Embed Size (px)
Citation preview
CONNECTIVE TISSUE
DISEASESLesley Davila, MD
Assistant Professor, Rheumatic Diseases
December 11, 2014
OUTLINEAutoantibodies
SLE
Systemic sclerosis
Mixed Connective Tissue Disease
ANA – anti nuclear antibody
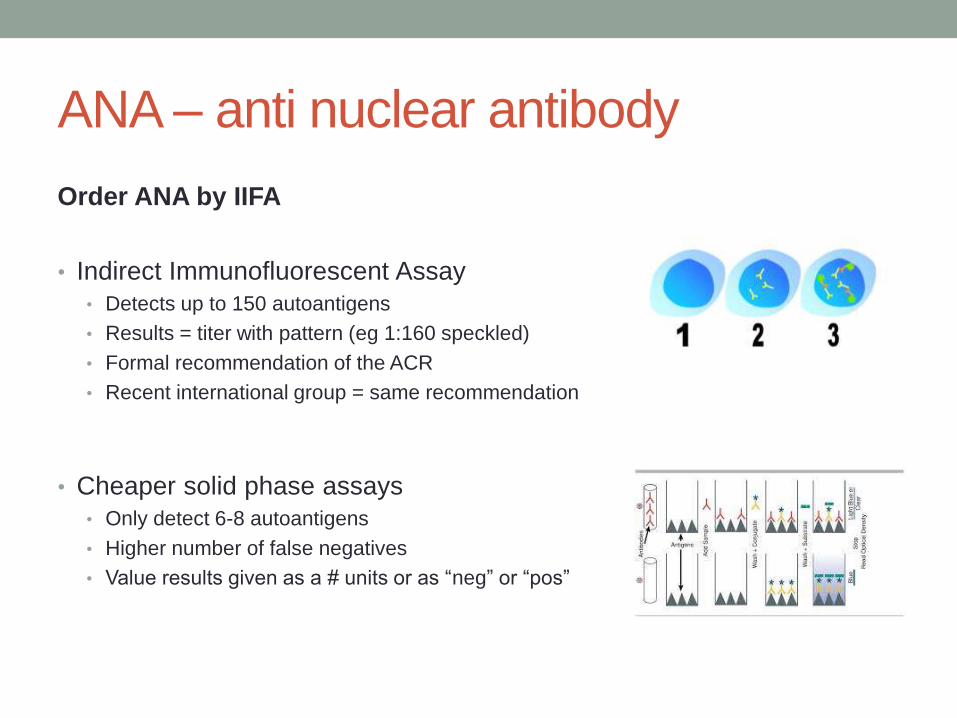
Order ANA by IIFA
• Indirect Immunofluorescent Assay
• Detects up to 150 autoantigens
• Results = titer with pattern (eg 1:160 speckled)
• Formal recommendation of the ACR
• Recent international group = same recommendation
• Cheaper solid phase assays
• Only detect 6-8 autoantigens
• Higher number of false negatives
• Value results given as a # units or as “neg” or “pos”
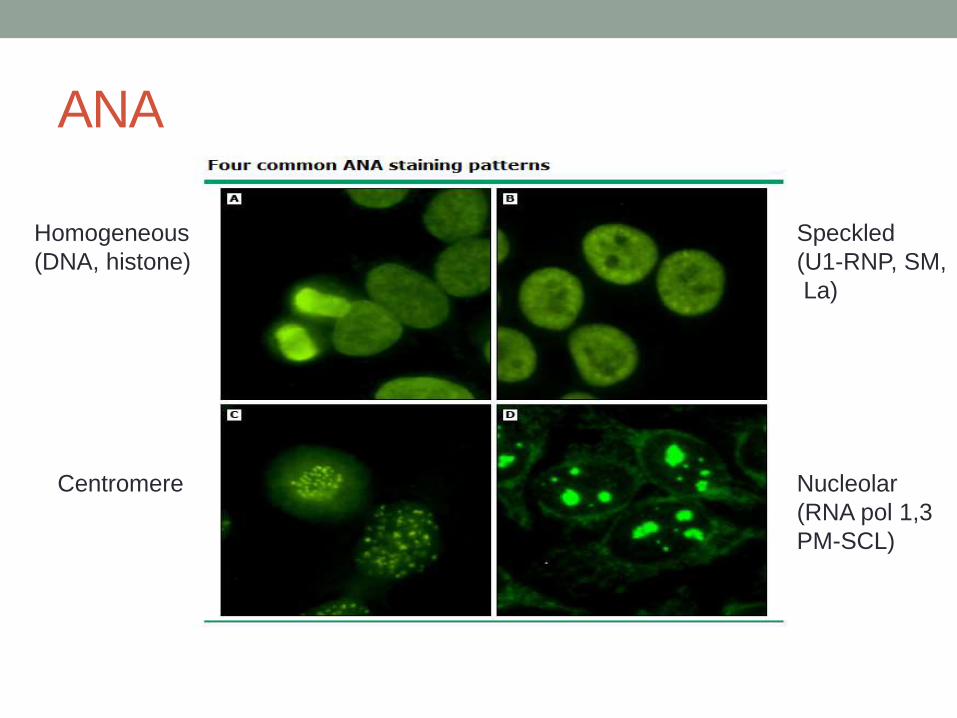
ANA
Homogeneous
(DNA, histone)
Speckled
(U1-RNP, SM,
La)
Centromere Nucleolar
(RNA pol 1,3
PM-SCL)
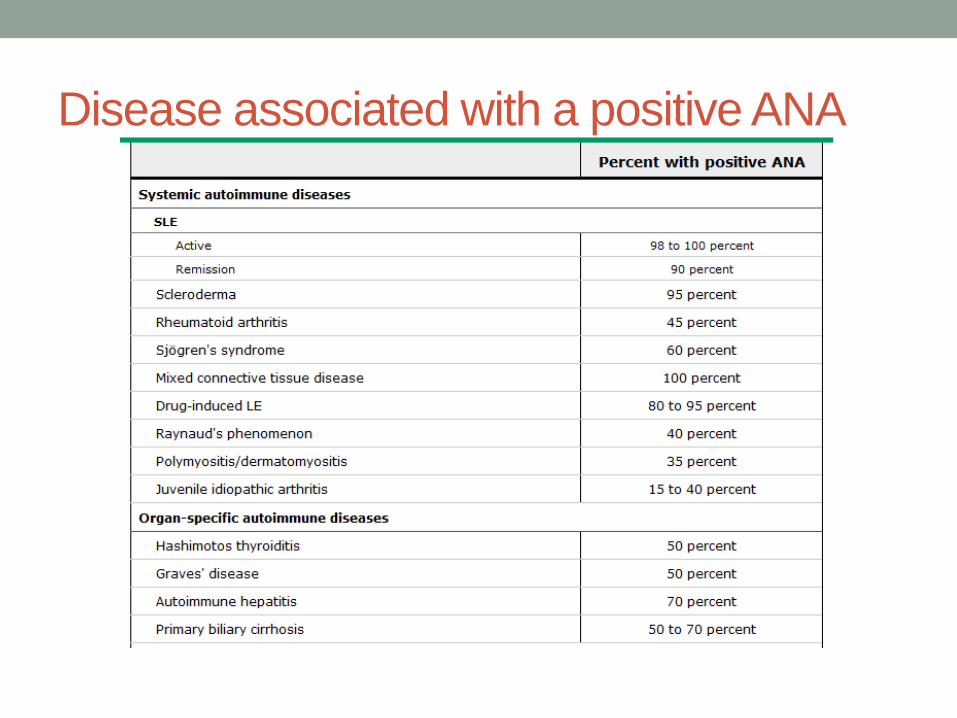
Disease associated with a positive ANA
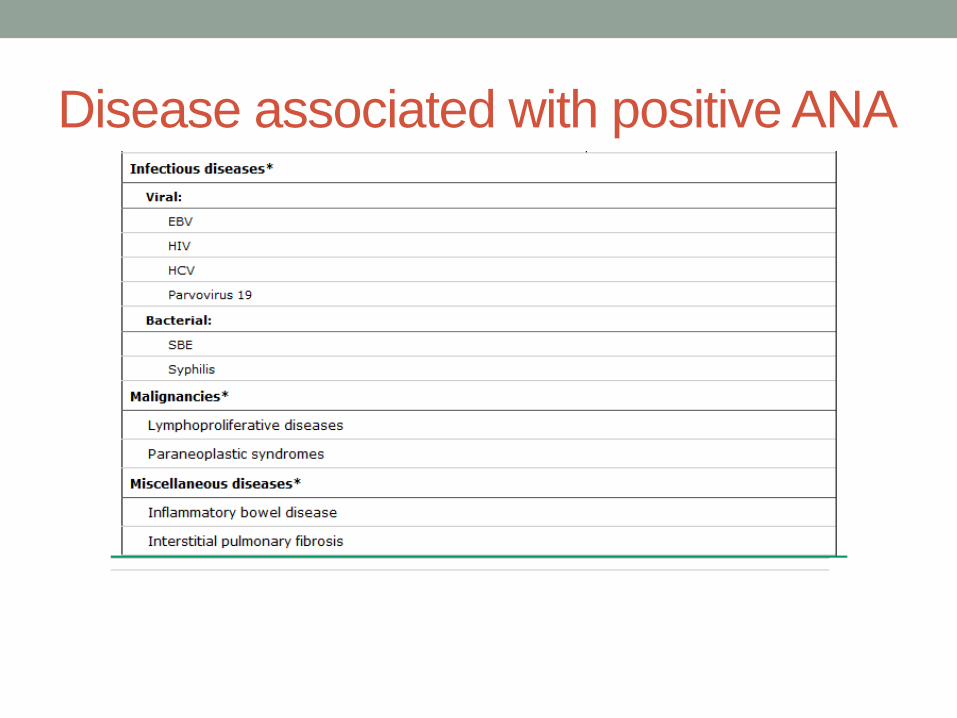
Disease associated with positive ANA
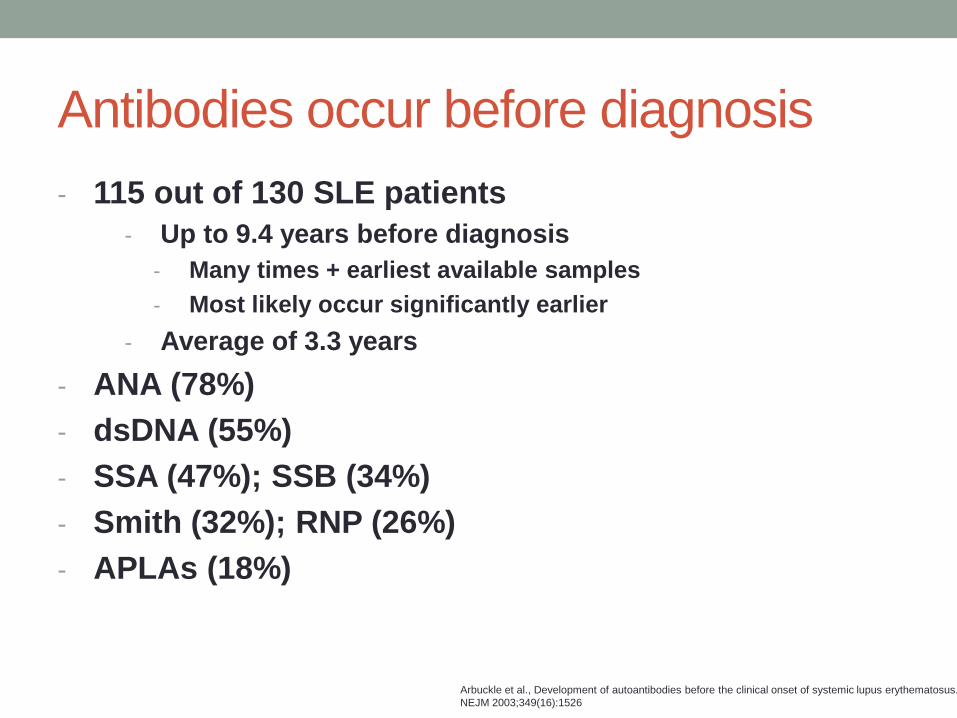
Antibodies occur before diagnosis
- 115 out of 130 SLE patients
