Embed Size (px)
Citation preview
Childhood Obesity—A Manmade Crisis
Mahesh Hiranandani
M.D

Our futureOur future
A growing crisis—Agenda today
• How significant is the problem……..
• National data …Regional figures
• When does this all begin…..
• Is parental attitude a cause for concern

Obesity: Consequences & Prevalence In India
• 45 million under 5 yr estimated to be obese.(22Million in India)
• Global prevalence of 10% in 5-17 yr age group.( 17% India)
• Obesity figures up by 23% from 1995 to 2010.
• One in six women and one in five men are overweight in INDIA.
• OBESITY figures are bulging dangerously at 70 millions.
• Almost 39% adults from Delhi fulfill the criteria for overweight.
• Private v/s Public school 25% v/s 9% (INDIA)
• Delhi Private school survey 34%.
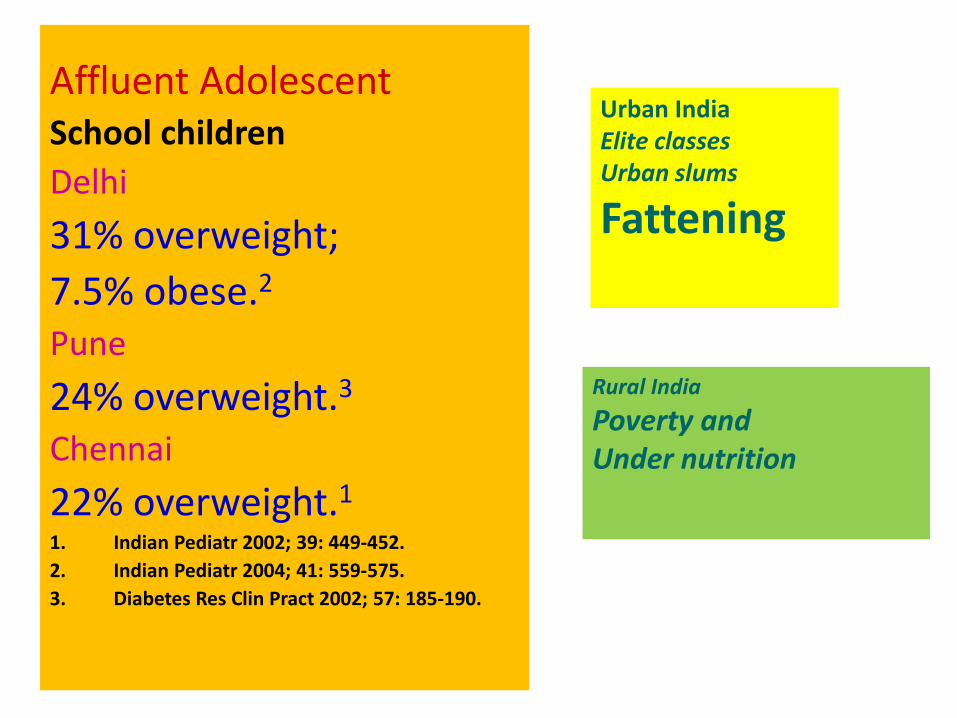
Affluent Adolescent School children
Delhi
31% overweight;
7.5% obese.2
Pune
24% overweight.3
Chennai
22% overweight.1
1. Indian Pediatr 2002; 39: 449-452.
2. Indian Pediatr 2004; 41: 559-575.
3. Diabetes Res Clin Pract 2002; 57: 185-190.
Rural India
Poverty and Under nutrition
Urban IndiaElite classes Urban slums
Fattening
Obesity & Life style diseases ……Importance for adolescent age
• Adolescent physicians and pediatricians have an important role in the prevention and control of the ‘epidemic.’ of Life style disorders
• As they begin in childhood (or even earlier, in fetal life), and Manifest due to interactions & accumulation of various risk factors, throughout the life cycle.
WHO/NMH/NPH/ Life course perspectives on coronary heart disease, stroke, and diabetes. WHO, Geneva, 0.1.4:2001.
Fall CHD. The fetal and early origins of adult disease. Review. Indian Pediatr 2003; 40:480-502
What is obesity ????
OBESITY is defined as a 20 % excess of calculated ideal weight for age ,sex and height of a child. It is associated with excess accumulation of fat in subcutaneous tissues & other organs of body.

Criteria for Chilhdhood obesity
• Weight to height charts
Obese if wt 20% more over recommended.
• Body fat percentage
Boys > 25% body fat
Girls > 31% body fat
• Body mass index(BMI)
Reliable indicator of body fat. Most popular.
Measures weight relative to height.
Inexpensive, easy to perform, age & sex specific
Body mass index(BMI)• Measure height of child to nearest centimeter.
• Weigh the child to nearest decimal faction in kg.
BMI == Weight in kg/ (Height in meters)x2
Plot the BMI on BMI for age /sex percentile chart
Weight status category Percentile range
Underweight <5%
Normal 5-85%
Overweight 85-95%
Obese > 95%
Interpretation of BMI
• BMI is a screening tool not a diagnostic one…
Heavy child may have high BMI for age . To determine if he is obese a few more tests are reqd.
• Age & sex specific for children & teens.
Amount of body fat changes with age.
Body fat quantum differs between boys & girls.
BMI age percentile chart for boys & girls is an accurate tool
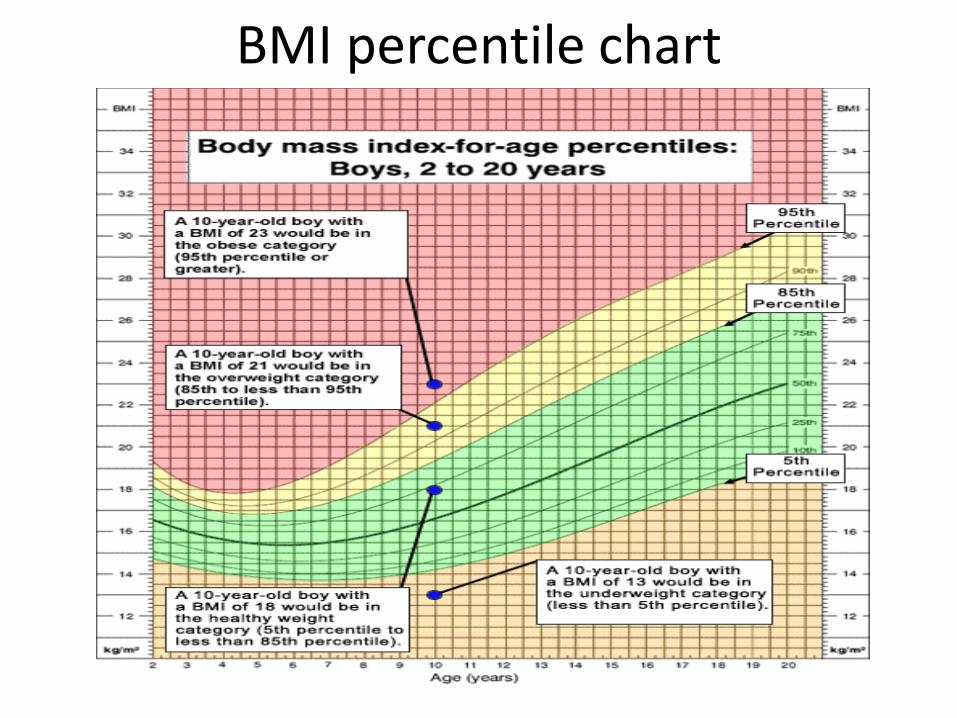
BMI percentile chart
Causes of childhood obesity
There are two major and basic causes of obesity:
* Too many calories in
* Too few calories out
Phases in evolution of obesity
• Role of Intrauterine growth pattern
• Relationship between birth weight & Future BMI.
• Insulin resistance ….LBW & obesity.
• Consistently protective role of breast feeding .
• Early menarche predisposes to obesity
• 80% obese adolescents will become obese adults.
Barker’s Hypothesis FOAD 1986
• Fetal origins of adult-onset diseases (FOAD)
• Under nutrition and unfavorable intrauterine environment at critical periods in early life can cause permanent changes (in both structure and function) in developing systems of the fetus (i.e. programming).
