Embed Size (px)
Citation preview

Complications Following Antireflux Surgery:
Recognition and Management
George Ferzli, MD, FACS

Anti-reflux surgery
• 1945 to present–Multiple methods and techniques:
• Nissen fundoplication• Dor wrap• Hill gastropexy ….
–Different approaches:• Laparotomy vs laparoscopy• Thoracotomy vs thoracoscopy
Rudolph Nissen, MD
INFLUENTIAL PEOPLE:
Lortat-Jacob, MD
AndreToupet, MD
Jacques Dor, MD
Ernst Heller, MD
Rudolph Nissen MD
Ivor Lewis, MD
J. Leigh Collis, MD
K. Alvin Merendino, MD
Lucius Hill, MD
Ronald Belsey, MD
Alan Thal, MD

Intra-operative complications
Pleura / lung breech during hiatal dissection

Intra-operative complications• Hemorrhage
– Short gastric vessels– Spleen– Liver retraction– Left inferior phrenic vein– Aberrant left hepatic vein– IVC– Cardiac tamponade from right ventricular
trauma (please remember that metal tacks could cause hemmoragic tamponade )

Post-operative complications
MEDICAL– Infectious– Pulmonary– Urinary infection– Arrhythmia
SURGICAL– Inadvertent vagus division – Leakage from GI tract – Subdiaphragamatic abscess
– Splenic upper pole devascularization
– Failed fundoplication repair
– Fistulas

Fistulas
• Gastro-bronchial fistulas– Intra-thoracic “slipped” wrap– 2° to gastric ulceration– Perigastric abscess– Erosion into bronchus
• Gastro-aortic fistulas
• Gastro-pericardial fistulas

Fistulas• Presentation
– Lower lobe abscess– Gastric contents
expectoration– Cough on lying down
• Diagnosis– UGI Series– Methylene blue staining– Measurement of bronchial
secretion pH
• Management– Control sepsis– Drainage– Division of fistula with or w/o
resection of affected organ– Delayed re-fashioning of diaphragm
and fundoplication

Failed anti-reflux surgery
Failure rate– Open fundoplication: 9% to 30%– Laparoscopic: 2% to 17%
When faced with failure:– Evaluate symptoms– Extensive workup

Failed antireflux symptoms
• Dysphagia• Regurgitation• Heartburn• Chest pain• Pulmonary symptoms• Nausea / vomiting• Abdominal bloating
• Make sure to obtain and review the old operative report

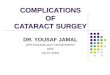
Pre-operative work-up• Esophagram
– Evaluate proximal and distal esophagus
– Estimate the size of the hiatal hernia
– May help diagnose a shortened esophagus (<5cm)
1. Iqbal et al. Reoperation for Failed Anti-Reflux Surgery. Ann Surg 2006; 244: 42-51.2. Furnée et al. Surgical Reintervention after Antireflux Surgery for Gastroesophageal Reflux
Disease: A prospective cohort study in 130 patients. Arch Surg 2008;143(3): 267-274.
GE junction
Confluence of diaphragm
Top of mediastinal gastric tissue
Not exceed 5cm for laparoscopy
Not exceed 2cm for
laparoscopy

Pre-operative work-up• EGD
– Determines presence or absence of cancer
– Direct inspection and biopsy….. BARRETT’S
– Peptic strictures, ulcers
– Size of hiatus
– Presence of food in stomach
– Location and tightness of fundoplication (dilator)
– Length of gastric tissue above fundoplication
– Presence of disrupted fundoplication
1. Iqbal et al. Reoperation for Failed Anti-Reflux Surgery. Ann Surg 2006; 244: 42-51.2. Furnée et al. Surgical Reintervention after Antireflux Surgery for Gastroesophageal Reflux
Disease: A prospective cohort study in 130 patients. Arch Surg 2008;143(3): 267-274.

Pre-operative work-up• Manometry
– Assessment of esophageal relaxation– Esophageal body dysmotility and wave amplitude– May help assessing fundoplication pressure– LES function and positioning
• pH Monitoring– If esophagitis on EGD
• Gastric emptying studies– If previous vagotomy– Old food regurgitation– Food within stomach at EGD after fasting
1. Iqbal et al. Reoperation for Failed Anti-Reflux Surgery. Ann Surg 2006;244: 42-51.2. Furnée et al. Surgical Reintervention after Antireflux Surgery for Gastroesophageal Reflux
Disease: A prospective cohort study in 130 patients. Arch Surg 2008;143(3): 267-274.

Predictability of mechanism of failure
Mechanism of failure % of pre-operative predictabilityCrus closure failure 96
Hiatal stenosis 20
Partial fundoplication disruption 86
Complete fundoplication disruption 86
Hypertensive fundoplication 92
Slipped fundoplication 89
Loose fundoplication 50
Short esophagus 37
Gastroparesis 100
Iqbal et al. 104 failed anti-reflux procedures
Iqbal et al. Reoperation for Failed Anti-Reflux Surgery. Ann Surg 2006; 244: 42-51.