- Up to 9.4 years before diagnosis
- Many times + earliest available samples
- Most likely occur significantly earlier
- Average of 3.3 years
- ANA (78%)
- dsDNA (55%)
- SSA (47%); SSB (34%)
- Smith (32%); RNP (26%)
- APLAs (18%)
Arbuckle et al., Development of autoantibodies before the clinical onset of systemic lupus erythematosus.
NEJM 2003;349(16):1526
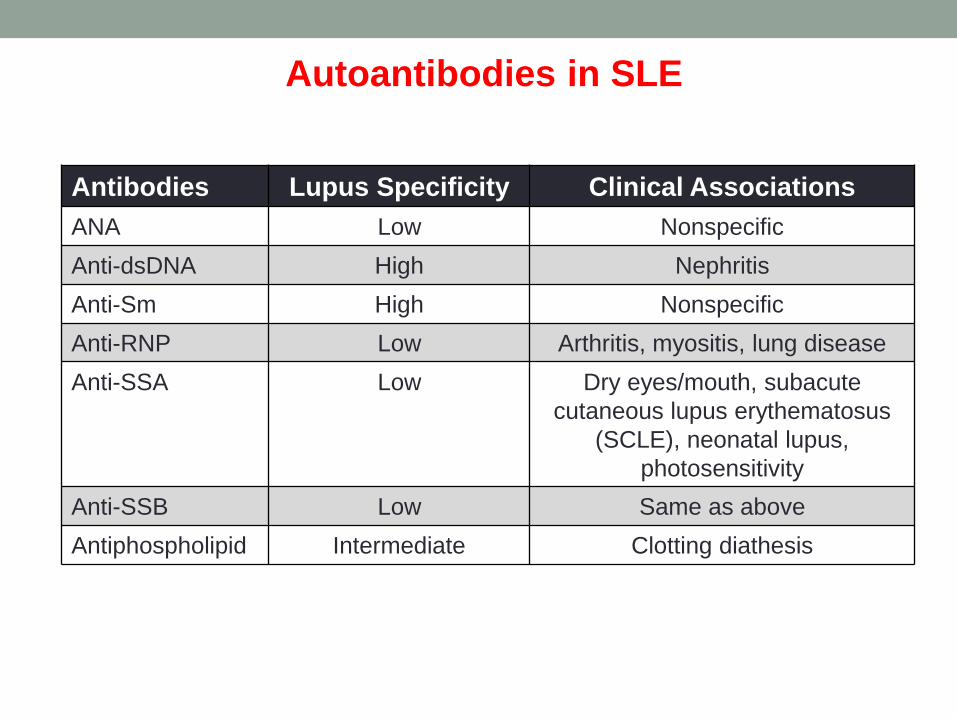
Autoantibodies in SLE
Antibodies Lupus Specificity Clinical Associations
ANA Low Nonspecific
Anti-dsDNA High Nephritis
Anti-Sm High Nonspecific
Anti-RNP Low Arthritis, myositis, lung disease
Anti-SSA Low Dry eyes/mouth, subacute
cutaneous lupus erythematosus
(SCLE), neonatal lupus,
photosensitivity
Anti-SSB Low Same as above
Antiphospholipid Intermediate Clotting diathesis
SYSTEMIC LUPUS
ERYTHEMATOSUSDiagnostic review
Therapeutic considerations
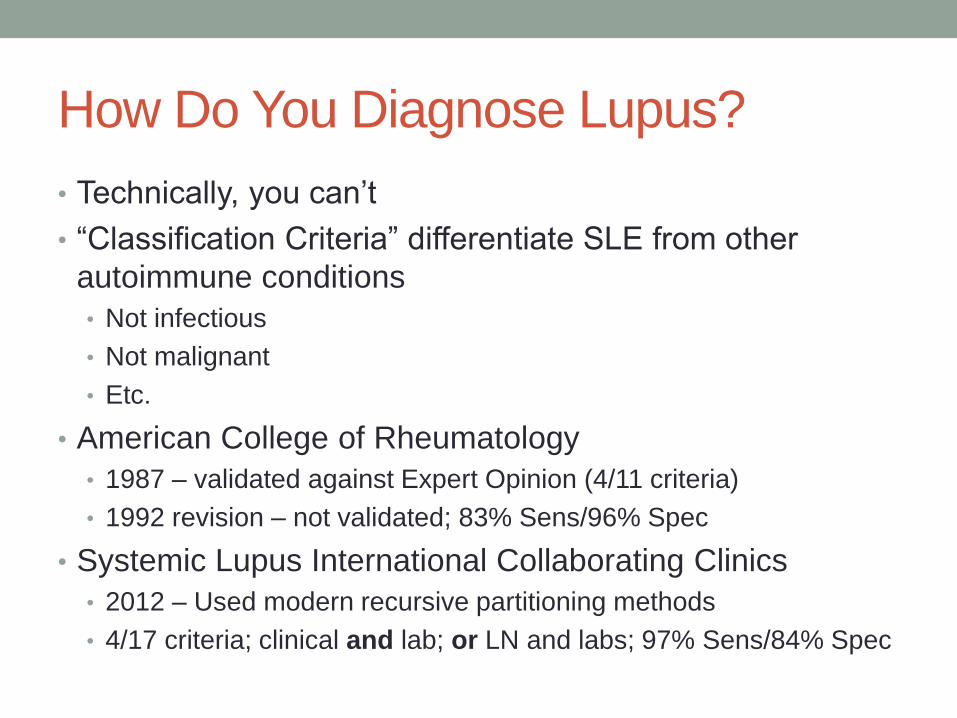
How Do You Diagnose Lupus?
• Technically, you can’t
• “Classification Criteria” differentiate SLE from other
autoimmune conditions
• Not infectious
• Not malignant