• May manifest as disease over a period of time due to `dysadaptation’ with changed environmental circumstances
Barker DJP. Mothers, babies and health in later life. Edinburgh: Churchill Livingstone, 1998.
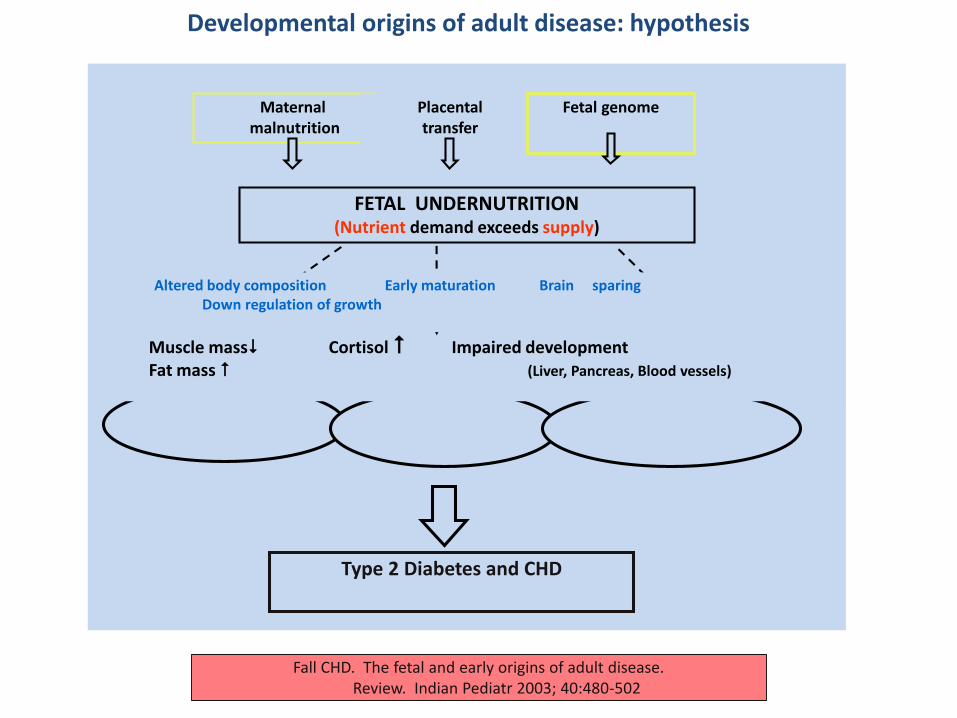
Maternal malnutrition
FETAL UNDERNUTRITION(Nutrient demand exceeds supply)
HYPERLIPIDAEMIAHYPERTENSION CENTRAL OBESITY INSULIN RESISTANCE
Type 2 Diabetes and CHD
Muscle mass Cortisol Impaired developmentFat mass (Liver, Pancreas, Blood vessels)
Placental transfer
Fetal genome
Altered body composition Early maturation Brain sparingDown regulation of growth
Fall CHD. The fetal and early origins of adult disease. Review. Indian Pediatr 2003; 40:480-502
Developmental origins of adult disease: hypothesis
Characteristics of obesity in India
• Frank obesity not as high as in the WestBut body composition & metabolism of Indians (asians in general) make them especially prone to ‘adiposity’ (fat content in the body) and its consequences.
• South Asians have at least 3 to 5% higher body fat for the same BMI as compared to Caucasians.
• The fat is typically located ‘centrally’ (i.e. waist, trunk) and around visceral organs - metabolically more dangerous than peripheral fat.
Indian cohort studies –pune -1
• Deleterious effects of accelerated weight gain in childhood i.e. ‘crossing of centiles’ especially in LBW babies.
• Indices of insulin resistance and CV risk factors were found to be highest in those that were born `small’ but were big by 8 years even though they were not obese in absolute terms.
