Embed Size (px)
Citation preview

Cervical carcinomaEndometrial carcinomaVulval disease

Second most common gynaecological cancer.
Annual risk for women over 35 years of age is 16 per 100,000
Peak incidence in between 45 and 55 years
Mean age 51.4 years
Recent trend towards younger age.
Cervical carcinoma

Cervical cancer usually grows outwards; creating a fungating mass. Occasionally inwards, enlarging the cervix.
More than 85% of cervical cancers are squamous cell carcinomas.
Rest are adenocarcinomas.
With time cancer spreads:1. Upwards to uterine cavity2. Downwards to vagina3. External iliac lymph nodes (47% cases)4. Obturator lymph nodes (20%)5. Hypogastric nodes (7%)6. Paracervical nodes (2%)


In earlier stage abnormal smear is the only way to detect as symptoms develop with invasive disease.
Per speculum examination and cervical is necessary if following symptoms are present:
1. Irregular per vaginal bleeding, particularly after intercourse
2. Pink vaginal discharge after urination
Diagnosis is confirmed by colposcopy or biopsy and endocervical curettage.
Diagnosis


Clinical staging is not able to detect spread to the liver and lymph nodes.
Ultrasound computed tomography (CT) and magnetic resonance imaging (MRI) are used.
CT can detects lymph node metastases, plus liver, urinary tract and bone involvement.
MRI has a role in detecting parametrial spread and is useful to evaluate pregnant women as it avoids radiation exposure to fetus.

International Federation of Obstetrics and Gynaecology (FIGO) classification for staging of carcinoma of uterine cervix
Stage Description
Stage 0 Cervical intraepithelial neoplasia 3 (CIN3)Carcinoma in situ
Stage 1 The carcinoma is confined to the cervix1A Invasion can only be diagnosed by microscopy with maximum depths ≤5.0mm and horizontal spread of ≤7.0mm1B Clinically visible
Stage 2 The carcinoma invades beyond the uterus but does not reach pelvic wall or lower third of vagina 2A No obvious parametrial involvement2B Obvious parametrial involvement
Stage 3 The carcinoma has reached the wall of the pelvis and/or the lower third of the vagina3A Reached lower third of the vagina3B Extension to pelvic wall or hydronephrosis or non functioning kidney
Stage 4 The carcinoma has spread beyond the true pelvis or has invaded the bladder or rectum4A Spread to adjacent organs4B Spread to distant organs


Lymph node involvement and 5 year survival rates of cervical carcinoma related to stage of the disease
Stage Lymph node involvement 5-year survival (%)
0 0 100
1A 0.5 95
1B 15 80
2A 25 66
2B 35 64
3 55 35
4 >65 14

Treatment of microinvasive (stage 1A) cancer depends on whether the woman wants to retain her uterus.
A cone biopsy with clear margins is an adequate treatment, otherwise a simple hysterectomy.
Stage 1B and early 2A is treated by radical hysterectomy followed by radiotherapy.
Radical hysterectomy involves removal of parametrium and pelvic lymphadenectomy and radiotherapy includes a combination of external beam and intracavity radiation.
Treatment

In younger women the ovaries can be preserved and relocated out of the potential radiotherapy field.
More advanced cervical carcinoma is treated by radiotherapy.
Bladder dysfunction, lymphoedema and sexual dysfunction are complications of treatment.
Chemotherapy has been used in both early stage (1B) and advanced disease.
This improves the 2 year survival rate from 79 to 89% and 63 to 75%


Disease of women in their middle years. Peak incidence in 55-65 year age group.
Women whose menopause is delayed beyond the age of 55, who are relatively infertile, and overweight or hypertensive are more likely to develop endometrial cancer.
If endometrial hyperplasia shows a pathology with complex hyperplasia with atypia 17-43% of women will develop endometrial cancer unless treated.
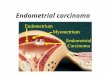
Endometrial carcinoma

The tumor may originate in any part of endometrium and grows slowly, tending to spread over a part of the endometrium before invading myometrium.
If the growth starts in lower part of uterus, the fungating mass block the cervix and fluid or pus may collect in uterus(pyometra)
Various histological patterns of adenocarcinoma are found on the histological examination of an endometrial biopsy or curettage.
The more undifferentiated the endometrial cells the worse the prognosis.