• Etc.
• American College of Rheumatology
• 1987 – validated against Expert Opinion (4/11 criteria)
• 1992 revision – not validated; 83% Sens/96% Spec
• Systemic Lupus International Collaborating Clinics
• 2012 – Used modern recursive partitioning methods
• 4/17 criteria; clinical and lab; or LN and labs; 97% Sens/84% Spec
The Best Mnemonics are Remembered
H Hematologic – thrombocytopenia, leukopenia or lymphopenia, AIHA
I Immunologic – anti-Sm, anti-DNA, anti-phospholipid, low complement
M Mucocutaneous – ACLE, SCLE, DLE, and/or oral/nasal ulcers (4 criteria!)
R Renal – proteinuria or red cell casts or LN by biopsy
S Serositis – must be provider documented
A Arthritis – must be provider documented
N Neurologic – Seizures or psychosis
A ANA
Technically, there are ~4,000 combinations of 4 different
items, but lupus commonly presents in a few ways…
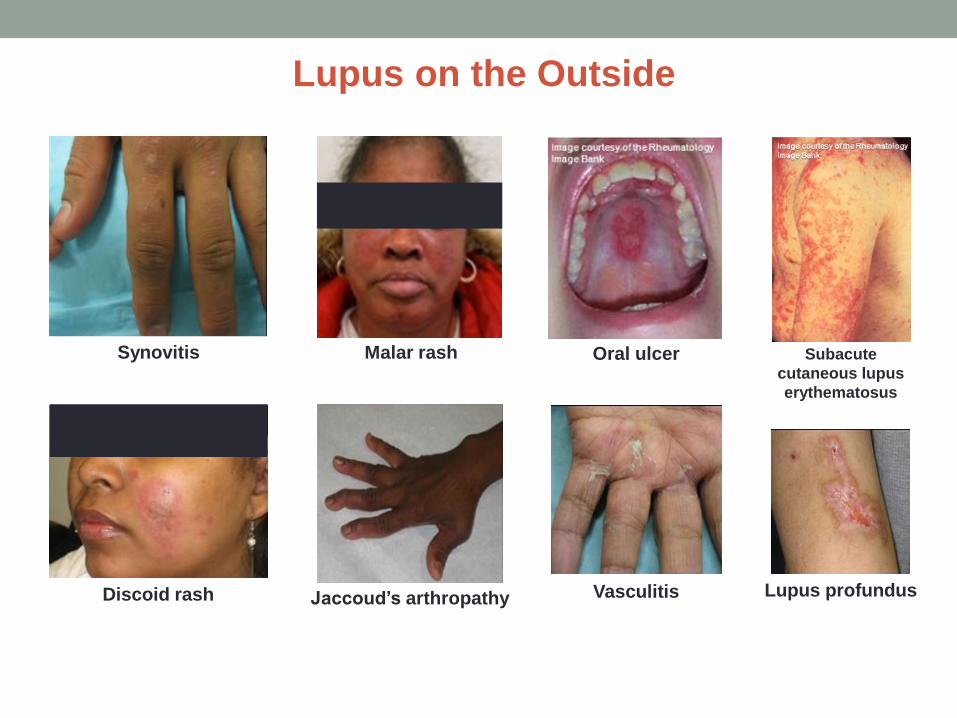
Lupus on the Outside
Malar rash
Synovitis Subacute
cutaneous lupus
erythematosus
Oral ulcer
Discoid rash Lupus profundus
Vasculitis
Jaccoud’s arthropathy
