Embed Size (px)
Citation preview

Subacute Osteomyelitis
Prepared by:Tg.Putri Madina bt Tg.Ariff @ Zainuddin

Introduction
- It is a distinct type of osteomyelitis- It has an insidious onset, mild symptoms, lack of
systemic reaction- Its relative mildness is due to:
a) Organism being less virulent OR
b) Patient more resistant OR
c) (Both)
- Subacute osteomyelitis occurs in a much wider variety of bones than acute osteomyelitis
- Most common site: Distal femur, Proximal & Distal Tibia

Causative Organism
a) Staphyloccocus aureus (30-60%)
b) Others (Streptococcus, Pseudomonas, Haemophilus influenzae)
c) Pseudomonas aeruginosa (IV drug user)
d) Salmonella (patient with sickle cell anaemia)
Gram positive Staphylococcus aureus

Clinical Features
a) Pain (several weeks / months)
b) Limping
c) Swelling & Local tenderness
d) Muscle wasting
e) Body temperature usually normal (no fever)

Radiological FindingClassic Brodie’s abscess- A circumscribed, round/oval cavity containing
pus and pieces of dead bone (sequestra) surrounded sclerosis
- Most commonly seen in tibial / femoral metaphysis
*may occur in epiphysis / cuboidal bone (eg: calcaneum)
- Metaphyseal lesion cause no / little periosteal reaction
- Diaphyseal lesion may be associated with periosteal new bone formation and marked cortical thickening

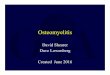
A circumscribed, oval cavity surrounded by a zone of sclerosis at the proximal tibia (Brodie’s abscess)
This is a lateral view X-ray of left tibia and fibula. There is a marked periosteal reaction at the diaphysis (Type IIb subacute OM)

Modified Classification of Subacute Osteomyelitis
Type I – Metaphyseal Ia - punched-out central metaphyseal lesion Ib - eccentric metaphyseal cortical erosion
Type II – Diaphyseal IIa - localized cortical and periosteal reaction IIb - medullary abscess in the diaphysis without cortical
destruction but with onionskin periosteal reaction
Type III – Epiphyseal IIIa - primary epiphyseal osteomyelitis IIIb - lesion that crosses the epiphysis and involves both the
epiphysis and the metaphysis
Type IV - Metaphyseal equivalent IVa - vertebral body with an erosive or destructive process IVb - involves the flat bones of the pelvis
IVc - involves the small bones, such as the tarsal bones


Investigation
a) X-ray (may resemble osteoid osteoma / malignant bone tumour)
b) Biopsy
c) Fluid aspiration & culture
d) ESR raised
e) WBC may be normal

Treatment
Conservative (if the diagnosis is not in doubt)
a) Immobilization
b) Antibiotics (flucloxacillin + fusidic acid) for 6weeks
Surgical (if the diagnosis is in doubt / failed conservative
treatment)
a) Open biopsy
b) Perform curettage on the lesion

Chronic Osteomyelitis
Prepared by:Tg.Putri Madina bt Tg.Ariff @ Zainuddin

Introduction
Definition:
“ A severe,persistent and incapacitating infection of bone and bone marrow ”

Causes
- It can be due to: a) progression / sequel / inadequate treatment of
acute osteomyelitis (presence of infection after 3 months of
antibiotic treatment) b) open fracture c) foreign implant (internal fixation)

Aetiological Agents
Usual organisms (with time there is always a mixed infection)
Staph.aureus(commonest)
Staph.pyogenesE.coliPseudomonasStaph.epidermidis(commonest in surgical implant)

Clinical Features
a) Pain
b) Pyrexia
c) Redness
d) Tenderness
e) Discharging sinus
(seropurulent discharge)

PathogenesisInadequate treatment of acute OM /
Foreign implant /Open fracture
Inflammatory process continues with timetogether with persistent infection by Staphylococcus aureus
Persistent infection in the bone leads to increasein intramedullary pressure due to inflammatory exudates (pus)
stripping the periosteum
Vascular thrombosis
Bone necrosis (Sequestrum formation)
New bone formation occur (Involucrum)
Multiple openings appear in this involucrum, through which exudates & debris from the sequestrum pass via the sinuses
(Sinus formation)


StageStage CharacteristicCharacteristic FeaturesFeatures
II MedullaryMedullary Endosteal diseaseEndosteal disease
IIII Superficial Superficial Cortical surface infected because of coverage Cortical surface infected because of coverage defectdefect
IIIIII LocalisedLocalised Cortical sequestrum that can be excised without Cortical sequestrum that can be excised without compromising stabilitycompromising stability
IVIV DiffuseDiffuse I, II and III plus mechanical instability before or I, II and III plus mechanical instability before or after debridement.after debridement.
Anatomical Type
Cierney and Mader staging system of Chronic Osteomyelitis

