Embed Size (px)
Citation preview

Clinical Assessment & Management of Prion Disease
Brian S. Appleby, M.D.Associate Professor
Department of Neurology

Objectives
• Understand how clinicians diagnose prion disease
• Describe tools used to diagnose prion disease• Provide update on clinical trials for prion
disease

“If it looks like a duck, quacks like a duck, then it’s probably a duck.”
Dr. Edward Tsou (GUH)
Horses versus Zebras

Diagnostic Syndromes
Pneumonia• Malaise• Cough• Fever• Chest/back pain• Shortness of breath
Creutzfeldt-Jakob disease (CJD)
• Dementia• Difficulty with gait• Incoordination• Abnormal movements• Weakness• Visual disturbances• Rapid progression

Appleby BS et al, Arch Neurol 2009Appleby BS et al, Arch Neurol 2009
What Clinicians See

Initial Diagnoses
Appleby BS et al, Prion 2008

#1 Rule for Diagnosing Prion Disease
Prion Disease

• Consequences of missing other diagnoses– Treatable– Reversible– Different Prognosis– Repeated work-ups later– Difficulty in accepting different diagnosis
Why?

Probable Sporadic CJD
≥2 Clinical Signs
• Dementia• Visual or cerebellar• Pyramidal or
extrapyramidal • Akinetic mutism
≥ 1 Diagnostic Test Result
• CSF 14-3-3 and <2 yrs duration
• PSWC’s on EEG• Brain MRI findings
Zerr I et al, Brain 2009

Conditions with CSF 14-3-3
Berg D et al, Nat Rev Neurosci 2003
• TBI• Seizures

EEG
CJD Non-CJD Total
PSWC’s 10 2 12
No PSWC’s 5 12 17
PSWC’s
Steinhoff BJ et al, Arch Neurol 1996

EEG
Parchi P et al, Ann Neurol 1999

≥ 1 of the Following(FLAIR and/or DWI)
• High signal abnormality in basal ganglia
• High signal abnormality in ≥ 2 cortical regions• Temporal• Parietal • Occipital Frontal
Zerr I et al, Brain 2009

Brain MRI
Zerr I et al, Brain 2009

Hamlin C et al, Neurology 2012

“Forest through the Trees”

Case Example
• 61 y.o. WF from St. Maarten’s Island with a history of alcohol abuse
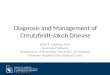
• 2 mo. h/o ataxia, apathy, myoclonus, and cognitive impairment
• Vitamin B12=249, folate=8.6, MCV=98

ExamGeneral: Vacant look, utilization behaviorSpeech: Dysarthric, apraxic, latent Thought Content: Appeared to be responding to visual hallucinationsMMSE: 12/30Motor: Mild rigidity UE (L>R), myoclonusGait: Ataxic, requires 2 person assist, dysmetria (L>R)

Brain MRI (DWI)

Experimental Treatment
Compound• Quinacrine • Pentosan polysulphate• Doxycycline
Outcome• no effect• may have effect in vCJD• verdict is unclear

Individuals with less impairment and better functioning chose quinacrineIndividuals with more impairment and less functioning declined quinacrine
Only 2 of 107 subjects chose randomization
Collinge J et al, Lancet Neurol 2009

“On the basis of the available evidence,the best possible outcome that couldbe expected after treatment withintraventricular PPS is that there maybe some temporary slowing or haltingof the disease progression. However,there is little likelihood of significantclinical improvement. Nor is there alikelihood of permanent halting ofdisease progression.”
CJD Support Network Newsletter, March 2004

German Observational StudyGroup Number of cases Median survival time
Doxycycline treated 21 292 days
Untreated (historical cntrl) 581 169 days
Log Rank test, p<0.001
p=0.019
PRNP codon 129 polymorphism
Zerr I, Prion 2008, Madrid, Spain

Symptomatic TreatmentSymptom Suggested Treatment
Psychosis/Agitation Low potency neuroleptics (e.g., quetiapine)
Myoclonus/Hyperstartle Long acting benzodiazepines (e.g., diazepam)Anticonvulsants (e.g., valproic acid)
Seizures Anticonvulsants
Dystonia/Contractures Passive movement Long acting benzodiazepines, Botulinum toxin injections
Constipation Bowel regimen (e.g., dulcolax)
Dysphagia/Rumination Thickener, cueing
Behavioral/Environmental changes first Start low and go slow Re-evaluate frequently

Thank You
• Patients and families• CJD Foundation• National Prion Disease Pathology Surveillance
Center• CJD Support Group Network