Embed Size (px)
Citation preview

DR.G BALAJI.PROF.DR.G. SUNDARAMURTHY’S UNIT

Disorders of blood coagulation:
Inherited or acquired coagulation disorders. Disorder of vessels
Disorders of platelets- quantity or function

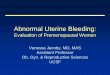
HemostasisBV Injury
PlateletPlateletAggregation
PlateletActivation
Blood VesselBlood Vessel Constriction
CoagulationCoagulation Cascade
Stable Hemostatic Plug
Fibrin formation
Reduced
Blood flow
Damage/contact.
Primary hemostatic plug
Neural
•CBC-Plt•BT,(CT)•PT•PTT
Platelet studyAntibody testsFactor Assay
Contact

Type of Bleedingecchymosespetechiaeepistaxisdeep soft tissue bleedhemarthrosesGI bleeding

Tests of Hemostasis:Screening tests:
Bleeding.T - 10m. Platelet & BV function Prothrombin.T – Extrinsic, aPTT – IntrinsicThrombin.T – common path.
Specific tests:Factor assays – hemophilia.Tests of thrombosis – TT, FDP, Platelet function studies:
Adhesion, Aggregation, Release tests.Bone Marrow study

Pre-analytic errors Problems with blue-top tube
Partial fill tubes Vacuum leak and citrate
evaporation
Problems with phlebotomy Heparin contamination Wrong label Slow fill Underfill Vigorous shaking
Biological effects• Hct ≥55 or ≤15
• Lipemia, hyperbilirubinemia, hemolysis
Laboratory errors• Delay in testing
• Prolonged incubation at 37°C
• Freeze/thaw deterioration

Bleeding timeMeasure of efficiency of vascular or
platelet phases. Do not discriminate between vascular
defects , thrombocytopenia or platelets dysfunction.
Not reproducible.Not a screening test . normal bleeding time do not exclude a
bleeding disorder- american society of clinical pathologists.

Platelets enumerationDirect or automated methods.Normal: 1.5 lakhs- 4.5 lakhsFalsely low platelets counts-
PSEUDOTHROMBOCYTOPENIA platelets agglutinins, paraproteinemias, giant platelets, lipemia, EDTA induced
platelets clumping.Flasely high platelets counts: Microspherocytes, WBC/RBC
fragments, pappenheimer bodies.

Platelets function assaysPlatelets aggregation using platelets rich
plasma.- standard method.Nephelometric or photometric measurements.ADP- produce platelets aggregation directly
irrespective of release of ADP from platelets.RISTOCETIN- antibiotic that induce platelets
aggregation in presence of von Willebrand factor.
Collagen, epinephrin, thrombin- cause platelet aggregation by release reaction.

Platelet function analyser- PFA 100hemoSTATUS SYSTEM- modified activated
clotting time test. To monitor cardio pulmonary bye-pass system.
Verify now systemHemostasis analysis system.DiaMed- Impact-R System

Coagulation testsAll tests on citrated plasma except D- Dimer.Nine parts of blood to one part of citrate.3.2% sodium citrate.Blue topped vacuum blood collection tubes.

Blood Coagulation & TestsBlood Coagulation & Tests

Activated partial thromboplastin timeIntrinsic and common pathway.When mixture of plasma and phospholipid
platelets substitute is re calcified, fibrin is formed in the presence of factors in intrinsic pathway and common pathway.
Platelet substitute-chloroform extract of brain, Inosithin- soyabean. Partial thromboplastin. Do not activate the
extrinsic pathway which require complete tissue thrombo plastin.

APTTPTT is used to detect factor deficiency ,
screen for lupus anti coagulantMonitor heparin anti coagulation.More sensitive to deficiency of VIII and
IX.Yields abnormal results if any factor level is
< than 15-30% of normal.PTT may be shortened by a high level of any
single factor. m/c is factorVIII.

APTTContact activation was provided by the glass
tube.Activators- ellagic acid, particulate silicates
such as celite or kaolin.No significant differences between adult and
children between 7-17 years.Shortened PTT Values is an independent risk
factors for death, thrombosis ,bleeding and morbidity.

PROTHROMBIN TIME:Extrinsic and common path way.Tissue factor, factor VII,X,V, prothrombin,
fibrinogen.Plasma is recalcifed in the presence of tissue
factor.Independent of platelet count.PT is used for controlling anti coagulant
therapy.More sensitive to deficiency of VII and X.

Prothrombin timeChildren between 7-17 years have PT value 1
second longer than adults.Use INTERNATIONAL NORMAL RATIO.STYPVEN time- Russel viper venom directly
initiate coagulation with out factor VII. Used to differentiate factorVII deficiency from factor- X deficiency.