• Accelerated growth in childhood is associated with early puberty and greater risk of obesity.
Bavdekar A, Yajnik CS, Caroline HD, Bapat S, Pandit A, Deshpande V., et al. Insulin resistance syndrome in 8-year-old Indian children – Small at birth, big at 8 years, or both ? Diabetes 1999; 48: 2422 – 2429.
Indian cohort studies –pune -2
Maternal Nutritional Studies have shown convincingly that this high risk body composition is present even at birth,
i.e. lower birth weight, lower muscle mass but relatively high fat mass and hyper insulinemia (`thin fat’ phenotype)
• It is possible that such fat offers survival benefits to newborns but also endangers predisposition to insulin resistance from birth itself.
Yajnik CS, Fall CHD, Koyaji KJ, Hirve SS, Rao S, Barker DJP, et al. Neonatal anthropometry: the thin-fat Indian baby. The Pune Maternal Nutrition Study. Int J Obes 2003;27:173-180.
“ Thin-fat “ baby
• Newborns, even relatively small at birth (BW < 2.9 kg) reported to have greater subscapularskin fold thickness, which is shown to correlate well with truncal obesity
• Also been shown that this adiposity tracks to 4 years of age
Krishnaveni GV, Hill JC, Veena SR, Fall CHD. Truncal obesity is present at birth and in early childhood in south Indian children. Indian Pediatr 2005; 42: 527-538
Agarwal KN, Saxena A, Bansal AK, Agarwal DKPhysical growth assessment in adolescence Indian Pediatr 2001; 38:
Causes of Obesity
• Environmental
Dietary habits.
Physical inactivity.
• Genetic
