Embed Size (px)
Citation preview

Common Eye Diseases and their Management

N.R. Galloway, W.M.K. Amoaku,P.H. Galloway and A.C. Browning
Common EyeDiseases and theirManagementThird Edition
With 146 Figures

A catalogue record for this book is available from the British Library
Library of Congress Control Number: 2005925513
ISBN-10: 1-85233-985-3 3rd edition e-ISBN 1-84628-033-8 Printed on acid-free paperISBN-13: 978-1-85233-985-2
ISBN 1-85233-050-3 2nd editionISBN 3-540-13659-2 1st edition
First published 1985Second edition 1999Third edition 2006
© Springer-Verlag London Limited 2006
Apart from any fair dealing for the purposes of research or private study, or criticism or review, as permittedunder the Copyright, Designs and Patents Act 1988, this publication may only be reproduced, stored or trans-mitted, in any form or by any means, with the prior permission in writing of the publishers, or in the case ofreprographic reproduction in accordance with the terms of licences issued by the Copyright Licensing Agency.
Enquiries concerning reproduction outside those terms should be sent to the publishers.The use of registered names, trademarks, etc. in this publication does not imply, even in the absence of a specificstatement, that such names are exempt from the relevant laws and regulations and therefore free for generaluse.
Product liability: The publisher can give no guarantee for information about drug dosage and applicationthereof contained in this book. In every individual case the respective user must check its accuracy by con-sulting other pharmaceutical literature.
Printed in Singapore (BS/KYO)
9 8 7 6 5 4 3 2 1
Springer Science+Business Mediaspringeronline.com
Nicholas R. Galloway, MBCHB, BA, FRCS, MD,FRCOphth
Surgeon EmeritusEye, Ear, Nose and Throat CentreUniversity HospitalQueen’s Medical CentreNottingham, UK
Winfried M.K. Amoaku, MBCHB, FRCS,FRCOphth, PhD
Senior Lecturer and Honorary Consultant Ophthalmologist, University of Nottingham and University Hospital, Queen’s Medical Centre, Nottingham, UK
Peter H. Galloway, MBBS, FRCOphthConsultant Ophthalmologist, St James’
University Hospital, Leeds, UK
Andrew C. Browning, BSc, FRCOphthDivision of Ophthalmology and Visual
Sciences, Eye, Ear, Nose and Throat Centre,University Hospital, Queen’s Medical Centre, Nottingham, UK
Artwork marked with symbol throughout the book is original to the 2nd edition (GallowayNR, Amoaku WMK. Common Eye Diseases and their Management, 2nd edition. Springer-VerlagLondon Ltd, 1999) and is being republished in this 3rd edition.

Preface to Third Edition
v
It is a pleasure to welcome two new authors who have contributed to the third editionof “Common Eye Diseases”: Peter Galloway and Andrew Browning. Six years have passedsince the last edition but even in this relatively short time there have been significantadvances in the diagnosis and management of eye disease and an update has becomenecessary. Each author has taken a block of chapters for revision and, where needed,illustrations have been added or removed. Apart from the four main authors, I amindebted to Mr Roland Ling for his invaluable work on the chapter on the retina andonce again to Professor Rubinstein for his help with the chapter on contact lenses.
The original aims of the book have not been changed. It remains as a textbook formedical students and those starting a career in ophthalmology, but also for those inprimary care who are likely to deal with eye problems, including nurses, optometristsand general practitioners.
It has been the intention to keep explanations as simple and nontechnical as possiblewithout losing scientific accuracy; more detailed accounts should be sought in the largertextbooks. An updated reference list for further reading is given at the end of the book.An internet version of this edition is being planned and, in order to keep down the retailprice, some financial help is needed. For this we are grateful for the interest of Pfizer Ltd,whose policy of educational support has allowed this edition to go forward at its presentlow price.
AcknowledgementsAlthough it is now many years since the first edition appeared, I still owe a great debt tomy former secretary, Mrs A. Padgett, for her original help in preparing the basis for thesefurther editions. No amount of word processing can replace this painstaking work. Inthis new edition, I have kept Geoffrey Lyth’s original cartoons, which will perhaps lightenthe heaviness of the text for those with an artistic bent. The two new authors have reviseda number of chapters and their fresh input to an ageing textbook has been essential andmuch appreciated.
Finally, I would like to acknowledge the help and encouragement from Melissa Mortonof Springer-Verlag, who has kept the ball bouncing back into my court with greatefficiency and thereby played an important part in ensuring the birth of this new edition.

Preface to Second Edition
Like the first edition, this textbook is intended primarily for medical students, but it isalso aimed at all those involved in the primary care of eye disease, including generalpractitioners, nurses and optometrists. The need for the primary care practitioner to bewell informed about common eye conditions is even more important today than whenthe first edition was produced. A recent survey from North London has shown that 30%of a sample of the population aged 65 and over are visually impaired in both eyes and alarge proportion of those with treatable eye conditions were not in touch with eye serv-ices. It is clear that better strategies for managing problems of eyesight need to be setup. One obvious strategy is the improved education of those conducting primary careand it is hoped that this book will contribute to this. For this second edition, I am grate-ful for the help of my coauthor Winfried Amoaku, whose personal experience in teach-ing medical students here in Nottingham has been invaluable. His expertise in themanagement of macular disease, now a major cause of sensory deprivation in the elderly,is also evident in these chapters.
The format of the book has not changed but some of the chapters have been expanded.For example, there is now a section dealing with the eye complications of acquiredimmune deficiency syndrome (AIDS). This problem barely existed at the time of the firstedition. Cataract surgery has changed a great deal in this short time and is becomingone of the commonest major surgical procedures to be performed in a hospital. Themanagement of glaucoma has also changed with the introduction of a range of new med-ications. Our aim has been to keep the original problem-oriented layout and to keep itas a book to read rather than a book to look at. There are a number of good atlases oneye disease and some of these are mentioned in the section at the end on further reading.Although the title of the book is “Common Eye Diseases”, some less common conditionsare mentioned and it is hoped that the reader will gain some overall impression of theincidence of different eye diseases.
vii
Contents
Preface to Third Edition . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . v
Preface to Second Edition . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . vii
Section I Introducing the Eye . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1
1. The Scope of Ophthalmology . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3
2. Basic Anatomy and Physiology of the Eye . . . . . . . . . . . . . . . . . . . . . . 7
3. Examination of the Eye . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 17
Section II Primary Eye Care Problems . . . . . . . . . . . . . . . . . . . . . . . . . . 27
4. Long Sight, Short Sight . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 29
5. Common Diseases of the Eyelids . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 33
6. Common Diseases of the Conjunctiva and Cornea . . . . . . . . . . . . . . . 45
7. The Red Eye . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 61
8. Failing Vision . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 67
9. Headache . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 71
10. Contact Lenses . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 77
Section III Problems of the Eye Surgeon . . . . . . . . . . . . . . . . . . . . . . . . 79
11. Cataract . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 81
x Contents
12. Glaucoma . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 91
13. Retinal Detachment . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 103
14. Squint . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 111
15. Tumours of the Eye and Adnexae . . . . . . . . . . . . . . . . . . . . . . . . . . . . 121
16. Ocular Trauma . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 129
Section IV Problems of the Medical Ophthalmologist . . . . . . . . . . . . . 135
17. Testing Visual Acuity . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 137
18. The Inflamed Eye . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 141
19. The Ageing Eye . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 149
20. The Child’s Eye . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 157
21. Systemic Disease and the Eye . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 165
22. Neuro-ophthalmology . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 179
23. Genetics and the Eye . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 189
24. Drugs and the Eye . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 195
Section V Visual Handicap . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 201
25. Blindness . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 203
Further Reading . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 207
Index . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 209
Section IIntroducing the Eye
Although the eye and its surrounding structureswould seem to provide an ideal anatomical andfunctional basis for specialisation, ophthalmol-ogy can no longer regard itself as a specialty onits own but more the heading for a group of sub-specialties. There are those who know all aboutthe pigment epithelium of the retina and yetbow to those who have a special knowledge ofthe bipolar cells in the retina. Over the past 100years the science has advanced at an unbeliev-able rate and with the increase in our knowledgehas come the development of treatments andcures, which have had a great impact on oureveryday lives.
The importance of the eye and its function issometimes underrated, but a consideration ofthe part played by vision in our consciousnessmakes us soon realise its value. If we think ofdreams, memories, photographs and almostanything in our daily existence, it is difficult toexpress them without visual references. After alittle careful consideration of the meaning ofblindness, it is easy to sense the rational andirrational fears that our patients present to us inthe clinic. Nevertheless, in a modern Europeancommunity the effects of blindness are not soapparent as in former years, and blind peopletapping their way about the street or begging for food are less in evidence to remind us of thedeprivation that they suffer. This is due to theeffective application of preventive medicine and the efficacy of modern surgical techniques.However, in the western world we have a newand increasing problem related to the increasing
number of elderly people in the population. Theproblem is that of sensory deprivation owing todegenerative disease. Degenerative changes inthe eye are now a major cause of blindness andalthough support services are being developedthere is still no effective cure.
The broad and detailed scientific interest inthe eye and vision is witnessed by the largenumber of journals, conferences and meetingsthat now exist, possibly more than in any otherspecialty. There are several hundred ophthal-mological journals all contributing to thescientific literature on the subject and many arenow accessible through the internet or on CD-ROM. As an organ of clinical specialisation,the eye does have a special advantage; it can be seen. Using the slit-lamp microscope it ispossible to examine living nerves, includingnervous system tissues and blood vessels, in amanner that is not possible in other parts of thebody without endoscopy or biopsy. So much are the component parts of the eye on display to the clinician that when a patient presents to a casualty department with symptoms, theexplanation of the symptoms should be madeevident by careful examination. Compare thiswith the vague aches and pains that present to the gastroenterologist or the neurologist,symptoms that might ultimately resolve with-out any cause being found for them. The student or newly qualified doctor must bewarned that if the patient presents with eyesymptoms and no abnormality can be foundafter examination, then he or she must look
1The Scope of Ophthalmology
3

4 Common Eye Diseases and their Management
again, because it is likely that something hasbeen missed.
Most of the work of the ophthalmologist isnecessarily centred on the globe of the eye it-self, and there are a number of conditions thatare limited to this region without there beingany apparent involvement of the rest of thebody. Ophthalmology is usually classified as a surgical specialty but it provides a bridgebetween surgery and medicine. Most of thesurgery is performed under the microscope andhere the application of engineering principles inthe design of finer and finer instruments hasplayed an important part. There is overlap withthe fields of the plastic surgeons and the neuro-surgeons. On the medical side, the ophthal-mologist has links with the physicians and particularly the diabetic specialists and cardiologists, not to mention paediatricians and dermatologists.
Historical BackgroundIn 1847, the English mathematician and inven-tor Charles Babbage showed a distinguishedophthalmologist his device for examining theinside of the eye, but unfortunately this wasnever exploited and it was not until 1851 thatHermann von Helmholtz published his classicdescription of his instrument, the ophthalmo-scope. He developed the idea from his knowl-edge of optics and the fact that he hadpreviously demonstrated the “red reflex” tomedical students with a not dissimilar instru-ment. In principle, he had, for the purposes ofhis demonstration, looked through a hole in asmall mirror, which reflected light from a lampinto the subject’s eye. This produced the redreflex in the pupil well known to photographersand night drivers and no doubt this fascinatedmedical students at that time. Von Helmholtzworked out that a similar device could be usedto inspect the inside of the eye. According tocorrespondence of the time, it took him about aweek to learn the technique of examining indetail the structures within the eye and he wrotea letter to his father telling him that he had madea discovery that was “of the utmost importanceto ophthalmology”. Soon after this, a mass ofdescriptive information on the optic fundusappeared in the scientific literature and modernclinical ophthalmology was born. The changes
in the eye associated with systemic diseasessuch as hypertension and anaemia becamerecognised. Several blinding conditions limitedto the eye itself, such as glaucoma and maculadegeneration, were also described at this time.
But we must not belittle the developmentsthat had occurred before the invention of theophthalmoscope. In the eighteenth century, con-siderable advances had been made in the tech-nique and instrumentation of cataract surgery,and the science of optics was being developedto enable the better correction of refractiveerrors in the eye. If we go back to the seven-teenth century, the existing ophthalmologicalservices were definitely limited, as is revealed inthe writings of the famous diarist, SamuelPepys. Although we have no record of his eyecondition other than his own, he did consult anoculist at the time and unfortunately receivedlittle comfort or effective treatment. His failingeyesight brought his diary to an abrupt end inspite of the use of “special glasses” and themedicaments, which caused him great pain.
Although records of eye surgical techniquesgo back as far as 3000 years, modern eye surgerywas largely developed thanks to the introduc-tion of cocaine and then of general anaesthesiaat the end of the nineteenth century. The use ofeserine eye drops to reduce the intraocular pres-sure in glaucoma was introduced at the sametime, this being the forerunner of a number ofdifferent medical treatments that are now avail-able. Cataract surgery saw great advances at the beginning of the twentieth century, with the introduction of the intracapsular cataractextraction. In the 1920s, successful attemptswere being made to replace the detached retina,which had previously been an irreversible causeof blindness. Such early surgical techniqueshave now been developed to produce some ofthe most dramatic means of restoring sight. Asa spin-off from the last war came a revolution-ary idea of “spare-part” surgery in the eye. Theobservation that crashed fighter pilots were ableto tolerate small pieces of perspex in their eyesled to the use of acrylic intraocular implants, thelens of the eye being replaced by an artificialone. Such spare-part surgery has now becomecommonplace, as will be seen in Chapter 11. Theoperating microscope was introduced in the1960s, and with it came the development of finesuture materials and the use of instruments toosmall for manipulation with the naked eye. This

The Scope of Ophthalmology 5
in turn has led to small incision techniques andsutureless surgery, which has made the day-casecataract operation a routine. Forty years ago,the vitreous was a surgical no-man’s land, butinstruments have now been developed that cancut, aspirate and inject fluid simultaneously, allthese procedures being carried out throughfine-bore needles. Membranes, blood or foreignbodies can now be removed from the vitreousas a routine. Much important eye disease isinherited and it is not surprising that veryimportant advances have occurred recently inthe field of ophthalmic genetics. The gene con-trolling the development of the eye has nowbeen identified and perhaps the answer to thetragic problem of inherited degenerative retinaldisease is on the horizon.
In the early days of the development of thespecialty, a number of specialised hospitals were built throughout the UK. The first of thesewas Moorfields Eye Hospital, founded largely tocombat the epidemic of trachoma, which wasprevalent in London at the time. Subsequentlyother eye hospitals appeared in the main citiesof this country, often the result of pressures oflocal needs such as the treatment of industrialaccidents. In recent years, there has been a ten-dency for eye departments to become incorpo-rated within the larger district general hospitals,although individual eye hospitals remain andare still being built.
Making a Career in OphthalmologyOphthalmology is a popular specialty and so theaspiring eye surgeon can expect considerablecompetition. There are certain essential require-ments. First, an initial interest in physics and
optics is helpful and most important is a considerable degree of manual dexterity. Goodbinocular vision goes along with the manualdexterity demanded by microscopic surgery.That is to say, the future surgeon should see wellout of each eye and should be able to use theeyes together to give proper stereoscopic vision.
In many cases, an interest in the subject isaroused in medical school by a mentor or a goodteacher. By and large, those who see ophthal-mology as a soft option are not happy in theircareer. Those who, as most doctors do, set out toimprove the lot of the patient, find the specialtyvery rewarding because it is undoubtedlyextremely effective in this respect.
In the UK, medically qualified graduates canstart their eye training with a senior houseofficer (SHO) job and thence look for a special-ist registrar post in one of the training centres.A question sometimes asked is what jobs as anSHO, other than ophthalmology, are best suitedto an eventual career in ophthalmology.Obvious ones are in plastic surgery, neurologyor neurosurgery but sometimes a seeminglyunrelated one can prove to be good experience.The membership part of the FRCOphthqualification is needed at this point and once onthe training ladder there is an exit examinationbefore training is completed. The rules abouttraining arrangements can vary from time totime and advice on this can be provided by theRoyal College of Ophthalmologists.A handbookfor trainees is supplied by the college on appli-cation. When the doctor is fully trained, he orshe can decide whether to start applying forconsultant posts or whether to gain a fellowshipin a subspecialty and perhaps obtain a higherdegree. At the present time consultant posts areoften advertised as requiring some specialexpertise, such as paediatric ophthalmology orretina surgery.
IntroductionThe eye is the primary organ of vision. Each oneof the two eyeballs is located in the orbit, whereit takes up about one-fifth of the orbital volume(Figure 2.1). The remaining space is taken up by the extraocular muscles, fascia, fat, bloodvessels, nerves and the lacrimal gland.
The eye is embryologically an extension ofthe central nervous system. It shares manycommon anatomical and physiological proper-ties with the brain. Both are protected by bonywalls, have firm fibrous coverings and a dualblood supply to the essential nervous layer inthe retina. The eye and brain have internal cav-ities perfused by fluids of like composition andunder equivalent pressures. As the retina andoptic nerve are outgrowths from the brain, it isnot surprising that similar disease processesaffect the eye and central nervous system. Thephysician should constantly remind himself orherself of the many disease conditions that cansimultaneously involve the eye and the centralnervous system.
Basic Structure of the Eye andSupporting StructuresThe GlobeThe eye has three layers or coats, three com-partments and contains three fluids (Figure 2.2).
1. The three coats of the eye are as follows:(a) Outer fibrous layer:
• cornea• sclera• lamina cribrosa.
(b) Middle vascular layer (“uveal tract”):• iris• ciliary body – consisting of the pars
plicata and pars plana• choroids.
(c) Inner nervous layer:• pigment epithelium of the retina• retinal photoreceptors• retinal neurons.
2. The three compartments of the eye are asfollows:(a) Anterior chamber – the space between
the cornea and the iris diaphragm.(b) Posterior chamber – the triangular space
between the iris anteriorly, the lens andzonule posteriorly, and the ciliary body.
(c) Vitreous chamber – the space behindthe lens and zonule.
3. The three intraocular fluids are as follows:(a) Aqueous humour – a watery, optically
clear solution of water and electrolytessimilar to tissue fluids except thataqueous humour has a low proteincontent normally.
(b) Vitreous humour – a transparent gelconsisting of a three-dimensional
2Basic Anatomy and Physiology of the Eye
7

8 Common Eye Diseases and their Management
network of collagen fibres with theinterspaces filled with polymerisedhyaluronic acid molecules and water. Itfills the space between the posteriorsurface of the lens, ciliary body andretina.
(c) Blood – in addition to its usual func-tions, blood contributes to the main-tenance of intraocular pressure. Mostof the blood within the eye is in thechoroid. The choroidal blood flow rep-resents the largest blood flow per unittissue in the body. The degree ofdesaturation of efferent choroidalblood is relatively small and indicatesthat the choroidal vasculature hasfunctions beyond retinal nutrition. Itmight be that the choroid serves as aheat exchanger for the retina, whichabsorbs energy as light strikes theretinal pigment epithelium.
Clinically, the eye can be considered to becomposed of two segments:
1. Anterior segment – all structures from(and including) the lens forward.
2. Posterior segment – all structures post-erior to the lens.
The Outer Layer of the EyeThe anterior one-sixth of the fibrous layer of theeye is formed by the cornea. The posterior five-
sixths are formed by the sclera and laminacribrosa. The cornea is transparent, whereas thesclera, which is continuous within it, is white.The junction of cornea and sclera is known asthe limbus. The cornea has five layers antero-posteriorly (Figure 2.3):
1. Epithelium and its basement membrane –stratified squamous type of epitheliumwith five to six cell layers of regulararrangement.
2. Bowman’s layer – homogeneous sheet ofmodified stroma.
3. Stroma – consists of approximately 90% of total corneal thickness. Consists oflamellae of collagen, cells and ground substance.
4. Descemet’s membrane – the basementmembrane of the endothelium.
5. Endothelium – a single layer of cells liningthe inner surface of Descemet’s membrane.
Cornea Iris
Ciliary body
Conjunctiva
Sclera
Choroid
Retina
Figure 2.2. Layers of the globe.
Epithelium
Bowman’s membrane
Stroma
Descemet’s membraneEndothelium
Figure 2.3. The cornea.
Semilunar folds
Upper palpebral furrow
Upper punctum
Caruncle
Lower punctumOpenings of tarsal glands
Mucocutaneous junction
Figure 2.1. Surface anatomy.

In the region of the limbus, the epithelium onthe outer surface of the cornea becomes con-tinuous with that of the conjunctiva, a thin,loose transparent nonkeratinising mucousmembrane that covers the anterior part of thesclera, from which it is separated by loose con-nective tissue. Above and below, the conjunctivais reflected onto the inner surface of the upperand lower lids. This mucous membrane, there-fore, lines the posterior surface of the eyelids and there is a mucocutaneous junction on the lid margin. Although the conjunctiva is con-tinuous, it can be divided descriptively into threeparts: palpebral (tarsal), bulbar and fornix.
The sclera consists of irregular lamellae ofcollagen fibres. Posteriorly, the external two-thirds of the sclera become continuous with thedural sheath of the optic nerve, while the innerone-third becomes the lamina cribrosa – thefenestrated layer of dense collagen fibresthrough which the nerve fibres pass from theretina to the optic nerve. The sclera is thickestposteriorly and thinnest beneath the insertionsof the recti muscles. There is a layer of looseconnective tissue deep to the conjunctiva, over-lying the sclera, called the episclera.
Middle LayerThe middle layer is highly vascular. If one wereto peel the sclera away from this layer (not aneasy task), the remaining structure wouldresemble a grape, as this middle layer, which iscalled the uvea, is heavily pigmented as well asbeing vascular. The anterior part of the uveaforms the bulk of the iris body and henceinflammation of the iris is called either anterioruveitis or iritis. The posterior part of the uvea iscalled the choroid.
The iris is the most anterior part of the uvea.It is a thin circular disc perforated centrally by the pupil. Contraction of the iris sphinctermuscle constricts the pupil, while contraction ofthe dilator pupillae muscle dilates the pupil.
The ciliary body is part of the uveal tissue andis attached anteriorly to the iris and the scleralspur; posteriorly it is continuous with thechoroid and retina. The ciliary body is alsoreferred to as the intermediate uvea.
The ciliary body is triangular in cross-section. The anterior side of the ciliary body isthe shortest and borders the anterior chamberangle; it gives origin to the iris. The outer side
of the triangle (mainly ciliary muscles) liesagainst the sclera. The inner side is divided intotwo zones: (1) the pars plicata forms the ant-erior 2 mm and is covered by ciliary processesand (2) the pars plana constitutes the posterior4.5-mm flattened portion of the ciliary body.The pars plana is continuous with the choroidand retina.
The choroid consists of the following:
• Bruch’s membrane – membrane on theexternal surface of the retinal pigmentepithelium (RPE). It consists of the base-ment membrane of RPE cells and chorio-capillaris. Between the two layers ofbasement membrane are the elastic andcollagenous layers. Small localised thick-enings of Bruch’s membrane (whichincrease with age) are called drusen.
• The choriocapillaris – a network of capil-laries supplying the RPE and outer retina.
• Layer of larger choroidal blood vesselsexternal to the choriocapillaris.
• Pigmented cells scattered in the choroidexternal to the choriocapillaris.
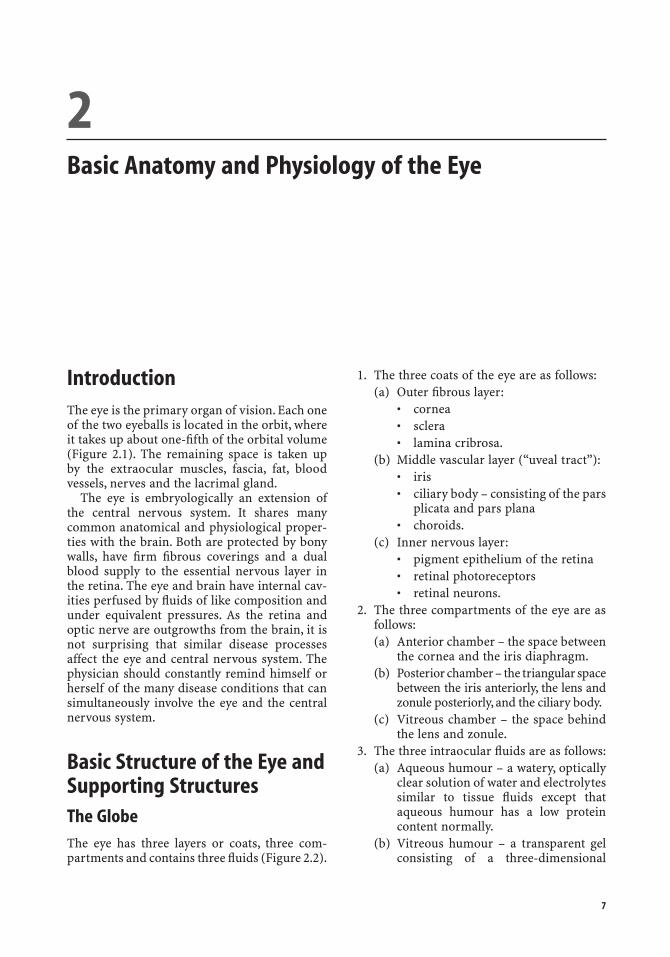
Inner LayerThe inner layer of the eye, which lines the vas-cular uvea, is the neurosensory layer. This layerforms the retina posteriorly; but, anteriorly itcomes to line the inner surface of the ciliarybody and iris as a two-layered pigment epithe-lium. These same layers can be traced into theretina, which is composed of an outer pigmentepithelium and an inner sensory part, whichcontains the rods and cones, bipolar cells andganglion cells (Figure 2.4). The junction of theretina and the pars plana forms a scallopedborder known as the ora serrata.
It is important to note that the photoreceptorcells are on the external side of the sensoryretina. The relationship of the retinal elementscan be understood most readily by following theformation of the optic cup. As the single-celllayer optic vesicle “invaginates” to form the two-cell layered optic cup, the initially superficialcells become the inner layer of the cup. The RPEdevelops from the outer layer of the cup, facingthe photoreceptors across the now obliteratedcavity of the optic vesicle. The neurons of thesensory retina differentiate from the inner layerof the optic cup.
Basic Anatomy and Physiology of the Eye 9
10 Common Eye Diseases and their Management
Blood SupplyThe blood supply of the globe is derived fromthree sources: the central retinal artery, theanterior ciliary arteries and the posterior ciliaryarteries. All these are derived from the ophthal-mic artery, which is a branch of the internalcarotid. The central retinal artery runs in theoptic nerve to reach the interior of the eye andits branches spread out over the inner surface ofthe retina supplying its inner half. The anteriorciliary arteries emerge from the insertion of therecti muscles and perforate the globe near theiris root to join an arterial circle in the ciliarybody. The posterior ciliary arteries are the finebranches of the ophthalmic artery, which pene-trate the posterior pole of the eye. Some of thesesupply the choroid and two or more largervessels run anteriorly to reach the arterial circlein the ciliary body. The larger vessels are knownas the long posterior ciliary arteries, and thosesupplying the choroid are known as the shortposterior ciliary arteries. The branches of thecentral retinal artery are accompanied by anequivalent vein, but the choroid, ciliary body and iris are drained by approximately fourvortex veins. These leave the posterior fourquadrants of the globe and are familiar land-marks for the retina surgeon (Figure 2.5).
Optic NerveThe optic nerve meets the posterior part of theglobe slightly nasal to the posterior pole andslightly above the horizontal meridian. Insidethe eye this point is seen as the optic disc. Thereare no light-sensitive cells on the optic disc –and hence the blind spot that anyone can find intheir field of vision. The optic nerve containsabout one million nerve fibres, each of whichhas a cell body in the ganglion cell layer ofthe retina (Figure 2.6). Nerve fibres sweep across the innermost part of the retina to reach
Ganglion cells
Bipolar cells
Rods and cones
Choroid
Pigment epithelium
Figure 2.4. The retina.
Lacrimal gland
Lacrimal artery
Long posterior ciliary artery
Optic nerve
Ophthalmic artery
Internal carotid artery
Figure 2.5. Blood supply of the eye.
MaculaOptic disc
Figure 2.6. The optic fundus.

Basic Anatomy and Physiology of the Eye 11
and pain is also sometimes experienced duringlaser coagulation treatment of the chorioretina– this would seem to prove the existence ofsensory fibres in the iris and choroid. Thecornea is extremely sensitive, but again, the onlysensory endings are those for pain.
The visual pathways include the following:
1. The retina:• rods and cones• bipolar cells• ganglion cells.
2. Axons of the ganglion cells visual andpupillary reflex pathways:• nerve fibre layer of retina• optic nerve• optic chiasm• optic tract.
3. Subcortical centres and relays:• superior colliculus – reflex control of
eye movements• pretectal nuclei – pupillary reflexes• lateral geniculate body – cortical relay.
4. Cortical connections:• optic radiations• visual cortex (area 17) – vision and
reflex eye movements• association areas (areas 18 and 19)• frontal eye field – voluntary eye
movements.
If the rods and cones are considered analo-gous to the sensory organs for touch, pressure,temperature, etc. then the bipolar cells may becompared to the first-order sensory neurons of the dorsal root ganglia. By the same token,the retinal ganglion cells can be compared to the second-order sensory neurons, whose cellbodies lie within the spinal cord or medulla.
The EyelidsThe eyelids may be divided into anterior andposterior parts by the mucocutaneous junction– the grey line (Figure 2.8). The eyelashes arisefrom hair follicles anterior to the grey line, whilethe ducts of the meibomian glands (modifiedsebaceous glands) open behind the grey line.The meibomian glands are long and slender,and run parallel to each other, perpendicular tothe eyelid margin, and are located in the tarsal
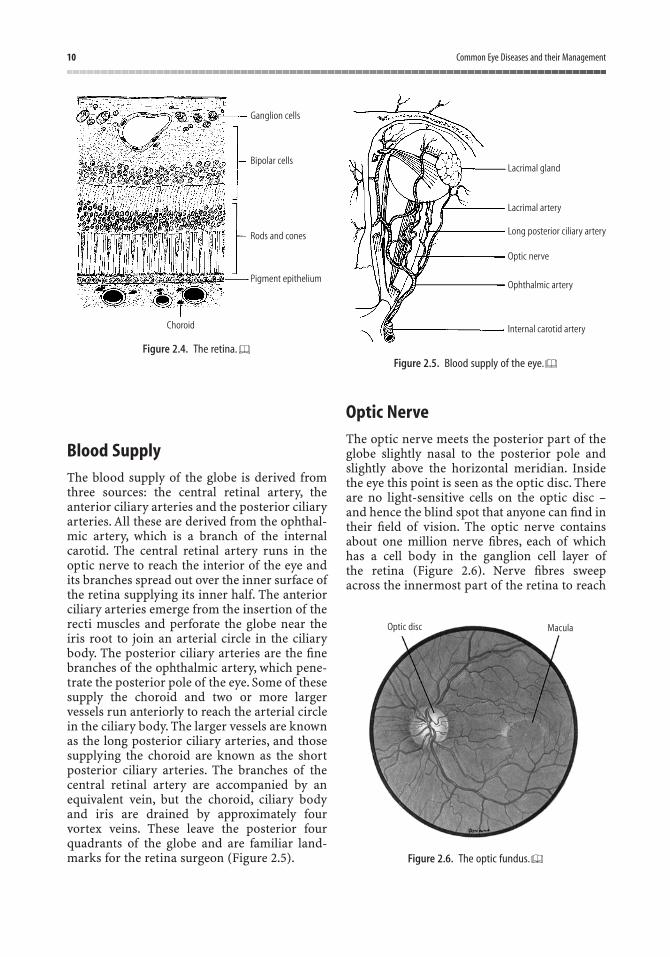
the optic disc. They can be seen with the ophthalmoscope by carefully observing the waylight is reflected off the inner surface of theretina (Figure 2.7). The retinal vessels are alsoembedded on the inner surface of the retina.There is therefore a gap, which is the thicknessof the transparent retina, between the retinalvessels and the stippled pigment epithelium.Apart from the optic nerve, the posterior pole ofthe globe is also perforated by several long andshort ciliary nerves. These contain parasympa-thetic, sympathetic and sensory fibres, whichmainly supply muscles of the iris (dilator andsphincter) and ciliary body (ciliary muscles).Patients can experience pain when the iris ishandled under inadequate local anaesthesia,
Figure 2.7. The normal fundus of a a Caucasian and b anAfrican. The background is darker in the African owing toincreased pigment in the retinal pigment epithelium (RPE). Thenerve fibre layer is noticeable, especially along the superior andinferior temporal arcades.
a
b

12 Common Eye Diseases and their Management
plate of the eyelids. The tarsal plate gives stiff-ness to the eyelids and helps maintain itscontour. The upper and lower tarsal plates areabout 1 mm thick. The lower tarsus measuresabout 5 mm in height, while the upper tarsusmeasures about 10–12 mm.
The orbicularis oculi muscle lies between the skin and the tarsus and serves to close theeyelids. It is supplied by the facial nerve. Theskin and subcutaneous tissue of the lids arethin. The inner surface of the eyelids is lined bythe palpebral conjunctiva.
The Lacrimal ApparatusThe major lacrimal gland occupies the superiortemporal anterior portion of the orbit. It hasducts that open into the palpebral conjunctivaabove the upper border of the upper tarsus.
Tears collect at the medial part of the palp-ebral fissure and pass through the puncta andthe canaliculi into the lacrimal sac, which term-inates in the nasolacrimal duct inferiorly. The
nasolacrimal duct opens into the inferiormeatus of the nose.
The Extraocular MusclesThere are six extraocular muscles that help tomove the eyeball in different directions: thesuperior, inferior, medial and lateral recti, andthe superior and inferior obliques. All thesemuscles are supplied by the third cranial nerveexcept the lateral rectus (supplied by the sixthnerve) and superior oblique (fourth nerve).
All the extraocular muscles except the inferior oblique originate from a fibrous ringaround the optic nerve (annulus of Zinn) at theorbital apex. The muscles fan out towards theeye to form a “muscle cone”. All the rectimuscles attach to the eyeball anterior to theequator while the oblique muscles attach behindthe equator. The optic nerve, the ophthalmicblood vessels and the nerves to the extraocularmuscles (except fourth nerve) are containedwithin the muscle cone (Figure 2.9).
The levator palpebrae superioris is associatedwith the superior rectus. It arises from justabove the annulus of Zinn, runs along the roofof the orbit overlying the superior rectus andattaches to the upper lid skin and anteriorsurface of the tarsal plate of the upper lid.Tenon’s capsule is a connective tissue coveringthat surrounds the eye and is continuous withthe fascial covering of the muscles.
Levator muscle of Muller
Levatorexpansion
Orbicularisoculi
Opening ofmeibomiangland
Figure 2.8. The eyelid.
Medialrectus
Superior oblique
Levator palpebrae superioris
Superior rectus
Optic nerve
Inferior rectus
Figure 2.9. Anatomy of the orbit.
Physiology of the EyeThe primary function of the eye is to form a clearimage of objects in our environment. Theseimages are transmitted to the brain through theoptic nerve and the posterior visual pathways.The various tissues of the eye and its adnexa are thus designed to facilitate this function.
The EyelidsFunctions include: (1) protection of the eyefrom mechanical trauma, extremes of temp-erature and bright light, and (2) maintenance of the normal precorneal tear film, which isimportant for maintenance of corneal healthand clarity.
Normal eyelid closure requires an intactnerve supply to the orbicularis oculi muscles(facial nerve). Eyelid opening is affected by thelevator palpebrae superioris supplied by theIIIrd cranial nerve.
The Tear FilmThe tear film consists of three layers: themucoid, aqueous and oily layers.
The mucoid layer lies adjacent to the cornealepithelium. It improves the wetting properties ofthe tears. It is produced by the goblet cells in theconjunctival epithelium.
The watery (aqueous) layer is produced bythe main lacrimal gland in the superotemporalpart of the orbit and accessory lacrimal glandsfound in the conjunctival stroma. This aqueouslayer contains electrolytes, proteins, lysozyme,immunoglobulins, glucose and dissolvedoxygen (from the atmosphere).
The oily layer (superficial layer of the tearfilm) is produced by the meibomian glands(modified sebaceous glands) of the eyelidmargins. This oily layer helps maintain the ver-tical column of tears between the upper andlower lids and prevents excessive evaporation.
The tears normally flow away through adrainage system formed by the puncta (inferiorand superior), canaliculi (inferior and sup-erior), the common canaliculus (opening intothe lacrimal sac) and the nasolacrimal duct(which drains into the nose).
The CorneaThe primary function of the cornea is refrac-tion. In order to perform this function, thecornea requires the following:
• transparency• smooth and regular surface• spherical curvature of proper refractive
power• appropriate index of refraction.
Corneal transparency is contributed to byanatomical and physiological factors:
1. Anatomical:• absence of keratinisation of epithelium• tight packing of epithelial cells• mucous layer providing smooth lubri-
cated surface• homogeneity of membranes – Bowman’s
and Descemet’s• regular arrangement of corneal lamel-
lae (parallel collagen fibres within eachlamella, with adjacent lamellae beingperpendicular). Regularity produces adiffraction grating
• paucity of corneal stromal cells, whichare flattened within lamellae
• interspaces – absence of blood vessels.2. Physiological
• active dehydration of the corneathrough Na+/HCO3
- metabolic pumplocated in the corneal endothelium.This dehydration is supplemented bythe physical barrier provided by thecorneal epithelium and endothelium.
The Aqueous HumourThe aqueous humour is an optically clear sol-ution of electrolytes (in water) that fills thespace between the cornea and the lens. Normalvolume is 0.3 ml. Its function is to nourish thelens and cornea.
The aqueous is formed by active secretion andultrafiltration from the ciliary processes in theposterior chamber. The fluid enters the anteriorchamber through the pupil,circulates in the anter-ior chamber and drains through the trabecularmeshwork into the canal of Schlemm,the aqueousveins and the conjunctival episceral veins.
Basic Anatomy and Physiology of the Eye 13
14 Common Eye Diseases and their Management
The aqueous normally contains a low con-centration of proteins, but a higher concentra-tion of ascorbic acid compared with plasma.Inflammation of the anterior uvea leads toleakage of proteins from the iris circulation intothe aqueous (= plasmoid aqueous).
The Vitreous BodyThe vitreous consists of a three-dimensionalnetwork of collagen fibres with the interspacesfilled with polymerised hyaluronic acid mole-cules, which are capable of holding large quan-tities of water. The vitreous does not normallyflow but is percolated slowly by small amountsof aqueous. There is liquefaction of the jelly withage, with bits breaking off to form floaters. Thisdegeneration occurs at an earlier age in myopes.
The LensThe lens, like the cornea, is transparent. It isavascular and depends on the aqueous for nour-ishment. It has a thick elastic capsule, which prevents molecules (e.g., proteins) moving intoor out of it.
The lens continues to grow throughout life,newlens fibres being produced from the outside andmoving inwards towards the nucleus with age.
The lens is comprised of 65% water and 35%protein. The water content of the lens decreaseswith age and the lens becomes less pliable.
The lens is suspended from the ciliary body by the zonule, which arises from the ciliary bodyand inserts into the lens capsule near the equator.
The Ciliary BodyThe ciliary muscle (within the ciliary body) is amass of smooth muscle, which runs circumfer-entially inside the globe and is attached to thescleral spur anteriorly. It consists of two mainparts:
1. Longitudinal (meridional) fibres – formthe outer layers and arise from the scleralspur and insert into the choroid. Contrac-tion of this part of the muscle exerts trac-tion on the trabecular meshwork and alsothe choroid and retina.
2. Circular fibres – form the inner part andrun circumferentially. Contraction movesthe ciliary processing inwards towards thecenter of the pupil leading to relaxation ofthe zonules.
AccommodationAccommodation is the process whereby relax-ation of zonular fibres allows the lens to becomemore globular, thereby increasing its refractivepower. When the ciliary muscles relax, thezonular fibres become taut and flatten the lens,reducing its refractive power. This is associatedwith constriction of the pupil and increaseddepth of focus.
Accommodation is a reflex initiated by visualblurring and/or awareness of proximity ofthe object of interest. The maximum amount of accommodation (amplitude of accommo-dation) is dependent on the rigidity of the lensand contractility of the ciliary muscle. As thelens becomes more rigid with age (and contrac-tions of the ciliary body reduce), accommo-dation decreases. Reading and other close work become impossible without optical correction – presbyopia.
The RetinaThis is the “photographic film” of the eye thatconverts light into electrical energy (transduc-tion) for transmission to the brain. It consists oftwo main parts:
1. The neuroretina – all layers of the retinathat are derived from the inner layer of theembryological optic cup.
2. The RPE – derived from the outer layer ofthe optic cup. It is comprised of a singlelayer of cells, which are fixed to Bruch’smembrane. Bruch’s membrane separatesthe outer retina from the choroid.
The retinal photoreceptors are located on theouter aspect of the neuroretina, an arrangementthat arose from inversion of the optic cup andallows close proximity between the photosens-itive portion of the receptor cells and theopaque RPE cells, which reduce light scattering.The RPE also plays an important role in regeneration/recycling of photopigments of theeye and during light–dark adaptation.

In order for the light to reach the photo-receptors to form sharp images, all layers of theretina inner to the photoreceptors must betransparent. This transparency is contributed toby the absence of myelin fibres from the retinalneurons. The axons of the retina ganglion cellsnormally become myelinated only as they passthrough the optic disc to enter the optic nerve.
There are two main types of photoreceptorsin the retina – the rods and the cones. In thefovea centralis the only photoreceptors arecones, which are responsible for acute vision(visual details) and colour vision. Outside thefovea, rods become more abundant towards theretinal periphery. The rods are responsible for
vision in poor (dim) light and for the wide fieldof vision.
The retinal capillary network (derived fromthe central retinal artery) extends no deeperthan the inner nuclear layer and nourishes theneuroretina from inside up to part of the outerplexiform layer. It is an end-arterial system. Thechoroid serves to nourish the RPE and the photoreceptors (by diffusion of nutrients).There are no blood vessels in the outer retina.The central fovea is completely avascular anddepends on diffusion from the choroidal circ-ulation for its nourishment. Thus, normal func-tioning of the retina requires normal retinal andchoroidal circulation.
Basic Anatomy and Physiology of the Eye 15

As in all other medical examinations, examin-ation of a patient with an eye problem shouldinclude history, physical examination andspecial investigation. The age as well as socialhistory, including the occupation of the patient,should not be forgotten in such evaluation. Asummary of such evaluation is provided inTable 3.1.
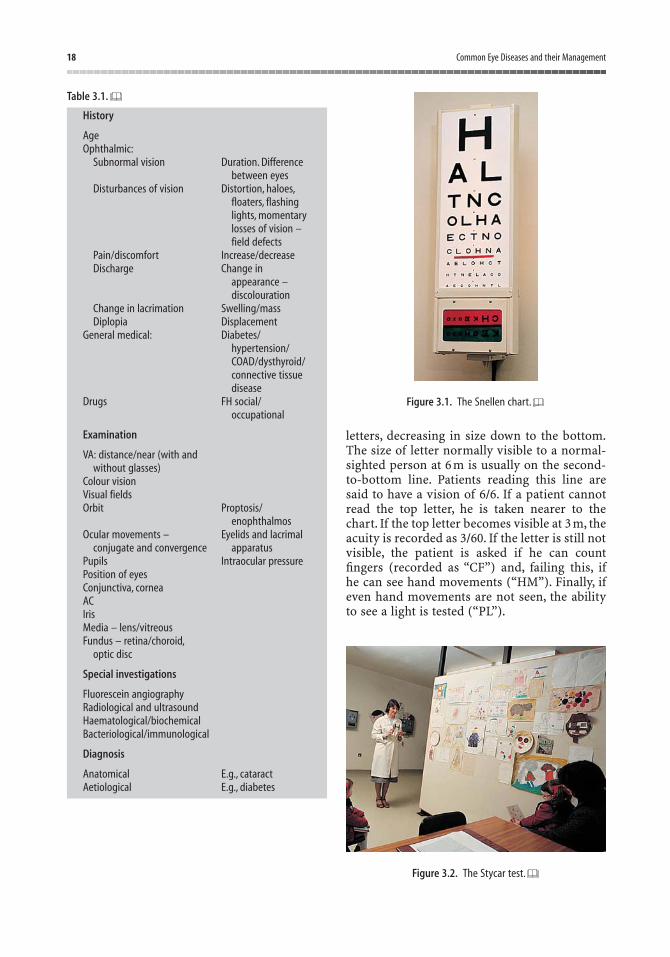
How to Find Out What aPatient Can SeeOne obvious way to measure sight is to ask thepatient to identify letters that are graded in size.This is the basis of the standard Snellen test forvisual acuity (Figure 3.1). This test only meas-ures the function of a small area of retina at theposterior pole of the eye called the macula. If westare fixedly at an object, for example a pictureon the wall, and attempt to keep our eyes as stillas possible, it soon becomes apparent that wecan only appreciate detail in a small part of thecentre of the field of vision. Everything aroundus is ill-defined and yet we can detect the slight-est twitch of a finger from the corner of our eyes.The macula region is specialised to detect finedetail, whereas the whole peripheral retina isconcerned with the detection of shape andmovement. In order to see, we use the periph-eral retina to help us scan the field of view. Theperipheral retina can be considered as equiv-alent to the television cameraman who moves
the camera around to the relevant views andallows the camera (or macula) to make sense ofthe scene. If the macula area is damaged by, forexample, age-related macular degeneration, thepatient might be unable to see even the largestprint on the test type and yet have no difficultyin walking about the room. Navigational visionis largely dependent on the peripheral field ofvision. On the other side of the coin, the patientwith marked constriction of the peripheral fieldof vision but preservation of the central fieldmight behave as though blind. The same patientcould read the test chart down to the bottomonce he has found it. This situation sometimesarises in patients with advanced chronic simple glaucoma.
It should be becoming clear that measuringthe visual acuity, although very useful, is not anadequate measure of vision on its own. For aproper clinical examination, we need to assessthe visual fields and colour vision. A number ofother facets of visual function can also be meas-ured, such as dark adaptation or the perceptionof flicker.
Visual AcuityThe familiar Snellen chart has one large letter atthe top, which is designed to be just visible to anormal-sighted person at 60 m. The chart isviewed from a distance of 6 m. If a patient is justable to see this large letter, the vision is recordedas 6/60. Below the large letter are rows of smaller
3Examination of the Eye
17
18 Common Eye Diseases and their Management
Table 3.1.
History
AgeOphthalmic:
Subnormal vision Duration. Difference between eyes
Disturbances of vision Distortion, haloes,floaters, flashing lights, momentary losses of vision – field defects
Pain/discomfort Increase/decreaseDischarge Change in
appearance – discolouration
Change in lacrimation Swelling/massDiplopia Displacement
General medical: Diabetes/hypertension/COAD/dysthyroid/connective tissue disease
Drugs FH social/occupational
Examination
VA: distance/near (with andwithout glasses)
Colour visionVisual fieldsOrbit Proptosis/
enophthalmosOcular movements – Eyelids and lacrimal
conjugate and convergence apparatusPupils Intraocular pressurePosition of eyesConjunctiva, corneaACIrisMedia – lens/vitreousFundus – retina/choroid,
optic disc
Special investigations
Fluorescein angiographyRadiological and ultrasoundHaematological/biochemicalBacteriological/immunological
Diagnosis
Anatomical E.g., cataractAetiological E.g., diabetes
letters, decreasing in size down to the bottom.The size of letter normally visible to a normal-sighted person at 6 m is usually on the second-to-bottom line. Patients reading this line aresaid to have a vision of 6/6. If a patient cannotread the top letter, he is taken nearer to thechart. If the top letter becomes visible at 3 m, theacuity is recorded as 3/60. If the letter is still notvisible, the patient is asked if he can countfingers (recorded as “CF”) and, failing this, ifhe can see hand movements (“HM”). Finally, ifeven hand movements are not seen, the abilityto see a light is tested (“PL”).
Figure 3.1. The Snellen chart.
Figure 3.2. The Stycar test.

Examination of the Eye 19
Young children and illiterates can be asked todo the “E” test, in which they must orient a largewooden letter “E” so that it is the same way upas an indicated letter “E” on a chart. Perhapsbetter than this is the Stycar test (Figure 3.2), inwhich the child is asked to point at the letter ona card that is the same as the one held up at 6 m. Other ways of measuring visual acuity arediscussed in Chapter 17.
Visual FieldSome measurements of the visual field can bemade by sitting facing the patient and asking ifthe movement of one’s fingers can be discerned.The patient is instructed to cover one eye witha hand and the observer also covers one of hiseyes so that he can check the patient’s fieldagainst his own. The test can be made moreaccurate by using a pin with a red head on it asa target. None of these confrontation methodscan match the accuracy of formal perimetry. Anumber of specialised instruments of varyingcomplexity are available. Using such equipment,the patient is presented with a number ofdifferent-sized targets in different parts of thevisual field, and a map of the field of vision ischarted. An accurate map of the visual field isoften of great diagnostic importance. In thepast, it was customary to map out the centralpart of the visual field using the Bjerrum screen,and the peripheral field using a perimeter. TheGoldmann perimeter was then introduced, andthis instrument allows both central and periph-eral fields to be plotted out on one chart. TheHumphrey field analyser is a further develop-ment in field testing. It provides an automatedvisual field recording system (Figure 3.3). It also
records the reliability of the patient by showingfalse-positive and false-negative errors. In prac-tice this is very useful, as poor reliability is oftenan explanation for poor performance.
Colour VisionThe Ishihara plates provide a popular and effec-tive method for screening for colour visiondefects (Figure 3.4). The patient is presentedwith a series of plates on which are printednumerous coloured dots. The normal-sightedsubject will see numbers on the majority of theplates, whereas the colour-defective patient willfail to see many of the numbers. The test is easyto do and will effectively screen out the morecommon red–green deficiency found in 8% ofthe male population. There are other tests avail-able that will measure blue–green defects, forexample, the City University test. Other tests,such as the Farnsworth 100 Hue test, are avail-able for the more detailed analysis of colourvision.
SpectaclesMeasurement of the visual acuity might not bevalid unless the patient is wearing the correctspectacles. Some patients, when asked to read aSnellen chart, will put on their reading glasses.As these glasses are designed for close work,the chart might be largely obscured and theuninitiated doctor might be surprised at the poor level of visual acuity (Figure 3.5). If theFigure 3.3. The Humphrey field analyser.
Figure 3.4. Ishihara plates for colour vision.

20 Common Eye Diseases and their Management
glasses have been left at home, long sight orshort sight can be largely overcome by askingthe patient to view the chart through a pinhole.Similarly, an appropriate spectacle correction(near) must be worn when testing visual fieldsand colour vision. In an ophthalmic depart-ment, a check of the spectacle prescription is aroutine part of the initial examination. Figure3.6 shows how the converging power of theoptical media and the length of the eye are mis-matched to produce the need to wear spectacles(the dotted lines indicate the paths for rays oflight without any corrective lens).
How to Start Examining an EyeEvaluating the PupilExamination of the pupil is best performed in adimly lit room.
Size and symmetry of pupils is assessed byasking the patient to fixate on a distant object,such as a letter on the Snellen chart. A dim lightis then directed on to the face from below so thatboth pupils can be seen simultaneously in thediffuse illumination. Normally, the two pupils inany individual are of equal size, although slightdifferences in size might be observed in up to20% of the population. Usually, physiologicalunequal pupils (anisocoria) remain unalteredby changing the background illumination.
In order to assess the pupil light reflex, astrong focal light is shone on the pupils, oneafter the other. The direct reaction and the consensual reaction (other pupil) are observed.If the afferent arc of the pupil pathway werenormal, the direct and consensual reactionswould be equal.
To assess the near response of the pupil, askthe patient to gaze at a distant object (e.g.,Snellen chart), then at a near object (e.g., hisown finger tip just in front of his nose). Observethe pupil as the patient changes gaze fromdistant to near fixation and vice versa. Gener-ally, if the pupil light reflex is intact, the nearreflex is normal.
External Eye and LidsThe eyelids should be inspected to make surethat the lid margins and puncta are correctly
I borrowed my husband‘s glasses. . . .
Figure 3.5. The uninitiated might be surprised at the poor levelof visual acuity.
HYPERMETROPE MYOPE
Figure 3.6. Optical defects of the eye.

Examination of the Eye 21
aligned against the globe and that there are noingrowing lashes. Early basal cell carcinomas(also known as rodent ulcers) on eyelid skin caneasily be missed, especially if obscured by cos-metics. The presence of ptosis should be notedand the ocular movements assessed by askingthe patient to follow a finger upwards, down-wards and to each side. Palpation of the skinaround the eyes can reveal an orbital tumour orswollen lacrimal sac. Palpation with the end ofa glass rod is sometimes useful to find points oftenderness when the lid is diffusely swollen.Such tenderness can indicate a primary infec-tion of a lash root or the lacrimal sac. Both sur-faces of the eyelids should be examined. Theinside of the lower lid can easily be inspected bypulling down the skin of the lid with the indexfinger. The upper lid can be everted by askingthe patient to look down, grasping the lashesgently between finger and thumb, and rollingthe lid margins upwards and forwards over acotton-wool bud or glass rod. The lid willusually remain in this everted position until thepatient is asked to look up. Foreign bodies quiteoften lodge themselves under the upper lid andthey can only be removed by this means. As ageneral rule, if a patient complains that there issomething in his eye, there usually is, and if youfind nothing, it is necessary to look again moreclosely or refer the patient for microscopicexamination. A feeling of grittiness can resultfrom inflammation of the conjunctiva and thismight be accompanied by evidence of purulentdischarge in the lashes. The presence of tearoverflow and excoriation of the skin in the outercanthus should also be noted.
The GlobeMuch ophthalmic disease has been describedand classified using the microscope. In spite ofthis, many of the important eye diseases can bediagnosed using a hand magnifier and anophthalmoscope. At this point, it is important tounderstand the principle of examining the eyewith a focused beam of light. If a pencil of lightis directed obliquely through the cornea andanterior chamber, it can be made to illuminatestructures or abnormalities that are otherwiseinvisible. One might inspect the glass sides andwater of a fish tank using a strong, focused torchin the same manner (Figure 3.7). Many ophthal-moscopes incorporate a focused beam of light
that can be used for this purpose. A magnifiedimage of the anterior segment of the eye can beviewed with a direct ophthalmoscope heldabout 1/3 m away from the eye through a +10 or+12 lens. The principle has been developed to ahigh degree in the slit-lamp (Figure 3.8). Thisinstrument allows a focused slit of light to beshone through the eye, which can then be exam-ined by a binocular microscope. By this means,an optical section of the eye can be created.The method can be compared with making a histological section, where the slice oftissue is made with a knife rather than a beam
Figure 3.7. Focal illumination.
Figure 3.8. Slit-lamp examination.

22 Common Eye Diseases and their Management
of light. The slit-lamp is sometimes called thebiomicroscope. By means of such optical aids,the cornea must be carefully inspected for scarsor foreign bodies. The presence of vascular con-gestion around the corneal margin might be ofsignificance. Closer inspection of the iris mightshow that it is atrophic or fixed by adhesions.Turbidity or cells in the aqueous might be seenin the beam of the inspection light. The lens andanterior parts of the vitreous can be examinedby the same means.
Once the anterior segment of the eye has beenexamined, the intraocular pressure is measured.The “gold-standard” method of measurement isto use the Goldmann tonometer (Figure 3.9),which relies on the principle of “applanation”.In essence, the application of this principle provides a derived measurement of intraocularpressure by flattening a small known area ofcornea with a variable force.The amount of forcerequired to flatten a specific area is proportionalto the intraocular pressure reading, and this is
read from a dial. The readings provided by thismeasurement are highly reproducible and aregiven in millimetres of mercury (mmHg).
Some optometrists, however, employ “air-puff” tonometers, which are more portable anddo not require attachment to a slit-lamp. Theseinstruments are excellent for screening but are generally not as accurate as applanationtonometers. A convenient hand-held instru-ment (the Tonopen) is available (Figure 3.10)and is commonly used by ophthalmologistswhen a slit-lamp is not available.
At this stage, the pupil can be dilated for better examination of the fundi and opticalmedia. A short-acting mydriatic is preferable,for example tropicamide 1% (Mydriacyl). Theseparticular drops take effect after 10 min and take 2–4 h to wear off. Patients should be warned thattheir vision will be blurred and that they will bemore sensitive to light over this period. Mostpeople find that their ability to drive a car isunimpaired, but there is a potential medicolegalrisk if the patient subsequently has a car accid-ent. Once the pupils have been dilated, the eyecan then be examined with the ophthalmoscope.
How to Use theOphthalmoscopeBefore the middle of the nineteenth century,nobody had seen the inside of a living eye andmuch of the science of medical ophthalmologywas unknown. In 1851, Hermann von Helmholtzintroduced his ophthalmoscope and it rapidlybecame used in clinics dealing with ophthalmo-logical problems. The task of von Helmholtz wasto devise a way of looking through the blackpupil and, at the same time, illuminate the interior of the globe. He solved the problem byFigure 3.9. The Goldmann tonometer.
Figure 3.10. The Tonopen.

Examination of the Eye 23
arranging to view the fundus of the eye throughan angled piece of glass. A light projected fromthe side was reflected into the eye by total inter-nal reflection. Most modern ophthalmoscopesemploy an angled mirror with a small hole in itto achieve the same end. They also incorporatea series of lenses that can be interposed betweenthe eye of the patient and that of the observer,thereby overcoming any refractive problemsthat might defocus the view. These lenses arepositioned by rotating a knurled wheel at theside of the ophthalmoscope. A number on theface of the instrument indicates the strength ofthe lens. When choosing an ophthalmoscope, itis worth remembering that large ones takelarger batteries, which last longer (or, better still,they might have rechargeable batteries); smallophthalmoscopes are handy for the pocket.Some ophthalmoscopes have a wider field ofview than others and this is an advantage whenlearning to use the instrument.
If examining the patient’s right eye, it is bestto hold the ophthalmoscope in the right handand view through one’s own right eye. A left eyeshould be viewed with the left eye using the lefthand (Figure 3.11). It is best if the patient isseated and the doctor is standing. The first thingto observe is the red reflex, which simply refersto the general reddish colouring seen throughthe pupil. If viewed from about 30 cm away fromthe eye, slight and subtle opacities or defects inthe optical media can be seen against the back-ground of the red reflex. The patient’s eye mustalways be brought into focus by rotating the lenswheel on the ophthalmoscope.
Having observed the red reflex, the eye can be approached closely and the focus of the
ophthalmoscope adjusted so that fundus detailbecomes visible. It is best to look for the opticdisc first, remembering its position nasal to theposterior pole and slightly above the horizontalmeridian. The patient should be asked to lookstraight ahead at this point. The importantpoints to note about the disc are the clarity ofthe margins, the colour, the nature of the centralcup, the vessel entry and the presence orabsence of haemorrhages. Once the disc hasbeen examined carefully, the vessels from thedisc can be followed. For example, the uppertemporal branch vessels can be followed out tothe periphery and back, then the lower tempo-ral branch vessels, then the upper nasal vesselsand then, finally, the lower nasal vessels. Havingexamined the vessels, ask the patient to lookdirectly at the ophthalmoscope light and themacular region should come into view. At first,this might look unremarkable, like a minute dotof light that follows our own light. More carefulexamination will reveal that it has a yellowishcolour. To obtain a highly magnified view ofthe macular region, it is usually necessary toexamine it with a special contact lens on the slit-lamp microscope, the Goldmann fundus lens. Afundus photograph is also helpful.After viewingthe macula, the general fundus backgroundshould be observed. The appearance heredepends on the complexion of the patient: in alightly pigmented subject, it is possible to seethrough the stippled pigment epithelium andobtain an indefinite view of the choroidal vas-culature. In heavily pigmented subjects, thepigment epithelium is uniformly black and prevents any view of the choroid, which liesbehind it. Finally, the peripheral fundus can beinspected by asking the patient to look to theextremes of gaze and by refocusing the ophthal-moscope. Examining the peripheral fundusdemands some special skill, even with theordinary ophthalmoscope, but it is best seenusing the triple-mirror gonioscope. This is amodified contact lens that has an angled mirrorattached to it. A view through this mirror isobtained using the slit-lamp microscope.
There are a number of other methods ofexamining the fundus. The ophthalmoscopedescribed above is known as the direct ophthal-moscope. The indirect ophthalmoscope wasintroduced shortly after direct ophthalmoscopy.If one examines an eye with the pupil dilatedthrough a mirror with a hole in it, the patientFigure 3.11. Direct ophthalmoscopy.
24 Common Eye Diseases and their Management
being at arm’s length from the observer and themirror being held close to the observer’s eye, thered reflex is seen. If a convex lens is placed inthe line of sight about 8 cm from the patient’seye, then, rather surprisingly, a clear wide fieldinverted view of the fundus is obtained. Theview can be made binocular, and the binocularindirect ophthalmoscope is an essential tool ofthe retinal surgeon (Figure 3.12). If we want a highly magnified view of the fundus, the slit-lamp microscope can be used. However, aspecial lens must be placed in front of thepatient’s eye. This can be in the form of thetriple-mirror contact lens (Figure 3.13). Inrecent years, it has become a routine practice toexamine the fundus with the slit-lamp andstrong convex lenses (e.g., VOLK +60, +78 or+90DS aspheric lenses). These high-power
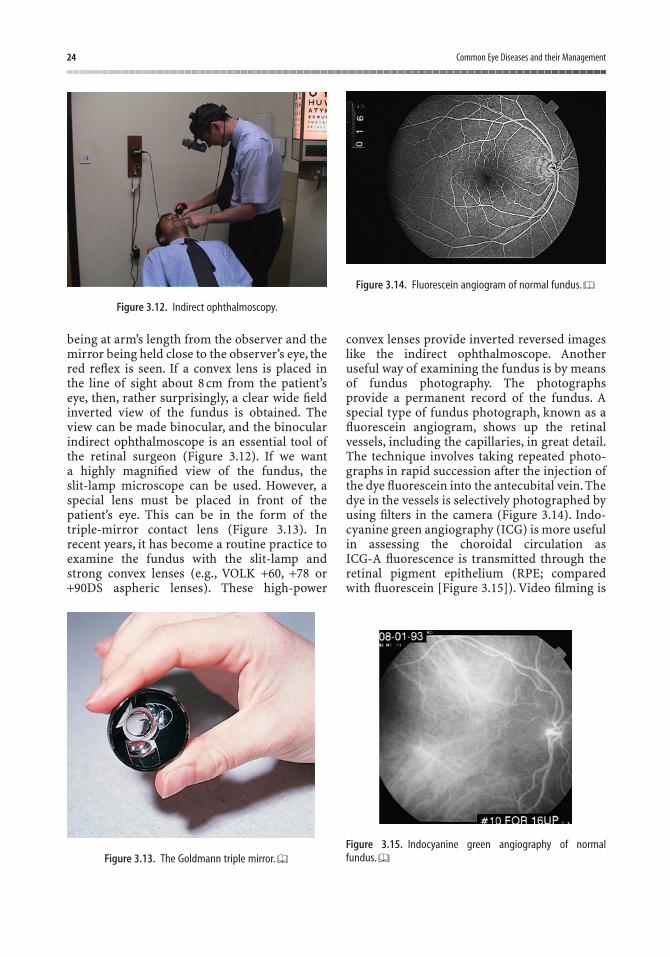
convex lenses provide inverted reversed imageslike the indirect ophthalmoscope. Anotheruseful way of examining the fundus is by meansof fundus photography. The photographsprovide a permanent record of the fundus. Aspecial type of fundus photograph, known as afluorescein angiogram, shows up the retinalvessels, including the capillaries, in great detail.The technique involves taking repeated photo-graphs in rapid succession after the injection ofthe dye fluorescein into the antecubital vein. Thedye in the vessels is selectively photographed byusing filters in the camera (Figure 3.14). Indo-cyanine green angiography (ICG) is more usefulin assessing the choroidal circulation as ICG-A fluorescence is transmitted through theretinal pigment epithelium (RPE; comparedwith fluorescein [Figure 3.15]). Video filming is
Figure 3.12. Indirect ophthalmoscopy.
Figure 3.13. The Goldmann triple mirror.
Figure 3.14. Fluorescein angiogram of normal fundus.
Figure 3.15. Indocyanine green angiography of normal fundus.
Examination of the Eye 25
becoming an important method for observingchanging events in the fundus and it is now pos-sible to view a real-time image of the opticfundus on a television screen using the scanninglaser ophthalmoscope. This type of equipmentwill undoubtedly become a routine tool for theophthalmologist.
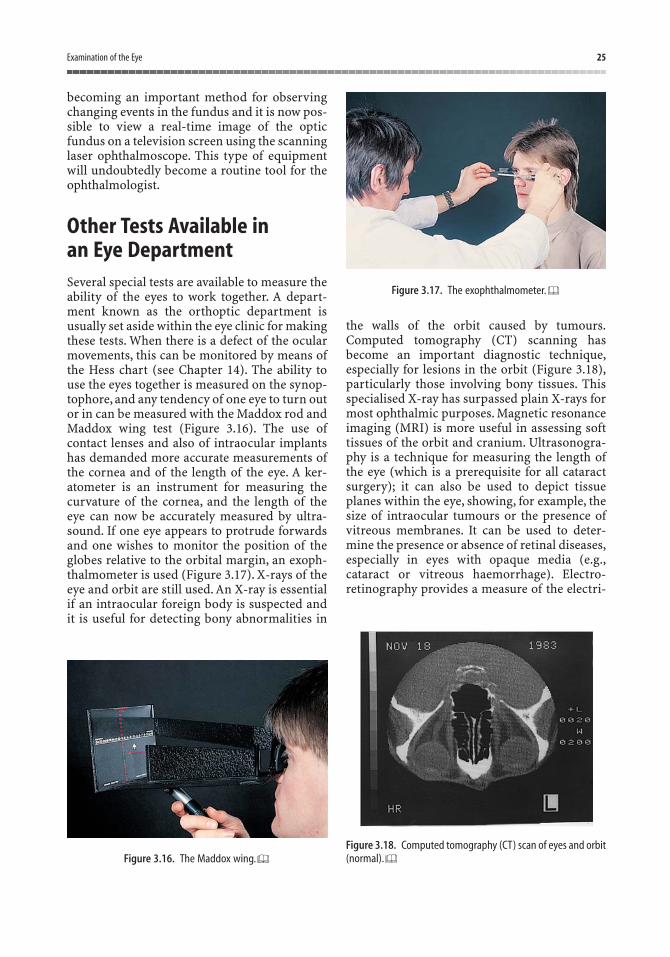
Other Tests Available in an Eye DepartmentSeveral special tests are available to measure theability of the eyes to work together. A depart-ment known as the orthoptic department isusually set aside within the eye clinic for makingthese tests. When there is a defect of the ocularmovements, this can be monitored by means ofthe Hess chart (see Chapter 14). The ability touse the eyes together is measured on the synop-tophore, and any tendency of one eye to turn outor in can be measured with the Maddox rod andMaddox wing test (Figure 3.16). The use ofcontact lenses and also of intraocular implantshas demanded more accurate measurements ofthe cornea and of the length of the eye. A ker-atometer is an instrument for measuring thecurvature of the cornea, and the length of theeye can now be accurately measured by ultra-sound. If one eye appears to protrude forwardsand one wishes to monitor the position of theglobes relative to the orbital margin, an exoph-thalmometer is used (Figure 3.17). X-rays of theeye and orbit are still used. An X-ray is essentialif an intraocular foreign body is suspected andit is useful for detecting bony abnormalities in
the walls of the orbit caused by tumours.Computed tomography (CT) scanning hasbecome an important diagnostic technique,especially for lesions in the orbit (Figure 3.18),particularly those involving bony tissues. Thisspecialised X-ray has surpassed plain X-rays formost ophthalmic purposes. Magnetic resonanceimaging (MRI) is more useful in assessing softtissues of the orbit and cranium. Ultrasonogra-phy is a technique for measuring the length ofthe eye (which is a prerequisite for all cataractsurgery); it can also be used to depict tissueplanes within the eye, showing, for example, thesize of intraocular tumours or the presence ofvitreous membranes. It can be used to deter-mine the presence or absence of retinal diseases,especially in eyes with opaque media (e.g.,cataract or vitreous haemorrhage). Electro-retinography provides a measure of the electri-
Figure 3.16. The Maddox wing.
Figure 3.17. The exophthalmometer.
Figure 3.18. Computed tomography (CT) scan of eyes and orbit(normal).

26 Common Eye Diseases and their Management
cal changes that take place in the retina whenthe eye is exposed to light. It can indicate retinalfunction in the same way that the electrocar-diogram indicates cardiac function. The visuallyevoked potential is a measure of minute electri-cal changes over the back of the scalp, whichoccur when the eyes are stimulated with aflashing light. This test has been shown to beuseful in detecting previous damage to the opticnerve in patients with suspected multiple sclerosis.
Technological advances have led to increas-ing dependence on imaging devices, such asdigital fundus cameras for retinal screening in patients with diabetes. In addition, recentlaser technologies, such as the Heidelberg retina tomograph, allow for a quick and easyway of scanning the optic nerve head in three dimensions (Figure 3.19) and the retinal nerve fibre layer. This is especiallyhelpful in evaluating changes in patients withglaucoma.
Figure 3.19. The Heidelberg retina tomograph.