Thrombin time:When thrombin is added to plasma the time required
for clot formation is a measure at which fibrin forms.Abnormal value when fibrinogen level is <70 to 100
mg/dl.Prolonged by heparin.Prolonged in qulitatively abnormal fibrinogen,
elevated FDP, paraproteinemias, hyper fibrinogenemias.
REPTILASE CLOTTING TIME- un affected by heparin.

D-DIMERS and FDP:FDP results from proteolytic cleavage of fibrin
by plasmin. Increased in DIC and fibrinolysis.RA factor or residual fibringen may yield false
positive results.D-DIMER- specific fibrin degradation
product.DDE- TRIMER.UN POLYMERISED FIBRIN MONOMER.

UREA CLOT LYSIS ASSAY:FACTOR XIII assay.XIII Stabilises fibrin.Deficiency leads to premature clot lysis.Screening test. Abnormal results should be
confirmed by quantitative measurements of XIII.

TESTS FOR FIBRINOLYSISEUGLOBULIN CLOT LYSIS TIME:Plasma euglobulin contains plasminogen
activators and fibrinogen.Rate of lysis of a fibrin clot prepared from
euglobin fraction is a measure of plasminogen activators.
EACA can inhibit plasminogen activators but not free plasmin. Shortened euglobulin lysis time in presence of EACA indicated presence of free plasmin.

Bio assays for coagulation factorsExtent to which an unknown sample corrects
the abnormality in plasma with a known deficiency is proportional to the content of the deficient factor in the sample.
Measured in units or percentage of normal.Normal- 50-150 units/dl or 50-150% of
normal.Factor V, VIII, X , prothrombin.

Tests for inhibitors of coagulationMixing studies or inhibitor screens.Small amount of patient’s plasma if contains
inhibitors of coagulation will impair coagulation in normal samples.
Based on PT or APTT.HEPARIN presence can be confirmed by
thrombin time or reptilase time, or correction with protamine sulphate.

Automated coagulation methodsThrombo elasto graph- demonstrates
changes during blood coagulation and fibrinolysis. Used in surgical settings.
Activated clotting time- whole blood clotting assay.
Used to monitor intrinsic pathway.In cardio pulmonary bye pass, dialysis,
cardiac catheterisation.

Chromogenic and flurogenic methodsArtificial substances when cleaved by
coagulation factors release chromogenic or fluroscopic peptides.
Prothrombin, VII, IX, X, anithrombin, heparin, plasmin.
More precise and less time consuming.Used mainly in research and large reference
labs.

Evaluation of the patientHistoryPhysical ExaminationLaboratory Evaluation

HistoryAre you a bleeder?
surgical challengesaccidents & injuriesdental extractionsmenstrual history

HistoryGeneralized haemostatic defect or local
defectBleeding from multiple sites, spontaneous
bleeding or excessive bleeding after injury
Inherited defect or acquired Family H/O bleeding disorder, age of onset of
disease or any other event ppting. the bleeding

Is Bleeding suggestive of – Vascular, Platelet or coagulation disorderVascular /platelet disorders – Easy bruising ,
spontaneous bleeding from small vessels esp into skin – Purpura and echymosis .
Mucous membrane bleeding – Epistaxis, mouth –gums and Menorrhagia.
Coagulation disorders – Hemarthrosis, muscle bleeds, bleeding after injury or surgery

Does it sound genetic?duration of bleeding historycongenital v. acquiredfamily history
examine pedigreedetermine inheritance

Medical Historyliver diseaserenal diseasemalignanciespoor nutrition (Vit. K or C deficiency)

FIVE DRUGS THAT INTERFERE WITH HEMOSTASIS
ASPIRIN ANTICOAGULANTS ANTIBIOTICS ALCOHOL ANTICANCER

Laboratory AssessmentGuided by historyScreening tests
PTaPTTplatelet countfibrinogenthrombin time

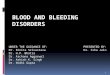
Partial Thromboplastin Time(PTT)
Prothrombin time(PT)
Intrinsic pathwayExtrinsic pathway
Common pathwayThrombin timeThrombin
Surface activating agent (Ellagic acid, kaolin)PhospholipidCalcium
Thromboplastin Tissue factor Phospholipid
Calcium
Fibrin clotFibrin clotFibrin Clot

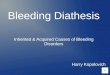
Initial Evaluation of a Bleeding Patient - 1Normal PT
Normal PTT
Consider evaluating for: Mild factor deficiency Monoclonal gammopathy Abnormal fibrinolysis Platelet disorder (2 anti-plasmin def) Vascular disorder Elevated FDPs
Ureasolubility
Normal
Abnormal Factor XIII
deficiency