Additional causes of failure
Wrong 1° Dx– Achalasia– Dysmotility– Carcinoma– Gastroparesis – Inadvertent vagotomy– Funnel stomach

Operative approach
• Open thoracotomy– Recommended when > 2 cm of
gastric tissue within thoracic cavity on esophagram
– Short esophagus suspected
• Laparotomy– Multiple previous failed
operations
• Laparoscopy– Patient did not meet above
criteriaIqbal et al. Reoperation for failed anti-reflux surgery. Ann Surg 2006;244: 42-51.
Not exceed 2cm for laparoscopy

Re-operative managementFundoplication inefficacy
– Too tight or too loose– Twisted wrap– Telescoping– Complete or partial disruption
Management: 1. Dismantling the fundoplication
a. Mobilization and division of short gastrics
2. Redo fundoplicationa. Toupet if wrap is too tightb. Dor if no esophageal peristalsis
Tuomo et al. Complications in Antireflux Surgery: National-Based Analysis of Laparoscopic and Open Fundoplications. Arch Surg 2008;143: 359-365.

Re-operative management
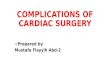
• Crus closure failure– Interrupted non-absorbable sutures– Mesh reinforcement
• Granderath et al– 24 patients with failed antireflux surgery– Circular hiatal mesh @ re-operation– 6% recurrence rate after 5 years– Improved functional parameters
• DeMeester scores• LES pressure
– Improved quality of life
Granderath et al. Laparoscopic Revisional Fundoplication with Circular Hiatal Mesh Prosthesis: The Long-Term Results. World J Surg 2008; 32: 999-1007.

Polypropylene mesh
Esophagus
• Do not use metal tacks
• Biologic mesh? dual mesh?
• No mesh at all? (remember original Toupet repair)
Mesh
Wrap
Circular mesh
Fundoplication

• Esophageal shortening– Skeletonized GEJ not easily reduced– At least 2 cm into peritoneal cavity in open
surgery and at least 3 cm for laparoscopy
• Management– Collis at least 4-5cm long (gastroplasty tube
from stomach)– Merendino (interposition of 15 cm small
bowel segment of jejunum between esophagus and stomach)
• Disadvantage– Neo-esophagus secretes acid– May lead to recurrent reflux or PUD
Re-operative management
Collis
4cm

Re-operative management• Wrong 1° diagnosis
– AchalasiaManagement: Heller myotomy
– Barrett’s/carcinomaManagement: Esophagectomy
– GastroparesisManagement: Pyloroplasty
– Esophageal dysmotilityManagement: Dor, or Toupet
Khajanchee et al. Laparoscopic Reintervention for Failed Antireflux Surgery. Arch Surg 2007;142(8): 785-792

Pitfalls• Collis gastroplasty should be done on 48 French
• Intraoperative perforations must be closed with sutures incorporating mucosa
• Must have intraoperative EGD during surgery
• Must use 60 bougie, it will allow a good asessment of the mobility of the fundic wrap and secure an adequate fundoplication
• Must ligate and divide short gastric vessels
• Do not hesitate to convert from laparoscopy to open

Complications and results after re-operation• Re-operation failure rate = 20% to 30%
• Inadequate crus closure
• Fundoplication disruption
• Influencing factors:– Collagen deficiency?– Hidden role of the patient
• Uncontrolled vomiting• Retching• Lifting
• Results after re-do surgery are worse than after 1° surgery1. Furnée et al. Surgical Reintervention after Antireflux Surgery for Gastroesophageal Reflux
Disease: A prospective cohort study in 130 patients. Arch Surg 2008;143(3): 267-274.2. Furnée EJB et al. Surgical Reintervention After Failed Antireflux Surgery: A Systematic
Review of the Literature. J Gastrointest Surg 2009. Published online ahead of print

Summary• Re-operative antireflux surgery
is feasible, difficult, but effective.
• Surgical approach should be tailored to suspected mechanism of failure using extensive pre-operative workup.
• Adequate mobilization and fundoplication dismantling are of utmost importance.
• Surgeon’s experience plays critical role in choice of re-operative approach.


Anti-reflux Surgery
RECOGNITIONAND
MANAGEMENTOF
COMPLICATIONS

Anti-reflux Surgery
• Multiple unanswered questions:– Role of laparoscopy
• As initial intervention• Redo
– Need for esophageal lengthening– Efficacy of partial fundoplication– Endoluminal therapy

Intra-operative complications
• Pulmonary– Pneumothorax / Pneumomediastinum
• Breach of pleura during hiatal dissection• Relieved by tube thoracostomy
– Pneumoperitoneum• CO2 rapidly dissipates after release
– Positive pressure ventilation– Absorption

Indications for Re-operation• Surgically correctable disorder
• Not amenable to medical management
• Furnée et al: Review of multiple studies – Pre-operative symptoms assessed by questionnaire– Work-up:
• EGD• Barium swallow• pH monitoring
Furnée EJB et al. Surgical Reintervention After Failed Antireflux Surgery: A Systematic Review of the Literature. J Gastrointest Surg 2009. Published online ahead of print

Re-operative management
• Initial laparoscopic approach– Prone to higher recurrence of dysphagia
– 15 patients with severe dysphagia after laparoscopic approach
None had short gastric vessel division during initial surgery!!!
Tuomo et al. Complications in Antireflux Surgery: National-Based Analysis of Laparoscopic and Open Fundoplications. Arch Surg 2008;143: 359-365.