Section IIPrimary Eye Care Problems
The aim of this section is to present some of themore commonly occurring eye conditions thatare likely to confront a casualty officer in thegeneral or eye casualty department, or a general
practitioner in his or her surgery. Some of theconditions can also be treated at primary carelevel but referral for more extensive investiga-tion and treatment is often required.
It is useful to distinguish between long-sightedand short-sighted patients as you will see laterin this chapter, but straight away we come acrossa problem with terminology. Think of the“short-sighted” old man who cannot see to readwithout glasses and, at the same time, the“short-sighted” young lady who cannot seeclearly in the distance. The term “short sight” isused in these instances unwittingly by thelayman to mean two different situations; eitherit can mean presbyopia (caused by diminishedfocusing power with ageing, as in the case of theold man) or it can mean myopia (caused by alarger eyeball, as in the case of the young lady).
Leaving aside presbyopia for the time being,we need to realise that the myopic person hasphysically larger than normal eyes, with ananteroposterior diameter of more than 24 mm,and, by contrast, the hypermetropic (or long-sighted person) person has smaller than usualeyes, with an anteroposterior diameter of lessthan 24 mm. To obtain a clear image, this abnor-mal length of the eye needs optical correctionwith a lens to bring light rays to a focus on theretina. The hypermetropic requires a convexlens to converge the rays, whereas the myopicperson requires a concave lens to make lightrays diverge before reaching the eye.
Glasses with convex lenses in them make theeyes look bigger and glasses with concave lensesin them make the eyes look smaller. Figure 4.1shows a long-sighted (hypermetropic) patientwhose glasses seem to enlarge the eyes andFigure 4.2 shows a short-sighted (myopic)
patient. The clinical importance of this is thatwith a little practice the physician can tell thedifference at a glance as the patient enters the room. This often helps with the diagnosisbecause certain eye diseases are associated withmyopia and others with hypermetropia.
The nature of the spectacle correction can beverified by moving the lens from side to side infront of one’s hand. If the hand appears to movein the opposite direction to that of the move-ment of the spectacle lens, it is convex (Figure4.3). The spectacles of the myopic patientcontain concave, or diverging, lenses and, ifthese are moved to and fro in front of one’shand, the hand appears to move in the samedirection as the movement. As a further clue,when we look at the hypermetrope from a slightangle, the line of the cheek goes out behind themagnifying lenses and vice versa for the myope(see Figures 4.1 and 4.2).
Here, again, let us remind ourselves thathypermetropia and myopia have nothing to dowith presbyopia, which is the failure of the eyesto focus on near objects, appearing in middleage. This is nothing to do with the length of theeyeball but is related to a diminished ability tochange the shape of the lens. It is corrected inotherwise normal eyes by using a convex lens.Obviously myopes, hypermetropes and thosewith no refractive error are all susceptible to presbyopia.
When we examine hypermetropic andmyopic eyes with the ophthalmoscope, we findthat there are physical differences between the
4Long Sight, Short Sight
29

30 Common Eye Diseases and their Management
Figure 4.1. A long-sighted person.
Figure 4.2. A short-sighted person.
Figure 4.3. Concave lens “with”; convex lens “against”. Try thisfor yourself in the clinic.
two. The optic disc of the hypermetrope tendsto be smaller and pinker, and in extreme cases,especially in children, the disc can appear to beswollen when in fact it is quite normal. By con-trast, the optic disc of the myope is larger andpaler with well-defined margins and can be mis-taken for an atrophic disc.
Hypermetropia is associated with certain eyeconditions, notably narrow-angle glaucoma andchildhood amblyopia of disuse. Myopia is asso-ciated with other conditions, particularly retinaldetachment, cataract and myopic retinal degen-eration.You must be aware, though, that whereas
Table 4.1. Eye disease and refractive error.
Myopia (“short sight”) Hypermetropia (“long sight”)
Conditions associated Conditions associated with with myopia hypermetropia
Retinal detachment Narrow-angle glaucomaMacula haemorrhages Concomitant squintCataract Amblyopia of disuseMyopic chorioretinal
degenerationDown’s syndromeKeratoconus (conical
cornea)
Conditions causing Conditions causing myopia hypermetropia
Large eye Small eyeCataract Retinal detachmentDiabetes mellitus Orbital tumoursAccommodation spasm, Macula oedema
or “pseudomyopia”Congenital glaucoma

Long Sight, Short Sight 31
with seeing flashes of light, he may be about tohave a retinal detachment.
If we take note of whether a patient is longsighted or short sighted at an early stage, thisinformation can influence the type of questionsthat are best asked when taking a history.
Finally, it is worth remembering that themyopic patient can see objects close at hand andread without glasses at any age, whereas thehypermetropic patient has to focus to see at all distances. If the hypermetrope has goodfocusing power (i.e., the younger patient), thedistance vision may be clear without glasses but when hypermetropia is more severe, theunaided vision is poor at all ranges.
refractive errors are extremely common, theseparticular conditions are relatively rare in thegeneral population. Table 4.1 shows a more com-prehensive list of these associations.
Having observed the nature of the spectaclelenses, we have now made a small step towardsdiagnosing the eye condition. If the patient is middle aged and complaining of eveningheadaches, seeing haloes around street lightsand, at the same time, blurring of vision,narrow-angle glaucoma is the wrong diagnosisif the patient is myopic. It could well be the right diagnosis if the patient is hypermetropic. If thepatient in Figure 4.2 were to complain of thesudden appearance of black spots combined
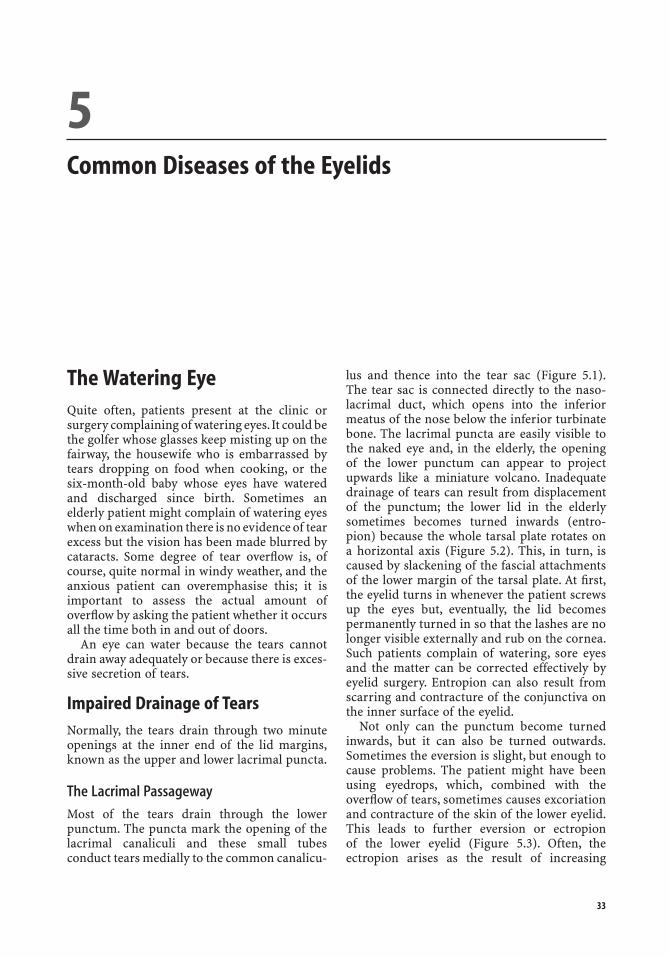
The Watering EyeQuite often, patients present at the clinic orsurgery complaining of watering eyes.It could bethe golfer whose glasses keep misting up on thefairway, the housewife who is embarrassed bytears dropping on food when cooking, or the six-month-old baby whose eyes have wateredand discharged since birth. Sometimes anelderly patient might complain of watering eyeswhen on examination there is no evidence of tearexcess but the vision has been made blurred bycataracts. Some degree of tear overflow is, ofcourse, quite normal in windy weather, and theanxious patient can overemphasise this; it isimportant to assess the actual amount ofoverflow by asking the patient whether it occursall the time both in and out of doors.
An eye can water because the tears cannotdrain away adequately or because there is exces-sive secretion of tears.
Impaired Drainage of TearsNormally, the tears drain through two minuteopenings at the inner end of the lid margins,known as the upper and lower lacrimal puncta.
The Lacrimal Passageway
Most of the tears drain through the lowerpunctum. The puncta mark the opening of thelacrimal canaliculi and these small tubesconduct tears medially to the common canalicu-
lus and thence into the tear sac (Figure 5.1).The tear sac is connected directly to the naso-lacrimal duct, which opens into the inferiormeatus of the nose below the inferior turbinatebone. The lacrimal puncta are easily visible tothe naked eye and, in the elderly, the opening of the lower punctum can appear to projectupwards like a miniature volcano. Inadequatedrainage of tears can result from displacementof the punctum; the lower lid in the elderlysometimes becomes turned inwards (entro-pion) because the whole tarsal plate rotates ona horizontal axis (Figure 5.2). This, in turn, iscaused by slackening of the fascial attachmentsof the lower margin of the tarsal plate. At first,the eyelid turns in whenever the patient screwsup the eyes but, eventually, the lid becomes permanently turned in so that the lashes are nolonger visible externally and rub on the cornea.Such patients complain of watering, sore eyesand the matter can be corrected effectively byeyelid surgery. Entropion can also result fromscarring and contracture of the conjunctiva onthe inner surface of the eyelid.
Not only can the punctum become turnedinwards, but it can also be turned outwards.Sometimes the eversion is slight, but enough tocause problems. The patient might have beenusing eyedrops, which, combined with theoverflow of tears, sometimes causes excoriationand contracture of the skin of the lower eyelid.This leads to further eversion or ectropion of the lower eyelid (Figure 5.3). Often, the ectropion arises as the result of increasing
5Common Diseases of the Eyelids
33
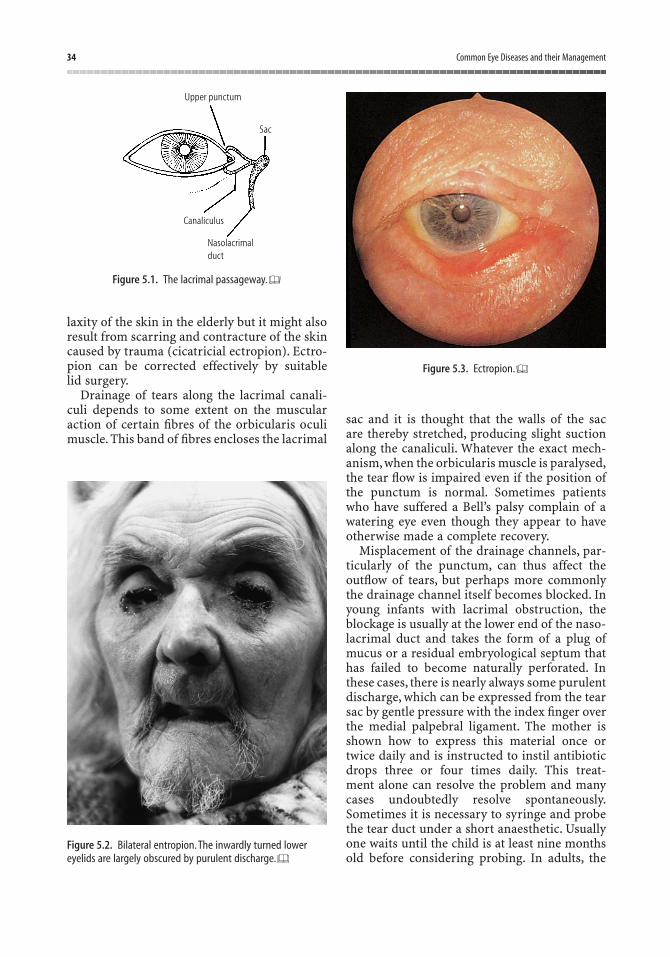
34 Common Eye Diseases and their Management
laxity of the skin in the elderly but it might alsoresult from scarring and contracture of the skincaused by trauma (cicatricial ectropion). Ectro-pion can be corrected effectively by suitable lid surgery.
Drainage of tears along the lacrimal canali-culi depends to some extent on the muscularaction of certain fibres of the orbicularis oculimuscle. This band of fibres encloses the lacrimal
sac and it is thought that the walls of the sac are thereby stretched, producing slight suctionalong the canaliculi. Whatever the exact mech-anism, when the orbicularis muscle is paralysed,the tear flow is impaired even if the position ofthe punctum is normal. Sometimes patientswho have suffered a Bell’s palsy complain of awatering eye even though they appear to haveotherwise made a complete recovery.
Misplacement of the drainage channels, par-ticularly of the punctum, can thus affect theoutflow of tears, but perhaps more commonlythe drainage channel itself becomes blocked. Inyoung infants with lacrimal obstruction, theblockage is usually at the lower end of the naso-lacrimal duct and takes the form of a plug ofmucus or a residual embryological septum thathas failed to become naturally perforated. Inthese cases, there is nearly always some purulentdischarge, which can be expressed from the tearsac by gentle pressure with the index finger overthe medial palpebral ligament. The mother isshown how to express this material once ortwice daily and is instructed to instil antibioticdrops three or four times daily. This treat-ment alone can resolve the problem and manycases undoubtedly resolve spontaneously.Sometimes it is necessary to syringe and probethe tear duct under a short anaesthetic. Usuallyone waits until the child is at least nine months old before considering probing. In adults, the
Upper punctum
Sac
Canaliculus
Nasolacrimalduct
Figure 5.1. The lacrimal passageway.
Figure 5.2. Bilateral entropion. The inwardly turned lowereyelids are largely obscured by purulent discharge.
Figure 5.3. Ectropion.
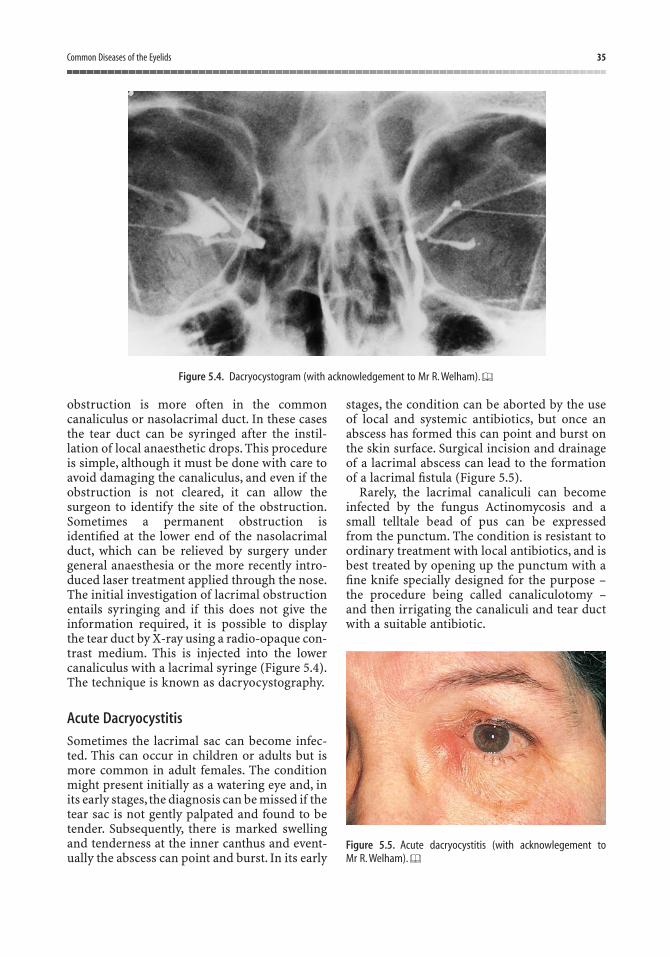
Common Diseases of the Eyelids 35
obstruction is more often in the commoncanaliculus or nasolacrimal duct. In these casesthe tear duct can be syringed after the instil-lation of local anaesthetic drops. This procedureis simple, although it must be done with care toavoid damaging the canaliculus, and even if theobstruction is not cleared, it can allow thesurgeon to identify the site of the obstruction.Sometimes a permanent obstruction isidentified at the lower end of the nasolacrimalduct, which can be relieved by surgery undergeneral anaesthesia or the more recently intro-duced laser treatment applied through the nose.The initial investigation of lacrimal obstructionentails syringing and if this does not give theinformation required, it is possible to displaythe tear duct by X-ray using a radio-opaque con-trast medium. This is injected into the lowercanaliculus with a lacrimal syringe (Figure 5.4).The technique is known as dacryocystography.
Acute Dacryocystitis
Sometimes the lacrimal sac can become infec-ted. This can occur in children or adults but ismore common in adult females. The conditionmight present initially as a watering eye and, inits early stages, the diagnosis can be missed if thetear sac is not gently palpated and found to betender. Subsequently, there is marked swellingand tenderness at the inner canthus and event-ually the abscess can point and burst. In its early
stages, the condition can be aborted by the useof local and systemic antibiotics, but once anabscess has formed this can point and burst onthe skin surface. Surgical incision and drainageof a lacrimal abscess can lead to the formationof a lacrimal fistula (Figure 5.5).
Rarely, the lacrimal canaliculi can becomeinfected by the fungus Actinomycosis and asmall telltale bead of pus can be expressed from the punctum. The condition is resistant toordinary treatment with local antibiotics, and isbest treated by opening up the punctum with afine knife specially designed for the purpose –the procedure being called canaliculotomy –and then irrigating the canaliculi and tear ductwith a suitable antibiotic.
Figure 5.4. Dacryocystogram (with acknowledgement to Mr R. Welham).
Figure 5.5. Acute dacryocystitis (with acknowlegement to Mr R. Welham).

36 Common Eye Diseases and their Management
The diagnosis of lacrimal obstruction there-fore depends firstly on an examination ofthe eyelids, secondly on syringing the tear ducts, and then if necessary dacryocystography.Figure 5.6 illustrates the diagnostic use oflacrimal syringing.
Excessive Secretion of TearsA wide range of conditions affecting the eye can cause an excessive production of tears, fromacute glaucoma to a corneal abscess, but thesedo not usually present as a watering eye becausethe other symptoms, such as pain or visual loss,are more evident to the patient. Occasionally theunwary doctor can be caught out by an irrita-tive lesion on the cornea, which mimics themore commonplace lacrimal obstruction. Forexample, a small corneal foreign body or aningrowing eyelash can present in this way. Notuncommonly, a loose lash may float into thelower lacrimal canaliculus where it mightbecome lodged, causing chronic irritation at theinner canthus. Its removal after weeks of dis-comfort produces instant relief and gratitude.
The Dry EyeA patient might complain of dryness of the eyessimply because the conjunctiva is inflamed, butwhen the tear film really is defective, the patientmight complain of soreness and irritationrather than dryness. The diagnosis of a dry eyedepends on a careful examination and it is quiteerroneous to assume that the tear film is inade-
quate simply because the patient complains ofdryness, or even if the symptoms appear to beimproved by artificial tears.
The normal tear film consists of three layersand the integrity of this film is essential forcomfort and more importantly for good vision.The anterior, or outermost, layer is formed bythe oily secretion of the meibomian glands andthe layer next to the cornea is mucinous to allowproper wetting by the watery component of thetears, which lies sandwiched between the two.This three-layered film is constantly maintainedby the act of blinking.
Causes• Systemic disease with lacrimal gland
involvement:– sarcoidosis– rheumatoid arthritis (Sjögren’s
syndrome).• Trachoma (chlamydial conjunctivitis and
keratitis – see next chapter).• Neuroparalytic keratitis.• Exposure keratitis.• Old age.• Other rare causes.
Signs
Slit-lamp Examination
In a normal subject, the tear film is evident as arim of fluid along the lid margin and adeficiency of this can be seen by direct exam-ination. Prolonged deficiency of tears can beassociated with the presence of filaments –microscopic strands of mucus and epithelialcells, which stain with Rose Bengal. Punctatestaining of the corneal epithelium is also seenafter applying a drop of fluorescein. In some dryeye syndromes, for example, ocular pemphigoidand Stevens–Johnson syndrome, keratin-isation of the cornea and conjunctiva with the formation of contracting adhesions between theopposed surfaces of the conjunctiva occurs. Asimilar change is apparent following chemicalor thermal burns of the eyes.
Schirmer’s Test
One end of a special filter paper strip is placedbetween the globe and the lower eyelid. The
13
2
Figure 5.6. Diagnostic use of lacrimal syringing. (1) Obstructionin canaliculus shown by regurgitation of saline back throughpunctum. (2) Common canaliculus obstruction shown by returnof saline through upper punctum. (3) Obstruction in naso-lacrimal duct shown by filling of lacrimal sac.
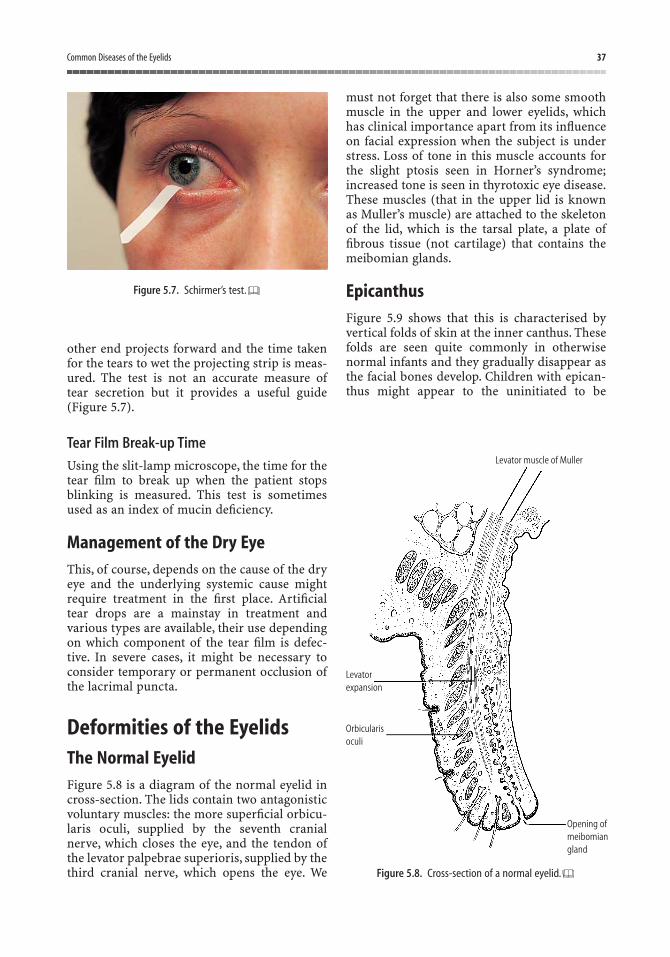
Common Diseases of the Eyelids 37
other end projects forward and the time takenfor the tears to wet the projecting strip is meas-ured. The test is not an accurate measure oftear secretion but it provides a useful guide(Figure 5.7).
Tear Film Break-up Time
Using the slit-lamp microscope, the time for thetear film to break up when the patient stopsblinking is measured. This test is sometimesused as an index of mucin deficiency.
Management of the Dry EyeThis, of course, depends on the cause of the dryeye and the underlying systemic cause mightrequire treatment in the first place. Artificialtear drops are a mainstay in treatment andvarious types are available, their use dependingon which component of the tear film is defec-tive. In severe cases, it might be necessary toconsider temporary or permanent occlusion ofthe lacrimal puncta.
Deformities of the EyelidsThe Normal EyelidFigure 5.8 is a diagram of the normal eyelid incross-section. The lids contain two antagonisticvoluntary muscles: the more superficial orbicu-laris oculi, supplied by the seventh cranialnerve, which closes the eye, and the tendon ofthe levator palpebrae superioris, supplied by thethird cranial nerve, which opens the eye. We
must not forget that there is also some smoothmuscle in the upper and lower eyelids, whichhas clinical importance apart from its influenceon facial expression when the subject is understress. Loss of tone in this muscle accounts forthe slight ptosis seen in Horner’s syndrome;increased tone is seen in thyrotoxic eye disease.These muscles (that in the upper lid is known as Muller’s muscle) are attached to the skeletonof the lid, which is the tarsal plate, a plate offibrous tissue (not cartilage) that contains themeibomian glands.
EpicanthusFigure 5.9 shows that this is characterised byvertical folds of skin at the inner canthus. Thesefolds are seen quite commonly in otherwisenormal infants and they gradually disappear asthe facial bones develop. Children with epican-thus might appear to the uninitiated to be
Figure 5.7. Schirmer’s test.
Levatorexpansion
Levator muscle of Muller
Orbicularisoculi
Opening ofmeibomiangland
Figure 5.8. Cross-section of a normal eyelid.

38 Common Eye Diseases and their Management
squinting and this can cause considerableparental anxiety. It is important to explain thatthe squint is simply an optical illusion once theabsence of any true deviation of the eyes hasbeen confirmed. Epicanthus persists into adultlife in Mongolian races, and occasionally it isseen in European adults. It can also be associ-ated with other eyelid deformities.
EntropionThis is an inversion of the eyelid. The commonform is the inversion of the lower eyelid seen inelderly patients. Often, the patient does notnotice that the eyelid is turned in but complainsof soreness and irritation. Closer inspectionreveals the inverted eyelid, which can berestored to its normal position by slight down-ward pressure on the lower eyelid, only to turnin again when the patient forcibly closes theeyes. The inwardly turned eyelashes tend to rubon the cornea and, if neglected, the conditioncan lead to corneal scarring and consequent lossof vision. The condition is often associated withmuscular eyelids and sometimes seems to beprecipitated by repeatedly screwing up the eyes.Slackening of the fascial sling of the lower eyelidwith ageing combined with the action of theorbicularis muscle allows this to happen. Thiscommon type of entropion is called spasticentropion and it can be promptly cured withoutleaving a visible scar by minor eyelid surgery.Entropion can also be seen following scarring ofthe conjunctival surface of the eyelids and onemust mention, in particular, the entropion of the
upper eyelid caused by trachoma. This is rare inthe UK but still common in the Middle East andcountries where trachoma is still rife.
EctropionThis commonly seen outward turning of thelower eyelid in the elderly is eminently treatableand responds well to minor surgery. Senileectropion can begin with slight separation ofthe lower eyelid from the globe, and the mal-position of the punctum leads to overflow oftears and conjunctival infection. Irritation of theskin by the tears and rubbing of the eyes lead toskin contracture and further downward pullingof the eyelids. Like entropion, ectropion can becicatricial and result from scarring of the skinof the eyelids. It can also follow a seventh cranialnerve palsy caused by complete inaction ofthe orbicularis muscle; this is called paralytic ectropion.
LagophthalmosThis is the term used to denote failure of properclosure of the eyelids caused by inadequateblinking or lid deformity. In all these cases, thecornea is inadequately lubricated and exposurekeratitis can develop. If untreated, this can leadto a serious situation; initially, the cornea showspunctate staining when a drop of fluorescein isplaced in the conjunctival sac and subsequently,a corneal ulcer might appear. This, in turn, canlead to the spread of infection into the eye andwithout prompt treatment with antibiotics, theeye might eventually be lost.
As a general principle, it is important torealise that the sight could be lost simplybecause the eyes cannot blink. The principleapplies especially to the unconscious or anaes-thetised patient, where a disaster can be avoidedby taping or padding the eyelids and applyingan antibiotic ointment.
BlepharospasmSlight involuntary twitching of the eyelids iscommon and not usually considered to be of any pathological significance other thanbeing a symptom of fatigue or sometimes of an anxiety state. The condition is termed“myokymia”. True blepharospasm is rare. It can
Figure 5.9. Epicanthus.

Common Diseases of the Eyelids 39
be unilateral or bilateral and cause great in-convenience and worry to the patient. It tendsslowly to become more marked over manyyears. A small proportion of patients eventuallydevelops Parkinsonism. Cases of recent onsetneed to be investigated because they mightresult from an intracranial space-taking lesion.In most cases, though, no underlying cause can be found. Patients with this type of ble-pharospasm (essential blepharospasm) canoften be treated quite effectively by injectingsmall doses of botulinum toxin into the eyelids,but these need to be repeated every few months.
Redundant Lid SkinExcessive skin on the eyelids is commonly seenin elderly people, often as a family characteris-tic. It might result from chronic oedema of theeyelids caused, for example, by thyrotoxic eyedisease or renal disease. The problem is madeworse in some cases by herniation of orbital fatthrough the orbital septum, and excision of theredundant skin and orbital fat might sometimesbe necessary.
PtosisDrooping of one upper lid is an important clin-ical sign. In ophthalmic practice, ptosis in chil-dren is usually congenital and in adults is eithercongenital or caused by a third cranial nervepalsy. These more common causes must alwaysbe kept in mind but there are a large number ofother possible ones. When confronted with apatient whose upper lid appears to droop, thefirst thing to decide is whether the eyelid reallyis drooping or whether the lid on the other sideis retracted. The upper lid might droop becausethe eye is small and hypermetropic or shrunkenfrom disease. Having eliminated the possibilityof such “pseudoptosis”, the various other causescan be considered, beginning on the skin of theeyelid – styes, meibomian cysts – and advan-cing centrally through muscle – myastheniagravis – along nerves – oculomotor palsy,Horner’s syndrome – to the brainstem. Markedptosis with the eye turned down and out and adilated pupil is an oculomotor palsy, whereasslight ptosis, often not noticed by the patient orsometimes by the doctor, is more likely to meanHorner’s syndrome. This syndrome is caused bydamage to the sympathetic nervous supply to
either upper or lower lids or both and is char-acterised by slight ptosis, small pupil, loss ofsweating on the affected side of the face andslight enophthalmos (posterior displacement ofthe globe).
The management of ptosis depends on thecause and thus on accurate diagnosis. Surgicalshortening of the levator tendon is effective insome cases of congenital ptosis and sometimesin long-standing third cranial nerve palsies.Before embarking on surgery, it is important toexclude myasthenia gravis and corneal anaes-thesia. Children with congenital ptosis need to be assessed carefully before consideringsurgery. In young children, ptosis surgery isindicated where the drooping lid threatens tocover the line of sight and where the ptosiscauses an unacceptable backwards tilt of thehead. In one rather strange type of congenitalptosis, the problem disappears when the mouthis opened and the patient might literally winkunavoidably when chewing. Careful consider-ation is needed before making the decision forsurgery in these cases.
Causes of Ptosis
• Pseudoptosis: small eye, atrophic eye, lidretraction on other side.
• Mechanical ptosis: inflammation, tumour,and excess skin.
• Myogenic ptosis: myasthenia gravis.• Neurogenic ptosis: sympathetic – Horner’s
syndrome, third cranial nerve palsy, anylesion in the pathway of these, carcinomaof the lung can cause Horner’s syndrome.
• Drugs: guanethidine eye drops causeptosis.
• Congenital: ask for childhood photograph,ask for family history.
Ingrowing Eyelashes (Trichiasis)The lashes could grow in an aberrant mannereven though the eyelids themselves are in goodposition. This might be the result of chronicinfection of the lid margins or follow trauma.Sometimes one or two aberrant lashes appearfor no apparent reason (Figure 5.10). The lashestend to rub on the cornea producing irritationand secondary infection. The condition isreferred to as “trichiasis”. When one or two
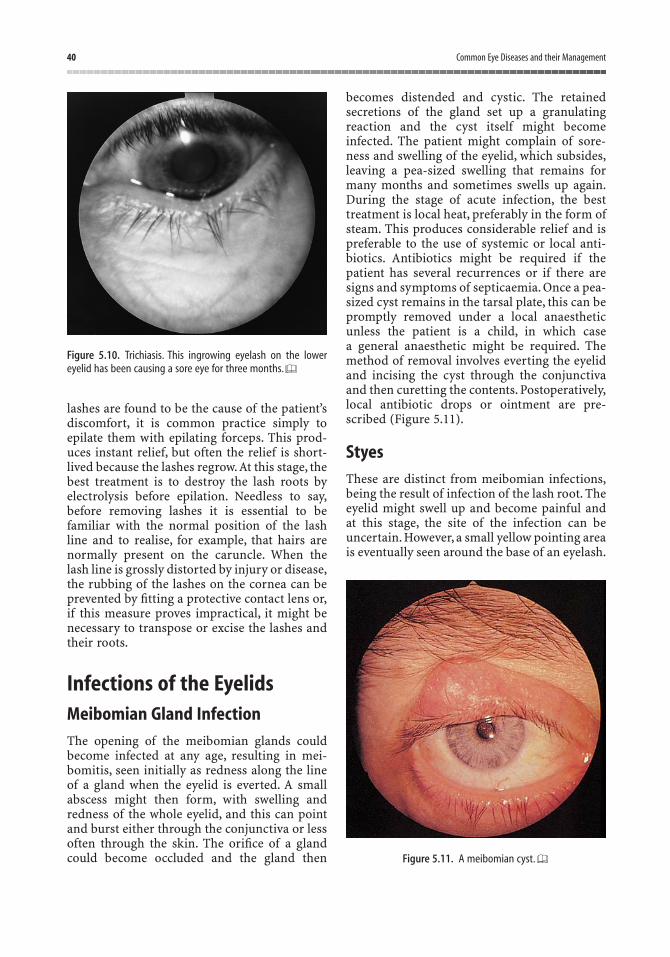
40 Common Eye Diseases and their Management
lashes are found to be the cause of the patient’sdiscomfort, it is common practice simply toepilate them with epilating forceps. This prod-uces instant relief, but often the relief is short-lived because the lashes regrow.At this stage, thebest treatment is to destroy the lash roots byelectrolysis before epilation. Needless to say,before removing lashes it is essential to befamiliar with the normal position of the lashline and to realise, for example, that hairs arenormally present on the caruncle. When the lash line is grossly distorted by injury or disease,the rubbing of the lashes on the cornea can beprevented by fitting a protective contact lens or,if this measure proves impractical, it might benecessary to transpose or excise the lashes andtheir roots.
Infections of the EyelidsMeibomian Gland InfectionThe opening of the meibomian glands couldbecome infected at any age, resulting in mei-bomitis, seen initially as redness along the lineof a gland when the eyelid is everted. A smallabscess might then form, with swelling andredness of the whole eyelid, and this can pointand burst either through the conjunctiva or lessoften through the skin. The orifice of a glandcould become occluded and the gland then
becomes distended and cystic. The retainedsecretions of the gland set up a granulatingreaction and the cyst itself might becomeinfected. The patient might complain of sore-ness and swelling of the eyelid, which subsides,leaving a pea-sized swelling that remains formany months and sometimes swells up again.During the stage of acute infection, the besttreatment is local heat, preferably in the form ofsteam. This produces considerable relief and ispreferable to the use of systemic or local anti-biotics. Antibiotics might be required if thepatient has several recurrences or if there aresigns and symptoms of septicaemia. Once a pea-sized cyst remains in the tarsal plate, this can bepromptly removed under a local anaestheticunless the patient is a child, in which case a general anaesthetic might be required. Themethod of removal involves everting the eyelidand incising the cyst through the conjunctivaand then curetting the contents. Postoperatively,local antibiotic drops or ointment are pre-scribed (Figure 5.11).
StyesThese are distinct from meibomian infections,being the result of infection of the lash root. Theeyelid might swell up and become painful andat this stage, the site of the infection can beuncertain. However, a small yellow pointing areais eventually seen around the base of an eyelash.
Figure 5.10. Trichiasis. This ingrowing eyelash on the lowereyelid has been causing a sore eye for three months.
Figure 5.11. A meibomian cyst.

Common Diseases of the Eyelids 41
Hot steaming, again, is effective treatment andonce the pus is seen, the eyelash can be gentlyepilated, with resulting discharge and sub-sequent resolution of the infection.
Children aged from about six to ten yearssometimes seem to go through periods of theirlives when they can be dogged by recurrent styesand meibomian infections, much to the distressof the parents. Under these conditions, frequentbaths and hairwashing are advised and some-times a long-term systemic antibiotic might beconsidered.Recurrent lid infections can raise thesuspicion of diabetes mellitus but in practice,this is rarely found to be an underlying cause.
Eyelid infections such as these rarely causeany serious problems other than a day or two offwork and it is extremely unusual for the infec-tion to spread and cause orbital cellulitis. Recur-rent swelling of the eyelid in spite of treatmentcan indicate the need for a lid biopsy becausesome malignant tumours can, on rare occasions,present in a deceptive manner.
BlepharitisThis refers to a chronic inflammation of the lidmargins caused by staphylococcal infection. Theeyes become red rimmed and there is usually anaccumulation of scales giving the appearance offine dandruff on the lid margins. The conditionis often associated with seborrhoea of the scalp.Sometimes it becomes complicated by recurrentstyes or chronic infection of the meibomianglands. The eye itself is not usually involved,although there could be a mild superficial punc-tate keratitis, as evidenced by fine staining of thelower part of the cornea with fluorescein. Inmore sensitive patients, the unsightly appear-ance can cause difficulties, but in more severecases, the discomfort and irritation can interferewith work. Severe recurrent infection can leadto irregular growth of the lashes and trichiasis.
In the management of these patients, it isimportant to explain the chronic nature of thecondition and the fact that certain individualsseem to be prone to it. Attention should be given to keeping the hair, face and hands asclean as possible and to avoid rubbing the eyes.When the scales are copious, they can be gentlyremoved with cotton-wool moistened insodium bicarbonate lotion twice daily. Dandruffof the scalp should also be treated with a suit-able shampoo. A local antibiotic can be applied
to the lid margins twice daily with good effectin many, but not all, cases. In severe cases withulceration of the lid margin, it might be neces-sary to consider prescribing a systemic anti-biotic, preferably after identifying the causativeorganism by taking a swab from the eyelids.Local steroids when combined with a localantibiotic are very effective treatment, but theprescriber must be aware of the dangers ofusing steroids on the eye and long-term treat-ment with steroids should be avoided. Steroidsshould not be used without monitoring theintraocular pressure.
Molluscum ContagiosumThis is a viral infection usually seen in children.The lesions on the eyelids are discrete, slightlyraised and umbilicated and usually multiple.There are also likely to be lesions elsewhere onthe body, especially the hands, and brothers orsisters might have the same problem. It is rarefor the eye itself to be involved. In persistentcases, an effective form of treatment with chil-dren is careful curettage of each lesion under ageneral anaesthetic; in adults, cryotherapy isused for individual lesions, especially if they areadjacent to the lid margin with the propensityto cause conjunctivitis.
Orbital CellulitisAlthough this is not strictly a lid infection, itmay be confused with severe meibomitis. Theinfection is deeper and the implications muchmore serious. In a child, where the condition ismore common, there is eyelid swelling, pyrexiaand malaise; urgent referral is needed. Thisapplies especially if there is diplopia or visualloss, because a scan will be required to decidewhether surgical intervention is going to beneeded to drain an infected sinus.
Lid TumoursBenign Tumours
Papilloma
Commonly seen on lids near or on the margin,these can be sessile or pedunculated, and are
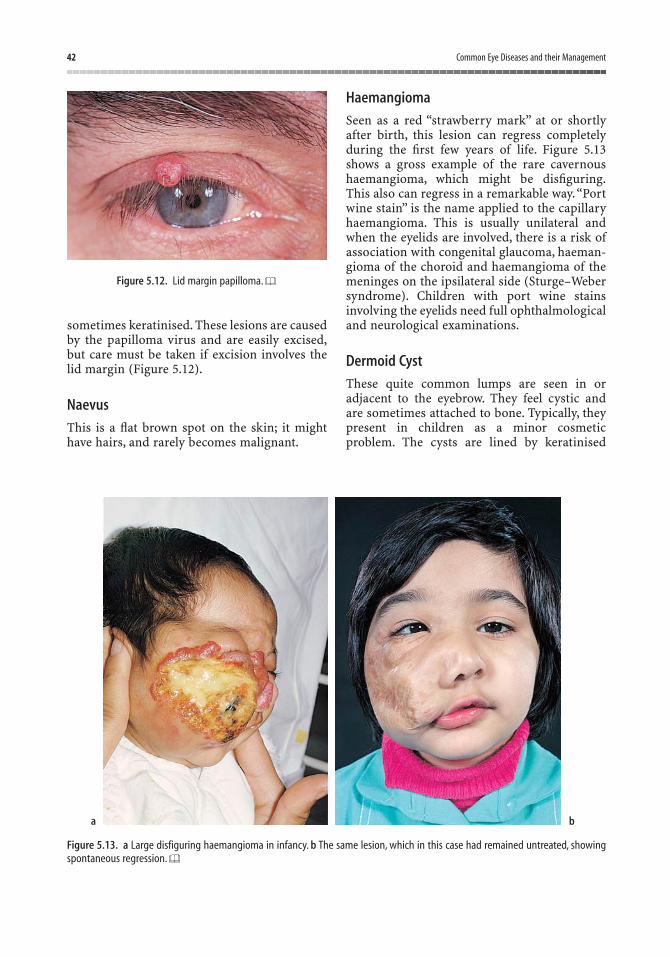
42 Common Eye Diseases and their Management
sometimes keratinised. These lesions are causedby the papilloma virus and are easily excised,but care must be taken if excision involves thelid margin (Figure 5.12).
Naevus
This is a flat brown spot on the skin; it mighthave hairs, and rarely becomes malignant.
Haemangioma
Seen as a red “strawberry mark” at or shortlyafter birth, this lesion can regress completelyduring the first few years of life. Figure 5.13shows a gross example of the rare cavernoushaemangioma, which might be disfiguring.This also can regress in a remarkable way.“Portwine stain” is the name applied to the capillaryhaemangioma. This is usually unilateral andwhen the eyelids are involved, there is a risk ofassociation with congenital glaucoma, haeman-gioma of the choroid and haemangioma of themeninges on the ipsilateral side (Sturge–Webersyndrome). Children with port wine stainsinvolving the eyelids need full ophthalmologicaland neurological examinations.
Dermoid Cyst
These quite common lumps are seen in or adjacent to the eyebrow. They feel cystic and are sometimes attached to bone. Typically, theypresent in children as a minor cosmeticproblem. The cysts are lined by keratinised
Figure 5.12. Lid margin papilloma.
Figure 5.13. a Large disfiguring haemangioma in infancy. b The same lesion, which in this case had remained untreated, showingspontaneous regression.
a b

Common Diseases of the Eyelids 43
epithelium and can contain dermal appendagesand cholesterol. A scan might be needed before removal because some extend deeply intothe skull.
Xanthelasma
These are seen as yellowish plaques in the skin;they usually begin at the medial end of the lids.They are rarely associated with diabetes, hyper-cholesterolaemia and histiocytosis. Usually,there is no associated systemic disease.
Malignant Tumours
Basal Cell Carcinoma
This is the most common malignant tumour ofthe lids, usually occurring on the lower lid. Itappears as a small lump, which tends to bleed,forming a central crust with a slightly raised hard surround. The tumour is locally invasiveonly but should be excised to avoid spread intobone.Even large lesions can be approached surg-ically (Figure 5.14) and “Mohs” micrographicsurgery is recognised as a tissue-sparing gold-standard approach in many centres. Radio-therapy is only occasionally used with a greaterrisk of recurrence than formal surgical excision.
Squamous Cell Carcinoma
This tends to resemble basal cell carcinoma and biopsy is needed to differentiate. It can alsobe mimicked by a benign self-healing lesionknown as keratoacanthoma.
Malignant Melanoma
This raised black-pigmented lesion is highlymalignant, but rare.
Allergic Disease of the EyelidsThis can present as one of two forms or a mixture of both. The more dramatic is acuteallergic blepharitis in which the eyelids swell uprapidly, often in response to contact with a plantor eyedrops. The cause must be found and elim-inated and treatment with local steroids mightbe needed. Chronic allergic blepharitis is seen inatopic individuals, for example hay fever suffer-ers or patients with a history of eczema. Thediagnosis might require a histological examin-ation of the conjunctival discharge. Drop treat-ment to alleviate symptoms includes mast cellstabilisers (such as lodoxamide) and histamineantagonists (such as emedastine), and theseagents could take weeks to take effect. Patientswith seasonal allergic conjunctivitis might require medication for a prolonged period overthe spring and summer months each year.
Lid InjuriesOne of the commonest injuries to the eyelids iscaused by the presence of a foreign body underthe eyelid – a subtarsal foreign body. A smallparticle of grit lodges near the lower margin ofthe lid, but to see it the lid must be everted.Every medical student should be familiar withthe simple technique of lid eversion. This is per-formed by gently grasping the lashes of theupper lid between finger and thumb and at thesame time placing a glass rod horizontallyacross the lid. The eyelid is then gently evertedby drawing the lid margin upwards and for-wards. The manoeuvre is only achieved if thepatient is asked to look down beforehand, andthe everted lid is replaced by asking the patientto look upwards. If a small foreign body is seen,it is usually a simple matter to remove it usinga cotton-wool bud (Figure 5.15).
Cuts on the eyelids can be caused by brokenglass or sharp objects, such as the ends of screw-drivers. The important thing here is to realisethat cuts on the lid margin can leave the patientwith a permanently watering eye if not sewn up
Figure 5.14. Cystic basal cell carcinoma that has extended toinvolve most of the upper eyelid.
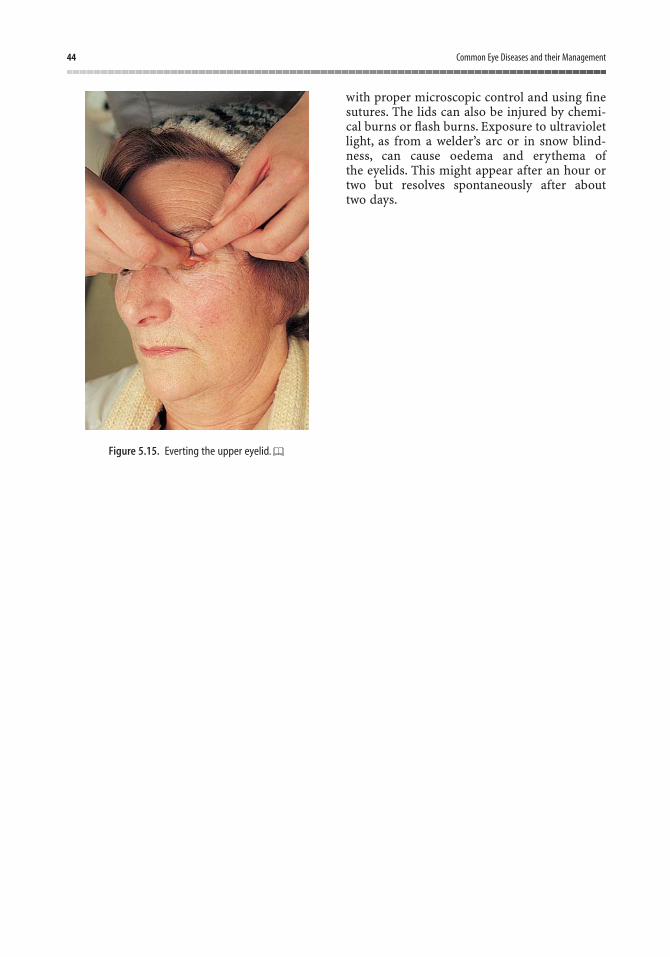
44 Common Eye Diseases and their Management
with proper microscopic control and using finesutures. The lids can also be injured by chemi-cal burns or flash burns. Exposure to ultravioletlight, as from a welder’s arc or in snow blind-ness, can cause oedema and erythema ofthe eyelids. This might appear after an hour ortwo but resolves spontaneously after about two days.
Figure 5.15. Everting the upper eyelid.
SubconjunctivalHaemorrhageThis is common and tends to occur spontaneo-usly or sometimes after straining, especiallyvomiting. It can also occur in acute haemor-rhagic conjunctivitis caused by certain virusesand occasionally bacterial conjunctivitis.The eyebecomes suddenly red and although the patientmight experience a slight pricking, the conditionis usually first noticed in the mirror or by afriend. The haemorrhage gradually absorbs inabout 14 days and investigations usually fail to reveal any underlying cause. Rarely, it is necessary to cauterise the site of bleeding if thehaemorrhage is repeated so often that it becomesa nuisance to the patient (Figure 6.1).
ConjunctivitisInflammation of the conjunctiva is extremelycommon in the general population and thegeneral practitioner is often expected to find outthe cause and treat this condition. If we considerthat the conjunctiva is a mucous membrane,which is exposed during the waking hours towind and weather more or less continuously,year in, year out, then it is not surprising thatthis membrane is rather susceptible toinflammation. Furthermore, the conjunctivacan be compared with the lining of a joint, theeye being considered as an unusual type of ball-
and-socket joint. The analogy takes on moremeaning when the relation between conjunc-tivitis and some joint diseases is seen.
There are a large number of different specificcauses of conjunctivitis. Some of these are inter-esting but rare and it is important that the studentobtains an idea of the relative importance andfrequency of the different aetiological factors.For this reason, in this chapter a more or less categorical list is given of the different causes. Inthe chapter on the red eye (Chapter 7), you willfind a plan of approach to the red eye that dealswith the importance and more common causes of conjunctivitis seen in day-to-day practice.
Although the conjunctiva is continuouslyexposed to infection, it has special protectionfrom the tears, which contain immunoglobulinsand lysozyme. The tears also help to wash awaydebris and foreign bodies and this protectiveaction can explain the self-limiting nature ofmost types of conjunctivitis.
SymptomsIn all types of conjunctivitis, the eye becomesred and feels irritable and gritty, as if there werea foreign body under the lid. There is usuallysome discharge and if marked this may makethe eyelids stick together in the mornings.Itchiness could also be present, especially incases of allergic conjunctivitis. The dischargearound the eyelids tends to make vision onlyintermittently blurred (if at all) and the patientmay volunteer that blinking clears the sight.
6Common Diseases of the Conjunctiva and Cornea
45

46 Common Eye Diseases and their Management
SignsVisual acuity is usually normal in conjunctiv-itis. The conjunctiva appears hyperaemic andthere can be evidence of purulent discharge onthe lid margins, causing matting together of theeyelashes. The redness of the conjunctivaextends to the conjunctival fornices and isusually less marked at the limbus. When a rim of dilated vessels is seen around the cornea, theexaminer must suspect a more serious inflam-matory reaction within the eye.Apart from beingred to a greater or lesser degree,the eyes also tendto water, but a dry eye might lead one to suspectconjunctivitis results from inadequate tearsecretion. Drooping of one or both upper lids isa feature of some types of viral conjunctivitisand this can be accompanied by enlargement of the preauricular lymph nodes. The ophthal-mologist should train himself or herself to feelfor the preauricular node as a routine part of theexamination of such a case. Closer inspection ofthe conjunctiva might reveal numerous smallpapillae, giving the surface a velvety look, or thepapillae may be quite large. Giant papillae underthe upper lids are a feature of spring catarrh, aform of allergic conjunctivitis. Close inspectionof the conjunctiva might also reveal follicles orlymphoid hyperplasia. Being deep to the epith-elium, they are small, pale, raised nodules and are commonly seen in viral conjunctivitis. Fol-licles under the upper lids are especially charac-teristic of trachoma.
MicroscopyThe examination of a severe case of conjunc-tivitis of unknown cause is not complete until
conjunctival scrapings have been taken. A dropof local anaesthetic is placed in the conjunctivalsac and the surface of the conjunctiva at the siteof maximal inflammation is gently scraped withthe blade of a sharp knife or a Kimura spatula.The material obtained is placed on a slide andstained with Gram’s stain and Giemsa stain. Theinfecting organism can thus be revealed or the cell type in the exudate might indicate theunderlying cause.
Conjunctival CultureIn most cases of conjunctivitis, it might be goodmedical practice to take a culture from the con-junctival sac and the eyelid margin, but such ameasure might not always be possible if amicrobiological service is not near at hand. Thecultures can be taken with sterile cotton-tippedapplicators and sent to the laboratory, in anappropriate medium, as soon as possible.
Causes• Bacterial.• Chlamydial.• Viral.• Other infective agents.• Allergic.• Secondary to lacrimal obstruction, corneal
disease, lid deformities, degenerations,systemic disease.
• Unknown cause.
Bacterial ConjunctivitisIn the UK, the commonest organisms to causeconjunctivitis are the pneumococcus, Haemo-philus spp. and Staphylococcus aureus. The lastmentioned is normally associated with chroniclid infections, and the acute purulent conjunc-tivitis, known more familiarly as “pink eye”, isusually caused by the pneumococcus. Chronicconjunctivitis can also be caused by Moraxellalacunata but this organism is rarely isolatedfrom cases nowadays. An important but rareform of purulent conjunctivitis is that caused byNeisseria gonorrhoeae; this is still an occasionalcause of a severe type of conjunctivitis seen inthe newborn babies of infected mothers.Untreated, the cornea also becomes infected,leading to perforation of the globe and perma-
Figure 6.1. Subconjunctival haemorrhage.

Common Diseases of the Conjunctiva and Cornea 47
nent loss of vision. Purulent discharge, rednessand severe oedema of the eyelids are features ofthe condition, which is generally known as oph-thalmia neonatorum (Figure 6.2). Ophthalmianeonatorum can also be caused by staphylococciand the chlamydia (see inclusion conjunctivitisof the newborn). The disease is notifiable andany infant with purulent discharge from theeyes, particularly between the second andtwelfth day postpartum, should be suspect. Atone time, special blind schools were filled withchildren who had suffered ophthalmia neonato-rum. An active campaign against this cause ofblindness began at the end of the last centurywhen Carl Crede introduced the principle ofcareful cleansing of the infant’s eyes and theinstillation of silver nitrate drops. Blindnessfrom this cause has now disappeared in the UKbut there is still a low incidence of ophthalmianeonatorum. Those affected require treatmentwith both topical medication (e.g., chloram-phenicol 0.5% eye drops) and intramuscularbenzylpenicillin (a cephalosporin, such as cefo-taxime, is an alternative). Both parents of thechild should also be assessed.
Pink eye is the name given to the type of acutepurulent conjunctivitis that tends to spreadrapidly through families or around schools. Theeyes begin to itch and within an hour or twoproduce a sticky discharge, which causes theeyelids to stick together in the mornings. If thedisease is mild, it can be treated by cleaningaway the discharge with cotton-wool, and itdoes not usually last longer than three to fivedays. More severe cases might warrant the pre-scription of antibiotic drops instilled hourlyduring the day for three days followed by fourtimes daily for five days. A conjunctival culture
should be taken before starting treatment.Commonsense precautions against spread ofthe infection should also be advised, althoughthey are not always successful.
Attempts to culture bacteria from the conjunc-tival sac of cases of chronic conjunctivitis do notyield much more than commensal organisms.
One particular kind of chronic conjunctivitisin which the inflammation is sited mainly nearto the inner and outer canthi is known asangular conjunctivitis with follicles on the superior tarsal conjunctiva. Another feature ofthis is the excoriation of the skin at the outercanthi from the overflow of infected tears. Theclinical picture has been recognised in associa-tion with infection by the bacillus M. lacunata.Often, zinc sulphate drops and the applicationof zinc cream to the skin at the outer canthusare sufficient treatment in such cases. Tetracy-cline ointment might be more effective.
Chlamydial ConjunctivitisThe chlamydia comprise a group of “largeviruses” that are sensitive to tetracycline anderythromycin and that cause relatively minordisability to the eyes in northern Europe and theUSA when compared with the severe and wide-spread eye infection seen especially in Africaand the Middle East. Inclusion conjunctivitis(“inclusion blenorrhoea”) is the milder form ofchlamydial infection and is caused by serotypeD to K of Chlamydia trachomatis. The conditionis usually, but not always, sexually transmitted.The conjunctivitis typically occurs one weekafter exposure. It can cause a more severe typeof conjunctivitis in the newborn child, whichcan also involve the cornea. The infection isusually self-limiting but often has a prolongedcourse, lasting several months. The diagnosisdepends on the results of conjunctival cultureand examination of scrapings and the associa-tion of a follicular conjunctivitis with cervicitisor urethritis.
Chlamydial conjunctivitis responds to treat-ment with tetracycline. In children and adults,tetracycline ointment should be used at leastfour times daily. In adults, the treatment can besupplemented with systemic tetracycline, butthis drug should not be used systemically inpregnant mothers or children under seven yearsof age. Azithromycin and other macrolide anti-biotics are known to be particularly effective
Figure 6.2. Ophthalmia neonatorum.

48 Common Eye Diseases and their Management
in treating systemic chlamydial infection;azithromycin can be given conveniently as aone-off dose. A referral to genitourinary med-icine is advisable on presentation, as a screeningmeasure, because reinfection from partners cantrigger a recurrent infection.
TrachomaAlthough a doctor practicing in the UK mightrarely see a case of trachoma, and even thenonly in immigrants, it is the commonest causeof blindness in the world and, furthermore, thedisease affects about 15% of the world’s pop-ulation. It is spread by direct contact and per-petuated by poverty and unhygienic conditions.Trachoma is caused by C. trachomatis serotypesA, B and C and affects underprivileged popula-tions living in conditions of poor hygiene.The disease begins with conjunctivitis, which,instead of resolving, becomes persistent, esp-ecially under the upper lid where scarring anddistortion of the lid can result. The inflam-matory reaction spreads to infiltrate the corneafrom above and ultimately the cornea itself canbecome scarred and opaque (Figure 6.3). At onetime, trachoma was common in the UK, esp-ecially after the Napoleonic wars at the end ofthe eighteenth century. It had been eliminatedby improved hygienic conditions long before theintroduction of antibiotics.
Adenoviral ConjunctivitisAcute viral conjunctivitis is common. Several ofthe adenoviruses can cause it. Usually, the eye
symptoms follow an upper respiratory tractinfection and, although nearly always bilateral,one eye might be infected before the other. Theaffected eye becomes red and discharges;characteristically, the eyelids become thickenedand the upper lid can droop. The ophthalmolo-gist’s finger should feel for the tell-tale tenderenlarged preauricular lymph node. In somecases, the cornea becomes involved and subep-ithelial corneal opacities can appear and persistfor several months (Figure 6.4). If such opacitiesare situated in the line of sight, the vision can beimpaired. There is no known effective treatmentbut it is usual to treat with an antibiotic drop toprevent secondary infection.
From time to time, epidemics of viral con-junctivitis occur and it is well recognised thatspread can result from the use of improperlysterilised ophthalmic instruments or even con-taminated solutions of eye drops, and poorhand-washing techniques.
Herpes Simplex ConjunctivitisThis is usually a unilateral follicular conjunc-tivitis with preauricular lymph node enlarge-ment. In children, it might be the only evidenceof primary herpes simplex infection.
Acute Haemorrhagic ConjunctivitisAcute haemorrhagic conjunctivitis is caused byenterovirus 70 (picornavirus) and usuallyoccurs in epidemics. The disease is hugely con-tagious but self-limiting.
Figure 6.3. Trachoma trichiasis of upper lid and corneal vasc-ularisation (with acknowledgement to Professor D. Archer).
Figure 6.4. Adenoviral keratoconjunctivitis.
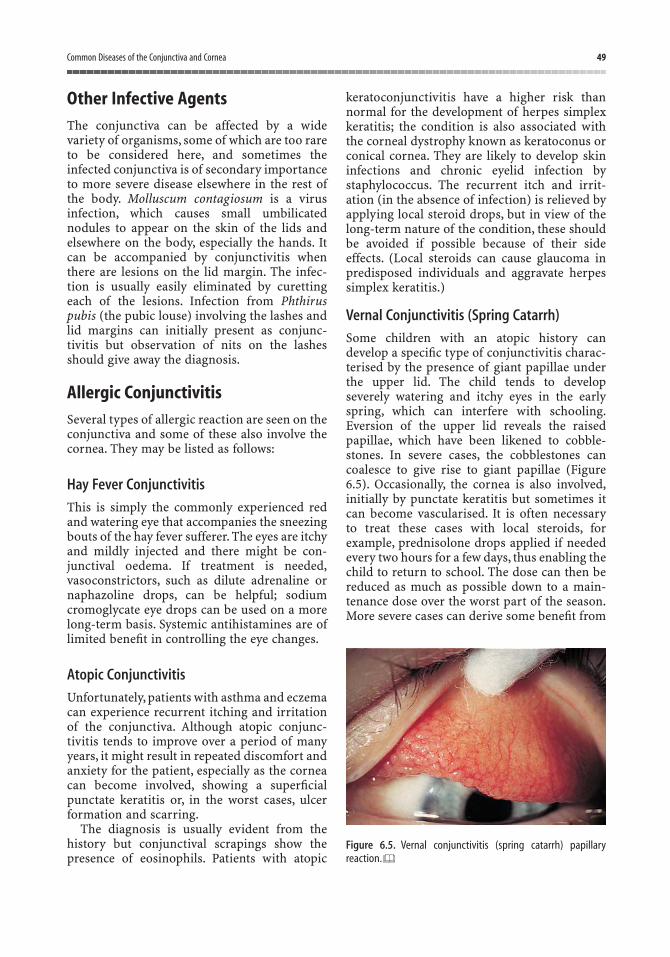
Common Diseases of the Conjunctiva and Cornea 49
Other Infective AgentsThe conjunctiva can be affected by a widevariety of organisms, some of which are too rareto be considered here, and sometimes theinfected conjunctiva is of secondary importanceto more severe disease elsewhere in the rest ofthe body. Molluscum contagiosum is a virusinfection, which causes small umbilicatednodules to appear on the skin of the lids andelsewhere on the body, especially the hands. Itcan be accompanied by conjunctivitis whenthere are lesions on the lid margin. The infec-tion is usually easily eliminated by curettingeach of the lesions. Infection from Phthiruspubis (the pubic louse) involving the lashes andlid margins can initially present as conjunc-tivitis but observation of nits on the lashesshould give away the diagnosis.
Allergic ConjunctivitisSeveral types of allergic reaction are seen on theconjunctiva and some of these also involve thecornea. They may be listed as follows:
Hay Fever Conjunctivitis
This is simply the commonly experienced redand watering eye that accompanies the sneezingbouts of the hay fever sufferer. The eyes are itchyand mildly injected and there might be con-junctival oedema. If treatment is needed,vasoconstrictors, such as dilute adrenaline ornaphazoline drops, can be helpful; sodium cromoglycate eye drops can be used on a morelong-term basis. Systemic antihistamines are oflimited benefit in controlling the eye changes.
Atopic Conjunctivitis
Unfortunately, patients with asthma and eczemacan experience recurrent itching and irritationof the conjunctiva. Although atopic conjunc-tivitis tends to improve over a period of manyyears, it might result in repeated discomfort andanxiety for the patient, especially as the corneacan become involved, showing a superficialpunctate keratitis or, in the worst cases, ulcerformation and scarring.
The diagnosis is usually evident from thehistory but conjunctival scrapings show thepresence of eosinophils. Patients with atopic
keratoconjunctivitis have a higher risk thannormal for the development of herpes simplexkeratitis; the condition is also associated withthe corneal dystrophy known as keratoconus orconical cornea. They are likely to develop skininfections and chronic eyelid infection bystaphylococcus. The recurrent itch and irrit-ation (in the absence of infection) is relieved byapplying local steroid drops, but in view of thelong-term nature of the condition, these shouldbe avoided if possible because of their sideeffects. (Local steroids can cause glaucoma inpredisposed individuals and aggravate herpessimplex keratitis.)
Vernal Conjunctivitis (Spring Catarrh)
Some children with an atopic history candevelop a specific type of conjunctivitis charac-terised by the presence of giant papillae underthe upper lid. The child tends to developseverely watering and itchy eyes in the earlyspring, which can interfere with schooling.Eversion of the upper lid reveals the raisedpapillae, which have been likened to cobble-stones. In severe cases, the cobblestones cancoalesce to give rise to giant papillae (Figure6.5). Occasionally, the cornea is also involved,initially by punctate keratitis but sometimes itcan become vascularised. It is often necessary to treat these cases with local steroids, forexample, prednisolone drops applied if neededevery two hours for a few days, thus enabling thechild to return to school. The dose can then bereduced as much as possible down to a main-tenance dose over the worst part of the season.More severe cases can derive some benefit from
Figure 6.5. Vernal conjunctivitis (spring catarrh) papillary reaction.
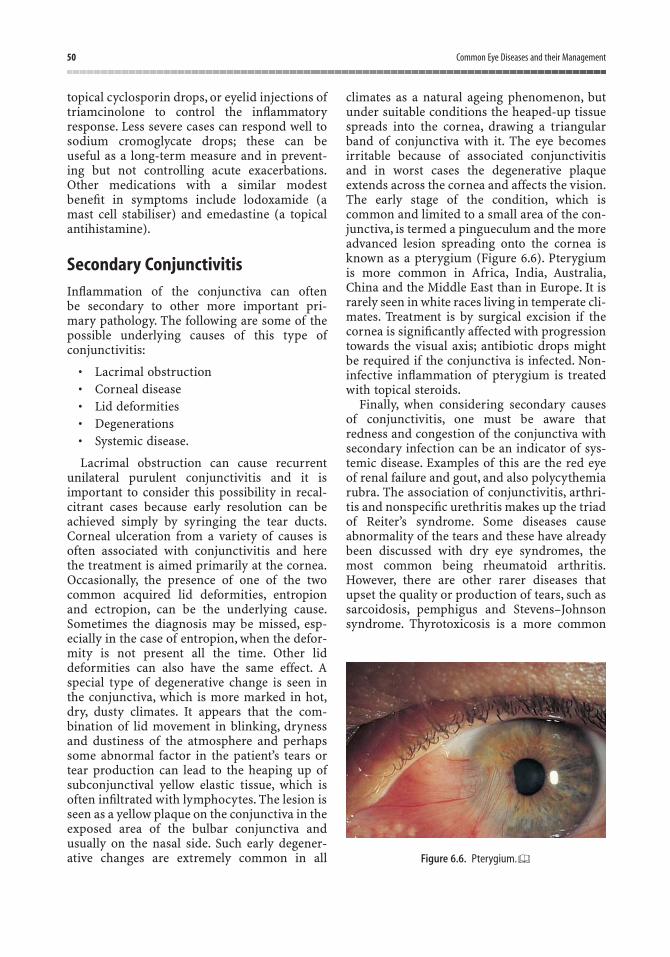
50 Common Eye Diseases and their Management
topical cyclosporin drops, or eyelid injections oftriamcinolone to control the inflammatoryresponse. Less severe cases can respond well tosodium cromoglycate drops; these can be useful as a long-term measure and in prevent-ing but not controlling acute exacerbations.Other medications with a similar modestbenefit in symptoms include lodoxamide (amast cell stabiliser) and emedastine (a topicalantihistamine).
Secondary ConjunctivitisInflammation of the conjunctiva can often be secondary to other more important pri-mary pathology. The following are some of thepossible underlying causes of this type ofconjunctivitis:
• Lacrimal obstruction• Corneal disease• Lid deformities• Degenerations• Systemic disease.
Lacrimal obstruction can cause recurrentunilateral purulent conjunctivitis and it isimportant to consider this possibility in recal-citrant cases because early resolution can beachieved simply by syringing the tear ducts.Corneal ulceration from a variety of causes isoften associated with conjunctivitis and herethe treatment is aimed primarily at the cornea.Occasionally, the presence of one of the twocommon acquired lid deformities, entropionand ectropion, can be the underlying cause.Sometimes the diagnosis may be missed, esp-ecially in the case of entropion, when the defor-mity is not present all the time. Other liddeformities can also have the same effect. Aspecial type of degenerative change is seen inthe conjunctiva, which is more marked in hot,dry, dusty climates. It appears that the com-bination of lid movement in blinking, drynessand dustiness of the atmosphere and perhapssome abnormal factor in the patient’s tears ortear production can lead to the heaping up ofsubconjunctival yellow elastic tissue, which isoften infiltrated with lymphocytes. The lesion isseen as a yellow plaque on the conjunctiva in theexposed area of the bulbar conjunctiva andusually on the nasal side. Such early degener-ative changes are extremely common in all
climates as a natural ageing phenomenon, butunder suitable conditions the heaped-up tissuespreads into the cornea, drawing a triangularband of conjunctiva with it. The eye becomesirritable because of associated conjunctivitisand in worst cases the degenerative plaqueextends across the cornea and affects the vision.The early stage of the condition, which iscommon and limited to a small area of the con-junctiva, is termed a pingueculum and the moreadvanced lesion spreading onto the cornea isknown as a pterygium (Figure 6.6). Pterygiumis more common in Africa, India, Australia,China and the Middle East than in Europe. It israrely seen in white races living in temperate cli-mates. Treatment is by surgical excision if thecornea is significantly affected with progressiontowards the visual axis; antibiotic drops mightbe required if the conjunctiva is infected. Non-infective inflammation of pterygium is treatedwith topical steroids.
Finally, when considering secondary causesof conjunctivitis, one must be aware thatredness and congestion of the conjunctiva withsecondary infection can be an indicator of sys-temic disease. Examples of this are the red eyeof renal failure and gout, and also polycythemiarubra. The association of conjunctivitis, arthri-tis and nonspecific urethritis makes up the triadof Reiter’s syndrome. Some diseases causeabnormality of the tears and these have alreadybeen discussed with dry eye syndromes, themost common being rheumatoid arthritis.However, there are other rarer diseases thatupset the quality or production of tears, such assarcoidosis, pemphigus and Stevens–Johnsonsyndrome. Thyrotoxicosis is a more common
Figure 6.6. Pterygium.

Common Diseases of the Conjunctiva and Cornea 51
systemic disease, which is associated with con-junctivitis, but the other eye signs, such as lidretraction, conjunctival oedema and proptosis,are usually more evident. A rather persistenttype of conjunctivitis is seen in patients withacne rosacea. Here, the diagnosis is usually, butnot always, made evident by the appearance ofthe skin of the nose, cheeks and forehead, butthe corneal lesions of rosacea are also quitecharacteristic (Figure 6.7). The cornea becomesinvaded from the periphery by wedge-shapedtongues of blood vessels associated with recur-rent corneal ulceration. Severe rosacea kerato-conjunctivitis is seen less commonly now,perhaps because it responds well to treatmentwith the combination of systemic doxycycline,lubricants for associated dry eye and the judi-cious use of weak topical steroids. Usually, it isalso necessary to instruct the patient to cleanthe lids and perform “lid hygiene”, as suchpatients are often also affected by blepharitis.
Corneal Foreign BodySmall particles of grit or dust commonlybecome embedded in the cornea and everycasualty officer is aware of the increasing inci-
dence of this occurrence on windy, dry days.Small foreign bodies also become embedded asthe result of using high-speed grinding toolswithout adequate protection of the eyes. Thedentist’s drill can also be a source of foreignbodies, but the most troublesome are those particles that have been heated by grinding orchiselling. It is important to have some under-standing of the anatomy of the cornea if one isattempting to remove a corneal foreign body.One must realise, for example, that the surfaceepithelium can be stripped off from the under-lying layer and can regrow and fill raw areaswith extreme rapidity. Under suitable cond-itions the whole surface epithelium can reformin about 48 h. The layer underlying, or posterior,to the surface epithelium is known as Bowman’smembrane and if this layer is damaged by theinjury or cut into unnecessarily by overzealoususe of surgical instruments, a permanent scarmight be left in the cornea.When the epitheliumalone is involved, there is usually no scar, andhealing results in perfect restoration of theoptical properties of the surface.
The stroma of the cornea is surprisinglytough, permitting some degree of boldnesswhen removing deeply embedded foreignbodies. It should be remembered that if thecornea has been perforated, the risk of intra-ocular infection or loss of aqueous dictates thatthe wound should be repaired under full sterileconditions in the operating theatre.
Signs and SymptomsPatients usually know when a foreign body hasgone into their eye and the history is clear-cut –but not always. Occasionally, the complaint issimply a red sore eye, which might have beenpresent for some time. Spotting these cornealforeign bodies is really lesson number one inocular examination. It involves employing theimportant basic principles of examining theanterior segment of the eye. Most foreign bodiescan be seen without the use of the slit-lampmicroscope if the eye is examined carefully andwith a focused beam of light. Figure 6.8 dem-onstrates the great advantage of the focusedbeam, and, in fact, this principle is used in slit-lamp microscopy. If the foreign body has beenpresent for any length of time, there will be aring of ciliary injection around the cornea
Figure 6.7. Acne rosacea.

52 Common Eye Diseases and their Management
caused by the dilatation of the deeper episcleralcapillaries, which lie near the corneal margin.Ciliary injection is a sure warning sign ofcorneal or intraocular pathology.
TreatmentThe aim of treatment is, of course, to remove theforeign body completely. Sometimes this is notas easy as it might seem, especially when a hotmetal particle lies embedded in a “rust ring”. Ininstances when it is clear that much digging isgoing to be needed, it can be prudent to leavethe rust ring for 24 h, after which it becomeseasier to remove. The procedure for removing aforeign body should be as follows: the patientlies down on a couch or dental chair and one ortwo drops of proparacaine hydrochloride 0.5%(Ophthaine) or a similar local anaesthetic areinstilled onto the affected eye. A good light on astand is needed, preferably one with a focusedbeam and the eyelids are held open with aspeculum (Figure 6.9). The doctor will alsousually require some optical aid in the form ofspecial magnifying spectacles, for example“Bishop Harman’s glasses” or the slit-lamp.Many foreign bodies can be easily removed witha cotton-wool bud (particularly those lodgedunder the upper lid), but otherwise at the slit-lamp a 25-gauge orange needle angled nearlyperpendicular to the plane of the iris can beused to lift off the foreign body. When theforeign body is more deeply embedded, abattery-powered handheld blunt-tipped drillcan be used to clean any rust deposits thatremain, again under the careful control of theslit-lamp microscope.
Once the foreign body has been removed, anantibiotic drop is placed in the eye and the lidsare then splinted together by means of a firmpad. There is no doubt that the corneal epi-thelium heals more quickly if the eyelids aresplinted in this way. It is usually advisable to seethe patient the following day if possible to makesure that all is well, and if the damaged spot onthe cornea is no longer staining with fluor-escein, the pad can be left off. Antibiotic dropsshould be continued at least three times dailyfor a few days after the cornea has healed. Thevisual acuity of the patient should always bechecked before final discharge.
There are one or two factors that shouldalways be borne in mind when treating patientswith corneal foreign bodies: in most instances,healing takes place without any problem but,rarely, the vision can be permanently impairedby scarring. Also, on rare occasions, the site of corneal damage becomes infected and if
Figure 6.8. Focal illumination of corneal foreign body.
Figure 6.9. Removing corneal foreign body.
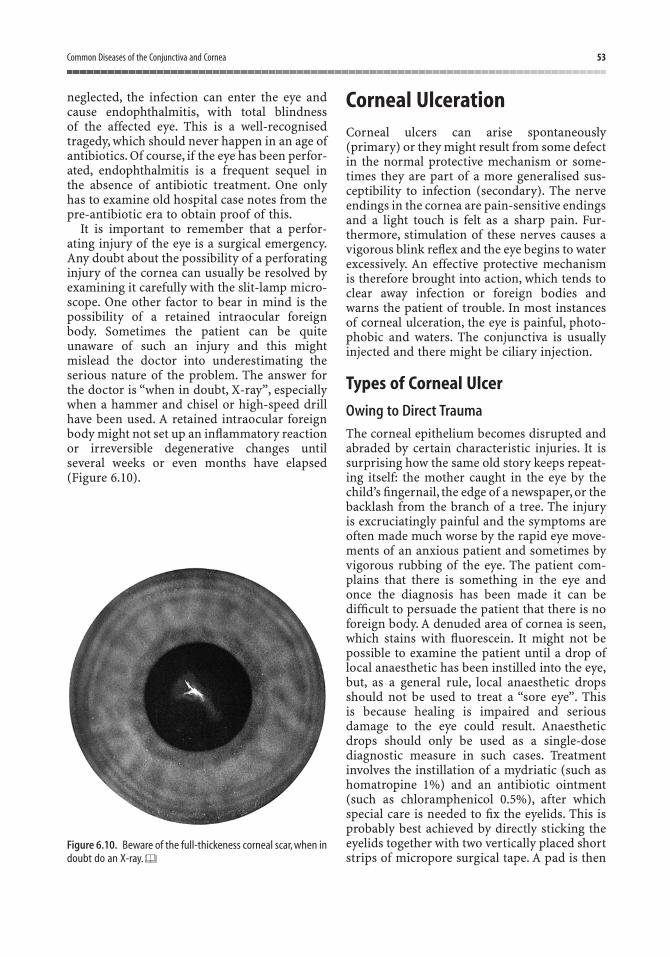
Common Diseases of the Conjunctiva and Cornea 53
neglected, the infection can enter the eye andcause endophthalmitis, with total blindness of the affected eye. This is a well-recognisedtragedy, which should never happen in an age ofantibiotics. Of course, if the eye has been perfor-ated, endophthalmitis is a frequent sequel in the absence of antibiotic treatment. One onlyhas to examine old hospital case notes from thepre-antibiotic era to obtain proof of this.
It is important to remember that a perfor-ating injury of the eye is a surgical emergency.Any doubt about the possibility of a perforatinginjury of the cornea can usually be resolved byexamining it carefully with the slit-lamp micro-scope. One other factor to bear in mind is thepossibility of a retained intraocular foreignbody. Sometimes the patient can be quiteunaware of such an injury and this mightmislead the doctor into underestimating theserious nature of the problem. The answer forthe doctor is “when in doubt, X-ray”, especiallywhen a hammer and chisel or high-speed drillhave been used. A retained intraocular foreignbody might not set up an inflammatory reactionor irreversible degenerative changes untilseveral weeks or even months have elapsed(Figure 6.10).
Corneal UlcerationCorneal ulcers can arise spontaneously(primary) or they might result from some defectin the normal protective mechanism or some-times they are part of a more generalised sus-ceptibility to infection (secondary). The nerveendings in the cornea are pain-sensitive endingsand a light touch is felt as a sharp pain. Fur-thermore, stimulation of these nerves causes avigorous blink reflex and the eye begins to waterexcessively. An effective protective mechanismis therefore brought into action, which tends toclear away infection or foreign bodies andwarns the patient of trouble. In most instancesof corneal ulceration, the eye is painful, photo-phobic and waters. The conjunctiva is usuallyinjected and there might be ciliary injection.
Types of Corneal Ulcer
Owing to Direct Trauma
The corneal epithelium becomes disrupted andabraded by certain characteristic injuries. It issurprising how the same old story keeps repeat-ing itself: the mother caught in the eye by thechild’s fingernail, the edge of a newspaper, or thebacklash from the branch of a tree. The injuryis excruciatingly painful and the symptoms areoften made much worse by the rapid eye move-ments of an anxious patient and sometimes byvigorous rubbing of the eye. The patient com-plains that there is something in the eye andonce the diagnosis has been made it can bedifficult to persuade the patient that there is noforeign body. A denuded area of cornea is seen,which stains with fluorescein. It might not bepossible to examine the patient until a drop oflocal anaesthetic has been instilled into the eye,but, as a general rule, local anaesthetic dropsshould not be used to treat a “sore eye”. This is because healing is impaired and seriousdamage to the eye could result. Anaestheticdrops should only be used as a single-dose diagnostic measure in such cases. Treatmentinvolves the instillation of a mydriatic (such ashomatropine 1%) and an antibiotic ointment(such as chloramphenicol 0.5%), after whichspecial care is needed to fix the eyelids. This isprobably best achieved by directly sticking theeyelids together with two vertically placed shortstrips of micropore surgical tape. A pad is then
Figure 6.10. Beware of the full-thickeness corneal scar, when indoubt do an X-ray.
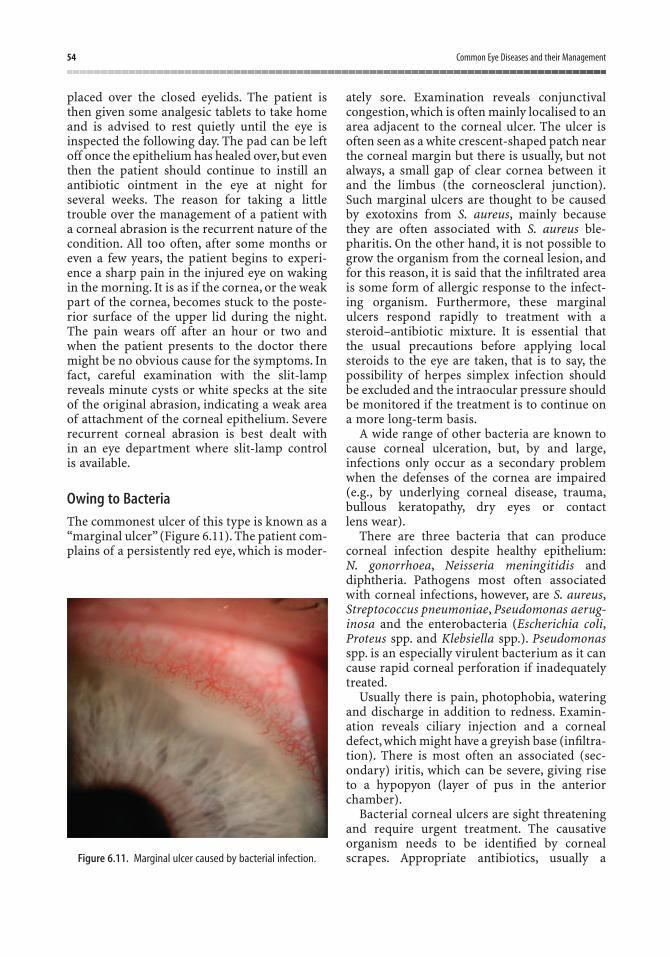
54 Common Eye Diseases and their Management
placed over the closed eyelids. The patient isthen given some analgesic tablets to take homeand is advised to rest quietly until the eye isinspected the following day. The pad can be leftoff once the epithelium has healed over, but eventhen the patient should continue to instill anantibiotic ointment in the eye at night forseveral weeks. The reason for taking a littletrouble over the management of a patient witha corneal abrasion is the recurrent nature of thecondition. All too often, after some months oreven a few years, the patient begins to experi-ence a sharp pain in the injured eye on wakingin the morning. It is as if the cornea, or the weakpart of the cornea, becomes stuck to the poste-rior surface of the upper lid during the night.The pain wears off after an hour or two andwhen the patient presents to the doctor theremight be no obvious cause for the symptoms. Infact, careful examination with the slit-lampreveals minute cysts or white specks at the siteof the original abrasion, indicating a weak areaof attachment of the corneal epithelium. Severerecurrent corneal abrasion is best dealt with in an eye department where slit-lamp control is available.
Owing to Bacteria
The commonest ulcer of this type is known as a“marginal ulcer” (Figure 6.11). The patient com-plains of a persistently red eye, which is moder-
ately sore. Examination reveals conjunctivalcongestion, which is often mainly localised to anarea adjacent to the corneal ulcer. The ulcer isoften seen as a white crescent-shaped patch nearthe corneal margin but there is usually, but notalways, a small gap of clear cornea between itand the limbus (the corneoscleral junction).Such marginal ulcers are thought to be causedby exotoxins from S. aureus, mainly becausethey are often associated with S. aureus ble-pharitis. On the other hand, it is not possible togrow the organism from the corneal lesion, andfor this reason, it is said that the infiltrated areais some form of allergic response to the infect-ing organism. Furthermore, these marginalulcers respond rapidly to treatment with asteroid–antibiotic mixture. It is essential thatthe usual precautions before applying localsteroids to the eye are taken, that is to say, thepossibility of herpes simplex infection shouldbe excluded and the intraocular pressure shouldbe monitored if the treatment is to continue ona more long-term basis.
A wide range of other bacteria are known tocause corneal ulceration, but, by and large,infections only occur as a secondary problemwhen the defenses of the cornea are impaired(e.g., by underlying corneal disease, trauma,bullous keratopathy, dry eyes or contact lens wear).
There are three bacteria that can producecorneal infection despite healthy epithelium:N. gonorrhoea, Neisseria meningitidis and diphtheria. Pathogens most often associatedwith corneal infections, however, are S. aureus,Streptococcus pneumoniae, Pseudomonas aerug-inosa and the enterobacteria (Escherichia coli,Proteus spp. and Klebsiella spp.). Pseudomonasspp. is an especially virulent bacterium as it cancause rapid corneal perforation if inadequatelytreated.
Usually there is pain, photophobia, wateringand discharge in addition to redness. Examin-ation reveals ciliary injection and a cornealdefect, which might have a greyish base (infiltra-tion). There is most often an associated (sec-ondary) iritis, which can be severe, giving riseto a hypopyon (layer of pus in the anteriorchamber).
Bacterial corneal ulcers are sight threateningand require urgent treatment. The causativeorganism needs to be identified by cornealscrapes. Appropriate antibiotics, usually a Figure 6.11. Marginal ulcer caused by bacterial infection.