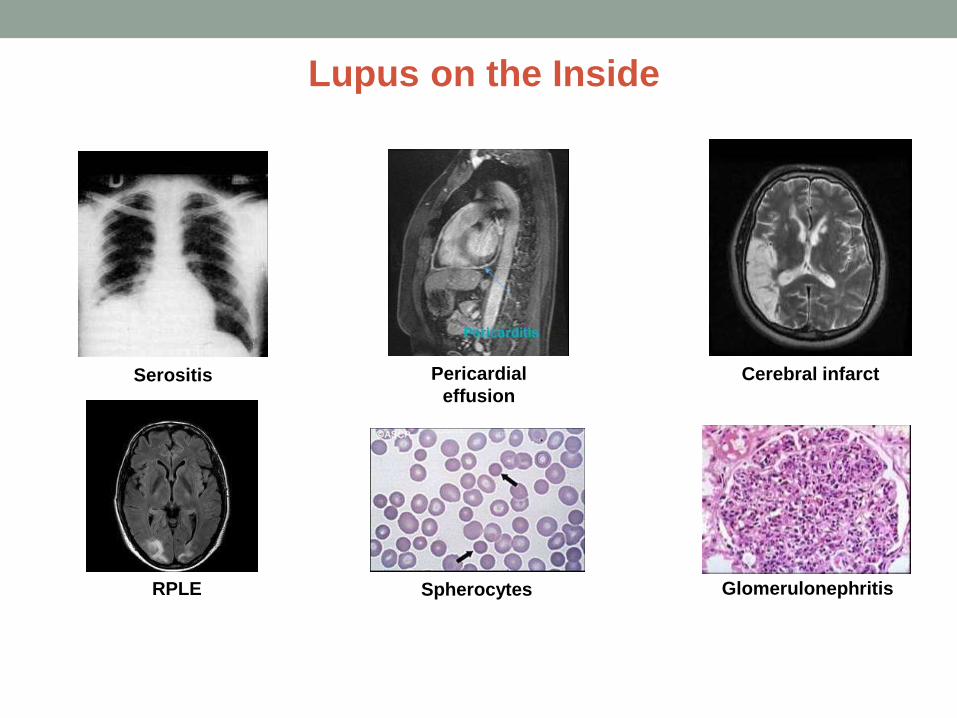
Lupus on the Inside
Serositis Pericardial
effusion
Cerebral infarct
GlomerulonephritisSpherocytesRPLE
C
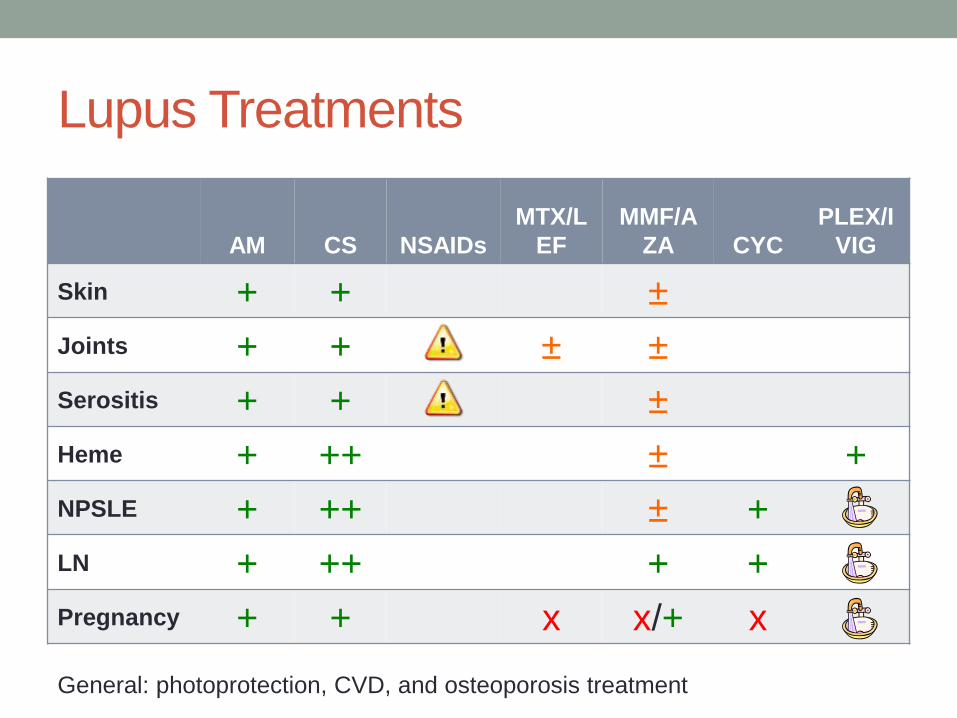
Lupus Treatments
AM CS NSAIDs
MTX/L
EF
MMF/A
ZA CYC
PLEX/I
VIG
Skin + + ±
Joints + + ± ±
Serositis + + ±
Heme + ++ ± +
NPSLE + ++ ± +
LN + ++ + +
Pregnancy + + x x/+ x
General: photoprotection, CVD, and osteoporosis treatment
Toll-like Receptors and SLE
• Toll-Like Receptors (TLRs) sense patterns associated
with pathogenic organisms – LPS, peptidoglycan,
bacterial and viral DNA/RNA
• TLR7 and TLR9 are endosomal – designed to sense
ingested microbial nucleic acids
• IgG-NA complexes are targeted to TLR7/9 leading to B
cell activation and autoantibody production
• Activation of TLR9 leads to anti-DNA in mouse models;
TLR7 to anti-RNA Abs. Genetic deficiency or chemical
inhibition reverse this.
• X-linked TLR7 may explain some of the gender effects in
both mouse and human models
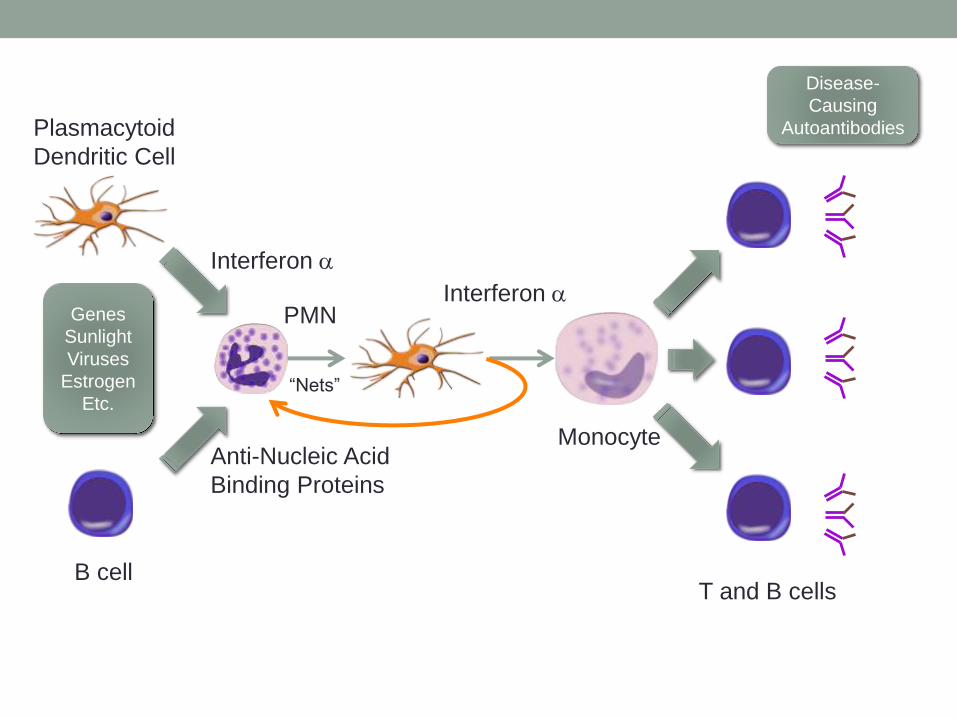
Genes
Sunlight
Viruses
Estrogen
Etc.