Initial Evaluation of a Bleeding Patient - 2
Normal PT
Abnormal PTT
Test for factor deficiency: Isolated deficiency in intrinsic pathway (factors VIII, IX, XI) Multiple factor deficiencies (rare)
Repeatwith
50:50mix
50:50 mix is normal
50:50 mix is abnormalTest for inhibitor activity:
Specific factors: VIII,IX, XI Non-specific (anti-phospholipid Ab)

Initial Evaluation of a Bleeding Patient - 3
Abnormal PTNormal PTT
Test for factor deficiency: Isolated deficiency of factor VII (rare) Multiple factor deficiencies (common) (Liver disease, vitamin K deficiency, warfarin, DIC)
Repeatwith
50:50mix
50:50 mix is normal
50:50 mix is abnormalTest for inhibitor activity:
Specific: Factor VII (rare) Non-specific: Anti-phospholipid (rare)

Initial Evaluation of a Bleeding Patient - 4Abnormal
PTAbnormal
PTT
Test for factor deficiency: Isolated deficiency in common pathway: Factors V, X, Prothrombin, Fibrinogen Multiple factor deficiencies (common) (Liver disease, vitamin K deficiency, warfarin, DIC)
Repeatwith
50:50mix
50:50 mix is normal
50:50 mix is
abnormalTest for inhibitor activity: Specific : Factors V, X, Prothrombin, fibrinogen (rare) Non-specific: anti-phospholipid (common)

Laboratory Evaluation of BleedingOverview
CBC and smear Platelet count ThrombocytopeniaRBC and platelet morphology TTP, DIC, etc.
Coagulation Prothrombin time Extrinsic/common pathwaysPartial thromboplastin time Intrinsic/common pathwaysCoagulation factor assays Specific factor deficiencies50:50 mix Inhibitors (e.g., antibodies)Fibrinogen assay Decreased fibrinogenThrombin time Qualitative/quantitative
fibrinogen defectsFDPs or D-dimer Fibrinolysis (DIC)
Platelet function von Willebrand factor vWDBleeding time In vivo test (non-specific)Platelet function analyzer (PFA) Qualitative platelet disorders
and vWDPlatelet function tests Qualitative platelet disorders

Liver Disease
Decreased synthesis of II, VII, IX, X, XI, and fibrinogen
Prolongation of PT, aPTT and Thrombin Time
Often complicated byGastritis, esophageal varices, DIC

Lab Results in Hemophilia, VWD and Vit K Def
Haemophilia V W Disease Vit K Deficiency
Bleeding Time Normal Increased Normal
PT Normal Normal Increased
APTT Increased + Increased ± Increased
V111 levels
Decreased ++ Decreased Normal
vWF levels Normal Decreased Normal

Hemophilia A Hemophilia B Von Willebrand Disease
Inheritance X linked X linked Autosomal dominant
Factor deficiency VIII IV VWF
Bleeding site(s) Muscle,joint
Surgical
Muscle ,joint Mucous
Skin
Prothrombin time Normal Normal Normal
Activated PTT Prolonged Prolonged Prolonged
Bleeding time Normal Normal Prolonged or normal
Factor VIII Low Normal Normal
VWF Normal Normal Low
Factor IX Normal Low Normal
Platelet aggregation Normal Normal Normal

Coagulation factor deficienciesSummarySex-linked recessive
Factors VIII and IX deficiencies cause bleedingProlonged PTT; PT normal
Autosomal recessive (rare) Factors II, V, VII, X, XI, fibrinogen deficiencies
cause bleedingProlonged PT and/or PTT
Factor XIII deficiency is associated with bleeding and
impaired wound healingPT/ PTT normal; clot solubility abnormal
Factor XII, prekallikrein, HMWK deficienciesdo not cause bleeding

SummarySymptom Platelet Coagulation Petechiae Yes No
Sites Skin & Mucosa
Deep Tissue
Time Immediate Delayed
Ecchymoses/Hematomas
Yes Yes

Summary Hemostatic Disorders BT Plt PT PTT
Vascular Dis - - - -
PLT Disorder - - - -
Factor 8/9 *Congenital - - -
Vit K / Liver*Acquired - - -
Combined (DIC) -

Tests are normal-Now what?simple purpurasenile purpuraFactor XIII deficiencyalpha-2-antiplasmin deficiencymild factor deficiencyamyloidosisvascular disorders

Still more?Hereditary hemorrhagic telangiectasiascurvyEhlers-Danlos syndromeHenoch-Schonlein purpurathe un-diagnosable fibrinolytic defect

Thank you