Embed Size (px)
Citation preview
CASE STUDY
-Dr.ApoorvaDCH 2nd yr
• 8 year old boy • Born out of non consanguineous marriage• c/o weakness of lower limbs since 3 years of age• Insidious onset , gradually progressed from the legs to involve the
thighs & hip
• Difficulty in getting up from sitting position• Difficulty in climbing stairs• History of stumbling on walking a long
distance• History of progressively increasing thickness of
calf muscles bilaterally• History of thinning of both thighs
• History of difficulty in swallowing • History of recurrent lower respiratory tract
infections• History of toe walking• Pain in the calves bilaterally on more than daily
activities
since 1 year
• No h/o difficulty in wearing footwear• No h/o difficulty in combing,changing shirt,washing face• No h/o impaired vision/abnormal smell/drooling of
saliva/deviation of angle of mouth while eating• No h/o stiffening of limbs/floppiness• No h/o altered sensations• No history s/o nystagmus/nodding movement of head• No h/o bowel/bladder incontinence• No h/o seizures/bed sores
• No h/o fever,rash,joint pains,headache,vomitings,convulsions,photophobia,altered
consciousness,head injury,chronic constipation,lethargy,cold intolerance,contact with case of TBprior to the onset of symptoms.• No h/o any drug intake• No h/o similar complaints in the family
BIRTH HISTORY
• Booked case.Received regular antenatal checkups,folic acid,iron tablets and immunization with tetanus toxoid.No h/o fever with rash/exposure to radiation/drugs/PIH/GDM/hypothyroidism.
• Born by elective caesarean section at term,cried immediately after birth,birth weight was 2.25kgs.
• On 4th DOL,h/o poor feeding and seizure like activity for which he received iv antibiotics for 14days.No h/o NNJ.
DEVELOPMENTAL HISTORY
• Delay in development of gross motor milestones. Can now walk without support for a distance of about 10 feet but stumbles and falls due to weakness.
• Can draw a triangle• Names weekdays• Knows times of the day
• NUTRITIONALLY has a deficit of 365 kcal and 25g protein