B cell
Plasmacytoid
Dendritic Cell
Anti-Nucleic Acid
Binding Proteins
Interferon a
PMN
“Nets”
Interferon a
Monocyte
Disease-
Causing
Autoantibodies
T and B cells
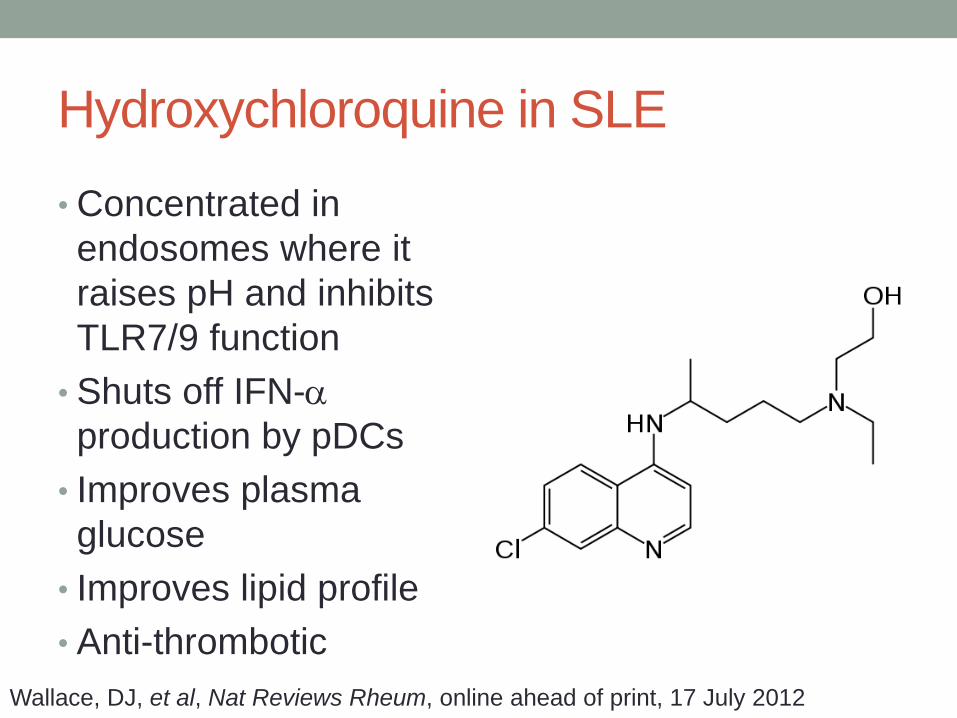
Hydroxychloroquine in SLE
• Concentrated in
endosomes where it
raises pH and inhibits
TLR7/9 function
• Shuts off IFN-a
production by pDCs
• Improves plasma
glucose
• Improves lipid profile
• Anti-thrombotic
Wallace, DJ, et al, Nat Reviews Rheum, online ahead of print, 17 July 2012
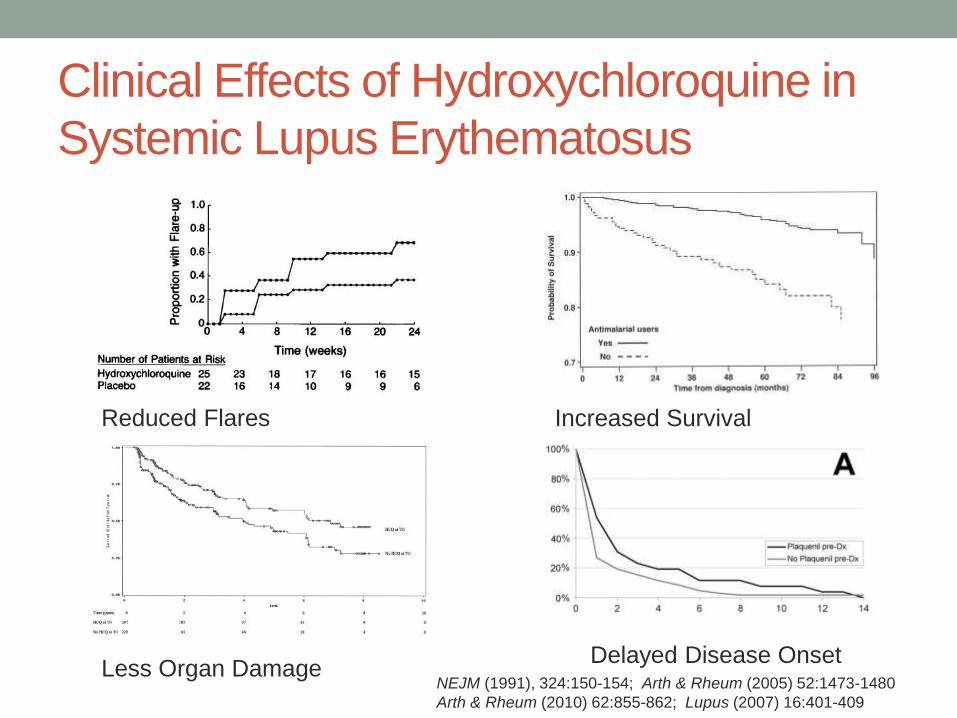
Clinical Effects of Hydroxychloroquine in
Systemic Lupus Erythematosus
Reduced Flares Increased Survival
Less Organ DamageDelayed Disease Onset
NEJM (1991), 324:150-154; Arth & Rheum (2005) 52:1473-1480
Arth & Rheum (2010) 62:855-862; Lupus (2007) 16:401-409
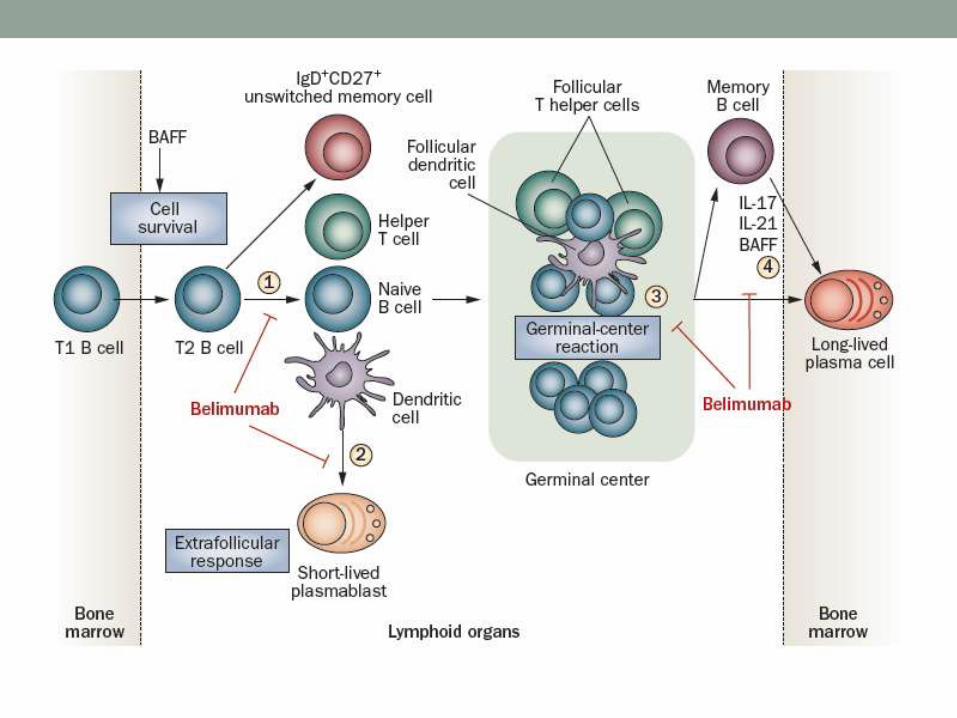
B Cell Cytokines BAFF and APRIL
• BAFF (BLyS) and APRIL are homotrimeric TNF family
members expressed by neutrophils, macrophages,
monocytes and dendritic cells
• Critical roles in B cell development and proliferation
• Overexpression in animal models leads to a lupus-like
illness; blockade prevents it.