Obese parents obese children
Prader willi synd, Bardet biedl synd.
• Endocrinal
Hypothyroidism, Cortisol excess, Gh def
Increased eating
• 10 calories extra per day can result in ½ kg weight gain per year.
• 150 calories extra per day== 7 kg per year.
• Cut out one cookie per day to lose those 7 kgs in year,.
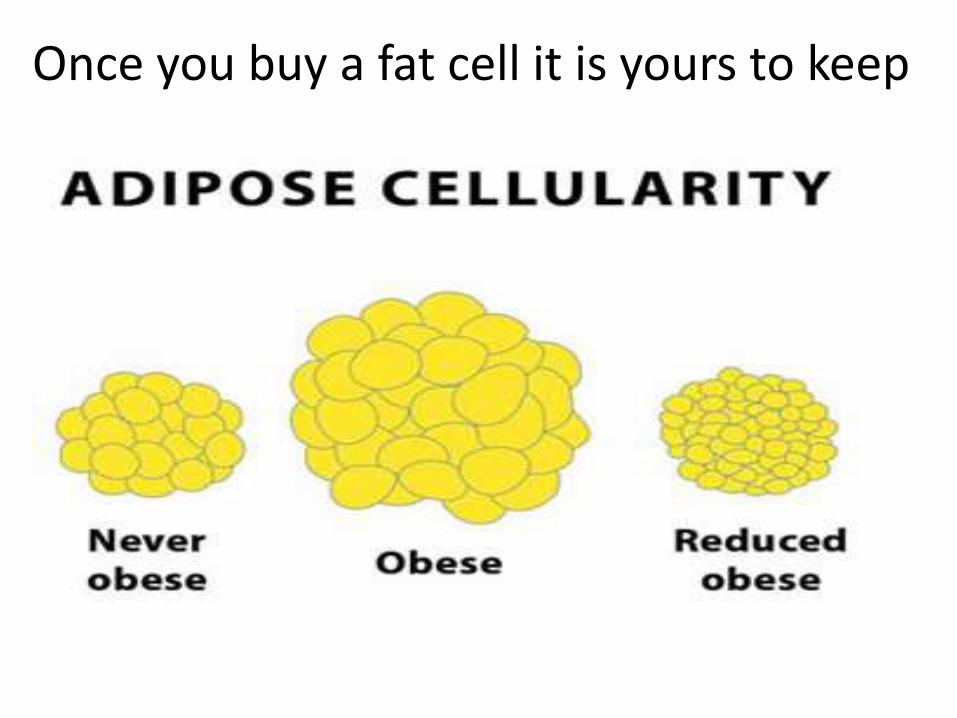
Once you buy a fat cell it is yours to keep
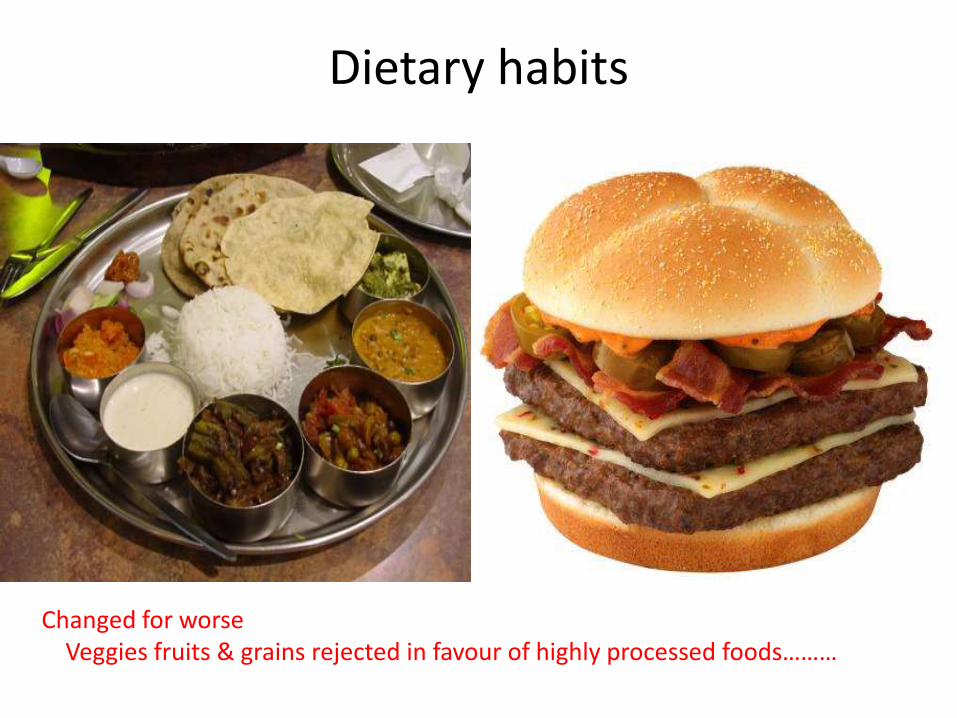
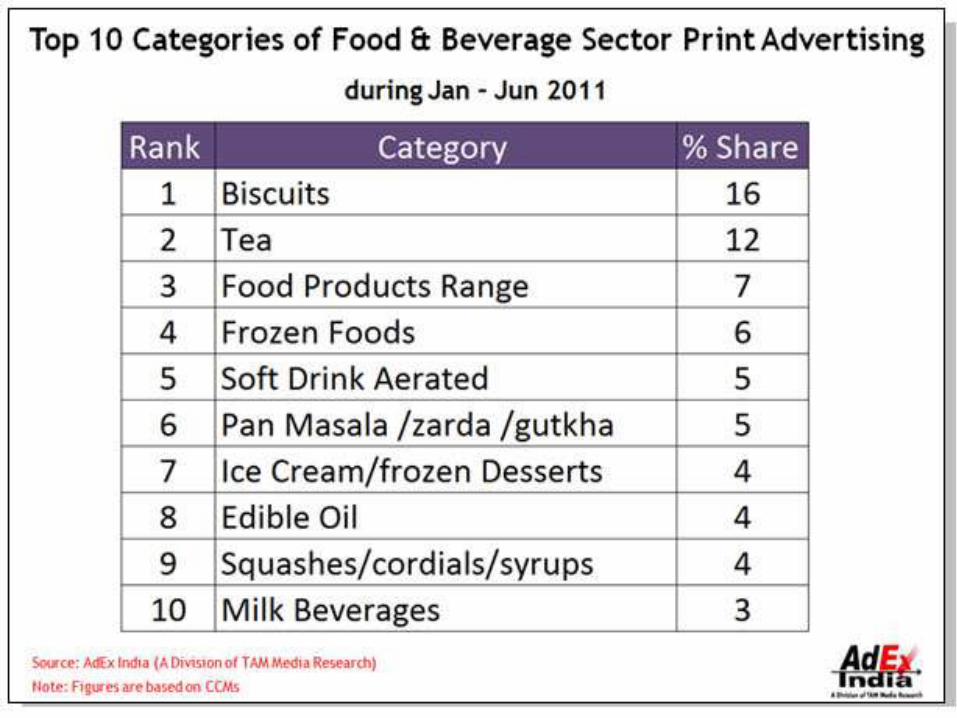
Dietary habits
Changed for worse Veggies fruits & grains rejected in favour of highly processed foods………
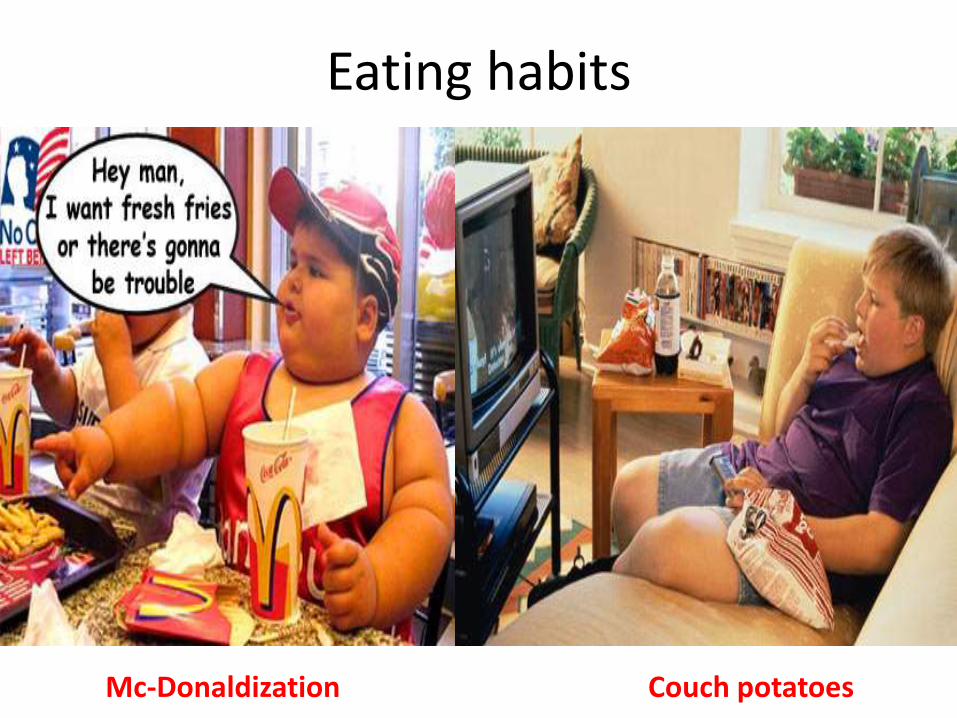
Eating habits
Mc-Donaldization Couch potatoes

Sugar laden drinks80% of urban children drink these daily
Each can contains 150-180 cals
One can soda increases risk by 60%
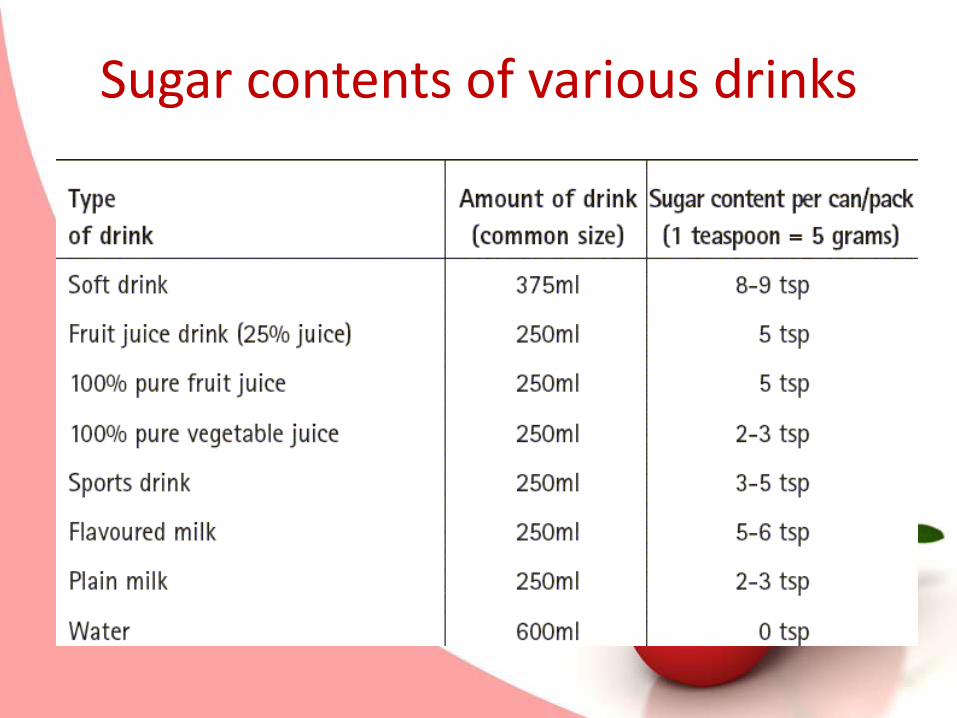
Sugar contents of various drinks
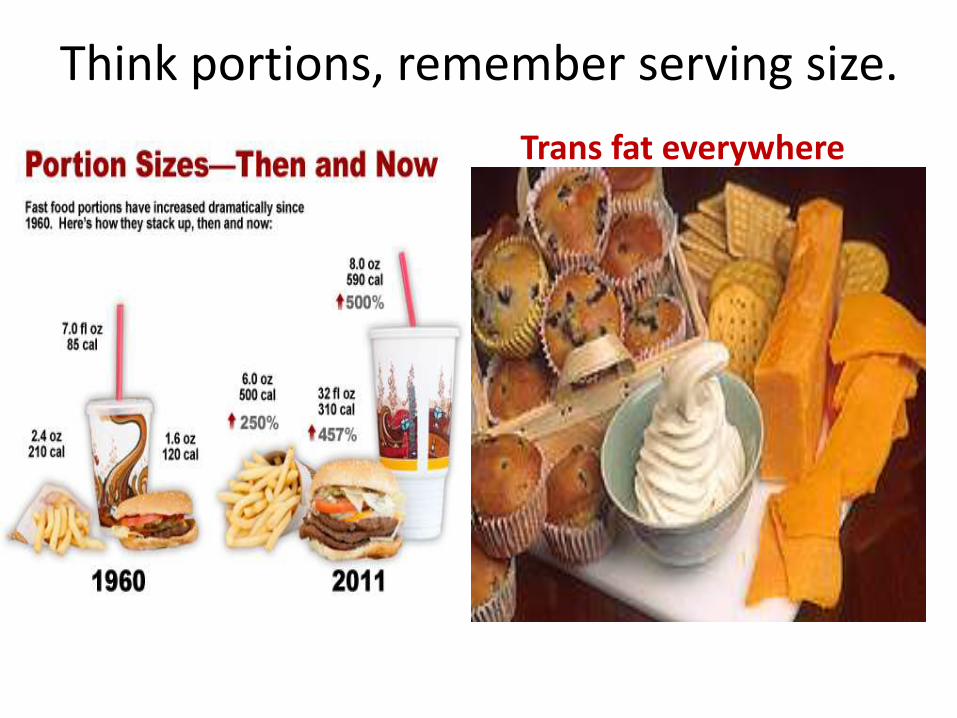
Think portions, remember serving size.
Trans fat everywhere
Trans fat
• French fries
• Samosa kachori
• Cookies & cakes
• Ice creams/Souffles
• Wafers/Chips/kurkure
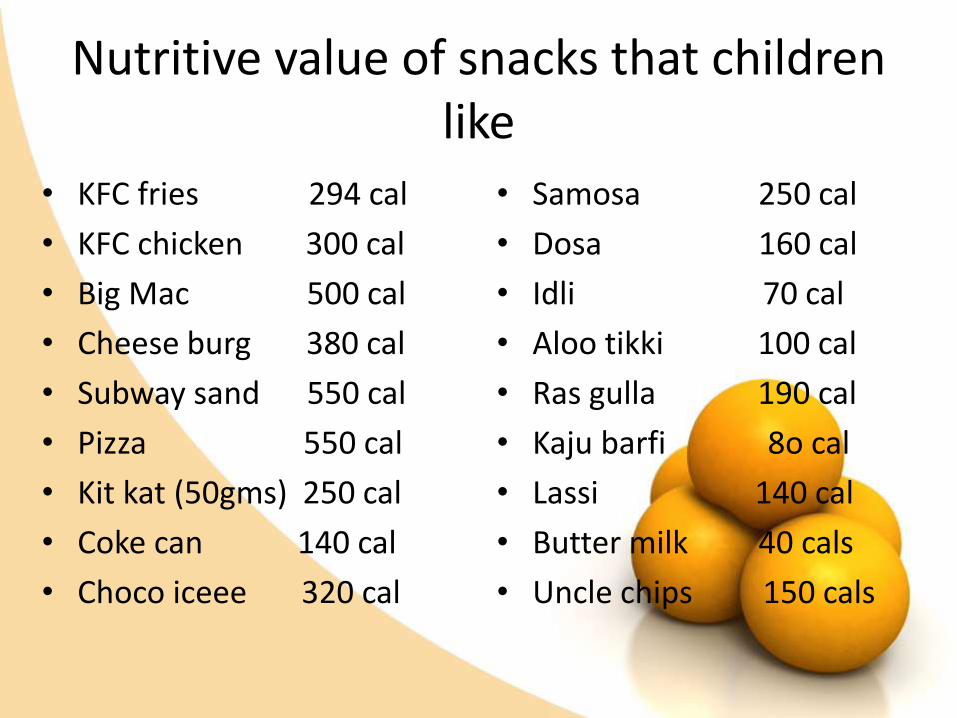
Nutritive value of snacks that children like
• KFC fries 294 cal
• KFC chicken 300 cal
• Big Mac 500 cal
• Cheese burg 380 cal
• Subway sand 550 cal
• Pizza 550 cal
• Kit kat (50gms) 250 cal
• Coke can 140 cal
• Choco iceee 320 cal
• Samosa 250 cal
• Dosa 160 cal
• Idli 70 cal
• Aloo tikki 100 cal
• Ras gulla 190 cal
• Kaju barfi 8o cal
• Lassi 140 cal
• Butter milk 40 cals
• Uncle chips 150 cals

Gone are the days…………….