• IMMUNIZED as per age
SUMMARY
• 8yr old boy, born out of non consanguineous marriage,with no significant birth history,with delay in development of gross motor milestones,admitted with c/o progressive weakness of lower limbs,since 3yrs of age,with proximal involvement more than distal,with hypertrophy of calf muscles
• Most probably-myopathy -> primary-> ?Muscular dystrophy
EXAMINATION• PR- 98/min• RR-18/min• BP-120/70mmHg• Temp-98.6 deg F• 2nd degree wasting acc to IAP• 2nd degree stunting acc to Mc Laren’s• US:LS ratio 1.1 : 1• HC-49cms• CC-58cms• Grade 2 PEM acc to IAP
• Bulk of tongue >>• Swelling present over anterior aspect of neck
which moves with deglutition• No neurocutaneous markers/skin rash• Upperlimbs- appear normal• Lowerlimbs- calf muscles appear
hypertrophied bilaterally
CNS
• Alert,conscious,well oriented• Intact memory• Normal intelligence• Slurring of speech +• Cranial nerves intact
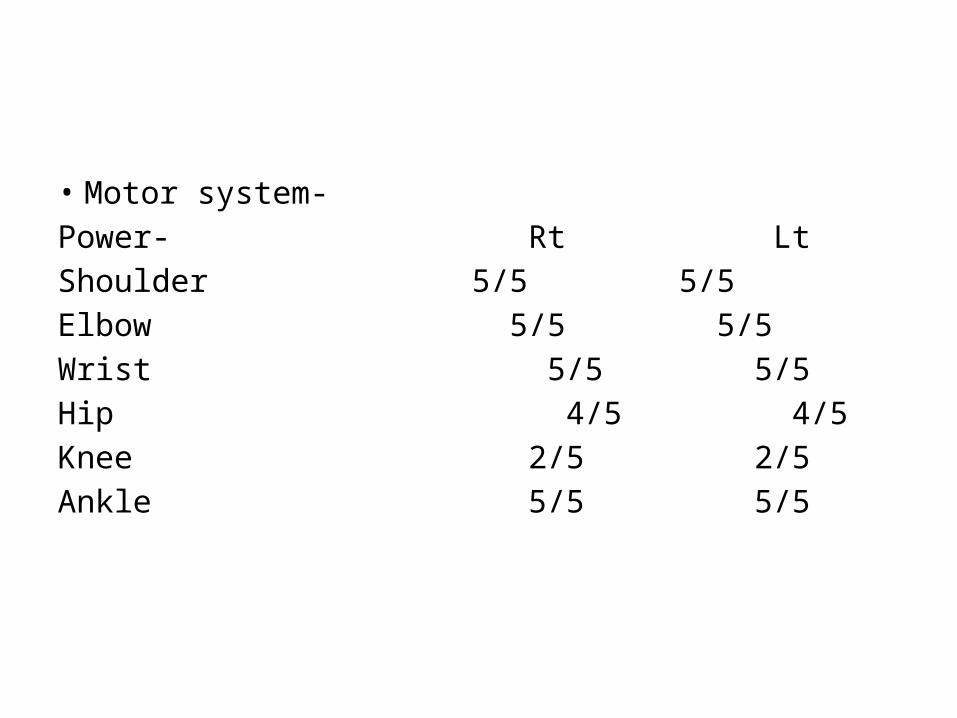
• Motor system-Power- Rt LtShoulder 5/5 5/5Elbow 5/5 5/5Wrist 5/5 5/5Hip 4/5 4/5Knee 2/5 2/5Ankle 5/5 5/5
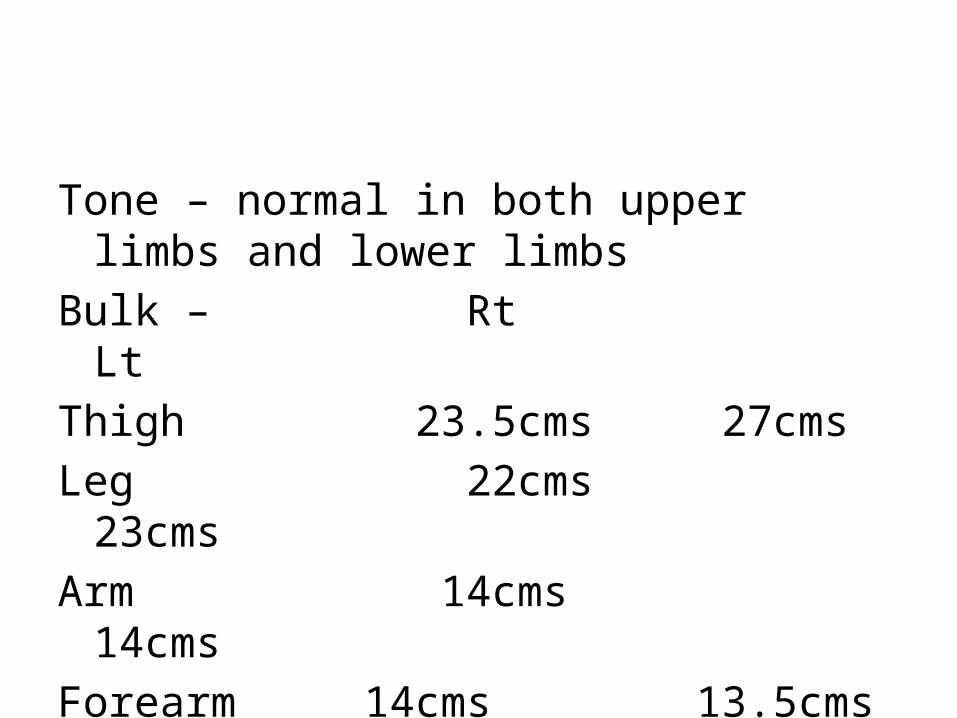
Tone – normal in both upper limbs and lower limbs
Bulk – Rt LtThigh 23.5cms 27cmsLeg 22cms 23cmsArm 14cms 14cmsForearm 14cms 13.5cms
• Relexes – Knee reflex absent bilaterallyAnkle reflex sluggish bilaterally• Waddling type of gait seen• Gower sign positive• Superficial,deep,cortical sensations intact• No cerebellar signs• Skull normal• Spine- scoliosis (rt.)• Autonomic system normal• No meningeal signs
RS – Normal vesicular breath sounds heard in all areas.No added sounds.
CVS- S1,S2 present.No murmurs.P/A-Scaphoid.Soft.Non tender.No organomegaly.
SUMMARY
• 8 yr old boy,with delay in development of gross motor milestones,with grade 2 PEM acc to IAP,with progressive weakness of lower limbs,proximal weakness more than distal weakness,most probably of muscle origin,with Gower’s sign positive,with hypertrophy of calf muscles,with waddling gait,with intact sensations,with absent knee jerks.