• Increased levels of BAFF and APRIL seen in human SLE
and rheumatoid arthritis
BAFF – B cell activating factor; BLyS – B Lymphocyte stimulator; APRIL – a
proliferation inducing ligand; BCMA – B cell maturation antigen; TACI –
transmembrane activator and calcium modulator and cyclophilin ligand
interactor
Mackay and Schneider, Nature Rev Immunol, 9:491-502, 2009
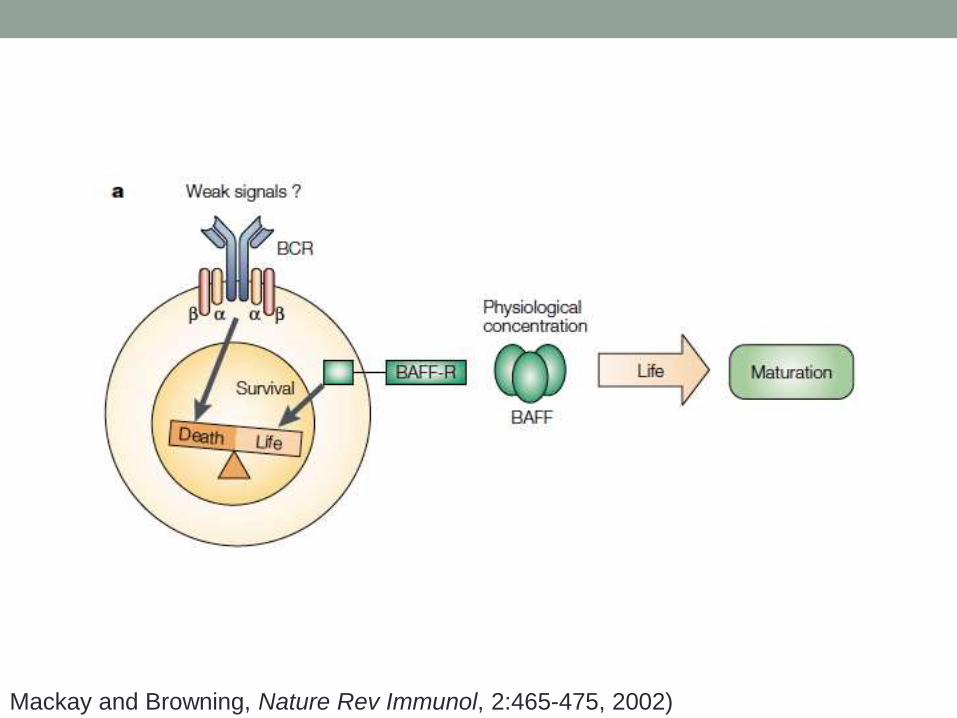
Mackay and Browning, Nature Rev Immunol, 2:465-475, 2002)
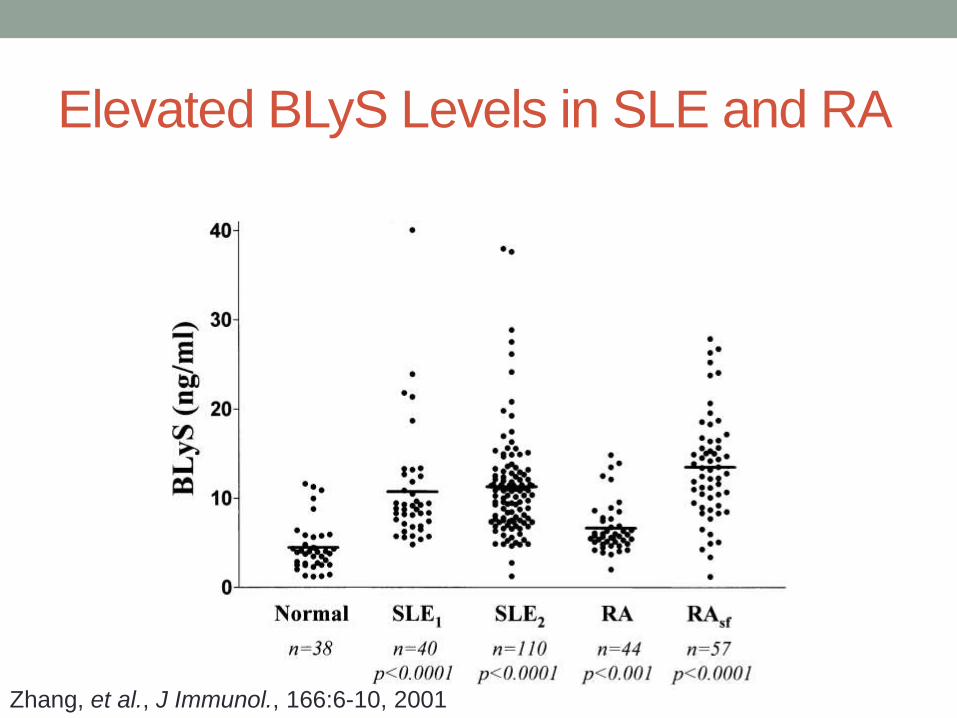
Elevated BLyS Levels in SLE and RA
Zhang, et al., J Immunol., 166:6-10, 2001
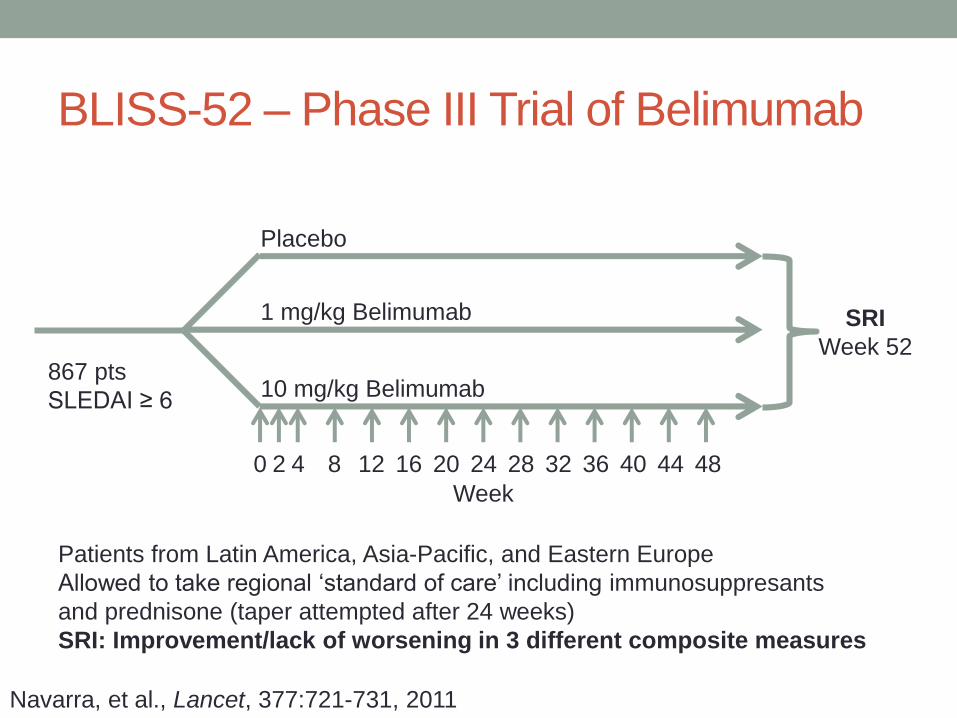
BLISS-52 – Phase III Trial of Belimumab
867 pts
SLEDAI ≥ 6
Placebo
1 mg/kg Belimumab
10 mg/kg Belimumab
0 2 4 8 12 16 20 24 28 32 36 40 44 48
Week
SRI
Week 52
Patients from Latin America, Asia-Pacific, and Eastern Europe
Allowed to take regional ‘standard of care’ including immunosuppresants
and prednisone (taper attempted after 24 weeks)
SRI: Improvement/lack of worsening in 3 different composite measures
Navarra, et al., Lancet, 377:721-731, 2011
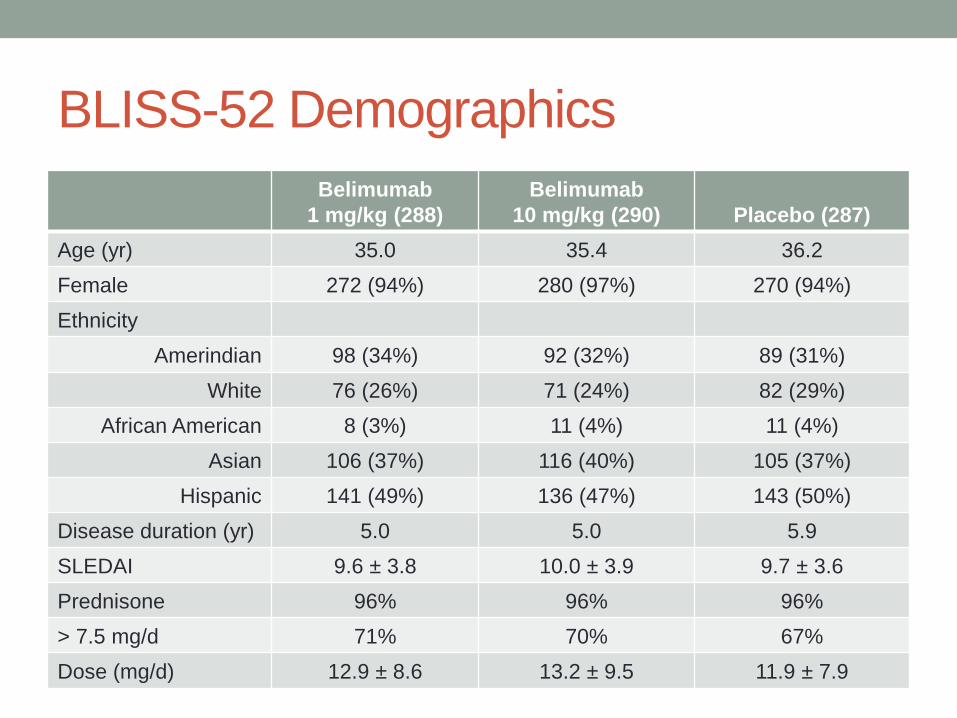
BLISS-52 Demographics
Belimumab
1 mg/kg (288)
Belimumab
10 mg/kg (290) Placebo (287)
Age (yr) 35.0 35.4 36.2
Female 272 (94%) 280 (97%) 270 (94%)
Ethnicity
Amerindian 98 (34%) 92 (32%) 89 (31%)
White 76 (26%) 71 (24%) 82 (29%)
African American 8 (3%) 11 (4%) 11 (4%)
Asian 106 (37%) 116 (40%) 105 (37%)
Hispanic 141 (49%) 136 (47%) 143 (50%)
