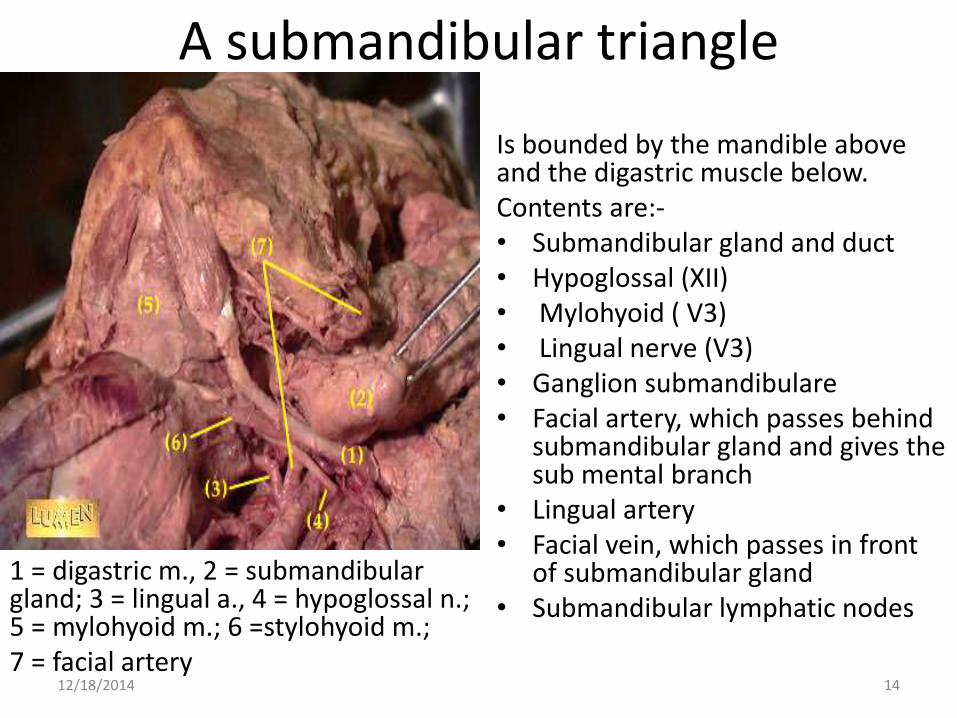
A submandibular triangle
1 = digastric m., 2 = submandibular gland; 3 = lingual a., 4 = hypoglossal n.; 5 = mylohyoid m.; 6 =stylohyoid m.; 7 = facial artery
Is bounded by the mandible above and the digastric muscle below.Contents are:-• Submandibular gland and duct • Hypoglossal (XII) • Mylohyoid ( V3) • Lingual nerve (V3) • Ganglion submandibulare• Facial artery, which passes behind
submandibular gland and gives the sub mental branch
• Lingual artery • Facial vein, which passes in front
of submandibular gland • Submandibular lymphatic nodes
12/18/2014 14

The hypoglossal nerve is a XII cranial, motor nerve to muscles of
tongue
• The hypoglossal nucleus is situated in the floor of VI ventricle-medulla.
• The nerve exits through the hypoglossal foramen and runs below the tongue in the submandibular triangle and supplies the musculature of tongue.
• Injury to the hypoglossal nerve will deviate the tongue towards the side of lesion.
• Left hypoglossal nerve injury and paralysis of the left side of the tongue.
• A month before this picture was taken, this patient's left hypoglossal nerve was injured during surgery on his carotid artery (carotid endarterectomy).
• This was immediately followed by deviation of the tongue to the same side as the injury.
12/18/2014 15