Clinical features
Serum CK level of 17000 iu/l
Blood PCR shows point mutation of dystrophin gene
Diagnosis: DUCHENNE’S MUSCULAR DYSTROPHY
DUCHENNE’S MUSCULAR DYSTROPHY
• Most common hereditary neuromuscular disease• X linked recessive inheritance• Mutation at Xp21 locus• Characterised by :1.Progressive weakness2.Hypertrophy of calves3.Proliferation of connective tissue in muscle4.Intellectual impairment
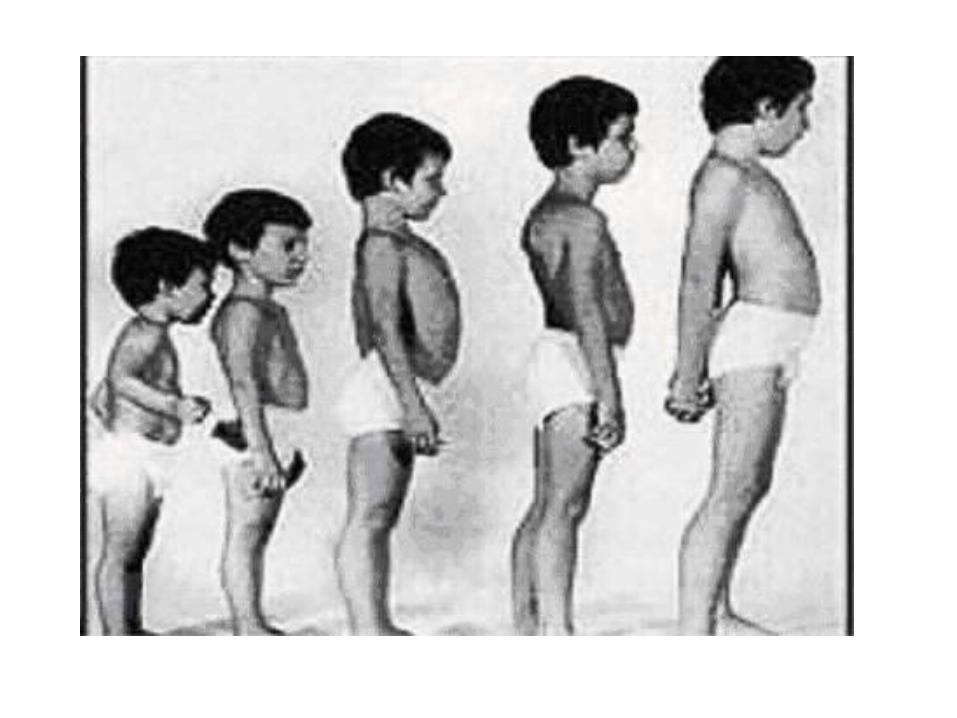
• Rarely symptomatic at birth/early infancy• Delay in development of early gross motor
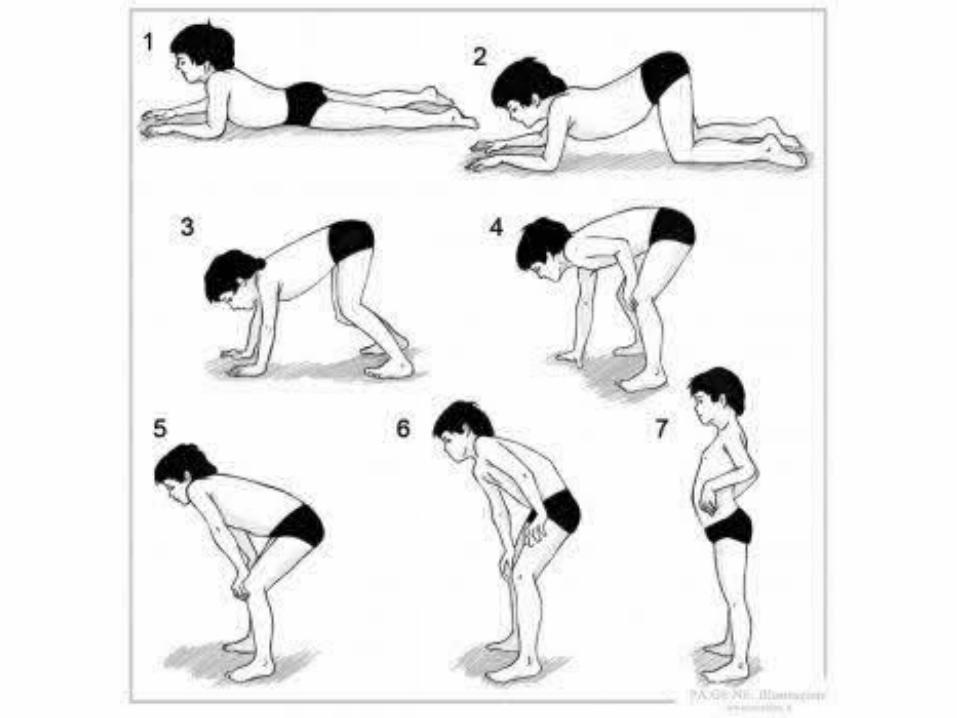
milestones• Gowers sign evident by age 3 yrs,fully
expressed by age 6yrs.• Waddling gait,toe walking,trouble in
running,walking upstairs
• Length of time a patient remains ambulatory varies.Most can walk with increasing difficulty until 10yrs age without orthopedic intervention