Bloody vaginal discharge.
Irregular bleeding; slight in amount and recurrent.
Watery vaginal discharge is uncommon.
Examination shows normal size uterus unless there is associated myomata or pyometra.
Any peri- or postmenopausal woman who has symptoms of irregular bleeding per vaginam or bloody vaginal discharge must be examined and endometrial and endocervical canal tissue sampled.
Clinical features

Using a hysteroscope the uterine cavity can be inspected and a biopsy taken under direct vision.
An alternate is to measure endometrial thickness by transvaginal ultrasonography.
If the endometrium is less than 5mm thick, endometrial cancer can be excluded.
Confirmation by hysteroscopy and biopsy or by curettage either using a biopsy curette or a formal curettage under general anesthesia

Two biopsy curettes are used Gynescan and Pipelle.
They are introduced through the cervix and rotated in the uterine cavity.
It is relatively a painless procedure. 60%
women experience discomfort or pain.
A negative biopsy in a symptomatic woman should be followed by a formal hysteroscopy and biopsy/curettage under anesthesia as there is a 10% false negative rate


Mass screening for endometrial cancer is neither practical nor justifiable with current techniques.
Pap smears detect 50% cases but is too unreliable to screen asymptomatic women.
Three groups are at high risk:1. Postmenopausal women taking unopposed oestrogen
therapy2. Females with family history of non-polyposis colorectal
cancer3. Premenopausal women with anovualatory cycles
They should be offered regular surveillance Women using tamoxifen are at risk if they have abnormal
vaginal bleeding
Screening



Over 75% women are diagnosed in early stage.
Total hysterectomy and bilateral oophorectomy is the treatment of choice.
Pelvic lymphadenectomy is performed with:1. Grade 3 disease (>50% non squamous or non morular
growth pattern)2. Grade 2 (6-50% non squamous or non morular growth
pattern)3. Tumors >2cm in diameter 4. Adenosquamous or clear cell or papillary serous carcinoma 5. >50% myometrial invasion6. Those who have cervical extension
Treatment

The excised uterus is examined histologically; if more than half of myomtrium’s thickness is invaded either whole pelvis irradiation (50Gy over 5 weeks) or hormone treatment is given.
3-4weeks after hysterectomy intravaginal irradiation is given of 40Gy to prevent recurrence in vagina.
Vagina may become stenosed making intercourse uncomfortable.
Bladder and rectal symptoms may arise as a result of radiation damage.
Medroxyprogesterone acetate 200-400mg is given orally if patient is unfit for surgery.

Depends on the stage of disease, the histological grade of tumor, the age and health of woman.
Women who have received treatment for low stage endometrial carcinoma and who have severe menopausal symptoms may be prescribed hormonal replacement therapy with no increased development of any residual cancer.
Follow up is recommended at 4 monthly intervals for first 3 years and annually thereafter.
The woman is examined abdominally and vaginally, checked to detect any large lymph nodes
Prognosis

The recommended treatment and 5-year survival rate of endometrial cancer related to the stage of the disease
Stage Recommended treatment 5-year survival rate (%)
1A Hysterectomy 88
1B Hysterectomy followed by vaginal vault and pelvic irradiation
80
IIA As for carcinoma of cervix 77
IIB As for carcinoma of cervix 67
III Hysterectomy and bilateral salpingo-oophorectomy if feasible plus radiation therapy
40
IV Palliative surgery, radiation therapy and progestogenic therapy
10

This condition is being increasingly diagnosed during colposcopic investigation of women presenting with pruritus vulvae or vulval warts.
The treatment options are watchful expectancy or local excision of the area in high grade VIN 3
Follow up is important as one third of patients have recurrent disease.
Between 4 and 8% of women with Paget’s disease have an underlying adenocarcinoma.
Treatment is by wide excision including the underlying dermis.
Long term surveillance is needed due to recurrence.
Vulval intraepithelial neoplasia (VIN)

Accounts for 3% of genital tract cancers.
Affects elderly women.
Growth starts as a lump or an ulcer on one labium majus (50% of cases) or on a labium minus (25% of cases)
In some cases various areas are affected.
In recent years a number of young women have been presenting with malignant change in a vulval condyloma.
Carcinoma of the vulva

Affected woman may have vulval itching for months and years or has had few symptoms or noticed the ulcer recently.
The lesion is hard nodule or ulcer with sloughing base and raised edges, which maybe small or large depending on duration of disease.
If cancer is large, lymph node involvement may have occurred in more than 50% of cases
Clinical


Either simple vulvectomy with dissection of the inguinofemoral lymph nodes for stage 1 disease (tumor = 2cm) or radical vulvectomy for stage 2 (confined to the vulva and >2cm in diameter) with inguinal, femoral and pelvic lymphadenectomy.
Wound necrosis is a troublesome complication after radical vulvectomy, and persistent leg oedema occurs in 20% of women.
Treatment

For advanced disease treatment needs to be individualized and depends on the degree of spread, age of woman and her general state of health.
Modalities employed include surgical excision, radiotherapy and chemotherapy.
5-year survival is 70% overall, for stage I 90%, stage II 75%, stage III 50% and stage IV 15%


Thank you