Common Diseases of the Conjunctiva and Cornea 55
combination of gentamicin and cefuroxime,which are applied frequently in hospital,provide a broad spectrum until the organismsare identified.
Owing to Acanthamoeba spp.
Acanthamoeba spp. are a free-living genus ofamoeba that has been increasingly associatedwith keratitis. The keratitis is usually chronicand can follow minor trauma. Contact lenswearers are particularly at risk of this infection.
Owing to Viruses
Apart from other rare types of virus infection,there is one outstanding example of this –herpes simplex keratitis. The condition seems tobe more common than it used to be, perhapsbecause the incidence of other types of cornealulcer has become less with the more liberal use of local antibiotics on the eye. Every eyecasualty department has a few patients with thisdebilitating condition, which can put a patientoff work for many months. Fortunately, it is onlya few cases that cause such a problem, and mostinstances of this common condition give rise toa week or ten days of incapacity. Herpes simplexis thought to produce a primary infection ininfants and younger children, which is trans-ferred from the lips of the mother and might besubclinical. Sometimes a vesicular rash developsaround the eyelids, accompanied by fever andenlargement of the preauricular lymph nodes.Whatever the initial manifestation of primaryinfection, it is thought that many members ofthe population harbour the virus in a latentform so that overt infection in an adult tends toappear in association with other illnesses. Mostpeople are familiar with the cold sores thatappear on the lips because of herpes simplex.Sometimes, after a cold, one eye becomes soreand irritable and inspection of the cornea showsthe characteristic corneal changes of herpessimplex infection. A slightly raised granular,star-shaped or dendriform lesion is seen, whichtakes up fluorescein (Figure 6.12a). The viruscan be cultivated from this lesion and the size of the dendriform figure is some guide to prognosis. A large lesion extending across thecornea, especially across the optical axis (i.e., thecentre of the cornea), is likely to be the one thatis going to give trouble and it is better that thepatient should be warned about it at this stage.
After a few days, or sometimes weeks, theepithelial lesion heals and at this point, completeresolution can occur or an inflammatory reac-tion can appear in the stroma deep to theinfected epithelium. The eye remains red andirritable to an incapacitating degree and furtherdendritic ulcers might subsequently appear. Inworse cases, the cornea can become anaestheticso that, although the eye might be more com-fortable, the problems of a numb cornea areadded to the original condition. Healing tendsto occur with a vascular scar.
Treatment of Herpes Simplex Keratitis
Antiviral agents are usually the first line oftreatment. Examples of currently used antiviralagents are idoxuridine, trifluorothymidine,cytarabine and acyclovir. The most effective isacyclovir. Unfortunately, none of these agents iscurative, but they are thought to have someeffect on acute rather than chronic cases. Earlydiagnosis and treatment seem to give the bestchance of avoiding recurrences. The removal ofvirus-containing epithelial cells (debridement)is now indicated only in cases that are resistantto antiviral agents, where there is toxicity to thedrugs, or there is difficulty in acquiring orapplying the antiviral agents. An antibiotic dropand cycloplegic are instilled and a firm pad andbandage applied. Touching the debrided areawith iodine is now obsolete. Following this pro-cedure, the eye can become very sore and thepatient is given an analgesic. Often the cornealepithelium will heal after 48 h and the conditionwill be cured. Larger ulcers might not respondsatisfactorily to this treatment. Steroids shouldnot be used in the treatment of dendritic ulcersof the cornea (Figure 6.12b). It is well recognisedthat steroid drops enhance the replication of theherpes simplex virus (Figure 6.12c). Theyreduce the local inflammatory reaction andcould give the false impression that the eye isimproving. However, persistent use of localsteroids in such cases could result in cornealthinning and even corneal perforation. Once thedendritic ulcer has healed, residual stromalinfiltration is then sometimes treated by care-fully gauged doses of steroids, but this should be under strict ophthalmological supervision.In more severe cases, secondary iritis or sec-ondary glaucoma can complicate the pictureand require special treatment. The decision
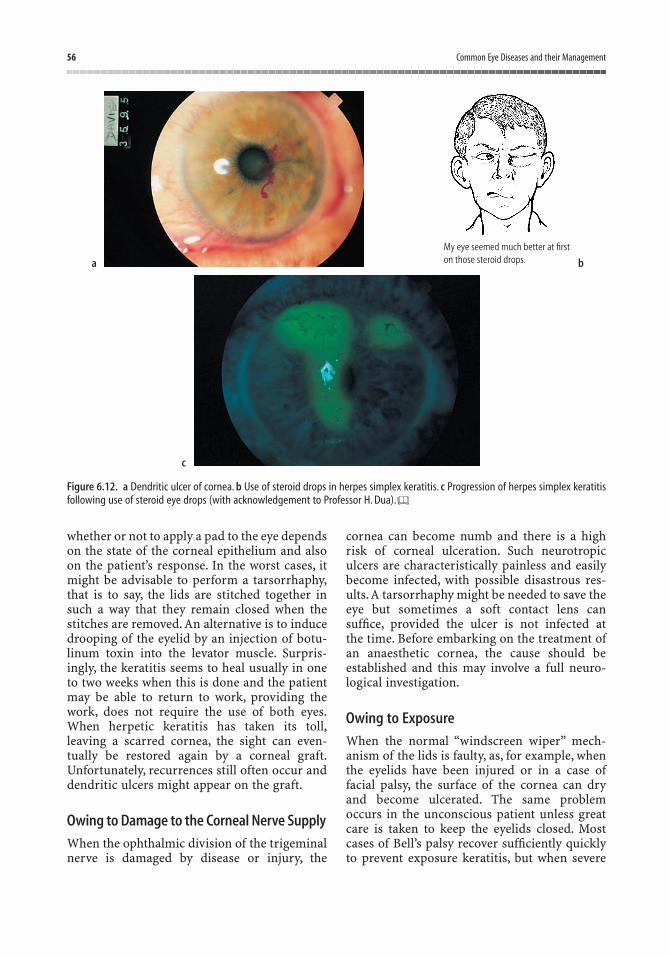
56 Common Eye Diseases and their Management
whether or not to apply a pad to the eye dependson the state of the corneal epithelium and alsoon the patient’s response. In the worst cases, itmight be advisable to perform a tarsorrhaphy,that is to say, the lids are stitched together insuch a way that they remain closed when thestitches are removed. An alternative is to inducedrooping of the eyelid by an injection of botu-linum toxin into the levator muscle. Surpris-ingly, the keratitis seems to heal usually in oneto two weeks when this is done and the patientmay be able to return to work, providing thework, does not require the use of both eyes.When herpetic keratitis has taken its toll,leaving a scarred cornea, the sight can even-tually be restored again by a corneal graft.Unfortunately, recurrences still often occur anddendritic ulcers might appear on the graft.
Owing to Damage to the Corneal Nerve Supply
When the ophthalmic division of the trigeminalnerve is damaged by disease or injury, the
cornea can become numb and there is a highrisk of corneal ulceration. Such neurotropiculcers are characteristically painless and easilybecome infected, with possible disastrous res-ults.A tarsorrhaphy might be needed to save theeye but sometimes a soft contact lens cansuffice, provided the ulcer is not infected at the time. Before embarking on the treatment ofan anaesthetic cornea, the cause should beestablished and this may involve a full neuro-logical investigation.
Owing to Exposure
When the normal “windscreen wiper” mech-anism of the lids is faulty, as, for example, whenthe eyelids have been injured or in a case offacial palsy, the surface of the cornea can dryand become ulcerated. The same problemoccurs in the unconscious patient unless greatcare is taken to keep the eyelids closed. Mostcases of Bell’s palsy recover sufficiently quicklyto prevent exposure keratitis, but when severe
My eye seemed much better at firston those steroid drops.
Figure 6.12. a Dendritic ulcer of cornea. b Use of steroid drops in herpes simplex keratitis. c Progression of herpes simplex keratitisfollowing use of steroid eye drops (with acknowledgement to Professor H. Dua).
a b
c

Common Diseases of the Conjunctiva and Cornea 57
and when recovery is poor, a tarsorrhaphy, or atleast treatment with an eye pad and local anti-biotic ointment at night, might be needed. Bot-ulinum toxin injection into the lid may obviatethe need for surgery; this has the effect of drop-ping the upper lid for approximately threemonths, and is a useful temporising measure insome cases. It is important to bear in mind thatthe same risk of corneal exposure is evident inpatients with severe thyrotoxic exophthalmos.
Corneal DystrophiesThere are a number of specific corneal dystro-phies, most of which are inherited and most ofwhich cannot be diagnosed without the aid ofthe slit-lamp microscope. For this reason, theywill not be dealt with in any detail here. A listfor reference is shown in Table 6.1.
Keratoconus (or conical cornea) is perhapsthe commonest. It is still rare in the general pop-ulation but is familiar to general practitionerslooking after student populations because ittends to appear in this age group. The conditionis bilateral and can be inherited as an autosomalrecessive trait, although most patients do nothave a positive family history. It should be sus-pected in patients who show a rapid change ofrefractive error, particularly if a large amount ofmyopic astigmatism suddenly appears. Often,but not always, there is an associated history ofasthma and hay fever. The cornea shows centralthinning and protrudes anteriorly. This can beobserved with the naked eye by asking thepatient to sit down and then standing behind
him so that one can look down on his down-turned eye. By holding up the upper lids, onecan make an estimate of the abnormal shape ofthe cornea by noting how the cornea shapes thelower lid. Alternatively, the patient’s cornea canbe observed using Placido’s disc. This ingeniousinstrument is simply a disc with a hole in thecentre, through which one observes the patient’scornea. On the patient’s side of the disc is aseries of concentric circles, which can be seen bythe observer reflected on the patient’s cornea(Figure 6.13). Distortion of these circles ind-icates the abnormal shape of the cornea. Ofcourse, more accurate assessment of the corneacan be made by observing it with the slit-lampmicroscope and still more information can beobtained by keratometry or corneal topography,that is, using an instrument to measure the curvature of the cornea in different meridians.Keratoconus tends to progress slowly andcontact lenses can be helpful. Sometimes acorneal graft is required. Less common cornealdystrophies include Fuch’s endothelial, stromaland anterior dystrophies.
Corneal DegenerationsApart from the inherited corneal dystrophies,certain changes are often seen in the corneawith ageing, such as arcus senilis and endothe-lial pigmentation. Band degeneration refers to adeposition of calcium salts in the anterior layersof the cornea. The calcification is first seen at themargin of the cornea in the nine o’clock andthree o’clock area, but it can gradually extend
Table 6.1. Corneal dystrophies.
Anterior dystrophies (corneal epithelium and Bowman’s membrane):
MicrocysticReis Buckler’s
Stromal dystrophies:LatticeMacularGranular
Posterior dystrophies (corneal endothelium and Descemet’s membrane):
Fuch’sPosterior polymorphous
Ectatic dystrophies:KeratoconusKeratoglobus
Figure 6.13. Keratoconus; Placido’s disc image.

58 Common Eye Diseases and their Management
across the normally exposed part of the cornea.It is seen in cases of chronic iridocyclitis, in par-ticular in patients with juvenile rheumatoidarthritis and also in those with sarcoidosis. Infact, band degeneration is seen in any eye thathas become degenerate or in cases of long-standing corneal disease (Figure 6.14).Althoughband degeneration can, if sufficiently advanced,be diagnosed quite easily with the naked eye,most degenerative conditions of the cornea canonly be diagnosed and classified under themicroscope. Other corneal degenerations include Salzmann’s nodular dystrophy and lipid keratopathies.
Corneal OedemaTo the naked eye, corneal oedema might not beobvious but careful inspection will reveal a lack of luster when the affected cornea is com-pared with that on the other side. The normalsparkle of the eye is no longer evident and theiris becomes less well defined. Microscopically,a bedewed appearance is seen, minute dropletsbeing evident in the epithelium. When thestroma is also involved, this can seem misty andmight also be infiltrated with inflammatorycells, which are seen as powdery white dots.When the oedema is long-standing, the dropletsin the epithelium coalesce to produce blisters or bullae.
The more important causes of cornealoedema are as follows:
• Acute narrow-angle glaucoma• Virus keratitis
• Trauma• Contact lenses• Postoperative• Fuch’s endothelial dystrophy.
When the intraocular pressure is suddenlyraised from any cause, the cornea becomes oedematous. The normal cornea needs to be relatively dehydrated in order to maintain itstransparency, and the necessary level of dehyd-ration seems to depend on active removal ofwater by the corneal endothelium, as well as anadequate oxygen supply from the tears. Themechanism is impaired not only by raising theintraocular pressure, but also by infection ortrauma. Senile degenerative changes might alsobe the sole underlying cause because of failureof the endothelial pumping mechanisms.Contact lenses, if ill fitting and worn for too longa period, can prevent adequate oxygen reachingthe cornea, with resulting oedema.
The management of corneal oedema dependson the management of the underlying cause.Oedema due to endothelial damage can respond,in its early stages, to local steroids and some-times a clear cornea can be maintained by the use of osmotic agents, such as hypertonic salineor glycerol. Chronic corneal oedema tends to bepainful and often acute episodes of pain occurwhen bullae rupture leaving exposed cornealnerves. In such cases, it can be necessary to con-sider a tarsorrhaphy, or in some instances, acorneal graft can prove beneficial. The pain ofcorneal oedema is a late symptom and in its early stages, oedema simply causes blurring ofthe vision and the appearance of coloured haloes around light bulbs. This is simply a “bathroom window” effect. Patients withcataracts also see haloes, so that defects in otherparts of the optical media of the eye might givea similar effect.
Absent Corneal SensationCorneal sensation is supplied by the fifth nerve.About 70 nerve fibres are present in the super-ficial layers of the cornea and they can often beseen when the cornea is examined with the slit-lamp microscope. They appear as white threadsrunning mainly radially. Asking the patient togaze straight ahead and then lightly touching the cornea with a fine wisp of cotton-wool can
Figure 6.14. Band keratopathy.

Common Diseases of the Conjunctiva and Cornea 59
assess corneal anaesthesia. Care must be takennot to touch the lid margins when doing this.The blink reflex is then noted and it is alsoimportant to ask the patient what has been felt.In the case of elderly people, the blink reflexmight be reduced, but a slight prick should beevident when the cornea is touched. Attempts to quantify corneal anaesthesia have led to thedevelopment of graded strengths of bristle,which can be applied to the cornea instead of cotton-wool.
Corneal anaesthesia can result from a lesionat any point in the fifth cranial nerve from thecornea to the brainstem. In the cornea itself,herpes simplex infection can ultimately result inanaesthesia. Herpes zoster is especially liable to lead to this problem and, because this con-dition can often be treated at home rather than in the ward, it will be considered in moredetail here.
Herpes Zoster OphthalmicusThis is caused by the varicella-zoster virus, thesame virus that causes chickenpox. It is thoughtthat the initial infection with the virus occurswith an attack of childhood chickenpox and thatthe virus remains in the body in a latent form,subsequently to manifest itself as herpes zosterin some individuals. The virus appears to lodgein the Gasserian ganglion. The onset of the con-dition is heralded by headache and the appear-ance of one or two vesicles on the forehead. Overthe next three or four days the vesicles multiplyand appear on the distribution of one or all ofthe branches of the fifth cranial nerve. Thepatient can develop a raised temperature andusually experiences malaise and considerablepain. Sometimes a chickenpox-like rash appearsover the rest of the body. The eye itself is mostat risk when the upper division of the fifth nerveis involved. There might be vesicles on the lidsand conjunctiva and, when the cornea isaffected, punctate-staining areas are seen, whichbecome minute subepithelial opacities. Afterfour days to a week, the infection reaches itspeak; the eyelids on the affected side might beclosed by swelling, and oedema of the lids mightspread across to the other eye (Figure 6.15). Thevesicles become pustular and form crusts,which are then shed over a period of two orthree weeks. In most cases, complete resolution
occurs with remarkably little scarring of theskin considering the appearance in the acutestage. However, the cornea can be rendered per-manently anaesthetic and the affected area ofskin produces annoying paresthesiae, amount-ing quite often to persistent rather severe neu-ralgia, which can dog the patient for many years.Other complications include extraocular musclepalsies or rarely, encephalitis. Iridocyclitis isfairly common and glaucoma can develop andlead to blindness if untreated. At present, thereis no known effective treatment other than theuse of local steroids and acyclovir for theuveitis, and acetazolamide or topical beta-blockers for the glaucoma. Administration ofsystemic acyclovir or famciclovir early in thedisease is known to reduce the severity of theneuralgia, but these medications need to beadministered as soon as possible after the onsetof symptoms for best effect. The disease has torun its course and the patient, who is usuallyelderly, could require much support and advice,especially when post-herpetic neuralgia issevere. It is accepted practice to treat the eye atrisk with antibiotic drops and a weak mydriatic.Analgesics are, of course, also usually needed,often on a long-term basis.
Other causes of corneal anaesthesia includesurgical division of the fifth cranial nerve fortrigeminal neuralgia or any space-occupyinglesion along the nerve pathway.The possibility ofexposure and drying of the cornea must alwaysbe borne in mind in the unconscious or theanaesthetized patient because corneal ulcerationand infection will soon result if this is neglected.
Figure 6.15. Herpes zoster ophthalmicus.

60 Common Eye Diseases and their Management
Corneal anaesthesia caused by nerve damageis nearly always permanent and, if it is complete,it can often be necessary to protect the eye bymeans of a tarsorrhaphy or botulinum toxin.
Lesser degrees of corneal anaesthesia can betreated by instilling an antibiotic ointment atnight and, if a more severe punctate keratitisdevelops, by padding the eye.
Redness of the eye is one of the commonestsigns in ophthalmology, being a feature of awide range of ophthalmological conditions,some of which are severe and sight threatening,whereas others are mild and of little cons-equence. Occasionally, the red eye can be thefirst sign of important systemic disease. It isimportant that every practicing doctor has anunderstanding of the differential diagnosis ofthis common sign, and a categorisation of thesigns, symptoms and management of the redeye will now be made from the standpoint of thenonspecialist general practitioner.
The simplest way of categorising thesepatients is in terms of their visual acuity. As ageneral rule, if the sight, as measured on theSnellen test chart, is impaired, then the causemight be more serious. The presence or absenceof pain is also of significance, but as thisdepends in part on the pain threshold of thepatient, it can be a misleading symptom.Disease of the conjunctiva alone is not usuallypainful, whereas disease of the cornea or iris isgenerally painful.
The red eye will, therefore, be consideredunder three headings: the red eye that sees welland is not painful, the red painful eye that cansee normally, and the red eye that does not seewell and is acutely painful.
Red Eye That Is Not Painfuland Sees NormallySubconjunctival HaemorrhageCareful examination of the eye will easilyconfirm that its redness is due to blood ratherthan dilated blood vessels, and the rednessmight be noticed by someone other than thepatient. The condition is common and resolvesin about 10–14 days. It is extremely unusual fora blood dyscrasia to present with subconjunc-tival haemorrhages. Although vomiting or ableeding tendency can also be rare causes,the normal practice is to reassure the patientrather than embark on extensive investigations,because the majority of cases are caused byspontaneous bleeding from a conjunctival cap-illary. This might be spontaneous and can resultfrom a sudden increase in venous pressure, forexample after coughing.
ConjunctivitisExamination of the eye reveals inflammation,that is, dilatation of the conjunctival capillariesand larger blood vessels, associated with moreor less discharge from the eye. The exact site of
7The Red Eye
61

62 Common Eye Diseases and their Management
the inflammation should be noted and it is esp-ecially useful to note whether the deeper capil-laries around the margin of the cornea areinvolved. The resulting pink flush encircling thecornea is called “ciliary injection” and is awarning of corneal or intraocular inflam-mation. For clinical purposes, it is useful todivide conjunctivitis into acute and chronictypes.
Acute Conjunctivitis
This is usually infective and caused by a bac-terium; it is more common in young people. Itcan spread rapidly through families or schoolswithout serious consequence other than a fewdays incapacity.When adults develop acute con-junctivitis, it is worth searching for a possibleunderlying cause, especially a blocked tear ductif the condition is unilateral. Sometimes aningrowing lash might be the cause or occasion-ally a free-floating eyelash lodges in the lacrimalpunctum. The important symptoms of acuteconjunctivitis are redness, irritation and stick-ing together of the eyelids in the mornings.Management entails finding the cause and usingantibiotic drops if the symptoms are severeenough to warrant this. However, it must beremembered that the inadequate and intermit-tent use of antibiotic eye drops could simplyencourage growth of resistant organisms.
Chronic Conjunctivitis
This is a common cause of the red eye and almosta daily problem in nonspecialised ophthalmicpractice. If we consider that the conjunctiva is amucous membrane that is exposed daily to theelements, it is perhaps not surprising that aftermany years it tends to become chronicallyinflamed and irritable. The frequency and nuisance value of the symptoms are reflected in the large across-the-counter sales of various eyewashes and solutions aimed at relieving “eye-strain” or “tired eyes”. The symptoms of chronicconjunctivitis are, therefore, redness and irrita-tion of the eyes, with a minimal degree of dis-charge and sticking of the lids. If there is anallergic background, itching might also be amain feature. The chronically inflamed conjunc-tiva accumulates minute particles of calciumsalts within the mucous glands. These conjunc-tival concretions are shed from time to time,pro-ducing a feeling of grittiness. When confrontedwith such a patient, there are a number of key
symptoms to be elicited and these can be relatedto a checklist of causes mentioned below.
The key symptoms of chronic conjunctivitisare as follows:
• Environmental factors, especially eyedrops, make-up or foreign bodies.
• Lids stick in mornings?• Do the eyes itch?• Emotional stress or psychiatric illness?
The following is a checklist of causes ofchronic conjunctivitis:
• Eyelids: deformities, such as entropion orectropion.
• Displaced eyelashes.• Chronic blepharitis.• Refractive error: a proportion of patients
who have never worn glasses and needthem or who are wearing incorrectly pre-scribed or out-of-date glasses present withthe features of chronic conjunctivitis, thesymptoms being relieved by the proper useof spectacles. The cause is not clear butpossibly related to rubbing the eyes.
• Dry eye syndrome: the possibility of adefect in the secretion of tears or mucus canonly be confirmed by more elaborate tests,but this should be suspected in patientswith rheumatoid arthritis or sarcoidosis.
• Foreign body: contact lenses and mascaraparticles are the commonest foreignbodies to cause chronic conjunctivitis.
• Stress: often a period of stress seems to be closely related to the symptoms andperhaps eye rubbing is also the cause inthese patients.
• Allergy: it is unusual to be able to incrim-inate a specific allergen for chronic con-junctivitis, unlike allergic blepharitis. Onthe other hand, hay fever and asthma couldbe the background cause.
• Infection: chronic conjunctivitis can beginas an acute infection, usually viral andusually following an upper respiratorytract infection.
• Drugs: the long-term use of adrenalinedrops can cause dilatation of the conjunc-tival vessels and irritation in the eye. In1974, it was shown that the beta-blockingdrug practolol (since withdrawn from themarket) could cause a severe dry eye

The Red Eye 63
syndrome in rare instances. Since thenthere have been several reports of mildreactions to other available beta-blockers,although such reactions are difficult to distinguish from chronic conjunctivitisfrom other causes.
• Systemic causes: congestive cardiac failure,renal failure,Reiter’s disease,polycythaemia,gout, rosacea, as well as other causes oforbital venous congestion, such as orbitaltumours, can all cause vascular congestionand irritation of the conjunctiva. Migrainecan also be associated with redness of the eye on one side and chronic alcoholism is acause of bilateral conjunctival congestion.
EpiscleritisSometimes the eye becomes red because ofinflammation of the connective tissue underly-ing the conjunctiva, that is, the episclera. Thecondition can be localised or diffuse. There is nodischarge and the eye is uncomfortable,althoughnot usually painful. The condition responds tosodium salicylate given systemically and to theadministration of local steroids or nonsteroidalanti-inflammatory agents. The underlying causeis often never discovered, although there is awell-recognised link with the collagen and dermatological diseases,especially acne rosacea.Episcleritis tends to recur and might persist forseveral weeks, producing a worrying cosmeticblemish in a young person (Figure 7.1).
Red Painful Eye That Can See NormallyScleritisInflammation of the sclera is a less commoncause of red eye. There is no discharge but theeye is painful. Vision is usually normal, unlessthe inflammation involves the posterior sclera.It is most often seen in association with rheumatoid arthritis and other collagen dis-eases and sometimes can become severe andprogressive to the extent of causing perforationof the globe (Figure 7.2).For this reason,steroidsmust be administered with extreme care. Treat-ment normally is with systemically adminis-tered nonsteroidal anti-inflammatory agents,for example flurbiprofen (Froben) tablets.
Red Painful Eye That Cannot SeeIt is worth emphasising again that the redpainful eye with poor vision is likely to be aserious problem, often requiring urgent admis-sion to hospital or at least intensive outpatienttreatment as a sight-saving measure. The fol-lowing are the principal causes.
Acute GlaucomaThe important feature here is that acute glau-coma occurs in long-sighted people and there is
Figure 7.2. Scleritis.
Figure 7.1. Episcleritis (with acknowledgement to Professor H. Dua).

64 Common Eye Diseases and their Management
usually a previous history of headaches andseeing haloes around lights in the evenings. Theraised intraocular pressure damages the irissphincter and for this reason, the pupil is semi-dilated. Oedema of the cornea causes the eye tolose its luster and gives the iris a hazy appear-ance (Figure 7.3). The eye is extremely tenderand painful and the patient could be nauseatedand vomiting. Immediate admission to hospitalis essential, where the intraocular pressure isfirst controlled medically and then bilaterallaser iridotomies or surgical peripheral iridec-tomies are performed to relieve pupil block.Mydriatics should not be given to patients withsuspected narrow-angle glaucoma without con-sultation with an ophthalmologist.
Acute IritisThe eye is painful, especially when attemptingto view near objects, but the pain is never sosevere as to cause vomiting. The cornea remainsbright and the pupil tends to go into spasm andis smaller than on the normal side (Figure 7.4).Acute iritis is seen from time to time mainly inthe 20–40-year age group, whereas acute glau-coma is extremely rare at these ages. Unlesssevere and bilateral, acute iritis is treated on anoutpatient basis with local steroids and mydria-tic drops. Some expertise is needed in the use of the correct mydriatic, and systemic steroidsshould be avoided unless the sight is in jeop-ardy. Because the iris forms part of the uvea,acute iritis is the same as acute anterior uveitis.In many cases, no systemic cause can be foundbut it is important to exclude the possibility of
sarcoidosis or ankylosing spondylitis. The condition lasts for about two weeks but tends to recur over a period of years. After two orthree recurrences there is a high risk of thedevelopment of cataract, although this mightform slowly.
Acute KeratitisThe characteristic features are sharp pain, oftendescribed as a foreign body in the eye, markedwatering of the eye, photophobia and difficultyin opening the affected eye. The clinical pictureis different from those of the above two cond-itions and the commonest causes are the herpessimplex virus or trauma. The possibility of aperforating injury must always be borne inmind. Sometimes children are reticent aboutany history of injury for fear of incriminating afriend, and sometimes a small perforatinginjury is surprisingly painless. The treatment ofacute keratitis has already been discussed inChapter 6 and the management of cornealinjuries will be considered in Chapter 16.
Neovascular GlaucomaThe elderly patient who presents with a blindand painful eye and who might also be diabeticshould be suspected of having neovascular glau-coma. Often, a fairly well-defined sequence ofevents enables the diagnosis to be inferred fromthe history, as in many cases secondary neo-vascular glaucoma arises following a centralretinal vein occlusion. Following retinal veinocclusion, patients typically notice that thevision of one eye becomes blurred over severalFigure 7.3. Acute angle-closure glaucoma.
Figure 7.4. Acute iritis. The pupil has been dilated with drops.

The Red Eye 65
hours or days. Some elderly patients do not seekattention at this stage and some degree of spon-taneous recovery can seem to occur before theonset of secondary glaucoma. Fortunately,only a modest proportion of cases develops thissevere complication, which usually occurs, sur-prisingly enough, after 100 days, hence the term “hundred-day glaucoma”. Once
the intraocular pressure rises, the eye tends tobecome painful and eventually degenerates in the absence of treatment, and sometimeseven in spite of treatment. This form ofsecondary glaucoma remains as one of the fewindications for surgical removal of the eye, ifmeasures to control intraocular pressure are unsuccessful.

Failing vision means that the sight, as measuredby the standard test type, is worsening. Thepatient might say “I can’t see so well doctor” orthey might feel that their spectacles need chang-ing. Some patients might not notice visual loss,especially if it is in one eye. Sometimes, morespecific symptoms are given; the vision might beblurred, for example in a patient with cataract, orobjects might appear distorted or straight linesbent if there is disease of the macular region ofthe retina. Disease of the macular can also makeobjects look larger or smaller.Double vision is animportant symptom because it can be the resultof a cranial nerve palsy,but if monocular, it couldbe caused by cataract. Patients quite often com-plain of floating black spots. If these move slowlywith eye movement, they might be caused bysome disturbance of the vitreous gel in the centreof the eye. If they are accompanied by seeingflashing lights, the possibility of damage to theretina needs to be kept in mind. “Vitreousfloaters” are common and in most instances areof little pathological significance. Patients quiteoften notice haloes around lights and, althoughthis is typical of an attack of acute glaucoma,haloes are also seen by patients with cataracts.Like many such symptoms, they are best notasked for specifically. The question “do you eversee haloes?” is likely to be followed by the answer“yes”. Night blindness is another such symptom.No one can see too well in the dark,but if a patienthas noticed a definite worsening of his or herability to see in dim light, an inherited retinaldegeneration, such as retinitis pigmentosa,might be the cause.
Failing Vision in an Eye ThatLooks Normal
When the Fundus Is Normal
Often a patient will present with a reduction ofvision in one or both eyes and yet the eyes them-selves look quite normal. In the case of a child,the parents may have noticed an apparentdifficulty in reading or the vision may have beennoticed to be poor at a routine school eye test.The next step is to decide whether the fundus isalso normal, but before dilating the pupil toallow fundus examination, it is important tocheck the pupil reactions and to eliminate thepossibility of refractive error. Once the glasseshave been checked and the fundus examined,the presence of a normal fundus narrows thefield down considerably. The likely diagnosisdepends on the age of the patient. Infants withvisual deterioration might require an examina-tion under anaesthesia to exclude the possibil-ity of a rare inherited retinal degeneration orother retinal disease. Other children, particu-larly those in the 9–12-year age group, must firstbe suspected of some emotional upset, perhapsdue to domestic upheaval or stress at school.This can make them reluctant to read the testtype. Sometimes such children discover thatexercising their own power of accommodationproduces blurring of vision and they mightpresent with accommodation spasm. The commonest cause of unilateral visual loss in
8Failing Vision
67

children is amblyopia of disuse. This importantcause of visual loss with a normal fundus is con-sidered in more detail in Chapter 14 on squint.When, for any reason, one retina fails to receivea clear and correctly orientated image for aperiod of months or years during the time ofvisual development, the sight of the eye remainsimpaired. The condition is treatable if caughtbefore the visual reflexes are fully developed,that is, before the age of eight years. Youngadults who present with unilateral visual lossand normal fundi could, of course, have amblyopia of disuse and the condition can beconfirmed by looking for a squint or a refractiveerror more marked on the affected side. Wemust also remember that retrobulbar neuritispresents in young people as sudden loss ofvision on one side with aching behind the eye and a reduced pupil reaction on the affected side. This contrasts with amblyopia of disuse, in which the pupil is normal.Migraine is another possibility to be consideredin such patients.
Elderly patients who present with visual lossand normal fundi might give the history of astroke and are found to have a homonymoushaemianopic defect of the visual fields causedby an embolus or thrombosis in the area of dis-tribution of the posterior cerebral artery.Hysteria and malingering are also causes ofunexplained visual loss, but these are extremelyrare and it is important that the patient is investigated carefully before such a diagnosis is made.
When the Fundus Is AbnormalQuite a proportion of patients who complain ofloss of vision with eyes that look normal onsuperficial inspection show changes on ophthal-moscopy. The three important potentially blind-ing but eminently treatable ophthalmologicalconditions must be borne in mind: cataract,chronic glaucoma and retinal detachment. It isan unfortunate fact that the commonest cause ofvisual loss in the elderly is usually untreatableat the present time. It is known as age-relatedmacular degeneration and forms part of thesensory deprivation, which is an increasingscourge in elderly people. These diseases are
limited to the eye itself, but disease elsewhere inthe body can often first present as a visualproblem. In this context, we must rememberwhat has been the commonest cause of blind-ness in young people – diabetic retinopathy, aswell as the occasional case of severe hyper-tension. Intracranial causes of visual loss areperhaps less common in general practice and,for this reason, are easily missed. Intracranialtumours can present in an insidious manner, inparticular the pituitary adenoma, and the diag-nosis might be first suspected by careful plot-ting of the visual fields. In the case of the elderlypatient who complains of visual deterioration inone eye, the ophthalmoscope all too commonlyreveals age-related macular degeneration, but it is also common to find that the patient has suffered a thrombosis of the central retinal vein or one of its branches. Unlike the situa-tion with a central retinal artery occlusion,which is less common, some vision is pre-served with a central retinal vein thrombosis inspite of the dramatic haemorrhagic fundusappearance. Temporal arteritis is anotherimportant vascular cause of visual failure in the elderly.
Finally, there are a large number of lesscommon conditions, only one or two of whichwill be mentioned at this point. At any age, theingestion of drugs can affect the eyesight, butthere are very few proven oculotoxic drugs still on the market. One important example ischloroquine. When a dose of 100 g in one year isexceeded, there is a risk of retinotoxicity, whichmight not be reversible. Although age-relatedmacular degeneration is normally seen in theover-60s, the same problem may occur inyounger people often with a recognised inherit-ance pattern. A completely different conditioncan also affect the macular region of youngadults, known as central serous retinopathy.This tends to resolve spontaneously after a few weeks, although treatment by laser coag-ulation is occasionally needed. Unilateral pro-gressive visual loss in young people can also be caused by posterior uveitis, which is the same as choroiditis. The known causes and manage-ment of this condition will be discussed inChapter 18.
The more common causes of failing vision in a normal-looking eye are summarised in Table 8.1.
68 Common Eye Diseases and their Management
Treatable Causes of Failing VisionNobody can deny that the practice of ophthal-mology is highly effective. Many eye diseasescan be cured or arrested, and it is possible torestore the sight fully from total blindness.Many of the commoner causes of blindness,especially in the third world, are treatable. Themost important treatable cause of visual failurein the UK is cataract, and, of course, no patientshould be allowed to go blind from this cause,although this does occasionally happen (Figure8.1). Retinal detachment is less common thancataract but it provides a situation where thesight could be lost completely and then be fullyrestored. For the best results, surgery must becarried out as soon as possible, before the retinabecomes degenerate, whereas delay beforecataract surgery does not usually affect theoutcome of the operation. Acute glaucoma isanother instance where the sight could be lostbut restored by prompt treatment. The treat-ment of chronic glaucoma has less impressionon the patient because it is aimed at preventingvisual deterioration, although in sight-savingterms it can be equally effective.
It is easy to overlook the value of antibioticsin saving sight. Before their introduction,many more eyes had to be removed followinginjury and infection. Systemic and locally
applied steroids also play a sight-saving role inthe management of temporal arteritis in theelderly and in the treatment of uveitis. In recentyears, the treatment of diabetic retinopathy hasbeen greatly advanced by the combined effect of laser coagulation and scrupulous control ofdiabetes. In the past, about one-half of patientswith the proliferative type of retinopathy wouldbe expected to go blind over five years and manyof these were young people at the height of their
Failing Vision 69
Table 8.1. Failing vision in a normal-looking eye.
Fundus normal Fundus abnormal
Child Refractive error CataractDisuse amblyopia Macular degenerationInherited retinal degeneration Posterior uveitisEmotional stress
Young adult Refractive error Diabetic retinopathyRetrobulbar neuritis Retinal detachmentIntracranial space-occupying lesion Macular diseaseDrug toxicity Hypertension
Posterior uveitis
Elderly Homonymous haemianopia Macular degenerationCentral vein thrombosisChronic glaucomaCataractVitreous haemorrhageTemporal arteritis
Figure 8.1. The family thought it was just old age.

careers. The proper management of oculartrauma often has a great influence on the visualresult, and the rare but dreaded complication of ocular perforating injuries – sympatheticophthalmia – can now be treated effectively with systemic steroids. Amblyopia of disuse hasalready been mentioned; the treatment isundoubtedly effective in some cases but theresults are disappointing if the diagnosis ismade when the child is too old or when there ispoor patient co-operation.
Untreatable Causes of Failing VisionOphthalmologists are sometimes asked if thesight can be restored to a blind eye and, as ageneral rule, one can say that if there is no per-ception of light in the eye, it is unlikely that thesight can be improved, irrespective of the cause.There are several ophthalmological conditionsfor which there is no known effective treatmentand it is sometimes important that the patientis made aware of this at an early stage in orderto avoid unnecessary anxiety, and perhapsunnecessary visits to the doctor. Most degener-ative diseases of the retina fail to respond totreatment. If the retina is out of place, it can bereplaced, but old retinae cannot be replacedwith new. So far, there has been no firm evidencethat any drug can alter the course of inheritedretinal degenerations, such as retinitis pigmen-tosa, although useful information is beginningto appear about the biochemistry and geneticsof these conditions. Age-related macular degen-eration tends to run a progressive course inspite of any attempts at treatment, and althoughmost patients do not become completely blind,
it accounts for loss of reading vision in manyelderly people. Some myopic patients are sus-ceptible to degeneration of the retina in lateryears; known as myopic chorioretinal degener-ation, it can account for visual deterioration inmyopes who have otherwise undergone suc-cessful cataract or retinal surgery.
Scarring of the retina following trauma isanother cause of permanent and untreatablevisual loss, but the most dramatic and irrevoca-ble loss of vision occurs following traumaticsection of the optic nerve. One must be carefulhere before dismissing the patient as untreat-able because on rare occasions a contusioninjury to the eye or orbit can result in a haem-orrhage into the sheath of the optic nerve. Somedegree of visual recovery can sometimes occurin these patients and it has been claimed thatrecovery might be helped by surgically openingthe nerve sheath. There is one odd exception to this dramatic form of blindness that canfollow optic nerve insult: visual loss due to opticneuritis. Patients with retrobulbar neuritis(optic neuritis) nearly always recover theirvision again, whether or not they receive treat-ment. The explanation is that the visual loss iscaused by pressure from oedema rather than todamage to the nerve fibres themselves. It ishardly necessary to say that any neurologicaldamage proximal to the optic nerve tends toproduce permanent and untreatable visual loss, as exemplified by the homonymous haemianopic field defect that can follow a cerebrovascular accident.
Malignant tumours of the eye come into thiscategory of untreatable causes of visual failurebut in fact serious attempts are now being madeto treat them with radiotherapy in specialisedunits and the prognosis appears to be improv-ing in some cases.
70 Common Eye Diseases and their Management

Headache must be one of the commonest symp-toms, and few specialities escape from the diag-nostic problems that it can present. We mustbegin with the realisation that more or lesseveryone suffers from headache at some time orother. In fact, the majority of headaches thatpresent have no detectable cause and are oftenlabelled psychogenic if there seems to be a back-ground of stress. The implication is that the suf-ferer is perhaps exaggerating mild symptoms inorder to gain sympathy from his or her spouse,or even perhaps the doctor. One must, of course,be extremely cautious about not acceptingsymptoms at their face value, and certainly cerebral tumours have been overlooked for thisreason. If the psychogenic headache is the com-monest, then the headache caused by raisedintracranial pressure and a space-occupyinglesion must be the most important. Betweenthese two, the whole spectrum of causes must beconsidered. It is essential, therefore, to memo-rise a permanent checklist in order that obviouscauses are not omitted.
HistoryOften the history is the total disease in theabsence of any physical signs and it is importantto note the nature of the pain, the total durationand frequency of the pain, the time of day itoccurs, and its relation to other events or thetaking of analgesics. Headaches that are present“all the time”and are described in fanciful terms
tend not to have an organic basis; the patientwith an organic headache is not usually smi-ling. The time of day could be important: raisedintracranial pressure has the reputation ofcausing an early morning headache, which isdescribed as bursting or throbbing and can bemade worse by straining or coughing. We mustalways remember the triad of headache, vomit-ing and papilloedema in this respect, especiallyas the vomiting might not be accompanied by nausea, and is not necessarily mentioned by the patient. The family history should also be noted, especially where there is a history of migraine.
ClassificationWhen considering the different common causesof headache, an anatomical classification is auseful way of providing a reference list. The following should be considered by the examining doctor.
Cerebrospinal FluidA rise or fall from normal of the cerebrospinalfluid pressure is associated with headache.When the pressure of the cerebrospinal fluid israised, the patient usually experiences a burst-ing pain, which can interrupt sleep or appear inthe early morning. It tends to be intermittentand is made worse by coughing or lying down.It can also, of course, be accompanied by
9Headache
71
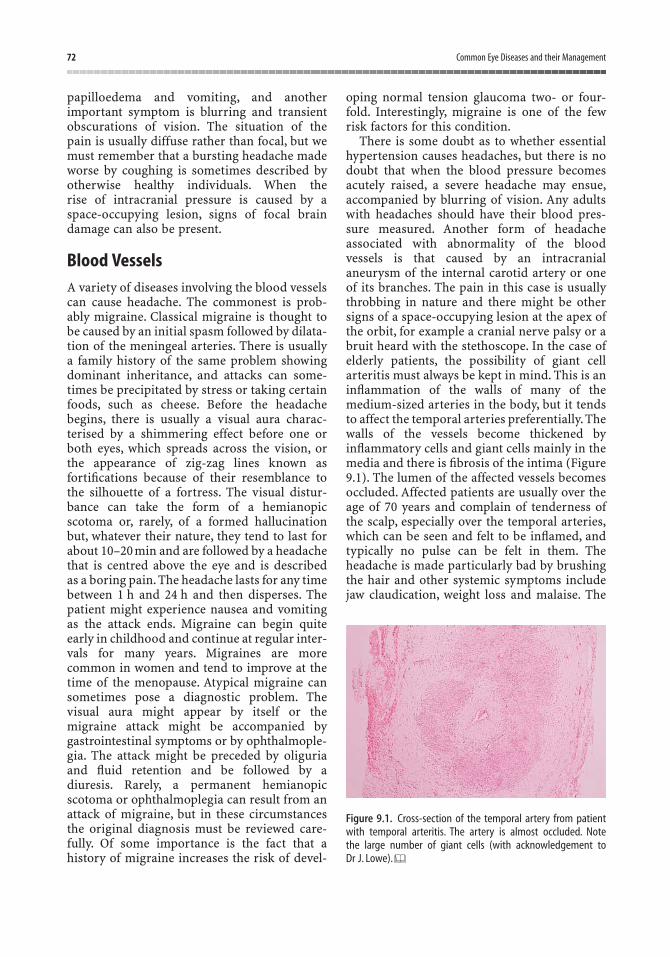
papilloedema and vomiting, and another important symptom is blurring and transientobscurations of vision. The situation of the pain is usually diffuse rather than focal, but wemust remember that a bursting headache madeworse by coughing is sometimes described byotherwise healthy individuals. When the rise of intracranial pressure is caused by aspace-occupying lesion, signs of focal braindamage can also be present.
Blood VesselsA variety of diseases involving the blood vesselscan cause headache. The commonest is prob-ably migraine. Classical migraine is thought tobe caused by an initial spasm followed by dilata-tion of the meningeal arteries. There is usuallya family history of the same problem showingdominant inheritance, and attacks can some-times be precipitated by stress or taking certainfoods, such as cheese. Before the headachebegins, there is usually a visual aura charac-terised by a shimmering effect before one orboth eyes, which spreads across the vision, orthe appearance of zig-zag lines known asfortifications because of their resemblance tothe silhouette of a fortress. The visual distur-bance can take the form of a hemianopicscotoma or, rarely, of a formed hallucinationbut, whatever their nature, they tend to last forabout 10–20 min and are followed by a headachethat is centred above the eye and is described as a boring pain. The headache lasts for any timebetween 1 h and 24 h and then disperses. Thepatient might experience nausea and vomitingas the attack ends. Migraine can begin quiteearly in childhood and continue at regular inter-vals for many years. Migraines are morecommon in women and tend to improve at thetime of the menopause. Atypical migraine cansometimes pose a diagnostic problem. Thevisual aura might appear by itself or themigraine attack might be accompanied by gastrointestinal symptoms or by ophthalmople-gia. The attack might be preceded by oliguriaand fluid retention and be followed by a diuresis. Rarely, a permanent hemianopicscotoma or ophthalmoplegia can result from anattack of migraine, but in these circumstancesthe original diagnosis must be reviewed care-fully. Of some importance is the fact that ahistory of migraine increases the risk of devel-
oping normal tension glaucoma two- or four-fold. Interestingly, migraine is one of the fewrisk factors for this condition.
There is some doubt as to whether essentialhypertension causes headaches, but there is nodoubt that when the blood pressure becomesacutely raised, a severe headache may ensue,accompanied by blurring of vision. Any adultswith headaches should have their blood pres-sure measured. Another form of headache associated with abnormality of the bloodvessels is that caused by an intracranialaneurysm of the internal carotid artery or oneof its branches. The pain in this case is usuallythrobbing in nature and there might be othersigns of a space-occupying lesion at the apex ofthe orbit, for example a cranial nerve palsy or abruit heard with the stethoscope. In the case ofelderly patients, the possibility of giant cellarteritis must always be kept in mind. This is aninflammation of the walls of many of themedium-sized arteries in the body, but it tendsto affect the temporal arteries preferentially. Thewalls of the vessels become thickened byinflammatory cells and giant cells mainly in themedia and there is fibrosis of the intima (Figure9.1). The lumen of the affected vessels becomesoccluded. Affected patients are usually over theage of 70 years and complain of tenderness ofthe scalp, especially over the temporal arteries,which can be seen and felt to be inflamed, andtypically no pulse can be felt in them. Theheadache is made particularly bad by brushingthe hair and other systemic symptoms includejaw claudication, weight loss and malaise. The
72 Common Eye Diseases and their Management
Figure 9.1. Cross-section of the temporal artery from patientwith temporal arteritis. The artery is almost occluded. Note the large number of giant cells (with acknowledgement to Dr J. Lowe).

importance of this type of headache rests on thefact that the eye is involved in about 60% ofcases and the patient can suddenly go blind inone eye and then a short time later go blind inthe other. Patients with giant cell arteritis invar-iably have a raised erythrocyte sedimentationrate (ESR) and C-reactive protein level (typi-cally the ESR is found to be above 70 mm/h). Atemporal artery biopsy is helpful in specific sit-uations to assist with the diagnosis, particularlyin those with indeterminate clinical findings.When giant cell arteritis is first considered as adiagnosis, it is advisable to start treatment withsystemic steroids without delay, before awaitingconfirmatory diagnosis on histology. Steroidtreatment is effective in preventing blindnessand is required usually for a 12–18-monthperiod. Once instituted, the response to treat-ment and the side effects should be very care-fully monitored, preferably in co-operation witha general physician with regular measurementof the ESR and other inflammatory markers.Other less common vascular causes of headacheinclude intracranial angioma and subarachnoidor subdural haemorrhage.
BloodChanges in the blood itself can also be asso-ciated with headache. It is easy to forget thatanaemic patients often have headaches, whichcan be cured by treating the anaemia. Likewise,patients with polycythaemia might also com-plain of headache. Hypoglycaemia is anotherrecognised cause; here, the symptoms occurafter strenuous exercise or insulin excess in adiabetic patient.
NervesIn many respects, cluster headache resemblesmigraine, although it is more common in men inthe third or fourth decade. The word “cluster”refers to the timing of the attacks, which can berepeated several times over a few weeks, fol-lowed by a period of remission for severalmonths. The pain is described as being severeand unilateral. There is conjunctival congestionand constriction of the pupil on the affectedside, and the attack can last from minutes tohours. Tenderness over the affected side ofthe face and nasal discharge are also features.Raeder’s paratrigeminal neuralgia probably
merges with cluster headache, being describedas severe ocular pain associated with meiosisand ptosis. Trigeminal neuralgia can be easilydistinguished from these other forms ofheadache by its distribution over one or all of theterminal branches of the trigeminal nerve andthe fact that the severe pain is triggered bytouching a part of the cheek or by chewing andswallowing. The pain is so severe that the patientcan become suicidal, and surgical division of thetrigeminal nerve at the level of the Gasserianganglion has been a method of treatment.
Postherpetic neuralgia is an extremely debil-itating form of headache experienced by elderlypeople after an attack of trigeminal herpeszoster. The pain seems to be more severe in theelderly and it can persist for many years. Thecause of the headache is usually evident whenone inspects the skin of the forehead, which isslightly whitened and scarred from the previousattack of herpes zoster. Apart from the use ofanalgesics, antidepressant drugs can also help,together with the application of local heat orvibration massage. Fortunately, the prompttreatment of the original attack of herpes zosterat primary care level with systemic acyclovirdoes seem to be reducing the incidence of thistroublesome condition.
BonesIn Paget’s disease of bone, the bones of the headenlarge and grow abnormally, the abnormalgrowth being associated with headache and,incidentally, an increase in hat size. The eyesthemselves might show optic atrophy, and closeinspection of the fundi can reveal the curiousappearance of wavy lines known as angioidstreaks. Oxycephaly is a congenital defect of theskull caused by premature closure of thesutures; patients sometimes complain ofheadache, as well as visual loss because of opticnerve compression. Multiple myeloma is thename given to a malignant proliferation ofplasma cells within the bone marrow. There isalso an excessive production of immunoglobu-lins. Osteolytic bone lesions occur especially inthe skull, and headache can be an accompani-ment. The disease is more common in theelderly and is accompanied by a high ESR. Diag-nosis is made by examining the urine forBence–Jones proteins and the serum for abnor-mal immunoglobulins. Disease of the cervical
Headache 73

vertebrae is another cause of headache, becauseof the effect of spasm of the neck muscles. Reliefof the pain by neck manipulation has beenclaimed, but the exact diagnosis must be madebefore embarking on such treatment.
MeningesIt is presumed that the pain and headache thataccompany meningitis or encephalitis are mediated through the sensory nerve supply to themeninges. The pain-sensitive structures in themiddle and anterior cranial fossa are supplied bythe fifth cranial nerve, and inflammation canproduce referred pain to the region of the eye.
The EyesThe classical eye headache is that of subacutenarrow-angle glaucoma. Here, the headache is an evening one, tends to be over one eye and is nearly always accompanied by blurring ofvision and seeing coloured haloes around streetlights. If the intraocular pressure is measuredwhen the headache is present and is found to benormal, it is unlikely that narrow-angle glau-coma is the correct diagnosis. On the otherhand, the diagnosis cannot be so easily excludedif the headache is absent at the time of exam-ination. Patients with narrow-angle glaucomaare long-sighted – therefore, beware the middle-aged, long-sighted patient with eveningheadaches and blurring of vision. Chronic open-angle glaucoma rarely causes headachebecause the rise of intraocular pressure is toogradual and not great enough. The possibilityshould be borne in mind when a patient exper-iences headaches following ocular trauma oreye surgery, that there might be secondary glau-coma. This type of glaucoma often respondswell to treatment but if ignored, can lead rapidlyto blindness. Acute iritis is associated withheadache but in practice rarely presents as suchbecause the other ocular symptoms overridethis. Patients developing endophthalmitis com-plain of severe pain in the eye and headache, thisbeing a particularly important symptom fol-lowing cataract surgery.
It has been argued that refractive error doesnot cause headache, but nothing could befurther from the truth. Refractive headache ismost commonly seen in uncorrected hyper-metropes, sometimes in children, but more
commonly in adults aged 30–40 years who arebeginning to have difficulty in accommodatingthrough their long-sightedness. For reasons ofvanity, patients might have been deliberatelyavoiding the use of glasses and it might have tobe explained to them that they have the choiceof having headaches or wearing glasses. In thepatient with no refractive error, the onset ofpresbyopia can be accompanied by headache,which is sometimes delayed until the morningafter prolonged reading. An otherwise normalperson aged 45 years should be suspected ofhaving presbyopic headaches. Uncorrectedmyopes do not usually complain of headaches.If the spectacle prescription is incorrect for any reason, a sensitive person can experienceheadache, but it is surprising how some peoplewill tolerate an incorrect spectacle lens withoutcomplaint. Ocular muscle imbalance is anuncommon cause of headache but it is an impor-tant one because it can be corrected with con-siderable relief to the patient.Usually, the patientshows a significant difference in refractive errorbetween the two eyes and when the eyes are dissociated by such means as the cover test orthe Maddox wing test, one eye tends to driftupwards or downwards. Relief of symptoms canbe achieved by incorporating a prism into thespectacle lens or, if the deviation is marked, byocular muscle surgery. Horizontal imbalance ofthe ocular movements is less closely linked withheadache, although there is a group of patients,usually young adults under stress, who seemunable to converge their eyes on near objects;instead, they allow one eye to drift outwardswhen reading. Some elderly patients have thesame problem but do not so often have asso-ciated headache. This so-called convergenceinsufficiency can be greatly improved by acourse of convergence exercises and providesone of the few instances where exercises of theeye muscles have any therapeutic value.
Pain Referred from Other SitesSinusitis is well recognised as a common causeof headache and the patient with headacheshould be questioned about recent upper res-piratory tract infections or a previous history ofsinus disease. Tenderness over the affected sinusis an important sign. The headache tends tobegin after rising in the morning and reaches a
74 Common Eye Diseases and their Management

peak later in the morning. Pain from an infectedtooth can be referred over the side of the faceand cause some diagnostic confusion but it isusually worse when chewing or biting. Painfrom a middle ear infection can cause similarproblems. The temporomandibular joint is arecognised source of referred pain over the sideof the face, and malfunctioning of the joint canresult from incorrect jaw alignment or poorlyfitting dentures.
DrugsOverindulgence in alcohol is one of the threecauses of morning headache; the other twobeing raised intracranial pressure and acutesinusitis. The diagnostic difficulty with alco-holism tends to be failure of the patient to admitor recognise excessive drinking. It might seemstrange that such a patient should ever seek adoctor’s opinion about headache, but alcoholics
do sometimes seek an ophthalmologicalopinion for their symptoms without relatingthem to alcohol intake, perhaps urged on by ananxious relative or friend. Chronic poisoning byother drugs is too rare a cause of headache inophthalmic practice to be considered here but itmight have to be borne in mind.
Posttraumatic HeadacheNearly all patients who have suffered asignificant head injury complain of headaches.The pain can remain severe for many monthsand in the worst case can last a few years.Usually, no obvious explanation can be foundapart from the original injury. The severity ofthe headache can sometimes appear to berelated to clinical depression following theinjury but other causes of headache, such asocular muscle imbalance or raised intracranialpressure, need to be excluded.
Headache 75

The widespread use of contact lenses means that the general practitioner and the ophthal-mic casualty department find themselves con-fronted with more and more patients who haverun into wearing problems of one kind oranother. For this reason, some of the likelyemergency requirements are considered here.
Types of Contact LensAs long ago as 1912, a glass contact lens wasbeing produced, but because of the manufactur-ing difficulties and wearing problems, the wide-spread use of this type of optical aid was delayeduntil the introduction of plastic scleral lenses in1937. The obvious advantage of placing a lensdirectly on the cornea over the wearing of spec-tacles is the cosmetic one, but the system alsohas optical advantages. Because the lens moveswith the eye, there are none of the problemsassociated with looking through the edge of thelens experienced by the wearer of spectacles. Inaddition, a more subtle effect is the more accu-rate representation of image size on the retina insubjects with high degrees of refractive error.
Although the original type of moulded scleralcontact lenses are still occasionally used, theyhave been largely replaced by the modern rigidand soft lenses, which are much smaller andthinner and hence cause less interference withcorneal physiology. Rigid lenses are made from gas-permeable plastics and have generallyreplaced the early “hard” lenses, which wereimpermeable to oxygen. In 1960, the hydrophilic
soft contact lens was introduced. This had thegreat advantage of being soft and malleable andhence more comfortable to wear, but optically ithas never been quite as good as the rigid lens,especially when the patient has high degrees ofastigmatism. Several different materials havenow been used in the production of soft lenses,although the basic material used is hydroxy-ethylmethacrylate. The different types of softlenses differ in their ability to take up water andtransmit oxygen.Lenses are now being made thatcan be worn for long periods without needing tobe removed and cleaned. Similarly, disposableand “planned-replacement” contact lenses arenow widely available. Care should be taken thatsuch lenses are used under professional care.
Soft contact lenses tend to absorb and adsorbmaterial from the tear film. It is particularlyimportant to ensure that a patient is not wearinga soft lens before fluorescein dye is instilled intothe eye.
Side EffectsIn general, soft contact lenses have more sideeffects than rigid lenses in the long term. Thecommonest complication of wearing moderncontact lenses is losing them. Patients are welladvised to have a pair of glasses at hand in casethey have contact-lens-wearing problems or alens is lost. More serious trouble can result from clumsy handling of the lens or leaving arigid lens in the eye for too long a period. Suchpatients quite often present with severe pain in
10Contact Lenses
77
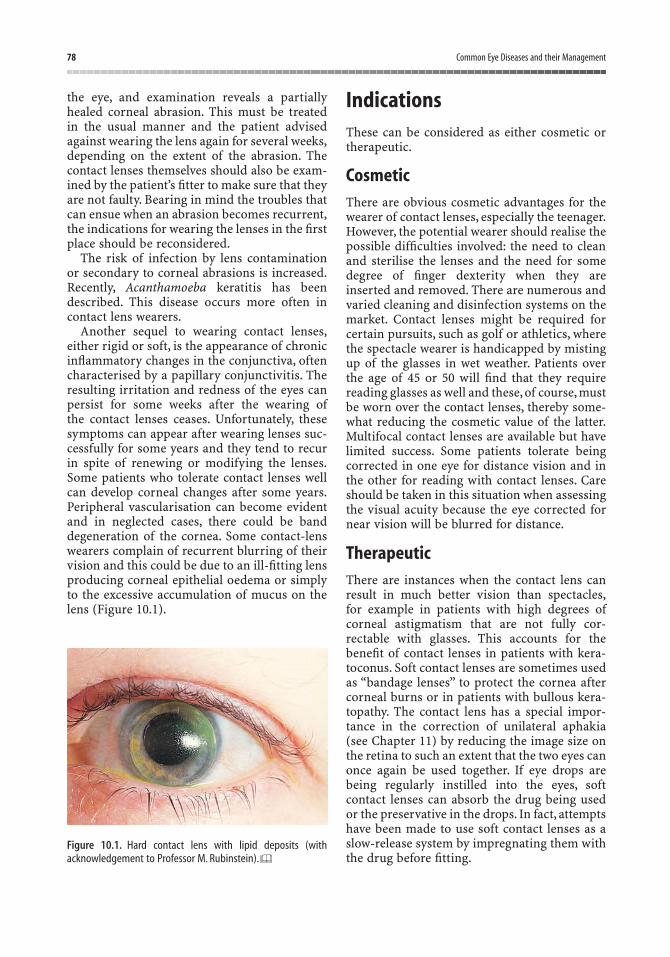
the eye, and examination reveals a partiallyhealed corneal abrasion. This must be treated in the usual manner and the patient advisedagainst wearing the lens again for several weeks,depending on the extent of the abrasion. Thecontact lenses themselves should also be exam-ined by the patient’s fitter to make sure that theyare not faulty. Bearing in mind the troubles thatcan ensue when an abrasion becomes recurrent,the indications for wearing the lenses in the firstplace should be reconsidered.
The risk of infection by lens contamination or secondary to corneal abrasions is increased.Recently, Acanthamoeba keratitis has beendescribed. This disease occurs more often incontact lens wearers.
Another sequel to wearing contact lenses,either rigid or soft, is the appearance of chronicinflammatory changes in the conjunctiva, oftencharacterised by a papillary conjunctivitis. Theresulting irritation and redness of the eyes canpersist for some weeks after the wearing ofthe contact lenses ceases. Unfortunately, thesesymptoms can appear after wearing lenses suc-cessfully for some years and they tend to recurin spite of renewing or modifying the lenses.Some patients who tolerate contact lenses wellcan develop corneal changes after some years.Peripheral vascularisation can become evidentand in neglected cases, there could be banddegeneration of the cornea. Some contact-lenswearers complain of recurrent blurring of theirvision and this could be due to an ill-fitting lensproducing corneal epithelial oedema or simplyto the excessive accumulation of mucus on thelens (Figure 10.1).
IndicationsThese can be considered as either cosmetic ortherapeutic.
CosmeticThere are obvious cosmetic advantages for thewearer of contact lenses, especially the teenager.However, the potential wearer should realise thepossible difficulties involved: the need to cleanand sterilise the lenses and the need for somedegree of finger dexterity when they areinserted and removed. There are numerous andvaried cleaning and disinfection systems on themarket. Contact lenses might be required forcertain pursuits, such as golf or athletics, wherethe spectacle wearer is handicapped by mistingup of the glasses in wet weather. Patients overthe age of 45 or 50 will find that they requirereading glasses as well and these, of course, mustbe worn over the contact lenses, thereby some-what reducing the cosmetic value of the latter.Multifocal contact lenses are available but havelimited success. Some patients tolerate beingcorrected in one eye for distance vision and inthe other for reading with contact lenses. Careshould be taken in this situation when assessingthe visual acuity because the eye corrected fornear vision will be blurred for distance.
TherapeuticThere are instances when the contact lens canresult in much better vision than spectacles,for example in patients with high degrees ofcorneal astigmatism that are not fully cor-rectable with glasses. This accounts for thebenefit of contact lenses in patients with kera-toconus. Soft contact lenses are sometimes usedas “bandage lenses” to protect the cornea aftercorneal burns or in patients with bullous kera-topathy. The contact lens has a special impor-tance in the correction of unilateral aphakia(see Chapter 11) by reducing the image size onthe retina to such an extent that the two eyes canonce again be used together. If eye drops arebeing regularly instilled into the eyes, softcontact lenses can absorb the drug being usedor the preservative in the drops. In fact, attemptshave been made to use soft contact lenses as aslow-release system by impregnating them withthe drug before fitting.
78 Common Eye Diseases and their Management
Figure 10.1. Hard contact lens with lipid deposits (withacknowledgement to Professor M. Rubinstein).

Section IIIProblems of the Eye Surgeon
The eye surgeon is confronted by problems thathave been selected to a greater or lesser extentby the general practitioner or the optometrist.In the larger teaching centres, he or she may bein a position to see patients selected in turn byother ophthalmologists and thus might be ableto gain a detailed experience of relatively fewaspects of the subject. In this section, the
cardinal eye problems that confront any eyesurgeon are described. Being surgical problems,they are all fairly rapidly responsive to treat-ment, sometimes involving the restoration ofsight to the blind patient. In other cases, the sur-gical treatment might simply arrest or delay theprogress of visual failure or relieve the patientof pain or discomfort.
“Cataract” means an opacity of the lens and it isthe commonest potentially blinding conditionthat confronts the eye surgeon. This is not to saythat every person with cataract is liable to goblind. Many patients have relatively slight lensopacities that progress slowly. Fortunately, theresults of surgery are good, a satisfactory im-provement of vision being obtained in over 90%of cases. It is usually possible to forewarn thepatients when there is an extra element of doubtabout the outcome. To the uninformed patient,the word “cataract” strikes a note of fear and itmight be necessary to explain that opacities inthe lens are extremely common in elderlypeople. It is only when the opaque lens fibresbegin to interfere with the vision that the term“cataract” is used. Many patients have a slightdegree of cataract, which advances so slowlythat they die before any visual problems arise.Nobody need now go blind from cataract;however, one still encounters elderly peoplewho, from ignorance or neglect, are left immo-bilised by this form of blindness, and it is esp-ecially important that the general practitioner isable to recognise the condition.
The LensThe human lens is a surprising structure. It isavascular and yet it is actively growing through-out life, albeit extremely slowly. It receives itsnourishment from the aqueous fluid that bathesit. The lens is enclosed in an elastic capsule and,
for this reason, tends to assume a sphericalshape, or would do if the moulding of the lensfibres allowed. In situ the shape of the lens ismaintained by a series of taut fibres known asthe zonule. The fibres exert radial tension on thelens but the tension is reduced when the circ-ular part of the ciliary muscle contracts. Thereduced tension of the zonule allows the lens toassume a more spherical shape and hence theanteroposterior diameter of the lens increases.As a result, the refracting power of the lensincreases, that is to say, light rays are more bentand the eye becomes focused on near objects.This process of accommodation, which is pro-duced by relaxation of the lens but contractionof the ciliary muscle, gradually becomes lesseffective as we grow older, probably because thelens becomes less malleable rather than becausethe ciliary muscle is becoming weaker. Thisreduction in the range of accommodationexplains why the little child will present anobject close to an adult’s eyes and expect him or her to see it clearly. It also explains why, in the mid-40s, it becomes necessary to hold abook further from one’s eyes if it is to be readeasily and also the subsequent inability to readwithout the assistance of a spectacle lens, whichprovides additional converging power. The needfor reading glasses occurs in people with normaleyes at about the age of 45 (presbyopia) but thisis only a milestone in a slowly progressive pathof deterioration that begins at birth.
Histological section of the lens reveals thatbeneath the capsule there is an anterior
11Cataract
81

epithelium with a single layer of cells, but nosuch layer is evident beneath the posteriorcapsule. Furthermore, if one follows the single-layered anterior epithelium to the equator of thelens, the epithelial cells can be seen to elongateprogressively and lose their nuclei as they aretraced into the interior of the lens. Thus, one candeduce from histological sections that the lensfibres are being continuously laid down fromthe epithelial cells at the equator. The actualarrangement of the lens fibres is quite complex,each fibre being made up of a prismatic six-sided band bound to its fellow by an amorphouscement substance.
Slit-lamp examination of the lens reveals thepresence of the lens sutures, which mark thepoints of junction of the end of the lens fibres.Two such sutures are usually seen, both oftentaking the form of the letter “Y”, the posteriorsuture being inverted. The lens fibres containproteins known as “crystallins” and have theproperty of setting up an antigen–antibodyreaction if they are released into the eye fromthe lens capsule. One other feature of the lens,which can usually be seen with the slit-lampmicroscope, is an object looking like a pig’s tail,which hangs from the posterior capsule. This isthe remains of the hyaloid artery, a vessel thatruns in the embryonic eye from the optic disc tothe vascular tunic of the lens, which is presentat that stage (Figure 11.1).
AetiologyHaving learned of the complex structure of thelens, perhaps one should be more surprised thatthe lens retains its transparency throughout lifethan that some of the lens fibres might becomeopaque. There are a number of reasons why lensfibres become opaque but the commonest andmost important is ageing. The various causeswill now be considered.
AgeThe majority of cataracts are associated with theageing process, and some of the biochemicalchanges in the lens fibres are now being under-stood. We know that certain families are moresusceptible to age-related cataract, but a degreeof opacification of the lens is commonplace inthe elderly. Often the opacity is limited to theperipheral part of the lens and the patient mightbe unaware of any problem. It is usual to limitthe term “cataract” to the situation where theopacities are causing some degree of visualimpairment. Elderly patients are often reas-sured to learn that their eye condition is part ofthe general ageing process and that only incertain instances does the opacification pro-gress to the point where surgery is required.
DiabetesThe new junior doctor working in an eye hos-pital must be impressed by the number of dia-betics with cataracts who pass through his orher hands, and might be forgiven for deducingthat diabetes is a common cause of cataract. Tosee the situation in perspective, one must realisethat both cataracts and diabetes are commondiseases of the elderly and coincide quite often.Of course, the matter has been investigated fromthe statistical point of view and it has beenshown that there is a somewhat higher incid-ence of cataract in diabetics, mainly becausethey tend to develop lens opacities at an earlierage. A special type of cataract is seen in youngdiabetics and in these cases, the lens can becomerapidly opaque in a few months. Fortunately,this is not common, usually occurring ininsulin-dependent (type 1) patients who havehad difficulty with the control of their diabetes.It is claimed that, in its early stages, this type of
82 Common Eye Diseases and their Management
Figure 11.1. Cross-section of a child’s lens: aqueous on left, vit-reous on right. Note the hyaloid remnant and the “Y” sutures(with acknowledgement to M. L. Berliner, 1949).