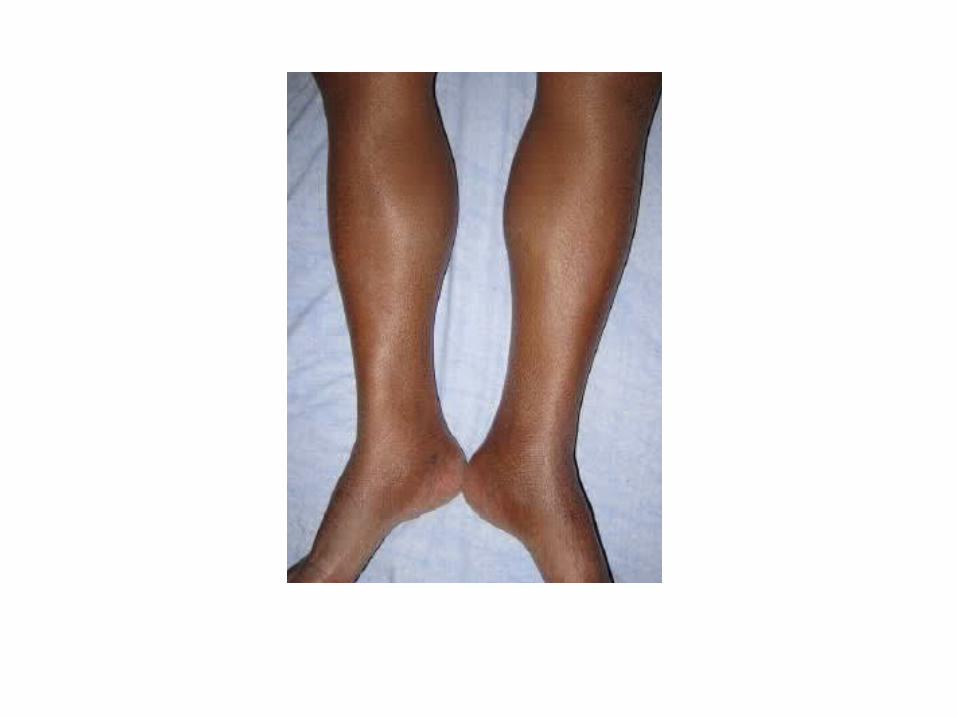
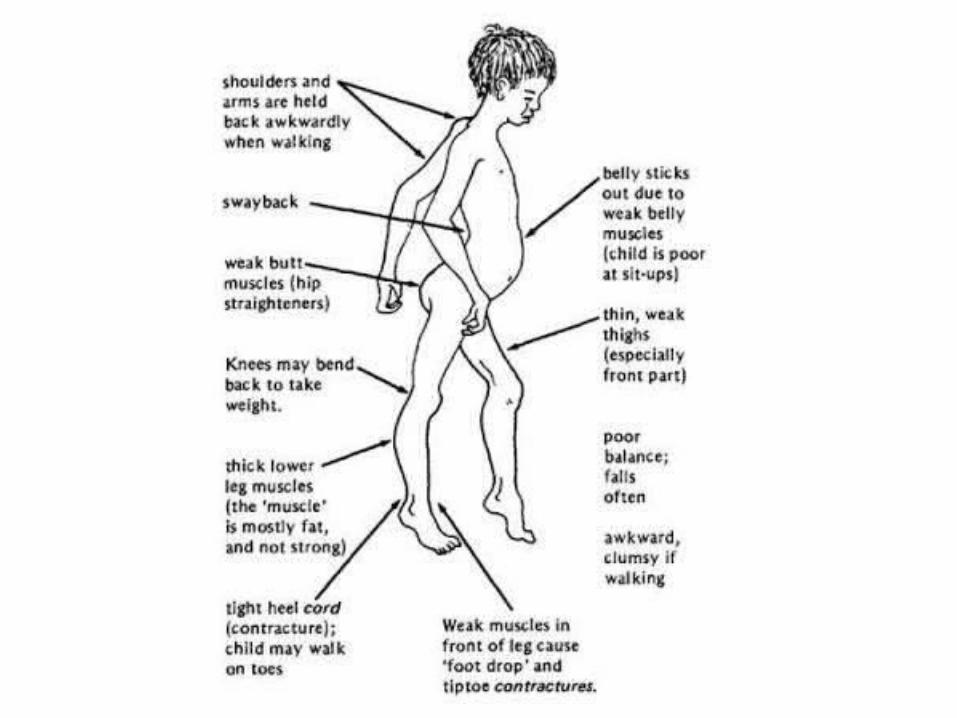
• With orthotic bracing,can walk upto 12yrs age• Scoliosis is common• Enlargement of calves and wasting of thigh
muscles seen
• Tongue hypertrophy +• Loss of knee deep tendon reflexes• Cardiomyopathy seen in 50-80% of patients with
this disease• Frequent pulmonary infections occur• Smooth muscle dysfunction,anal/urethral
sphincter involvement rare• Minor intellectual impairment occurs in all
patients• Increased risk of epilepsy• Death occurs by 18-20yrs age
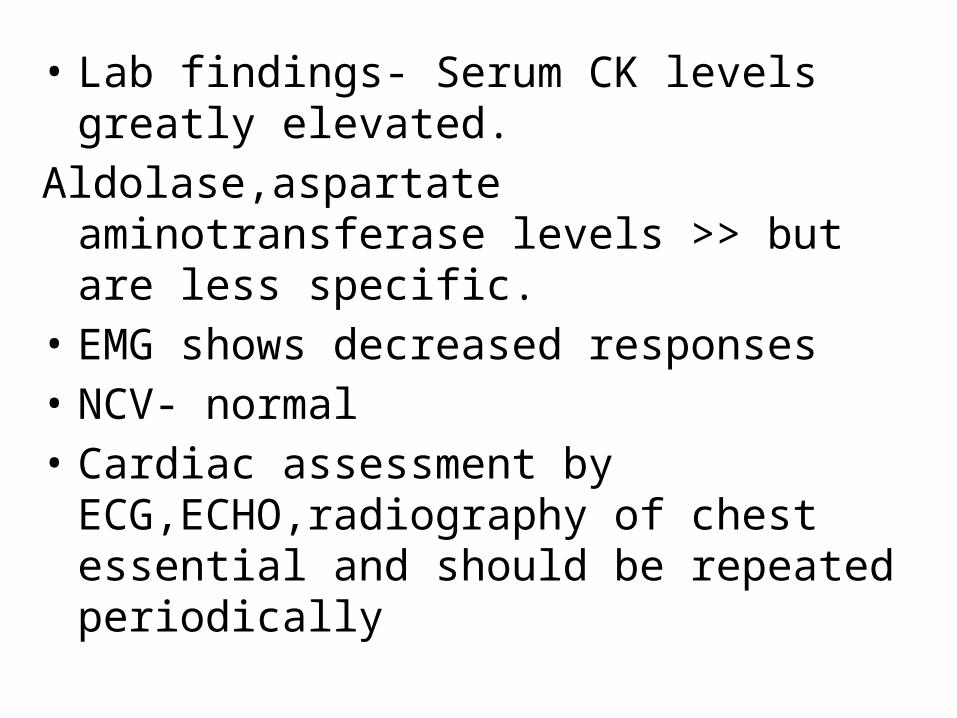
• Lab findings- Serum CK levels greatly elevated.Aldolase,aspartate aminotransferase levels >>
but are less specific.• EMG shows decreased responses• NCV- normal• Cardiac assessment by ECG,ECHO,radiography
of chest essential and should be repeated periodically
• Diagnosis –
Clinical features of DMD + elevated CK levels
PCR for dystrophin gene mutation ( muscle biopsy may be deferred)
If PCR is normal and clinical suspicion is high
More specific dystrophin immunocytochemistry done on muscle biopsy sections
• Muscle biopsy shows connective tissue proliferation,scattered degenerating and regenerating muscle fibres,mononuclear inflammatory cell infiltrates,dense fibres
DUCHENNE’S VERSUS BECKER’S
• Treatment- No cure.No method to slow progression
Good nutritionPhysiotherapy,ambulation delays contracturesPrompt treatment of respiratory infectionsDigoxin in cardiac failureSteroids(prednisone/prednisolone/deflazacort)
THANK YOU !



