Disease duration (yr) 5.0 5.0 5.9
SLEDAI 9.6 ± 3.8 10.0 ± 3.9 9.7 ± 3.6
Prednisone 96% 96% 96%
> 7.5 mg/d 71% 70% 67%
Dose (mg/d) 12.9 ± 8.6 13.2 ± 9.5 11.9 ± 7.9
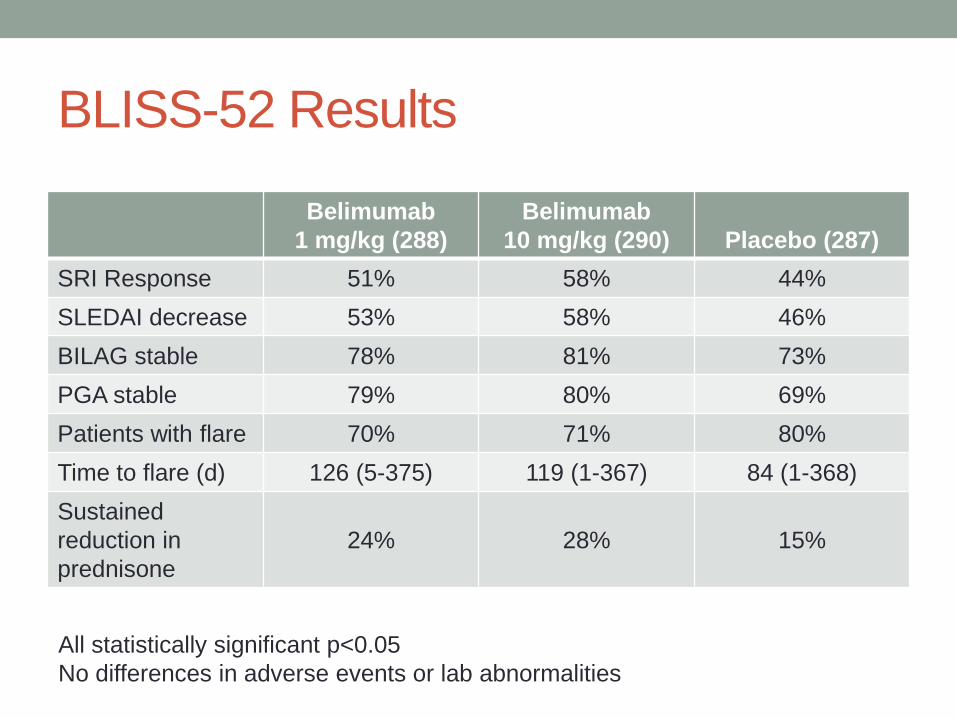
BLISS-52 Results
Belimumab
1 mg/kg (288)
Belimumab
10 mg/kg (290) Placebo (287)
SRI Response 51% 58% 44%
SLEDAI decrease 53% 58% 46%
BILAG stable 78% 81% 73%
PGA stable 79% 80% 69%
Patients with flare 70% 71% 80%
Time to flare (d) 126 (5-375) 119 (1-367) 84 (1-368)
Sustained
reduction in
prednisone
24% 28% 15%
All statistically significant p<0.05
No differences in adverse events or lab abnormalities
BAFF/APRIL as Therapeutic Targets
• Belimumab (Benlysta) approved by FDA in 2011 for active, autoantibody-positive SLE in addition to standard therapy• Trial endpoint not obvious in practice
• In combined analysis, all benefit seen in patients with low C3 and high anti-DNA titers
• Not tested in nephritis or CNS disease
• Expensive ($35,000/yr)
• Atacicept (Merck) – TACI-Ig fusion protein blocks both BAFF and APRIL; trial suspended for safety
• Tabalumab (Lilly) – Anti-BAFF in Phase 2/3
• Blisibimod (Amgen/Anthera) – BAFF inhibitor fusion protein
Lupus Nephritis (LN) is:
• Common
• Affects 60% of adults and 80% of children with systemic lupus
erythematosus
• Severe
• 10-30% progress to ESRD in 15 yr
• Most important predictor of mortality in SLE
• Treatable
• But how should we treat it?
• How well are we doing?