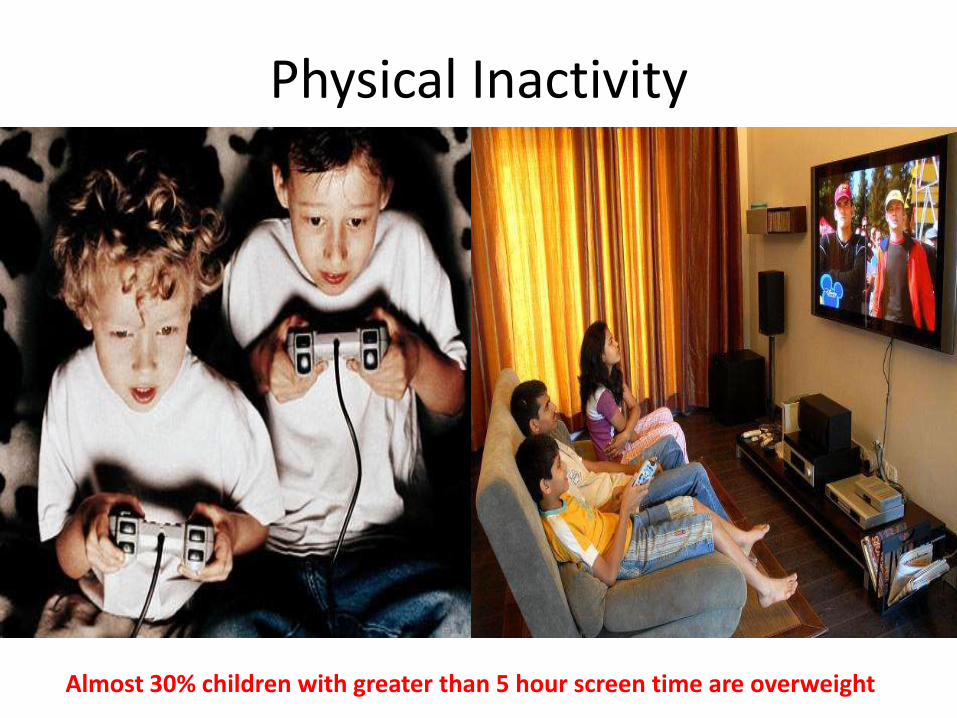
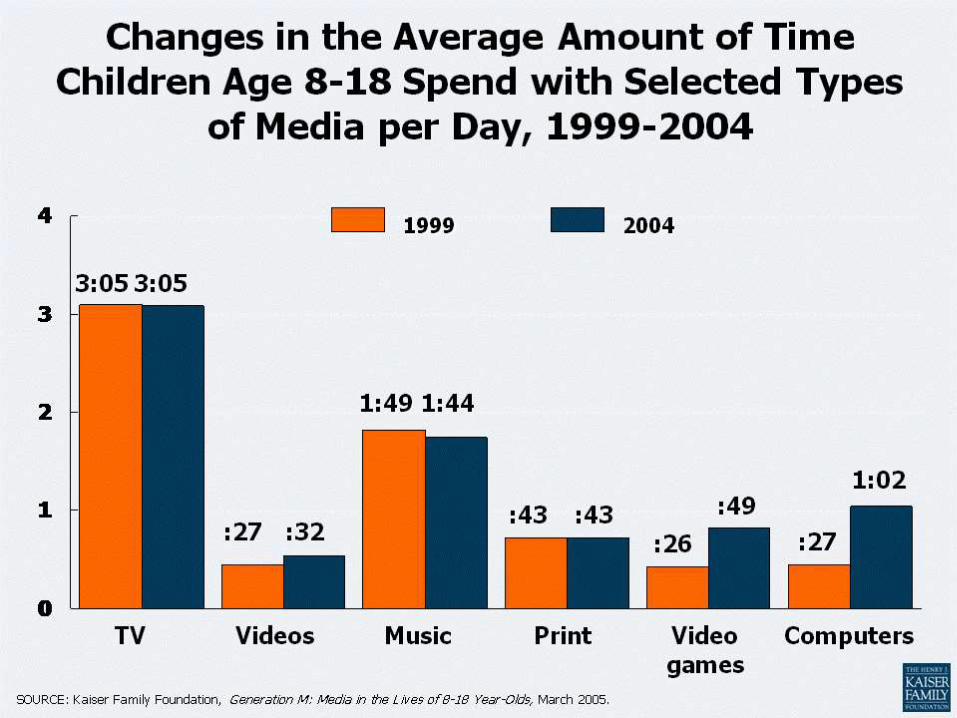
Physical Inactivity
Almost 30% children with greater than 5 hour screen time are overweight
How media trick children’s taste buds
Wrapping affects their preferences.
Even carrots,milk & apple juice tasted better.
Kids see Mc-Donalds label and start salivating.
Parental misconception
• Chubby child is considered a healthy child.
• To keep a child in that state ….It is essential to overfeed.
• Mother is the Meal-planner of a baby’s diet.
• Even educated parents lack practical knowledge.
• Wide gap between nutrition Knowledge & behaviour.
• Indian snacks are considered healthy.
• Junk food provides respite from healthy food planning.
What’s our Dilemma & Role ?
“My child is not fat but big boned.”“He hardly eats…….only one dry chapati & sabzi….”
Reject these notions in a firm yet subtle manner
OUR ROLE
• To Educate,Educate & Educate.One at a time.ChildrenAdults
Treatment of childhood obesityTreatment depends upon the age & associated problems.
* Below 7 years;
Goal is to maintain weight than weight loss.
Allows the child to add inches not kilograms.
* Above 7 years
Weight loss is recommended at a rate of 1kg/mon
5 2 1 0Every day
• 5 or more fruits & vegetables
• 2 hours or less recreational screen time*
• 1 hour or more of physical activity
• 0 sugary drinks, more water & low fat milk
* Keep TV computer out of bed room. No screen time under age of 2 years.
Thanks for your attention
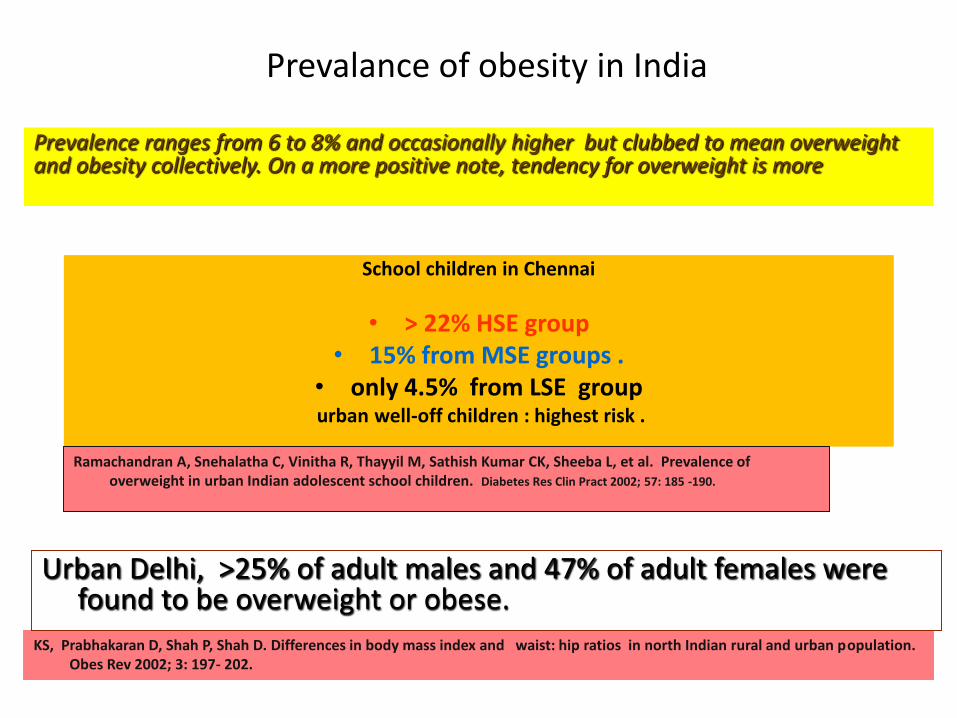
Prevalance of obesity in India
School children in Chennai
• > 22% HSE group • 15% from MSE groups .
• only 4.5% from LSE groupurban well-off children : highest risk .
Ramachandran A, Snehalatha C, Vinitha R, Thayyil M, Sathish Kumar CK, Sheeba L, et al. Prevalence of overweight in urban Indian adolescent school children. Diabetes Res Clin Pract 2002; 57: 185 -190.
KS, Prabhakaran D, Shah P, Shah D. Differences in body mass index and waist: hip ratios in north Indian rural and urban population. Obes Rev 2002; 3: 197- 202.
Prevalence ranges from 6 to 8% and occasionally higher but clubbed to mean overweight and obesity collectively. On a more positive note, tendency for overweight is more
Urban Delhi, >25% of adult males and 47% of adult females were found to be overweight or obese.

Where do parents begin
• Remember it took time for our children to gain weight , and it will take time for them to lose weight.
• Aim for small steps to begin the process.
MONITORING AND COUNSELLING THE ADOL
• Most FOAD related disorders can be prevented or effectively managed if picked up early in life.
• Main focus of preventive programmes should be directed towards prevention of obesity throughout childhood and adolescence.
• Public health campaign directed towards life style changes in the family / society as a whole.
• Benefits of healthy eating, increased physical activity & reduction in sedentary activities have to be inculcated from early age.
• School based programmes most likely to be successful but health authorities and media have an important role to play to spread awareness.
Greydanus DE, Bhave Swati. Obesity and adolescents. Time for increased activity. Indian Pediatr 2004; 41: No 6
Acanthosis NigricansIndian studies
• This simple diagnostic marker in a clinical examination in office practice was seen in seen in 20% of obese adolescents,
• who also had high insulin and C-peptide levels with normal HbA1c level
Subramaniam V, Jayashree R, Rafi M. Prevalence Overweight and obesity in Chennai 1981& 1998. Indian Pediatrics 2003; 40: 332-336.
Identify a role model for your child amongst your friends……….
Common causes of decreased physical activity
• Increased concerns of safety issues outdoors.