cataract can be reversible, but such an occur-rence is so rare that it has not presented muchopportunity for study.
Secondary CausesCataract can be secondary to disease in the eyeor disease elsewhere in the body.
Secondary to Disease in the Eye
More or less any terminal event in the eye tendsto be associated with cataract. Advanced uncon-trolled glaucoma is often associated with anopaque lens, as are chronic iridocyclitis andintraocular tumours. Certain specific eye dis-eases are accompanied by cataract; for example,patients who suffer from the inherited retinaldegeneration, retinitis pigmentosa, sometimesdevelop a particular type of opacity in the pos-terior part of the lens. The removal of such acataract can sometimes restore a considerableamount of vision, at least for a time.
Secondary to Disease Elsewhere
It might be recalled that the lens is ectodermal,being developed as an invagination of the over-lying surface ectoderm. It is not surprising,therefore, that some skin diseases are associatedwith cataract. In particular, patients sufferingfrom asthma and eczema might present to theeye surgeon in their late 50s. Dysfunction of the parathyroid glands is a rare cause ofcataract and Down’s syndrome is a morecommon association.
Trauma
Contusion
A direct blow on the eye, if it is severe enough,can cause the lens to become opaque. An injuryfrom a squash ball is a typical example of thetype of force required. Sometimes the appear-ance of the cataract might be delayed even forseveral years. The onset of unilateral cataractmust always make one suspect the possibility ofprevious injury, but a cause-and-effect relation-ship can be difficult to prove in the absence ofany other signs of previous contusion. It seemsunlikely that a cataract would form unless therehad been a direct blow on the eye itself, although
occasionally medicolegal claims are made forcompensation when a cataract has developedfollowing a blow on the side of the head.
Perforation
A perforating wound of the eye bears a muchhigher risk of cataract formation. If the perf-orating object (e.g., a broken beer glass) passesthrough the cornea without touching the lens,the lens is usually spared and, in the absence of significant contusion, a cataract does not form. This, of course, also depends on carefulmanagement of the corneal wound and the prevention of infection. Unfortunately, suchperforating injuries can also involve splitting ofthe lens capsule, with spilling out of the lensfibres into the anterior chamber. The series ofevents following such an injury is dependent onthe age of the individual. When the lens capsuleof a child is ruptured, a vigorous inflammatoryreaction is set up in the anterior chamber andthe lens matter will usually gradually becomeabsorbed, in the absence of treatment, over aperiod of about a month. This leaves behind thelens capsule and often a clear pupil. In spite ofthis, the patient cannot see clearly because mostof the refractive power of the eye is lost. This hasserious optical consequences and the need foran artificial intraocular lens. When the lenscapsule of an adult is ruptured, a similarinflammatory reaction ensues, but there tendsto be more fibrosis, and a white plaque of fibroustissue could remain to obstruct the pupil.Rarely, it is possible for a lens to be perforatedwith subsequent opacity limited to the site ofperforation – indeed, one occasionally sees aforeign body within the lens surrounded byopaque fibres but limited to a small part ofthe lens.
Radiation
Visible light does not seem to cause cataract,although claims have been made that indiv-iduals from white races living for long periodsin the tropics can show a higher incidence ofcataract. In practice, this is not easy to confirm.In spite of public misapprehension, ultravioletlight probably does not cause cataract either,because the shorter wavelengths fail to pene-trate the globe. These shorter wavelengthsbeyond the blue end of the visible spectrum can
Cataract 83

produce a dramatic superficial burn of thecornea, which usually heals in about 48 h. Thisinjury, which is typified by “snow blindness” and“welders’ flash”, will be discussed in Chapter 15.Prolonged doses of infrared rays can producecataract; this used to be seen occasionally inglassblowers and steel workers, but the wearingof goggles has now more or less eliminated this. X-rays and gamma rays can also producecataracts, as was witnessed by the mass ofreports that followed the explosion of theatomic bombs at Nagasaki and Hiroshima inJapan. Radiation cataract is now seen followingwhole-body radiation for leukaemia but the riskis only significant when therapeutic doses ofX-rays are used.
Congenital FactorsMany of the cases of congenital cataract seen inophthalmic practice are inherited. Sometimesthere is a dominant family history and there aremany other possible associated defects, some of which fit into named syndromes. Acquiredcongenital cataract can result from maternalrubella infection during the first trimester ofpregnancy. The association of deafness, con-genital heart lesions and cataract must always beborne in mind. The ophthalmic house surgeonmust take special care when examining the con-genital cataract case preoperatively and likewise,the paediatric house surgeon must bear in mindthat congenital cataracts might be overlooked,especially if they are not severe. Sometimes thecataracts can be slight at birth and graduallyprogress subsequently, or sometimes they canremain stationary until later years.
ToxicityToxic cataracts are probably rare, althoughseveral currently used drugs have been incrim-inated, the most notable being systemic steroids.Chlorpromazine has also been shown to causelens opacities in large doses, and so has the useof certain meiotics, including pilocarpine. Muchof our knowledge of drug-induced cataracts is based on former animal experiments. Thepotential danger of new drugs causing cataractwas shown in the 1930s after the introduction ofdinitrophenol as a slimming agent. This pro-duced a large number of lens opacities before itwas eventually withdrawn.
Symptoms
Many patients complain of blurred vision,which is usually worse when viewing distantobjects. If the patient is unable to read smallprint, the surgeon might suspect that otherpathology, such as macular degeneration, couldbe present. One must bear in mind that someelderly patients say that they cannot read whenit is found that they can read small print if care-fully tested. It is a curious fact that when thecataract is unilateral, the patient can claim thatthe loss of vision has been quite sudden. Elu-cidation of the history in these cases sometimesreveals that the visual loss was noted whenwashing and observing the face in the mirror.When one hand is lowered before the other, theunilateral visual loss is noticed for the first timeand interpreted as a sudden event. The historyin cataract cases might be further confused by anatural tendency for patients to project theirsymptoms into the spectacles, and several pairsmight be obtained before the true cause of theproblem is found. In order to understand thesymptoms of cataract, it is essential to under-stand what is meant by index myopia. Thissimply refers to the change in refractive powerof the lens, which occurs as a preliminary tocataract formation. Index myopia can also result from uncontrolled diabetes. If we imaginean elderly patient who requires reading glasses(for presbyopia) in the normal way but noglasses for viewing distant objects, the onset ofindex myopia will produce blurring of distancevision, but also the patient will discover to hisor her surprise that it is possible to read againwithout glasses. In the same way, the hyper-metropic patient will become less hyper-metropic and find that it is possible to see againin the distance without glasses. The ageingfibres in the precataractous lens become moreeffective at converging light rays so that parallelrays of light are brought to a focus more anteri-orly in the eye.
Apart from blurring of vision, the cataractpatient often complains of monocular diplopia.Sometimes even a slight and subtle opacity inthe posterior part of the lens can cause thepatient to notice, for example, that car rear lightsappear doubled, and this can be reproduced with the ophthalmoscope light. Monoculardiplopia is sometimes regarded as a rather
84 Common Eye Diseases and their Management
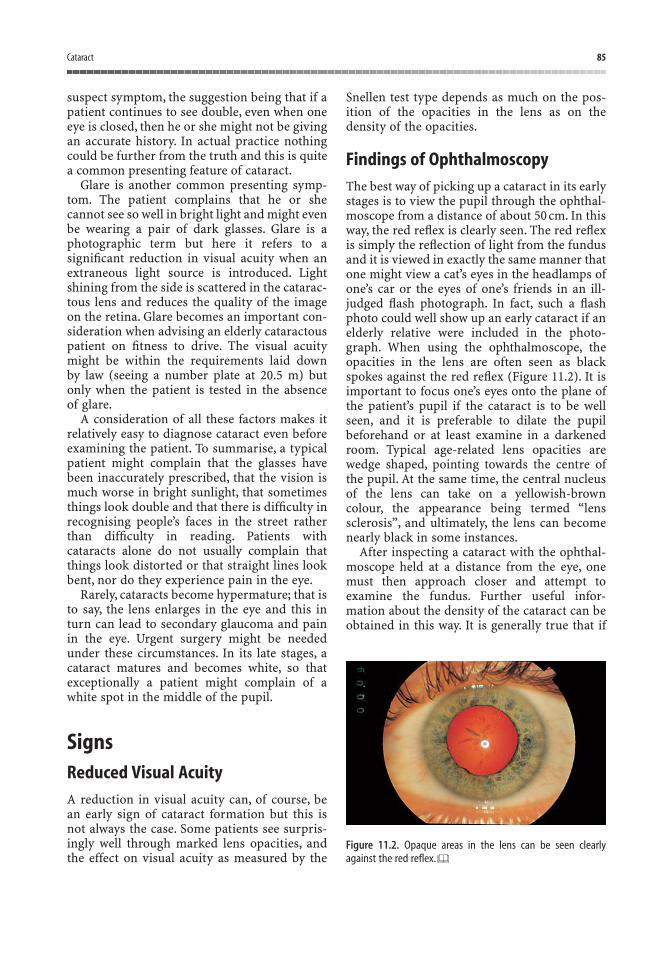
suspect symptom, the suggestion being that if apatient continues to see double, even when oneeye is closed, then he or she might not be givingan accurate history. In actual practice nothingcould be further from the truth and this is quitea common presenting feature of cataract.
Glare is another common presenting symp-tom. The patient complains that he or shecannot see so well in bright light and might evenbe wearing a pair of dark glasses. Glare is aphotographic term but here it refers to asignificant reduction in visual acuity when anextraneous light source is introduced. Lightshining from the side is scattered in the catarac-tous lens and reduces the quality of the imageon the retina. Glare becomes an important con-sideration when advising an elderly cataractouspatient on fitness to drive. The visual acuitymight be within the requirements laid down by law (seeing a number plate at 20.5 m) butonly when the patient is tested in the absence of glare.
A consideration of all these factors makes itrelatively easy to diagnose cataract even beforeexamining the patient. To summarise, a typicalpatient might complain that the glasses havebeen inaccurately prescribed, that the vision ismuch worse in bright sunlight, that sometimesthings look double and that there is difficulty inrecognising people’s faces in the street ratherthan difficulty in reading. Patients withcataracts alone do not usually complain thatthings look distorted or that straight lines lookbent, nor do they experience pain in the eye.
Rarely, cataracts become hypermature; that isto say, the lens enlarges in the eye and this inturn can lead to secondary glaucoma and painin the eye. Urgent surgery might be neededunder these circumstances. In its late stages, acataract matures and becomes white, so thatexceptionally a patient might complain of awhite spot in the middle of the pupil.
SignsReduced Visual AcuityA reduction in visual acuity can, of course, be an early sign of cataract formation but this isnot always the case. Some patients see surpris-ingly well through marked lens opacities, andthe effect on visual acuity as measured by the
Snellen test type depends as much on the pos-ition of the opacities in the lens as on thedensity of the opacities.
Findings of OphthalmoscopyThe best way of picking up a cataract in its earlystages is to view the pupil through the ophthal-moscope from a distance of about 50 cm. In thisway, the red reflex is clearly seen. The red reflexis simply the reflection of light from the fundusand it is viewed in exactly the same manner thatone might view a cat’s eyes in the headlamps ofone’s car or the eyes of one’s friends in an ill-judged flash photograph. In fact, such a flashphoto could well show up an early cataract if anelderly relative were included in the photo-graph. When using the ophthalmoscope, theopacities in the lens are often seen as blackspokes against the red reflex (Figure 11.2). It isimportant to focus one’s eyes onto the plane ofthe patient’s pupil if the cataract is to be wellseen, and it is preferable to dilate the pupilbeforehand or at least examine in a darkenedroom. Typical age-related lens opacities arewedge shaped, pointing towards the centre ofthe pupil. At the same time, the central nucleusof the lens can take on a yellowish-browncolour, the appearance being termed “lens sclerosis”, and ultimately, the lens can becomenearly black in some instances.
After inspecting a cataract with the ophthal-moscope held at a distance from the eye, onemust then approach closer and attempt toexamine the fundus. Further useful infor-mation about the density of the cataract can beobtained in this way. It is generally true that if
Cataract 85
Figure 11.2. Opaque areas in the lens can be seen clearlyagainst the red reflex.
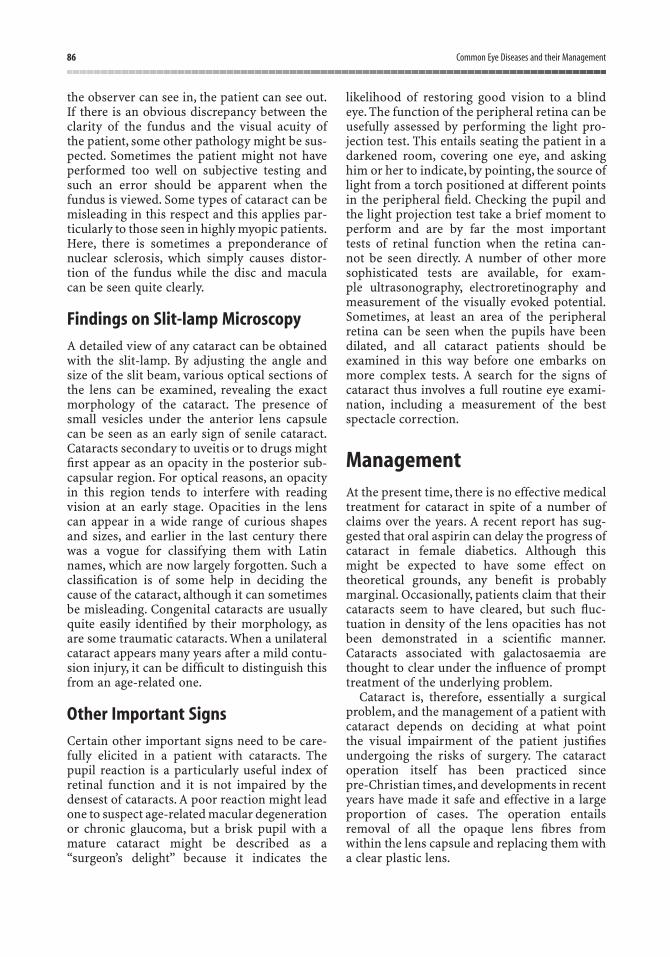
the observer can see in, the patient can see out.If there is an obvious discrepancy between theclarity of the fundus and the visual acuity ofthe patient, some other pathology might be sus-pected. Sometimes the patient might not haveperformed too well on subjective testing andsuch an error should be apparent when thefundus is viewed. Some types of cataract can bemisleading in this respect and this applies par-ticularly to those seen in highly myopic patients.Here, there is sometimes a preponderance ofnuclear sclerosis, which simply causes distor-tion of the fundus while the disc and macula can be seen quite clearly.
Findings on Slit-lamp MicroscopyA detailed view of any cataract can be obtainedwith the slit-lamp. By adjusting the angle andsize of the slit beam, various optical sections ofthe lens can be examined, revealing the exactmorphology of the cataract. The presence ofsmall vesicles under the anterior lens capsulecan be seen as an early sign of senile cataract.Cataracts secondary to uveitis or to drugs mightfirst appear as an opacity in the posterior sub-capsular region. For optical reasons, an opacityin this region tends to interfere with readingvision at an early stage. Opacities in the lens can appear in a wide range of curious shapesand sizes, and earlier in the last century therewas a vogue for classifying them with Latinnames, which are now largely forgotten. Such aclassification is of some help in deciding thecause of the cataract, although it can sometimesbe misleading. Congenital cataracts are usuallyquite easily identified by their morphology, asare some traumatic cataracts. When a unilateralcataract appears many years after a mild contu-sion injury, it can be difficult to distinguish thisfrom an age-related one.
Other Important SignsCertain other important signs need to be care-fully elicited in a patient with cataracts. Thepupil reaction is a particularly useful index ofretinal function and it is not impaired by thedensest of cataracts. A poor reaction might leadone to suspect age-related macular degenerationor chronic glaucoma, but a brisk pupil with amature cataract might be described as a“surgeon’s delight” because it indicates the
likelihood of restoring good vision to a blindeye. The function of the peripheral retina can beusefully assessed by performing the light pro-jection test. This entails seating the patient in adarkened room, covering one eye, and askinghim or her to indicate, by pointing, the source oflight from a torch positioned at different pointsin the peripheral field. Checking the pupil andthe light projection test take a brief moment toperform and are by far the most important tests of retinal function when the retina can-not be seen directly. A number of other moresophisticated tests are available, for exam-ple ultrasonography, electroretinography andmeasurement of the visually evoked potential.Sometimes, at least an area of the peripheralretina can be seen when the pupils have beendilated, and all cataract patients should be examined in this way before one embarks onmore complex tests. A search for the signs ofcataract thus involves a full routine eye exami-nation, including a measurement of the bestspectacle correction.
ManagementAt the present time, there is no effective medicaltreatment for cataract in spite of a number ofclaims over the years. A recent report has sug-gested that oral aspirin can delay the progress ofcataract in female diabetics. Although thismight be expected to have some effect on theoretical grounds, any benefit is probablymarginal. Occasionally, patients claim that theircataracts seem to have cleared, but such fluc-tuation in density of the lens opacities has notbeen demonstrated in a scientific manner.Cataracts associated with galactosaemia arethought to clear under the influence of prompttreatment of the underlying problem.
Cataract is, therefore, essentially a surgicalproblem, and the management of a patient withcataract depends on deciding at what point the visual impairment of the patient justifiesundergoing the risks of surgery. The cataractoperation itself has been practiced since pre-Christian times, and developments in recentyears have made it safe and effective in a largeproportion of cases. The operation entailsremoval of all the opaque lens fibres fromwithin the lens capsule and replacing them witha clear plastic lens.
86 Common Eye Diseases and their Management

In the early part of the last century the tech-nical side of cataract surgery necessitatedwaiting for the cataract to become “ripe”. Nowa-days no such waiting is needed and it istheoretically possible to remove a clear lens. Thedecision to operate is based on whether thepatient will see better afterwards. Moderncataract surgery can restore the vision in aremarkable way and patients often say that theyhave not seen so well for many years. Indeed,many patients have quite reasonable visionwithout glasses but this cannot be guaranteedand, because the plastic lens implant gives afixed focus, glasses will inevitably be needed forsome distances. Probably the worst thing thatcan happen after the operation is infectionleading to endophthalmitis and loss of the sightof the eye. Although this only occurs in aboutone out of a thousand cases, the patient con-templating cataract surgery needs to be aware ofthe possibility. Before the operation, it is now aroutine to measure the length of the eye and thecorneal curvature. Knowing these two measure-ments, one can assess the strength of lensimplant that is needed. When deciding on thestrength of implant, it is necessary to considerthe other eye. The aim is usually to make the twoeyes optically similar because patients find itdifficult to tolerate two different eyes.
When to OperateEven though the decision to operate on acataract must be made by the ophthalmicsurgeon, optometrists and the nonspecialistgeneral practitioner need to understand the rea-soning behind this decision. Elderly patientstend to forget what they have been told in theclinic and might not, for example, understandwhy cataract surgery is being delayed whenmacular degeneration is the main cause of visualloss. An operation is usually not required if thepatient has not noticed any problem, althoughsometimes the patient can deny the problemthrough some unexpressed fear. The require-ments of the patient need to be considered; thoseof the chairbound arthritic 80-year-old subjectwho can still read small print quite easily are dif-ferent from the younger business person whoneeds to be able to see a car number plate at 20.5 m in order to drive. The visual acuity byitself is not always a reliable guide.Some patientswho have marked glare might need surgery with
a visual acuity of 6/9, whereas others with lessvisual demands might be quite happy with avision of 6/12 or 6/18. Early surgery might beneeded to keep a joiner or bus driver at work forwhich good binocular vision is needed.
Age of the PatientBy itself, the age of the patient need have littleinfluence on the decision to operate. Manypeople over the age of 100 years have had theircataracts successfully removed. The generalhealth of the patient must be taken into accountand this can influence one’s decision in unex-pected ways. Occasionally, one is presented witha patient who has difficulty with balancing,perhaps as a result of Ménière’s disease or someother cause. The patient asks for cataractsurgery in the hope that this will cure theproblem. Unless the cataracts are advanced,the result might be disappointing. Sometimescataract surgery is requested in a nearly blind,demented patient on the grounds that thedementia will improve with improvement of thevision. Although this occasionally happens,often the patient’s mental state is made worseeven though the sight is better. This raises someinteresting ethical problems for the surgeon and relatives.
In the case of the child with congenitalcataracts, the indications for surgery dependlargely on the degree of opacification of the lens.An incomplete cataract might permit a visualacuity of 6/12 or 6/18 and yet the child could beable to read small print by exercising the largeamount of available focusing power. Such achild could undergo normal schooling, andcataract surgery might never be required. A complete cataract in both eyes demands earlysurgery and this can be undertaken during thefirst few months of life. There is a high risk thatone eye could become amblyopic in these youngpatients, even after cataract surgery.
Traumatic CataractThis is usually a unilateral problem in a youngerpatient and sometimes the nature of the damageto the eye prevents the insertion of an intra-ocular lens. The patient could be left with nolens in the eye, a situation known as aphakia.Vision can be restored by a strong convex spectacle lens but the difference between the
Cataract 87

two eyes makes it impossible to wear glasses.This is partly because everything looks muchbigger with the corrected aphakic eye; the imageon the retina is abnormally large. By wearing acontact lens on the cornea, the optical problemsmight be solved, but it is an unfortunate fact thatpatients with traumatic cataracts usually haveworking conditions that are unsuited to thewearing of a contact lens.
The Cataract OperationEvery medical student should witness at leastone cataract operation during the period oftraining. It is an example of a classical pro-cedure, which has been practiced for 3000 years.The earliest method for dealing with cataractwas known as couching. This entailed pushingthe lens back into the vitreous, where it wasallowed to sink back into the fundus of the eye.Although this undoubtedly proved a simple andsatisfactory procedure in some instances, therewas a tendency for the lens to set up a vigorousinflammatory reaction within the eye, with sub-sequent loss of sight.
Modern cataract surgery was founded by theFrench surgeon Jacques Daviel in the eighteenthcentury. The operation that he devised involvedseating the patient in a chair and making anincision around the lower half of the cornea.The lens was then removed through theopening. The results claimed were remarkableconsidering the technical difficulties that hemust have encountered. Subsequently, the pro-cedure was facilitated by lying the patient downand making the incision around the upper partof the cornea where, in the postoperativeperiod, it was protected by the upper eyelid. Theuse of local anaesthesia was introduced at theend of the nineteenth century and at the sametime, attempts were made to suture the corneaback into position. By the beginning of thetwentieth century, two methods had evolved forthe actual removal of the lens. The safest waywas to incise the anterior lens capsule and thenwash out or express the opaque nucleus, pre-serving the posterior lens capsule as a protec-tive wall against the bulging vitreous face. Thisis known as the extracapsular technique. Theintracapsular cataract extraction became thestandard operation of choice in most patientsover the age of 50 years during the early part ofthe twentieth century. It involved removing the
complete lens within its capsule and, by thismeans, avoided subsequent operations to openup residual opaque posterior capsule.
Perhaps the most dramatic change in cataractsurgery has occurred in the latter half of thetwentieth century, with the introduction ofintraocular acrylic lens implants. Initially, theywere mostly employed with intracapsularsurgery, but a new technique for extracapsularsurgery was then developed and found to besuccessful with implants. Many different typesand designs of intraocular lens have been usedover the years. Figure 11.3 shows a commonlyused type of lens implant. The trend is nowtowards smaller incision surgery and the use offoldable or injectable implants, which unfoldinto position as they are being inserted into theeye. An important and widely used technique isphakoemulsification. Here, the opaque lensnucleus is removed through a complex cannula,which breaks up the lens matter ultrasonicallybefore sucking it from the eye (Figures 11.4, 11.5and 11.6).
88 Common Eye Diseases and their Management
Figure 11.3. A typical plastic intraocular implant. There are dif-ferent designs to suit different surgical techniques.
Figure 11.4. Type of probe used for phakoextraction of theopaque lens nucleus.

Time Spent in HospitalMany cataract operations are now done underlocal anaesthesia as day cases. General anaes-thesia is preferred in younger patients and esp-ecially where there is a risk of straining ormoving during the procedure as, for example,when the patient is deaf. An overnight stay isneeded after a general anaesthetic in manycases. The elderly patient living alone with norelatives is also usually kept overnight in hospi-tal but the trend is towards more and more day-
case work, dictated partly by economic reasons,but also by safer surgery.
ConvalescenceIt is a fair generalisation to say that an eyerequires about four to six weeks for full healingto take place following a cataract operation. Onthe other hand, most of the healing takes placein the first two weeks. It is usual for patients toreturn to work after two weeks. After phakoe-mulsification, glasses can be prescribed at thispoint but after larger incision surgery the pre-scription of new glasses is usually done after amonth. The visual recovery is undoubtedlyquicker after small incision surgery but the ulti-mate visual result is probably no better thanwhen a larger incision is used. Most hospitalsprovide a “hand-out” of do’s and don’ts for thepatients. The important thing is for the patientto avoid rubbing the eye and to seek immediatemedical advice if the eye becomes painful,because this can indicate infection, whichrequires immediate treatment to prevent blind-ness. Following routine cataract surgery, it isusual to instill antibiotic drops combined with asteroid (usually in one bottle) four times dailyfor three to four weeks.
Infection is the rare but dreaded complicationand this is usually heralded by pain, redness,discharge and deterioration of vision. The infec-tion might be acquired from the patient’s owncommensal eyelid flora or from contaminationat the time of surgery. The commonest types ofbacterial infection are streptococcal and staphy-lococcal species. About 10–20% of patientsdevelop opacification of the posterior lenscapsule behind the implant after months oryears. This is simply cured by making anopening in the capsule with a special type oflaser. This is a day-case procedure, whichrequires no anaesthetic and takes two or threeminutes. When corneal sutures have been used,these can sometimes need to be removed andthis can also be done on a “while-you-wait”basisin the outpatient department.
SummaryAt primary care level, it is important to be ableto diagnose cataract but also to understand thebenefits and risks of cataract surgery in order to
Cataract 89
Figure. 11.5. Injection of intraocular lens implant through small incision.
Figure 11.6. Intraocular lens implant within capsular bag.

90 Common Eye Diseases and their Management
be able to give the patient advice as to when thecataract is bad enough to need an operation. Anunderstanding of the meaning of aphakia andthe optical consequences of an implant are alsouseful. Most patients who present with cataractsare diagnosed as having age-related cataractsand investigations as to the cause are limited totests to exclude diabetes and to confirm that thepatient is fit for surgery. An understanding ofthe symptoms of cataract is helped by under-standing the meaning of index myopia.
Figure 11.7 is a final reminder of the signsand symptoms of cataract. An elderly womanwould not normally be able to read small print without glasses and this lady’s eyes must be abnormal. She might have inheritedmyopia, allowing her to see near objects withoutthe need for a presbyopic lens, but the myopiacould also be index myopia, which in turn could be caused by early cataract formation.Another cause of index myopia could be uncontrolled diabetes.
Figure 11.7. An elderly person cannot read without glassesunless he or she is myopic. Myopia in the elderly can be causedby cataract. (“Rembrandt’s mother”, with acknowledgement toRijksmuseum-Stichting.)

The word “glaucoma” refers to the apparentgrey–green colour of the eye suffering from anattack of acute narrow-angle glaucoma. Now-adays the term has come to cover a group of eyediseases characterised by raised intraocularpressure. These diseases are quite distinct andthe treatment in each case is quite different.Glaucoma might be defined as a “pathologicalrise in the intraocular pressure sufficientenough to damage vision”. This is to distinguishthe normal elevation of intraocular pressureseen in otherwise normal individuals. Here, weconsider what is meant by the “normal intra-ocular pressure”.
Normal Intraocular PressureMeasurement of the intraocular pressure in alarge number of normal subjects reveals anormal distribution extending from pressuresof 10–12 mmHg to 25–28mmHg. The pattern ofdistribution fits a Gaussian curve, so that themajority of subjects have a pressure of about 16 mmHg. For clinical purposes, it is necessaryto set an arbitrary upper limit of normal. By and large, the eye can stand low pressuresremarkably well, but when the pressure isabnormally high, the circulation of bloodthrough the eye becomes jeopardised andserious damage can ensue. For clinical pur-poses, an upper level of 21 mmHg is oftenaccepted. Above this level, suspicions are raisedand further investigations undertaken.
Maintenance of Intraocular PressureIf the eye is to function as an effective opticalinstrument, it is clear that the intraocular pres-sure must be maintained at a constant level. Atthe same time, an active circulation of fluidthrough the globe is essential if the structureswithin it are to receive adequate nourishment.The cornea and sclera form a tough fibrous andunyielding envelope and within this an evenpressure is maintained by a balance between theproduction and drainage of aqueous fluid.
Aqueous is produced by the ciliary epi-thelium by active secretion and ultrafiltration. Acontinuous flow is maintained through thepupil, where it reaches the angle of the anteriorchamber.
On reaching the angle of the anteriorchamber, aqueous passes through a grill knownas the trabecular meshwork and then reaches acircular canal embedded in the sclera known asSchlemm’s canal. This canal runs as a ringaround the limbus (corneoscleral junction) andfrom it, minute channels radiate outwardsthrough the sclera to reach the episcleral circ-ulation. These channels are known as aqueousveins and they transmit clear aqueous to theepiscleral veins, which lie in the connectivetissue underlying the conjunctiva. In actual fact,the proof of the route of drainage of aqueouscan be verified by any medical student – itsimply entails examining the white of the eye
12Glaucoma
91

around the cornea with extreme care, using thehigh power of the slit-lamp microscope. After atime, one can sometimes detect that some of thedeeper veins convey parallel halves of blood andaqueous in the region beyond the junction ofaqueous and episcleral vein.
The relative parts played by ciliary epitheliumand trabecular meshwork in maintaining whatis a remarkably constant intraocular pressurethroughout life are not fully understood. Itwould appear that the production of aqueous isan active secretion, whereas the drainage ismore passive, although changing the tone of theciliary muscle can alter the rate of drainage. Innormal subjects, the intraocular pressure doesnot differ in the two eyes by more than about 3 mmHg. Wider differences can lead one tosuspect early glaucoma, especially if there is afamily history of the disease. The normalintraocular pressure undergoes a diurnal varia-tion, being highest in the early morning andgradually falling during the first half of the day.This diurnal change could become exaggeratedas the first sign of glaucoma.
Measurement of Intraocular PressureThe gold-standard method of intraocular pres-sure measurement is Goldmann applanationtonometry. The Goldmann tonometer is sup-plied as an accessory to the slit-lamp micro-scope. The principle of applanation is as follows:when two balloons are pushed together so thatthe interface is a flat surface, the pressure withinthe two balloons must be equal. By the sameargument, when a fixed flat surface is pressedagainst a spherical surface, such as the cornea,at the point at which the spherical surface isexactly flattened, the intraocular pressure isequal to the pressure being applied. The app-lanation head is a small Perspex rod with aflattened end, which is fitted to a moveable arm.The tension applied to the moveable arm can bemeasured directly from a dial on the side of theinstrument. The observer looks through the rodusing the microscope of the slit-lamp, and thepoint at which exact flattening occurs can thusbe gauged. For applanation tonometry, thepatient is seated at the slit-lamp and not lyingdown but it is still necessary to instill a drop oflocal anaesthetic beforehand. Because the
measurement of the intraocular pressure is sucha basic requirement in any eye clinic, attemptshave been made to introduce even more rapidand efficient devices. Perhaps the most ingen-ious to date is the tonometer, which measuresthe indentation of the cornea in response to apuff of air by a photoelectric method. This air-puff tonometer is less accurate than applan-ation, but it is useful for screening, althoughabnormal results should be confirmed by Goldmann tonometry.
Clinical Types of GlaucomaIt has been mentioned above that the word“glaucoma” refers to a group of diseases. Forclinical purposes, these can be subdivided intofive types:
1. Primary open-angle glaucoma.2. Normal pressure glaucoma.3. Acute angle-closure glaucoma.4. Secondary glaucoma.5. Congenital glaucoma.
Primary Open-angle GlaucomaThe first important point to note about thisdisease is that it is common, occurring in about1% of the population over the age of 50 years.The second point is that the disease is inherited,and whereas the practice of screening the wholepopulation for the disease is problematic interms of finance, it is well worth screening thefamilies of patients with the disease if those overthe age of 40 years are selected. This leads to thethird point, which is that the incidence increaseswith age, being rare under the age of 40 years.This insidious, potentially blinding diseaseaffects those who are least likely to notice itsonset, and elderly patients with advancedchronic open-angle glaucoma are still seen fromtime to time in eye clinics.
Primary open-angle glaucoma occurs morecommonly in high myopes and diabetics;patients with Fuchs’ corneal endothelial dystro-phy and retinitis pigmentosa also have a higherincidence. Glaucoma is commoner in differentracial groups. For example, individuals ofAfrican descent, especially those from WestAfrica and the Caribbean, carry a significantlygreater risk of glaucoma.
92 Common Eye Diseases and their Management

Pathogenesis and Natural History
Histologically, there are remarkably few changesto account for the raised intraocular pressure,at least in the early stages of the disease.Subsequently, degenerative changes have beendescribed in the juxtacanalicular trabecularmeshwork, with endothelial thickening andoedema in the lining of Schlemm’s canal. It hasbeen shown that in the majority of cases theproblem is one of inadequate drainage ratherthan excessive secretion of aqueous. In theuntreated patient, the chronically raised pres-sure leads to progressive damage to the eye andeventual blindness. The rate of progress of thedisease varies greatly from individual to indiv-idual. It is possible for gross visual loss to occurwithin months, but the process may take fiveyears. Younger eyes survive a raised pressurerather better than older eyes, which couldalready have circulatory problems. Few eyes canwithstand a pressure of 50 mmHg for more thana week or two or a pressure of 35 mmHg formore than a few months.
Primary open-angle glaucoma is nearlyalways bilateral, but often the disease begins inone eye, the other eye not becoming involvedimmediately. It is important to realise that theprogress of chronic glaucoma can be arrested bytreatment, but unfortunately, many ophthalmol-ogists experience the natural history of thedisease by seeing neglected cases.
Symptoms
Most patients with chronic glaucoma have no symptoms. That is to say, the disease is insidious and is only detected at a routine eyeexamination, either by an optometrist or ophthalmologist, before the patient notices any visual loss. Occasionally, younger patientsnotice a defect in their visual field but this isunusual. Unfortunately, the peripheral loss ofvisual field can pass unnoticed until it hasreached an advanced stage.
Signs
The three cardinal signs are:
1. Raised intraocular pressure.2. Cupping of the optic disc.3. Visual field loss.
The intraocular pressure creeps up graduallyto 30–35 mmHg, and it is this gradual rise thataccounts for the lack of symptoms. Such a risein intraocular pressure impairs the circulationof the optic disc, and the nerve fibres in thisregion become ischaemic. The combined effect of raised intraocular pressure and atrophy of nerve fibres results in gradual excavation ofthe physiological cup, and it is extremely usefulto be able to identify this effect of raisedintraocular pressure at an early stage. Figure12.1 shows an optic disc undergoing variousstages of pathological cupping. In the firstinstance, the central physiological cup becomesenlarged, with its long axis arranged vertically.Notching of the neuroretinal rim of the opticdisc tissue, especially in the inferotemporal andsuperotemporal region, is common. The edge ofthe optic disc cup corresponds to the bend inthe blood vessels as they cross the disc surface.In some eyes the area of pallor can correspondto the cup, while in others the cup is larger than
Glaucoma 93
Figure 12.1. The effect of glaucoma on the optic disc.

the area of pallor. It is particularly useful toobserve the way in which the vessels enter andleave the nerve head (Figure 12.2). A flame-shaped haemorrhage at the disc margin can beseen. Localised loss of retinal nerve fibres can be observed, especially with a red-free light.Diagnostic instrumentation, such as the GDxnerve fibre layer analyser, is capable of measur-ing the thickness of the retinal nerve fibre layerin microns, and offers an adjunctive objectivemeasure for diagnosing and monitoring glaucoma (Figure 12.3).
The changes in the visual field can bededuced from observing the disc and from con-sidering the arrangement of the nerve fibres inthe eye. If we gaze fixedly with one eye at a spoton the wall and then move a small piece of paperon the end of a paper clip, or even the end of ourindex finger, in such a manner as to explore ourperipheral field, it is soon possible to locate theblind spot. In the case of the right eye, this isfound slightly to the right of the point of fixationbecause it represents the projected position of
the optic nerve head in the right eye. The blindspot is rounded and about 8–12° lateral to andslightly below the level of fixation. It has alreadybeen mentioned that the glaucomatous disc isinitially excavated above and below so that thepatient with early glaucoma has a blank area inthe visual field extending in an arcuate mannerfrom the blind spot above and below fixation.This typical pattern of field loss is known as thearcuate scotoma (Figure 12.4). If the glaucomaremains uncontrolled, this scotoma extendsperipherally and centrally. It can be seen thateven at this stage the central part of the fieldcould be well preserved and the patient can stillbe able to read the smallest letters on the Snellentest chart. If the field loss is allowed to progressfurther, the patient becomes blind.
94 Common Eye Diseases and their Management
Figure 12.2. a Glaucomatous cupping of the disc early cupping;b advanced cupping.
Figure 12.3. GDx nerve fibre scan result.
Figure 12.4. Superior arcuate visual field defect, right eye.
a
b

Treatment
For many years, the mainstay of treatment forprimary open-angle glaucoma has been the useof miotic drops. The miotic of choice was pilocarpine, starting with a 1% solution andincreasing to 4% if needed. Subsequently, beta-blockers, for example, timolol, levubunolol(Betagan) and betaxolol (Betoptic) replacedpilocarpine, and now prostaglandin analogues,for example, latanoprost (Xalatan) have largelyreplaced beta-blockers as first-line medications(Table 12.1). In practice, these medications areoften used in combination.
Pilocarpine itself is effective in reducingintraocular pressure. After about half an hourfrom the moment of instillation, the pupilbecomes small and the patient experiencesdimming of the vision, aching over the eyebrowand a spasm of accommodation, which blurs thedistance vision. At the same time, the intra-ocular pressure in the majority of fresh cases ofglaucoma falls to within the normal range.After about 4 h, the intraocular pressure beginsto rise again and the side effects wear off. This,of course, means that a further drop of pilo-carpine must be instilled if good control is to becontinued. It is here that we find the mostdifficult problem of treatment. Human nature issuch that drops are rarely instilled four timesdaily on a regular basis, although patients are
genuinely anxious to preserve their eyesight.Compliance with glaucoma medication is amajor problem when medications are takenmore than once daily, and is a relativelycommon reason for disease progression.
Timolol and other beta-blockers are effectiveover a 12-h period and need to be instilled onlytwice daily. As an ocular hypotensive agent,these are probably not quite as effective as pilo-carpine, but many cases of chronic glaucoma arenow satisfactorily controlled by them and furthermore, the drug may be used in combin-ation with pilocarpine. Beta-blockers have thefurther advantage that they do not cause anymiosis. The main side effects of beta-blockersare bronchospasm, reduced cardiac contrac-tility and bradycardia. They are, therefore,contraindicated in patients with chronic obs-tructive airway disease, heart block, hypo-tension and bradycardia.
The cholinergic drugs (such as pilocarpine)and the anticholinesterase drugs (such asechothiopate iodide) act by increasing the rateof outflow of aqueous, whereas timolol isthought to inhibit the production of aqueous.Adrenaline drops also have the effect of reduc-ing aqueous production and they have been inuse for some years as a supplement to pilo-carpine. However, their effect is not powerfuland they tend to cause chronic dilatation ofthe conjunctival vessels in some patients, as well
Glaucoma 95
Table 12.1. Topical glaucoma medication.
Drug type Examples Mechanism of action
ß-Blockers Timolol Reduce aqueous productionBetaxololLevubunololCarteolol
Cholinergics Parasympathomimetics: Increase aqueous outflow throughPilocarpine trabecular meshwork
Anticholinesterases:Phospholine iodide
Adrenergic agonists Adrenaline and prodrug Decrease aqueous production and(Dipivefrine) increase uveoscleral outflow
a2-Agonist Brimonidine
Carbonic anhydrase Dorzolamide Reduce aqueous productioninhibitors
Prostaglandins Latanoprost Increased uveoscleral outflow(prostaglandin 2a)
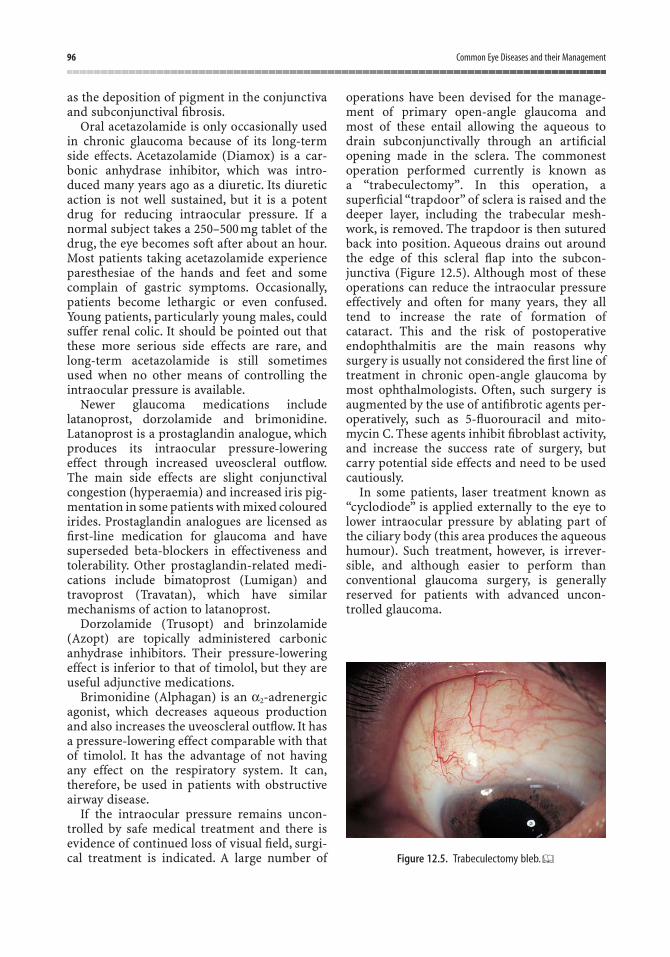
as the deposition of pigment in the conjunctivaand subconjunctival fibrosis.
Oral acetazolamide is only occasionally usedin chronic glaucoma because of its long-termside effects. Acetazolamide (Diamox) is a car-bonic anhydrase inhibitor, which was intro-duced many years ago as a diuretic. Its diureticaction is not well sustained, but it is a potentdrug for reducing intraocular pressure. If anormal subject takes a 250–500 mg tablet of thedrug, the eye becomes soft after about an hour.Most patients taking acetazolamide experienceparesthesiae of the hands and feet and somecomplain of gastric symptoms. Occasionally,patients become lethargic or even confused.Young patients, particularly young males, couldsuffer renal colic. It should be pointed out thatthese more serious side effects are rare, andlong-term acetazolamide is still sometimes used when no other means of controlling theintraocular pressure is available.
Newer glaucoma medications includelatanoprost, dorzolamide and brimonidine.Latanoprost is a prostaglandin analogue, whichproduces its intraocular pressure-loweringeffect through increased uveoscleral outflow.The main side effects are slight conjunctival congestion (hyperaemia) and increased iris pig-mentation in some patients with mixed colouredirides. Prostaglandin analogues are licensed asfirst-line medication for glaucoma and havesuperseded beta-blockers in effectiveness andtolerability. Other prostaglandin-related medi-cations include bimatoprost (Lumigan) andtravoprost (Travatan), which have similar mechanisms of action to latanoprost.
Dorzolamide (Trusopt) and brinzolamide(Azopt) are topically administered carbonicanhydrase inhibitors. Their pressure-loweringeffect is inferior to that of timolol, but they areuseful adjunctive medications.
Brimonidine (Alphagan) is an a2-adrenergicagonist, which decreases aqueous productionand also increases the uveoscleral outflow. It hasa pressure-lowering effect comparable with thatof timolol. It has the advantage of not havingany effect on the respiratory system. It can,therefore, be used in patients with obstructiveairway disease.
If the intraocular pressure remains uncon-trolled by safe medical treatment and there isevidence of continued loss of visual field, surgi-cal treatment is indicated. A large number of
operations have been devised for the manage-ment of primary open-angle glaucoma andmost of these entail allowing the aqueous todrain subconjunctivally through an artificialopening made in the sclera. The commonestoperation performed currently is known as a “trabeculectomy”. In this operation, asuperficial “trapdoor” of sclera is raised and thedeeper layer, including the trabecular mesh-work, is removed. The trapdoor is then suturedback into position. Aqueous drains out aroundthe edge of this scleral flap into the subcon-junctiva (Figure 12.5). Although most of theseoperations can reduce the intraocular pressureeffectively and often for many years, they alltend to increase the rate of formation ofcataract. This and the risk of postoperativeendophthalmitis are the main reasons whysurgery is usually not considered the first line oftreatment in chronic open-angle glaucoma bymost ophthalmologists. Often, such surgery isaugmented by the use of antifibrotic agents per-operatively, such as 5-fluorouracil and mito-mycin C. These agents inhibit fibroblast activity,and increase the success rate of surgery, butcarry potential side effects and need to be usedcautiously.
In some patients, laser treatment known as“cyclodiode” is applied externally to the eye tolower intraocular pressure by ablating part ofthe ciliary body (this area produces the aqueoushumour). Such treatment, however, is irrever-sible, and although easier to perform than conventional glaucoma surgery, is generallyreserved for patients with advanced uncon-trolled glaucoma.
96 Common Eye Diseases and their Management
Figure 12.5. Trabeculectomy bleb.

Normal-pressure GlaucomaThis condition is similar to primary open-angle glaucoma except that the intraocular pressure is within normal limits (i.e., 21 mmHgor less at the initial and subsequent visits). Thecondition is probably caused by low perfusionpressure at the optic nerve head so that thenerve head is susceptible to damage at normalintraocular pressure.
Certain conditions that can mimic normalpressure glaucoma include compressive lesionsof the optic nerve and chiasma, carotid ischemiaand congenital optic disc anomalies.
Treatment of normal-pressure glaucomaaims to reduce intraocular pressure to 12 mmHgor less.
Management
Most eye units now run special clinics fordealing with glaucoma patients. From what hasbeen said, it should be clear that patients withglaucoma require much time and attention.Initially, the nature of the disease must beexplained and patients must realise that thetreatment is to arrest the progress of the cond-ition and not to cure it. Furthermore, any visualloss that occurs is irretrievable, so that regularfollow-up visits are essential for checking theintraocular pressure and carefully assessing thevisual fields.
The initial treatment is a single topical agent – usually a prostaglandin analogue. Thesecond-line treatments of choice are beta-blockers, brimonidine or dorzolamide. Com-monly, patients with glaucoma require severaldifferent medications to control intraocularpressure effectively.
Increasingly, optometrists are providing specialist care for patients with glaucoma.Some optometrists work alongside hospital consultant-led teams, others work in the com-munity to “refine referrals” and reduce thenumber of false-positive referrals to a specialistglaucoma clinic.
Acute Angle-closure GlaucomaThis condition is less common than chronicopen-angle glaucoma, making up about 5% ofall cases of primary glaucoma. It is a much moredramatic condition than the chronic disease and
fits in more closely with the popular lay idea of“glaucoma”. It tends to affect a slightly youngerage group than chronic glaucoma and onlyoccurs in predisposed individuals. There is aparticular type of eye that is liable to developacute glaucoma: this is a small hypermetropiceye with a shallow anterior chamber. One rarelymeets a myope with acute glaucoma in Cau-casians (in Asian populations, however, angleclosure and myopia more often coexist).
Pathogenesis and Natural History
Eyes that are predisposed to develop closed-angle glaucoma generally have a shallow anter-ior chamber and are often hypermetropic. Thereis forward bowing of the iris, which is moreevident in these individuals, and the cornealdiameter is slightly smaller than in normal eyes.Another factor is the gradual, but slight, increasein size of the lens, which takes place with ageing.Raised intraocular pressure in angle closure iscaused by occlusion of the angle by the iris rootand it can be precipitated by dilating the pupil.An uncontrolled acute attack of glaucoma canlead to rapid and permanent loss of the sight ofthe affected eye. Although it is known that occa-sionally patients recover spontaneously fromsuch an attack, they could be left with chronicangle closure and a picture similar to that ofchronic open-angle glaucoma. About half thepatients with closed-angle glaucoma willdevelop a similar problem in the other eye ifsteps are not taken to prevent this, and it will beseen that prophylactic treatment for the othereye is now the rule.
Symptoms
The subacute attack. Here, it might be helpful toconsider a typical patient, who might be a maleor female, aged about 50 years. Such a patientwould have a moderate degree of hyper-metropia and rather a narrow gap between iris and cornea, as shown by the shallow anteriorchamber. During the autumn months, thispatient’s pupil might be noted to be slightlywider, as one might expect with the dimmer illu-mination, and one evening the pupil dilatessufficiently to allow the iris root to nudge acrossthe angle and obstruct the flow of aqueous.Immediately, the intraocular pressure risesacutely, perhaps to 30 mmHg or 40 mmHg andpain is felt over the eye. At the same time, the
Glaucoma 97

acute rise of pressure causes the cornea tobecome oedematous. Because it is evening, thepatient observes that streetlights when viewedthrough the oedematous cornea appear to havecoloured rings around them, as if they werebeing viewed through frosted glass. At thispoint, the patient retires to bed and on sleepingthe pupil becomes small and the intraocularpressure rise is relieved. After several of theseattacks, the patient might seek attention fromthe family doctor. Patients present as healthypeople with evening headaches associated withblurring of the vision and they are wearingmoderately thick convex lenses in their specta-cles. Subacute glaucoma is easily missed, partlybecause it is rare among the large number ofsufferers from headache. If attention is notsought at this stage or if the diagnosis is missed,one evening the acute attack develops.
The acute attack. After a number of subacuteattacks, an irreversible turn of events can occur.The iris root becomes congested, raising theintraocular pressure further and producingfurther congestion. The headache becomesmuch worse and the vision becomes seriouslyimpaired. The doctor, who might be called in thefollowing morning, is confronted with a patientwho is nauseated and vomiting and at first sight,an acute abdominal problem might be sus-pected, until the painful red eye should makethe diagnosis obvious. Sometimes acute glau-coma does not cause much pain or nausea and in these cases, the physical signs in the eyebecome especially important (Figure 12.6).
Signs
The most obvious physical sign is the semi-dilated fixed pupil. The iris and the constrictingsphincter muscle of the pupil are damaged bythe raised intraocular pressure. The pupil is not able to constrict and after a day or two theiris becomes depigmented, taking on the greyatrophic colour that gave glaucoma its name.Prompt and effective treatment should preventany damage to the iris. The eye is red and a pinkfrill of engorged deeper capillaries is seenaround the corneal margin; this important sign,as opposed to conjunctival inflammation, isknown as ciliary injection. Corneal oedema canusually be detected without optical aids byobserving the lack of luster in the eye and anyattempts to assess the hardness of the eye by
palpating it through the eyelids will elicitanother sign, that of tenderness of the globe.The visual acuity might be reduced to “handmovements” in a severe attack. There are tworather subtle signs that often persist perm-anently after the acute attack has been resolved.The first is the presence of a white, irregularmicroscopic deposit just deep to the anteriorsurface of the lens, and the second is the pres-ence of whorl atrophy in the iris. The pattern ofthe iris becomes twisted as if the sphincter hasbeen rotated slightly. Both these signs canprovide useful evidence of a previous attack thathas resolved spontaneously.
Measurement of the intraocular pressure atthis point could reveal a reading of 70 mmHg ormore. Gentle palpation of the globe is usuallyenough to confirm that the eye has the consis-tency of a brick, especially when the pressuresof the two eyes are compared. It should berealised that digital palpation of the globe canbe misleading and the method cannot be usedto detect smaller rises in intraocular pressurewith any degree of reliability (Table 12.2).
Examination of the other eye will reveal ashallow anterior chamber. Shining a focused
98 Common Eye Diseases and their Management
Figure 12.6. Acute angle-closure glaucoma.
Table 12.2. Signs of acute glaucoma.
• Corneal oedema with resulting poor visual acuity• Shallow anterior chamber• Ciliary injection• Semidilated oval pupil (caused by iris ischaemia)• Tenderness of globe• Hard eye

beam of light obliquely through the cornea andnoting the width of the gap between where thelight strikes the cornea and where it strikes the iris can assess the depth of the anteriorchamber. After inspecting a few normal eyes inthis way, the observer can soon learn when ananterior chamber is abnormally shallow. Thisfacility is important to anyone who intends toinstill mydriatic drops into an eye. A shallowanterior chamber does not contraindicatemydriatic drops but it does indicate the need forextreme caution and care that the pupil is after-wards restored to its normal size. The angle ofthe anterior chamber itself is not exposed todirect inspection and it can only be seen througha gonioscope (Figure 12.7). This instrument is acontact lens with a mirror mounted on it andthrough it, the width of the angle can be esti-mated. If the angle is open, the various struc-tures adjacent to the iris root and inner surfaceof the peripheral cornea can be identified.Gonioscopy forms a routine part of the exam-ination of any patient with glaucoma, althoughin acute narrow-angle glaucoma the presence ofa closed angle can often be presumed by thepresence of the other physical signs.Where thereis any doubt, it might be necessary to apply adrop of hypertonic glycerol to the cornea to clearthe oedema before applying the gonioscope.
The sooner closed-angle glaucoma is diag-nosed and treated, the better are the results oftreatment. Unfortunately, it is in the early sub-acute stage of the disease that the diagnosis canbe difficult. A number of provocative tests havebeen devised for the patient who presents withsuspicious symptoms but a normal intraocularpressure. The simplest test is the “dark roomtest”. The patient’s intraocular pressure is meas-
ured before he or she is seated in a darkenedroom for half an hour. The intraocular pressureis again measured immediately after this, and arise in pressure of more than 5 mmHg can betaken to be significant. Certain drugs can havea similar effect by having a mildly mydriaticaction when taken by mouth. The pheno-thiazines have been incriminated in this respect.Of course, such drugs will have no adverse effecton patients who have already been treated andidentified as cases of narrow- or closed-angleglaucoma. Only in unsuspected cases of sub-acute narrow-angle glaucoma is there a real riskof precipitating an acute attack.
Treatment
Acute narrow-angle glaucoma is a surgicalproblem and any patient suffering from the con-dition requires urgent admission to hospital. Todo less than this is to undertreat the conditionand run the risk of producing chronic narrow-angle glaucoma. On admission, the affected eyeis treated with intensive miotic drops. A typicalregimen would be the application of pilocarpine4% every minute for 5 min, then every 5 min for an hour, followed by instillation every hour.This treatment is supported by an injection of acetazolamide. If the renal function is unim-paired, acetazolamide can be given intra-venously (usually 500 mg) followed by an oraldose of 250 mg four times a day. Topical beta-blockers and/or alpha-agonists, for example apraclonidine (Iopidine), and reduction ofinflammation and iris congestion by topicalsteroids can help achieve a quicker lowering of intraocular pressure. In many cases, thesemeasures relieve the acute attack within hours.However, some patients can require an intra-venous infusion of mannitol.During this period,the patient is kept in bed and analgesics are givenif required. It is important that the other eye isalso treated with pilocarpine 2% four times a dayin order to prevent a second disaster.
Once the intraocular pressure has been con-trolled, the cure is maintained by performing aperipheral iridotomy or iridectomy. This allowsthe bulging iris bombe to sink backwards like apunctured ship’s sail and is a sure means of pre-venting further acute attacks. Usually, the felloweye is at risk of a similar problem and is laseredat the same time. In some patients, the angle ofthe anterior chamber remains partially occluded
Glaucoma 99
Figure 12.7. Preparing for gonioscopy.

by peripheral adhesions from the iris. In thesecases, a simple peripheral iridectomy might notbe adequate and it might be necessary to carryout a drainage operation, such as a trabeculec-tomy. Most patients with acute narrow-angleglaucoma are cured by surgery, although a smallproportion develops cataracts in later years. The prognosis in adequately treated narrow-angleglaucoma is, therefore, good, but in the absenceof treatment the result is disastrous.
The treatment of narrow-angle glaucoma hasundergone a small revolution over the past fewyears. This is because a new generation of lasershas appeared, which make it possible to perfor-ate the iris quite simply. The yttrium–aluminum–garnet (YAG) laser has replaced sur-gical iridectomy in most cases. A special contactlens is used to focus the laser on the peripheraliris, and one or two full-thickness openings inthe peripheral iris are created. Following suchlaser treatment, topical steroids and pupildilatation are given to minimise the effects ofuveitis. Occasionally, trabeculectomy surgery isperformed if intraocular pressures remain per-sistently high despite other treatments.
Secondary GlaucomaThe intraocular pressure can become raised asthe result of a number of different diseaseprocesses in the eye quite apart from the causes of primary glaucoma, which have justbeen described.
Secondary to Vascular Disease in the Eye
Central retinal vein thrombosis. This is acommon cause of sudden blurring of the visionof one eye in the elderly. The retinal veins canbe seen to be dilated and surrounded by haem-orrhages. In some cases, recovery is marred bya rise in intraocular pressure, which typicallyappears approximately three months after theonset of the condition. The prompt appearanceof this painful complication has given it thename of “hundred-day glaucoma”. This type ofglaucoma is usually difficult to control and evensurgical measures can prove ineffective. Atypical feature is the appearance of a vascularmembrane over the anterior surface of the iris and sometimes the angle of the anteriorchamber. This vascularised tissue lends a
pinkish hue to the iris and is termed rubeosisiridis. Patients with a central retinal vein throm-bosis followed by secondary glaucoma haveanother problem because there is a recognisedassociation between chronic open-angle glau-coma and central retinal vein occlusion. Thismeans that some patients who present with anoccluded vein are found to have chronic glau-coma in the other eye.
Diabetes. Patients with severe diabeticretinopathy can also develop rubeosis iridis andsecondary glaucoma. The vascular occlusive fea-tures of diabetic eye disease give it many resem-blances to central retinal vein thrombosis andthe secondary glaucoma that develops is alsoresistant to medical treatment. Panretinal laser photocoagulation, when applied early,causes regression of the rubeosis. The ultimateoutcome is sometimes a blind and painful eye,which has to be removed.
Secondary to Uveitis
During an attack of acute iridocyclitis theintraocular pressure is often below normalbecause the production of aqueous by the ciliarybody is reduced. When the normal productionof aqueous is resumed, it can induce a rise inpressure because the outflow channels have beenobstructed by inflammatory exudate. This typeof secondary glaucoma responds to vigoroustreatment of the iridocyclitis, and here it isessential to dilate and not constrict the pupil andto apply steroid treatment. Acetazolamide andtopical beta-blockers, for example timolol and levubunolol, might also be required. The type ofsecondary glaucoma that develops after the iridocyclitis of herpes zoster infections can beparticularly insidious. The intraocular pressurecan remain high without obvious pain and withrelatively slight inflammatory changes in theeye. Secondary glaucoma usually responds wellto treatment and once the underlying inflam-mation has subsided, the eye returns to normal.
In iridocyclitis, glaucoma can also be causedby pupil block (inability of aqueous to pass fromthe posterior to anterior chamber) because ofposterior synechiae (adhesions between the irisand lens). Treatment is YAG laser iridotomy.
Secondary to Tumours
Malignant melanoma of the choroid andretinoblastoma can cause glaucoma. The raised
100 Common Eye Diseases and their Management
intraocular pressure can be an important diag-nostic feature when a suspected lesion is seen inthe fundus.When a patient presents with a blindglaucomatous eye, the possibility of malignancymust always be in the back of one’s mind.
Secondary to Trauma
Trauma can precipitate a rise in intraocularpressure in a number of different ways. Some-times, especially in children, bleeding can occurinto the anterior chamber after a contusioninjury. This can seriously obstruct the flow ofaqueous both through the pupil and into theangle. Such an episode of bleeding can occur onthe second or third day after the injury, turninga slight event into a very serious problem. Onother occasions, a contusion injury might causesplitting or recession of the angle, which is associated with glaucoma. The iridocyclitis that follows perforating injuries tends to becomplicated by glaucoma and the ophthalmol-ogist must be constantly aware of such a complication.
Drug-induced Glaucoma
Local and systemic steroids can cause a rise inintraocular pressure and this is more likely tooccur in patients with a family history of glau-coma. Steroid glaucoma is a well-recognisedphenomenon and “steroid responders” can beidentified by measuring the intraocular pressurebefore and after instilling a drop of steroid. Theless potent steroids, hydrocortisone and pred-nisolone, are less likely to cause this problem and other steroids have been manufactured that have less effect on intraocular pressure, but the anti-inflammatory strength is significantlyweaker. The use of systemic steroids can be associated with glaucoma; asthmatics who usesteroid inhalers frequently are at a significantlygreater risk of developing glaucoma.
The possibility of inducing an attack of acuteglaucoma by drugs has already been mentioned.
Secondary to Abnormalities in the Lens
A cataractous lens can become hypermature and swell up, pushing the iris diaphragmforward and obstructing the angle of the anter-ior chamber.This is referred to as phacomorphic
glaucoma. Removing the lens relieves the situa-tion. Phacolytic glaucoma occurs when a maturecataract causes a type of uveitis. This is thoughtto result from leakage of lens proteins throughthe lens capsule.A dislocated or subluxated lens,either the result of trauma or as a congenitalabnormality, can be associated with a rise inintraocular pressure.
Congenital or DevelopmentalGlaucomaThese glaucomas occur in eyes in which ananomaly present at birth produces an intra-ocular pressure rise.
This type of glaucoma is extremely rare andit is often, though not always, inherited. Thismeans that the affected child might be broughtto the ophthalmologist by the parents becausethey are aware of the condition in the family.Children could be born with raised intraocularpressure and for these cases, the prognosis is notso good as in those where the pressure rise doesnot occur until after the first few months of life.
In primary developmental glaucoma, theglaucoma is caused by a defective developmentof the angle of the anterior chamber, andgonioscopy shows that the normal features ofthe angle are obscured by a pinkish membrane.Raised intraocular pressure in infancy has adramatic effect because it causes enlargement of the globe. This can best be observed bynoting an increase in the corneal diameter. Theenlarged eye has given the condition the nameof buphthalmos or “bull’s eye” (Figure 12.8).
Glaucoma 101
Figure 12.8. Congenital glaucoma: note the enlarged leftcornea (with acknowledgement to Mr R. Gregson).

Other important signs are photophobia andcorneal oedema. The diagnosis is confirmed by an examination under anaesthesia, whichincludes measuring the corneal diameters andthe intraocular pressure. Surgical treatment isnearly always required and this involves passinga fine knife through the peripheral cornea sothat the point reaches the opposite angle ofthe anterior chamber. Once in the angle, it is
moved gently to and fro to open up the em-bryonic tissue that covers the trabecular mesh-work (goniotomy). The other (or secondary)developmental glaucomas include the rubellasyndrome, aniridia, mesodermal dysgenesis,Peter’s anomaly and the phacomatoses, wherethe intraocular pressure rise is associated with other ocular and systemic developmentalanomalies.
102 Common Eye Diseases and their Management
Detachment of the retina signifies an inwardseparation of the sensory part of the retina fromthe retinal pigment epithelium (RPE). There isan accumulation of fluid in the space betweenthe neural retina and the RPE known as subreti-nal fluid (Figure 13.1). The retina bulges inwardslike the collapsed bladder of a football. Oncedetached, the retina can no longer function and,in humans, it tends to remain detached, unlesstreatment is available.
Although the condition is relatively rare inthe general population, it is important forseveral reasons. First, it is a blinding conditionthat can be treated effectively and often dra-matically by surgery. Second, retinal detach-ment can on occasions be the first sign ofmalignant disease in the eye. Finally, nowadaysthe condition can often be prevented by pro-phylaxis in predisposed eyes.
IncidenceRetinal detachment is rare in the general pop-ulation but an eye unit serving a population of500,000 might expect to be looking after threeor four cases a week. It can be seen, therefore,that a doctor in general practice might see a caseonce in every two or three years, especially if weconsider that some retinal detachment patientsgo directly to eye casualty departments withoutseeking nonspecialist advice. Although childrenare sometimes affected, the incidence increaseswith age and reaches a maximum in the 50–60-
year age group. There is a smaller peak in themid-20s to 30s owing to traumatic detachmentsin young males.
Certain groups of people are especially liableto develop detachment of the retina: severelyshortsighted patients have been shown to havean incidence as high as 3.5% and about 1% of aphakic patients (see Chapter 11) havedetachments.
In just under one-quarter of cases,if there is nointervention, the other eye becomes affected at a later date. This means that the sound eye mustbe examined with great care in every instance.
PathogenesisThere is an embryological explanation forretinal detachment in that the separating layersopen up a potential space that existed during theearly development of the eye, as described pre-viously (Chapter 2). The inner lining of the eyedevelops as two layers. In its earliest stages ofdevelopment, the eye is seen as an outgrowth of the forebrain, the optic vesicle, the cavity ofwhich is continuous with that of the forebrain.The vesicle becomes invaginated to form theoptic cup, and the two-layered cup becomes thetwo-layered lining of the adult eye. Anteriorly inthe eye, the two layers line the inner surface ofthe iris and ciliary body. Posterior to the ciliarybody, the outer of the two layers remains as asingle layer of pigmented cells, known as the
13Retinal Detachment
103

pigment epithelium. The inner of the two layersbecomes many cells thick and develops into thesensory retina. In the adult, the sensory retina isclosely linked, both physically and metabol-ically, with the RPE and, in particular, the production of visual pigment relies on this juxtaposition. When the retina becomesdetached and the sensory retina is separatedfrom the RPE, the retina can no longer functionand the sight is lost in the detached area. BothRPE and sensory retina are included in the term“retina” and in this sense “retinal detachment”is a misnomer.
The retina receives its nourishment from twosources: the inner half deriving its blood supplyfrom the central retinal artery, and the outer halffrom the choroid. The important foveal regionis supplied mainly by the choroid. When theretina is detached, the central retinal arteryremains intact and continues to supply itbecause it is also detached with it. The outer half of the retina is deprived of nourishment,being separated from the RPE and choroid.Eventually degenerative changes appear, thefovea being affected at an early stage. It is inter-esting that after surgical replacement the retinaregains much of its function during the first fewdays but further recovery can occur over as longa period as one or even two years.
ClassificationDetachment of the retina can be classified asfollows: rhegmatogenous retinal detachment,
tractional retinal detachment, and exudativeretinal detachment.
Rhegmatogenous Retinal DetachmentThis is the most common form of retinaldetachment, caused by the recruitment of fluidfrom the vitreous cavity to the subretinal spacevia a full-thickness discontinuity (a retinal“break”) in the sensory retina.
Retinal “breaks” can be further subdividedinto “tears”, which are secondary to dynamicvitreoretinal traction, and “holes”, which are theresult of focal retinal degeneration (see below).
Tractional Retinal DetachmentThis form of retinal detachment develops as aresult of tractional forces within the vitreous gelpulling on the retina, causing the retina to be tented up from the RPE. The pure form oftractional retinal detachment is different fromrhegmatogenous retinal detachment in thatthere are no retinal breaks. Examples of trac-tional retinal detachment include proliferativediabetic retinopathy and vitreomacular tractionsyndrome.
Exudative Retinal DetachmentThis group of retinal detachments also occurs inthe absence of retinal breaks. The fluid gainsaccess to the subretinal space through anabnormal choroidal circulation (e.g., from achoroidal malignant melanoma) or, rarely, sec-ondary to inflammation of the RPE or deeperlayers of the eye (e.g., scleritis).
Rhegmatogenous Retinal DetachmentThe Presence of Breaks in Retinal DetachmentIt was noticed as long ago as 1853, only a shorttime after the invention of the ophthalmoscope,that many detached retinae have minute full-thickness discontinuities (breaks) in them, but it was not until the 1920s that the full signific-ance of these breaks as the basic cause of thedetachment became realised. The breaks can
104 Common Eye Diseases and their Management
Figure 13.1. Histology of retinal detachment showing the location of subretinal fluid.This eye has an underlying choroidalmelanoma.

be single or multiple and are more commonlysituated in the anterior or more peripheral partof the retina. In order to understand how thesebreaks occur, it is necessary to understand something of retinal degeneration and vitreouschanges.
Retinal DegenerationWhen examining the peripheral retina of other-wise normal subjects, it is surprising to find thatfrom time to time there are quite striking degen-erative changes. Perhaps this is not so surprisingwhen one considers that the retinal arteries areend arteries and these changes occur in theperipheral parts of the retina supplied by thedistal part of the circulation. Peripheral retinaldegenerations are more commonly seen inmyopic eyes, especially in association withMarfan’s and Ehlers–Danlos syndromes andStickler’s disease (see reading list).
Different types of degeneration have beendescribed and named and certain types arerecognised as being the precursors to formationof retinal breaks. The most important degener-ations are lattice degeneration and retinal tufts.Lattice degenerations consist of localised areasof thinning in the peripheral retina. Progressivethinning of the retina within areas of latticedegeneration can eventually lead to formationof retinal “holes”.
In addition, both lattice degenerations andretinal tufts also represent areas with abnor-mally strong adhesions between the vitreousand the retina. The presence of exaggeratedvitreoretinal adhesions can result in the for-mation of retinal “tears” within areas of latticedegeneration and retinal tufts during posteriorvitreous detachment (see below).
The VitreousThe normal vitreous is a clear gel, which occu-pies most of the inside of the eye. Its consistencyis similar to that of raw white of egg and, beinga gel, it takes up water and salts. It is made up ofa meshwork of collagen fibres whose interspacesare filled with molecules of hyaluronic acid. Thevitreous is adherent to the retina at the oraserrata (junction of ciliary body and retina) andaround the optic disc and macula. If we moveour eyes, the vitreous moves, and, beingrestrained by its attachment, swings back to its
original position again. The vitreous is usuallyperfectly transparent but most people becomeaware of small particles of cellular debris, whichcan be observed against a clear backgroundsuch as a blue sky or an X-ray screen (vitreousfloaters). These particles can be seen to moveslowly with eye movement and appear to havemomentum, just as one would expect if one con-siders the way the vitreous moves.
Posterior Vitreous DetachmentVitreous floaters are commonplace and tend toincrease in number as the years pass. But the vit-reous undergoes a more dramatic change withage. Often in the late 50s, it becomes more fluidand collapses from above, separating from itsnormal position against the retina and event-ually lying as a contracted mobile gel in theinferior and anterior part of the cavity of theglobe. The rest of the globe is occupied by clearfluid. This then is the process known as poste-rior vitreous detachment (PVD).
When this happens, the patient might com-plain of something floating in front of the visionand also the appearance of flashing lights. Thisis because the mobile shrunken vitreous some-times causes slight traction on the retina. As arule, the same symptoms are then experiencedsubsequently in the other eye. On the otherhand, it is also common to find a detached vit-reous in an elderly person’s eye in the absenceof any symptoms.
Retinal Breaks FormationIn the majority of eyes the vitreous separates“cleanly” from the retina during PVD. Such“uncomplicated” PVD is common and is usuallyof no pathological significance. Unfortunately,on rare occasions, the collapsing vitreous causesa retinal “tear” to form at a point of abnormallystrong adhesion between vitreous and retina, forexample within an area of lattice degeneration orretinal tufts. There might even be an associatedvitreous haemorrhage, when the PVD causes theavulsion of a peripheral retinal blood vessel.
Mechanism of RhegmatogenousRetinal DetachmentOnce a retinal tear forms as a result of abnor-mal vitreous traction following PVD, the fluid
Retinal Detachment 105

from within the vitreous cavity can gain accessto the subretinal space through the retinal tear.The progressive accumulation of fluid in thesubretinal space eventually causes the retina toseparate from the underlying RPE, similar towallpaper being stripped off a wall. This inwardseparation of the retina from the RPE throughthe recruitment of fluid via a retinal break is the basis for “rhegmatogenous” retinal detach-ment, which is the most common form ofretinal detachment.
Rhegmatogenous RetinalDetachment Associated with TraumaMost rhegmatogenous retinal detachmentsoccur as a result of spontaneous PVD-inducedretinal breaks. However, retinal tears can alsooccur as a result of trauma. A perforating injuryof the eye can produce a tear at any point in theretina, but contusion injuries commonlyproduce tears in the extreme retinal peripheryand in the lower temporal quadrant or the super-ior nasal quadrant. This is because the lowertemporal quadrant of the globe is most exposedto injury from a flying missile, such as a squashball. The threatened eye makes an upward movement as the lids attempt to close. Tears ofthis kind often take the form of a dialysis, theretina being torn away in an arc from the oraserrata.Warning symptoms in these patients areusually masked by the symptoms of the originalinjury and they tend to present some months, oroccasionally years, after the original injury withthe symptoms of a retinal detachment. This isunfortunate because the tear can be treated if itis located before the detachment occurs.
Signs and Symptoms of Retinal Tear and Retinal DetachmentLet us now consider a typical patient, possibly amyope in the mid-50s, either male or female,who suddenly experiences the symptoms of“flashes and floaters”, sometimes spontaneouslyor sometimes after making a sudden head move-ment. Proper interpretation of such symptoms
can save sight and they will, therefore, be con-sidered in more detail.
Flashes (“Photopsiae”)When questioned, the patient usually says thatthese are probably present all the time but areonly noticeable in the dark. They seem to beespecially apparent before going to sleep atnight. The flashes are usually seen in the periph-eral part of the visual field. They must be dis-tinguished from the flashes seen in migraine,which are quite different and are usually fol-lowed by headache. The migrainous subjecttends to see zig-zag lines, which spread out fromthe centre of the field and last for about 10 min.Elderly patients with a defective vertebrobasilarcirculation may describe another type of pho-topsia in which the flashing lights tend to occuronly with neck movements or after bending.
FloatersIt has already been explained that black spotsfloating in front of the vision are commonplacebut often called to our attention by anxiouspatients. When the spots are large and appearsuddenly, they can be of pathologicalsignificance. For some reason, patients oftenrefer to them as tadpoles or frogspawn, or evena spider’s web. It is the combination of thesesymptoms with flashing lights that makes it important.
Flashes and floaters appear because the vit-reous has tugged on the retina, producing thesensation of light, and often when the tearappears there is a slight bleeding into the vit-reous, causing the black spots. When clear-cutsymptoms of this kind appear, they must not beoverlooked. The eyes must be examined fullyuntil the tear in the retina is found. Sometimes,a small tear in the retina is accompanied by alarge vitreous haemorrhage and thus suddenloss of vision.
ShadowOnce a retinal tear has appeared, the patientmight seek medical attention, and effectivetreatment of the tear can ensue. Unfortunately,some patients do not seek attention, or, if theydo, the symptoms might be disregarded. Indeed,in time the symptoms might become less, but
106 Common Eye Diseases and their Management
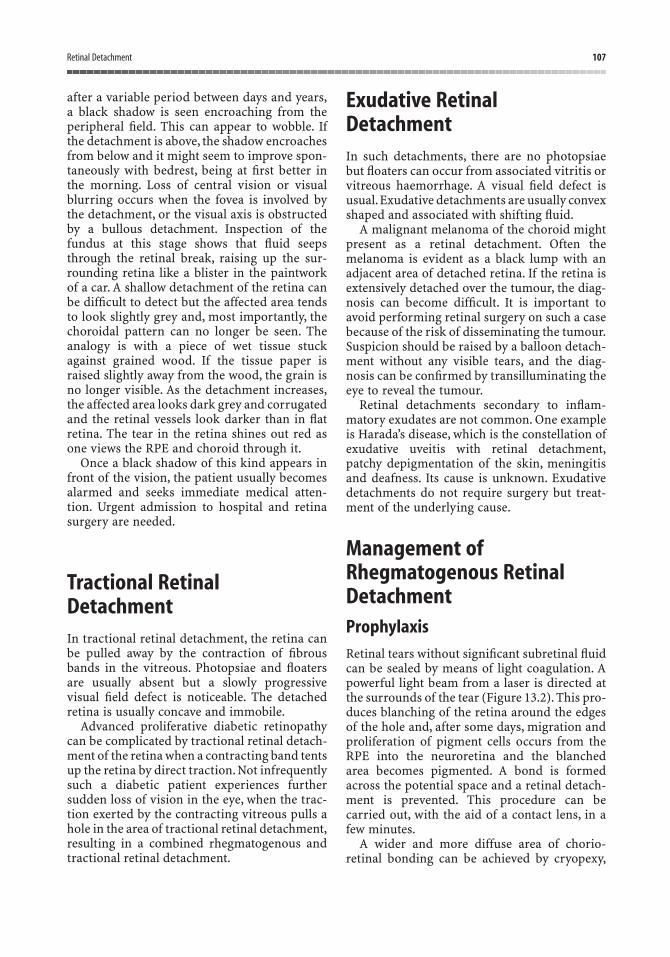
after a variable period between days and years,a black shadow is seen encroaching from theperipheral field. This can appear to wobble. Ifthe detachment is above, the shadow encroachesfrom below and it might seem to improve spon-taneously with bedrest, being at first better inthe morning. Loss of central vision or visualblurring occurs when the fovea is involved bythe detachment, or the visual axis is obstructedby a bullous detachment. Inspection of thefundus at this stage shows that fluid seepsthrough the retinal break, raising up the sur-rounding retina like a blister in the paintworkof a car. A shallow detachment of the retina canbe difficult to detect but the affected area tendsto look slightly grey and, most importantly, thechoroidal pattern can no longer be seen. Theanalogy is with a piece of wet tissue stuckagainst grained wood. If the tissue paper israised slightly away from the wood, the grain isno longer visible. As the detachment increases,the affected area looks dark grey and corrugatedand the retinal vessels look darker than in flatretina. The tear in the retina shines out red asone views the RPE and choroid through it.
Once a black shadow of this kind appears infront of the vision, the patient usually becomesalarmed and seeks immediate medical atten-tion. Urgent admission to hospital and retinasurgery are needed.
Tractional RetinalDetachmentIn tractional retinal detachment, the retina canbe pulled away by the contraction of fibrousbands in the vitreous. Photopsiae and floatersare usually absent but a slowly progressivevisual field defect is noticeable. The detachedretina is usually concave and immobile.
Advanced proliferative diabetic retinopathycan be complicated by tractional retinal detach-ment of the retina when a contracting band tentsup the retina by direct traction. Not infrequentlysuch a diabetic patient experiences furthersudden loss of vision in the eye, when the trac-tion exerted by the contracting vitreous pulls ahole in the area of tractional retinal detachment,resulting in a combined rhegmatogenous andtractional retinal detachment.
Exudative RetinalDetachmentIn such detachments, there are no photopsiaebut floaters can occur from associated vitritis orvitreous haemorrhage. A visual field defect isusual.Exudative detachments are usually convexshaped and associated with shifting fluid.
A malignant melanoma of the choroid mightpresent as a retinal detachment. Often themelanoma is evident as a black lump with anadjacent area of detached retina. If the retina isextensively detached over the tumour, the diag-nosis can become difficult. It is important toavoid performing retinal surgery on such a casebecause of the risk of disseminating the tumour.Suspicion should be raised by a balloon detach-ment without any visible tears, and the diag-nosis can be confirmed by transilluminating theeye to reveal the tumour.
Retinal detachments secondary to inflam-matory exudates are not common. One exampleis Harada’s disease, which is the constellation ofexudative uveitis with retinal detachment,patchy depigmentation of the skin, meningitisand deafness. Its cause is unknown. Exudativedetachments do not require surgery but treat-ment of the underlying cause.
Management ofRhegmatogenous RetinalDetachmentProphylaxisRetinal tears without significant subretinal fluidcan be sealed by means of light coagulation. Apowerful light beam from a laser is directed atthe surrounds of the tear (Figure 13.2). This pro-duces blanching of the retina around the edgesof the hole and, after some days, migration andproliferation of pigment cells occurs from theRPE into the neuroretina and the blanched area becomes pigmented. A bond is formedacross the potential space and a retinal detach-ment is prevented. This procedure can becarried out, with the aid of a contact lens, in afew minutes.
A wider and more diffuse area of chorio-retinal bonding can be achieved by cryopexy,
Retinal Detachment 107
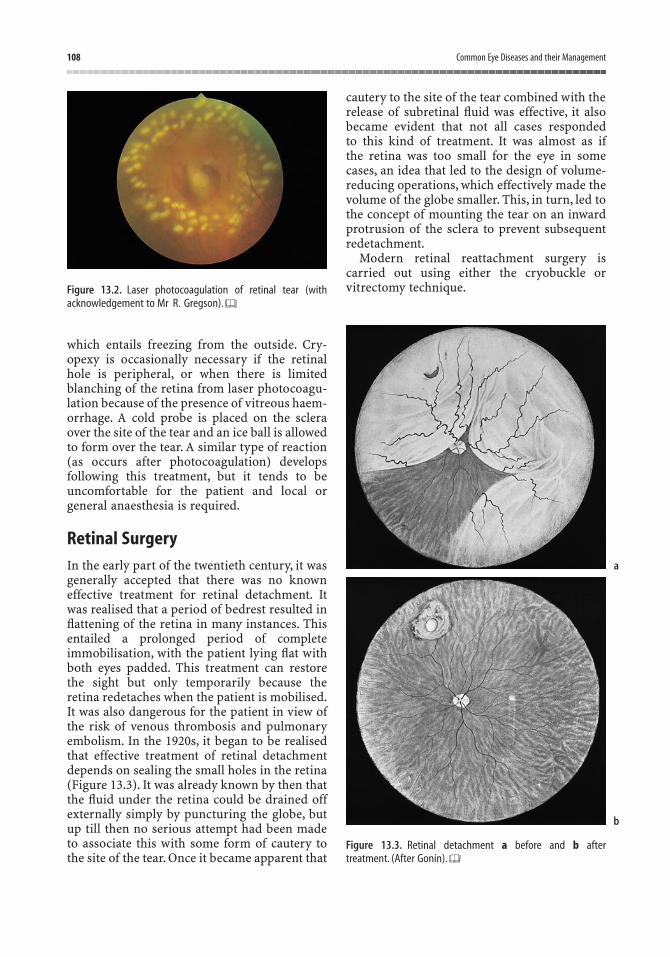
which entails freezing from the outside. Cry-opexy is occasionally necessary if the retinalhole is peripheral, or when there is limitedblanching of the retina from laser photocoagu-lation because of the presence of vitreous haem-orrhage. A cold probe is placed on the scleraover the site of the tear and an ice ball is allowedto form over the tear. A similar type of reaction(as occurs after photocoagulation) develops following this treatment, but it tends to beuncomfortable for the patient and local orgeneral anaesthesia is required.
Retinal SurgeryIn the early part of the twentieth century, it wasgenerally accepted that there was no knowneffective treatment for retinal detachment. Itwas realised that a period of bedrest resulted inflattening of the retina in many instances. Thisentailed a prolonged period of complete immobilisation, with the patient lying flat withboth eyes padded. This treatment can restorethe sight but only temporarily because theretina redetaches when the patient is mobilised.It was also dangerous for the patient in view ofthe risk of venous thrombosis and pulmonaryembolism. In the 1920s, it began to be realisedthat effective treatment of retinal detachmentdepends on sealing the small holes in the retina(Figure 13.3). It was already known by then thatthe fluid under the retina could be drained offexternally simply by puncturing the globe, butup till then no serious attempt had been madeto associate this with some form of cautery tothe site of the tear. Once it became apparent that
cautery to the site of the tear combined with therelease of subretinal fluid was effective, it alsobecame evident that not all cases responded to this kind of treatment. It was almost as ifthe retina was too small for the eye in somecases, an idea that led to the design of volume-reducing operations, which effectively made thevolume of the globe smaller. This, in turn, led tothe concept of mounting the tear on an inwardprotrusion of the sclera to prevent subsequentredetachment.
Modern retinal reattachment surgery iscarried out using either the cryobuckle or vitrectomy technique.
108 Common Eye Diseases and their Management
Figure 13.2. Laser photocoagulation of retinal tear (withacknowledgement to Mr R. Gregson).
Figure 13.3. Retinal detachment a before and b after treatment. (After Gonin).
a
b
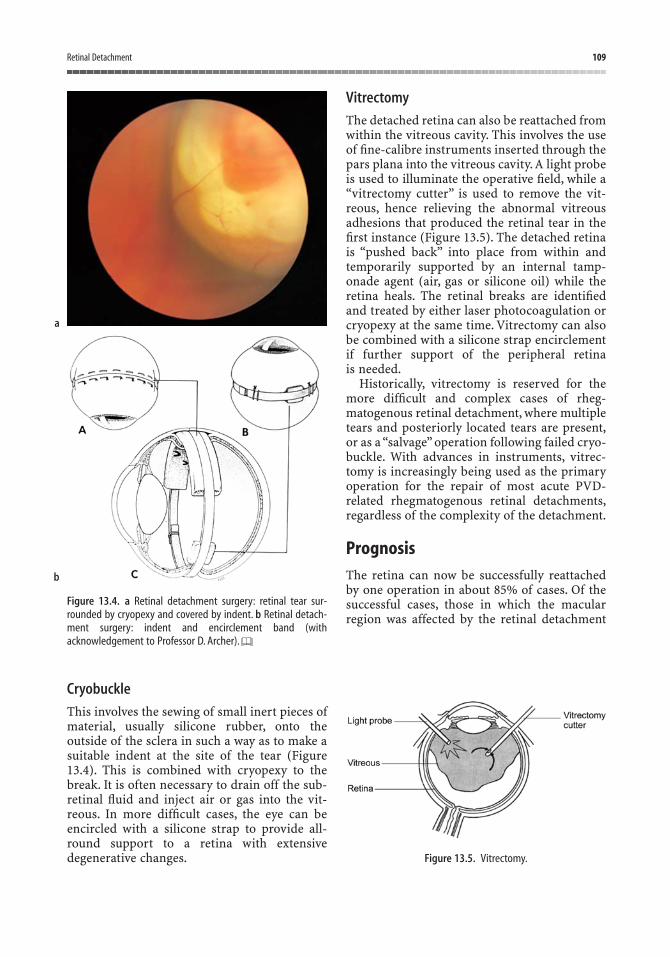
Cryobuckle
This involves the sewing of small inert pieces ofmaterial, usually silicone rubber, onto theoutside of the sclera in such a way as to make asuitable indent at the site of the tear (Figure13.4). This is combined with cryopexy to thebreak. It is often necessary to drain off the sub-retinal fluid and inject air or gas into the vit-reous. In more difficult cases, the eye can beencircled with a silicone strap to provide all-round support to a retina with extensive degenerative changes.
Vitrectomy
The detached retina can also be reattached fromwithin the vitreous cavity. This involves the useof fine-calibre instruments inserted through thepars plana into the vitreous cavity. A light probeis used to illuminate the operative field, while a“vitrectomy cutter” is used to remove the vit-reous, hence relieving the abnormal vitreousadhesions that produced the retinal tear in thefirst instance (Figure 13.5). The detached retinais “pushed back” into place from within andtemporarily supported by an internal tamp-onade agent (air, gas or silicone oil) while theretina heals. The retinal breaks are identifiedand treated by either laser photocoagulation orcryopexy at the same time. Vitrectomy can alsobe combined with a silicone strap encirclementif further support of the peripheral retina is needed.
Historically, vitrectomy is reserved for themore difficult and complex cases of rheg-matogenous retinal detachment, where multipletears and posteriorly located tears are present,or as a “salvage” operation following failed cryo-buckle. With advances in instruments, vitrec-tomy is increasingly being used as the primaryoperation for the repair of most acute PVD-related rhegmatogenous retinal detachments,regardless of the complexity of the detachment.
PrognosisThe retina can now be successfully reattachedby one operation in about 85% of cases. Of thesuccessful cases, those in which the macularregion was affected by the retinal detachment
Retinal Detachment 109
Figure 13.4. a Retinal detachment surgery: retinal tear sur-rounded by cryopexy and covered by indent. b Retinal detach-ment surgery: indent and encirclement band (withacknowledgement to Professor D. Archer).
Figure 13.5. Vitrectomy.
a
b

do not achieve a full restoration of their centralvision, although usually the peripheral fieldrecovers. The degree of recovery of centralvision in such macula-detached cases dependslargely on the duration of the macula detach-ment before surgery. Even when the retina hasbeen detached for two years, it is still possible torestore useful navigational vision.
The main cause of failure of modern retinalreattachment surgery is proliferative vitreo-retinopathy. This is characterised by excessive
“scarring” following initial retinal reattachmentsurgery, with the formation of fibrous tractionalmembrane within the eye, resulting in recurrentdetachment of the retina.
When retinal surgery has failed, furthersurgery might be required and for a few patientsa series of operations is necessary. If it isthought that more than one operation is goingto be needed, it is helpful to the patient if he is warned about this before the treatment is started.
110 Common Eye Diseases and their Management