ClassClass Host’s immune Host’s immune systemsystem
FeaturesFeatures
A hostA host NormalNormal Immunocompetent with good local Immunocompetent with good local vascularityvascularity
B host B host CompromisedCompromised Local or systemic factors that compromise Local or systemic factors that compromise immunity or healingimmunity or healing
C hostC host ProhibitiveProhibitive Minimal disability, prohibitive morbidity Minimal disability, prohibitive morbidity anticipated, poor prognosis for cure, treatment anticipated, poor prognosis for cure, treatment worse than diseaseworse than disease
Physiological class

Imaging
1) X-ray examination- Usually show bone resorption (patchy loss of density /
osteolytic lesion)- Thickening & sclerosis around the bone- Presence of sequestra- Occasionaly it may present as a Brodie’s abscess
surrounded by vascular tissue and area of sclerosis
2) Radioisotope scintigraphy- Sensitive but not specific- Technetium labelled hydroxymethylene diphosphonate
(99mTc-HDP) may show increased activity in both perfusion phase and bone phase
3) CT scan & MRI- Show the extent of bone destruction, reactive oedema,
hidden abscess and sequestra

AP & lateral view of the left wrist show a lobulated osteolytic lesion with well-defined borders and surrounding sclerosis at the distal radius. Minimal expansion, mild periosteal reaction and soft tissue swelling are present.

Sclerosing osteomyelitis of the lower tibia. Note the bone expansion and marked sclerosis.
Sequestrum at lower tibia

Other Investigation
a) ESR & WBC may be increasedb) Antistaphyloccocal antibody titres may be
elevatedc) Fluid aspiration from sinus + culture & sensitivity
Isolation of the agent from the bone or the blood. In hematogenous OM, positive blood cultures
often obviate the need for a bone biopsy when there is associated radiographic or radionuclide scan evidence of OM.
In chronic OM, sinus tract cultures are not reliable Antibiotic treatment should not be based on the
results of sinus tract cultures. In most instances, bone biopsy cultures are
mandatory to guide specific antimicrobial therapy.

TreatmentPatient evaluation
(History taking, PE, Investigation)
Disease assessment(Anatomic & Physiologic classification)
Identification of organism(Biopsy + Culture)
Antibiotic administration
Host alteration(No smoking, no alcohol, nutrition, control DM, BP)
Surgical treatment(Debridement, Deep space management)
Follow up

1) Antibiotics
- Chronic infection is seldom eradicated by antibiotics alone
- Bactericidal drugs are important to: a) Stop the spread of infection to healthy bone b) Control acute flares
- The choice of antibiotic used must be: a) Capable of penetrating sclerotic bone b) Non toxic with long term use
- Eg of antibiotics used in treating chronic osteomyelitis (Fusidic acid, Clindamycin, Cefazolin)
- Antibiotic (IV route) is given for 10 days prior to surgery
- After the last major debridement surgery, antibiotic is continued for another 6 weeks (min) but usually >3months[*treat until inflammatory parameters (ESR) are normal]

2) Surgical Treatment
- After 10 days of antibiotic administration, debridement is
done to remove:
a) All the infected tissue
b) Dead / devitalised bone (Sequestrectomy)
c) Sinus tract
- Debridement approach used is direct & atraumatic
- Wound is left open (stent dressing) EXCEPT:
a) Compromised hosts (Class B host); ankle, hand, spine
b) Type II lesions (primary soft tissue reconstruction and/or host alteration)
c) Minimal necrosis osteomyelitis

- After debridement is done, a large dead space is left in
the bone- Among the methods of
managing dead space:
a) Open cancellous grafting (Papineau technique)
b) Primary closure with local tissue (+/- cancellous grafts)
c) Primary closure with transferred tissues (+/- cancellous grafts)
d) Primary closure over antibiotic impregnated beads

- Papineau technique:
Cavity is packed with small cancellous bone graft (preferably autogenous) mixed with an antibiotic and fibrin sealant
- Primary closure with transferred tissue:
In muscle flap transfer, a suitable large wad of muscle with its blood supply intact can be mobilized and laid into the cavity. The surface is later closed with a split-skin graft
- Primary closure with antibiotic impregnated beads:
Porous gentamicin-impregnated beads are used to sterilize the cavity. It is easier but less successful. Furthermore, they are extremely difficult to be removed if not taken out by 2-3 weeks

1) Pathological Fracture- This occurs in the bone weakened by
chronic osteomyelitis2) Deformity
– In children the focus of osteomyelitis destroys part of the epiphysis growth plate.
3) Shortening/ lengthening- Destruction of growth plate arrest growth.- Stimulation of growth plate due to
hyperemia.
Complications

Thank You