• Increased TV viewing, Computer use, video game playing.
• Reduced physical education and recess in school.
• Over-scheduling so family life is disrupted.
• Decreased family activity time together.

Indian cohort studies-delhi
• An increase of BMI of 1 SD from 2 to 12 years of age, • increased the odds ratio for disease (IGT / DM) by
1.36. in young adults
• It is now evident that our traditional understanding of concepts of `catch up growth’ in childhood, and ‘healthy’ weight gain during adolescence may need redefining.
Bhargava SK, Sachdev HPS, Fall CHD, Osmond C, Lakshmy R, Barker DJP, et al. Relation of serial changes in childhood body-mass index to impaired glucose tolerance in young adulthood
New Eng J Med 2004; 350: 865-875.

Activity history
• Ability to walk or ride a bike to school.
• Time in play.
• Schools curriculum.
• After school and weekend activity.
• Activity of both parent.
• Screen & media time.
Dietary history
• Caretakers who feed the child.( Maid or grandparents)
• Food diary
High calorie foods that are low in nutritional value
Fast foods /Ready to eat snacks
Intake of juices sodas & sports drinks
Milk intake ( Formula,buffaloes)
Psychosocial history
• Depression
• School & social issues
• Substance abuse
There are many ways to celebrate at school
• Non food ways ( Active game chosen, visit to a factory, community service at orphanage).
• Healthy snacks ( fruit tray/smoothie,Idli,Kathi rolls).
• Healthy non sugar drinks ( Lemonade, lassi,Ice tea).
Unfortunately parents offer the stiffest resistance
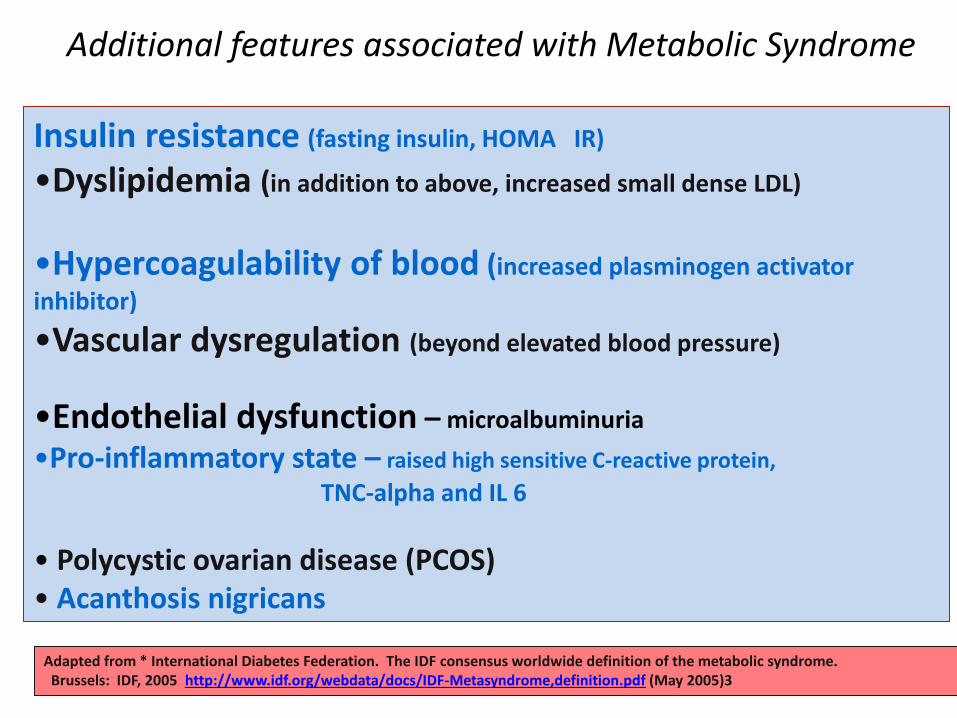
Additional features associated with Metabolic Syndrome
Insulin resistance (fasting insulin, HOMA IR)
•Dyslipidemia (in addition to above, increased small dense LDL)
•Hypercoagulability of blood (increased plasminogen activator
inhibitor)
•Vascular dysregulation (beyond elevated blood pressure)
•Endothelial dysfunction – microalbuminuria
•Pro-inflammatory state – raised high sensitive C-reactive protein,
TNC-alpha and IL 6
• Polycystic ovarian disease (PCOS)• Acanthosis nigricans
Adapted from * International Diabetes Federation. The IDF consensus worldwide definition of the metabolic syndrome.Brussels: IDF, 2005 http://www.idf.org/webdata/docs/IDF-Metasyndrome,definition.pdf (May 2005)3
Tips for the teachers
Just another thing to add to your
already busy day!
Academic pressure
• High burden of school work.
• Academic Competitiveness.
• Hopeless education system.
• Pressure to achieve grades & careers.
•
10 strategies for success
• Encourage healthy choices for snacks and celebrations.
• Encourage water & low fat milk instead of sugar laden drinks.
• Discourage the use of food as reward, use physical activity as a reward.
• Participate in local or state activity that promote activity & healthy eating.
• Include community groups in wellness promotion.
• Involve & educate families in initiatives that promote activity & healthy eating.
• Incorporate physical activity into the school day.
• Develop 5-2-1-0 friendly policy.
• Collaborate with parents,nutritionist & teachers.
• Educate, educate & educate children as well as parents on evils of obesity.
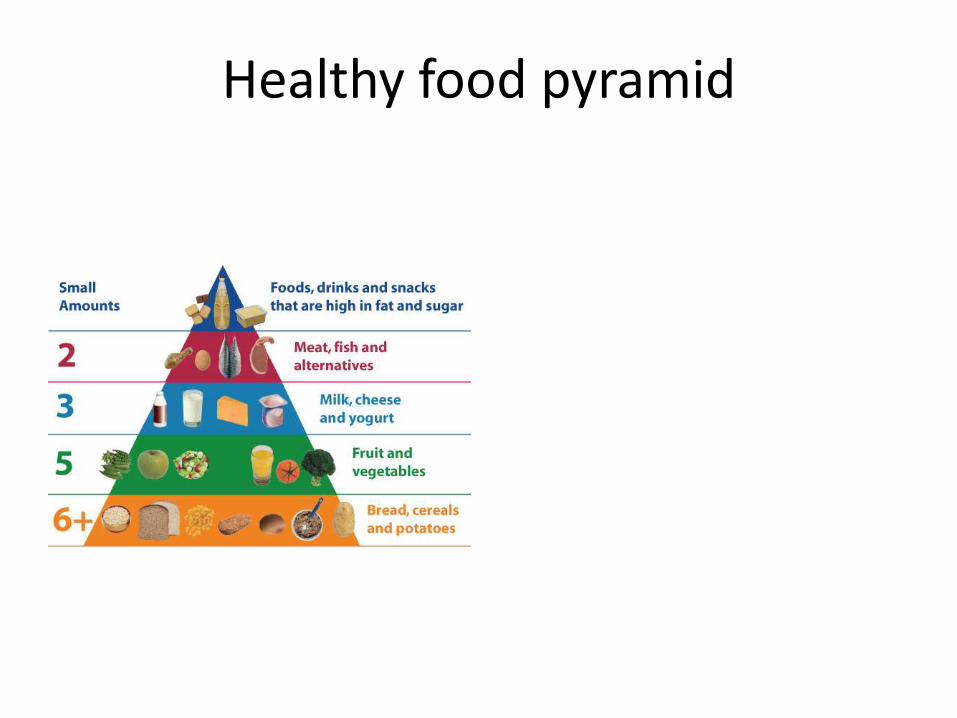
Healthy food pyramid
Obesity statistics
• 40% children eat out once in a week.
• 70% children eat chips once or more in a week.
• 45% eat burger/pizza/fries once a week.
• 60% drink cola once or more in a week.
• 70% million people classified as overweight/obese.
• 65% of urban adult women in India are obese.
• 30-50% urban Indians are overweight.
Misra et al 2008
Unpublished data
Genetic factors or family history
• Adoption studies found a high correlation between obesity in adopted children & their biologic parents.
• Twins reared together or apart have similar rates of obesity.
• Having two obese parents increases a childs risk of obesity up to 80%.
• Genetics a rare cause ,environment the culprit .