The word “squint” refers to a failure of the visualaxes to meet at the point of regard. For normalvision, each eye must be focused on and linedup with the object of regard. The fact that wehave two eyes positioned some 60 mm apartmeans that we can accumulate considerablymore data about our environment than wouldbe possible with one eye alone. This can best beexemplified by considering what happens whenone eye is suddenly lost as the result of injuryor disease. Apart from the obvious loss of visualfield, which necessitates turning the head to theblind side, the patient experiences impaired dis-tance judgement. The skilled worker notices adeterioration in the ability to perform fine tasksand the elderly notice that they pour tea into thesaucer rather than the cup. In time, depth per-ception might improve and the patient adapts tothe defect to some extent; children can adapt to one-eyed vision in a remarkable way. But, itseems that modern civilised living does nothave such great demands for binocular visionnow that many tasks are carried out bymachines. It is no coincidence that thoseanimals whose survival depends on catchingtheir food by means of accurate distance judge-ment have their eyes placed in front of theirhead, enabling the two eyes to be focusedtogether on their prey.
Investigation of a normal human populationreveals that although the eyes are situated on thefront of the face, they do not always worktogether, and it will be seen that there are anumber of reasons why the mechanism might
fail. The ability to use the eyes together is calledbinocular vision. It can be measured and gradedby presenting each eye separately, but simul-taneously, with a series of images. The instru-ment used to do this is called a synoptophore(Figure 14.1).
1. Simultaneous macular perception is said tobe present if the subject can see two dis-similar images that are presented simul-taneously to each eye, for example atriangle to one eye and a circle to the other.
2. Fusion is present if the subject can see twoparts of a whole image as one whole wheneach half is presented to a separate eye, forexample a picture of a house to one eye anda picture of a chimney to the other, and thewhole picture is maintained as one as theeyes converge. The range of fusion can bemeasured in degrees.
3. Stereopsis, the third grade of binocularvision, is present if, when slightly dis-similar views of an object are presented to each eye separately, a single three-dimensional view of the whole is seen.Stereopsis itself can also be graded iffine degrees of impairment of binocularfunction need to be measured.
This ability of ours to put together the imagesfrom each eye and make a single picture in ourminds seems to develop during the early yearsof life and furthermore, its development seemsto depend on visual input. Below the age of eight
14Squint
111

years, any misalignment of the eyes that disturbs binocular vision can permanentlydamage this function.
If the alignment of the eyes is disturbed forany reason during childhood, the child might atfirst, as one might expect, notice double visionbut quickly learns to suppress the image fromone eye, thereby eliminating the annoyance ofdiplopia at the expense of binocular vision. Infact, most, but not all, children learn to suppresswhen using monocular instruments, switchingthe other eye on again when the instrument isnot being used. Prolonged suppression seems tolead to a more permanent state of visual losscalled amblyopia of disuse. The word “ambly-opia” simply means blindness. Suppression is atemporary switching off of one eye when theother is in use, whereas amblyopia of disuse is apermanent impairment of vision, which couldaffect the career prospects of the patient.Amblyopia of disuse can also occur if the sightof one eye is defective as the result of opacitiesin the media, even though the alignment of theeyes has not been disturbed. Again, this onlyoccurs in children under the age of eight years.Covering one eye of a baby could lead to per-manent impairment of the vision of that eye, aswell as impairment of the ability to use the eyestogether. An adult can have one eye covered formany months or even years without sufferingvisual loss.
Before considering the causes and effects ofsquint in children and adults, it is necessary toknow something of the different kinds of squint.
Types of SquintIn lay terms, the word squint can just meanscrewing up the eyes but here we are referringto a deviation of one eye from the line of sight.This might be present all the time or just whenthe patient is tired. It is important to noticewhether the eye movements are normal. Forexample, if there is weakness of one lateralrectus muscle, the affected eye will not turnoutward and the angle of the squint will bemuch greater when looking to that side. Mostchildhood squints are not associated with weak-ness of one or more extraocular muscles so thatthe angle of the squint is the same in all direc-tions of gaze. The deviation of the squint can behorizontal or sometimes vertical or the eyescould be convergent or divergent.
Squint in ChildhoodDuring the first few weeks of life the eyes mightseem to wander about aimlessly with limitedability to fix. Between the ages of two and sixmonths, fixation becomes steadier even thoughthe fovea is not fully developed, and by the ageof six months convergence on a near object canbe maintained for several seconds. Even at birth,some degree of following movement of the eyescan be seen in response to a flashing light, butonly the most gross squints can be diagnosedduring these early months of life. If the eyes aredefinitely squinting at the age of six months,urgent referral to an ophthalmologist is indic-ated. Before this or when there is some doubt,referral to an orthoptic screening service can be considered. These have been set up in manyparts of the country. Orthoptists might beregarded as “physiotherapists of the eyes” andthey are trained to examine the eye movementsin great detail. We need to detect squints earlyin children for the following reasons:
1. The squint could be caused by serious un-derlying intracranial or intraocular disease.
2. The squint can result in amblyopia, whichis more effectively treated, the younger the child.
3. The cosmetic effect of a squint is an impor-tant consideration.
112 Common Eye Diseases and their Management
Figure 14.1. The synoptophore. An instrument for measuringthe angle of deviation of a squint and the ability of the eyes towork together.
Amblyopia of DisuseA special word is needed about this curious con-dition, which accounts for unilateral impair-ment of vision in over 2% of the population.Anyeye casualty officer is familiar with the patientwith a foreign body on the cornea of one eyeand the other eye being amblyopic. (“How can Idrive home with this patch on, doctor?”) Thewords “lazy eye” are sometimes used but in layterms this can also mean squint.
The eye suffering from amblyopia of disuseshows certain features:
• Impaired Snellen visual acuity but usuallyable to decipher vertical lines of lettersbetter than horizontal ones.
• Normal fundus.• Small residual squint or, if not, the affected
eye relatively hypermetropic.• An indefinite central scotoma, which
is difficult to assess by routine visual field testing.
• History of poor vision in one eye sincechildhood.
The diagnosis of amblyopia can be by exclu-sion but it must never be reached without acareful examination of the eyes. In recent years,there has been a considerable research interestin this subject and there appear to be nerve con-duction anomalies in the occipital cortex, whichcan be induced by visual deprivation.
Causes of Squint in Childhood• Refractive error – hypermetropia, myopia.• Opaque media – corneal opacities,
cataract, uveitis.• Disease of retina or optic nerve –
retinoblastoma, optic atrophy.• Congenital or acquired weakness of
extraocular muscles.• Abnormalities of facial skeleton leading to
displacement of extraocular muscles.
Refractive Error
In order to understand how refractive error cancause squint, one must first understand how theact of accommodation is linked to the act ofconvergence. That is to say, we must realise that
when we focus upon an object, not only is eachindividual eye separately focused on it, but theeyes swivel together by the requisite amount toallow them both to view the object at once. Agiven amount of accommodation must, there-fore, be associated with an equivalent amount ofconvergence. In hypermetropic subjects thisrelationship is disturbed. In order to overcomehypermetropia, the eyes must accommodateand sometimes this excessive focusing inducesan excess of convergence, hence causing asquint. This type of accommodative squint canbe fully corrected by wearing spectacles: whenthe glasses are on, the eyes are straight; andwhen they are off, one eye turns in. More often,the squint is only partially accommodative andis improved, but not eliminated, by wearingglasses. The convergent squint associated withhypermetropia is the commonest type ofchildhood squint.
Opaque Media
Congenital cataract can occasionally present asa squint. In a similar manner, a corneal opacity,as might result from herpes simplex keratitis orinjury, can cause a squint to appear. A com-pletely blind eye from whatever cause tends toconverge if the blindness occurs in early child-hood. Blindness of one eye in an adult tends toresult in a divergent squint. This is sometimes auseful indicator of the age of onset of blindness.
Disease of the Retina or Optic Nerve
Such a possibility provides an important reasonfor the careful examination of the fundus inevery case.
Congenital or Acquired Muscle Weakness
Sixth, third or fourth cranial nerve palsies aresometimes seen after head injuries and thesurgeon must always bear in mind the possibil-ity of a sixth or other cranial nerve palsy beingassociated with raised intracranial pressure.Myasthenia gravis is extremely rare in childrenbut it can present as a squint. In some cases ofsquint there is a degree of facial asymmetry.These patients might also have “asymmetricaleyes”, one being myopic or hypermetropic rela-tive to the other. Sometimes there is no refrac-tive error but there might be an asymmetry of
Squint 113
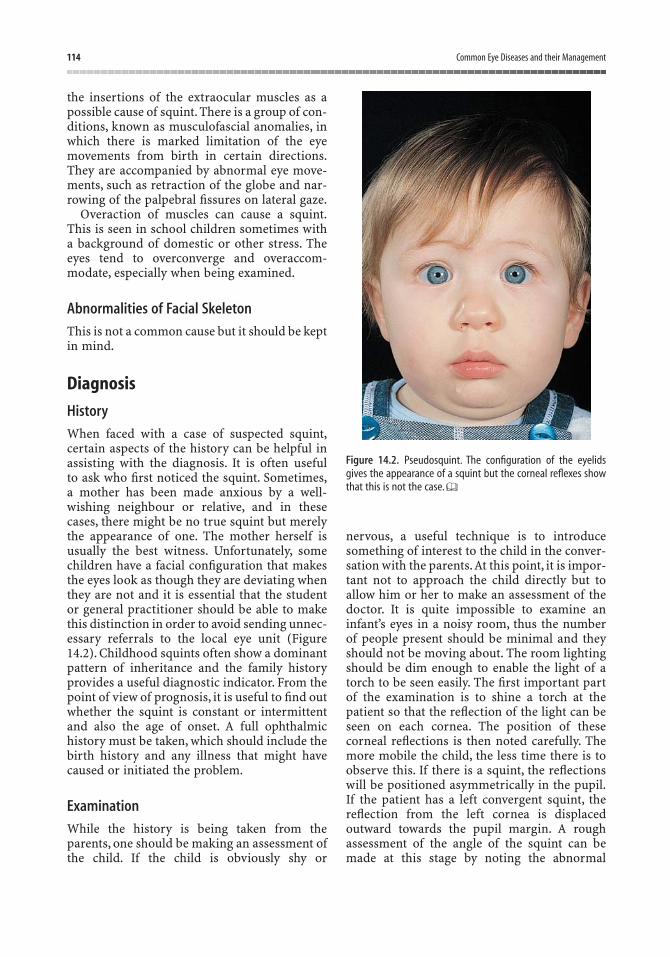
the insertions of the extraocular muscles as apossible cause of squint. There is a group of con-ditions, known as musculofascial anomalies, inwhich there is marked limitation of the eyemovements from birth in certain directions.They are accompanied by abnormal eye move-ments, such as retraction of the globe and nar-rowing of the palpebral fissures on lateral gaze.
Overaction of muscles can cause a squint.This is seen in school children sometimes witha background of domestic or other stress. Theeyes tend to overconverge and overaccom-modate, especially when being examined.
Abnormalities of Facial Skeleton
This is not a common cause but it should be keptin mind.
Diagnosis
History
When faced with a case of suspected squint,certain aspects of the history can be helpful inassisting with the diagnosis. It is often useful to ask who first noticed the squint. Sometimes,a mother has been made anxious by a well-wishing neighbour or relative, and in thesecases, there might be no true squint but merelythe appearance of one. The mother herself isusually the best witness. Unfortunately, somechildren have a facial configuration that makesthe eyes look as though they are deviating whenthey are not and it is essential that the studentor general practitioner should be able to makethis distinction in order to avoid sending unnec-essary referrals to the local eye unit (Figure14.2). Childhood squints often show a dominantpattern of inheritance and the family historyprovides a useful diagnostic indicator. From thepoint of view of prognosis, it is useful to find outwhether the squint is constant or intermittentand also the age of onset. A full ophthalmichistory must be taken, which should include thebirth history and any illness that might havecaused or initiated the problem.
Examination
While the history is being taken from theparents, one should be making an assessment ofthe child. If the child is obviously shy or
nervous, a useful technique is to introducesomething of interest to the child in the conver-sation with the parents.At this point, it is impor-tant not to approach the child directly but toallow him or her to make an assessment of thedoctor. It is quite impossible to examine aninfant’s eyes in a noisy room, thus the numberof people present should be minimal and theyshould not be moving about. The room lightingshould be dim enough to enable the light of atorch to be seen easily. The first important partof the examination is to shine a torch at thepatient so that the reflection of the light can beseen on each cornea. The position of thesecorneal reflections is then noted carefully. Themore mobile the child, the less time there is toobserve this. If there is a squint, the reflectionswill be positioned asymmetrically in the pupil.If the patient has a left convergent squint, thereflection from the left cornea is displacedoutward towards the pupil margin. A roughassessment of the angle of the squint can bemade at this stage by noting the abnormal
114 Common Eye Diseases and their Management
Figure 14.2. Pseudosquint. The configuration of the eyelidsgives the appearance of a squint but the corneal reflexes showthat this is not the case.

position of the reflection. One of the difficultiesexperienced at this point is because of the con-tinuous movement of the child’s eyes, whichmakes it difficult at first to know whether thelight is being accurately fixated. By gentlymoving the torch slightly from side to side, it isusually possible to confirm that the child islooking, albeit momentarily, at the light.
Once the light reflections have been exam-ined, the cover test can be performed. Onceagain the reflection of light from each eye isnoted, but this time one of the eyes is smartlycovered, either with the back of the hand or acard. If the fixating eye is covered, a movementof the nonfixing eye to take up fixation can thenbe observed (Figure 14.3). After some practice,it is possible to detect even slight movements ofthis kind. The result of the test can be mislead-ing if the nonfixing eye is too weak to take up fixation, and quite often, an assessment ofthe vision of the nonfixing eye can be made atthis stage.
If, having performed this first stage of thecover test, no deviation can be detected, thecover can be quickly swapped from one eye tothe other and any movement of the covered eyecan be noted. That is to say, the latent deviation
produced by covering one eye is spotted bynoting the small recovery movement made bythe previously covered eye. Finally, the cover testmust be repeated with the patient looking at adistant object. One type of squint in particularcan be missed unless this is done. This is thedivergent squint seen in young children, whichis often only present when viewing distantobjects. The parents might have noticed anobvious squint and yet testing by the doctor inthe confines of a small room reveals nothingabnormal,with ensuing consternation all round.
After the cover test has been performed, it isnecessary to test the ocular movements todetermine whether there is any muscle weak-ness. At this stage, it is usual to instil a mydri-atic and cycloplegic drop (e.g., cyclopentolate1% or 0.5%) in order to obtain a measure of therefractive error, by retinoscopy, when the eyesare completely at rest. Next, the optic fundi areexamined.
In most instances, the nature of the squintbecomes apparent by this stage and furthertesting of the binocular function and moreaccurate measurement of the angle of the squintare carried out using the synoptophore.
Management of Squint in Childhood
Glasses
Any significant refractive error is corrected bythe prescription of glasses. Sometimes thesquint is completely straightened when glassesare worn but more often the control is partial,the glasses simply acting to reduce the angle ofthe squint. Glasses can be prescribed in a childas young as six to nine months if really neces-sary. It is important that the parents have a fullunderstanding of the need to wear glasses ifadequate supervision is to be expected. Whenthe spectacles are removed at bedtime, a previ-ous squint might appear to become even worseand the parents should be warned about thispossible rebound effect.
Orthoptic Follow-up
The orthoptic department forms an integral andimportant part of the modern eye unit. It is runand manned by orthoptists who carry out thecareful measurement of visual acuity with andwithout glasses and the measurement of eye
Squint 115
Left eye covered
Right eye covered
RIGHT CONVERGENT SQUINT
Figure 14.3. The cover test.

movements and binocular function. Once thepatient has been seen for the initial visit, followup in the orthoptic department is arranged andthe question of treatment by occlusion of thegood eye has to be considered. By covering the good eye for a limited period, the sight of theamblyopic eye can be improved.The younger thechild, the better are the chances of success. Inolder children beyond the age of seven or eightyears, not only is amblyopia more resistant totreatment, but the treatment itself can interfereseriously with school work. The type andamount of occlusive treatment have to beplanned and discussed with the parents. Some-times atropine eye drops are used as an alterna-tive to patching one eye. Orthoptic exercises can also be used in an attempt to strengthenbinocular function.
Surgery
If the squint is not controlled by glasses, surgeryshould be considered. Some parents ask if anoperation can be carried out as a substitute for wearing glasses. Unfortunately, surgery tocorrect refractive error is not yet at a stage whereit can be applied to children with squints. Squintsurgery involves moving the muscle insertionsor shortening the muscles and from the cosmeticpoint of view is highly effective. The adjustmentof the muscles is measured in millimetres to correspond with the angle of the squint indegrees. Sometimes two or more operations areneeded because of occasionally unpredictableresults, but from the cosmetic point of view,nobody need suffer the indignity of a squint,even though a series of operations might beneeded. Once the eyes have been put straight or nearly straight by surgery, the functionalresult depends on the previous presence of goodbinocular vision and good vision in each eye.
Squint occurs in about 2% of the populationand so it is a common problem, but only a small proportion of these cases eventuallyrequire surgery. The commonest type of squintin childhood is the accommodative convergentsquint associated with hypermetropia and heresurgery is indicated only when spectacles proveinadequate. Divergent squints are less commonbut more often require early surgery.
The aim of treatment for a child with squintis to make the eyes look straight, to make eacheye see normally and to achieve good binocular
vision. Unfortunately, all too often, the first oneof these aims alone is achieved in spite ofmodern methods of treatment. The fault mightlie partly in late referral or difficulty withpatient co-operation but better methods oftreatment are needed.
Squint in AdultsAdults who present with a squint have usuallysuffered defective action of one or more of theextraocular muscles. It is important to have abasic understanding of these muscles.
Anatomy of the Extraocular MusclesThe extraocular muscles can be divided intothree groups: the horizontal recti, the verticalrecti and the obliques.
The Horizontal Recti
The medial and lateral recti act as yoke muscles,like the reins of a horse. They rotate the eyeabout a vertical axis. The lateral rectus abductsthe eye (turns it out) and the medial rectusadducts the eye (turns it in).
The Vertical Recti
These act as vertical yoke muscles but they rundiagonally from their origin at the apex of theorbit to be inserted 7 mm or 8 mm behind thelimbus above and below the globe. The action ofthese muscles depends on the initial position ofthe eye. For example, the primary action of thesuperior rectus is to elevate the abducted eyeand the inferior rectus depresses the abductedeye. The secondary action of the superior rectusis to adduct and intort the adducted eye; theinferior rectus adducts and extorts the adductedeye. Intorsion and extorsion refer to rotationabout an anteroposterior axis through theglobe. The important thing to realise is that theaction of these muscles depends on the positionof the eye (Figure 14.4).
The Obliques
These are also vertical yoke muscles but they runon a different line to the vertical recti. The supe-rior oblique depresses the adducted eye (makes
116 Common Eye Diseases and their Management

the eye go down when it is turned in) and theinferior oblique elevates the adducted eye.
When a patient has a fourth cranial nervepalsy on the right side, the right eye can nolonger look down when it is turned in becauseof the defective action of the superior obliquemuscle. Double vision is experienced, which ismaximal (i.e., widest displacement of images)when looking down to the left.
When a patient has a sixth cranial nerve palsyon the right side, the right eye can no longerabduct or turn outwards. A right convergentsquint is seen and the patient experiencesdouble vision, which is worse when looking tothe right.There might be a head turn to the right.
When a patient has a third cranial nerve palsyon the right side, the right eye is turned downand to the right and, if the palsy is complete, theupper lid droops and the pupil is dilated. Move-ment of the eye is limited.
Causes of Adult SquintAdults who present with a squint usually have awell-defined ocular muscle palsy. This can becaused by a pathological process at any pointfrom the brain, through the nerve to the muscle.This will be discussed elsewhere but two impor-tant causes are disseminated sclerosis in theyounger age groups and hypertensive vasculardisease in older patients. Diabetes is anotherimportant cause that must be excluded in all age groups.
Some adult squints prove to be concomitantsquints neglected from childhood. Sometimes alatent squint, which has been well controlledthroughout childhood, breaks down in adult life.
In adult life, a blind eye tends to turn out-wards and a divergent squint can be due solelyto impaired vision in one eye.
DiagnosisIn contrast to the situation with children, whousually present with concomitant squint asso-ciated with hypermetropia, the sudden onset ofa squint in adult life is extremely disablingbecause of intractable double vision. The doublevision is less apparent when the lesion is morecentral, involving the level of the cranial nervenucleus or above. In the latter case, the patienttends to complain more of blurred vision and confusion.
A carefully taken history can reveal the diag-nosis. First, it is necessary to ensure that thedouble vision is only present with both eyesopen and then the patient can be questionedabout the position of the second image andwhether the separation of the images is maximalin any particular direction of gaze. The durationand constant or intermittent nature of the squintmust be determined, as must the history of anyassociated disease, past or present.
Once the history has been obtained, thenature of the squint can be investigated by thecover test and measured by the Maddox wingand Maddox rod. An accurate record of theimpaired muscle action can be recorded on theHess screen.
Maddox Wing
This ingenious but simple device is held in the patient’s hand. By looking through the
Squint 117
Intorts the adducted eye Elevates the abducted eye
Figure 14.4. Primary and secondary actions of the superior rectus muscle.
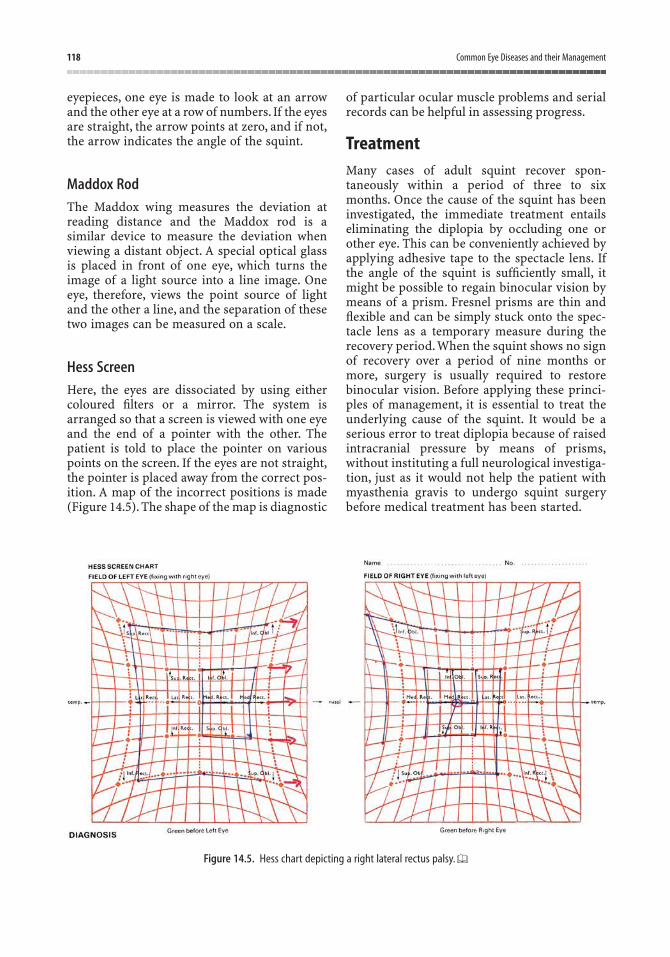
eyepieces, one eye is made to look at an arrowand the other eye at a row of numbers. If the eyesare straight, the arrow points at zero, and if not,the arrow indicates the angle of the squint.
Maddox Rod
The Maddox wing measures the deviation atreading distance and the Maddox rod is asimilar device to measure the deviation whenviewing a distant object. A special optical glassis placed in front of one eye, which turns theimage of a light source into a line image. Oneeye, therefore, views the point source of lightand the other a line, and the separation of thesetwo images can be measured on a scale.
Hess Screen
Here, the eyes are dissociated by using eithercoloured filters or a mirror. The system isarranged so that a screen is viewed with one eyeand the end of a pointer with the other. Thepatient is told to place the pointer on variouspoints on the screen. If the eyes are not straight,the pointer is placed away from the correct pos-ition. A map of the incorrect positions is made(Figure 14.5). The shape of the map is diagnostic
of particular ocular muscle problems and serialrecords can be helpful in assessing progress.
TreatmentMany cases of adult squint recover spon-taneously within a period of three to sixmonths. Once the cause of the squint has beeninvestigated, the immediate treatment entailseliminating the diplopia by occluding one orother eye. This can be conveniently achieved byapplying adhesive tape to the spectacle lens. Ifthe angle of the squint is sufficiently small, itmight be possible to regain binocular vision bymeans of a prism. Fresnel prisms are thin andflexible and can be simply stuck onto the spec-tacle lens as a temporary measure during therecovery period. When the squint shows no signof recovery over a period of nine months ormore, surgery is usually required to restorebinocular vision. Before applying these princi-ples of management, it is essential to treat theunderlying cause of the squint. It would be aserious error to treat diplopia because of raisedintracranial pressure by means of prisms,without instituting a full neurological investiga-tion, just as it would not help the patient withmyasthenia gravis to undergo squint surgerybefore medical treatment has been started.
118 Common Eye Diseases and their Management
Figure 14.5. Hess chart depicting a right lateral rectus palsy.

Ocular Muscle ImbalanceMild latent squints can sometimes go undetec-ted until a period of stress or perhaps excessivereading precipitates symptoms of eyestrain andheadache. The effort to maintain both eyes inline causes the symptoms. The latent deviationcould be inward or outward but because mostpeople’s eyes tend to assume a slightly divergentposition when completely at rest, a degree of latent divergence (exophoria) is almost the rule and of no significance. Vertical muscleimbalance is less well tolerated and even a slight deviation can cause symptoms. Small butsignificant degrees of vertical muscle imbalance
are seen in otherwise normal individuals whoshow a marked difference in refractive errorbetween the two eyes or in those with facialasymmetry. The provision of a small prismincorporated into the spectacle lenses of suchpatients can produce dramatic relief, but wemust always remember that the appearance ofan ocular muscle imbalance might be the firstindication of more serious disease. A small ver-tical deviation can be the first sign of a tumourof the lacrimal gland or thyrotoxic eye diseaseand a wide range of investigations might beneeded before one can be satisfied with theexcellent but sometimes deceptive results ofsymptomatic treatment.
Squint 119
In this chapter the more important oculartumours will be considered. There are a con-siderable number of other rare tumours and theinterested student should refer to one of themore specialised and comprehensive textbooksof ophthalmology for further reading.
The GlobeExpanding tumours in the eye present diagnos-tic problems because it is not usually possible tobiopsy them.
Choroidal MelanomaThe most common primary intraocular tumouris the malignant melanoma of the choroid. Inwhite people, the tumour has an incidence of onein 2500 and the average age at presentation is 50years. The incidence rises with age with a peakat 70 years. However, it is important to appre-ciate that no age is exempt because choroidalmelanomas have been reported in children asyoung as three years. It is extremely rare in blackpeople. It differs from melanoma of the skin inthat it grows more slowly and metastasises late.Most choroidal melanomas are thought to orig-inate from choroidal nevi, which are present inup to 10% of the population. At first, it is seen asa raised pigmented oval area, which can be any-where in the fundus (Figure 15.1). It is usuallybrown in colour although it can be amelanotic(or greyish).As the tumour enlarges there might
be an associated exudative retinal detachmentor, less often, secondary glaucoma. Other asso-ciated features might include choroidal haemor-rhage and serial photography might be neededto confirm the growth. The usual presentation iswith decreased vision or a visual field defect.Diagnosis is confirmed with careful clinicalexamination, including indirect ophthalmo-scopy and slit-lamp biomicroscopy (contact lens or volk lens examination), fluoresceinangiography, ultrasonography and transvitrealfine-needle aspiration in equivocal cases. Themost common site for metastases is the liver,so abdominal ultrasound, serum liver functiontests, and chest X-ray should be performed atregular intervals. The appearance of liver metas-tases can be delayed for several years and canoccur even if the eye has been removed, sig-nifying micrometastases at the time of presen-tation. Approximately 40% of patients developliver metastases within ten years of the initialdiagnosis, while the estimated five-year mortal-ity rate for treated medium-size melanomas isbetween 15% and 23%. The differential diagno-sis of choroidal melanoma includes retinaldetachment, metastatic choroidal tumours, wetmacular degeneration, large choroidal nevi,choroidal haemangioma or choroidal effusion.Historically, treatment involved enucleation(removal of the globe); today, however, manyalternative eye-sparing treatments are available,partly dependent on the size and local spread of the tumour. Options include radiotherapy(external plaque, proton beam or helium ion),
15Tumours of the Eye and Adnexae
121

laser photocoagulation for small lesions, localresection and transpupillary thermotherapy.Untreated, the tumour can extend into the orbit and provide an unpleasant problem for the patient.
Choroidal MetastasesThese make up the most common intraoculartumours in adults. Although lesions can bedemonstrated in at least 1–2.5% of patients withcarcinomas, many cases remain asymptomaticunless the macula is involved. In males, the mostcommon primary tumour is found in the lungand in females, it is the breast. The metastatictumours are usually treated with external beam radiotherapy.
RetinoblastomaThis is a rare tumour of childhood, which arisesnot from the choroid but, as its name suggests,from the retina. It is, however, the commonest
primary intraocular tumour in children, with anincidence of one in 15,000 live births. It showscertain rather strange and unusual features. It is not usually present from birth, but occursmost frequently in infancy to age three years(although it can occur in older patients); it iseither inherited as an autosomal dominant traitor can be sporadic in nature. Approximately40% of cases are considered to be inherited. Inone-third of inherited cases it appears in botheyes. A change in the RB1 gene on chromosome13 is found in the inherited cases. Initially, it canbe seen in an individual, suspected on accountof the family history, as a small white, raisedmass. Examination under anaesthesia is essen-tial in such cases because the tumour might bein the extreme periphery of the fundus. A largertumour can present as a white mass in the pupil(“leucocoria”) and such an appearance ininfancy demands immediate referral to an ophthalmologist (Figure 15.2). Other presentingfeatures include strabismus, secondary glau-coma, proptosis or intraocular inflammatorysigns. Computed tomography (CT) scanningand ultrasound might show a calcified intra-ocular mass. Extension tends to occur locallyalong the optic nerve and enucleation is oftenlife saving. Until recently, enucleation was thetreatment of choice and cure rates of 90–95%were achieved. Nowadays, eye-sparing therapyis preferred, in an attempt at avoiding the physical and psychological trauma involved inenucleating a young child. Alternative treat-ment options include initial systemic tumourchemoreduction with carboplatin-based regi-mens, followed by external beam radiotherapy,plaque radiotherapy, cryotherapy or laser pho-tocoagulation. Genetic counselling is essentialfor these patients in order to prevent theincreasing incidence of the tumours, which willresult from effective medical treatment.
Melanoma of the IrisThis rare iris tumour usually presents as a sol-itary iris nodule, which might or might not bepigmented. It can cause distortion of the pupil,which can be an early warning sign. Other fea-tures that can point to the diagnosis are local-ised lens opacity, iris neovascularisation andelevation of intraocular pressure. Melanoma ofthe iris is extremely slow growing and probablymuch less malignant than choroidal melanoma,
122 Common Eye Diseases and their Management
Figure 15.1. Choroidal melanoma poorly pigmented (amelan-otic) melanoma a fundus photograph. b Bisected eye showingpigmented and nonpigmented portions of melanoma in sameeye (with acknowledgement to Mr A. Foss).
a
b
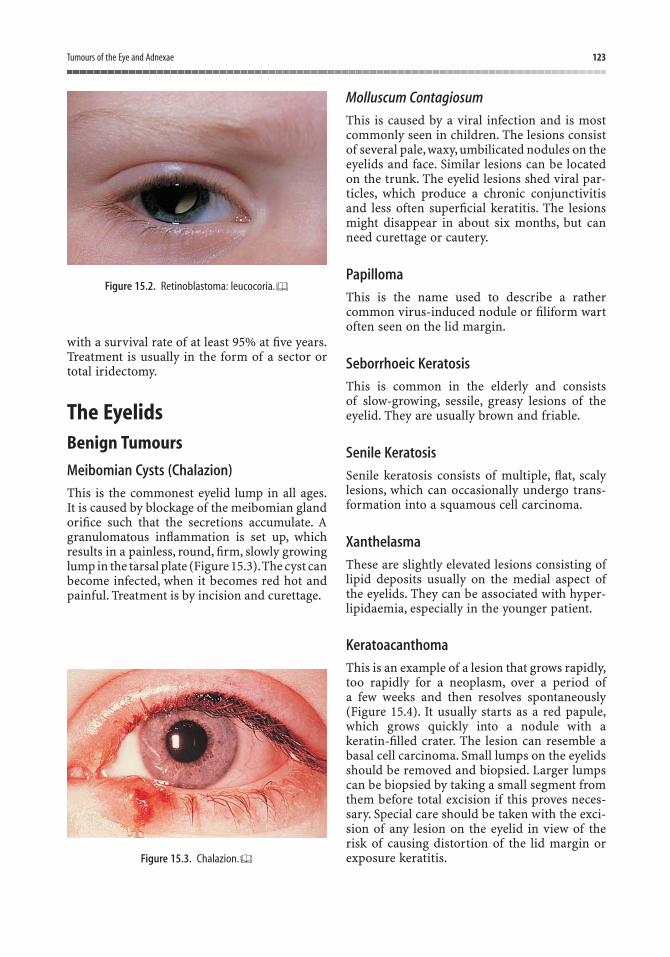
with a survival rate of at least 95% at five years.Treatment is usually in the form of a sector ortotal iridectomy.
The EyelidsBenign Tumours
Meibomian Cysts (Chalazion)
This is the commonest eyelid lump in all ages.It is caused by blockage of the meibomian glandorifice such that the secretions accumulate. Agranulomatous inflammation is set up, whichresults in a painless, round, firm, slowly growinglump in the tarsal plate (Figure 15.3).The cyst canbecome infected, when it becomes red hot andpainful. Treatment is by incision and curettage.
Molluscum Contagiosum
This is caused by a viral infection and is mostcommonly seen in children. The lesions consistof several pale, waxy, umbilicated nodules on theeyelids and face. Similar lesions can be locatedon the trunk. The eyelid lesions shed viral par-ticles, which produce a chronic conjunctivitisand less often superficial keratitis. The lesionsmight disappear in about six months, but canneed curettage or cautery.
Papilloma
This is the name used to describe a rathercommon virus-induced nodule or filiform wartoften seen on the lid margin.
Seborrhoeic Keratosis
This is common in the elderly and consists of slow-growing, sessile, greasy lesions of theeyelid. They are usually brown and friable.
Senile Keratosis
Senile keratosis consists of multiple, flat, scalylesions, which can occasionally undergo trans-formation into a squamous cell carcinoma.
Xanthelasma
These are slightly elevated lesions consisting oflipid deposits usually on the medial aspect ofthe eyelids. They can be associated with hyper-lipidaemia, especially in the younger patient.
Keratoacanthoma
This is an example of a lesion that grows rapidly,too rapidly for a neoplasm, over a period ofa few weeks and then resolves spontaneously(Figure 15.4). It usually starts as a red papule,which grows quickly into a nodule with akeratin-filled crater. The lesion can resemble abasal cell carcinoma. Small lumps on the eyelidsshould be removed and biopsied. Larger lumpscan be biopsied by taking a small segment fromthem before total excision if this proves neces-sary. Special care should be taken with the exci-sion of any lesion on the eyelid in view of therisk of causing distortion of the lid margin orexposure keratitis.
Tumours of the Eye and Adnexae 123
Figure 15.2. Retinoblastoma: leucocoria.
Figure 15.3. Chalazion.
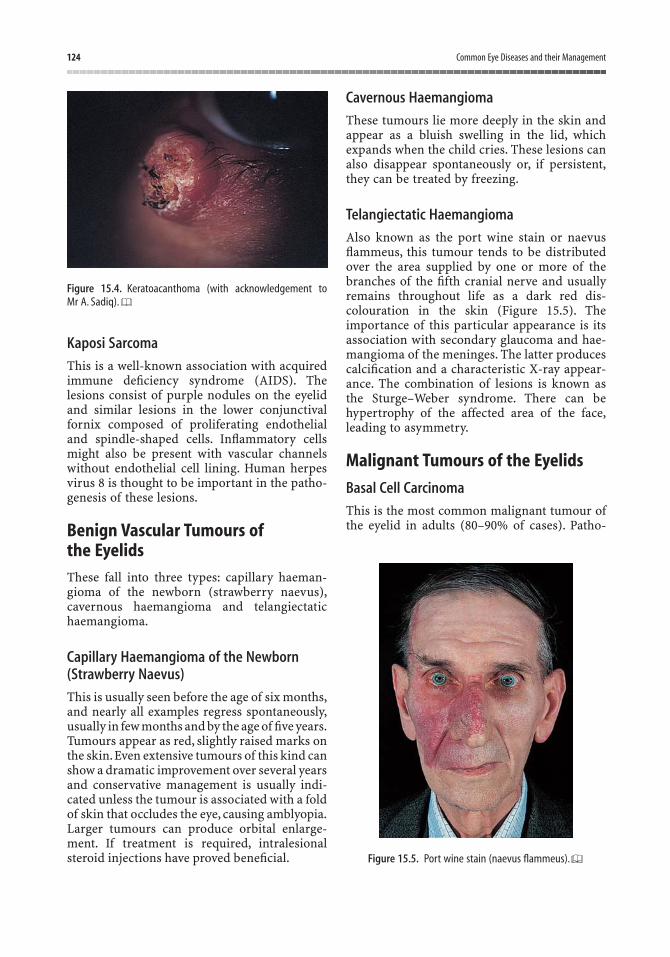
Kaposi Sarcoma
This is a well-known association with acquiredimmune deficiency syndrome (AIDS). Thelesions consist of purple nodules on the eyelidand similar lesions in the lower conjunctivalfornix composed of proliferating endothelialand spindle-shaped cells. Inflammatory cellsmight also be present with vascular channelswithout endothelial cell lining. Human herpesvirus 8 is thought to be important in the patho-genesis of these lesions.
Benign Vascular Tumours of the EyelidsThese fall into three types: capillary haeman-gioma of the newborn (strawberry naevus),cavernous haemangioma and telangiectatichaemangioma.
Capillary Haemangioma of the Newborn(Strawberry Naevus)
This is usually seen before the age of six months,and nearly all examples regress spontaneously,usually in few months and by the age of five years.Tumours appear as red, slightly raised marks onthe skin.Even extensive tumours of this kind canshow a dramatic improvement over several yearsand conservative management is usually indi-cated unless the tumour is associated with a foldof skin that occludes the eye, causing amblyopia.Larger tumours can produce orbital enlarge-ment. If treatment is required, intralesionalsteroid injections have proved beneficial.
Cavernous Haemangioma
These tumours lie more deeply in the skin andappear as a bluish swelling in the lid, whichexpands when the child cries. These lesions canalso disappear spontaneously or, if persistent,they can be treated by freezing.
Telangiectatic Haemangioma
Also known as the port wine stain or naevusflammeus, this tumour tends to be distributedover the area supplied by one or more of thebranches of the fifth cranial nerve and usuallyremains throughout life as a dark red dis-colouration in the skin (Figure 15.5). Theimportance of this particular appearance is itsassociation with secondary glaucoma and hae-mangioma of the meninges. The latter producescalcification and a characteristic X-ray appear-ance. The combination of lesions is known asthe Sturge–Weber syndrome. There can behypertrophy of the affected area of the face,leading to asymmetry.
Malignant Tumours of the Eyelids
Basal Cell Carcinoma
This is the most common malignant tumour ofthe eyelid in adults (80–90% of cases). Patho-
124 Common Eye Diseases and their Management
Figure 15.4. Keratoacanthoma (with acknowledgement to Mr A. Sadiq).
Figure 15.5. Port wine stain (naevus flammeus).

genesis is related to exposure to ultraviolet light,hence it most frequently involves the lower lid and medial canthus. The tumour begins as asmall insignificant nodule, which turns into asmall crater-like lesion with a slightly raised,pearly-coloured edge with fine dilated bloodvessels on its surface (Figure 15.6). Although thetumour rarely metastasises, it is locally invasive,and, therefore, early diagnosis and treatment isimportant. In the early stages, it is a simplematter to remove the lesion and confirm thediagnosis by biopsy, but if left the tumour tendsto spread into surrounding structures and intothe underlying bone and orbit (Figure 15.7).Treatment depends on the size, extent and loca-tion of the tumour. Usually, surgical excisionwith wide margins is the technique of choice,either by a simple excisional biopsy or by themore complex Mohs’ procedure. The moreextensive, neglected basal cell carcinomata are treated by radical surgery, cryotherapy orpalliative radiotherapy.
Squamous Cell Carcinoma
Squamous cell carcinoma is the second mostcommon malignant eyelid lesion and cons-titutes 5–10% of cases. It occurs most commonlyin the elderly and is related to sunlight exp-osure. The tumour can initially resemble a basalcell carcinoma, although the edges are usuallynot rolled. Spread tends to occur to the locallymph nodes (preauricular for the upper lid andsubmandibular for the lower lid). Treatment issimilar to a basal cell carcinoma. Sebaceous Gland Carcinoma
This uncommon tumour constitutes 1–3% ofmalignant eyelid tumours (higher in Asians). Itarises from the meibomian glands in the tarsalplate. It appears as a discrete, firm nodule, whichoften presents as a “recurrent chalazion”, therebydelaying diagnosis. Treatment involves wide excision with or without radiotherapy. Mortalityranges from 6% to 30%, depending on site, size,symptom duration and histological classification.
Melanoma of the Eyelid
Malignant melanoma of the eyelids is similar tomalignant melanoma elsewhere, appearing as araised, often shiny, black lump. It metastasises atan early stage and the prognosis does not seemto be altered by excision.
Tumours of the Eye and Adnexae 125
Figure 15.6. Early basal cell carcinoma of medial canthus.
Figure 15.7. Extensive basal cell carcinoma involving the orbitand extending across the nose to the opposite side. a Clinicalphotograph; b computerised tomography scan.
a
b
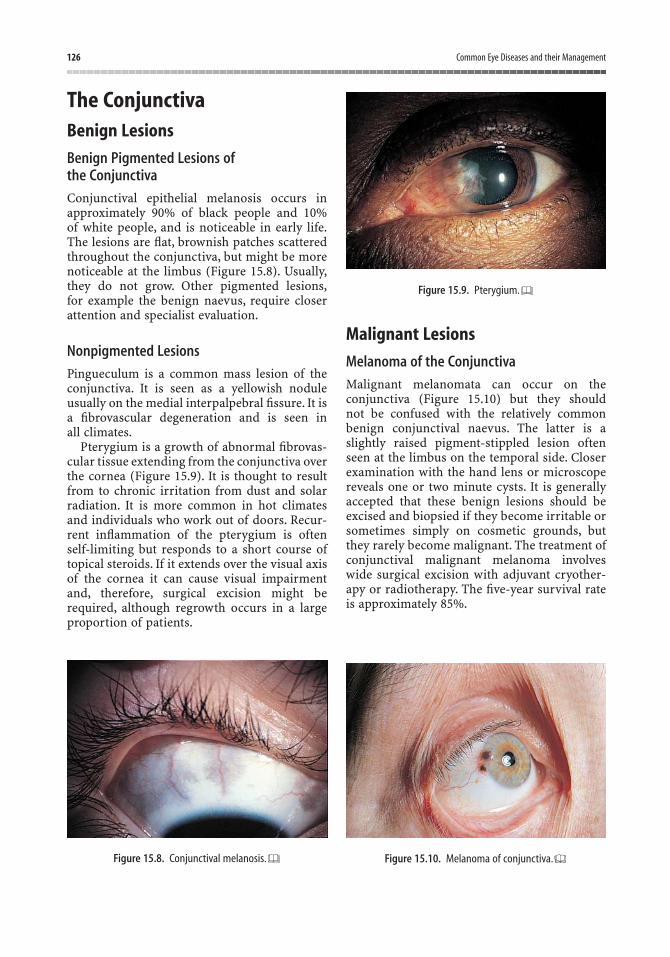
The ConjunctivaBenign Lesions
Benign Pigmented Lesions of the Conjunctiva
Conjunctival epithelial melanosis occurs inapproximately 90% of black people and 10% of white people, and is noticeable in early life.The lesions are flat, brownish patches scatteredthroughout the conjunctiva, but might be morenoticeable at the limbus (Figure 15.8). Usually,they do not grow. Other pigmented lesions,for example the benign naevus, require closerattention and specialist evaluation.
Nonpigmented Lesions
Pingueculum is a common mass lesion of theconjunctiva. It is seen as a yellowish noduleusually on the medial interpalpebral fissure. It isa fibrovascular degeneration and is seen in all climates.
Pterygium is a growth of abnormal fibrovas-cular tissue extending from the conjunctiva overthe cornea (Figure 15.9). It is thought to resultfrom to chronic irritation from dust and solarradiation. It is more common in hot climatesand individuals who work out of doors. Recur-rent inflammation of the pterygium is oftenself-limiting but responds to a short course oftopical steroids. If it extends over the visual axisof the cornea it can cause visual impairmentand, therefore, surgical excision might berequired, although regrowth occurs in a largeproportion of patients.
Malignant Lesions
Melanoma of the Conjunctiva
Malignant melanomata can occur on the conjunctiva (Figure 15.10) but they should not be confused with the relatively commonbenign conjunctival naevus. The latter is aslightly raised pigment-stippled lesion oftenseen at the limbus on the temporal side. Closerexamination with the hand lens or microscopereveals one or two minute cysts. It is generallyaccepted that these benign lesions should beexcised and biopsied if they become irritable orsometimes simply on cosmetic grounds, butthey rarely become malignant. The treatment ofconjunctival malignant melanoma involveswide surgical excision with adjuvant cryother-apy or radiotherapy. The five-year survival rateis approximately 85%.
126 Common Eye Diseases and their Management
Figure 15.10. Melanoma of conjunctiva.Figure 15.8. Conjunctival melanosis.
Figure 15.9. Pterygium.

The Orbit (see Table 15.1)Lacrimal Gland and Sac TumoursLacrimal gland tumours can either be inflam-matory, mixed cell tumours or adenocarcino-mas. They present with proptosis or a mass inthe outer part of the eyelid superotemporalorbit. Lacrimal sac tumours are less commonand present with sac swelling. Benign lesionsand infections need to be excluded.
Dermoid CystThis cystic swelling is usually seen at the level ofthe eyebrow in the upper outer part of the orbit.It is smooth and fluctuant and often fixed to bone.Sometimes a deeper part of the cyst can occupya cavity in the bone and a computed tomography(CT) scan is advisable when this is suspected.Rupture of the cyst can lead to profound orbitalinflammation. Excision on cosmetic grounds andfor diagnosis is usually indicated.
Cavernous HaemangiomaThis is the commonest primary neoplasm ofthe orbit in adults. It is benign. It is unusual for surgery to be necessary in such cases. It isusually located within the muscle cone, andgives rise to axial proptosis.
Glioma of the Optic NerveThis rare tumour causes progressive proptosisand optic atrophy but it can be slow growing.There is an association with Von Reckling-hausen’s disease (neurofibromatosis type 1) and the presence of pigmented patches in theskin should make one suspect this. Treatment by
surgical resection and/or radiotherapy is indi-cated if intracranial spread is documented.
RhabdomyosarcomaThis rare but highly malignant orbital tumouris seen in children. Its growth is so rapid that itmay be misdiagnosed as orbital cellulitis. If acorrect diagnosis is made at an early stage, thereis some hope of reaching a cure by combiningradiotherapy and chemotherapy. The tumour isthought to arise from striated muscle and thehistological diagnosis is confirmed by findingstriation in the tumour cells. It is usually locatedin the superonasal orbit.
Metastatic Tumours and Tumours from Neighbouring SitesA wide variety of tumours can invade the orbitand produce proptosis and often diplopia. Lym-phoma is one example. It can present as an iso-lated lesion or in association with Hodgkin’sdisease or leukaemia. Examples of local spreadfrom adjacent structures include carcinoma of the nasopharynx, carcinoma of the lacrimalgland and meningioma. In children, orbitalmetastases arise most commonly from neuro-blastoma and Ewing’s sarcoma. In the adult, thecommonest primary sites are bronchus, breast,prostate and kidneys.
“Pseudotumour” (Idiopathic OrbitalInflammatory Disease)This is an inflammatory swelling in the orbit ofunknown cause, which can present with pain,proptosis and diplopia. A mass might be palpa-ble in the orbit and biopsy reveals nonspecificinflammatory tissue consisting mainly of lym-phocytes. Diagnosis can eventually be made by exclusion of other causes of proptosis. Insevere cases, a course of systemic steroidsand/or radiotherapy is usually effective.
Exophthalmos and ProptosisBoth these terms mean forward protrusion ofthe eyes but traditionally exophthalmos refersto the bilateral globe protrusion in thyroiddisease. Proptosis refers to unilateral forward
Tumours of the Eye and Adnexae 127
Table 15.1. Primary orbital tumours.
Vascular Capillary haemangiomaCavernous haemangiomaLymphangioma
Neural Optic nerve gliomaMeningiomaNeurofibromatoma
Lacrimal glandLymphoproliferativeRhabdomyosarcomaHistiocytosis

128 Common Eye Diseases and their Management
displacement of the globe from whatever cause.In practice, the terms tend to be used ratherloosely and are now almost synonymous.
Causes of Proptosis (see Table 15.2)
When one eye seems to bulge forward, thedoctor might have a serious problem on hishands and the following likely causes should be considered:
• Pseudoproptosis. An apparent bulgingforward of the eye occurs if the eye is toobig, as in unilateral high myopia, or if theother eye is sunken following a blow-outfracture of the maxilla (orbital floor).These need to be distinguished from a true proptosis.
• Thyrotoxicosis. This is the commonestcause of unilateral or bilateral proptosis;diagnosis is achieved from the history,examination and tests of thyroid function(Figure 15.11).
• Infection. Orbital cellulitis, usually fromneighbouring sinuses, requires urgentotorhinological opinion.
• Trauma. Proptosis can occur as a result of retro-orbital haemorrhage. Diagnosisshould be possible from the patient’s history.
• Haemangioma. This can expand afterbending down or crying.Ultrasound and CTscanning can confirm the diagnosis. Occa-sionally, angiography might be required.
• Pseudotumour. Biopsy should be carriedout if possible, and other causes excluded.
• Mucocele of sinuses. Diagnose by X-ray orCT scan.
• Lymphoproliferative disease. A biopsy, fullblood count and sternal marrow punctureshould be carried out.
• Others. There are a large number of pos-sible but rare causes of proptosis.
Assessment of ProptosisIn the clinic, proptosis is best assessed by stand-ing behind the seated patient and asking him tolook down. The position of each globe in rel-ation to the lids and face can be best seen by thismeans. Proptosis can be measured by means of an exophthalmometer. A number of suchinstruments are on the market and they dependon measuring the distance from the rim of theouter margin of the orbit to the level of theanterior part of the cornea. These measure-ments are not always accurate (especially for the novice) but best results are achieved byensuring that they are made by the same person,using the same instrument on each occasion fora given patient.
Once thyroid disease and trauma have beenexcluded, the patient would require furtherinvestigations including systemic examination,full blood picture, orbital ultrasound, CT scan,magnetic resonance imaging (MRI) scan,possibly carotid angiography and sometimesorbital biopsy.
Figure 15.11. Proptosis: dysthyroid disease.
Table 15.2. Causes of proptosis.
• Endocrine• Vascular abnormalities• Inflammatory disorders• Primary orbital tumours• Metastases

The fact that injuries to the eye and its sur-rounding region demand special attention andcreate great concern for patient and doctor isself-evident when the eye alone is involved, butwhen other life-threatening injuries are present,the eye injury, seeming slight at the time, mightbe overlooked. Sometimes, the eyelids might be so swollen that it is difficult to examine the eyes and a serious perforating injury could beobscured. When other injuries are present andan anaesthetic is needed, it is essential that theeyes are examined carefully, if possible underthe same anaesthetic. As in the case of injurieselsewhere, those to the eye demand urgent andimmediate treatment, and neglect can result intragedy even though the problem might have atfirst seemed slight.
Injuries to the GlobeContusionThe eye casualty officer comes to recognise afamiliar pattern of contusion, the effect ofsquash ball injuries and blows from flyingobjects in industry or after criminal assault.Injuries from industrial causes have nowbecome quite uncommon thanks to bettercontrol by means of protective clothing andproper guarding of machinery.As a result, sport-ing injuries have become more evident,althoughhere increasing public concern has also led tosome improvement. Notable instances of good
control are the use of protective guards in icehockey and cricket. The surrounding orbitalmargin provides good protection to the eyesfrom footballs and even tennis and cricket balls,but the rare golf ball contusion injury usuallyleads to loss of the sight of the eye. Squash ballsand especially shuttle cocks have earned a badreputation for inflicting contusion injuries and,from the economic point of view, leading to lossof time at work and hospital expenses.
The extent of damage to the eye from con-tusion depends on whether it has been possibleto close the eyelids in time before the momentof impact. If the lids have been closed, bruisingand swelling of the eyelids is marked and theinjury to the eye might be minimal. It must beremembered though that this is not an infalliblerule and the eyes themselves must always becarefully examined, even when there is extremeswelling of the lids. It is always possible toexamine an eye, if necessary using an eye spec-ulum under general anaesthesia. In the primarycare situation, one must be very careful not toapply more than gentle pressure to the eyelidsin case the globe of the eye has been perforatedand when there is doubt, referral to the eyedepartment is advisable. The important clinicalfeatures of contusion injury are best consideredby looking at the anatomical parts of the eye.
Cornea
The most common injury to the cornea is fromthe corneal foreign body and this has already
16Ocular Trauma
129
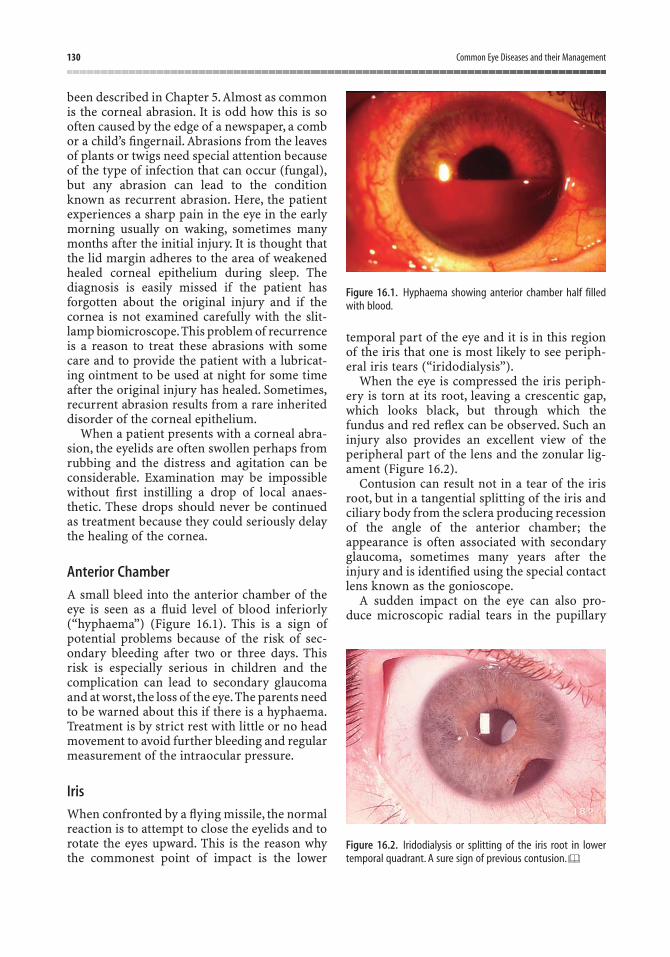
been described in Chapter 5.Almost as commonis the corneal abrasion. It is odd how this is sooften caused by the edge of a newspaper, a combor a child’s fingernail. Abrasions from the leavesof plants or twigs need special attention becauseof the type of infection that can occur (fungal),but any abrasion can lead to the conditionknown as recurrent abrasion. Here, the patientexperiences a sharp pain in the eye in the earlymorning usually on waking, sometimes manymonths after the initial injury. It is thought thatthe lid margin adheres to the area of weakenedhealed corneal epithelium during sleep. Thediagnosis is easily missed if the patient has forgotten about the original injury and if thecornea is not examined carefully with the slit-lamp biomicroscope.This problem of recurrenceis a reason to treat these abrasions with somecare and to provide the patient with a lubricat-ing ointment to be used at night for some timeafter the original injury has healed. Sometimes,recurrent abrasion results from a rare inheriteddisorder of the corneal epithelium.
When a patient presents with a corneal abra-sion, the eyelids are often swollen perhaps fromrubbing and the distress and agitation can beconsiderable. Examination may be impossiblewithout first instilling a drop of local anaes-thetic. These drops should never be continuedas treatment because they could seriously delaythe healing of the cornea.
Anterior Chamber
A small bleed into the anterior chamber of theeye is seen as a fluid level of blood inferiorly(“hyphaema”) (Figure 16.1). This is a sign ofpotential problems because of the risk of sec-ondary bleeding after two or three days. Thisrisk is especially serious in children and thecomplication can lead to secondary glaucomaand at worst, the loss of the eye.The parents needto be warned about this if there is a hyphaema.Treatment is by strict rest with little or no headmovement to avoid further bleeding and regularmeasurement of the intraocular pressure.
Iris
When confronted by a flying missile, the normalreaction is to attempt to close the eyelids and torotate the eyes upward. This is the reason whythe commonest point of impact is the lower
temporal part of the eye and it is in this regionof the iris that one is most likely to see periph-eral iris tears (“iridodialysis”).
When the eye is compressed the iris periph-ery is torn at its root, leaving a crescentic gap,which looks black, but through which thefundus and red reflex can be observed. Such aninjury also provides an excellent view of theperipheral part of the lens and the zonular lig-ament (Figure 16.2).
Contusion can result not in a tear of the irisroot, but in a tangential splitting of the iris andciliary body from the sclera producing recessionof the angle of the anterior chamber; theappearance is often associated with secondaryglaucoma, sometimes many years after theinjury and is identified using the special contactlens known as the gonioscope.
A sudden impact on the eye can also pro-duce microscopic radial tears in the pupillary
130 Common Eye Diseases and their Management
Figure 16.2. Iridodialysis or splitting of the iris root in lowertemporal quadrant. A sure sign of previous contusion.
Figure 16.1. Hyphaema showing anterior chamber half filledwith blood.
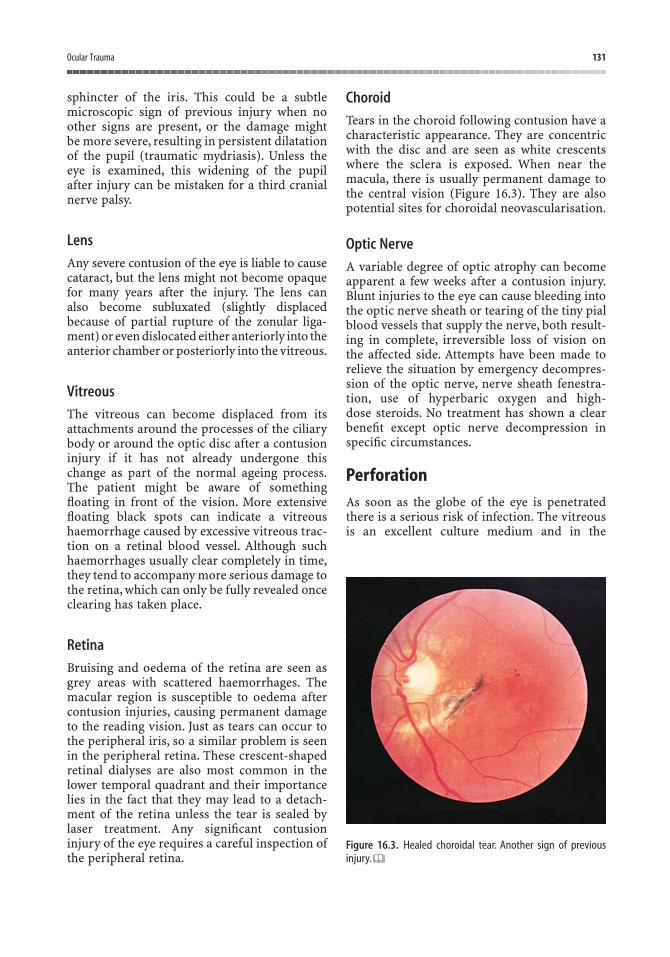
sphincter of the iris. This could be a subtlemicroscopic sign of previous injury when noother signs are present, or the damage might be more severe, resulting in persistent dilatationof the pupil (traumatic mydriasis). Unless theeye is examined, this widening of the pupil after injury can be mistaken for a third cranialnerve palsy.
Lens
Any severe contusion of the eye is liable to causecataract, but the lens might not become opaquefor many years after the injury. The lens can also become subluxated (slightly displaced because of partial rupture of the zonular liga-ment) or even dislocated either anteriorly into theanterior chamber or posteriorly into the vitreous.
Vitreous
The vitreous can become displaced from itsattachments around the processes of the ciliarybody or around the optic disc after a contusioninjury if it has not already undergone thischange as part of the normal ageing process.The patient might be aware of somethingfloating in front of the vision. More extensivefloating black spots can indicate a vitreoushaemorrhage caused by excessive vitreous trac-tion on a retinal blood vessel. Although suchhaemorrhages usually clear completely in time,they tend to accompany more serious damage tothe retina, which can only be fully revealed onceclearing has taken place.
Retina
Bruising and oedema of the retina are seen asgrey areas with scattered haemorrhages. Themacular region is susceptible to oedema aftercontusion injuries, causing permanent damageto the reading vision. Just as tears can occur tothe peripheral iris, so a similar problem is seenin the peripheral retina. These crescent-shapedretinal dialyses are also most common in thelower temporal quadrant and their importancelies in the fact that they may lead to a detach-ment of the retina unless the tear is sealed bylaser treatment. Any significant contusioninjury of the eye requires a careful inspection ofthe peripheral retina.
Choroid
Tears in the choroid following contusion have acharacteristic appearance. They are concentricwith the disc and are seen as white crescentswhere the sclera is exposed. When near themacula, there is usually permanent damage tothe central vision (Figure 16.3). They are alsopotential sites for choroidal neovascularisation.
Optic Nerve
A variable degree of optic atrophy can becomeapparent a few weeks after a contusion injury.Blunt injuries to the eye can cause bleeding intothe optic nerve sheath or tearing of the tiny pialblood vessels that supply the nerve, both result-ing in complete, irreversible loss of vision on the affected side. Attempts have been made torelieve the situation by emergency decompres-sion of the optic nerve, nerve sheath fenestra-tion, use of hyperbaric oxygen and high-dose steroids. No treatment has shown a clearbenefit except optic nerve decompression inspecific circumstances.
PerforationAs soon as the globe of the eye is penetratedthere is a serious risk of infection. The vitreousis an excellent culture medium and in the
Ocular Trauma 131
Figure 16.3. Healed choroidal tear. Another sign of previousinjury.
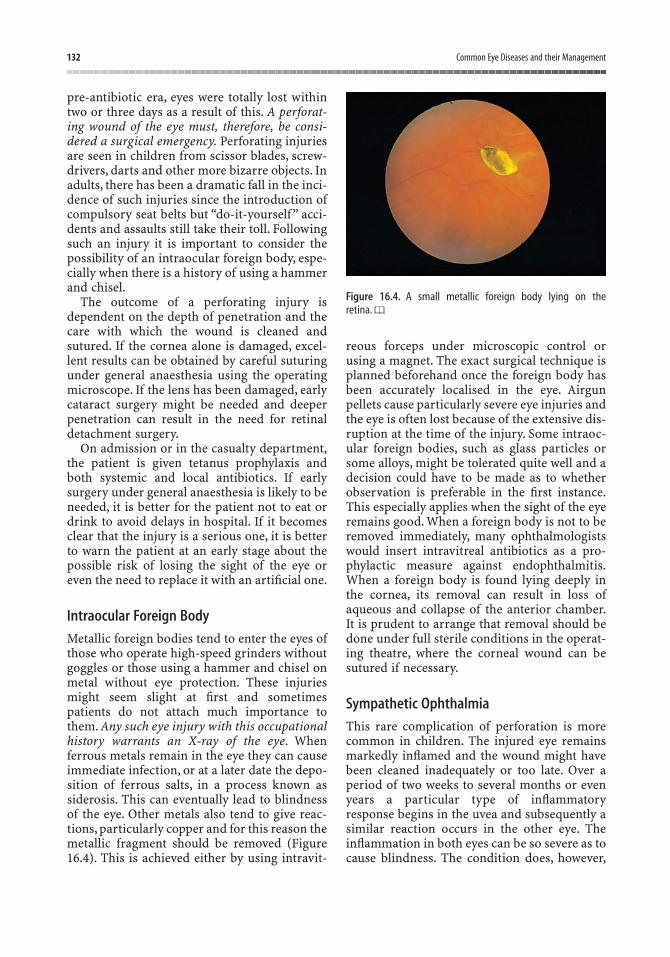
pre-antibiotic era, eyes were totally lost withintwo or three days as a result of this. A perforat-ing wound of the eye must, therefore, be consi-dered a surgical emergency. Perforating injuriesare seen in children from scissor blades, screw-drivers, darts and other more bizarre objects. Inadults, there has been a dramatic fall in the inci-dence of such injuries since the introduction ofcompulsory seat belts but “do-it-yourself” acci-dents and assaults still take their toll. Followingsuch an injury it is important to consider thepossibility of an intraocular foreign body, espe-cially when there is a history of using a hammerand chisel.
The outcome of a perforating injury isdependent on the depth of penetration and thecare with which the wound is cleaned andsutured. If the cornea alone is damaged, excel-lent results can be obtained by careful suturingunder general anaesthesia using the operatingmicroscope. If the lens has been damaged, earlycataract surgery might be needed and deeperpenetration can result in the need for retinaldetachment surgery.
On admission or in the casualty department,the patient is given tetanus prophylaxis andboth systemic and local antibiotics. If earlysurgery under general anaesthesia is likely to beneeded, it is better for the patient not to eat ordrink to avoid delays in hospital. If it becomesclear that the injury is a serious one, it is betterto warn the patient at an early stage about thepossible risk of losing the sight of the eye oreven the need to replace it with an artificial one.
Intraocular Foreign Body
Metallic foreign bodies tend to enter the eyes ofthose who operate high-speed grinders withoutgoggles or those using a hammer and chisel onmetal without eye protection. These injuriesmight seem slight at first and sometimespatients do not attach much importance tothem. Any such eye injury with this occupationalhistory warrants an X-ray of the eye. Whenferrous metals remain in the eye they can causeimmediate infection, or at a later date the depo-sition of ferrous salts, in a process known assiderosis. This can eventually lead to blindnessof the eye. Other metals also tend to give reac-tions, particularly copper and for this reason themetallic fragment should be removed (Figure16.4). This is achieved either by using intravit-
reous forceps under microscopic control orusing a magnet. The exact surgical technique isplanned beforehand once the foreign body hasbeen accurately localised in the eye. Airgunpellets cause particularly severe eye injuries andthe eye is often lost because of the extensive dis-ruption at the time of the injury. Some intraoc-ular foreign bodies, such as glass particles orsome alloys, might be tolerated quite well and adecision could have to be made as to whetherobservation is preferable in the first instance.This especially applies when the sight of the eyeremains good. When a foreign body is not to beremoved immediately, many ophthalmologistswould insert intravitreal antibiotics as a pro-phylactic measure against endophthalmitis.When a foreign body is found lying deeply inthe cornea, its removal can result in loss ofaqueous and collapse of the anterior chamber.It is prudent to arrange that removal should bedone under full sterile conditions in the operat-ing theatre, where the corneal wound can besutured if necessary.
Sympathetic Ophthalmia
This rare complication of perforation is morecommon in children. The injured eye remainsmarkedly inflamed and the wound might havebeen cleaned inadequately or too late. Over aperiod of two weeks to several months or evenyears a particular type of inflammatoryresponse begins in the uvea and subsequently asimilar reaction occurs in the other eye. Theinflammation in both eyes can be so severe as tocause blindness. The condition does, however,
132 Common Eye Diseases and their Management
Figure 16.4. A small metallic foreign body lying on the retina.

respond well to steroid treatment and it isextremely rare. Occasionally, one sees patientswho have an artificial eye complaining of tran-sient blurring of the vision of their remainingeye. They need to be examined carefully forsigns of uveitis.
Injuries to the EyelidsLoss or destruction of eyelid tissue shouldalways be treated as a threat to vision. The upperlid especially is important in this respect. Theimmediate concern is to ensure that the corneais properly covered when the eyelids are closed.If more than one-third of the margin of theupper lid is lost, this must be replaced by graft-ing from the lower lid. When less than one-thirdis missing, the gaping wound can usually beclosed directly. Up to one-third of the lower lidcan also be closed by direct suturing. Whenmore than this is lost or when it has been trans-ferred to the upper lid, a slide of tissue from thelateral canthus can be effected, combined if nec-essary with a rotating cheek flap.
One of the most important features of therepair of lid injuries is the method of suturing.If the lid margin is involved, the repair shouldbe made using the operating microscope andthe fine suture material available in an eyedepartment (Figure 16.5). An untidy repair canresult in a permanently watering eye because ofkinking of the eyelid. This interferes with theproper moistening of the cornea during blink-ing or when asleep. Special attention must be
paid when the medial part of the eyelid has beentorn, as this contains the lacrimal canaliculus.Again, unless repair is carried out using anaccurate technique under general anaesthesia intheatre, the risk of a permanently watering eyeis increased.
Contusion of the eyelids, otherwise known asa black eye, is of course a common problem,especially on Saturday nights in a general cas-ualty department. Usually, the presence of ablack eye is an indication that the afflicted wassmart enough to close his eye in time to avoidinjury to the globe. It is unusual to find damageto the eyes after Saturday night fist-fights, unless a weapon was involved. Broken beer glassesproduce devastating injuries to the eyes as wellas to the eyelids.
Injuries to the OrbitBlows on the side of the cheek and across oneor other eye occur in fights, industrial accidentsand road traffic accidents. The most commontype is the “blow-out fracture”. Here the globeand contents of the orbit are forced backwards,causing fracture of the orbital floor and dis-placement of bone downwards into the antrumof the maxillary sinus. The inferior rectusmuscle becomes tethered in the wound so thatthere is mechanical limitation of upward move-ment. The infraorbital nerve, which traversesthe orbital floor, can also be injured, producinganaesthesia of the skin of the cheek. Once thesurrounding swelling has subsided, the post-erior displacement of the globe becomesobvious and the globe of the eye itself oftenshows evidence of contusion. A considerableimprovement from the functional and cosmeticpoint of view can be obtained by positioning aplastic or Teflon implant in the floor of the orbitafter freeing the prolapsed tissue.
Fractures of the skull that extend into the orbitcan be accompanied by retro-orbital haemor-rhage and proptosis.Cranial nerve palsies affect-ing the ocular movements are also commonlyseen in this type of injury and the vision can beaffected by optic nerve damage.A blow on the eyecan result in sudden blindness with at first noother evidence of injury (apart from an afferentpupillary defect), but subsequently, the optic disc becomes pale and atrophic after two or three weeks.
Ocular Trauma 133
Figure 16.5. Full thickness lower lid laceration.

