Embed Size (px)
Citation preview

Congenital Cardiac Lesions

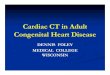
Fetal Circulation
Ductus Venosus
Ductus Arteriosus
Foramen Ovale

Three Shunts of Fetal Circulation
• Ductus Arteriosus– Protects lungs against circulatory overload– Allows RV to strengthen– High pulmonary vascular resistance, low
pulmonary blood flow– Carries moderately saturated blood
• Ductus Venosus– Connects umbilical vein to IVC– Flow regulated via sphincter– Conducts highly oxygenated blood
• Foramen Ovale– Shunts highly oxygenated blood from RA to LA

Circulatory Changes at Birth
• Aeration of Lungs at Birth– Increase in pulmonary blood flow-
raising LA pressure to higher than that of the IVC
– Thinning of walls of PA secondary to stretch as lungs increase in size with first few breaths

Changes Associated with First Breath
• Alveoli open• Pressure in R. heart decreases• Pressure in the L. heart increases as
blood returns from highly vascularized pulmonary tissue to the LA

Fate of the shunts• Foramen Ovale:
– Closes at birth due to decreased flow from placenta and IVC
– Pulmonary venous return causes pressure in LA to be higher than that in RA
• Ductus Arteriosus:– Due to decreased pulmonary vascular resistance, PA
pressure falls below systemic pressure and blood flow through DA is diminished
– Closure mediated by bradykinin– Prostaglandin E2 may reopen DA
• Umbilical Vessels– Constrict at birth and are then tied and cut

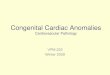
The Normal Heart

Cyanosis in the Newborn• Arterial oxygen saturation less than
90%• Common Causes:
– Intrinsic pulmonary disease– Congenital heart lesions– Central nervous system depression with
hypoventilation

Cyanotic Heart Lesions• The 5 Ts
– Tetralogy of Fallot– Transposition of the Great Arteries– Truncus Arteriosus– Tricuspid Atresia– Total Anomalous Pulmonary Venous
Return

Tetralogy of Fallot• 4 lesions
– Overriding aorta– Right ventricular hypertrophy– Ventricular septal defect– Right ventricular outflow tract
obstruction
• Cyanosis varies with the degree of outflow tract obstruction and size of VSD
• Characterized by hypercyanotic episodes- Tet Spells
• Cyanosis is caused by Right Left shunting through the VSD

• Correction– Early repair, unless
patient is premature or low birth weight
– VSD is closed with patch
– Obstructing RV muscle is removed
– All other outflow tract abnormalities are addressed
Tetralogy of Fallot

Transposition of the Great Arteries
• Most common cyanotic condition that requires hospitalization in first 2 weeks of life
• Aorta arises from RV and carries oxygenated blood to the lungs

Transposition of the Great Arteries
• Survival depends on allowing bloodflow from the 2 outflow tracts to mix.– Prostaglandins augment ductal flow– Inter-atrial septum may be opened with
balloon septostomy– Surgical correction requires removal of
aorta and pulmonary artery from their origins and re-attached to the correct ventricles

Truncus Arteriosus• Single artery arises
from the heart, supplying both aorta and pulmonary artery.
• VSD below the truncal valve allows mixing of right and left ventricular blood
• Degree of cyanosis is variable
• Presents with progressive heart failure

Truncus Arteriosus• Medical Management
– Digoxin and Diuretics• Surgical Repair
– Usually required by 2-3 months of age– VSD is closed– PA trunk is separated from truncus– Conduit created between RV and PA using a
valved graft– May require further procedures if conduit
becomes obstructed, if graft calcifies, or if patient outgrows repair

Tricuspid Atresia• Tricuspid valve fails
to develop, therefore leaving no connection between RA and RV (which is hypoplastic)
• Desaturated blood from RA must cross through PFO to LA and LV

Tricuspid Atresia• Repair allows venous return to flow passively
to the lungs without a pumping chamber.• Pulmonary blood flow is dependent on low
pulmonary vascular resistance and elevated CVP
• Repair not usually performed in neonatal period- but rather over a series of procedures– Systemic to PA shunt– SVC to PA shunt (followed by ligation of first
shunt)– Glenn Shunt– IVC to PA shunt– completion Fontan

Right-Sided Heart Lesions– Other right-sided cardiac abnormalities
that may present with or without cyanosis include:• Pulmonary Valve and Infundibular Stenosis• Pulmonary Regurgitation• Absence of the pulmonary valve• Pulmonary Artery Stenosis• Tricuspid Stenosis• Double-chambered right ventricle• Ebstiens anomaly

Acyanotic Heart Lesions• Acyanotic congenital heart disease: a
group of cardiac diseases with a Left to Right shunt or left heart abnormality
• Acyanotic lesions make up about one third of congenital heart disease.