I Don’t Want to Grow Up
• 25% of children who are obese at age 6 will be obese as an adult
• 75% of children who are obese at age 12 will be obese as an adult
Social Difficulties
• Obese children…
– are stereotyped as “unhealthy, academically unsuccessful & lazy”
– may be teased or verbally abused by other children
– can become excluded from being a part of social groups and/or other activities
Social Difficulties
• Obese children…
– are stereotyped as “unhealthy, academically unsuccessful & lazy”
– may be teased or verbally abused by other children
– can become excluded from being a part of social groups and/or other activities
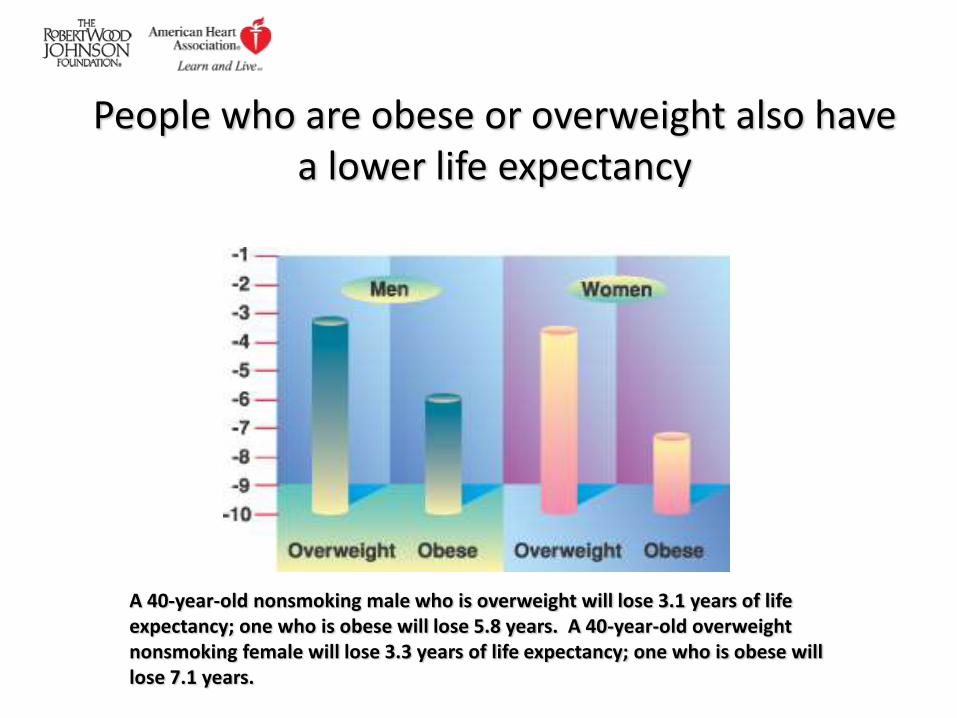
People who are obese or overweight also have a lower life expectancy
A 40-year-old nonsmoking male who is overweight will lose 3.1 years of life expectancy; one who is obese will lose 5.8 years. A 40-year-old overweight nonsmoking female will lose 3.3 years of life expectancy; one who is obese will lose 7.1 years.

How to Tell If Your Child is Overweight or Obese
Indicators
• Growth Chart– height and weight can be compared and plotted
• Skin fold thickness– measured at the triceps with a caliper that pinches the skin and
together and will be higher in obese children
• BMI (Body Mass Index)– is best measurement to take because it is age and gender specific
What is BMI?
• BMI is used to identify overweight and obesity in children
• BMI = weight (kg)/height (m)²
• For children, BMI is age and gender specific and is consistent with adult index, so it can be used continuously from two years of age to adulthood
Are you at risk?
• The Center for Disease Control avoids using the word “obesity” for children
• Instead they suggest two levels of overweight:
1.) 85th percentile: At-risk level (overweight)
2.) 95th percentile: Severe-level (obesity)
What does the 95th percentile BMI score mean?
• Correlates to BMI score of 30, which is the marker for obesity in adults
• Indication for children and adolescents to have an in-depth medical assessment
• Identifies children that are likely to have obesity persist into adulthood
• Is associated with elevated blood pressure and lipid in older adolescents which increases risk of diseases
What are the Causes?
The Family Atmosphere
• According to the American Obesity Association, parents are the most important role models for children.
• Obesity tends to run in families– Eating patterns play a role
• Children of active parents are six times more likely to be physically active than kids whose parents are sedentary
Television & Nutrition
• Commercials feature many junk foods that promote weight gain
– fast food, soft drinks, sweets and sugar-sweetened breakfast cereals
• Children seem to passively consume excessive amounts of energy-dense foods while watching TV
The typical American child spends about 44.5 hours per week using media outside of school.
Pick-up or Delivery?
• Today, families eat fewer meals together and fewer meals at home
– Children tend to eat more food when meals are eaten at a restaurant
– Plenty of children eat fast food on a regular basis
– Take-out food like pizza or chinese is also popular
Between 1977 and 1996, portion sizes grew in the U.S., not only at fast-food outlets but also in homes and restaurants
• One study of portion sizes for typical items showed that:
– Salty snacks increased from 132 calories to 225 calories
– Soft drinks increased from 144 calories to 193 calories
– French fries increased from 188 calories to 256 calories
– Hamburgers increased from 389 calories to 486 calories
Vending Machines
• Soda
– each 12-oz (though now most are 20-oz) sugared soft drink consumed daily increases a child’s risk of obesity by 60%
– risk of lack of calcium if students choose sweetened drinks with no nutritional value instead of milk, a good source of vitamins, minerals and protein
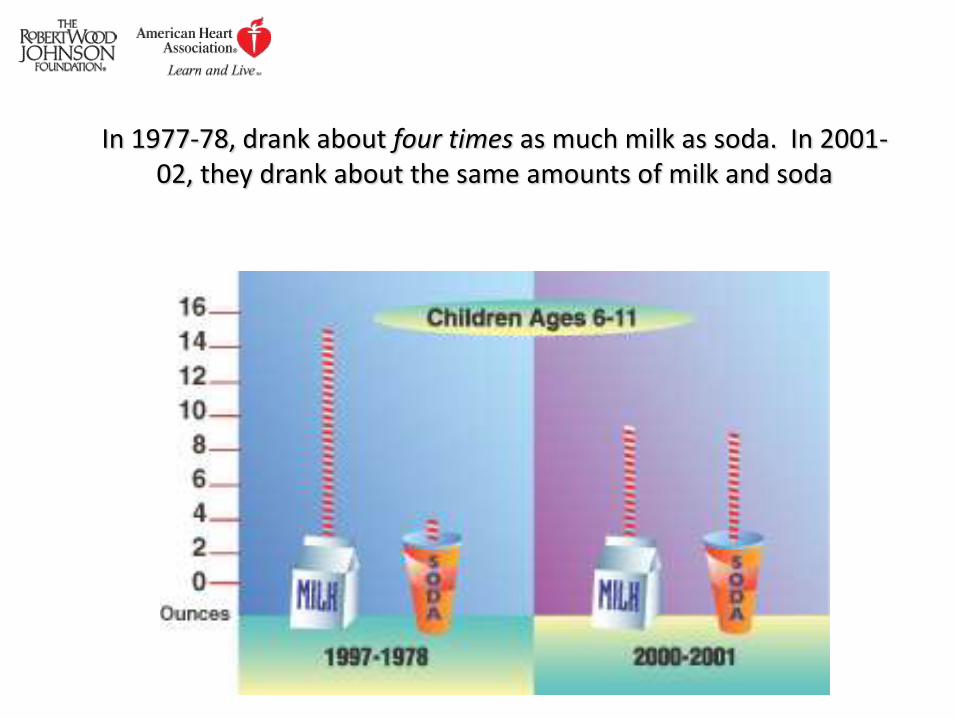
In 1977-78, drank about four times as much milk as soda. In 2001-02, they drank about the same amounts of milk and soda
Simple Solutions
Keys to Preventing Obesity
• Teaching healthy behaviors at a young age is important since change becomes more difficult with age
• Education in physical activity and nutrition are the cornerstones of preventing childhood obesity
• Schools and families are the two most critical links to decreasing the prevalence of childhood obesity
Parent’s role in Prevention
Create an active environment
Limit amount of TV watching
Plan active family trips such as hiking or skiing
Enroll children in a structured activity that they enjoy
Parent’s role (cont.)