Radiational InjuriesThe eyes might be exposed to a wide range ofelectromagnetic radiation from the shorterwavelength ultraviolet rays through the wave-lengths of visible light to the longer infraredwaves, X-rays and microwaves. X-rays passstraight through the eye without being focusedby the optical media and, in large enough doses,can cause generalised damage. It is important torealise that therapeutic but not diagnostic dosesof X-rays tend to cause cataracts and the eyemust be suitably screened during treatment.Excessive doses of X-rays also cause stenosis ofthe lacrimal canaliculi, destruction of the secre-tory cells within the lacrimal glands and retinalneovascularisation. As one might expect, visiblelight does not normally damage the eyes,although an intense light source can be absorbedby the pigment epithelium behind the retina andconverted to heat, producing a macular burn.After eclipses of the sun, there are usually anumber of patients who arrive in the casualtydepartments of eye hospitals with macularoedema and sometimes serious permanentimpairment of visual acuity. Sun gazing, withconsequent retinal damage, has been reportedafter taking lysergic acid diethylamide (LSD).
The laser beam provides a source of intenselight, which is used widely in ophthalmology asa deliberate means of producing gentle burns inthe retina or making holes in the lens capsuleafter cataract surgery. However, uncontrolleduse of lasers can cause blinding foveal burns asthe subject tends to look directly at the beammomentarily, until they realise what it is. Ultra-violet rays, which are shorter than visible light,do not normally penetrate the eye but in largeenough doses produce burns of the eyelids andcornea. On the skin this is seen as erythaemaand later pigmentation, and on the cornea apunctate keratitis is seen with the slit-lamp.Ultraviolet damage of this kind is seen aftergazing with unprotected eyes at welder’s arcs,after exposure of the eyes to sunray lamps, andafter exposure to the sun under certain condi-tions such as in snow on mountain tops. Allthese types of ultraviolet injury show a delayed
effect, the symptoms appearing 2 h or 3 h afterexposure and lasting for about 48 h. There isusually severe pain and photophobia so that it might not be possible to open the eyes,hence the term “snow blindness”. The use oflocally applied steroid and antibiotic dropshastens recovery.
Unlike ultraviolet light, infrared rays pene-trate the eye and can cause cataract. A specifickind of thermal cataract has been well des-cribed in glass-blowers and furnace workers but this is now rarely seen because of the use ofprotective goggles. Microwaves, in the form ofdiathermy, can cause cataract but the eye mustbe in the path of the beam if damage is to occur,and microwave ovens would not be expected tobe dangerous in this respect. Concern is quiteoften expressed in the press or elsewhere aboutthe possibility of radiation damage to the eyesfrom visual display units. Such damage hasnever been demonstrated any more than it hasfrom the face of a television set. Someone notused to working with a visual display unit whois suddenly made to spend several hours a dayin front of one might experience eyestrain, esp-ecially if incorrect spectacles are worn.
Chemical InjuriesThese are quite common but usually not severeenough to warrant hospital attention. In indus-trial premises there is now nearly always a first-aid post with facilities to wash out the eyes.Plain water or a salt solution is the best fluid touse and valuable time may be lost if washing isdelayed in order to search for a specific antidote.More severe burns can result from the catalystsused in the manufacture of plastics or fromalkalis, such as caustic soda. Alkalis penetratethe eye rapidly as they saponify lipids withincell membranes, aiding passage, and can quicklyreach the posterior segment. Acid burns as fromexploding car batteries are quite commonlyseen in large casualty departments but areusually less severe as acids tend to coagulatecorneal proteins, thereby slowing penetration.
134 Common Eye Diseases and their Management

Section IVProblems of the Medical Ophthalmologist

Measurement of visual acuity is the mostimportant part of the ocular assessment per-formed by the doctor and yet it is surprisinghow often the nonspecialist omits it in exam-ination. It has already been shown that the differential diagnosis of the red eye can besimplified by noting the vision in the affectedeye. After injuries of the eye, it is just as impor-tant to note the vision in the uninjured eye as inthe injured eye. Simple measurement of visualacuity is of limited value without a knowledgeof the spectacle correction or whether thepatient is wearing the appropriate spectacles.The best corrected visual acuity (i.e., with lensesin place) therefore needs to be recorded for eacheye. This corrected visual acuity can also be est-imated with a pinhole held in front of the eye.The effect of the pinhole is to eliminate theeffect of refraction by the cornea and the lenson the extremely thin beam of light produced bythe pinhole.
Measuring the visual acuity means measuringthe function of the macula, which is of courseonly a small part of the whole retina. A patientmight have grossly impaired visual acuity andyet have a normal visual field, enabling him towalk about and lead a normal life apart frombeing unable to read. This state of affairs is seenin patients with age-related macular degenera-tion and can be compared with the situation inwhich a patient has grossly constricted visualfields but normal macular function, as is some-times seen in retinitis pigmentosa or advancedprimary open-angle glaucoma. Here, the patient
appears to be blind, being unable to find his wayabout, but he might surprise the ophthalmolo-gist by reading the visual acuity chart from topto bottom once he has found it.
The simplest way to measure visual acuitymight be to determine the ability to distinguishtwo points when placed close together (resolu-tion). Such a method was supposed to have beenused by the Arabs when choosing their horse-men. They chose only those who were able toresolve the two stars that form the second “star”in the tail of the Great Bear constellation. Apoint source of light such as a star, although itis infinitely small, forms an image with a diam-eter of about 11mm on the retina. This is becausethe optical media are not perfect and allowsome scattering of the light. In practice, it is pos-sible for a person with normal vision to distin-guish two points if they are separated by 1 mm when placed 10 m away. Two such pointswould be separated by 2mm on the retina. Thismight be surprising considering that a spot oflight casts a minimum size of image of 11 mmbecause of scatter, but such an image is notuniform, being brighter in the centre than at theperiphery. In fact, the resolving power of the eyeis limited by the size of the cones, which have adiameter of 1.5mm.
In the clinic, the distance visual acuity ismeasured by asking the patient to read a stan-dard set of letters, the Snellen chart. This isplaced at a distance of 6 m from the eye. Thesingle large letter at the top of this chart isdesigned to be just discernible to a normal-
17Testing Visual Acuity
137
sighted person at a range of 60 m. If the patient’svision is so poor that only this and no smallerletter can be seen at 6 m, the vision is recordedas the fraction “6/60”. The normal-sightedperson who can read the chart down to thesmaller letters designed to be discerned at 6 mis recorded as having a visual acuity of 6/6. Thenormal range of vision extends between 6/4 and6/9, depending on the patient’s age. In someEuropean countries, the visual acuity isexpressed as a decimal instead of a fraction.Therefore, 6/60 would be expressed as 0.1. In theUSA, metres are replaced by feet, so 6/6 becomes20/20. This is where the term “twenty twenty”vision originates from, meaning clear or near-perfect vision. Recently, a new type of visualacuity chart has entered use in the clinic and inresearch studies. It is called the LogMAR chartand differs from the conventional Snellen chart(Figure 3.1) by having five letters on each linerather than the “pyramid” shape of the Snellenchart. There are also smaller differences in typesize between lines. Some of the advantages ofusing this new chart are that the measurementof poor visual acuity is more accurate as morelarger letters are included and small changes in acuity are easier to detect (easier to detectdisease progression or treatment success).
The near visual acuity is also measured usinga standard range of reading types in the style ofnewsprint and, here, care must be taken toensure that the correct spectacles for near workare used if the patient is over the age of 45 years(Figure 17.1). Normally, the results of testing thenear visual acuity are in agreement with thosefor measuring distance vision providing thecorrect spectacles are worn if needed.
The visual acuity of each eye must always bemeasured by placing a card carefully over oneeye and then transferring this to the other eyewhen the first eye has been tested. The visualacuity of both eyes together is usually the sameor fractionally better than the vision of thebetter of the two eyes tested individually. Incertain special circumstances, the binocularvision can be worse than the vision of each eye tested separately (e.g., in cases of maculardisease causing distortion).
A number of other tests have been developedto measure visual acuity in the nonliteratepatient. Infants below the reading age can bemeasured with surprising accuracy using theStycar test. Here, letters of differing size are
shown to the child, who is asked to point to thesame letter on the card, which is given to him.Up to the age of 18 months or two years, theoptokinetic drum might be used. This makesuse of the phenomenon of optokinetic nystag-mus produced by moving a set of verticallyarranged stripes across the line of sight. Whenthe stripes are sufficiently narrow, they are nolonger visible and fail to produce any nystag-mus. The eyes are examined using a gradedseries of stripes. This kind of test can be used tomeasure visual acuity in animals other thanman. The “E” test is a way of measuring thevisual acuity of illiterate patients. This is basedon the Snellen type but the patient is presentedwith a series of letter “E”s of different sizes andorientations and is given a wooden letter “E” tohold in the hands. He is then instructed to turnthe wooden letter to correspond with the letterindicated on the chart.
The Snellen type has the great advantage ofbeing widely used and well standardised, but itmust be realised that it is a measure of some-thing more complex than simply the function of the macula area of the retina. It involves adegree of literacy and also speech, and testing
138 Common Eye Diseases and their Management
The newsprint these days isn’t whatit used to be. . . .
Figure 17.1. Reading glasses in presbyopia.

shy children or elderly patients can sometimesbe misleading.
Other ways of measuring visual acuity havebeen developed. One is to assess the patient’sability to resolve a grating. Here, the word“grating” refers to a row of black-and-whitestripes where the black merges gradually intothe white. Such a grating can be varied by alter-ing either the contrast of black and white or thewidth of the stripes (the “frequency”). Thus, fora given individual, the threshold for contrastand frequency (contrast sensitivity) can bemeasured. This type of test has certain theor-etical advantages over standard methods but itis not widely used clinically as a routine. Finally,the electrical potentials generated by the retinaand optic nerve can be measured to give an esti-mate of visual acuity when the eye is presentedwith targets of varying size and contrast. Thismethod is useful in infants and in the assess-ment of adults with nonorganic visual loss.
Measuring for SpectaclesIf a patient has not been tested recently for spec-tacles, not only can the measurement of visualacuity be inaccurate, but the symptoms mightbe caused by the need for a correct pair ofglasses. The measurement, which determinesthe type of spectacles needed, requires skilldeveloped by practice and the use of the rightequipment. The most obvious way to measuresomeone for a pair of glasses is to try the effectof different lenses and ask the patient whetherthe letters are seen better with one lens oranother. This is known as subjective testing and,by itself, it is not a accurate method becausesome patients’ observations as to the clarity ofletters can be unreliable. Furthermore, a healthyyoung person might see quite clearly with awide range of lenses simply by exercising theciliary muscle (i.e., accommodation). Fortu-nately, the refractive error of the eye can bemeasured by an objective method and ananswer can be reached without consulting thepatient. The method entails observing the rateof movement of the shadow of the iris againstthe red reflex from the fundus of the eye afterinterposing different strengths of lenses(retinoscopy). In order to make an accuratemeasurement of the spectacle requirement,
both objective and subjective refractions areperformed and the results compared.
Objective RefractionThe patient is fitted with a spectacle trial frameinto which different lenses can be slotted. In thecase of young children, it is usually advisable toinstill a mydriatic and cycloplegic drop before-hand to eliminate focusing. The ophthalmol-ogist then views the eye to be examined throughan instrument known as a retinoscope, from a distance of about one arm’s length. The redreflex can be seen and the instrument is thenmoved slightly so that the light projected fromthe retinoscope moves to and fro across thepupil. The shadow of the iris on the red reflex isthen seen to move, and the direction and speedof movement depend on the refractive error ofthe patient. By interposing different lenses in thetrial frame, the movement of the iris shadow canbe “neutralised” and the exact refractive errordetermined. The trial frame can accommodateboth spherical and cylindrical lenses so that theamount of astigmatism can be measured.
Subjective RefractionHere, considerable skill is also needed becausemany patients become quite tense when beingtested in this way and might not initially giveaccurate answers. Lenses both stronger andweaker than the expected requirement areplaced in the trial frames and the patient isasked to read the letters of the Snellen chart andto say whether they are more or less clear. Anumber of supplementary tests are available,which enable one to check the patients’ answers.It can be seen that the word “refraction” refersto the total test for glasses, although the sameword refers to the bending of the rays of light as they pass from one medium to another.Accurate refraction takes 10 min or 15 min toperform, or longer in difficult cases and it is anessential preliminary to an examination of theeye itself.
Automated RefractionIn recent years attempts have been made todevelop an automated system of refraction, andinstruments are now commercially available.They are, however, still expensive and not always
Testing Visual Acuity 139

accurate when there are opacities in the opticalmedia, or when the patient overaccommodates.One further way of assessing the refractive errorwithout asking the patient any questions is bymaking use of the visually evoked response.This is the name given to the minute electricalchanges detectable over the back of the scalpwhen the eyes are exposed to a repeated stim-ulus, usually a flashing checkerboard.When finechecks are viewed, interposing different lensescan modify the response. This method is ofgreat interest but it is still not reliable and takestime to perform.
Considering the importance of the measure-ment of visual acuity, it is not surprising that a
number of tests have been developed for this,but the simple Snellen chart remains an essen-tial part of any doctor’s surgery. It must beremembered that this is a measure of functionin the centre of the visual field only and it is pos-sible to have advanced loss of peripheral visionwith normal visual acuity, as is seen sometimesin patients with chronic glaucoma or retinitispigmentosa. The assessment of the rest of thevisual field has also been standardised and anumber of instruments have been developed tomeasure it. These have already been describedin Chapter 3 together with various other meas-urements of different aspects of vision.
140 Common Eye Diseases and their Management
In an earlier chapter, we have already seen that“the red eye” is an important sign in ophthal-mology, and there are a number of reasons whythe eye can become inflamed.When the exposedparts of the eye, such as the conjunctiva and thecornea, are the primary sites of inflammation,the cause is usually infection or trauma.Common examples are chronic conjunctivitis ora corneal foreign body. However, here we aregoing to consider a type of inflammation thatarises deeper in the eye and primarily from theuvea. The uvea has a tendency to becomeinflamed for no apparent external reason and inthis respect can be compared to a joint; indeed,there is a recognised association between uveitisand arthritis. In spite of the fact that the eye isopen to microscopic examination, the exactcause of uveitis is usually obscure,although thereis evidence to indicate a relationship with otherkinds of autoimmune disease. Uveitis can bedivided into anterior or posterior uveitis; ante-rior uveitis is the same entity as iridocyclitis,andposterior uveitis is the same as choroiditis.Apartfrom the uvea, the sclera and the episclera (thatis, the connective tissue deep to the conjunctivaand overlying the sclera) can also be affected bysimilar inflammatory changes.
Anterior UveitisSymptomsThe patient suffering from acute anterior uveitisis usually aware that there is something seriously
amiss with the eye. The vision is blurred and theeye aches and can often be extremely painful.Photophobia is usual and often pain on focusingon near objects is a feature. The age incidence iswide but anterior uveitis is commonly seen inthe third and fourth decades of life, and everyeye casualty officer becomes familiar with thisparticular form. When the disease presents forthe first time in the elderly, the underlying causeis likely to be different and age provides animportant diagnostic feature. Acute anterioruveitis usually appears quite suddenly over aperiod of about 24h and then resolves on treat-ment in two or three weeks; however, it may lastas long as six weeks. A further exacerbationmight occur during this period and there is a strong tendency towards recurrence after a few months or several years in the same or theother eye.
SignsThe eye is red, but of especial importance is thepresence of a pink flush around the cornea (theciliary flush), which indicates an inflammatoryprocess either in the cornea or within the anter-ior chamber of the eye itself. The pupil is smallbecause the iris sphincter goes into spasm.Thus, the pupil of iritis is small and treatmentis aimed at making it larger, whereas the pupilof acute glaucoma is large and treatment isaimed at making it smaller. Unless there is sec-ondary glaucoma, the cornea remains brightand clear, but with a pen torch it might be pos-
18The Inflamed Eye
141

sible to see that the aqueous looks turbid. Thatis to say, a beam of light shone through theaqueous resembles a beam of sunlight shiningthrough a dusty room (Figure 18.1). Normally,of course, the aqueous is crystal clear even whenexamined with the slit-lamp biomicroscope.
The presence of an occasional cell in theaqueous can be normal, especially if the pupilhas been dilated with mydriatic eye drops, butsuspicion should be raised if more than three orfour cells are seen. In fact, the early diagnosis ofanterior uveitis can entail careful slit-lampexamination. It is usual to discriminate betweenthe presence of cells in the aqueous and thepresence of flare. The latter reflects a highprotein content and is a feature of more long-standing disease. Because there are convectioncurrents in the aqueous, inflammatory cells areswept down the centre of the posterior surfaceof the cornea and become adherent to it, oftenforming a triangular-shaped spread of depositsknown as keratic precipitates, or “KP”s (Figure18.2). The microscopic appearance of the KP isdetermined by the type of cells. If a granulo-matous type of inflammatory reaction is takingplace, involving epithelioid cells and macro-phages, the KP might be large, resembling oildroplets (“mutton fat KP”). This form of KP isseen in uveitis associated with sarcoidosis andalso tuberculosis and leprosy. When theinflammation is nongranulomatous, a finedusting of the posterior surface of the corneacould be evident. KPs tend to become absorbed
but they can remain more permanently as pig-mented spots on the endothelium.
Anterior uveitis is often associated with theformation of adhesions between the posteriorsurface of the iris and the lens. These are calledposterior synechiae and become evident whenattempts are made to dilate the pupil becauseparts of the iris remain stuck to the pupil givingit an irregular appearance. In severe cases ofanterior uveitis, pus can collect in the anteriorchamber to the extent that a fluid level can beseen where the layer of pus has formed inferi-orly. This is known as hypopyon – literally,“pusbelow” (Figure 18.3). A hypopyon is an indica-tion of severe disease in the eye and the patient
142 Common Eye Diseases and their Management
Figure 18.1. Flare.
Figure 18.2. Keratic precipitates.
Figure 18.3. Hypopyon. In addition, there are red blood cellsand fibrinous exudate in the anterior chamber (with acknowl-edgement to Professor H. Dua).

should preferably be treated in hospital as aninpatient. Hypopyon tends to occur in certainspecific types of anterior uveitis. It is occasion-ally seen in elderly diabetics with inadequatelytreated corneal ulcers, particularly those withvascular occlusive disease. It is also seen inBehçet’s disease, which is a rare disorder char-acterised by hypopyon uveitis, and ulceration ofthe mouth and genitalia. A hypopyon is occa-sionally seen following cataract surgery and insuch cases can be infective or noninfective inorigin. It is fortunately a rare complication ofmodern cataract surgery and the use of intra-ocular acrylic lenses.
ComplicationsThe visual prognosis of acute anterior uveitis as commonly seen in young people is usuallygood unless recurrences are frequent. Chronicuveitis is more prone to complications. Sec-ondary glaucoma can cause serious problemsand a careful check on the intraocular pressuremust be maintained. The rise in intraocularpressure might be due to direct obstruction ofthe aqueous outflow by inflammatory cells or bythe presence of adhesions between the periph-eral part of the iris and the posterior surface ofthe cornea (peripheral anterior synechiae).Sometimes, especially when treatment has beeninadequate, the posterior synechiae sticking the pupil margin to the anterior surface of thelens become extensive enough to obstruct thepassage of aqueous through the pupil. The irisbulges forward, giving the appearance known asiris bombe. Secondary glaucoma can also resultfrom the use of topical steroids in predisposedindividuals. Cataract is a further serious com-plication, which can appear after repeatedattacks of anterior uveitis. It nearly always firstaffects the posterior subcapsular zone of the lensand, unfortunately, interferes with the vision atan early stage. Cataracts can also result fromlong-term use of topical or systemic steroids.
CausesFor the majority of patients who present to eyeoutpatient departments with this condition, nospecific cause is found. However, there are manyknown causative agents. The ophthalmologist isobliged to exclude at least some of these, eventhough he knows that more often than not a
negative result will be obtained. It is necessaryto explain this to patients otherwise consider-able anxiety might be created by the fact that“no cause can be found” for their complaint.When we say no cause can be found, we reallymean that there is no evidence of any associatedsystemic disease and this should be of somereassurance to the patient.
It has already been mentioned that it can behelpful to consider the age of the patient whentrying to eliminate the possibility of underlyingsystemic disease. Uveitis is rare in young chil-dren, but when seen, the possibility of juvenilerheumatoid arthritis must be borne in mind.In young adults, sarcoidosis, gonorrhoea,Reiter’s disease and ankylosing spondylitis areall recognised associations. In former years,tuberculosis was high on the list of suspectedcauses but this would appear to be a lesscommon cause nowadays. Herpes simplex andzoster can also cause anterior uveitis. Septic fociin adjacent structures, such as dental sepsis orsinusitis, have also been under suspicion butthese are now thought to be relatively unimpor-tant. In the case of the elderly, the onset ofanterior uveitis can prove to be a recurrence of previous attacks and the same underlyingcauses must be suspected, but here there is alsothe possibility of lens-induced uveitis asso-ciated with hypermature cataract. Three othertypes specific of anterior uveitis must be men-tioned at this stage.
Sympathetic OphthalmiaThis is a rare but dramatic response of the uveain both eyes to trauma. The significance of thecondition rests in the fact that although thetrauma has only affected one eye, the inflam-matory reaction occurs in both. It can followperforating injuries, especially when uvealtissue has become adherent to the wound edges.Occasionally it can occur following intraocularsurgery. The injured eye, which is referred to as the “exciting eye”, remains severely inflamedand, after an interval of between two weeks andseveral years, the uninjured eye (“sympathisingeye”) becomes affected. The inflammation in thesympathising eye usually starts in the region of the ciliary body and spreads anteriorly andposteriorly. It is granulomatous. Careful woundtoilet and repair of the injured eye can prob-ably prevent many cases, as can also removal of
The Inflamed Eye 143

blind, painful and inflamed eyes within the crit-ical two-week period following injury.
Heterochromic IridocyclitisThis type of anterior uveitis presents in 20–40year olds and is usually unilateral. The visionbecomes blurred and the iris becomes depig-mented. The eye usually remains white, theinflammatory reaction is low grade and chronic;posterior synechiae do not develop. Theinflammation does not usually respond at all totreatment. Cataracts and chronic glaucomaoccur commonly. The condition has been mim-icked by denervating the sympathetic supply ofthe eyes in experimental animals and it seemspossible that there might be a neurologicalcause, unrelated and distinct from other typesof uveitis.
Pars Planitis (Intermediate Uveitis)This refers to a low-grade inflammatoryresponse, which is seen in young adults. It affectsboth eyes in up to 80% of cases, although theseverity can be asymmetrical. There is minimalevidence of anterior uveitis and the patientcomplains of floating spots in front of thevision. Inspection of the fundus reveals vitreousopacities and careful inspection of the periph-eral retina shows whitish exudates in the over-lying vitreous. A mild-to-moderate peripheralretinal phlebitis can occur. The condition runsa chronic course and occasionally can be com-plicated by cataract, cystoid macular oedema and tractional retinal detachment. The cause isunknown in the majority of cases, althoughthere is a known association with sarcoidosis.
Treatment and ManagementOnce the diagnosis has been made, it is usual toembark on a number of investigations, guidedin part by the history and especially taking intoaccount any previous chest or joint disease. AnX-ray of the chest, and a blood count, includingmeasurement of the erythrocyte sedimentationrate (ESR), are routine in most clinics, but theexpense of further investigations is now oftenspared if the patient appears completely fit andwell in other respects. The history and back-ground of the patient might lead one to suspectthe possibility of venereal disease. In the case of
some infective types of anterior uveitis, thediagnosis is usually made before the uveitisappears because the condition occurs as a sec-ondary event. This is the case following herpessimplex keratitis and also in patients withherpes zoster affecting the upper division of thefifth cranial nerve. By contrast, anterior uveitiscan be an important clue to the diagnosis of avenereal disease.
The treatment involves the administration oflocal steroids and mydriatic drops. When thecondition is severe, a subconjunctival injectionof steroid should be given and relief of symp-toms can be further achieved by local heat in theform of a warm compress.Atropine is the mydri-atic of first choice except in the mildest cases,when homatropine or cyclopentolate drops canbe used. Steroid drops should be administeredevery hour during the acute stage and thengradually tailed off over a period of a few weeks.Systemic steroids are not usually indicated andshould be reserved for those cases in which thesight becomes seriously jeopardised. If anyunderlying systemic disease is identified, then,of course, this should also be treated if effectivetreatment is available. The proper managementof anterior uveitis demands the expertise of aspecialist ophthalmologist and, when the condi-tion is affecting both eyes, it might be preferableto admit the patient to hospital.
A special word of warning is needed for thosepatients who have undergone previous intra-ocular surgery. For these patients, what is nor-mally a mild infective conjunctivitis can lead tointraocular infection. The development of anter-ior uveitis, weeks, and occasionally even years,after the operation, can indicate disastrous consequences if urgent and intensive antibiotictreatment is not applied.
Posterior UveitisSymptomsWhen the choroid,as opposed to the ciliary bodyand iris, becomes inflamed, the eye is not usuallypainful or red and the patient complains ofsevere blurring or loss of vision. If the focus ofchoroiditis remains peripheral, the diseasemight remain unnoticed, as is witnessed by therelatively frequent observation of isolatedhealed foci in the fundi of asymptomaticpatients. Often, the inflammation spreads from
144 Common Eye Diseases and their Management

choroid to retina and then to the vitreous.Whenthis happens the vision becomes markedlyblurred, even when the original focus is remotefrom the macula region. Alternatively, theinflammation might originate from the retinaand spread to involve the choroid and vitreoussubsequently. Choroiditis at the macula itselfusually leads to permanent loss of central vision.
SignsIn its early stages, choroiditis can be seen as agrey or yellowish raised area, which can be dis-crete or multiple and anywhere in the fundus. Acellular reaction could appear in the overlyingvitreous, seen as localised misting with theophthalmoscope, and eventually the whole vit-reous can become clouded, obscuring any viewof the fundus and the original site of inflamma-tion. The patient usually presents at this stage sothat the origin of the problem only becomesapparent after the inflammation has subsided.Retinitis manifests as an indistinct white cloudyarea. When a patch of choroiditis heals, themargins become pigmented and a white patchof bare sclera remains (Figure 18.4). This is theresult of atrophy of the pigment epithelium andchoroid. Sometimes larger choroidal vesselssurvive as a clearly seen network overlying thewhite sclera surrounded by a pigment halo.During the active stage, inspection of the vit-reous with the slit-lamp reveals the presence ofcells and often the anterior chamber also con-tains cells. Posterior uveitis comes into the dif-ferential diagnosis of a white eye with failingvision. When the vitreous becomes cloudy, thecondition must be distinguished from vitreoushaemorrhage. The latter nearly always occursacutely over a period of hours, whereas thecloudiness following uveitis takes a few days todevelop. Examination of the vitreous with theslit-lamp can reveal whether the vitreous isfilled with inflammatory cells or red cells.Retinal vasculitis can occur. A predominantlyarteriolar inflammation can indicate a viralcause, whereas venous involvement is morecommon with other aetiologies. Optic nerveinflammation or oedema can also occur.
CausesAs in the case of anterior uveitis, it is oftenimpossible to pinpoint any systemic cause andthe condition seems to be confined to the eye.
However, a number of systemic associationshave been recognised and often are related tospecific types of posterior uveitis.
ToxoplasmosisToxoplasma gondii is a parasite, a protozoancarried by cats. Man and other intermediatehosts can be infected. In the adult with theacquired infection, systemic symptoms areusually mild. Similarly, the ocular symptoms ofacquired toxoplasmosis can be mild. However, asevere form of acquired ocular toxoplasmosishas been recognised. In such cases, there hasbeen contact with wild cats in stables. In the caseof infected pregnant mothers, the child in utero
The Inflamed Eye 145
Figure 18.4. Chorioretinitis: a active with hazy vitreous;b inactive scar.
a
b
could be infected by the more severe congenitalform of the disease. The organism enters thebrain as well as the eyes and can cause mentaldeficiency and epilepsy. A characteristic type ofcalcification is seen on skull X-ray or computedtomography (CT) scan. In the eye, a focal typeof choroiditis often affects both eyes and this isusually at the posterior pole in the macularregion. Histologically, the toxoplasma organismis found in the eye lesions. The diagnosis can beconfirmed by sending some blood for serologi-cal tests. Four such tests are currently in useclinically: the toxoplasma dye test, indirectfluorescent antibody test, haemaglutination testand enzyme-linked immunosorbent assay(ELISA). These tests must be interpreted care-fully because a high proportion of the popula-tion becomes infected at some point and thepositive results increase with age, even in thosewith no clinical evidence of infection. For thisreason, the diagnosis can be less easy inacquired toxoplasmosis, where evidence of sys-temic involvement can be slight or absent. It hasbeen shown that there is a higher incidence ofpositive dye tests in patients with posterioruveitis than in the normal population, but in anindividual case it is often necessary to demon-strate a changing titre in order to confirm thediagnosis. The most specific of these tests is the ELISA.
All the currently available antitoxoplasmatreatments have potentially serious side effects.Therefore, not all active toxoplasma retino-choroiditis lesions require treatment. Suchtreatment is required only if an active lesioninvolves or threatens the fovea and/or opticnerve. Treatment is also required when there issevere vitritis.
A combination of pyrimethamine and sulfa-diazine has been recommended, but such treat-ment can cause a serious fall in the white cellcount. An alternative antimicrobial treatment isclindamycin. This needs to be given with a sul-fonamide in order to reduce the risk of colitis.Other antitoxoplasma agents include atova-quone. It is generally accepted that systemicsteroids have some beneficial effect and can help to clear the vitreous more rapidly, but thistreatment should be given only with antimicro-bial cover. Steroids on their own will produceexacerbation or progression of the chorioretin-itis. In fact, the majority of cases resolve spon-taneously, leaving more or less chorioretinal
scarring at the macular region. Recurrences arefairly common, with or without treatment, andthe fresh choroidal inflammation tends to ariseat the edge of a previous scar.
ToxocariasisToxocariasis is caused by Toxocara cati (fromcats) or T. canis (from dogs). This nematode hasbeen found in the enucleated eyes of youngpatients with a severe type of chorioretinitis.It is a unilateral disease found in children whoare in close contact with puppies or eat dirt(through faecal contamination). The vitreoustends to be filled with a white mass of inflam-matory cells so that the presence of a tumourmight be suspected (e.g., retinoblastoma). End-ophthalmitis tends to develop in these cases andthe sight of one eye might be completely lost.During the acute stage, the peripheral blood can show an eosinophilia. Treatment is un-satisfactory and includes a combination ofantihelminthic agent taken by mouth (thioben-dazole or diethylcarbamazine) and steroids.
TuberculosisIn former years this was considered to be acommon cause of posterior uveitis, clinicianshaving been impressed by the number of patientswith a previous history of tuberculosis. The rela-tionship seems less likely now that tuberculosishas been almost eliminated from the population.However, this diagnosis must not be forgottenespecially in the immunosuppressed patient and those with recalcitrant or atypical uveitis,as there is currently a slight re-emergence ofthe disease. Choroidal tubercles are a well-described entity: these raised yellowish granulo-matous foci were used as a diagnostic feature ofmiliary tuberculosis and, occasionally, chronicpulmonary tuberculosis.They are usually seen inextremely ill patients and the yellowish tuberclesbecome pigmented as they heal. Treatment is asfor systemic tuberculosis.
SarcoidosisThe eye is frequently involved in sarcoidosis.Involvement usually takes the form of an anterior or posterior uveitis. The choroiditis is more often peripheral and accompanied by
146 Common Eye Diseases and their Management
inflammatory changes in the retinal veins.Sheathing of the veins can be seen and thevision might be impaired by macular oedema.The inflammatory changes might be similar tothose seen in pars planitis. When the diagnosisis suspected, the conjunctiva and skin should besearched for possible nodules, which can bebiopsied, and an X-ray of the chest can revealenlargement of the hilar lymph nodes. Themanagement of the ophthalmological problemmight involve treatment with local and systemicsteroids but the opinion of a physician special-ising in sarcoidosis is essential and should besought before embarking on treatment.
Presumed Ocular HistoplasmosisHistoplasmosis is a fungal infection (causativeagent Histoplasma capsulatum). Infection withthis organism occurs throughout the world butis more common in the Mississippi Valley anddoes not occur in the UK. A severe pneumonitiscan occur but most cases are asymptomatic.
Presumed ocular histoplasmosis is not seenin patients with active histoplasmosis. The evi-dence for infection in the originally describedcases was necessarily circumstantial – hence theexpression “presumed ocular histoplasmosis”.The syndrome consists of a certain type ofhaemorrhagic macular lesion (choroidal neo-vascularisation) combined with discrete foci ofperipheral choroiditis and peripapillary scars.
SyphilisSyphilis is a chronic infection caused by Tre-ponema pallidum. Iridocyclitis occurs inpatients with secondary acquired syphilis. It is a bilateral disease in which the iris vessels areparticularly engorged. Chorioretinitis can beeither multifocal or diffuse and involves the mid periphery and peripapillary area. In thehealed phase, perivascular bone spicule pig-mentation could be seen similar to thatobserved in retinitis pigmentosa.
In congenital syphilis, other possible featuresoccur such as deafness and corneal scarringfrom previous interstitial keratitis. The scat-tered pigmentation in the fundus might suggestan inherited retinal degeneration but a carefulfamily history together with electrodiagnostictesting of the eyes usually enables one to distin-guish the two conditions. It is also important to
carry out serological testing. The T. pallidumimmobilisation test and the fluorescent tre-ponemal antibody test are the most sensitiveand specific.
Behçet’s DiseaseBehçet’s disease is a multisystem disease asso-ciated with HLA–B5. It was originally thought to occur only in the Mediterranean and Japan,where it is most common. It is characterised byan obliterative vasculitis. The clinical syndromeconsists of oral and genital ulceration in com-bination with recurrent uveitis and skin lesions.The uveitis consists of recurrent bilateral non-granulomatous anterior and/or posterioruveitis. Central nervous system involvementoccurs as a serious form of the disease.
Other CausesA wide variety of infective agents have beenshown to cause posterior uveitis on rare occa-sions. The leprosy bacillus and the coxsackiegroup of viruses are two examples chosen frommany. Sympathetic ophthalmia has already beenmentioned as a specific form of uveitis followinginjury. An especially rare but intriguing form ofuveitis is known as the Vogt–Koyanagi–Haradasyndrome, in which is seen the combination ofvitiligo, poliosis, meningo-encephalitis, uveitisand exudative retinal detachments.
The Role of Autoimmunity in UveitisAlthough it has been recognised for a long timethat bacterial and viral infection can account for some cases of uveitis, it has also been recognised that the majority of cases fail toshow any evidence of this. Furthermore, inmany instances the eye disease may be associ-ated with known autoimmune disease elsewherein the body. There are several different ways inwhich the uvea might be expected to become thefocus of an antigen–antibody reaction. Aforeign agent such as a virus might reside in theuvea and cause an antibody response, whichcoincidentally involves uveal tissue, or, on theother hand, a foreign agent might react with a
The Inflamed Eye 147

specific marker on the cell membrane toproduce a new active antigen. It is now recog-nised that patients who inherit certain of thehuman leucocyte antigens (HLA) are more sus-ceptible to particular types of uveitis, forexample the uveitis seen in ankylosingspondylitis and Reiter’s disease (HLA–B27). Ithas been suggested that HLA might act as thespecific marker in these cases. A further way inwhich the uvea might become the centre of animmune response concerns the question ofself-recognition. It now appears that there is a mechanism in the body that normally pre-vents antibodies in the serum from actingagainst our own tissues. This active suppressionis maintained by a population of thymus-derived lymphocytes (T lymphocytes) knownas T-suppressor cells. There is evidence tosuggest that sympathetic ophthalmitis mightarise from inhibition of the T-suppressor cellsafter uveal antigens have been introduced intothe bloodstream. Patients with juvenile rheum-atoid arthritis occasionally develop uveitis,whereas rheumatoid disease in adults is morecommonly associated with the dry eye syn-drome and episcleritis.
ManagementIncreased interest in immunological diseases inrecent years, which has accompanied advancesin tissue grafting and cancer research, has led to attempts to treat uveitis with means otherthan steroids. Immunosuppressive agents, suchas cyclosporin A, tacrolimus, azathioprine, andcyclophosphamide, are now sometimes used tosupplement or replace steroids in difficult cases.If posterior uveitis is not due to any recognisableinfective cause, it is usual to start treatment withsystemic steroids if the visual acuity becomessignificantly impaired or if the lesion is close to the macula. Large doses of systemic steroidsare best administered on an inpatient basis,especially if the sight is threatened. This has theadded advantage of allowing a more detailedpretreatment examination and investigations,and often the opinion of a general physician orimmunologist can be valuable at this stage.Secondary glaucoma might also need to betreated and immunosuppressive agents can beadministered to resistant cases. When posterioruveitis keeps recurring at the edge of previoushealed foci, laser coagulation has been used in
selected patients with toxoplasma retinocho-roiditis. The rationale of this treatment is todestroy any remaining encysted organisms.
Endophthalmitis andPanophthalmitisWhen inflammatory changes in the posterioruvea extend into the vitreous and there is anextensive involvement of the centre of the globe,the patient is said to have endophthalmitis.Further extension of the inflammation into theanterior segment of the eye and into the scleraleads to panophthalmitis. Endophthalmitis isone of the feared results of infection after injuryor surgery but it can prove reversible with inten-sive antibiotic treatment. When endophthal-mitis and panophthalmitis are not properly and aggressively treated, the sight is usually lost permanently and after months or years thewhole eye begins to shrink.
Episcleritis and ScleritisBoth these conditions form part of the differen-tial diagnosis of the red eye. The episclera is theconnective tissue underlying the conjunctivaand it can become selectively inflamed, eitherdiffusely or in localised nodules. In the case ofepiscleritis, close inspection of the eyes showsthat the inflammation is deeper than the con-junctiva and there is a notable absence of anydischarge. The eye is red and can be gritty butnot painful. Episcleritis is seen from time totime in the casualty department and the patient might be otherwise perfectly fit andwell. Such cases tend to recur and some developsigns of dermatological disease. The condi-tion responds to local steroids, but systemicaspirin can also prove effective. Scleritis is less common and more closely linked withrheumatoid arthritis and other collagen dis-eases. The eye is red (diffuse or localised) andpainful. In severe cases, the sclera can be-come eroded with prolapse of uveal tissue.Topical treatment is of no benefit. The conditionresponds to systemic anti-inflammatory agents,particularly oral flurbiprofen (Froben), whichcan be supplemented with systemic steroidsand/or immunosuppressants.
148 Common Eye Diseases and their Management

Although the eye and its supporting structuresundergo a number of well-defined changes withage, the distinction between these involutionalchanges and disease is not always clear cut. Forthe elderly patient, it is often reassuring to knowthat the problem is part of a “normal” processrather than the result of a specific illness andperhaps sometimes an artificial demarcation isdrawn for the benefit of the patient.
The increase in number of elderly peoplepresents problems in ophthalmology. A highproportion of elderly people instill drops intotheir eyes, either prescribed for them or as self-medication. It is important that adequateadvice is received. Advising the elderly is oftentime consuming and might entail speaking to ayounger relative or neighbour, but an adequateexplanation of the disease or problems willavoid anxiety and probably the need for furthersubsequent unnecessary consultation.
The three commonest diseases of the elderlyeye are cataract, glaucoma and age-relatedmacular degeneration (AMD). The first can becured, the second arrested or prevented, whilethe third generally tends to run a progressivecourse and treatment is unsatisfactory atpresent, although significant progress has beenmade recently. Attempts to measure the inci-dence of these problems have produced a widerange of figures. Out of a population of elderlypersons complaining of impaired vision, about30% turn out to have a cataract and a similarnumber to have AMD, whereas 5% or less havechronic open-angle glaucoma. Visual impair-
ment owing to glaucoma is more prevalent andoccurs at an earlier age in blacks than in whites.Although there is an unexpectedly high inci-dence of cataract in patients with chronicsimple glaucoma, the association of maculardegeneration with cataract or glaucoma is more random.
Changes in the Eyes with AgeThe External EyeThe eyelids tend to lose their elasticity andbecome less firmly opposed to the globe. Theupper and lower lid margins become progres-sively lower so that whereas in the infant theupper lid can ride level with or slightly above thecorneal margin, in an elderly subject the upperlid might cross a significant part of the uppercornea. An area of white can be seen betweenthe lower margin of the cornea and the lowerlid. Some limitation of the ocular movements is accepted as normal in the elderly, especiallylimitation of upward gaze. The conjunctivatends to become more lax and a thin fold of con-junctiva might be trapped between the lidswhen blinking if this becomes excessive. Insome elderly patients, there is loss of connectivetissue around the lacrimal puncta so that theopening is seen elevated slightly from the rest of the lid. Degenerative plaques are seen on the bulbar conjunctiva in the exposed region
19The Ageing Eye
149

and the conjunctiva is especially prone tochronic inflammation.
The GlobeArcus senilis is the name given to the circularwhite infiltrate seen around the margin of thecornea. The lens gradually loses its plasticitythroughout life and this results in a progressivereduction in the focusing power of the eye. Thisloss of focusing ability is also contributed to bythe progressive loss of ciliary muscle tone. Achild might be able to observe details of anobject held 5 cm from the eye, but as a result ofhardening of the lens and weakening of theciliary muscle, the nearest point at which anobject can be kept in focus gradually recedes.This progressive degeneration tends to passunnoticed until the eye is no longer able to focusto within the normal reading distance. Thisusually occurs at the age of 45 years if the eyesare otherwise normal, and the phenomenon iscalled presbyopia. Some degree of opacity ofthe lens fibres is common in old age and onlywhen this becomes more extensive is the term“cataract” used. The pupil becomes smaller withage and does not show the wide range of adjust-ment to illumination seen in younger people.The vitreous shows an increase in small opaci-ties visible to the subject as “vitreous floaters”.A more dramatic degenerative change, whichoccurs in a high proportion of normal individ-uals in the 60–70-year age group, is detachmentof the vitreous. The formed part of the vitreousseparates from the retina, usually above at first,leaving a fluid-filled gap between the retina andposterior vitreous face. Movement of the vitre-ous face can cause troublesome symptoms, forexample flashing lights and floaters, but often avitreous detachment goes unnoticed and is anincidental finding on examination of the eye.The important association between sudden vitreous detachment and subsequent retinaldetachment has already been discussed inChapter 13. The appearance of the fundus alsoshows gradual changes; the retinal arteriolesbecome straighter and narrower, as also do thevenules. Colloid bodies or drusen are more com-monly seen because of degenerative changes inBruch’s membrane and the pigment epithelium,and peripheral chorioretinal degeneration ismore evident. The young retina is more shinythan the old retina and in the elderly the normal
light reflex is less marked. The optic disc tendsto become somewhat paler and a degree of opticatrophy is accepted by many clinicians as a senilechange unrelated to disease.
Eye Disease in the ElderlyThe prevalence of blindness increases with age.The prevalence and causes of blindness alsovary from one community to another depend-ing on the age structure of the population andenvironmental conditions. In England andWales (1980), the prevalence of blindness wasfound to be nine per 100,000 children under fiveyears of age and 2324 per 100,000 individualsabove 75 years.
A recent survey in the USA has shown that theincidence of cataract in the 45–64-year-old population is 5.6% for males and 2.1% forfemales. The incidence is slightly higher in theNegro population, and rises to 21.6% for malesand 26.8% for females in the 65–75-year-oldpopulation. In the same age group (65–75 years),the incidence of AMD is 9.6% for males and 6.9% for females. Both these conditions are,therefore, common and they demand time andmedical expertise, both at the primary care leveland in hospital.
With increasing longevity throughout theworld, especially in the developing countries,there will be a continuing increase in thenumber of blind people, especially those suffer-ing from diseases related to age, such ascataracts, glaucoma and macular degeneration.
Age-related Macular DegenerationAMD is the commonest cause of incurableblindness in the elderly in western countries. Itis a bilateral disease in which visual loss in thefirst eye usually occurs at about 65 years of age.The second eye is involved at the rate of approx-imately 10% per annum and accounts for half ofall registered visual impairments in the UK.
There are two main types of AMD: “dry” oratrophic, and “wet” or neovascular. Blindness isusually associated with the wet form of AMD,and among the eyes with severe visual loss,80–90% of cases are because of wet AMD, while10–20% are because of the dry form.
Older patients with macular degenerationcomplain of blurring of their vision and inability
150 Common Eye Diseases and their Management

The Ageing Eye 151
to read. Younger or more observant patientsnotice that straight edges might look kinked.Usually one eye is considerably more affectedthan the other, although both eyes can be affected simultaneously. Because the degener-ative process is limited to the macula, the periph-eral field remains unaffected and the patient canwalk around quite normally. Difficulty in recog-nising faces or in seeing bus numbers is also acommon complaint. The wet form occurs morecommonly in Caucasians and about one-third ofthe patients give a family history of similar prob-lems. Several preventable factors, includingsmoking, systemic hypertension, cardiovasculardisease and low antioxidant intake, are asso-ciated with increased risk of AMD.
In the early stages of dry AMD, inspection ofthe fundus shows spots of pigment in themacular region. Drusen are also often seen(Figure 19.1). These are small round yellowishspots, often scattered over the posterior pole.Unfortunately, the word “drusen” has been usedrather loosely in ophthalmology to refer to twoor three types of swelling seen in the fundus. Itis used to describe the rare mulberry-liketumours seen around the optic nerve head intuberose sclerosis and it is also used when refer-ring to the multiple shiny excrescences seen onthe optic disc as a congenital abnormality.Drusen seen at the posterior pole of the eye asa senile change are also known as “colloidbodies” and perhaps this term is preferable.
Under the microscope, colloid bodies are seenas a degenerative change in Bruch’s membrane.Drusen can have varying degrees of hyperpig-mentation. Most eyes with drusen maintaingood vision, but a significant number willdevelop progressive atrophy of the retinalpigment epithelium (RPE) and choriocapillaris.This is inevitably associated with photoreceptorloss (Figure 19.2). There is usually a moderateloss of vision. This atrophic change in the RPE, choroid and photoreceptors is referred to as “dry” AMD. This is because there is noleakage of fluid or bleeding into the retina orsubretinal space.
In the “wet type” of macular degeneration a fan of new vessels arises from the choroid –choroidal neovascularisation (CNV).The growthof these new vessels seems to be importantbecause they invade the breaks in Bruch’s membrane. Serous or haemorrhagic exudatetends to occur and this can be either under theRPE or subretinal (Figure 19.3).A sudden loss ofcentral vision might be experienced as the resultof such an episode.Subsequently,“healing”of theleaking vascular complex results in scar tissueformation, which further destroys the centralvision permanently.
The terms “classic” and “occult” describe the different patterns of CNV leakage onfluorescein angiography.
Management
No effective treatment is available for dry AMD.There is an increasing vogue for administeringFigure 19.1. Drusen.
Figure 19.2. Dry macular degeneration.

vitamins A, C and E, selenium, copper, zinc,zeaxanthin, carotenoids and lutein preparationsto patients. These have been shown to protectagainst progression of dry AMD to moreadvanced stages of the disease in high-riskpatients. They are thought to reduce the dam-aging effects of light on the retina through theirreducing and free-radical scavenging actions.
Some types/stages of wet AMD are treatable.Currently, there are two clinically proven treat-ments for wet AMD, although the treatment forsome eyes is still unsatisfactory.
Controlled trials of the effect of laser photo-coagulation of the choroidal new vessels haveshown that this treatment is useful inextrafoveal CNV (i.e., when the leakage is notdirectly under the fovea). Laser photocoag-ulation ablates the CNV. It is important thatthose cases that are likely to benefit from treat-ment are first identified quickly. At the presenttime, this entails photography of the fundus and fluorescein angiography, and infraredangiography with indocyanine green. Often
patients present at the stage when new vesselshave already advanced across the macularregion to the subfoveal area or where the foveahas already been permanently damaged byhaemorrhage or exudate, making effective lasertreatment impossible. Only about 10–20% ofcases of CNV are eligible for laser photocoag-ulation. Another limitation of laser treatment isthe high rate of recurrence of the CNV within ashort time following treatment.
The second proven treatment is photo-dynamic therapy (PDT) with verteporfin (Visu-dyne). PDT specifically targets the CNVcomplex for damage by low-energy laser, butavoids damage to the unaffected tissue, includ-ing the photoreceptors. This treatment aims topreserve vision.
Apart from photocoagulation and PDT, thereare other treatment modalities currently underinvestigation. These include radiotherapy,thermal thermotherapy and drugs includingtriamcinolone, anercortave, and vascularendothelial growth factor (VEGF) aptamers or
152 Common Eye Diseases and their Management
Figure 19.3. Wet macular degeneration: a Fundus photograph:early disease. b Fundus photograph: advanced disease.c Fluorescein angiogram: early disease.
a
c
b

antagonists, which are delivered via injectionsinto the vitreous.
Practical measures can be taken in the man-agement of these patients to alleviate theirhandicap. Telescopic lenses might be needed forreading or watching television and full consid-eration should be given to the question of blindregistration. It is important to explain the natureof the condition and prognosis to the patient.This can alleviate considerable anxiety and fearof total blindness and help the patient come toterms with the problem. In most cases, one eyeis involved first, the other following suit withinone to three years. The vision, as measured onthe Snellen chart, progressively deteriorates toless than 6/60, but the peripheral field remainsunaffected so the patient is able to find his orher way about, albeit with some difficulty.
CataractThis common condition in the elderly eye hasalready been considered, but it is important thatevery physician can identify and assess thedensity of a cataract in relation to the patient’svision. The physician must realise the potentialof cataract surgery in the restoration of vision.Cataract surgery is required only if vision issufficiently reduced so far as to interfere withthe patient’s normal lifestyle. The contraindica-tions for cataract surgery are few and even inextreme old age the patient can benefit. Surgerymight be delayed if the patient has only one eyeor if there is some other pathology in the eye,which is likely to affect the prognosis. The needfor someone to assist the patient in the instil-lation of eye drops and the domestic choresduring the postoperative period might requiresome attention but is not a contraindication.About one-third of the population aged over 70years suffers from a cataract, but the quotedfigures vary according to the diagnostic criteria.If an elderly person has an opaque lens, whichobscures any view of the fundus with theophthalmoscope, and the pupil reacts quickly,then he or she is likely to do well after surgery.It is useful to remember that the reading visionis usually fairly well preserved even when thecataract is quite dense, and if the patient is unable to read, there might be coincidentalAMD, except if the cataract is of the posteriorsubcapsular type.
GlaucomaThe various types of glaucoma have also beenconsidered already, and the reader would realisethat glaucoma is simply the manifestation of agroup of diseases, each of which has a differentprognosis and treatment. Chronic simple, oropen-angle, glaucoma is the important kind inthe elderly because it often remains undiag-nosed. The physician and optometrist can playa vital part in the screening of this disease bybecoming familiar with the nature of glauco-matous cupping of the optic disc. About 1% ofthe population over the age of 55 years isthought to suffer from chronic simple glaucomaand the figure could rise to as high as 30% inthose over 75 years. In most instances, the treat-ment is simple but requires the co-operationand understanding of the patient. The treatmentis preventative of further visual loss rather thancurative. Chronic simple glaucoma is bestmanaged in an eye unit on a long-term basis. Bythis means, the visual fields and intraocularpressure can be accurately monitored and thetreatment adjusted as required. More recently,the care of glaucoma patients is being sharedbetween hospital units and selected (trained)optometrists in the community.
Deformities of the EyelidsBoth entropion and ectropion are common inthe elderly and a complaint of soreness and irritation in the eyes as well as watering shouldalways prompt a careful inspection of theconfiguration of the eyelids. Entropion isrevealed by pressing the finger down on thelower lid so that the inverted lid becomeseverted again to reveal the lash line. Sometimesentropion can be intermittent and not present atthe time of examination, but usually under thesecircumstances there is a tell-tale slight inversionof the lid, which is made apparent by compar-ing the two sides. Ectropion is nearly always anobvious deformity because of the easy visibilityof the reddened and everted conjunctiva, butslight degrees of ectropion are less obvious. Thelower punctum alone can be slightly everted,causing a watering eye, and the symptoms mightbe relieved by applying retropunctal cautery tothe conjunctiva. Both ectropion and entropionrespond well to lid surgery and there is no
The Ageing Eye 153

reason why geriatric patients should put up withthe continued discomfort and irritation when a complete cure is readily available. These liddeformities can recur sometimes and requirefurther lid surgery, but careful surgery in thefirst instance should largely prevent this.
Temporal ArteritisThis condition, also known as giant cell arter-itis, seen only in the elderly, can rapidly causetotal blindness unless it is treated in time. Thedisease is more common than was originallysupposed but it is rare under the age of 50 years.Medium-sized vessels, including the temporalarteries, become inflamed and the thickening ofthe vessel wall leads to occlusion of the lumen.Histologically, the inflammatory changes arecharacterised by the presence of foreign bodygiant cells and the thickening of the vessel wallis at the expense of the inner layers so that thetotal breadth of the vessel might not be altered.In early disease, the inflammatory changes tendto be segmental so that a single biopsy of a smallsegment of the temporal artery does not alwaysreveal the diagnosis.
Patients with temporal arteritis usuallypresent in the eye department with blurring ofvision or unilateral loss of vision. Typically,these symptoms are accompanied by headacheand tenderness of the scalp so that brushing thehair might be painful. Often there is low-gradefever and there can be aches and pains in themuscles and joints, as well as other evidence ofischaemia in the brain and heart. Scalp ulcera-tion and jaw claudication can occur. The blur-ring of vision is caused by ischaemia of the opticnerve head or occasionally central retinal arteryocclusion. The diagnosis rests largely on findinga raised erythrocyte sedimentation rate (ESR),elevated C-reactive protein levels and a positivetemporal artery biopsy in an elderly patientwith these symptoms. Palpation of the temporalarteries reveals tenderness and sometimesthickening and the absence of pulsation is auseful sign. Polymyalgia rheumatica is a syn-drome consisting of muscle pain and stiffnessaffecting mainly the proximal muscles withoutcranial symptoms.
Inspection of the fundus in a patient withvisual symptoms shows pallor and oftenswelling of the optic nerve head and narrowingof the retinal arterioles (Figure 19.4). Once the
disease is suspected, a biopsy is essential andthis should be done without delay. Treatmentcan be commenced immediately, sometimeseven before biopsy. However, it is advisable thatthe lag between starting treatment and biopsy is as short as possible (preferably less than two weeks). The symptoms disappear rapidlyafter administering systemic steroids, initiallyin a high dose (e.g., prednisolone 120 mg per day), and the dosage is then reduced rapidly according to the level of the ESR. Oncethe ESR is down to normal levels, a mainten-ance dose of systemic steroids is continued,if necessary for several months (on average 18 months).
Temporal arteritis is recognised as a self-limiting condition. About one-quarter of allpatients are liable to become blind unless ade-quate treatment is administered and in someinstances, extraocular muscle palsies causingdiplopia and ptosis can confuse the diagnosis.For simplicity, one might summarise the diseaseby saying it causes headache in patients aged over70 years with an ESR over 70 and who requiretreatment with over 70 mg of prednisolone.
StrokePatients who complain of visual symptoms aftera stroke quite often have an associated homony-mous hemianopia and the association betweenhemiplegia and homonymous hemianopiashould always be borne in mind. A simple con-frontation field test might be all that is requiredto confirm this in a patient with poor vision and
154 Common Eye Diseases and their Management
Figure 19.4. Giant cell arteritis: ischaemic optic neuropathy.

normal fundi following a hemiplegic episode.The vertical line of demarcation between blindand seeing areas is well defined and can cutthrough the point of fixation. Fortunately, thecentral 2° or 3° of the visual field are oftenspared. When there is so-called macular spar-ing, the visual acuity as measured by the Snellenchart can be normal. Patients tend to complainof difficulty in reading if the right homonymousfield is affected rather than the left, andalthough they might be able to read individualwords, they have great difficulty in following the line of print. Thus, a patient with a righthemiplegia and a right homonymous hemi-anopia might have normal fundi and visual
acuity of 6/6 and yet be unable to read the news-paper. The picture can be further complicatedby true dyslexia and the patient might admit tobeing able to see the paper and yet be unable tomake any sense of it. Dyslexia might be sus-pected if other higher functions, such as speech,have been affected by the stroke. One of the fea-tures of a homonymous hemianopic defect inthe visual field is the patient’s complete lack ofinsight into the problem, so that even a doctormight fail to notice it in himself. It is unusual fora homonymous hemianopia to show any signsof recovery, but once the patients understandthe nature of the handicap they can learn toadapt to it to a surprising degree.
The Ageing Eye 155
How the Normal FeaturesDiffer from Those in an AdultAt birth the eye is large, reaching adult size atabout the age of two years. One might expectthat before the eye reaches its adult size, it wouldbe long-sighted, being too small to allow paral-lel rays of light to be brought to a focus on theretina. In actual fact, the immature lens is moreglobular and thus compensates for this by itsgreater converging power. None the less, morethan three-quarters of children aged under fouryears are slightly hypermetropic. The slightchange of refractive error that occurs as theygrow compares with the more dramatic changein axial length from 18 mm at birth to 24 mm inthe adult. The slight degree of hypermetropiaseen in childhood tends to disappear in adoles-cence. Myopia is uncommon in infancy buttends to appear between the ages of six and nineyears and gradually increases over subsequentyears. The rate of increase of myopia is maximalduring the growing years and this can often bea cause of parental concern.
The iris of the newborn infant has a slate-greycolour because of the absence of stromal pig-mentation. The normal adult colouration doesnot develop fully until after the first year. Thepupil reacts to light at birth but the reaction canbe sluggish and it might not dilate effectively inresponse to mydriatic drops. The fundus tendsto look grey and the optic disc somewhat pale,deceiving the uninitiated into thinking that it is
atrophic. The foveal light reflex, that is the spotof reflected light from the fovea, is absent or ill-defined until the infant is four to six months old.By six months the movement of the eyes shouldbe well co-ordinated, and referral to an ophthal-mologist is needed if a squint is suspected.Once children learn to identify letters, at the ageof four or five years, the Snellen chart can beemployed to measure visual acuity, which bythis age is normally 6/9 or 6/6. The Stycar testcan be used for three- to four-year olds or sometimes younger children and a similar levelof visual acuity is seen as soon as the child isable to co-operate with the test conditions.Stycar results tend to be slightly better thanSnellen results when measured in the samechild, perhaps because the Stycar test involvesseeing a single letter rather than a line.
How to Examine a Child’s EyeThe general examination of the eye has beenconsidered already, but in the case of the child,certain aspects require special consideration.Before the age of three or four years, it might notbe possible to obtain an accurate measure of thevisual acuity, but certain other methods thatattempt to measure fixation are available. Therolling ball test measures the ability of the childto follow the movement of a series of white balls graded into different sizes. Another testmakes use of optokinetic nystagmus, which canbe induced by making the child face moving
20The Child’s Eye
157

vertical stripes on a rotating drum. The size ofthe stripes is then reduced until no movementof the eyes is observed. In practice, a carefulexamination of the child’s ability to fix a light,and especially the speed of fixation, is helpful.The behaviour of the child can also be a helpfulguide, for example the response to a smile or the recognition of a face. Sometimes grosslyimpaired vision in infancy is overlooked orinterpreted as a psychiatric problem, but suchan error can usually be avoided by carefulophthalmological examination. The reaction ofthe pupils is an essential part of any visualassessment. One of the difficulties in examiningchildren is that they are rarely still for more thana few seconds at a time, and any attempts atrestraint usually make matters worse. Beforestarting the examination, it is useful to gain thechild’s confidence by talking about things thatmight interest him or her, not directly but inconversation with the parent. In fact, it is sometimes better to ignore the anxious childdeliberately during the first few minutes of theinterview. Once the young patient has summedyou up, hopefully in a favourable light, then agentle approach in a quiet room is essential forbest co-operation. The cover test can only beperformed well under such conditions and oncethis has been done the pupils and anterior partof the eye can be examined, first with a handlens but if possible with the slit-lamp micro-scope. Fundus examination and measurementof any refractive error demand dilatation ofthe pupils and paralysis of accommodation.Cyclopentolate 1% or tropicamide 1% are bothused in drop form for this purpose. The indirectophthalmoscope is a useful tool when examin-ing the neonatal fundus, the wide field of viewbeing an advantage in these circumstances. Ifthe infant is asleep in the mother’s arms, this can be beneficial because it is a simple matter to raise one eyelid and peer in without wakingthe patient. In the case of children between theages of three and six years, fundus examinationcan be more easily achieved by sitting down andasking the standing patient to look at some spotor crack on the wall while the optic disc islocated. On some occasions the child hasbecome too excited or anxious to allow a properexamination and here one might have to decidewhether it is reasonable to postpone the exam-ination for a week or whether the matter seemsurgent enough to warrant proceeding with an
examination under anaesthesia. A casualty situation, which occurs from time to time, iswhen a child is brought in distressed with a sus-pected corneal foreign body or perhaps a per-forating injury. Here, it is simplest to wrap thepatient in a blanket so as to restrain both armsand legs and then examine the cornea byretracting the lids with retractors. Particularcare must be taken when examining an eye with a suspected perforating injury in view ofthe risk of causing prolapse of the contents ofthe globe. Any ophthalmological examinationdemands placing one’s head close to that of thepatient and this can alarm a child unless it isdone sufficiently slowly and with tact. It is some-times helpful to make the child listen to a smallnoise made with the tongue or ophthalmoscopeto ensure at least temporary stillness.
Screening of Children’s EyesIn an ideal world, all children’s eyes would beexamined at birth by a specialist and again at sixmonths to exclude congenital abnormalities andamblyopia.This is rarely achieved,although mostchildren in the UK are examined by a nonspe-cialist at these points. Most children are alsoscreened routinely in school at the age of sixyears, and any with suspected poor vision arereferred for more detailed examination. Afurther examination is often conducted at the ageof nine or ten years and again in the early teens.The commonest defect to be found is refractiveerror,that is simply a need for glasses without anyother problem. The ophthalmological screeningis usually performed by a health visitor in thepreschool years and a school nurse for older chil-dren.Screening tends to include measurement ofvisual acuity alone but checking any availablefamily history of eye problems would be helpful.When there is a difference in the visual acuity ofeach eye, the screener should suspect the possi-bility of a treatable medical condition rather thanjust a refractive error. A test of colour visionshould also be included in the screening pro-gramme for older children and this can be con-veniently done using the Ishihara plates. It isworth remembering that colour blindness affects8% of men and 0.4% of women and it might haveimportant implications on the choice of a job. Itis also equally important to realise that colourblindness can vary considerably in degree and
158 Common Eye Diseases and their Management
can often be so mild as to cause only minimalinconvenience to the sufferer.
Congenital Eye DefectsLacrimal ObstructionThe watering of one or both eyes soon after birthis a common problem. The obstruction is nor-mally at the lower end of the nasolacrimal duct,where a congenital plug of tissue remains. Infec-tion causing purulent discharge can be treatedeffectively by the use of antibiotic drops.Although these should clear the unpleasant dis-charge, the eye continues to water as long as thetear duct is blocked. The mother can be shownhow to massage the tear sac. This manoeuvrecauses mucopurulent material to be expressedfrom the lower punctum when there is a block-age and can be used as a diagnostic test. Ifcarried out regularly, this helps to relieve theobstruction. In most cases, spontaneous reliefof the obstruction occurs, but if this does notoccur after about six to nine months, probingand syringing of the lacrimal passageway undergeneral anaesthesia is an effective procedure,which can be done as a day case. It is importantto remember that a watering eye can be causedby excessive production of tears as well as inade-quate drainage, and in a child, a corneal foreignbody or even congenital glaucoma might be mis-taken for lacrimal obstruction by the unwary.
EpicanthusThis relatively minor defect at the medialcanthus is formed by a bridge of skin runningvertically. This is seen normally in some orien-tal races. In Europeans it usually disappears asthe bridge of the nose develops, but its impor-tance lies in the fact that it can give the mis-leading impression that a squint is present.Severe epicanthus can be repaired by a plasticprocedure on the eyelids.
PtosisCongenital drooping of the eyelid can be uni-lateral or bilateral and sometimes shows a dominant inheritance pattern. The ptosis can beassociated with other lid deformities. Referralfor surgery is indicated if there is significant
head tilt and especially if the lid covers thevisual axis. See Chapter 5 for more informationabout eyelid deformities.
Congenital NystagmusChildren with congenital nystagmus are usuallybrought to the department because their parentshave noticed that their eyes seem to be continu-ously wobbling about. Such abnormal and per-sistent eye movements might simply occurbecause the child cannot see (sensory nystag-mus) or they might be caused by an abnormalityof the normal control of eye movements (motornystagmus). It is important to distinguish con-genital nystagmus from acquired nystagmusbecause of a space-occupying intracranial lesion.
Sensory Congenital Nystagmus
The roving eye movements are described aspendular, the eyes tending to swing from side toside. Examination of the eyes reveals one of thevarious underlying causes: congenital cataract,albinism, aniridia, optic atrophy or other causesof visual impairment in both eyes. A specialkind of retinal degeneration known as Leber’samaurosis can present as congenital nystagmus.The condition resembles retinitis pigmentosa,being a progressive degeneration of the rodsand cones, and occurs at a young age. It tends tolead to near blindness at school age. Patientswith congenital nystagmus usually need to beexamined under general anaesthesia, and elec-troretinography (a technique that can detectretinal degenerations at an early stage) shouldbe performed at the same time.
Motor Congenital Nystagmus
The exact cause of this type of nystagmus isusually never ascertained but a proportion ofsuch cases show recessive inheritance. Otherabnormalities might be present, such as mentaldeficiency, but many children are otherwiseentirely normal. The nystagmus tends to bejerky, with the fast phase in the direction of gazeto the right or left. The distance vision is usuallyimpaired to the extent that the patient mightnever be able to read a car number plate at 23 m. The near vision, on the other hand, isusually good, enabling many patients with thisproblem to graduate through university.
The Child’s Eye 159
Spasmus Nutans
This term refers to a type of pendular nystag-mus, which is present shortly after birth andresolves spontaneously after one or two years.Like other forms of congenital nystagmus, it canbe associated with head nodding.
Albinism
The lack of pigmentation might be limited tothe eye, ocular albinism, or it might be gener-alised. The typical albino has pale pink skin andwhite hair, eyebrows and eyelashes. There isoften congenital nystagmus. The optic fundusappears pale and the choroidal vasculature iseasily seen. The iris has a grey–blue colour butthe red reflex can be seen through it, giving theiris a red glow. Albinism is inherited in a reces-sive manner and can be partial or complete.Albinos need strong glasses to correct theirrefractive error, which is usually myopic astig-matism. Dark glasses are also usually requiredbecause of photophobia. Tinted contact lensescan sometimes be helpful.
Structural Abnormalities of the GlobeThere are many different developmental abnor-malities of the globe but most of these are for-tunately rare. Coloboma refers to a failure offusion of the foetal cleft of the optic cup in theembryo. Coloboma of the iris is seen as akeyhole-shaped pupil and the defect can extendinto the choroid, so that the vision might beimpaired. Inspection of the fundus reveals anoval white area extending inferiorly from theoptic disc. Children can be born without an eye(anophthalmos) or with an abnormally smalleye (microphthalmos). It is always important tofind out the full extent of this type of abnor-mality and if the mother has noticed somethingamiss in the child’s eye, referral to a paediatricophthalmologist is required without delay.Often a careful discussion of the prognosis withboth parents is needed.
Aniridia
Aniridia (congenital absence of the iris) can beinherited as a dominant trait and can be asso-ciated with congenital glaucoma.The lens can besubluxated or dislocated from birth. This might
be suspected if the iris is seen to be tremulous.This strange wobbling movement of the iris usedto be seen in the old days after cataract surgerywithout an implant, but it is now still seen afterinjuries to the eye and signifies serious damage.Congenital subluxation of the lens is seen as part of Marfan’s syndrome (congenital heartdisease, tall stature, long fingers, high archedpalate). Congenital glaucoma has already beendiscussed in the chapter on glaucoma; it can beinherited in a dominant manner and is the resultof persistent embryonic tissue in the angle of theanterior chamber. When the intraocular pres-sure is raised in early infancy, the eye becomesenlarged, producing buphthalmos (“bull’s eye”).This enlargement with raised pressure does notoccur in adults.
Congenital Cataract
The lens can be partially or completely opaqueat birth. Congenital cataract is often inheritedand can be seen appearing in a dominantmanner together with a number of other con-genital abnormalities elsewhere in the body. Thecondition might also be acquired in utero, thebest known example of this being the cataractcaused by rubella infection during the firsttrimester of pregnancy: remember the triad ofcongenital heart disease, cataract and deafnessin this respect. Minor degrees of congenitalcataract are sometimes seen as an incidentalfinding in an otherwise normal and symptom-less eye. The nature of the cataract usually helpswith the diagnosis. The lens fibres are laid downfrom the outside of the lens throughout life. Ifthe opaque lens fibres are laid down in utero,this opaque region can remain in the centre ofthe lens. Only when the cataract is thick does itpresent as a white appearance in the pupil andoften it is difficult to detect it. It is important toexamine the red reflex and see whether thedarker opaque lens fibres show up. The surgeonhas to decide whether the vision of the child hasbeen significantly affected and unless thecataracts are dense it might be better to waituntil the school years approach in order toobtain a more accurate measure of the vision.Sometimes the vision can turn out to be sur-prisingly good with apparently dense cataracts.The surgical technique is similar to that forcataract surgery in the adult. Before the intro-duction of lens implants, the risk of developinga retinal detachment in later life was high in
160 Common Eye Diseases and their Management

these patients. When the cataract is unilateral,this presents a special case because the affectedeye tends to be amblyopic, thus preventing auseful surgical result.
Other Eye Conditions in ChildhoodAbnormalities of RefractionNowadays children whose vision is impairedbecause they need a pair of glasses are usuallydiscovered by routine school testing of theirvisual acuity. They might also present to thedoctor because the parents have noticed themscrewing up their eyes or blinking excessivelywhen doing their homework. Some children cantolerate quite high degrees of hypermetropiawithout losing visual acuity simply by exercis-ing their accommodation, and unless thereappears to be a risk of amblyopia or squint,glasses might not be needed. By contrast, evenslight degrees of myopia, if both eyes areaffected, can interfere with school work. Myopiadoes not usually appear until between the agesof five and 14 years, and most commonly atabout the age of 11.
SquintThis exceedingly common inherited problem ofchildhood has already been considered, but it isworth summarising some of the main features.All cases of squint require full ophthalmologicalexamination because the condition can be asso-ciated with treatable eye disease,most commonlyamblyopia of disuse. There is no reason why anypatient,child or adult,should suffer the indignityof looking “squint eyed” because the eyes can bestraightened by surgery. In spite of this, it is notalways possible to restore the full simultaneoususe of the two eyes together (binocular vision).In general, the earlier in life that treatment isstarted, the better the prognosis.
Amblyopia of DisuseThis has been defined as a unilateral impair-ment of visual acuity in the absence of any otherdemonstrable pathology in the eye or visualpathway. This rather negative definition fails toexplain that there is a defect in nerve conduc-tion because of inadequate usage of the eye in
early childhood. The word “amblyopia” meansblindness and tends to be used rather loosely byophthalmologists. It is most commonly used torefer to amblyopia of disuse (“lazy eye”) but itis also used to refer to loss of sight caused bydrugs. Amblyopia of disuse is common andsome patients even seem unaware that they haveany problem until they suffer damage to theirsound eye. This weakness of one eye resultswhen the image on the retina is out of focus orout of position for more than a few days ormonths in early childhood or, more specifically,below the age of eight years. Amblyopia ofdisuse, therefore, arises as the result of a squintor a one-sided anomaly of refraction, or it canoccur as the result of opacities in the opticalmedia of the eye. A corneal ulcer in the centreof the cornea of a young child can rapidly leadto amblyopia. Once a clear image has been pro-duced on the retina, either by the wearing ofspectacles or other treatment, the vision in theweak eye can be greatly improved by occludingthe sound eye. The younger the patient, thebetter are the chances of improving the visionby occlusion. Beyond the age of eight years it isunlikely that any significant improvement canbe achieved by this treatment and, by the sametoken, it is unlikely that amblyopia will appearafter the age of eight years.An adult could suffertotal occlusion of one eye for several monthswithout experiencing any visual loss in theoccluded eye.
LeucocoriaThis term means “white pupil” and it is animportant sign in childhood. There are anumber of conditions that can produce thiseffect in early childhood. The important thing torealise is that if a mother notices “somethingwhite” in the pupil, the matter must never beoverlooked and requires immediate investiga-tion. The differential diagnosis includes con-genital cataract, opaque nerve fibres in theretina, retinopathy of prematurity, endophthal-mitis, some rare congenital abnormalities ofthe retina and vitreous and, not common butmost important, retinoblastoma.
Retinopathy of PrematurityIn the early 1940s, premature infants withbreathing difficulties began to be treated withoxygen, and 12 years elapsed before it was
The Child’s Eye 161

realized that the retinopathy seen in prematurechildren was caused by this treatment. Duringthe course of oxygen therapy in a prematureinfant, the retinal vessels become narrowed andthe optic disc becomes pale. When the oxygentreatment is stopped, the retinal vessels becomeengorged and new vessels grow from theperipheral arcades in the extreme periphery ofthe fundus. This growth of abnormal vesselsleads to vitreous haemorrhage, retinal detach-ment and fibrosis of the retina. The infant canrapidly become blind, although some are mini-mally affected. The management of the con-dition now involves screening of those childrenat risk and monitoring of blood oxygen levels.When the condition occurs, treatment withcryotherapy to the peripheral retina has beenshown to be beneficial. Now that children arebeing born at an earlier and earlier stage, itseems that extreme prematurity runs the risk ofblindness from this cause even in the absence ofsupplementary oxygen.
Ophthalmia NeonatorumIt is important to realise that in the early part ofthis century, a large proportion of the inmatesof blind institutions had suffered from oph-thalmia neonatorum. The disease affects pri-marily the conjunctiva and cornea and is theresult of infection by organisms resident in thematernal birth passage. The gonococcus was the most serious cause of blindness but anumber of other bacteria have been incrimi-nated, including staphylococci, streptococci andpneumococci. It has also been shown thatchlamydial infection of the genital tract can lead to the same problem, as can infection by the herpes simplex virus. The blindness thatresulted from this condition was so serious thatany excessive discharge from the eyes has beena notifiable disease in this country since 1914.Ophthalmia neonatorum is caused by unhy-gienic conditions at birth and its relative raritynowadays is because of the fact that midwivesare trained to screen for the condition. Bacter-ial conjunctivitis usually occurs between thesecond and fifth day after birth, whereaschlamydial infection tends to occur a little later,between the sixth and tenth day. Purulent ormucopurulent discharge is evident and theeyelids can become tense and swollen so that itis difficult to open them and carry out the all-
important examination of the cornea. When thedisease is suspected, the infant should be admit-ted to hospital and treated with penicillin dropsevery hour. Diagnosis is achieved by taking aconjunctival culture before treatment is startedand by looking for the inclusion bodies of thechlamydial virus in a smear. The history ofinfection in the parents needs to be exploredand managed by a genitourinary specialist.
UveitisUveitis is rare in childhood; it can take the formof choroiditis, sometimes shown to be becauseof toxoplasmosis or toxocara, or the form ofanterior uveitis sometimes associated withStill’s disease. The management of these cases issimilar to that of the adult, but recurrences canresult in severe visual loss in spite of treatment.
Optic AtrophyOne must be rather wary about the diagnosis ofoptic atrophy in young children because theoptic discs tend to look rather pale in normalindividuals. Occasionally, unilateral visual losswith or without a squint is found to be associ-ated with pallor of the disc on one side.Confirmed optic atrophy, either unilateral orbilateral, requires a full neurological investig-ation. The causes of optic atrophy in childhoodare numerous but the important ones can belisted as follows:
• Causes of optic atrophy without systemicdisease include:
– hereditary optic atrophy– drug toxicity.• Causes of optic atrophy with systemic
disease include:– glioma of chiasm and craniopharyngioma– post meningitic– post traumatic after head injury– hydrocephalus– cerebral palsy– disorders of lipid metabolism.
Juvenile Macular DegenerationThis is a rare cause of progressive visual loss inchildren, the diagnosis being made perhaps
162 Common Eye Diseases and their Management

once in a lifetime at primary care level. For thisreason, the diagnosis can easily be missed, esp-ecially as the patient finds difficulty in readingbut no difficulty in walking around. Some casesshow dominant inheritance and so the familyhistory can be important.
The PhakomatosesThe three conditions – Von Recklinghausen’sneurofibromatosis, tuberose sclerosis (Bourn-ville’s disease) and Von Hippel–Lindau disease –are classed together under this name. They allinvolve the eye but might not become evidentuntil later life. Often, examination of the eye
reveals the diagnosis. In Von Recklinghausen’sneurofibromatosis, multiple neuro-fibromataare seen on the skin, and the eyelids may beenlarged and distorted. Gliomata can develop inthe optic nerves and scattered pigment “cafe aulait” patches are seen in the skin. Brown nodulescan be seen on the iris. In tuberose sclerosis,mental deficiency and epilepsy are associatedwith a raised nodular rash on the cheeks andmulberry-like tumours in the optic fundus. VonHippel–Lindau disease presents to the ophthal-mologist as angiomatosis retinae. Vasculartumours appear in the peripheral retina,which can leak and expand and lead to detach-ment of the retina. Similar tumours can bepresent intracranially.
The Child’s Eye 163
DiabetesDiabetes mellitus affects 1–2% of the UK popu-lation. The disease is more prevalent in othercountries. Diabetic retinopathy is the common-est cause of legal blindness in patients betweenthe age of 20 and 65 years such that about 1000people are registered blind from diabetes peryear in the UK. The management of diabetic eyedisease has improved greatly over the past 20years so that much of the blindness can now beprevented. In spite of this, most general prac-titioners are aware of tragic cases of rapidly pro-gressive blindness in young diabetics. The moreserious manifestations of diabetes in the eyetend to affect patients in the prime of life. Thetragedy is even greater when one considers thatthis blindness is largely avoidable.
Diabetes is, therefore, the most important sys-temic (noninfective) disease that gives rise toblindness. Many diabetics remain free of eyeproblems, but a diabetic is 25 times more likely to become blind than other members ofthe population.
When taking an eye history from diabeticpatients, it is especially important to note theduration of the diabetes and the age of onset,because the incidence of diabetic retinopathy ismost related to the duration of diabetes. Otherrisk factors are listed in Table 21.1.
Diabetic retinopathy is extremely rare underthe age of ten years; it does not usually appearuntil the disease has been present for someyears. Juvenile-onset diabetics usually take
longer to show eye changes than those with alate onset.
Although diabetic retinopathy is the mostserious ocular complication, the eye can beaffected in a number of other ways and it is con-venient to consider the various ocular manifes-tations of diabetes in an anatomical manner,beginning anteriorly.
EyelidsIt is usual to check the urine of patients pre-senting with recurrent styes but in practice, it isunusual for diabetes to be diagnosed in this way.Xanthelasma of the eyelids is said to be slightlymore common in diabetics.
Ocular MovementsElderly diabetic patients are more prone todevelop transient third and sixth cranial nervepalsies than nondiabetics of the same age group.Sometimes isolated third nerve palsy can bepainful and the pupil is spared. A fasting bloodsugar might be required in patients presentingwith isolated third nerve palsies. Hypertensionand arteriosclerosis need exclusion.
Cornea and ConjunctivaSome diabetics have microcirculatory changes,for example conjunctival vascular irregularityand dilatation. Corneal ulcers in diabetics canprove particularly troublesome. Minor trauma
21Systemic Disease and the Eye
165

to the cornea can lead to the formation of indo-lent chronically nonhealing or infected ulcers,which respond slowly to intensive treatmentwith local antibiotics. Inadequate treatment canlead to endophthalmitis and loss of the eye. Thisproblem occurs especially in diabetics withsevere vascular disease and typically in a patientwho has had to have a gangrenous leg removed.
Anterior ChamberA particular kind of iritis is occasionally seen indiabetics after cataract surgery when there is asevere plastic reaction. It is important that suchcases are treated adequately to prevent thedevelopment of posterior synechiae, which willmake subsequent fundal examination difficult.Many surgeons consider it advisable, therefore,to use mydriatic drops (cyclopentolate) aftercataract surgery in diabetics.
IrisThe iris itself often shows degenerative changesin longstanding diabetics. The pupil can reactsluggishly and fail to dilate widely after theinstillation of mydriatic drops. The surgeon canappreciate that pigment is easily lost from theiris when it is handled, and it is interesting thata characteristic vacuolation of the pigmentepithelium lining the posterior surface of theiris is seen in histological sections. When dia-betes seriously interferes with the circulation ofthe eye, the iris can become covered on its anter-ior surface by a fibrovascular membrane. To thenaked eye, the iris takes on a pinkish colour, butexamination with the slit-lamp biomicroscopeor a magnifying lens soon reveals the minuteirregular blood vessels on its surface. Theappearance is known as “rubeosis iridis” or neovascularisation of the iris (Figure 21.1). Neo-vascular glaucoma occurs once the rubeosis
involves the anterior chamber angle. If leftuntreated, few eyes with rubeosis iridis retainuseful sight. The iris should be examined care-fully before pupillary dilation.
LensIt was mentioned in an earlier chapter that diabetics tend to develop senile cataracts at anearlier stage than normal. Once developed,cataracts also progress more quickly in diabet-ics compared with nondiabetics. In addition, arapidly advancing type of cataract is seen inyoung poorly controlled patients. This is a truediabetic cataract. This cataract is bilateral andconsists of snowflake posterior or anterior opac-ities, matures rapidly and is similar to the rarecataract seen in starvation from whatever cause.The routine testing of urine of patients withcataracts produces a good return of positiveresults, making this an essential screening test.
It was also mentioned in a previous chapterthat the refractive power of the lens mightchange in response to a rise in the blood sugarlevel. This results from increased hydration ofthe lens in patients with high uncontrolledblood sugar levels. Undiscovered diabetics quiteoften become short-sighted because of this so-called index myopia. They can then obtain somedistance glasses and subsequently consult theirdoctor, who treats their diabetes. By this timethe glasses are made and, of course, turn out tobe unsatisfactory, because the index myopia can improve with treatment. In some instancesindex myopia proves irreversible, being the firstsign of cataract formation.
166 Common Eye Diseases and their Management
Table 21.1. Risk factors for diabetic retinopathy.
• Age• Duration of diabetes• Smoking• Hypertension• Poor diabetic control• Hyperlipidaemia• Renal impairment• Pregnancy
Figure 21.1. Rubeosis iridis.