Acyanotic Congenital Heart Lesions
• Acyanotic heart lesions with left-to-right shunts include:– ASD– VSD– PDA– AV Canal Defects

Atrial Septal Defects• Most commonly occurs in
the ostium secundum- covering the central portion of the inter-atrial septum.
• Generally asymptomatic for the first 3 decades of life.
• Symptoms may include exercise intolerance, dyspnea on exertion, and fatigue cause by right heart failure and pulmonary hypertension
• Stroke can result from paradoxical emboli.

Atrial Septal Defects• The decision to close and ASD is
based on the size of the shunt and the presence or absence of symptoms.
• Closure is indicated in patients who are symptomatic or who have systemic embolization.
• Smaller defects may be closed using trans-catheter techniques, thus avoiding sternotomy and bypass

Ventricular Septal Defect• May be anywhere in
intra-ventricular septum- clinical course depends on the shunt size and involvement of pulmonary vascular bed.
• Approx ½ of all VSDs are small, and more than ½ close spontaneously.– Highest closure rates in
the first decade of life.

Ventricular Septal Defect

Ventricular Septal Defect• Eisenmenger’s complex:
– Left Right shunt causes pulmonary hypertension with resulting reversal of the direction of the shunt.
– Ultimately the resistance in the lungs may exceed the resistance in the arteries of the rest of the body, which leads to a reversal of flow from Left Right to Right Left shunt.
– Reversal of the shunt leads to cyanosis, dyspnea, hemoptysis, reduced exercise tolerance, syncope, palpitations, and atrial fibrillation
– Brain events such paradoxical embolus, thrombosis, and hemorrhage may occur.
– Heart failure suggests a poor prognosis, and sudden death is possible.

Patent Ductus Arteriosus• Ductus Arteriosus
connects the descending aorta to the main pulmonary trunk near the origin of the left subclavian
• Normal postnatal closure results in fibrosis- which becomes the ligamentum arteriosum.
• Small PDA does not increase risk for heart failure- but does carry a risk for bacterial endocarditis.

Patent Ductus Arteriosus• Without ligation- there is an ongoing risk
for bacterial endocarditis, heart failure, and development of Eisenmenger’s complex.
• Ligation of PDA• May be closed surgically or via transcatheter
procedure• Endocarditis prophylaxis is not required after
ligation• Cardiac function generally returns to normal

Acyanotic Heart LesionsAcyanotic heart lesions with left heart
abnormalities include: – Aortic Stenosis– Aortic Regurgitation– Coarctation of the Aorta – Anomalous Right Subclavian or
Innominate arteries– Aortic Atresia– Mitral Atresia, Mitral Stenosis, Mitral
Regurgitation, Mitral Prolapse

Coarctation of the Aorta• Coarctation usually
occurs just distal to the left subclavian artery at the ligamentum arteriosum– May also occur just
proximal to the left subclavian.
• Causes systemic hypertension and secondary LVH with heart failure.

Coarctation of the Aorta

Coarctation of the Aorta• Diagnosis:
– Young adults may be aysmptomatic except for hypertension and decreased lower extremity pulses.
– May be seen on CXR- characterized by the “3 sign”- coarct segment between dilated left subclavian above and convexity of descending aorta below.
• Treatment:– Considered for patients with gradients greater than
30 mm Hg on cardiac cath.– Balloon angioplasty is the treatment of choice

Review• Cyanotic Heart Lesions; Right Left Shunts
and right sided lesions:– tetralogy of Fallot– Transposition of the Great Arteries– Truncus Arteriosus– Tricuspid Atresia– Total Anomalous Pulmonary Venous Return
• Acyanotic Lesions; Left Right Shunts and left sided lesions:– ASD– VSD– PDA– Coarctation of Aorta