• Create a healthy eating environment– Implement the same healthy diet for entire family,
not just selected individuals
– Avoid using food as a reward or the lack of food as a punishment
– Encourage kids to “eat their colors;”
(food bland in color often lack nutrients)
– Don’t cut out treats all together, think in moderation, or kids will indulge
Schools Are Only Exercising Our Minds
• According to the Center for Disease Control and Prevention:
– Nationwide, approximately 56% of high school students were enrolled in a physical education class and only 29% attended PE class daily (1999)
What Should Schools Revise?
• POLICY
– Schools should establish policies that require daily physical education and comprehensive health education in grades K-12
– Schools and government should provide adequate funding, equipment, and supervision for programs that meet needs of all students
It’s as Easy as Cake…
THE
END
Get moving
• Exercise regularly. Get active together as a family.
• Encourage children to enjoy physical activity that burns calories & uses different muscles.
• Find fun ways to be active inside & outside house.
• Practice sports at home.
• Involve your child in a carwash, shifting the furniture etc.
• Start in small steps, 10 mins and build to 60 mins.
Ways to encourage better eating habits for your child
• Offer kid size servings.
• Only milk at breakfast is poor choice……offer something filling eg parantha, fruit,idli/dosa,halwa ,corn flakes….
• Encourage drinking low fat milk & water.
• Plan evening snacks esp for after play hunger pangs.
• Avoid skipping meals.
• Put in that extra effort to prepare a snack than offer cookies.
Help your child become more active
• Boundaries-set time limits on TV/Computers/games..for all family members
• Play- Encourage daily activity..ride a bike,toss a ball, walk a dog.
• Family time- adopt a life style to involve children…after dinner walk, car wash, shifting of furnitures etc.
• Encourage-provide opportunities to choose activities like hiking photography, gardening etc.
• Enjoy- Make sure the activity is not viewed as a punishment.
Families need your education and support to experience success
• Prioritize need for change in family functioning.
• Acquire skills & knowledge to effect changes.
• Set realistic goals.
Education
• Model good habits
• Healthy foods
Child’s ideas ….. Respect his likes & dislikes
Make them palatable… Offer alternatives
Portion size & serving size… Use hands
Small steps
Exercise & activity
Mutually agreeable changes with parents.
Make changes a family affair.
How to be perfect role model …
• Never skip meals…infact indulge in healthy snacking.
• Limit junk food in the house.
• Eat & prepare food with your children.
• Try new foods but never force your child to try them.
• Turn off the TV while eating.
• Be active yourself & involve the child .
Common misconceptions
• My child & I deserve blame for his weight problem.
• My child will lose those extra pounds….Baby fat.
• He seems overweight but then we all are big boned.
• Because he is heavy ….Needs to eat to stay healthy.
• My child’s weight problem needs a quick fix.

How can food marketing contribute….
• The food industry creates and promotes
products that children enjoy
eating……….
• Why not create food that children like
but which is lower in sugar,salt and
fat….
• And use Shahrukh khans & Tendulkars
to model a health lifestyle & promote
healthy food products……
Laboratory testing & imaging
• Fasting glucose
• Lipid panel
• Liver function tests
• Plain radigraphs
• Abdominal ultrasound.

Small steps to healthier living
A journey of a thousand miles begins with a single first step.
Chinese proverb
An ounce of prevention is worth a pound of cure
• Prevention is the key strategy for current epidemic.
Primary prevention & Secondary prevention
• Priority population for intervention
Weight loss in adults difficult.
Greater number of interventions for children.
• Effectiveness of prevention methods.
Focus on reducing inactivity & encouraging free play.
Forced exercise & reduced food intake difficult.
Are you a role model for your child !
Behaviour is learned from observation…Good or bad
Please ask yourself following……
Do you snack all day long?
Do you eat in front of the TV?
Do you eat when you are bored or stressed ?
Do you eat dessert at every meal ?
Do you skip breakfast ?
Do you have soda/juice with your meals ?
Do you diet all the time and have a fear of food ?
Parting words
• Do not become discouraged. Become involved , and be a good role model.
• Remember small steps have enormous benefits: Decrease 100 cals a day & increase physical activity to burn 100 cals a day to lose weight healthfully.
• Children can and do succeed at changing lifestyles.
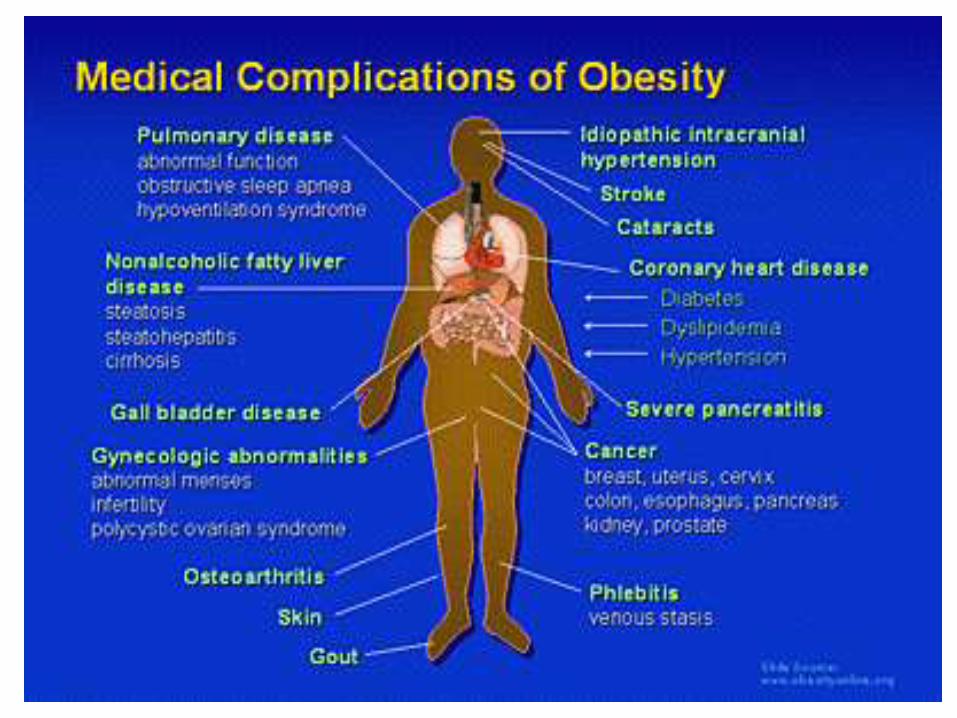
Co-morbidities with Obesity
• Diabetes
• Hypertension METABOLIC SYNDROME
• Dyslipidemia
• Sleep apnea
• Asthma & other breathing problems
• Early puberty or menarche
• Low self esteem & bullying
• Behaviour & learning problem
• Depression
Small steps to healthier lifestyle
Physical activity
Get moving• Limit media usage to no more than 2 hours.
• Emphasize activity, not exercise.
• Find activities your child likes.
• If you want active child ,be active yourself.
• Start in small steps, 10 mins and build upto 6o mins.

Exercise recommendations
• Children : 60 minutes daily five days a week of vigorous physical activity that makes them sweat.
• Adults: 30 minutes of the same five days a week.
• Key point: Find something you & your child enjoy and schedule it right into your day.
Small steps to healthy lifestyle
Eating
Eating• Think portions…..
• Switch it up…atta for maida, Brown bread/Rice for white , Dosa for pizza, nimbu pani for coke…
• Offer healthy meals & snacks…frying to steaming or baking
• Everything in moderation. Nothing bad or good Don’t eliminate ,just reduce it.
• Involve the entire family…Have children help you prepare a meal and eat together as a family..
• Be a good role model.
Think of ReplacementPancake for a Malpua



Prevent Obesity & overweight• HOME Reduce time spent in front of screen.
Build physical activity into routine.
• Schools School tiffins meet nutrition standards
Provide foods that are low fat/cal/sugars
Encourage quality physical education.
• Work Opportunities for activities at work
• Community Popularize fruit/veggie servings
Control the portion size
“An ounce of prevention is worth a pound of cure”