Retina and VitreousDiabetic retinopathy is the most serious compli-cation of diabetes in the eye and often reflectssevere vascular disease elsewhere in the body.There are two kinds of diabetic retinopathy:background and proliferative. Background re-tinopathy is common when diabetes has beenpresent for some years and is less of a threat tothe sight than the proliferative variety. Diabeticmaculopathy is a special form of retinopathy thatcan occur with either background or prolifera-tive disease. It is important that the doctor is ableto recognise diabetic retinopathy and especiallyimportant that he or she should be familiar withthe warning signs that indicate proliferativechanges and significant maculopathy.
Diabetic retinopathy is essentially a smallvessel disease affecting the retinal precapillaryarterioles, capillaries and venules. The largervessels can be involved. The vascular disease cantake the form of vascular leakage or closure,with resultant ischaemia, or both.
Background RetinopathyThere are usually no ophthalmic symptoms initially, but inspection of the fundi of most dia-betics who have had the disease for ten years ormore reveals, at first, a few microaneurysms.They are often on the temporal side of themacula but often scattered over the posteriorpole of the fundus (Figure 21.2). These mightcome and go over months and the overallpicture could be unchanged for several years.The vision is not affected unless the micro-aneurysms are clustered round the macularregion and leak fluid, resulting in macularoedema. Exudates are also seen and these tendto form rings around areas of diseased vessels,although only one part of the ring might bepresent at any given point. These are yellowish-white deposits with well-defined edges, whichare the result of precipitation of leaked lipo-proteins from diseased blood vessels. Capillarydilatation is a more subtle sign of diabeticretinopathy. Haemorrhages, which can be small(“dot”) or large blot, result from the venous endof capillaries and are in the deep retina. Flame-shaped haemorrhages can also occur in thenerve fibre layer. “Cotton-wool” spots representaxoplasmic accumulation adjacent to micro-infarction of the retinal nerve fibre layer. They
are greyish-white with poorly defined fluffyedges. Histological examination of diseasedretina has shown areas of capillary closure andcapillary microaneurysms. The vessel walls havethickened basement membranes and loss ofmural cells (pericytes) (Figure 21.3).
The Preproliferative StageProliferative retinopathy is typically seen inpoorly controlled diabetics (usually type I diabetes). The situation can become bad quicklyand it is important to be able to recognise thewarning signs, which occur before proliferation.There are three of them: a large number of darkblot haemorrhages, irregular calibre and dila-tation of the retinal veins (beading) and finally,the presence of intraretinal microvascularabnormalities. These warning signs can herald
Systemic Disease and the Eye 167
Figure 21.2. Background diabetic retinopathy. a Early: micro-aneurysms and haemorrhages. b Severe: extensive haemor-rhages, cotton-wool spots and venous dilatation.
a
b
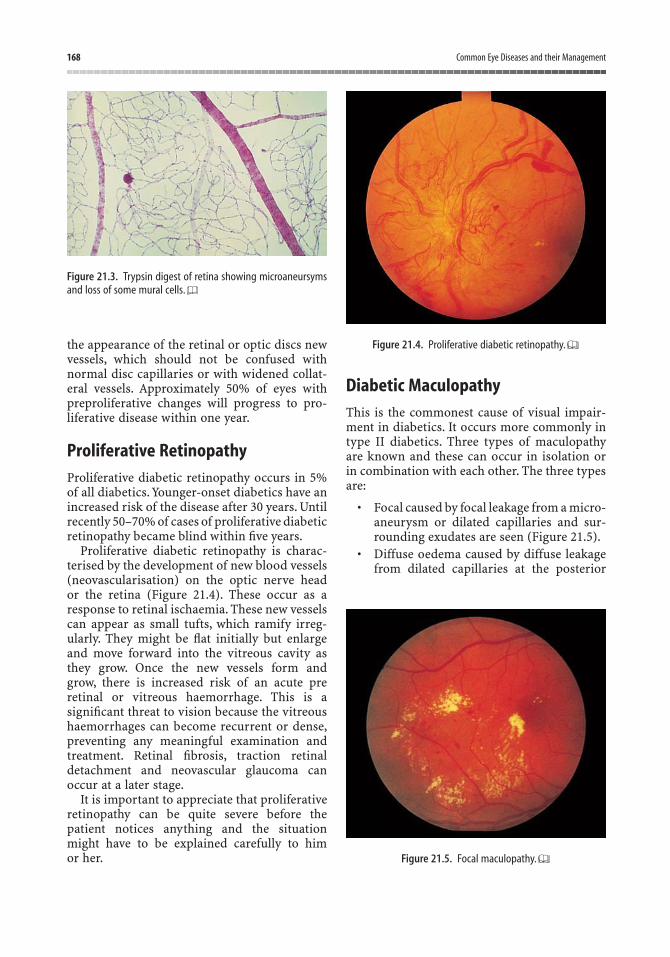
the appearance of the retinal or optic discs newvessels, which should not be confused withnormal disc capillaries or with widened collat-eral vessels. Approximately 50% of eyes withpreproliferative changes will progress to pro-liferative disease within one year.
Proliferative RetinopathyProliferative diabetic retinopathy occurs in 5%of all diabetics. Younger-onset diabetics have anincreased risk of the disease after 30 years. Untilrecently 50–70% of cases of proliferative diabeticretinopathy became blind within five years.
Proliferative diabetic retinopathy is charac-terised by the development of new blood vessels(neovascularisation) on the optic nerve head or the retina (Figure 21.4). These occur as aresponse to retinal ischaemia. These new vesselscan appear as small tufts, which ramify irreg-ularly. They might be flat initially but enlargeand move forward into the vitreous cavity asthey grow. Once the new vessels form and grow, there is increased risk of an acute preretinal or vitreous haemorrhage. This is asignificant threat to vision because the vitreoushaemorrhages can become recurrent or dense,preventing any meaningful examination andtreatment. Retinal fibrosis, traction retinaldetachment and neovascular glaucoma canoccur at a later stage.
It is important to appreciate that proliferativeretinopathy can be quite severe before thepatient notices anything and the situation might have to be explained carefully to him or her.
Diabetic MaculopathyThis is the commonest cause of visual impair-ment in diabetics. It occurs more commonly intype II diabetics. Three types of maculopathyare known and these can occur in isolation orin combination with each other. The three typesare:
• Focal caused by focal leakage from a micro-aneurysm or dilated capillaries and sur-rounding exudates are seen (Figure 21.5).
• Diffuse oedema caused by diffuse leakagefrom dilated capillaries at the posterior
168 Common Eye Diseases and their Management
Figure 21.3. Trypsin digest of retina showing microaneursymsand loss of some mural cells.
Figure 21.4. Proliferative diabetic retinopathy.
Figure 21.5. Focal maculopathy.
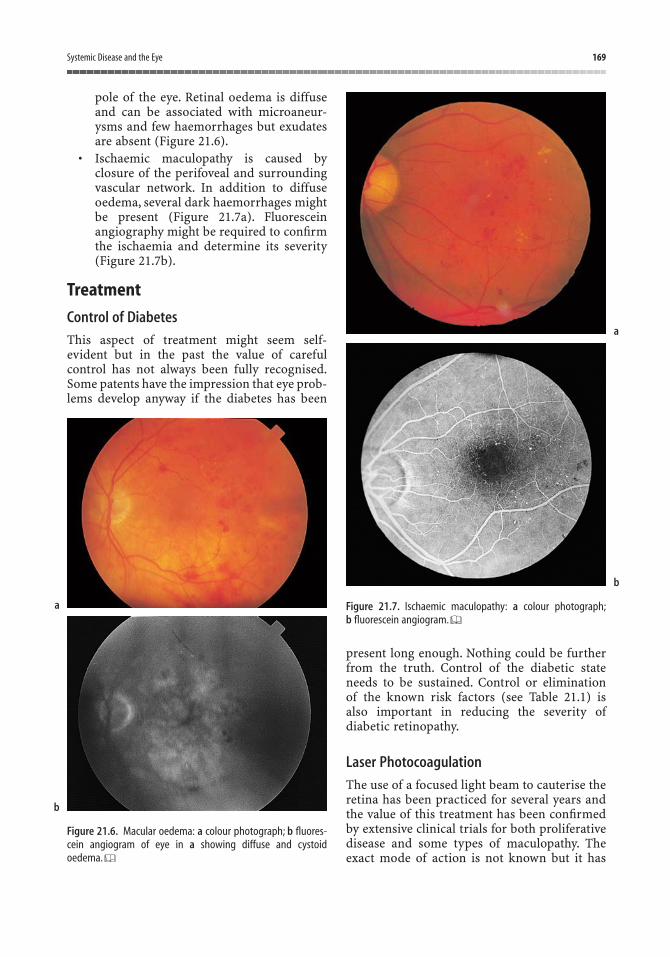
pole of the eye. Retinal oedema is diffuseand can be associated with microaneur-ysms and few haemorrhages but exudatesare absent (Figure 21.6).
• Ischaemic maculopathy is caused byclosure of the perifoveal and surroundingvascular network. In addition to diffuseoedema, several dark haemorrhages mightbe present (Figure 21.7a). Fluoresceinangiography might be required to confirmthe ischaemia and determine its severity(Figure 21.7b).
Treatment
Control of Diabetes
This aspect of treatment might seem self-evident but in the past the value of carefulcontrol has not always been fully recognised.Some patents have the impression that eye prob-lems develop anyway if the diabetes has been
present long enough. Nothing could be furtherfrom the truth. Control of the diabetic stateneeds to be sustained. Control or elimination of the known risk factors (see Table 21.1) is also important in reducing the severity ofdiabetic retinopathy.
Laser Photocoagulation
The use of a focused light beam to cauterise theretina has been practiced for several years andthe value of this treatment has been confirmedby extensive clinical trials for both proliferativedisease and some types of maculopathy. Theexact mode of action is not known but it has
Systemic Disease and the Eye 169
Figure 21.6. Macular oedema: a colour photograph; b fluores-cein angiogram of eye in a showing diffuse and cystoid oedema.
Figure 21.7. Ischaemic maculopathy: a colour photograph;b fluorescein angiogram.
a
b
a
b

been suggested that the photocoagulation ofischaemic areas prevents the release of some, asyet unidentified, vasoformative factor in prolif-erative disease. The treatment must be appliedpromptly in the early proliferative stage orsometimes before. About 2500–3000 burns (of500mm spot size) are needed in an eye with pro-liferative retinopathy. This might require severaltreatment sessions (Figure 21.8). The laser treat-ment of focal and diffuse maculopathy involvesapplication of small number of burns (of 100–200mm spot size) to the leaking area, avoidingthe fovea. Ischaemic maculopathy generally isless amenable to laser treatment.
Glaucoma Surgery
Drainage surgery might be needed if neovascu-lar glaucoma is not controlled by medicalmeans. Rubeosis iridis initially requires pan-retinal laser photocoagulation. Chronic simpleglaucoma can also be more common in diabet-ics. Drainage surgery in these cases is less suc-cessful than in nondiabetics. Special measuresneed to be taken to avoid failure.
Vitreo-retinal Surgery
There have been dramatic advances in the tech-nical side of vitreous surgery in recent years so
that it is now possible to remove a persistent vitreous haemorrhage and to divide or removefibrous tissue,even from the surface of the retina,and relieve traction retinal detachment. Vitrec-tomy for vitreous haemorrhage tends to be per-formed sooner these days because of the relativesafety of the technique. It can be combined withintraoperative laser photocoagulation.
PrognosisA better understanding of diabetic retinopathyhas resulted from the use of more accuratemethods of investigation, especially fluoresceinangiography, and also the routine use of indirectophthalmoscopy and slit-lamp microscopy.Serial fundus photography and the use of ultra-sound have also been important. This betterunderstanding and modern technology have ledto more effective treatment so that the moresevere ocular complications are now largelyavoidable. Blindness tends to be limited to thosecases where social or other circumstances makemanagement difficult. Patient education is vitalin order to maintain continuing improvement in visual prognosis for diabetics. After 20 years,75% of diabetics will develop some form of retinopathy. About 70% of patients with pro-liferative retinopathy will progress to blindnessif untreated in five years.
Thyroid Eye DiseaseDysthyroid eye disease is an autoimmunedisease in which the manifestations can benotable in the hyperthyroid, euthyroid orhypothyroid phase. Although the ophthalmicfeatures of thyroid disease are often diagnosedin the hyperthyroid phase, a significant numberof patients may be euthyroid (i.e., have no otherevidence of thyroid disease) or less oftenhypothyroid at the time of detection of the eye changes. Thus, the ophthalmic disease might precede, be coincidental or follow the systemic manifestations.
Grave’s disease is a term used to describe themost common form of hyperthyroidism thathas an autoimmune basis. Hyperthyroidism can arise from other conditions, for examplethyroid tumour or pituitary dysfunction. Itusually affects women between 20 and 45 years.Usually it is characterised by goitre, infiltrative
170 Common Eye Diseases and their Management
Figure 21.8. Panretinal laser photocoagulation in proliferativediabetic retinopathy.
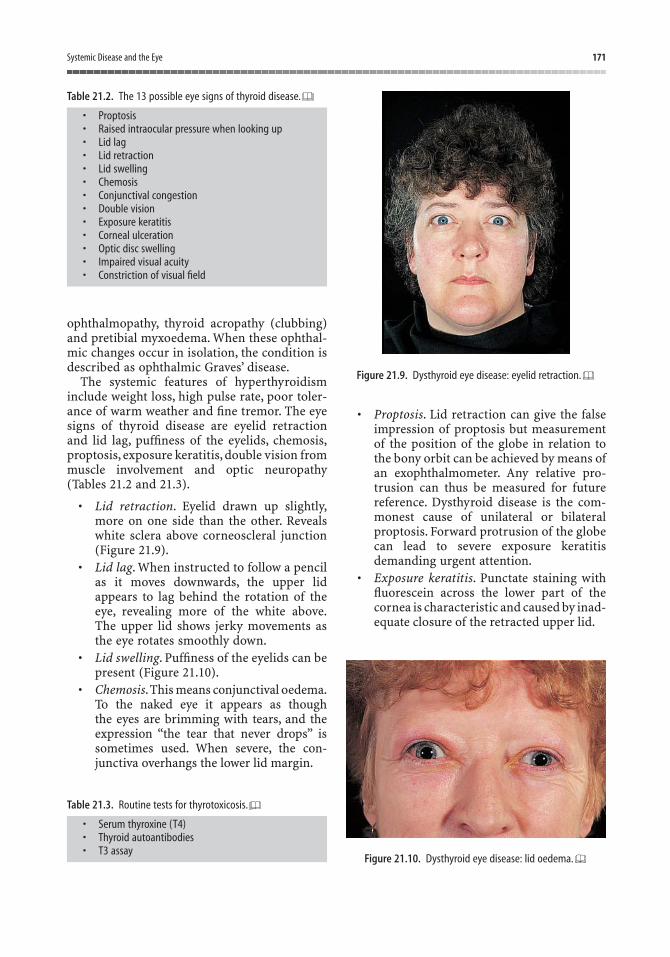
ophthalmopathy, thyroid acropathy (clubbing)and pretibial myxoedema. When these ophthal-mic changes occur in isolation, the condition isdescribed as ophthalmic Graves’ disease.
The systemic features of hyperthyroidisminclude weight loss, high pulse rate, poor toler-ance of warm weather and fine tremor. The eyesigns of thyroid disease are eyelid retractionand lid lag, puffiness of the eyelids, chemosis,proptosis, exposure keratitis, double vision frommuscle involvement and optic neuropathy(Tables 21.2 and 21.3).
• Lid retraction. Eyelid drawn up slightly,more on one side than the other. Revealswhite sclera above corneoscleral junction(Figure 21.9).
• Lid lag. When instructed to follow a pencilas it moves downwards, the upper lidappears to lag behind the rotation of theeye, revealing more of the white above.The upper lid shows jerky movements asthe eye rotates smoothly down.
• Lid swelling. Puffiness of the eyelids can bepresent (Figure 21.10).
• Chemosis.This means conjunctival oedema.To the naked eye it appears as though the eyes are brimming with tears, and theexpression “the tear that never drops” issometimes used. When severe, the con-junctiva overhangs the lower lid margin.
• Proptosis. Lid retraction can give the falseimpression of proptosis but measurementof the position of the globe in relation tothe bony orbit can be achieved by means ofan exophthalmometer. Any relative pro-trusion can thus be measured for future reference. Dysthyroid disease is the com-monest cause of unilateral or bilateralproptosis. Forward protrusion of the globecan lead to severe exposure keratitisdemanding urgent attention.
• Exposure keratitis. Punctate staining withfluorescein across the lower part of thecornea is characteristic and caused by inad-equate closure of the retracted upper lid.
Systemic Disease and the Eye 171
Table 21.2. The 13 possible eye signs of thyroid disease.
• Proptosis• Raised intraocular pressure when looking up• Lid lag• Lid retraction• Lid swelling• Chemosis• Conjunctival congestion• Double vision• Exposure keratitis• Corneal ulceration• Optic disc swelling• Impaired visual acuity• Constriction of visual field
Table 21.3. Routine tests for thyrotoxicosis.
• Serum thyroxine (T4)• Thyroid autoantibodies• T3 assay
Figure 21.9. Dysthyroid eye disease: eyelid retraction.
Figure 21.10. Dysthyroid eye disease: lid oedema.
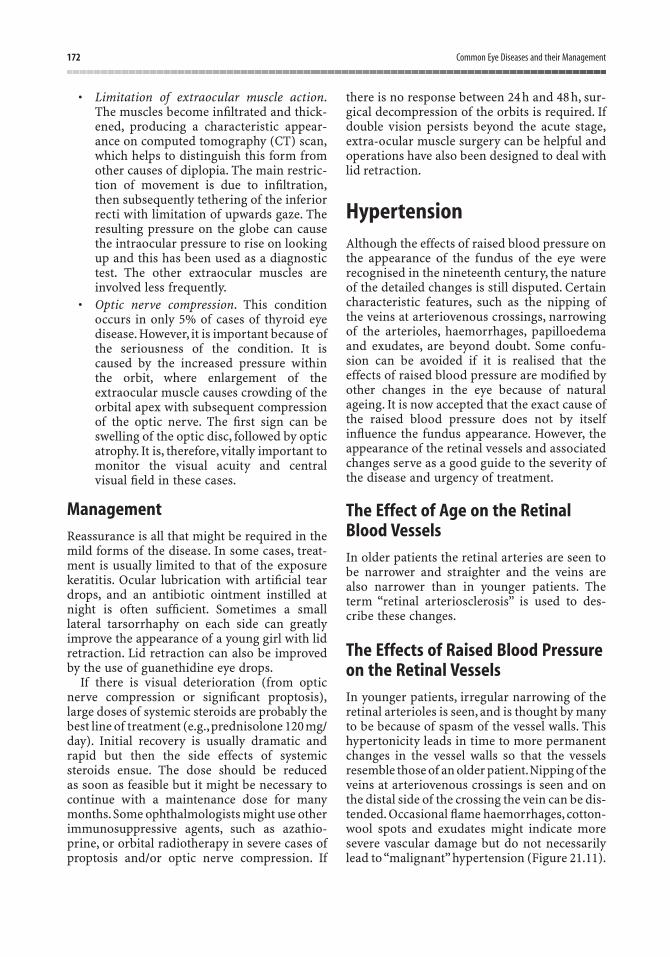
• Limitation of extraocular muscle action.The muscles become infiltrated and thick-ened, producing a characteristic appear-ance on computed tomography (CT) scan,which helps to distinguish this form fromother causes of diplopia. The main restric-tion of movement is due to infiltration,then subsequently tethering of the inferiorrecti with limitation of upwards gaze. Theresulting pressure on the globe can causethe intraocular pressure to rise on lookingup and this has been used as a diagnostictest. The other extraocular muscles areinvolved less frequently.
• Optic nerve compression. This conditionoccurs in only 5% of cases of thyroid eyedisease. However, it is important because ofthe seriousness of the condition. It iscaused by the increased pressure withinthe orbit, where enlargement of theextraocular muscle causes crowding of theorbital apex with subsequent compressionof the optic nerve. The first sign can beswelling of the optic disc, followed by opticatrophy. It is, therefore, vitally important tomonitor the visual acuity and centralvisual field in these cases.
ManagementReassurance is all that might be required in themild forms of the disease. In some cases, treat-ment is usually limited to that of the exposurekeratitis. Ocular lubrication with artificial teardrops, and an antibiotic ointment instilled atnight is often sufficient. Sometimes a smalllateral tarsorrhaphy on each side can greatlyimprove the appearance of a young girl with lidretraction. Lid retraction can also be improvedby the use of guanethidine eye drops.
If there is visual deterioration (from opticnerve compression or significant proptosis),large doses of systemic steroids are probably thebest line of treatment (e.g.,prednisolone 120 mg/day). Initial recovery is usually dramatic andrapid but then the side effects of systemicsteroids ensue. The dose should be reduced as soon as feasible but it might be necessary to continue with a maintenance dose for manymonths.Some ophthalmologists might use otherimmunosuppressive agents, such as azathio-prine, or orbital radiotherapy in severe cases ofproptosis and/or optic nerve compression. If
there is no response between 24 h and 48 h, sur-gical decompression of the orbits is required. Ifdouble vision persists beyond the acute stage,extra-ocular muscle surgery can be helpful andoperations have also been designed to deal withlid retraction.
HypertensionAlthough the effects of raised blood pressure onthe appearance of the fundus of the eye wererecognised in the nineteenth century, the natureof the detailed changes is still disputed. Certaincharacteristic features, such as the nipping ofthe veins at arteriovenous crossings, narrowingof the arterioles, haemorrhages, papilloedemaand exudates, are beyond doubt. Some confu-sion can be avoided if it is realised that theeffects of raised blood pressure are modified byother changes in the eye because of naturalageing. It is now accepted that the exact cause ofthe raised blood pressure does not by itselfinfluence the fundus appearance. However, theappearance of the retinal vessels and associatedchanges serve as a good guide to the severity ofthe disease and urgency of treatment.
The Effect of Age on the RetinalBlood VesselsIn older patients the retinal arteries are seen tobe narrower and straighter and the veins arealso narrower than in younger patients. Theterm “retinal arteriosclerosis” is used to des-cribe these changes.
The Effects of Raised Blood Pressureon the Retinal VesselsIn younger patients, irregular narrowing of theretinal arterioles is seen, and is thought by manyto be because of spasm of the vessel walls. Thishypertonicity leads in time to more permanentchanges in the vessel walls so that the vesselsresemble those of an older patient.Nipping of theveins at arteriovenous crossings is seen and onthe distal side of the crossing the vein can be dis-tended. Occasional flame haemorrhages, cotton-wool spots and exudates might indicate moresevere vascular damage but do not necessarilylead to “malignant” hypertension (Figure 21.11).
172 Common Eye Diseases and their Management

In older patients, the already narrowedvessels tend to show less dramatic changes.Hypertonicity of the vessel walls is not seen butarteriovenous nipping remains an importantsign and haemorrhages might be present inmore severe cases. The cotton-wool spots ofhypertension reflect ischaemic damage to thenerve fibre layer caused by obstruction of theretinal precapillary arterioles. Exudates arecaused by abnormal vascular permeability.
“Malignant” HypertensionOccasionally,patients with a severe hypertensiveproblem present directly to the ophthalmologistbecause their main symptom is blurring of thevision, the other more usual symptoms beingless evident. On examination, the visual acuitymight be only slightly reduced unless there issignificant macular oedema and there might besome enlargement of the blind spot and con-striction of the visual fields. Inspection of thefundus reveals marked swelling of the optic disc,the oedema often extending well away from thedisc with scattered flame-shaped haemorrhages.If the diastolic blood pressure is above 110–120 mmHg, there is little doubt about the diag-nosis, but below this level it is essential to bearin mind the possibility of raised intracranialpressure from other causes. When hypertensionis as severe as this, the patient should be treatedas an acute medical emergency and referredwithout delay to the appropriate physician.
Other Associated Vascular Changes
Retinal Vascular Occlusion
This is more common in hypertensive patientscompared with normotensives. The most fre-quent occurrence is the central retinal veinocclusion (CRVO), although branch retinal veinocclusions can occur at arteriovenous crossings.The fundus appearance in CRVO is dramaticwith numerous scattered haemorrhages andswelling of the optic disc, and the patient expe-riences sudden blurring of vision in one eye(Figure 21.12). This can be compared withocclusion of the central retinal artery, which isless common and in which the prognosis is uni-formly worse. Here, the fundus appears pale andthe arteries are narrowed. There is a cherry-redspot at the macula.
Systemic Disease and the Eye 173
Figure 21.11. Hypertensive retinopathy: haemorrhages,cotton-wool spots, exudates, vascular calibre changes.
Figure 21.12. a Central retinal vein occlusion and b macularbranch retinal vein occlusion.
a
b
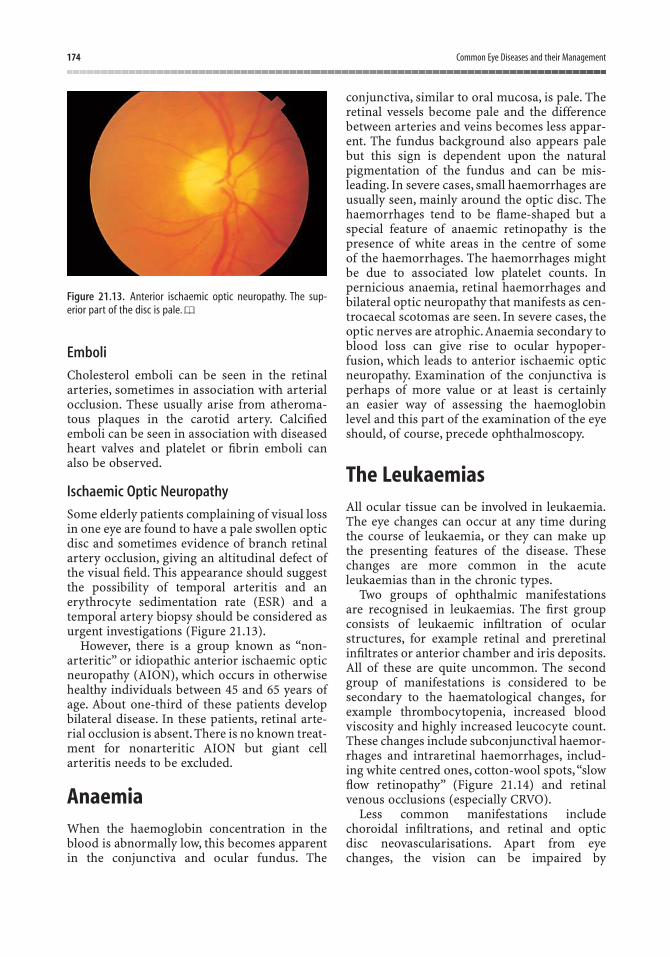
Emboli
Cholesterol emboli can be seen in the retinalarteries, sometimes in association with arterialocclusion. These usually arise from atheroma-tous plaques in the carotid artery. Calcifiedemboli can be seen in association with diseasedheart valves and platelet or fibrin emboli canalso be observed.
Ischaemic Optic Neuropathy
Some elderly patients complaining of visual lossin one eye are found to have a pale swollen opticdisc and sometimes evidence of branch retinalartery occlusion, giving an altitudinal defect ofthe visual field. This appearance should suggestthe possibility of temporal arteritis and an erythrocyte sedimentation rate (ESR) and atemporal artery biopsy should be considered asurgent investigations (Figure 21.13).
However, there is a group known as “non-arteritic” or idiopathic anterior ischaemic opticneuropathy (AION), which occurs in otherwisehealthy individuals between 45 and 65 years ofage. About one-third of these patients developbilateral disease. In these patients, retinal arte-rial occlusion is absent. There is no known treat-ment for nonarteritic AION but giant cellarteritis needs to be excluded.
AnaemiaWhen the haemoglobin concentration in theblood is abnormally low, this becomes apparentin the conjunctiva and ocular fundus. The
conjunctiva, similar to oral mucosa, is pale. Theretinal vessels become pale and the differencebetween arteries and veins becomes less appar-ent. The fundus background also appears palebut this sign is dependent upon the natural pigmentation of the fundus and can be mis-leading. In severe cases, small haemorrhages areusually seen, mainly around the optic disc. Thehaemorrhages tend to be flame-shaped but aspecial feature of anaemic retinopathy is thepresence of white areas in the centre of some of the haemorrhages. The haemorrhages mightbe due to associated low platelet counts. In pernicious anaemia, retinal haemorrhages andbilateral optic neuropathy that manifests as cen-trocaecal scotomas are seen. In severe cases, theoptic nerves are atrophic.Anaemia secondary toblood loss can give rise to ocular hypoper-fusion, which leads to anterior ischaemic opticneuropathy. Examination of the conjunctiva isperhaps of more value or at least is certainly an easier way of assessing the haemoglobin level and this part of the examination of the eyeshould, of course, precede ophthalmoscopy.
The LeukaemiasAll ocular tissue can be involved in leukaemia.The eye changes can occur at any time duringthe course of leukaemia, or they can make upthe presenting features of the disease. Thesechanges are more common in the acuteleukaemias than in the chronic types.
Two groups of ophthalmic manifestations are recognised in leukaemias. The first groupconsists of leukaemic infiltration of ocularstructures, for example retinal and preretinalinfiltrates or anterior chamber and iris deposits.All of these are quite uncommon. The secondgroup of manifestations is considered to be secondary to the haematological changes, forexample thrombocytopenia, increased bloodviscosity and highly increased leucocyte count.These changes include subconjunctival haemor-rhages and intraretinal haemorrhages, includ-ing white centred ones, cotton-wool spots,“slowflow retinopathy” (Figure 21.14) and retinalvenous occlusions (especially CRVO).
Less common manifestations includechoroidal infiltrations, and retinal and opticdisc neovascularisations. Apart from eyechanges, the vision can be impaired by
174 Common Eye Diseases and their Management
Figure 21.13. Anterior ischaemic optic neuropathy. The sup-erior part of the disc is pale.
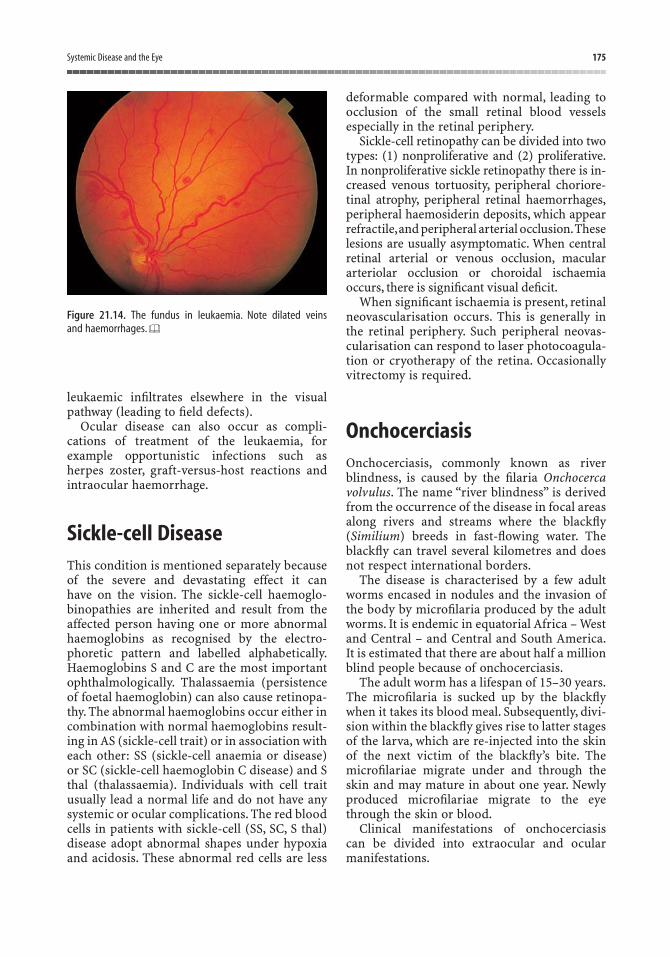
leukaemic infiltrates elsewhere in the visualpathway (leading to field defects).
Ocular disease can also occur as compli-cations of treatment of the leukaemia, forexample opportunistic infections such as herpes zoster, graft-versus-host reactions andintraocular haemorrhage.
Sickle-cell DiseaseThis condition is mentioned separately becauseof the severe and devastating effect it can have on the vision. The sickle-cell haemoglo-binopathies are inherited and result from theaffected person having one or more abnormalhaemoglobins as recognised by the electro-phoretic pattern and labelled alphabetically.Haemoglobins S and C are the most importantophthalmologically. Thalassaemia (persistenceof foetal haemoglobin) can also cause retinopa-thy. The abnormal haemoglobins occur either incombination with normal haemoglobins result-ing in AS (sickle-cell trait) or in association witheach other: SS (sickle-cell anaemia or disease)or SC (sickle-cell haemoglobin C disease) and Sthal (thalassaemia). Individuals with cell traitusually lead a normal life and do not have anysystemic or ocular complications. The red bloodcells in patients with sickle-cell (SS, SC, S thal)disease adopt abnormal shapes under hypoxiaand acidosis. These abnormal red cells are less
deformable compared with normal, leading toocclusion of the small retinal blood vesselsespecially in the retinal periphery.
Sickle-cell retinopathy can be divided into twotypes: (1) nonproliferative and (2) proliferative.In nonproliferative sickle retinopathy there is in-creased venous tortuosity, peripheral choriore-tinal atrophy, peripheral retinal haemorrhages,peripheral haemosiderin deposits, which appearrefractile,and peripheral arterial occlusion.Theselesions are usually asymptomatic. When centralretinal arterial or venous occlusion, macular arteriolar occlusion or choroidal ischaemiaoccurs, there is significant visual deficit.
When significant ischaemia is present, retinalneovascularisation occurs. This is generally inthe retinal periphery. Such peripheral neovas-cularisation can respond to laser photocoagula-tion or cryotherapy of the retina. Occasionallyvitrectomy is required.
OnchocerciasisOnchocerciasis, commonly known as riverblindness, is caused by the filaria Onchocercavolvulus. The name “river blindness” is derivedfrom the occurrence of the disease in focal areasalong rivers and streams where the blackfly(Similium) breeds in fast-flowing water. Theblackfly can travel several kilometres and doesnot respect international borders.
The disease is characterised by a few adultworms encased in nodules and the invasion ofthe body by microfilaria produced by the adultworms. It is endemic in equatorial Africa – Westand Central – and Central and South America.It is estimated that there are about half a millionblind people because of onchocerciasis.
The adult worm has a lifespan of 15–30 years.The microfilaria is sucked up by the blackflywhen it takes its blood meal. Subsequently, divi-sion within the blackfly gives rise to latter stagesof the larva, which are re-injected into the skinof the next victim of the blackfly’s bite. Themicrofilariae migrate under and through theskin and may mature in about one year. Newlyproduced microfilariae migrate to the eyethrough the skin or blood.
Clinical manifestations of onchocerciasis can be divided into extraocular and ocular manifestations.
Systemic Disease and the Eye 175
Figure 21.14. The fundus in leukaemia. Note dilated veins and haemorrhages.

Extraocular FeaturesSkin involvement is in the form of pruritis – amaculopapular rash, which can be associatedwith hypo- or hyperpigmentation, dermal andepidermal atrophy or “onchodermatitis”.
There might be subcutaneous nodules, whichare firm, round masses in the dermis and sub-cutaneous tissue, especially close to joints in thehead and shoulder.
Ocular FeaturesIntraocular microfilariae can be seen in the anterior chamber.Dead microfilariae are usuallyseen in the cornea (especially peripherally).
Other ocular features are punctate keratitisand sclerosing keratitis; anterior uveitis, usuallyof the nongranulomatous type with loss ofthe pigment frill, and posterior synechiae arecommon. Secondary cataract and glaucoma can develop.
Chorioretinitis of the chronic nongranulo-matous type can occur, with secondary degen-erative changes in the retinal pigmentepithelium (RPE) neuroretina and the chorio-capillaries. There might be granular atrophy ofthe RPE, subretinal fibrosis, retinal arteriolarattenuation and vasculitis. Optic atrophy andneuropathy are not uncommon.
Diagnosis is confirmed by skin snip and theMazzoti test, which depends on a Herxheimerreaction to a single dose of diethylcarbamazine.Care is required with this test because the reac-tion could be severe.
ManagementOne method is by vector control. An inter-national (World Health Organisation) program-me, the onchocerciasis control programme, hasbeen successful in reducing the endemicity ofthe disease in the Volta river basin.
Chemotherapy of infected patients now usesIvermectin, which in a single dose rids thepatient of microfilariae for one to two years.This medication needs to be repeated overseveral years in mass administration projects.
Diethylcarbamazine is the older treatment forthe microfilariae but is more toxic and requiresto be taken over a two- to three-week period.Adult worms can only be killed by suramin, orremoved surgically.
Acquired Immune DeficiencySyndrome (AIDS)Acquired immune deficiency syndrome (AIDS)refers to the final stages of infection by thehuman immunodeficiency virus (HIV). Theearlier stages of the disease are often asympto-matic (Table 21.4).
In western countries, AIDS commonly affectshomosexuals, haemophiliacs, and intravenousdrug abusers, although there is now a significantheterosexual and paediatric pool of patients. InAfrica, it is generally a heterosexual disease, anda significant paediatric population is alsoknown. Transmission is through sexual inter-course, parenteral or transplacental routes.
Ocular features occur in 75% of patients withAIDS. The major ocular complications of AIDSoccur later in the disease and can be predictedby CD4 T-cell levels. At CD4 level >200 ¥ 106/Lcommon ocular complications are toxoplas-mosis and herpes zoster ophthalmicus andretinitis, while at CD4 levels <50 ¥ 106/L cyto-megalovirus (CMV) retinitis is common.
AIDS microangiopathy (noninfectious) occursin about 50% of patients (in both developing and western countries). It consists of microa-neurysms, telangiectasia, cotton-wool spots anda few retinal haemorrhages. Retinal peripheralperivascular sheathing may sometimes occur in the absence of intraocular infections.
Other ocular involvement of AIDS in-cludes infections with opportunistic and
176 Common Eye Diseases and their Management
Table 21.4. Classification of human immunodeficiency virus(HIV) infection (Centers for Disease Control, Atlanta, 1992).
Group I Acute infection: asymptomatic with seroconversion
Group II Asymptomatic carrierGroup III Generalised, persistent
lymphadenopathies; usually good state of general health
Group IV AIDSSub- (A) Constitutional (cachexia, fever, etc.).groups (B) Neurological.
(C) Infections diagnostic of AIDS.(D) Malignancies.(E) Others, e.g. CD4 count <200 ¥ 106/L.

nonopportunistic organisms (e.g., CMV, crypto-coccus and molluscum contagiosum) (Figures21.15 and 21.16). Neoplasms of the conjunctiva,lids and orbit, and neurophthalmic complica-tions are other features.
In western countries, the commonest ophthal-mic complication of AIDS is CMV retinitis,while in developing countries (such as Africa),CMV is not a major problem. Herpes zoster ophthalmicus and conjunctival carcinoma arecommon in AIDS patients in Africa and AIDSpatients die of other complications, for exampletuberculosis. Therefore, short-term survivalfrom AIDS itself is a problem in developingcountries, while in western countries quality oflife for the longer term is the main problem.
Treatment with the highly active antiretro-viral therapy (HAART) regimen leads to signi-
ficant elevation of CD4 T-cell levels such that theocular complications, especially opportunisticinfections, are less commonly encountered.
Ophthalmological Signs of AIDS1. Noninfectious retinopathy:
(a) cotton-wool spots(b) retinal haemorrhages(c) microvascular changes.
2. Opportunistic infections:(a) Involvement of posterior segment:
• CMV retinitis• acute retinal necrosis (herpes
simplex, herpes zoster)• toxoplasmic chorioretinitis• Pneumocystis carinii choroiditis• tuberculous choroiditis• endophthalmitis caused by Candida
albicans – usually intravenous drugusers
• cryptococcus chorioretinitis• syphilitic retinitis
(b) Involvement of anterior segment:• chronic keratitis and keratouveitis
caused by herpes zoster and herpessimplex
• keratoconjunctivitis caused by CMV,microsporum and gonococcus
• corneal ulcer caused by Candida albi-cans, and bacteria (Pseudomonasaeruginosa, Staphylococcus aureus,and Staphylococcus epidermidis)
• syphilitic and toxoplasmic iridocyclitis• conjunctivitis caused by CMV,herpes
zoster and herpes simplex• bacterial conjunctivitis.
3. Neoplasms:(a) conjunctival, palpebral and orbital
Kaposi’s sarcoma(b) intraocular lymphoma(c) other neoplasms:
• conjunctival squamous carcinoma• palpebral and orbital lymphoma.
4. Neuro-ophthalmological signs:(a) Involvement of cranial nerves:
Systemic Disease and the Eye 177
Figure 21.15. Cytomegalovirus retinitis in acquired immunedeficiency syndrome (AIDS).
Figure 21.16. Human immunodeficiency virus retinopathy.

• internuclear ophthalmoplegia• third, fourth and sixth cranial
nerve palsies• retrobulbar neuritis and papillitis
(b) Homonymous haemianopia(c) AIDS–dementia complex with cortical
blindness.5. Other signs:
(a) Conjunctiva:• nonspecific conjunctivitis• keratoconjunctivitis sicca• nonspecific conjunctiva micro-
vascular changes in the inferiorperilimbal bulbar region (haemor-rhages, microaneurysms, columnfragmentation, dilatation and irreg-ular vessel diameter)
• bacterial conjunctivitis(b) Cornea:
• nonspecific punctate keratitis(c) Sclera:
• necrotising scleritis.
(d) Retina:• talc-induced retinopathy (only
intravenous drug users)(e) Eyelids:
• herpes zoster ophthalmicus• palpebral molluscum contagiosum• palpebral cryptococcosis
(f) Orbit:• orbital apex granuloma• orbital pseudotumour• orbital infiltration by Aspergillus,
Pneumocystis carinii• orbital cellulitis
(g) Visual and refraction defects:• night blindness because of vitamin
A and E malabsorption• progression of myopia• decreased accommodation
(h) Acute closed-angle (bilateral) glau-coma caused by choroidal effusion.
178 Common Eye Diseases and their Management
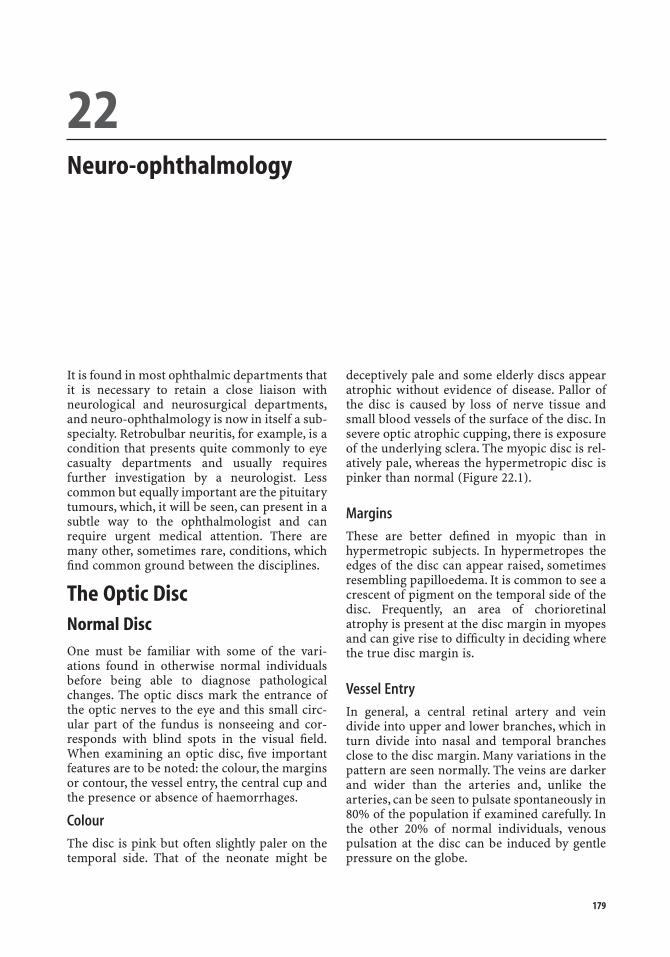
It is found in most ophthalmic departments thatit is necessary to retain a close liaison withneurological and neurosurgical departments,and neuro-ophthalmology is now in itself a sub-specialty. Retrobulbar neuritis, for example, is acondition that presents quite commonly to eyecasualty departments and usually requiresfurther investigation by a neurologist. Lesscommon but equally important are the pituitarytumours, which, it will be seen, can present in asubtle way to the ophthalmologist and canrequire urgent medical attention. There aremany other, sometimes rare, conditions, whichfind common ground between the disciplines.
The Optic DiscNormal DiscOne must be familiar with some of the vari-ations found in otherwise normal individualsbefore being able to diagnose pathologicalchanges. The optic discs mark the entrance ofthe optic nerves to the eye and this small circ-ular part of the fundus is nonseeing and cor-responds with blind spots in the visual field.When examining an optic disc, five importantfeatures are to be noted: the colour, the marginsor contour, the vessel entry, the central cup andthe presence or absence of haemorrhages.
Colour
The disc is pink but often slightly paler on thetemporal side. That of the neonate might be
deceptively pale and some elderly discs appearatrophic without evidence of disease. Pallor ofthe disc is caused by loss of nerve tissue andsmall blood vessels of the surface of the disc. Insevere optic atrophic cupping, there is exposureof the underlying sclera. The myopic disc is rel-atively pale, whereas the hypermetropic disc ispinker than normal (Figure 22.1).
Margins
These are better defined in myopic than inhypermetropic subjects. In hypermetropes theedges of the disc can appear raised, sometimesresembling papilloedema. It is common to see acrescent of pigment on the temporal side of thedisc. Frequently, an area of chorioretinalatrophy is present at the disc margin in myopesand can give rise to difficulty in deciding wherethe true disc margin is.
Vessel Entry
In general, a central retinal artery and veindivide into upper and lower branches, which inturn divide into nasal and temporal branchesclose to the disc margin. Many variations in thepattern are seen normally. The veins are darkerand wider than the arteries and, unlike thearteries, can be seen to pulsate spontaneously in80% of the population if examined carefully. Inthe other 20% of normal individuals, venouspulsation at the disc can be induced by gentlepressure on the globe.
22Neuro-ophthalmology
179

Central Cup
The centre of the disc is deeper (i.e., furtheraway from the observer) than the peripheralpart. This central cup occupies about one-third(or less) of the total disc diameter in normalsubjects. The ratio between the vertical diame-ter of the cup and the total disc diameter isknown as the cup-to-disc ratio. Thus, thenormal cup-to-disc ratio is <0.3.
Haemorrhages
Haemorrhages are never seen on or adjacent to normal discs. If present, they warrant further investigation.
Congenital Disc AnomaliesA number of minor congenital abnormalitiesare seen on the disc. In an astigmatic eye, thedisc is often oval. The central cup might be filledin by “drusen” – small hyaline deposits, whichcan be found on the surface or buried in the sub-stance of the disc. This appearance can mimicpapilloedema. Alternatively, the central cupmight be hollowed out further by a congenitalpit in the disc. Myelinated retinal nerve fibresare recognised by their strikingly white appear-ance, which obscures any underlying vessels,and their fluffy margin (see Figure 22.3). Thecentral cup can be filled in by persistent rem-nants of the hyaloid artery (Bergmeister’spapilla), which runs in the embryo from disc tolens. Some of these and other congenital abnor-malities of the disc can be associated with visualfield defects that are not progressive but whichcan cause diagnostic confusion.
Pale Disc
Optic Atrophy
Optic atrophy means loss of nerve tissue on thedisc, and the resulting abnormal pallor ofthe disc must be accompanied by a defect in thevisual field, but not necessarily by a reduction inthe visual acuity. It must be remembered thatthe disc tends to be somewhat pale and the cupof disc tends to be larger in short-sighted eyesand care must be taken in diagnosing opticatrophy in such cases. The number of smallvessels, which can be counted on the disc, issometimes used as an index of atrophy indifficult cases.
Classification of the causes of optic atrophyusually includes the term “consecutive opticatrophy”, referring to atrophy following retinaldegeneration. The terms primary and second-ary atrophy are also used but because theseterms are confusing a simple aetiologicalclassification will be used here. It should beborne in mind that it is not usually possible todetermine the cause of optic atrophy by theappearance of the optic disc. Even the cupped,pale disc of chronic glaucoma can be mimickedby optic atrophy because of chiasmal compres-sion. When optic atrophy follows swelling of theoptic disc, there is more gliosis than when it is“primary”, that is, caused by disease in the nerve
180 Common Eye Diseases and their Management
Figure 22.1. Normal optic disc in a myope and b hypermetrope.
a
b
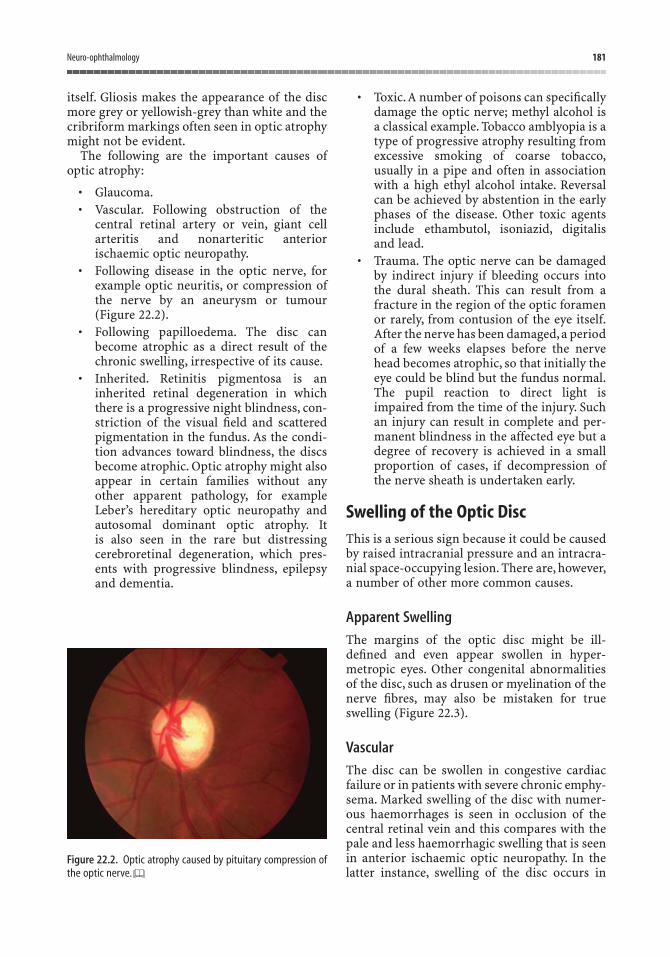
itself. Gliosis makes the appearance of the discmore grey or yellowish-grey than white and thecribriform markings often seen in optic atrophymight not be evident.
The following are the important causes ofoptic atrophy:
• Glaucoma.• Vascular. Following obstruction of the
central retinal artery or vein, giant cellarteritis and nonarteritic anterior ischaemic optic neuropathy.
• Following disease in the optic nerve, forexample optic neuritis, or compression ofthe nerve by an aneurysm or tumour(Figure 22.2).
• Following papilloedema. The disc canbecome atrophic as a direct result of thechronic swelling, irrespective of its cause.
• Inherited. Retinitis pigmentosa is aninherited retinal degeneration in whichthere is a progressive night blindness, con-striction of the visual field and scatteredpigmentation in the fundus. As the condi-tion advances toward blindness, the discsbecome atrophic. Optic atrophy might alsoappear in certain families without anyother apparent pathology, for exampleLeber’s hereditary optic neuropathy andautosomal dominant optic atrophy. It is also seen in the rare but distressingcerebroretinal degeneration, which pres-ents with progressive blindness, epilepsyand dementia.
• Toxic.A number of poisons can specificallydamage the optic nerve; methyl alcohol isa classical example. Tobacco amblyopia is atype of progressive atrophy resulting fromexcessive smoking of coarse tobacco,usually in a pipe and often in associationwith a high ethyl alcohol intake. Reversalcan be achieved by abstention in the earlyphases of the disease. Other toxic agentsinclude ethambutol, isoniazid, digitalis and lead.
• Trauma. The optic nerve can be damagedby indirect injury if bleeding occurs intothe dural sheath. This can result from afracture in the region of the optic foramenor rarely, from contusion of the eye itself.After the nerve has been damaged,a periodof a few weeks elapses before the nervehead becomes atrophic, so that initially theeye could be blind but the fundus normal.The pupil reaction to direct light isimpaired from the time of the injury. Suchan injury can result in complete and per-manent blindness in the affected eye but adegree of recovery is achieved in a smallproportion of cases, if decompression ofthe nerve sheath is undertaken early.
Swelling of the Optic DiscThis is a serious sign because it could be causedby raised intracranial pressure and an intracra-nial space-occupying lesion. There are, however,a number of other more common causes.
Apparent Swelling
The margins of the optic disc might be ill-defined and even appear swollen in hyper-metropic eyes. Other congenital abnormalitiesof the disc, such as drusen or myelination of thenerve fibres, may also be mistaken for trueswelling (Figure 22.3).
Vascular
The disc can be swollen in congestive cardiacfailure or in patients with severe chronic emphy-sema. Marked swelling of the disc with numer-ous haemorrhages is seen in occlusion of thecentral retinal vein and this compares with thepale and less haemorrhagic swelling that is seenin anterior ischaemic optic neuropathy. In thelatter instance, swelling of the disc occurs in
Neuro-ophthalmology 181
Figure 22.2. Optic atrophy caused by pituitary compression ofthe optic nerve.
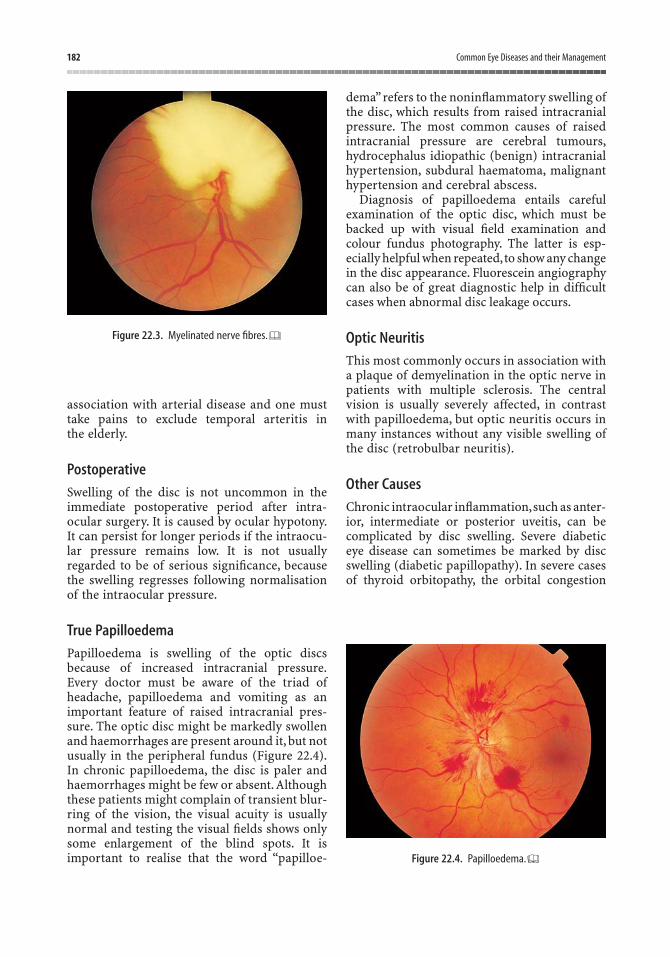
association with arterial disease and one musttake pains to exclude temporal arteritis in the elderly.
Postoperative
Swelling of the disc is not uncommon in theimmediate postoperative period after intra-ocular surgery. It is caused by ocular hypotony.It can persist for longer periods if the intraocu-lar pressure remains low. It is not usuallyregarded to be of serious significance, becausethe swelling regresses following normalisationof the intraocular pressure.
True Papilloedema
Papilloedema is swelling of the optic discsbecause of increased intracranial pressure.Every doctor must be aware of the triad ofheadache, papilloedema and vomiting as animportant feature of raised intracranial pres-sure. The optic disc might be markedly swollenand haemorrhages are present around it, but notusually in the peripheral fundus (Figure 22.4).In chronic papilloedema, the disc is paler andhaemorrhages might be few or absent. Althoughthese patients might complain of transient blur-ring of the vision, the visual acuity is usuallynormal and testing the visual fields shows onlysome enlargement of the blind spots. It isimportant to realise that the word “papilloe-
dema”refers to the noninflammatory swelling ofthe disc, which results from raised intracranialpressure. The most common causes of raisedintracranial pressure are cerebral tumours,hydrocephalus idiopathic (benign) intracranialhypertension, subdural haematoma, malignanthypertension and cerebral abscess.
Diagnosis of papilloedema entails carefulexamination of the optic disc, which must bebacked up with visual field examination andcolour fundus photography. The latter is esp-ecially helpful when repeated,to show any changein the disc appearance. Fluorescein angiographycan also be of great diagnostic help in difficultcases when abnormal disc leakage occurs.
Optic Neuritis
This most commonly occurs in association witha plaque of demyelination in the optic nerve inpatients with multiple sclerosis. The centralvision is usually severely affected, in contrastwith papilloedema, but optic neuritis occurs inmany instances without any visible swelling ofthe disc (retrobulbar neuritis).
Other Causes
Chronic intraocular inflammation,such as anter-ior, intermediate or posterior uveitis, can be complicated by disc swelling. Severe diabetic eye disease can sometimes be marked by discswelling (diabetic papillopathy). In severe casesof thyroid orbitopathy, the orbital congestion
182 Common Eye Diseases and their Management
Figure 22.3. Myelinated nerve fibres.
Figure 22.4. Papilloedema.

can cause disc swelling (dysthyroid optic neu-ropathy). In both instances, the doctor should bewarned that serious consequences might ensueunless prompt treatment is applied. Infiltrationof the disc by leukaemia, lymphoma or chronicgranulomata (as in sarcoidosis) can also causedisc swelling.
Multiple SclerosisThis common and important neurologicaldisease can often present initially as an eyeproblem and its proper management requirescareful co-ordination at the primary care level.It is important to realise that multiple sclerosisshould not be diagnosed after one single attackof optic or retrobulbar neuritis because thiscould cause unnecessary alarm about some-thing that might never happen. Studies haveshown that between 45% and 80% of patientswith optic neuritis will develop multiple sclero-sis after 15 years of follow-up. Furthermore,optic neuritis has causes other than multiplesclerosis. The diagnosis of multiple sclerosisshould be made by a neurologist and is based onfinding additional evidence of the disease else-where in the body.
The cause of multiple sclerosis is not known,but the disease is characterised by the appear-ance of multiple inflammatory foci in relation tothe myelin sheaths of nerves throughout thecentral nervous system. The demyelinationplaques are detectable on magnetic resonanceimaging scans of the brain. The optic nervebetween globe and chiasm is commonly involvedat an early stage and there might be a delay ofseveral years before other features of the diseaseappear.Young or middle-aged people are mainlyaffected and the prognosis is worse when thedisease is acquired at an early age.
Ocular Findings
Optic or Retrobulbar Neuritis
This is an important cause of unilateral suddenloss of vision in a white eye in a young person.The patient complains of pain behind the eye onattempting to move it and there is often a greyor coloured patch in the centre of the field ofview. In severe cases, the sight of the affected eye
can be lost completely. On examination, a rela-tive afferent pupil defect on the affected sidemight be the only objective evidence of disease.It is essential to test the pupil before dilating itwith eye drops. The fundus is often normal ini-tially (retrobulbar neuritis), although there canbe slight swelling of the optic disc (optic neuri-tis). After two or three weeks the optic discstarts to become pale. The visual prognosis isgenerally good. Most patients make a completeor nearly complete recovery after 6–12 weeks.The attack is unilateral in 90% of cases, althoughthere is a risk that the other eye can be affectedat a later date and recurrent attacks in one orboth eyes can cause permanent damage to thevision. Fortunately, it is extremely rare for apatient to be made blind by multiple sclerosis.
The diagnosis at the time of the acute attackrelies on the history and noting the pupil reac-tion. It is often advisable to make the diagnosisin retrospect. The patient might give a history ofvisual loss in one eye, which has recovered, andat a later date, presents with other nonocularsigns and symptoms of demyelinating disease.If it can be confirmed that the patient has had aprevious attack of optic neuritis, this can help inthe confirmation of the diagnosis of dissemi-nated sclerosis. Under these circumstances, thepallor of the disc can be helpful, but carefulassessment of the colour vision, visual acuityand measurement of the visually evoked poten-tial can provide conclusive evidence. At the timeof the acute attack, testing the visual field mightreveal a central scotoma. The size of this defectdiminishes as healing occurs, often leaving asmall residual defect between blind spot andcentral area.
Corticosteroids administered systemicallycan speed up recovery of vision. However,the final visual outcome is unchanged by such treatment.
Nystagmus
This usually appears at a later stage than opticneuritis and might only be evident in lateralgaze. It is often horizontal.
Internuclear Ophthalmoplegia
Whereas double vision is a common symptomin multiple sclerosis, it is unusual to see an
Neuro-ophthalmology 183

184 Common Eye Diseases and their Management
obvious defect of the ocular movements.Sometimes it can be seen that one eye fails to turn inwards when the patient is asked to look to the opposite side, and yet when thepatient is made to converge the eyes on a nearobject, the medial rectus moves normally.This failure of the muscle action with certain co-ordinated eye movements only (i.e., limita-tion of adduction), while the opposite abducting eye shows nystagmus, is termed “internuclearophthalmoplegia”. It is characteristic of multi-ple sclerosis when seen in young people (whenthe internuclear ophthalmoplegia is usuallybilateral and is caused by a demyelinating lesionin the pons) but usually has a vascular cause inthe elderly (when it is usually unilateral).
Other Features
Other types of ocular muscle dysfunction, forexample a lateral rectus palsy or ptosis, are rare.Careful inspection of the fundi in some casesreveals inflammatory changes around theretinal vessels, especially in the periphery(peripheral retinal vasculitis).
Defects in the Visual FieldsThe pattern of a visual field defect gives usefullocalising information for lesions in the visualpathway. The right half of each retina is linked
by nerves to the right occipital cortex and thesplitting of nerve fibres from each half occurs at the chiasm. For this reason, lesions in the optic nerve anterior to the chiasm tend to cause unilateral defects, whereas those pos-terior to the chiasm produce hemianopic or quadrantianopic defects (Figure 22.5). Corticallesions tend to be more congruous. That is to say, the blind areas on each side tend to besimilar in shape and size. Cortical lesions alsoshow better preservation of central vision(“macular sparing”). A special type of fielddefect is seen with expanding pituitarytumours, the resulting pressure on the centre ofthe chiasm producing a bitemporal defect.Localised defects in the retina produce equiva-lent localised defects in the visual field on theaffected side. Defects because of ocular diseaseare relatively common as, for example, thoseseen in the elderly with glaucoma. Care must betaken to interpret field defects with this pos-sibility in mind. Notice from the diagram inFigure 22.5 that the right half of the visual field is represented in the left half of each retina and thus, the left half of the brain.This complies with the general rule that events occurring on the right side of the bodyare represented on the left side of the brain. It issurprising how patients might be unaware of asevere visual field defect, especially in hemi-anopia, providing that the macula is spared(Figure 22.6).
Retina
11
L R
Visual Fields
2
3
4
5
2
4
3
Optic nerve
Optic chiasma
Optic tract
Lateral geniculatebody
Optic radiation
Occipital cortex
Figure 22.5. The visual pathway.