The lingual nerve is a branch from trigeminal nerve
• It is a sensory nerve to anterior 2/3rd
of tongue and carries general sensation of touch, pain and temperature.
• The special sensation of taste from anterior 2/3rd of tongue is carried by chorda tympani branch of facial nerve.
• The chorda tympani nerve joins the lingual nerve in the infratemporalfossa.
• The chorda tympani nerve also carry secretomotor fibers for submandibular and sublingual salivary glands.
• The lingual nerve can be injured during tooth extraction.
• As a result of injury taste and general sensation from anterior 2/3rd tongue will be lost.
There will be Loss of secretion from submandibular and sublingual glands ipsilateral to the lesion apart from Loss of taste from anterior 2/3 of tongue ipsilateral to the lesion.
12/18/2014 16
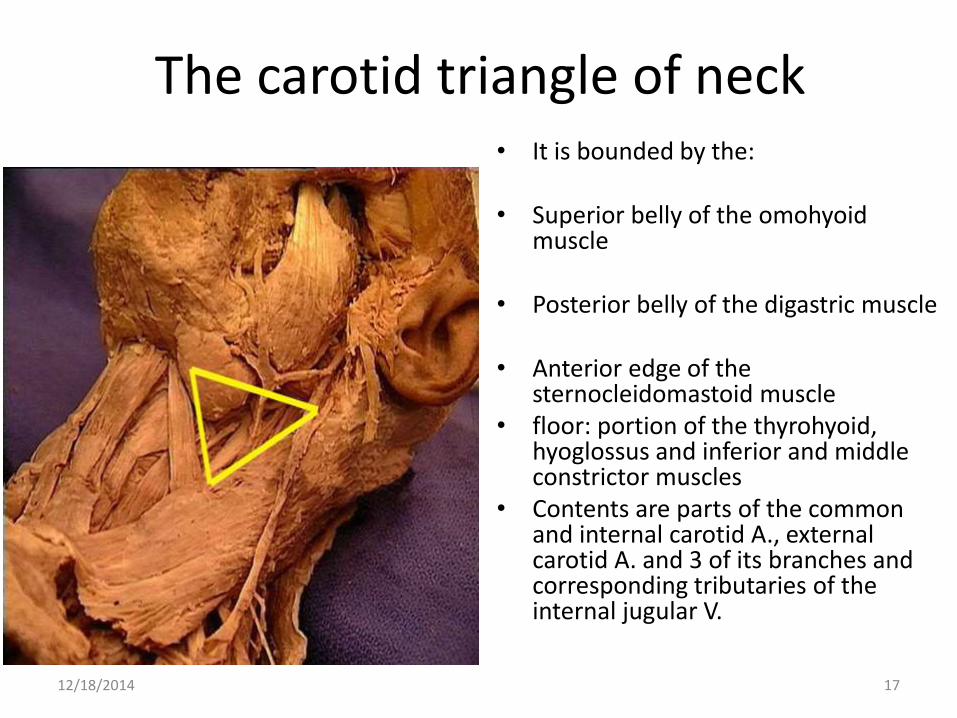
The carotid triangle of neck• It is bounded by the:
• Superior belly of the omohyoidmuscle
• Posterior belly of the digastric muscle
• Anterior edge of the sternocleidomastoid muscle
• floor: portion of the thyrohyoid, hyoglossus and inferior and middle constrictor muscles
• Contents are parts of the common and internal carotid A., external carotid A. and 3 of its branches and corresponding tributaries of the internal jugular V.
12/18/2014 17

The carotid vessels are the main blood vessels for brain, head and neck areas.
• The left common carotid arises from arch of aorta.
• The right is a branch from brachiocephalic trunk.
• The common carotid vessel is enclosed in carotid sheath ( which is a modified deep fascia of neck). The other structures enclosed in the carotid sheath are internal carotid artery, internal jugular vein and vagus nerve.
• The common carotid divides into external and internal branches at the level of upper border of thyroid cartilage.
• There are 8 branches arising from external carotid, 2 terminal branches, 2 dorsal branches and remaining 4 are ventral branches.
• The internal carotid enters the cranial cavity to supply the brain through the carotid canal, that passes through the petrous temporal bone.
12/18/2014 18

Clinical case of carotid body tumour
12/18/2014 19
12/18/2014 20
• A 68-year-old female noticed a 2.5 x 1.5 cm neck lump superficial to the left sternocleidomastoid (SCM) muscle.
• Relevant past medical history included a lumpectomy for malignant breast neoplasm in 2003.
• Ultrasound confirmed a solid lesion superficial to the left SCM.
• CT showed an enhancing lobulated mass lesion splaying the left internal and external carotid artery and compressing the left internal jugular vein, it extended posteriorly curling behind the SCM muscle and terminated in a superficial component overlying the muscle.
• In view of her previous history of breast carcinoma core biopsy was performed with histology suggestive of metastatic carcinoma possibly a neuroendocrine tumour.
• Immunohistochemistry confirmed neuroendocrine differentiation typical for paraganglioma.
• Twenty four hour urinary catecholamine studies were normal.
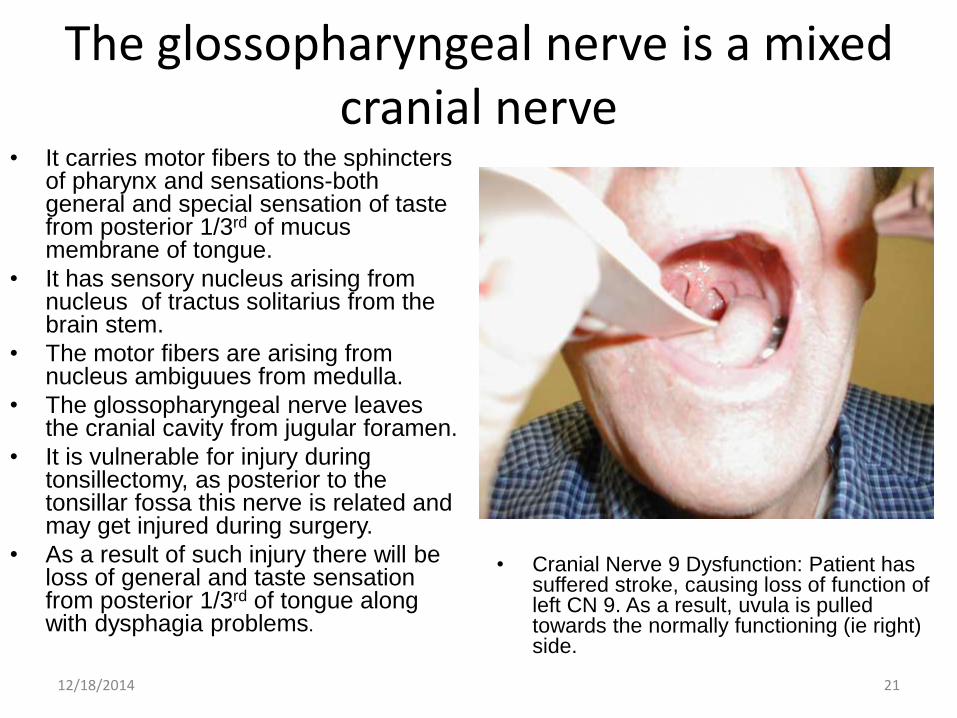
The glossopharyngeal nerve is a mixed cranial nerve
• It carries motor fibers to the sphincters of pharynx and sensations-both general and special sensation of taste from posterior 1/3rd of mucus membrane of tongue.
• It has sensory nucleus arising from nucleus of tractus solitarius from the brain stem.
• The motor fibers are arising from nucleus ambiguues from medulla.
• The glossopharyngeal nerve leaves the cranial cavity from jugular foramen.
• It is vulnerable for injury during tonsillectomy, as posterior to the tonsillar fossa this nerve is related and may get injured during surgery.
• As a result of such injury there will be loss of general and taste sensation from posterior 1/3rd of tongue along with dysphagia problems.
• Cranial Nerve 9 Dysfunction: Patient has suffered stroke, causing loss of function of left CN 9. As a result, uvula is pulled towards the normally functioning (ie right) side.
12/18/2014 21