Neuro-ophthalmology 185
Abnormalities of the PupilThe pupil constricts and dilates largely underthe action of the sphincter muscle, which linesthe pupil margin. It is supplied by parasym-pathetic fibres travelling within the third cranialnerve. The afferent stimulus is conveyed alongthe optic nerves and decussates at the opticchiasm and continues as the optic tract. Thespecific pupillomotor nerve fibres leave theoptic tract without synapsing in the lateralgeniculate nucleus and pass to the pretectalnucleus of the midbrain, where they synapsewith interneurons. The interneurons project toboth Edinger–Westphal nuclei (part of the thirdcranial nerve nucleus). The pupillomotor fibresthen travel within the third cranial nerve to thepupil constrictor muscles of the ipsilateral eyevia the ciliary ganglion (Figure 22.7).
The dilator muscle is arranged radially withinthe iris and responds to the sympathetic nervesconveyed in the sympathetic plexus overlyingthe internal carotid artery. These fibres, in turn,arise from the superior cervical ganglion. Thesympathetic supply to the dilator muscle, there-fore, runs a long course from the hypothalamusto the midbrain and spinal cord, and then upagain from the root of the neck with the inter-nal carotid artery.
Miosis refers to a small pupil, mydriasis to alarge pupil (big word, big pupil). The pupilgrows smaller with age, as does reactivity. Inyoung children the pupils are relatively largeand sometimes anxious parents bring up theirchildren because they are concerned about this.During sleep, the pupils become small. Whenexamining the eye with the ophthalmoscope, itis evident that the pupil constricts more vigor-ously when the macula is examined than whenthe more peripheral fundus is stimulated withthe ophthalmoscope light.When an eye is totallyblind, usually there is no light pupil reaction, butas a general rule, the pupils remain of equal size.It should be apparent from Figure 22.7 that thepatient with cortical blindness (lesion withinthe occipital cortex) might have a normal pupilreaction. We must also remember that a pupilmight not react to light because it is mechani-cally bound down to the lens by adhesions (pos-terior synechiae). When both maculae aredamaged by senile macular degeneration, the
My car keeps knocking my gate post.(Hemianopes should never drive)
Figure 22.6. The effects of hemianopia.
Ciliary ganglion
Optic tract
Lateral geniculatenucleus
Pretecto-oculomotortract
Pretectal nucleus
EdingerWestphalnucleus
Rednucleus
IIInerva
Opticnerve
Figure 22.7. The pupillary pathway.

pupils can be slightly wider than normal and might show sluggish reactions. A relativeafferent pupil defect (also known as a MarcusGunn pupil) implies optic nerve or severeretinal disease.
The Abnormally Dilated PupilThe most common reason for unilateral mydri-asis is drugs in the form of locally administeredeye drops, either prescribed by an ophthalmicdepartment or obtained from a friend’s medi-cine cabinet. The next most common cause isprobably the Adie’s pupil, a condition that ismore common in young female patients. Theaffected pupil is usually dilated and contractsslowly in response to direct and indirect stimu-lation. In bright light, the pupil might constrictslowly on the affected side and take some time todilate in the dark. The vision might also beblurred, particularly at near fixation because ofthe effect of the disease process on the ciliarymuscle (necessary for accommodation). Thepupillary constriction to near fixation is tonicand prolonged and worm-like. When this tonicpupil reaction is combined with absent tendonjerks in the limbs, it is known as Holmes–Adie syndrome. When the vision is blurred and the pupil widely dilated, the symptoms can be partially relieved by the use of a weakmiotic.After a delay of months or years,the othereye may become affected. The overall disabilityis minimal and the condition has not so far beenrelated to any other systemic disease. It isthought to have an underlying viral aetiology.
Acute narrow-angle glaucoma can occasion-ally present in this manner and confusion canarise if the eye is not red; however, closer exami-nation of the eye should make the diagnosisobvious. Because the nerve fibres, which causeconstriction of the pupil, are conveyed in the oculomotor nerve,oculomotor palsy if complete,is associated with mydriasis. For this reason,dilatation of the pupil can be a serious sign ofraised intracranial pressure after head injury.One pupil might be wider than the other as a con-genital abnormality (congenital anisocoria).
The Abnormally Constricted PupilAgain, drugs are a common cause. Miotic dropsare still encountered in the treatment of
glaucoma and the constricted pupils of the mor-phine addict are well known if not so commonlyseen. When a constricted pupil on one side isobserved it is important to note the position ofthe eyelids. A slight degree of associated ptosisindicates the possibility of Horner’s syndrome.The total syndrome comprises miosis, narrow-ing of the palpebral fissure because of paralysisof the smooth muscle in the eyelids (Müller’smuscle), loss of sweating over the affected sideof the forehead, a slight reduction of the intra-ocular pressure and enophthalmus (sunkenglobe). Horner’s syndrome can be caused by awide diversity of lesions anywhere along thesympathetic pathway. While a Pancoast’s apicallung tumour is classically associated withHorner’s syndrome, it is quite often noted in theelderly as an isolated finding and investigationfails to reveal a cause. The Argyll Robertson(AR) pupil is a rare but famous example of themiosed pupil, which responds to accom-modation but not to direct light. This type ofpupil reaction was originally described as beingclosely associated with syphilis of the centralnervous system. Visual acuity is normal in such patients.
Double VisionDouble vision (diplopia) can be monocular orbinocular. Monocular diplopia, that is, diplopiathat is still present when one eye is closed, isquite common and is usually due to a cataractor corneal disease. Some patients say that theycan see double when they mean that the visionis blurred.A clear distinction must, therefore, bemade. Binocular double vision of recent onsetshould always be treated as a serious symptom.It is usually disabling, preventing the patientfrom working or even walking about. Somepatients discover that the symptoms are relievedby placing a patch over one eye. Slight degreesof double vision can be compensated by a headtilt or turn and the nature of the adopted headposture can help to identify the cause of thedouble vision. In the same way, if the history is elucidated carefully, noting, for example,whether the diplopia is worse for near or dis-tance vision or whether there is horizontal orvertical displacement of the second image, thena possible cause can be suspected even beforeexamining the patient.
186 Common Eye Diseases and their Management

Assessment of Eye Movements in DiplopiaThe complaint of double vision suggests that theseparate eyes are not both fixed on the point ofregard. The eye that is “off line” sees the objectof regard but it appears displaced. This failureof the eyes to work together is because of mal-function of one or a group of eye muscles or theneurological mechanisms that control them.
From the clinical point of view, it is conven-ient to divide the eye muscles into horizontaland vertical groups. The horizontal muscles, themedial and lateral recti, are easy to understandbecause their actions are in one plane and theysimply adduct (turn in) or abduct (turn out) theglobe. The vertical recti are best considered ashaving primary and secondary actions. It isimportant to realise that the action of the ver-tical recti changes with the position of theglobe. For example, when the eye is abducted thesuperior rectus elevates the globe, but when the eye is adducted the superior rectus rotatesthe eye inwards round an anterior–posterioraxis (intorts). In a similar manner, the inferioroblique elevates the adducted eye and extortsthe abducted eye (Figure 22.8). In order to testthe action of the superior oblique muscle, onemust first ask the patient to adduct the eye andtest for depression in adduction. That is to say,a superior oblique palsy prevents the eye fromlooking down when it is turned in. The mainline of action of the vertical recti is seen when
the eye is abducted and that of the obliques isseen when the eye is adducted.
Examination of a patient with double visionentails first of all testing the gross eye move-ments in the cardinal positions of gaze and thennoting the degree of separation of the images inthese various positions. The Hess chart is one ofseveral ingenious methods of recording theabnormal eye movements. The principle is toplace a green filter before one eye and a red filterbefore the other and to ask the patient to lookat a screen on which are placed a number ofsmall illuminated white dots. The patient is thenasked to localise the dots with a pointer. Theamount of false localisation can then be meas-ured in all positions of gaze. This technique isinvaluable when assessing the recovery of anocular muscle palsy.
Young children adapt to double vision rapidlyby suppressing the image from one eye, andunder the age of eight years the suppression canlead to permanent amblyopia if the situation isnot relieved. In adults, the double vision maypersist and be disabling for months or evenyears if not treated by incorporating prisms intothe spectacles or by muscle surgery.
Causes of Diplopia
Ocular Muscle Imbalance
It will be recalled from the chapter on squintthat some patients have a latent squint, which iscontrolled much of the time but sometimesbecomes overt. A typical example is the hyper-metrope with esophoria who begins to com-plain of double vision when working for anexamination. This problem can be solved simplyby prescribing suitable spectacles. Sometimesanxious patients who have had a squint sincechildhood begin to notice their double visionagain, having suppressed one image for manyyears. The symptoms are usually relieved withthe cause of the anxiety.
Sixth Cranial Nerve Palsy
The affected eye is converged because of a weak-ness of the lateral rectus muscle. It occurs mostcommonly as an isolated microvascular episodein hypertensive elderly patients and heals spon-taneously in three to six months. Elderly dia-betics are also more prone to sixth cranial nerve
Neuro-ophthalmology 187
Superior rectus
Lateral rectus
Inferior rectusOptic nerva
Superior rectus
Medialrectus
Superioroblique
Figure 22.8. The extraocular muscles.

palsies. In young patients, the possibility of mul-tiple sclerosis or even raised intracranial pres-sure must be borne in mind.
Fourth Cranial Nerve Palsy
The eye fails to look down when it is turned inand might be turned slightly up when the othereye is looking straight ahead. Trauma (a blowover the head) is an important cause in youngerpatients but a full investigation for an intra-cranial space-occupying lesion is usually needed.
Third Cranial Nerve Palsy
The eye is turned out and slightly down, thepupil is dilated and ptosis is usually severeenough to close the eye. Trauma is an importantcause in young people but a posterior com-municating aneurysm should also be consid-ered, particularly if it is associated with pain.Other causes include demyelination, diabetes,microvascular occlusion and herpes zosterinfection. Recovery of nerve function particu-larly after compressive lesions can lead to a phe-nomenon known as aberrant regeneration. Thiscan manifest as atypical pupil or lid responseson attempted eye movement.
Thyrotoxicosis
Patients with this condition develop doublevision because the extraocular muscles becomeinfiltrated with inflammatory cells. The action
of the inferior recti in particular becomesimpaired and diplopia on upward gaze is acommon sign. When the inflammation hassettled, the infiltrating cells are replaced byfibrous tissue, further restricting muscle action.
Myasthenia Gravis
This disease presents sometimes with diplopiawith or preceded by ptosis,which becomes worseas the day goes by. Any one extraocular muscleor group of muscles can be affected. The symp-toms and signs show a transient improvementseconds after the intravenous injection of edro-phonium chloride (Tensilon). Diagnosis can beconfirmed by high serum titres of acetylcho-line receptor antibodies. Approximately 10% ofcases are associated with a thymoma, which canbecome malignant. A chest X-ray is, therefore,mandatory in any patient suspected of havingmyasthenia gravis. Treatment is with an anti-cholinesterase such as pyridostigmine.
Blow-out Fracture of the Orbit
A special cause of double vision following injuryis the trapping of extraocular muscles,usually theinferior rectus, in the line of fracture. The patientexperiences double vision on looking upwardsand the limitation of movement is evident.There might be a relative enophthalmos.Surgicalintervention to repair the orbital wall defectmight be required if the patient suffers from prolonged diplopia or marked enophthalmus.
188 Common Eye Diseases and their Management
Many eye diseases are inherited or have familialclustering. It is, therefore, always advisable toenquire about the family history when inter-viewing a patient with an ophthalmologicalcomplaint. Some types of inherited eye diseaselead to blindness and relatives of patients withsuch conditions often seek advice concerningtheir risk of developing the disease. Patientsmight also consult with a view to prenataltesting, particularly if the disease leads toblindness at a young age.
Recent advances in molecular biology haveled to a dramatic increase in our understandingof eye diseases. The discovery and the unravell-ing of the role of numerous ocular disease geneshas also helped in our understanding of normaleye development and functioning. Because ofthe advances made in ophthalmic moleculargenetics, we are now able to refer to an inher-ited ocular condition not only by the mode ofinheritance, but also to denote the abnormalchromosome, the abnormal gene’s position onthe chromosome and its nucleotide sequence.To date, over 150 different gene defects have been described for retinal conditions alone(www.sph.uth.tmc.edu/retnet/home.htm). Formany disorders, we also now know the role theabnormal gene plays in the pathogenesis ofthe disease, either because it leads to the pro-duction of an abnormally functioning proteinor because the gene defect leads to the abnor-mal regulation of nearby or distant genes. Oncethe abnormal gene product (protein) associatedwith a disease can be identified, then drugs can
be designed specifically, either to suppress itsproduction or to replace the lost function.
Examples of eye disease that have beenmapped out to different chromosomes areshown in Table 23.1.
Several methods are used in molecularbiology to link disease to particular gene loci.Work usually starts by finding and classifyingthe disease in question in a large family or seriesof families. Next, the disease chromosome issought (unless the inheritance pattern is X-linked, then this step can be omitted) and thenthe position of the gene in question is graduallynarrowed down (by the use of linkage analysisfollowed by chromosome walking). This usuallyproduces a region of the chromosome on whicha number of candidate genes are found.Sequencing of these genes and comparison withnormal individuals or animal models usuallyallows the disease gene to be identified (this canbe a very time-consuming operation). Once the sequence of the gene is known, this can becompared on computer databases with similarknown genes and the putative structure andfunction of the disease gene and its product can be determined. The potential of the latterhas been greatly improved by the project tosequence the entire human genome.
Eye screening in selected patients at risk ofinherited disease might detect important life-threatening conditions, for example familialadenomatous polyposis, retinoblastoma,Marfan’s syndrome, neurofibromatosis and vonHippel Lindau disease.
23Genetics and the Eye
189
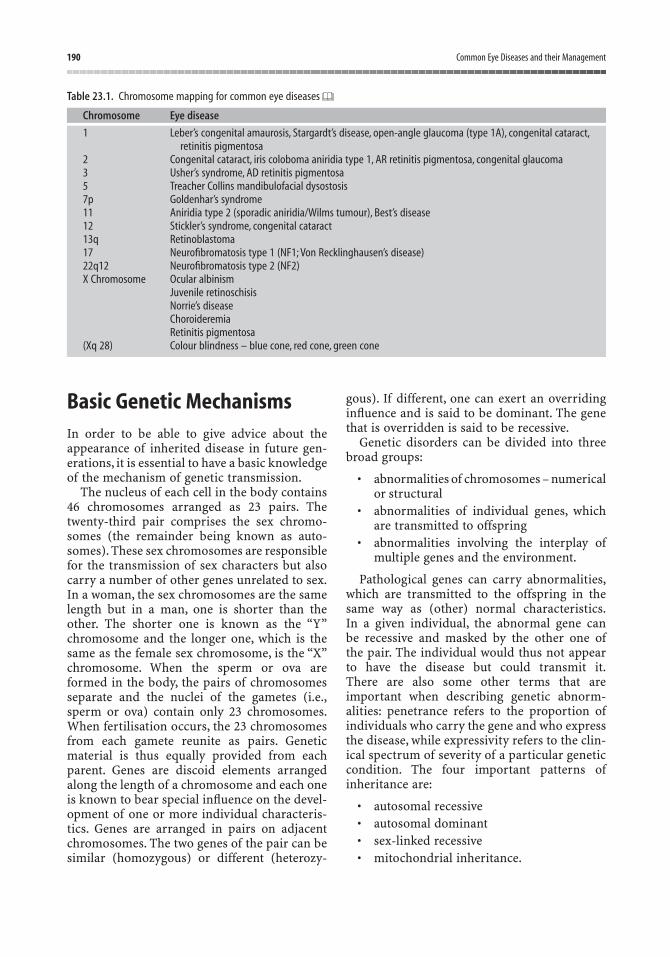
Basic Genetic MechanismsIn order to be able to give advice about theappearance of inherited disease in future gen-erations, it is essential to have a basic knowledgeof the mechanism of genetic transmission.
The nucleus of each cell in the body contains46 chromosomes arranged as 23 pairs. Thetwenty-third pair comprises the sex chromo-somes (the remainder being known as auto-somes). These sex chromosomes are responsiblefor the transmission of sex characters but alsocarry a number of other genes unrelated to sex.In a woman, the sex chromosomes are the samelength but in a man, one is shorter than the other. The shorter one is known as the “Y”chromosome and the longer one, which is thesame as the female sex chromosome, is the “X”chromosome. When the sperm or ova areformed in the body, the pairs of chromosomesseparate and the nuclei of the gametes (i.e.,sperm or ova) contain only 23 chromosomes.When fertilisation occurs, the 23 chromosomesfrom each gamete reunite as pairs. Geneticmaterial is thus equally provided from eachparent. Genes are discoid elements arrangedalong the length of a chromosome and each oneis known to bear special influence on the devel-opment of one or more individual characteris-tics. Genes are arranged in pairs on adjacentchromosomes. The two genes of the pair can besimilar (homozygous) or different (heterozy-
gous). If different, one can exert an overridinginfluence and is said to be dominant. The genethat is overridden is said to be recessive.
Genetic disorders can be divided into threebroad groups:
• abnormalities of chromosomes – numericalor structural
• abnormalities of individual genes, whichare transmitted to offspring
• abnormalities involving the interplay ofmultiple genes and the environment.
Pathological genes can carry abnormalities,which are transmitted to the offspring in thesame way as (other) normal characteristics.In a given individual, the abnormal gene can be recessive and masked by the other one ofthe pair. The individual would thus not appearto have the disease but could transmit it.There are also some other terms that are important when describing genetic abnorm-alities: penetrance refers to the proportion ofindividuals who carry the gene and who expressthe disease, while expressivity refers to the clin-ical spectrum of severity of a particular genetic condition. The four important patterns ofinheritance are:
• autosomal recessive• autosomal dominant• sex-linked recessive• mitochondrial inheritance.
190 Common Eye Diseases and their Management
Table 23.1. Chromosome mapping for common eye diseases
Chromosome Eye disease
1 Leber’s congenital amaurosis, Stargardt’s disease, open-angle glaucoma (type 1A), congenital cataract,retinitis pigmentosa
2 Congenital cataract, iris coloboma aniridia type 1, AR retinitis pigmentosa, congenital glaucoma 3 Usher’s syndrome, AD retinitis pigmentosa5 Treacher Collins mandibulofacial dysostosis7p Goldenhar’s syndrome11 Aniridia type 2 (sporadic aniridia/Wilms tumour), Best’s disease12 Stickler’s syndrome, congenital cataract13q Retinoblastoma17 Neurofibromatosis type 1 (NF1; Von Recklinghausen’s disease)22q12 Neurofibromatosis type 2 (NF2)X Chromosome Ocular albinism
Juvenile retinoschisisNorrie’s diseaseChoroideremiaRetinitis pigmentosa
(Xq 28) Colour blindness – blue cone, red cone, green cone
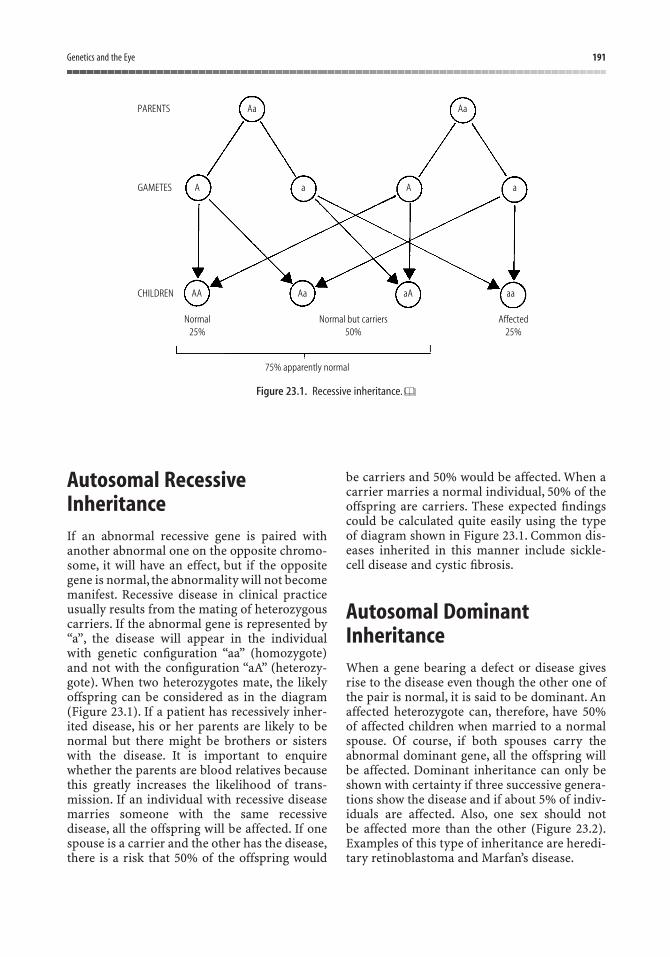
Autosomal RecessiveInheritanceIf an abnormal recessive gene is paired withanother abnormal one on the opposite chromo-some, it will have an effect, but if the oppositegene is normal, the abnormality will not becomemanifest. Recessive disease in clinical practiceusually results from the mating of heterozygouscarriers. If the abnormal gene is represented by“a”, the disease will appear in the individualwith genetic configuration “aa” (homozygote)and not with the configuration “aA” (heterozy-gote). When two heterozygotes mate, the likelyoffspring can be considered as in the diagram(Figure 23.1). If a patient has recessively inher-ited disease, his or her parents are likely to benormal but there might be brothers or sisterswith the disease. It is important to enquirewhether the parents are blood relatives becausethis greatly increases the likelihood of trans-mission. If an individual with recessive diseasemarries someone with the same recessivedisease, all the offspring will be affected. If onespouse is a carrier and the other has the disease,there is a risk that 50% of the offspring would
be carriers and 50% would be affected. When acarrier marries a normal individual, 50% of theoffspring are carriers. These expected findingscould be calculated quite easily using the typeof diagram shown in Figure 23.1. Common dis-eases inherited in this manner include sickle-cell disease and cystic fibrosis.
Autosomal DominantInheritanceWhen a gene bearing a defect or disease givesrise to the disease even though the other one ofthe pair is normal, it is said to be dominant. Anaffected heterozygote can, therefore, have 50% of affected children when married to a normalspouse. Of course, if both spouses carry theabnormal dominant gene, all the offspring willbe affected. Dominant inheritance can only beshown with certainty if three successive genera-tions show the disease and if about 5% of indiv-iduals are affected. Also, one sex should not be affected more than the other (Figure 23.2).Examples of this type of inheritance are heredi-tary retinoblastoma and Marfan’s disease.
Genetics and the Eye 191
AaPARENTS Aa
AGAMETES
AACHILDREN
Normal25%
Normal but carriers50%
Affected25%
75% apparently normal
Aa aA aa
a A a
Figure 23.1. Recessive inheritance.
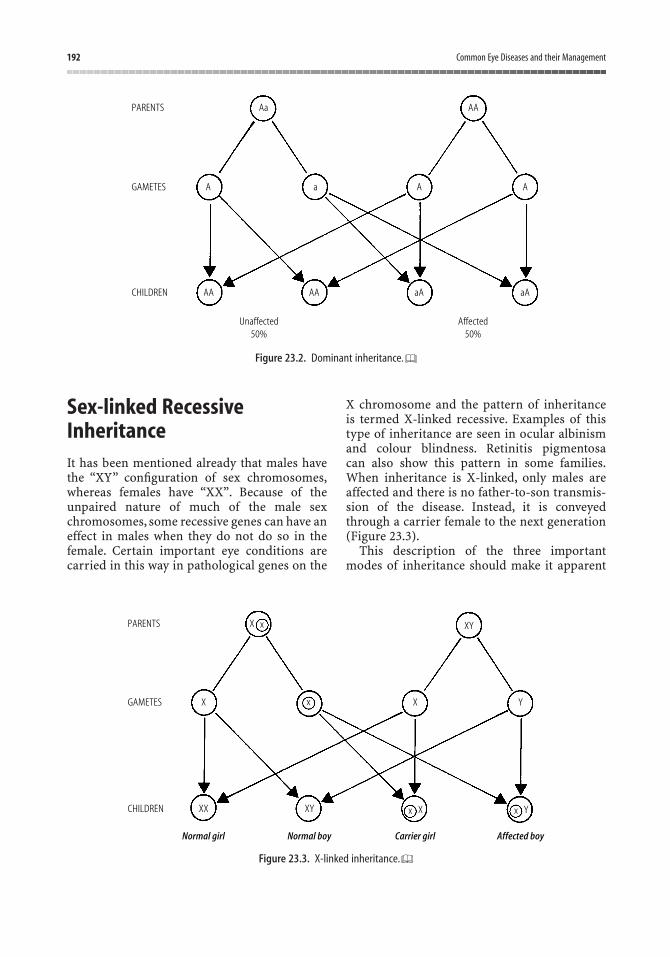
Sex-linked RecessiveInheritanceIt has been mentioned already that males havethe “XY” configuration of sex chromosomes,whereas females have “XX”. Because of theunpaired nature of much of the male sexchromosomes, some recessive genes can have aneffect in males when they do not do so in thefemale. Certain important eye conditions arecarried in this way in pathological genes on the
X chromosome and the pattern of inheritance is termed X-linked recessive. Examples of thistype of inheritance are seen in ocular albinismand colour blindness. Retinitis pigmentosa can also show this pattern in some families.When inheritance is X-linked, only males areaffected and there is no father-to-son transmis-sion of the disease. Instead, it is conveyedthrough a carrier female to the next generation(Figure 23.3).
This description of the three importantmodes of inheritance should make it apparent
192 Common Eye Diseases and their Management
Aa
A
AA
PARENTS
GAMETES
CHILDREN AA
Unaffected50%
Affected50%
aA aA
A Aa
AA
Figure 23.2. Dominant inheritance.
XPARENTS
X X
XYXX
Normal girl Normal boy Carrier girl Affected boy
Y
XYx
GAMETES
CHILDREN
x
x X x Y
Figure 23.3. X-linked inheritance.

that it is possible to predict the likely diseaseincidence in offspring. It should also be realisedthat such predictions can only be based oncareful and extensive investigation of the family.Although some eye diseases are known to followa fixed pattern of inheritance, others, notablyretinitis pigmentosa, can be inherited in differ-ent ways in different families. In most largecentres, there are now genetic clinics in whichtime is devoted specifically to the investigationof families and also to the detection of carriers.
Mitochondrial InheritanceMitochondria are the only organelles of the cellbesides the nucleus that contain their own DNA.They also have their own machinery for syn-thesising RNA and proteins. Instead of in-dividual chromosomes, mitochondria containcircular DNA similar to bacteria (from whichthey are thought to be derived). MitochondrialDNA contains 37 genes,predominately encodingthe enzymes necessary for the respiratory chain.All mitochondria in the zygote are derived from the ovum; therefore, a mother carrying a mito-chondrial DNA mutation will pass it on to all ofher children (maternal inheritance) but only herdaughters will pass it on to their children. Mito-chondrial DNA mutations are usually manifestclinically in tissues with a high metabolicdemand, for example brain, nerve, retina,muscle and renal tubule. Examples of ophthal-mic diseases caused by mitochondrial DNAmutations include Leber’s hereditary optic neu-ropathy, chronic progressive external ophthal-moplegia, maternally inherited diabetes anddeafness, and Kearns–Sayre syndrome.
Chromosomal AbnormalitiesMicroscopic studies of the chromosomes them-selves have revealed that abnormal numbers ofchromosomes can be produced by a fault at the
moment of fertilisation. These might be causedby changes in numbers or structure of chromo-somes. Numerical chromosomal changesinclude the absence of a chromosome (mono-somy), as in Turner’s syndrome, or an additionalchromosome (trisomy), as in Down’s syndrome.Cytogenetic studies have shown that patientswith Down’s syndrome have an additionalchromosome, which is indistinguishable fromchromosome 21. Down’s syndrome is morecommon in children born to older women andthe eye changes include narrow palpebralfissures with a characteristic slant, cataract, highmyopia and rather intriguing grey spots on theiris known as Brushfield’s spots. Brushfield’sspots are sometimes seen in otherwise normalindividuals. Turner’s syndrome (one missing Xchromosome) and Klinefelter’s syndrome (anextra X chromosome) are further examples ofdisease in which there are known to be abnor-malities of the chromosome, which are visibleunder the microscope. People with these lasttwo diseases are of interest to the ophthalmol-ogist on account of the abnormal but predic-table manner in which they inherit colour blindness.
Structural abnormalities occur when recom-bination or reconstitution in an altered formfollows chromosomal breaks. Such changes canbe in the form of deletions, duplication inver-sions, translocations or isochromosomes.
Multifactorial DiseasesThese are disorders that arise from an interplayof genetic and environmental influences. Thegenetic contribution is made up of at least twoabnormal genes acting in concert to express a“dosage-related” type effect, which is signifi-cantly influenced by several environmentalfactors. This leads to variable phenotypicexpression. Examples include diabetes mellitus,some malignancies and perhaps age-relatedmacular degeneration.
Genetics and the Eye 193
It is possible to achieve a high concentration ofmany drugs in the eye by applying them as eyedrops. In this way, a high local concentration canbe reached with minimal risk of systemic sideeffects. However, the systemic side effects ofdrops cannot be discounted, particularly in sus-ceptible individuals. For example, timolol dropscan precipitate asthma and slow the pulse ratein elderly patients, and pilocarpine drops cancause sweating and nausea. The action of localmedications can be prolonged by incorporatingthem in an ointment, but for most purposesdrops are supplied in 5 ml or 10 ml containers.After the container has been opened, it shouldnot be kept for longer than one month. In orderto avoid undue stinging, drops can be bufferedto near the pH of tears and they contain a pre-servative, such as benzalconium chloride. Itmust be borne in mind that patients whodevelop an allergic reaction to drops might bereacting to the preservative. Single-applicationcontainers are also used, which do not contain apreservative but are expensive.
Eye lotions are usually prescribed in 200 mlquantities and are used to irrigate the conjunc-tival sac. Sodium chloride eye lotion is used in first aid to flush out foreign bodies or irritant chemicals. Fresh mains tap water is anadequate substitute.
One of the major drawbacks of using eyedrops is that, although high local concentrationsof the drug are achieved in the anterior segmentof the eye, little if any drug penetrates to theposterior segment. Drops are, therefore, of little
use in treating diseases of the vitreous andretina. One way of delivering a drug to the posterior segment is to give it systemically.An example of this is the use of systemic pred-nisolone for posterior uveitis. This treatmentmethod has the drawback of systemic sideeffects. This can be reduced by delivering thedrug to the posterior segment by local injectioneither directly into the vitreous, along theorbital floor, within the sub-Tenon’s space or inthe subconjunctival space.
Treatment of InfectionChloramphenicol is rarely used as a systemicdrug nowadays, but it has been useful for manyyears in the form of eye drops. It remains a drugof choice in the UK for superficial eye infections.Other broad-spectrum antibiotics in useinclude gentamycin, framycetin, tobramycinand neomycin, as well as ciprofloxacin andofloxacin. When an infection of the eye is sus-pected, a culture is taken from the conjunctivalsac and treatment started with a wide-spectrumantibiotic. Systemic and intravitreal administra-tion might be needed if the infection is intra-ocular. A number of antiviral drugs are nowavailable, but acyclovir in the form of Zoviraxointment is the most widely used treatment ofherpes simplex keratitis. The use of systemicacyclovir and famcyclovir for herpes zosterophthalmicus has made a great impact on theseverity of ocular complications.
24Drugs and the Eye
195

Drops That Widen the PupilThe pupils can be dilated either by local block-ade of the parasympathetic pathway or by localstimulation of the sympathetic pathway.
Parasympathetic AntagonistsRoutine mydriasis to allow examination of thefundus is best achieved by tropicamide 0.5% or1% drops because the effect lasts for only about3 h. Cyclopentolate 1% (0.5% in babies) can lastfor 24 h, but because of its cycloplegic effect(blockade of accommodation) is preferable forthe examination of children’s eyes when refrac-tion is also needed. Dilating the pupil runs therisk of inducing an attack of acute narrow-angleglaucoma in a predisposed individual. Becausethe vision could remain blurred, driving shouldbe avoided within the first 6–8 h after mydriasis.Atropine in drop form is a long-acting mydri-atic, which is used when it is necessary toprevent or break down adhesions between irisand lens in acute iritis (posterior synechiae). Itis also used in the treatment of amblyopia inchildren. Its effect lasts for about seven days.Allergic reactions are quite common and occa-sionally systemic absorption can cause centralnervous system symptoms of atropine toxicity.
Sympathetic AgonistPhenylephrine (5 or 10% drops) is a sympath-omimetic amine. It is used with a parasym-pathetic antagonist when extremely wide pupildilation is required (e.g., for intraocular surgeryor for peripheral retinal examination). There arereports of severe acute hypertension after use of10% drops.
Drops That Constrict the PupilIn the past, meiotics have been widely used forthe treatment of chronic open-angle glaucoma.Pilocarpine is available in 1%, 2%, 3% or 4%solutions. Although it is effective in reducing the intra-ocular pressure, the side effects ofdimming of vision and accommodation spasmcan be disabling and mean that this treatmenthas largely been superceded. Pilocarpine is stillused in the treatment of acute glaucoma attacks
to constrict the pupil and open up the closeddrainage angle. Sometimes it is necessary toconstrict the pupil rapidly during the course ofintraocular surgery and this is achieved byinstilling acetylcholine directly into the anter-ior chamber. Strong meiotics run the risk ofcausing retinal detachment in susceptible indiv-iduals. Meiotics have been used to reverse the effect of mydriatic drops used for fundusexamination, but this practice is no longer recommended as a routine because it is unnecessary and the symptoms of meiosis maymake matters worse.
Drugs in the Treatment ofOpen-angle GlaucomaThere has been a small revolution involving thetype of eye drops used for the treatment of glau-coma in recent times. For years, the mainstay oftreatment was pilocarpine and the topical beta-blockers, for example timolol, but the potentialsystemic side effects of these drugs have led tothe introduction of other novel types of ocularhypotensive agents. In general, these new agents can be divided into alpha2-adrenergicagonists, carbonic anhydrase inhibitors andprostaglandin analogues.
The production of aqueous humour can bereduced by either blockade of the beta-receptorson the ciliary body epithelial cells (i.e., with a beta-blocker) or by agonism of the alpha2-receptors. Brimonidine and apraclonidine areboth alpha2-receptor agonists and show goodefficacy compared with timolol. A significantnumber of patients, however, do develop anallergy to these agents and this has limited theirwidespread use. Acetazolamide was introducedas a diuretic many years ago; although not a verygood diuretic, it has proved to be a potent ocularhypotensive when given orally. Again because ofside effects its use has been restricted to short-term treatment. In 1995, dorzolamide wasintroduced and more recently, brinzolamide has become available. These are also carbonicanhydrase inhibitors but they are available indrop form and are able to penetrate the cornea.Their ocular hypotensive effects are generallynot as great as topical beta-blockers but they areuseful as adjuvant agents. It has recently beendiscovered that a second aqueous outflow route
196 Common Eye Diseases and their Management

exists in the eye – the uveoscleral route. It isknown that certain prostaglandins increase theflow of aqueous via this route and a number oftopical prostaglandin F2a analogues are nowavailable. Latanoprost, travoprost and bimato-prost have all been shown to as effective astopical beta-blockers with minimal side effects.
All these medications have the problem ofcompliance. Elderly patients may forget to instilldrops on a regular basis. In some cases, eveninstillation of three different glaucoma dropsfails to control the intraocular pressure. In theseinstances, the only sure way of lowering the pressure is by glaucoma drainage surgery.
Drugs in the Treatment ofAcute Angle-closure GlaucomaAngle-closure glaucoma is a surgical problem.Once the acute attack has been aborted by theuse of intensive pilocarpine drops and Diamox,a small hole is made in the iris with theYttrium–Aluminium–Garnet (YAG) laser toallow redirection of the flow of aqueous. Inmany patients this provides a permanent cure.Beta-blockers may also be used during the acute stage and more recently the alpha2-agonist apraclonidine has been shown to be auseful adjunct.
Drugs in the Treatment ofAllergic Eye DiseaseWith the increasing incidence of atopy, the treat-ment of allergic eye disease has gained inimportance in recent years. Treatments aredesigned to interfere with either the type 1(immunoglobulin E [IgE]-mediated) or type 4(delayed) hypersensitivity response, both ofwhich are thought to be important in diseasepathogenesis. For mild disease, initial treatmentshould involve antigen avoidance (if known)and frequent use of artificial tears (hypromel-lose) to wash away antigens from the ocular andconjunctival surface. Treatment of more severedisease involves the use of systemic or topicalantihistamines (levocabastine, emedastine andazelastine), which are helpful for relief of symp-
toms, and topical mast cell stabilisers (sodiumcromoglicate, nedocromil sodium and lodox-amide), which are useful in disease preventionif used regularly. The treatment of severe (sight-threatening) disease involves the use of coursesof topical and occasionally oral steroids.
Local Anaesthesia inOphthalmologyProxymetacaine (Ophthaine) is a useful short-acting anaesthetic drop that is comfortable toinstill and so is particularly useful when exam-ining children.Amethocaine and benoxinate arealso widely used but are longer-acting and stingquite markedly. Local anaesthetic drops shouldnot be used as pain relievers on a long-termbasis because the anaesthetized cornea becomesulcerated and severe infection of the eye canoccur. Lignocaine (1% or 2%) with or withoutadrenaline is injected into the eyelids for lidsurgery. Local anaesthesia for intraocularsurgery is obtained by topical drops, sub-Tenon’s injection, periorbital injection (outsidethe cone of extraocular muscles) or sometimesretrobulbar injection (within the muscle cone)of lignocaine. For a longer effect, this is some-times combined with marcaine.
Drugs and Contact LensesAs a rule, contact lenses should not be wornwhen the eye is being treated with drops. Theexception is when the contact lenses themselvesare being used for some therapeutic purpose.Soft hydrophilic contact lenses can take up andstore the preservative from some kinds of drop.The preservative benzalkonium chloride is espe-cially liable to be absorbed onto a contact lens.When it is essential that drops are administeredto a patient wearing contact lenses, it is oftenpossible to prescribe in the form of single-dosecontainers that do not contain a preservative.
Artificial TearsArtificial tears provide one of a number of meas-ures that are used to treat tear deficiency. Othermeasures include occlusion of the lacrimal
Drugs and the Eye 197

puncta or the use of mucolytic agents. The firststep is to make the diagnosis. Once a deficiencyof tears has been confirmed, the mainstay oftreatment is hypromellose.Adsorptive polymersof acrylic acid can also give symptomatic relief.Polyvinyl alcohol is another compound presentin a number of tear substitutes. Recently, a newagent, sodium hyaluronate (0.1%) has beenshown to improve symptom relief and improvethe ocular surface abnormalities in cases ofsevere dry eye. By their nature, tear substitutestend to adhere to the surface of the eye and inthe conjunctival sac. For this reason, their pro-longed use is liable to give rise to preservativereactions. Preservative-free preparations areoften preferable. Some patients with a severe dryeye problem might need to instill the dropsevery hour or even more frequently.
Anti-inflammatory Drugs and the EyeLocal steroids are widely used in the treatmentof eye disease; systemic steroids are not usedunless the sight of the eye is threatened. It mustbe remembered that systemic steroids give thepatient a sense of well-being, which might givea false impression of the real benefit obtained.Furthermore, systemic steroids can have seriousand life-threatening side effects, such as ver-tebral collapse through osteoporosis and perfor-ated gastric ulcer (Figure 24.1).
Local steroids should also be applied withcaution, and it is a good rule always to have aspecific reason for giving them.That is to say,theyshould not be prescribed just to make red eyesturn white without a clear diagnosis.The reasonsfor this are two-fold: first, local steroids enhancethe multiplication of viruses, especially herpessimplex; and second, they can cause glaucoma incertain predisposed individuals. In such indiv-iduals, the instillation of one drop of steroid cancause a temporary rise of intraocular pressure.The most potent steroid in this respect is dexam-ethasone, followed by betamethasone, pred-nisolone and hydrocortisone.It has been claimedthat rimexolone, clobetasone and fluorometho-lone are relatively safe in this respect.
Recently, a number of nonsteroidal anti-inflammatory drugs (NSAIDs) have been madeavailable in topical form (diclofenac [Voltarol
Ophtha], ketorolac [Acular] and flurbiprofen[Ocufen]) to reduce our dependence on topicalsteroids. They have been shown to be of use inthe treatment of postcataract surgery inflam-mation and in reducing the pain after excimerlaser surgery and corneal abrasions.
Anti-angiogenic Drugs and the EyeUncontrolled angiogenesis (growth of newblood vessels) is a common finding in manypotentially blinding conditions, such as prolif-erative diabetic retinopathy, central retinal veinocclusion, wet age-related macular degenera-tion (ARMD) and retinopathy of prematurity.Inhibiting their growth offers us the hope ofdramatically reducing the number of patientsgoing blind each year. It is thought that theangiogenic response is caused by elevated levelsof a cytokine called vascular endothelial growthfactor (VEGF) produced by abnormal orischaemic cells within the eye. Attempts toreduce the levels of VEGF and hence turn off theangiogenic drive have involved intravitreal
198 Common Eye Diseases and their Management
Steroids give a patient a feelingof well-being. . . .
Figure 24.1. There might be a false impression of the realbenefit obtained.

injections of anti-VEGF antibodies or oligonu-cleotide aptamers, which bind VEGF, or theintravitreal/sub-Tenon’s injection of an anti-angiogenic steroid (triamcinolone). All of thesetreatments are showing great promise in clini-cal trials. An alternative mechanism of treat-ment is the destruction of preformed newvessels. Recently, a new type of treatment for wetARMD has seen the use of a light-activated dye,injected intravenously, which preferentiallylocates in the choroidal neovascular membrane(photodynamic therapy). Activation of the dyeby light of a specific wavelength causes throm-bosis and destruction of blood vessels harbour-ing the dye. Treatment of patients with oneparticular subtype of wet ARMD (classic withno occult blood vessels) has shown stabilisationof vision in 60–70% of cases.
Damage to the Eyes by DrugsAdministered SystemicallyThere are a number of drugs, which if given in excessive doses, can lead to severe visualhandicap and blindness. Some of these are stillavailable on prescription. Chloroquine andhydroxychloroquine in excessive doses can leadto pigmentary degeneration of the retina and
blindness. Certain antipsychotic drugs can alsocause fundus pigmentation in excessive doses;melleril and chlorpromazine have been incrim-inated in this respect in the past. Recently, anumber of cases of uveitis have been reportedin patients using bisphosphonates for the treat-ment and prevention of osteoporosis. Interest-ingly, sudden visual loss has been reported in a number of patients taking the oral anti-inflammatory COX-2 inhibitors (celecoxib androfecoxib). The vision has returned to normalupon cessation of treatment.
Apart from causing glaucoma in somepatients, systemic steroids are thought toincrease the rate of formation of cataracts.Ethambutol and isoniazid can cause opticatrophy. Sometimes excessive doses of quinineare taken as an abortifacient and as the patientsregain consciousness they are found to be blindfrom quinine toxicity. Methyl alcohol is toxic tothe ganglion cells of the retina and blindness isa hazard of meths drinkers. It sometimes con-taminates crudely prepared alcoholic beveragesleading to unexpected loss of vision. The list ofdrugs with ocular side effects is large and thereader should consult a specialised textbook for more information. Nowadays, disasters andindeed lawsuits should be avoidable if the drugliterature is checked before prescribing an unfamiliar drug.
Drugs and the Eye 199
Section VVisual Handicap

Blindness marks the failure or inefficacy ofophthalmological treatment. Once a patientbecomes permanently blind, he or she might belost from the care of the ophthalmologist. Thismeans that the ophthalmologist might not havepersonal experience of the size of the problemand might not be in a position to experience therelative incidences of different causes of blind-ness. The keeping of accurate statistics is ofgreat importance, and in order to keep statis-tical records it is necessary to have a cleardefinition of blindness. Many people who dreadblindness imagine having no perception of lightin each eye. Fortunately, this situation is uncom-mon, but many people are severely debilitatedby visual loss.
In the UK, the major problem is among theelderly where visual loss is often combined withdefective hearing. Sensory deprivation is thus amajor scourge at the present time; the problemis undoubtedly going to be much worse as theproportion of elderly people increases.
DefinitionIn the UK, the statutory definition of blindnessrefers to persons who “are so blind as to beunable to perform any work for which eyesightis essential”. When a patient’s vision falls belowthis level, registration as a blind person can beconsidered. This is a voluntary process, whichallows the patient access to the social servicesfor the visually handicapped, as well as certain
tax concessions. Registration is usually initiatedin the hospital clinic. Some patients are referredby their general practitioners or social workersfor registration by the ophthalmic specialist. Aspecial form is completed and copies go to thepatient, the general practitioner, the social serv-ices department and the Office of Populationand Censuses.
Certain guidelines are laid down when con-sidering blind registration; the visual acuityshould be less than 3/60 in the worse eye but ifthe field of vision is constricted, the visual acuity might be better than this. Patients whosevision is not bad enough for blind registrationbut none the less have significant visual handi-cap can have their name placed on the partiallysighted register. In these patients the binocularvision should normally be worse than 6/18.Patients sometimes erroneously claim thebenefits of the partially sighted because theyhave only one eye, even though the remainingeye is normal. When the vision with one or botheyes is 6/18 or better, the patient is not usuallyconsidered to be partially sighted.When one eyeis completely lost through injury or disease, theamount of incapacity is set for medicolegal pur-poses at about 10%. In actual fact, the amount ofincapacity depends a great deal on the age of thepatient.A child can adapt to a remarkable degreeto being one-eyed, even to the extent of beingable to perform with skill at ball games. Adultswho become one-eyed find difficulty in judgingdistances or performing fine manual tasks.More importantly, a number of occupations are
25Blindness
203
specifically barred to those whose vision is poorin one eye.
Benefits for the VisuallyHandicappedThere is no blind pension in the UK but thoseregistered blind have a special income taxallowance and some exemptions from deduc-tions from income support. Blind persons canhave parking concessions and a free NationalHealth Service (NHS) sight test, as well as railcards and bus passes. Disability living allowancecan be available for blind people under the age of65 years but for the over-65s, only those who areboth blind and deaf can qualify. Those seekingthese concessions should consult an expert in thefield. There are a number of voluntary organisa-tions that run clubs, social centres and supplyvarious other aids and benefits. For example, theRoyal National Institute for the Blind (RNIB)provides a comprehensive range of servicesincluding the popular talking-book service. Italso supplies regular funds for research into thecauses of blindness.
The system of registration applies equally tochildren. In this instance, registration callsattention to the need for special educationalrequirements. These can include a specialistresource teacher, low visual aids, and otherspecial supplies and equipment. If necessary,special schooling might need to be considered.
Standards of Vision forVarious OccupationsThe standards for various occupations can varyfrom year to year and are more or less exacting,depending on the occupation. In the UK, inorder to drive a private motor vehicle, one mustbe able, in good daylight, to read a number platewith glasses or contact lenses at 67 feet or 20.5 m.A full binocular field of vision is also nowrequired. This must extend at least 120° horizon-tally and 20° above and below. The field is measured by perimetry using a standard target.It is assumed that any healthy person applyingto drive has a normal field of vision but if thedriver has any eye condition that might lead tovisual handicap, he or she must declare it. Thedriver and vehicle licensing centre might then
ask for a report from an ophthalmologist or anoptometrist. Double vision is a bar to driving, ifit cannot be corrected by prisms in the glassesor the wearing of an eye patch.
Colour BlindnessThis is not blindness in any sense of the word andindeed some colour-blind individuals areunaware of any problem until their colour visionis tested.Of the male population,8% suffers fromsome form of congenital colour blindness. Thisis usually in the form of “red–green blindness”.Inheritance of this type of defect is sex-linked sothat unaffected female carriers pass the gene to 50% of their sons. The screening of schoolchildren for colour blindness is now widely practiced because of the occupational implica-tions. The Ishihara test is the simplest and thebest test for congenital colour blindness. Occu-pations that entail the reading of colouredwarning lights or the matching of colours usuallydemand some form of colour vision test on entry.It is an advantage to the child to be aware of anydefect during the early years of schooling.
Incidence and Causes of BlindnessIn England and Wales, the prevalence of blind-ness in 1980 for children under five years was9:100,000. This figure increased to 2324:100,000for adults over 75 years. In the western world,blindness in children is largely because of inher-ited genetic disease and birth trauma. In adultsaged 20–60 years, the major causes are diseasesof the retina, including diabetic retinopathy andoptic atrophy. Over the age of 60 years, maculardegeneration, glaucoma and cataract are theimportant problems.
In Africa and Asia, the causes of blindness arerather different; many children become blindfrom corneal scarring associated with vitamin A deficiency and measles. Cataract is the mostimportant cause in adults but in certain areas,for example southern Sudan, onchocerciasisand trachoma are still a serious problem.
It is apparent that the problems of blindnessin Europe and North America are different fromthose in poorer parts of the world where muchcould still be done by improving standards ofnutrition and living conditions.
204 Common Eye Diseases and their Management

Aids for the BlindThe most widely recognised aid and symbol ofblindness is the white stick. It is also one of themost useful aids because it identifies the patientas blind and encourages others to give assis-tance. Many blind people are concerned thatthey appear ill-mannered when failing to recog-nise someone and are grateful for some indica-tion of their handicap.
Many different electronic devices have beentried but by and large these are only useful toyounger patients who can make full use of them.Scanning systems are now available which,when moved across the page, can read out thepage. Most blind patients are unable to affordthis type of aid. Many of these devices rely onthe patient’s hearing to identify an audiblewarning signal, but most blind people prefer touse their undistracted sense of hearing as animportant clue to their whereabouts.
Guide dogs are specially trained by the GuideDogs for the Blind Society and the patient mustalso take part in the training. Some youngpeople find that a guide dog can expand theirmobility to a great degree.
Certain tactile aids are also useful, the bestknown of which is Braille. This system ofreading for the blind was introduced fromFrance more than 100 years ago. The letters ofthe alphabet are represented by numbers ofraised dots on stiff paper. Blind children canlearn Braille rapidly and develop a high readingspeed. Some adults find that their fingers are notsufficiently sensitive and this applies especiallyto diabetics. Books in Braille are now availablein many different languages. Tape recordings ofbooks and newspapers are now very popularamong blind and partially sighted people ofall ages. The Talking-Book Service provides acomprehensive library for the use of the visually disabled.
There are numerous other gadgets that can be helpful to the blind and partially sighted;a popular one is the device that can indicatewhether a teacup is full or not. For those withsome residual vision, a special telephone padwith large numbers on it can be helpful. Otheringenious devices range from relief maps thatcan be felt by the blind person, to a telephonethat speaks back through the earpiece the digitthat has just been pressed. Research has alsobeen carried out on aids that signal the positionof objects by means of electrical stimuli to the
skin and even by means of implanted electrodesin the visual cortex.
One important advance has been voice synthesis by computers. Many current modelshave this facility, so that the user can hearemails, and programmes are available to allowprinting in Braille. In spite of these advances, theelderly visually handicapped patient can benefitmost from someone who is prepared to give thetime to read out letters or books. Some volun-tary local societies can provide this service.
When the patient has a visual acuity of betterthan 6/60, much can be achieved by the use ofoptical magnification. An ordinary hand mag-nifying glass is the simplest and can often be themost effective form of assistance. If this is notadequate and the patient has been a keen reader,a telescopic lens can be fitted to a spectacleframe with advantage. These multi-lens systemsare known as low visual aids and hence thepopular “LVA” clinics in eye departments for thetesting and provision of these items. Apart fromspecial telescopic lenses, closed-circuit televi-sion aids are now available: a small televisioncamera is held over the page and a magnifiedview of the written material is presented on atelevision screen.
The well-being of a blind or partially sightedperson can be greatly enhanced by relativelysimple social measures. Advice in the homeabout the use of gas or electricity can be impor-tant and the patient can be made aware of theavailability of local social clubs for the blind orkeep-fit classes and bus outings. An elderlypatient who plays the piano can be helped by the provision of an enlarged photocopy of a favourite piece of music. In spite of all these various possibilities, one must not for-get that the simplest and most useful reading aid for a partially sighted person is a good light directed onto the page. The distance ofthe bulb from the page is as important as thewattage of the bulb.
Artificial EyesThese can be made of glass or plastic molded to the shape of the eye socket and painted tomatch the other eye. Usually they are removedand washed at night by the patient and replacedthe following morning. A slight degree of dis-charge from the socket is the rule but excessive
Blindness 205

discharge can indicate that the socket is becom-ing infected. This, in turn, might be because ofroughening of the artificial eye with wear. Underthese circumstances, arrangements should bemade for the prosthesis to be replaced or pol-ished. It should always be borne in mind that apatient with an artificial eye might have had theeye removed because it contained a malignanttumour, in which case one must consider the possibility of local or systemic spread of thetumour. A well-made artificial eye is almostundetectable to the untrained eye but normalmovements of the eye can be restricted. Nowa-days, the use of orbital prostheses deep to theconjunctiva and attached to the eye muscles givesgreatly increased movement. After many yearsand after renewing the artificial eye on severaloccasions,the eye can appear to sink downwards.
Surgical removal of an eye (enucleation) is con-sidered in the following circumstances:
• when the eye is blind and painful• when the eye contains a malignant tumour• when the eye is nearly blind and sym-
pathetic ophthalmitis is a risk following aperforating injury.
Before having an eye removed, the patientmust be made fully aware of all the advantagesand disadvantages. A general anaesthetic isneeded and the patient remains in hospital forone to two nights after the operation. It iscommon practice to fit the socket with a trans-parent plastic “shell” for a few weeks until theartificial eye is fitted.
206 Common Eye Diseases and their Management

Bron AJ, Tripathi R, Watwick R, Marshall J.Wolff ’s anatomy of the eye and orbit, 8thedn. London: Chapman & Hall, 1997.
Hamilton AMP, Gregson R, Fish GE. Text atlas ofthe retina. London: Martin Dunitz, 1998.
Kanski JJ. Clinical ophthalmology, 5th edn.Oxford: Butterworth-Heinemann, 2003.
Tasman W, Jaeger EA, Parks MM, Benson WE.Duane’s clinical ophthalmology (six volumes).Philadelphia, PA: Lippincott-Raven, 2004.
Further Reading
207

Anti-inflammatory drugs, 198Antiangiogenic drugs, 198–199Aqueous humor, 13–14Arcuate scotoma, 94Arcus senilis, 50, 57, 150Artificial eyes, 205–206Artificial tears, 197–198Atopic conjunctivitis, 49Autoimmunity in uveitis,
147–148management, 148
Autosomal dominant inheritance,191
Autosomal recessive inheritance,191
BBacterial conjunctivitis, 46–47Band degeneration, 57–58, 78Basal cell carcinoma, 43,
124–125Benign vascular tumors of
eyelids, 124Binocular vision, 5, 111–112, 116,
118, 161Blepharitis, 41Blepharospasm, 38–39Blindness, 203–207
aids for blind, 205artificial eyes, 205–206causes of, 204color blindness, 204defined, 203–204incidence, 204
Index
209
AAcanthamoeba, 55Accommodation, 14, 30, 67, 81, 95,
113, 139, 158, 161, 178, 182,186, 196
Acquired immune deficiencysyndrome, 176–178
neoplasms, 177neuro-ophthalmological signs,
177–178noninfectious retinopathy, 177ophthalmological signs,
177–178opportunistic infections, 177
Acuity testing, 137–140Acute angle closure glaucoma,
97–100, 197acute attack, 98pathogenesis, 97signs, 98–99subacute attack, 97–98symptoms, 97–98treatment, 99–100
Acute glaucoma, 63–64Acute hemorrhagic conjunctivitis,
48Acute iritis, 64Acute keratitis, 64Adenoviral conjunctivitis, 48Adnexae, tumors of, 121–128Age, effect on retinal blood
vessels, 172Aging eye, 149–156
cataract, 153
changes in eye, 149–150external eye, 149–150globe, 150
eye disease in elderly, 150–156eyelid deformities, 153–154glaucoma, 153macular degeneration, age-
related, 150–153management, 151–153
stroke, 154–155temporal arteritis, 154
AIDS. See Acquired immunedeficiency syndrome
Aids for blind, 205Albinism, 159–160, 190, 192Allergic conjunctivitis, 49Allergic eye disease, 197Amblyopia of disuse, 113, 161Anatomy of eye, 7–16Anemia, 174Anesthesia, 197Aniridia, 160Anterior chamber, contusion, 130Anterior uveitis, 141–144
causes, 143complications, 143heterochromic iridocyclitis, 144pars planitis, 144signs, 141–143sympathetic ophthalmia,
143–144symptoms, 141treatment and management,
144

Blindness (cont.)occupational standards of
vision, 204visually handicapped, 204
Blood pressure, effect on retinalvessels, 172–173
Blood supply of eye, 10Bowman’s layer, 8Bruch’s membrane, 9, 14, 150–151Brushfield’s spots, 193Buphthalmos, 101, 160
CCapillary hemangioma of
newborn, 124Career in ophthalmology, 5Cataract, 81–90, 153
age, 82congenital factors, 84contusion, 83diabetes, 82–83etiology, 82–84lens, 81–82management, 86–89opthalmoscopy, 85–86perforation, 83radiation, 83–84secondary causes, 83
to disease elsewhere, 83to disease in eye, 83
signs, 85–86slit-lamp microscopy, 86surgery, 87
age of patient, 87cataract operation, 88convalescence, 89time spent in hospital, 89traumatic cataract, 87–88
symptoms, 84–85toxicity, 84trauma, 83–84visual acuity reduction, 85
Cavernous hemangioma, 124, 127Central retinal vein thrombosis,
68, 100Cerebrospinal fluid, 71–72Chalazion, 123Chemical injuries, 134Childhood squint, 112–116Child’s eye, 157–164
adult eye, contrasted, 157amblyopia of disuse, 161congenital eye defects, 159–161
epicanthus, 159examination, 157–158globe, structural abnormalities,
160–161aniridia, 160congenital cataract, 160–161
juvenile macular degeneration,162–163
lacrimal obstruction, 159leucocoria, 161nystagmus, congenital, 159–160
albinism, 160motor congenital nystagmus,
159sensory congenital
nystagmus, 159spasmus nutans, 160
Ophthalmia neonatorum, 162optic atrophy, 162phakomatoses, 163ptosis, 159refraction abnormalities, 161retinopathy of prematurity,
161–162screening, 158–159squint, 161uveitis, 162
Chlamydial conjunctivitis, 47–48Choroid, contusion, 131Choroidal melanoma, 121–122Choroidal metastases, 122Chromosomal abnormalities, 190,
193Ciliary body, 14Color blindness, 204Color vision, 19Congenital albinism, 160Congenital cataract, 160–161Congenital glaucoma, 101–102Congenital motor congenital
nystagmus, 159Congenital sensory congenital
nystagmus, 159Congenital spasmus nutans, 160Conjunctival disease, 45–60
conjunctivitis, 45–51acute hemorrhagic
conjunctivitis, 48adenoviral conjunctivitis,
48allergic conjunctivitis, 49bacterial conjunctivitis,
46–47
210 Index
causes, 46chlamydial conjunctivitis,
47–48conjunctival culture, 46herpes simplex
conjunctivitis, 48infective agents, 49microscopy, 46secondary conjunctivitis,
50–51signs, 46symptoms, 45trachoma, 48
corneal foreign body, 36, 51–53,129, 158
signs and symptoms, 51–52treatment, 52–53
subconjunctival hemorrhage,45
Conjunctival tumors, 125–126benign lesions, 125–126benign pigmented lesions,
125–126malignant lesions, 126melanoma of conjunctiva,
126nonpigmented lesions, 126
Conjunctivitis, 45–51, 61–63acute conjunctivitis, 62causes, 46chronic conjunctivitis, 62–63conjunctival culture, 46microscopy, 46signs, 46symptoms, 45
Contact lenses, 77–78, 197cosmetic, 78indications, 78side-effects, 77–78therapeutic, 78types, 77
Contusion, 129–131anterior chamber, 130choroid, 131cornea, 129–130iris, 130–131lens, 131optic nerve, 131retina, 131vitreous, 131
Cornea, 13contusion, 129–130layers, 8

transparencyanatomical, 13physiological, 13
Corneal disease, 45–60absent corneal sensation, 58–59corneal degenerations, 57–58corneal dystrophies, 57corneal edema, 58corneal ulceration, 53–57
corneal ulcer, 53–57Corneal nerve supply, 56Corneal ulcer, 53–57
bacteria, 54–55direct trauma, 53–54
Cortical connections, 11Cosmetic contact lenses, 78Cryobuckle, 109Cytomegalovirus retinitis, 177
DDacryocystitis, acute, 35–36Deformities of eyelids, 37–40
blepharospasm, 38–39ectropion, 38entropion, 38epicanthus, 37–38ingrowing eyelashes, 39–40lagophthalmos, 38normal eyelid, 37ptosis, 39
causes, 39redundant lid skin, 39
Dendritic ulcer, 55–56Dermoid cyst, 42–43, 127Descemet’s membrane, 8Detachment, retinal, 103–110
exudative retinal detachment,104
flashes, 106incidence, 103pathogenesis, 103–104
classification, 104rhegmatogenous retinal
detachment, 104–106breaks in retinal detachment,
104–105mechanism of, 105–106posterior vitreous
detachment, 105retinal breaks formation, 105retinal degeneration, 105with trauma, 106vitreous, 105
signs and symptoms, 106–107tractional retinal detachment,
104Diabetes, 82–83, 100, 165–170
anterior chamber, 166background retinopathy, 167control of, 169cornea, 165–166diabetic maculopathy, 168–169
diffuse edema, 168–169focal, 168ischemic, 169
eyelids, 165glaucoma surgery, 170iris, 166laser photocoagulation,
169–170lens, 166ocular movements, 165preproliferative stage, 167–168prognosis, 170proliferative retinopathy, 168retina, 167treatment, 169vitreo-retinal surgery, 170
Diplopia. See Double visionDouble vision, 18, 41, 84, 112, 118,
127, 154, 172, 186–188blow-out fracture of orbit, 188causes of, 187–188eye movement assessment, 187fourth cranial nerve palsy, 188myasthenia gravis, 188ocular muscle imbalance, 187sixth cranial nerve palsy,
187–188third cranial nerve palsy, 188thyrotoxicosis, 188
Drops constricting pupil, 196Drops widening pupil, 196Drugs, 195–200
acute angle closure glaucoma,197
allergic eye disease, 197anti-inflammatory drugs, 198antiangiogenic drugs, 198–199artificial tears, 197–198contact lenses, 197drops constricting pupil, 196drops widening pupil, 196infection treatment, 195local anesthesia, 197open angle glaucoma, 196–197
Index 211
parasympathetic antagonists,196
sympathetic agonist, 196systemically-administered
drug, damage to eyes by,199
Dry eye, 36–37causes, 36management, 37Schirmer’s test, 36–37signs, 36–37slit-lamp examination, 36tear film break-up time, 37
EEctropion, 38Emboli, 174Endophthalmitis, 148Endothelium, eye, 8Entropion, 38Epicanthus, 37–38, 159Episcleritis, 63, 148Examination of eye, 17–26
color vision, 19external eye, 20–21glasses, 19–20globe, 21–22initiation of, 20–22lids, 20–21ophthalmoscope use, 22–24pupil evaluation, 20tests, 25–26visual acuity, 17–19visual field, 19
Exophthalmos, 127–128External eye, 20–21Extraocular muscle anatomy,
116–117Extraocular muscles, 12Exudative retinal detachment,
104, 107Eyelashes, ingrowing, 39–40Eyelid deformities, 37–40,
153–154blepharospasm, 38–39ectropion, 38entropion, 38epicanthus, 37–38ingrowing eyelashes, 39–40lagophthalmos, 38normal eyelid, 37ptosis, 39redundant lid skin, 39

Eyelid disease, 33–44allergic disease of eyelids, 43dry eye, 36–37
causes, 36management, 37Schirmer’s test, 36–37signs, 36–37slit-lamp examination, 36tear film break-up time, 37
infections of eyelids, 40–41blepharitis, 41meibomian gland infection,
40Molluscum contagiosum, 41orbital cellulitis, 41styes, 40–41
lid injuries, 43–44lid tumors, 41–43
benign tumors, 41–43malignant tumors, 43
watering eye, 33–36tear drainage, 33–36tear secretion, 36
Eyelid injury, 133Eyelid tumor, 123–125
basal cell carcinoma, 124–125benign tumors, 123–124benign vascular tumors of
eyelids, 124capillary hemangioma of
newborn, 124cavernous hemangioma, 124Kaposi sarcoma, 124keratoacanthoma, 123malignant tumors of eyelids,
124–125meibomian cysts, 123melanoma of eyelid, 125Molluscum contagiosum, 123papilloma, 123sebaceous gland carcinoma,
125seborrhoeic keratosis, 123senile keratosis, 123squamous cell carcinoma, 125telangiectatic hemangioma, 124xanthelasma, 123
Eyelids, 11–13
FFacial skeleton abnormalities, 114Flashes, 106Floaters, 106
Fluorescein angiography, 18, 121,152, 169
Fusion, 111, 160
GGanglion cells, axons of, 11Genetic abnormalities, 190Genetics, 189–194
autosomal dominantinheritance, 191
autosomal recessiveinheritance, 191
chromosomal abnormalities,190, 193
genetic abnormalities, 190genetic mechanisms, 190mitochondrial inheritance, 193multifactorial diseases, 193multiple genes, 190sex-linked recessive
inheritance, 192–193Giant cell arteritis, 72–73, 154Glasses, 19–20
measuring for, 139–140automated refraction,
139–140objective refraction, 139subjective refraction, 139
Glaucoma, 91–102, 153acute angle closure glaucoma,
97–100acute attack, 98natural history, 97pathogenesis, 97signs, 98–99subacute attack, 97–98symptoms, 97–98treatment, 99–100
clinical types, 92–102congenital glaucoma, 101–102developmental glaucoma,
101–102intraocular pressure
maintenance of, 91–92measurement of, 92normal, 91
neovascular, 64–65normal pressure glaucoma, 97
management, 97primary open angle glaucoma,
92–96natural history, 93pathogenesis, 93
212 Index
signs, 93–94symptoms, 93treatment, 95–96
secondary glaucoma, 100–101to abnormalities in lens, 101drug-induced glaucoma, 101to trauma, 101to tumors, 100–101to uveitis, 100to vascular disease in eye,
100surgery, 170
Glioma of optic nerve, 127Globe, 7–8, 21–22
anterior chamber, 7anterior segment, 8aqueous humor, 7blood, 8coats of, outer fibrous layer, 7compartments of, 7inner nervous layer, 7intraocular fluids, 7middle vascular layer, 7outer fibrous layer, 7posterior chamber, 7posterior segment, 8segments, 8structural abnormalities,
160–161aniridia, 160congenital cataract, 160–161
uveal tract, 7vitreous chamber, 7vitreous humor, 7–8
Globe injuries, 129–133contusion, 129–131
anterior chamber, 130choroid, 131cornea, 129–130iris, 130–131lens, 131optic nerve, 131retina, 131vitreous, 131
perforation, 131–133intraocular foreign body, 132sympathetic ophthalmia,
132–133Globe tumors, 121–123
choroidal melanoma, 121–122choroidal metastases, 122melanoma of iris, 122–123retinoblastoma, 122
Gonioscopy, 99, 101Grave’s disease, 170
HHay fever conjunctivitis, 49Headache, 71–76
blood, 73blood vessels, 72–73bones, 73–74cerebrospinal fluid, 71–72classification, 71drugs, 75eyes, 74meninges, 74nerves, 73pain, referred, 74–75patient history, 71post-traumatic headache, 75
Hemangioma, 42, 128Hemorrhage, subconjunctival, 45Herpes simplex conjunctivitis, 48Herpes simplex keratitis, 55–56Herpes zoster ophthalmicus,
59–60Hess screen, 118Heterochromic iridocyclitis, 144Histoplasmosis, 147Horizontal recti, 116Hypertension
age, effect on retinal bloodvessels, 172
blood pressure, effect on retinalvessels, 172–173
malignant hypertension, 173vascular changes associated
with, 173–174emboli, 174ischemic optic neuropathy,
174retinal vascular occlusion,
173Hypopyon, 54, 142–143
IIdiopathic orbital inflammatory
disease, 127Infections of eyelids, 40–41
blepharitis, 41meibomian gland infection,
40Molluscum contagiosum, 41orbital cellulitis, 41styes, 40–41
Inflamed eye, 141–148anterior uveitis, 141–144
causes, 143complications, 143heterochromic iridocyclitis,
144pars planitis, 144signs, 141–143sympathetic ophthalmia,
143–144symptoms, 141treatment and management,
144autoimmunity in uveitis,
147–148management, 148
endophthalmitis, 148episcleritis, 148panophthalmitis, 148posterior uveitis, 144–147
causes, 145presumed ocular
histoplasmosis, 147sarcoidosis, 146–147signs, 145symptoms, 144–145syphilis, 147toxocariasis, 146toxoplasmosis, 145–146tuberculosis, 146
scleritis, 148Inner layer of eye, 9Intermediate uveitis, 144Intraocular foreign body, 132Iris, contusion, 130–131Ischemic optic neuropathy, 174
JJuvenile macular degeneration,
162–163
KKaposi sarcoma, 124Keratic precipitates, 142Keratoacanthoma, 123Keratoconus, 30, 49, 57, 78
LLacrimal apparatus, 12–13Lacrimal gland tumor, 127Lacrimal obstruction, 159Lacrimal passageway, 33–35Lagophthalmos, 38
Index 213
Laser photocoagulation, 169–170Lens, 14
contusion, 131Leucocoria, 161Leukemias, 174–175Lid tumors, 41–43
benign tumors, 41–43dermoid cyst, 42–43hemangioma, 42nevus, 42papilloma, 41–42xanthelasma, 43
malignant tumors, 43basal cell carcinoma, 43squamous cell carcinoma, 43
Local anesthesia, 197Long sight, 29–32Lymphoproliferative disease, 128
MMacular degeneration, age-
related, 150–153management, 151–153
Maddox rod, 118Maddox wing, 117–118Malignant hypertension, 173Malignant tumors of eyelids,
124–125Meibomian gland infection, 40Melanoma of conjunctiva, 126Melanoma of eyelid, 125Melanoma of iris, 122–123Meninges, 74Metastatic tumors, 127Middle layer of eye, 9Mitochondrial inheritance, 193Molluscum contagiosum, 41Motor congenital nystagmus, 159Mucocele of sinuses, 128Multifactorial diseases, 193Multiple genes, 190Multiple sclerosis, 183–184
internuclear ophthalmoplegia,183–184
nystagmus, 183ocular findings, 183–184optic neuritis, 183retrobulbar neuritis, 183
NNeovascular glaucoma, 64–65Neuro-ophthalmology, 179–188
double vision, 186–188

Neuro-ophthalmology (cont.)blow-out fracture of orbit,
188causes of, 187–188eye movement assessment,
187fourth cranial nerve palsy,
188myasthenia gravis, 188ocular muscle imbalance, 187sixth cranial nerve palsy,
187–188third cranial nerve palsy, 188thyrotoxicosis, 188
multiple sclerosis, 183–184internuclear
ophthalmoplegia, 183–184nystagmus, 183ocular findings, 183–184optic neuritis, 183
optic disc, 179–183atrophy, optic, 180–181central cup, 180color, 179congenital disc anomalies,
180hemorrhages, 180margins, 179normal, 179–180pale disc, 180–181swelling, 181–183vessel entry, 179
pupil abnormalities, 185–186constricted pupil, 186dilated pupil, 186
visual field defects, 184–185Nevus, 42Noninfectious retinopathy, 177Nonpigmented lesions, 126Normal pressure glaucoma, 97
management, 97Nystagmus, congenital, 159–160
albinism, 160motor congenital nystagmus,
159sensory congenital nystagmus,
159spasmus nutans, 160
OOccupational standards of vision,
204Ocular muscle imbalance, 119
Onchocerciasis, 175–176extraocular features, 176management, 176ocular features, 176
Opaque media, 113Open angle glaucoma, 196–197Ophthalmia neonatorum, 162Ophthalmoscope use, 22–24Opportunistic infections, 177Opthalmoscopy, 85–86Optic atrophy, 162Optic disc, 179–183
atrophy, optic, 180–181causes of, 181following disease in optic
nerve, 181following papilledema, 181glaucoma, 181inherited, 181toxic, 181trauma, 181vascular causes, 181
central cup, 180color, 179congenital disc anomalies, 180hemorrhages, 180margins, 179normal, 179–180pale disc, 180–181swelling, 181–183
optic neuritis, 182postoperative, 182true papilledema, 182vascular, 181–182
vessel entry, 179Optic nerve, 10–11
axons of ganglion cells visual,11
contusion, 131cortical connections, 11papillary reflex pathways, 11retina, 11subcortical centers, relays, 11visual pathways, 11
Orbital cellulitis, 41Orbital injuries, 133Orbital tumors, 127–128
cavernous hemangioma, 127dermoid cyst, 127glioma of optic nerve, 127lacrimal gland tumor, 127metastatic tumors, 127pseudotumor, 127
214 Index
rhabdomyosarcoma, 127sac tumor, 127
Outer layer of eye, 8–9basement membrane,
epithelium, 8Bowman’s layer, 8cornea layers, 8Descemet’s membrane, 8endothelium, 8epithelium, and its basement
membrane, 8stroma, 8
PPain, referred, 74–75Painful eye
failing vision, 63–65normal vision, 63
scleritis, 63Papilledema, 182Papilloma, 41–42, 123Parasympathetic antagonists, 196Pars planitis, 144Perforation, 131–133
intraocular foreign body, 132sympathetic ophthalmia,
132–133Phakomatoses, 163Photopsiae, 106Physiology of eye, 7–16
accommodation, 14aqueous humor, 13–14ciliary body, 14
circular fibers, 14longitudinal fibers, 14
cornea, 13eyelids, 13lens, 14retina, 14–15
neuroretina, 14RPE, 14–15
tear film, 13vitreous body, 14
Pingueculum, 50, 126Polycythemia, 50, 63, 73Post-traumatic headache, 75Posterior uveitis, 144–147
causes, 145presumed ocular
histoplasmosis, 147sarcoidosis, 146–147signs, 145symptoms, 144–145

syphilis, 147toxocariasis, 146toxoplasmosis, 145–146tuberculosis, 146
Postherpetic neuralgia, 73Presbyopia, 14, 29, 74, 81, 84, 138,
150Primary open angle glaucoma,
92–96pathogenesis, 93signs, 93–94symptoms, 93treatment, 95–96
Proliferative retinopathy, 168Proptosis, 127–128
assessment of, 128causes of, 128hemangioma, 128infection, 128lymphoproliferative disease,
128mucocele of sinuses, 128pseudoproptosis, 128pseudotumor, 128thyrotoxicosis, 128trauma, 128
Pseudoproptosis, 128Pseudotumor, 127–128Ptosis, 39, 159
causes, 39Pupil abnormalities, 185–186
constricted pupil, 186dilated pupil, 186
Pupil evaluation, 20
RRadiation, 83–84Radiational injuries, 134Red eye, 61–66
conjunctivitis, 61–63acute conjunctivitis, 62chronic conjunctivitis, 62–63
episcleritis, 63failing vision, 67–69
fundus abnormal, 68fundus normal, 67–68treatable causes of, 69–70untreatable causes of, 70
painful, failing vision, 63–65acute glaucoma, 63–64acute iritis, 64acute keratitis, 64neovascular glaucoma, 64–65
painful eye, normal vision, 63scleritis, 63
painless, normal vision, 61–63subconjunctival hemorrhage,
61Redundant lid skin, 39Refraction abnormalities, 161Retina, 14–15
contusion, 131neuroretina, 14
Retinal detachment, 103–110exudative retinal detachment,
104, 107flashes, 106floaters, 106incidence, 103management, 107–110pathogenesis, 103–104
classification, 104prognosis, 109–110prophylaxis, 107–108retinal surgery, 108–109
cryobuckle, 109vitrectomy, 109
rhegmatogenous retinaldetachment, 104–106
breaks in retinal detachment,104–105
mechanism of, 105–106posterior vitreous
detachment, 105retinal breaks formation, 105retinal degeneration, 105with trauma, 106vitreous, 105
shadow, 106–107signs and symptoms, 106–107tractional retinal detachment,
104, 107Retinal vascular occlusion, 173Retinoblastoma, 122Retinopathy of prematurity,
161–162Rhabdomyosarcoma, 127Rhegmatogenous retinal
detachment, 104–106breaks in retinal detachment,
104–105mechanism of, 105–106posterior vitreous detachment,
105retinal breaks formation, 105retinal degeneration, 105
Index 215
with trauma, 106vitreous, 105
Rubella, 84, 102, 160Rubeosis iridis, 100, 166, 170
SSarcoidosis, 146–147Schirmer’s test, 36–37Schlemm’s canal, 91, 93Sebaceous gland carcinoma, 125Seborrhoeic keratosis, 123Secondary conjunctivitis, 50–51Secondary glaucoma, 100–101
to abnormalities in lens, 101drug-induced glaucoma, 101to trauma, 101to tumors, 100–101to uveitis, 100to vascular disease in eye, 100
central retinal veinthrombosis, 100
diabetes, 100Senile keratosis, 123Sensory congenital nystagmus,
159Sex-linked recessive inheritance,
192–193Shadow, 106–107Short sight, 29–32Sickle-cell disease, 175Slit-lamp examination, 36, 86Spectacles. See GlassesSpring catarrh, 49–50Squamous cell carcinoma, 43, 125Squint, 111–120, 161
in adults, 116–118amblyopia of disuse, 113causes of, 113, 117in childhood, 112–116diagnosis, 114, 117–118examination, 114–115extraocular muscle anatomy,
116–117horizontal recti, 116obliques, 116–117vertical recti, 116
facial skeleton abnormalities,114
fusion, 111glasses, 115Hess screen, 118history, 114Maddox rod, 118
Squint (cont.)Maddox wing, 117–118management, 115–116muscle weakness, 113–114ocular muscle imbalance, 119opaque media, 113optic nerve disease, 113orthoptic follow-up, 115–116refractive error, 113retinal disease, 113simultaneous macular
perception, 111stereopsis, 111surgery, 116synoptophore, 111treatment, 118types of, 112
Stereopsis, 111Strawberry nevus, 124Stroke, 154–155Stroma, 8Structure of eye, 7–13
blood supply, 10extraocular muscles, 12eyelids, 11–12globe, 7–8
blood, 8coats of, outer fibrous layer,
7compartments of, 7inner nervous layer, 7intraocular fluids, 7middle vascular layer, 7posterior chamber, 7posterior segment, 8segments, 8vitreous chamber, 7vitreous humor, 7–8
inner layer, 9lacrimal apparatus, 12–13middle layer, 9optic nerve, 10–11
axons of ganglion cellsvisual, 11
cortical connections, 11subcortical centers, relays, 11visual pathways, 11
outer layer of eye, 8–9Bowman’s layer, 8cornea layers, 8Descemet’s membrane, 8endothelium, 8stroma, 8
Stycar test, 18–19, 138, 157Styes, 40–41Subconjunctival hemorrhage, 45Subcortical centers, relays, 11Supporting structures of eye,
7–13Sympathetic agonist, 196Sympathetic ophthalmia, 132–133,
143–144Synoptophore, 111Syphilis, 147Systemic disease, 165–178
acquired immune deficiencysyndrome, 176–178
neoplasms, 177neuro-ophthalmological
signs, 177–178noninfectious retinopathy,
177ophthalmological signs,
177–178opportunistic infections, 177
anemia, 174diabetes, 165–170
anterior chamber, 166background retinopathy,
167conjunctiva, 165–166control of, 169cornea, 165–166diabetic maculopathy,
168–169eyelids, 165glaucoma surgery, 170iris, 166laser photocoagulation,
169–170lens, 166ocular movements, 165preproliferative stage,
167–168prognosis, 170proliferative retinopathy,
168retina, 167treatment, 169vitreo-retinal surgery, 170vitreous, 167
hypertension, 172–174age, effect on retinal blood
vessels, 172blood pressure, effect on
retinal vessels, 172–173
216 Index
malignant hypertension, 173vascular changes associated
with, 173–174leukemias, 174–175onchocerciasis, 175–176
extraocular features, 176management, 176ocular features, 176
sickle-cell disease, 175thyroid eye disease, 170–172
chemosis, 171exposure keratitis, 171extraocular muscle action
limitation, 172lid lag, 171lid retraction, 171lid swelling, 171management, 172optic nerve compression,
172proptosis, 171
Systemically-administered drug,damage to eyes by, 199
TTear drainage, 33–36
acute dacryocystitis, 35–36lacrimal passageway, 33–35
Tear film, 13break-up time, 37
Tear secretion, 36Telangiectatic hemangioma,
124Temporal arteritis, 154Testing visual acuity, 137–140
glasses, measuring for, 139–140automated refraction,
139–140objective refraction, 139subjective refraction, 139
Tests of visual acuity, 25–26Thyroid eye disease, 170–172
exposure keratitis, 171lid lag, 171lid retraction, 171lid swelling, 171
Thyrotoxicosis, 128Toxicity, 84Toxocariasis, 146Toxoplasmosis, 145–146Trachoma, 48Tractional retinal detachment,
104, 107
Trauma, ocular, 129–134chemical injuries, 134eyelid injury, 133globe injuries, 129–133
contusion, 129–131perforation, 131–133
orbital injuries, 133radiational injuries, 134
Traumatic cataract, 87–88Trichiasis, 39–40Tuberculosis, 146Tumors of eye, adnexae, 121–128
UUveitis, 162
intermediate, 144
VVernal conjunctivitis, 49–50Vertical recti, 116Visual acuity, 17–19Visual field, 19Visual field defects, 184–185Vitrectomy, 109Vitreo-retinal surgery, 170
Index 217
Vitreous, contusion, 131Vitreous body, 14
WWatering eye, 33–36
tear drainage, 33–36acute dacryocystitis, 35–36lacrimal passageway, 33–35
tear secretion, 36
XXanthelasma, 43, 123