The muscular triangle• The boundaries of the muscular
triangle are:
• Superiorly: The hyoid bone• Medially: Imaginary midline of
the neck• Supero-laterally: Superior belly
of the omhyoid muscle• Infero-laterally: Inferior portion
of the sternocleidomastoid muscle.
• It does however contain some muscles – the infrahyoidmuscles, the pharynx, and the thyroid, parathyroid glands.
12/18/2014 22
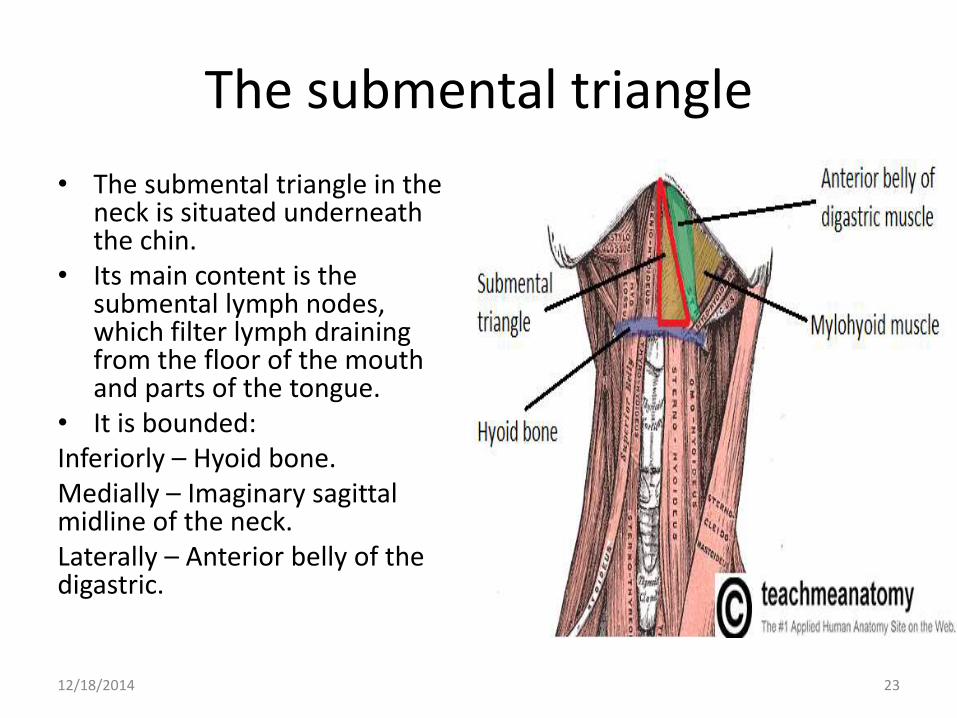
The submental triangle
• The submental triangle in the neck is situated underneath the chin.
• Its main content is the submental lymph nodes, which filter lymph draining from the floor of the mouth and parts of the tongue.
• It is bounded:Inferiorly – Hyoid bone.Medially – Imaginary sagittal midline of the neck.Laterally – Anterior belly of the digastric.
12/18/2014 23

References
• http://www.labome.org/research/Carotid-body-tumour-presenting-in-an-unusual-anatomical-fashion.html
• http://www.yale.edu/cnerves/cn7/cn7_28.html
• http://teachmeanatomy.info/neck/areas/anterior-triangle/
• http://meded.ucsd.edu/clinicalmed/head.htm
12/18/2014 24