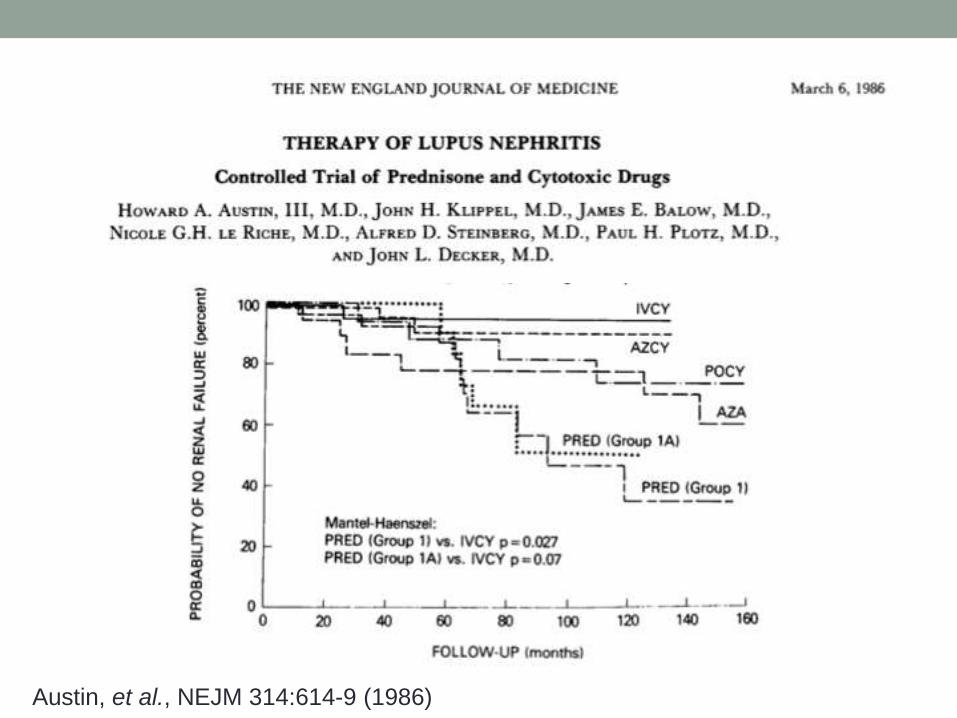
Austin, et al., NEJM 314:614-9 (1986)
Cyclophosphamide – The Drug to Beat in
Lupus Nephritis• Boumpas, et al., Lancet 1992
• “NIH Regimen” of 6 monthly followed by 6 quarterly doses of 0.5-
1.0 g/m2 IV CTX
• Gourley, et al., Ann Intern Med 1996
• IV cyclophosphamide plus IV methylprednisolone achieved 85%
remission compared to 62% for CTX alone and 29% for MP alone
• Houssiau, et al., Arthritis Rheum 2002
• Euro-Lupus Trial: Induction with 500 mg CTX every 2 wk x 6
followed by azathioprine as effective as high-dose CTX with less
toxicity
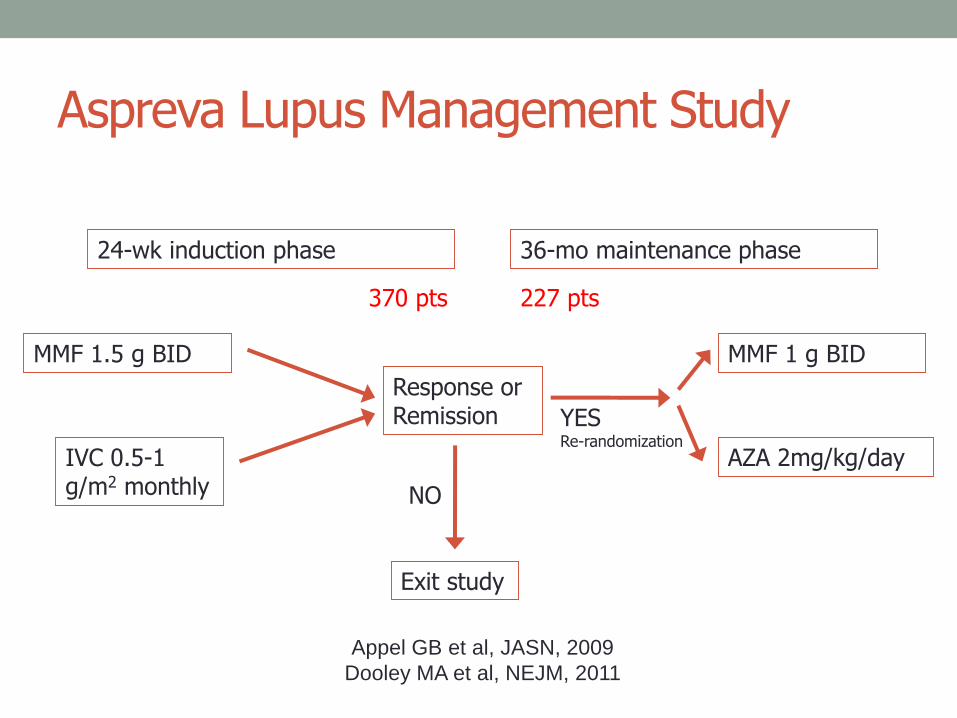
Aspreva Lupus Management Study
Appel GB et al, JASN, 2009
Dooley MA et al, NEJM, 2011
MMF 1.5 g BID
IVC 0.5-1 g/m2 monthly
Response or Remission
MMF 1 g BID
AZA 2mg/kg/day
Exit study
YESRe-randomization
NO
24-wk induction phase 36-mo maintenance phase
370 pts 227 pts
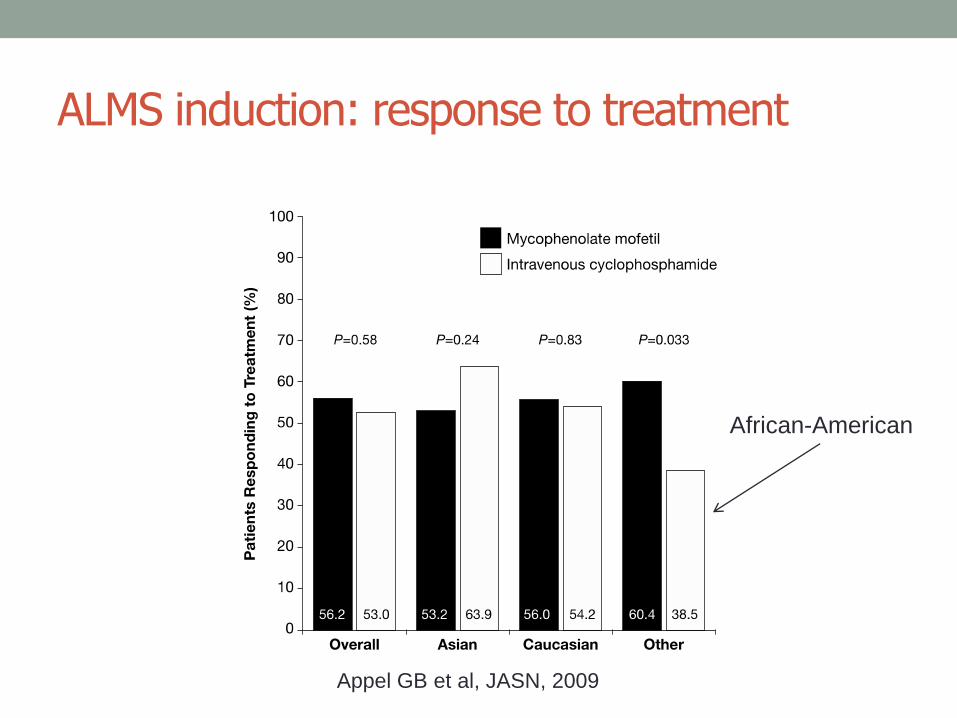
ALMS induction: response to treatment
Appel GB et al, JASN, 2009
African-American
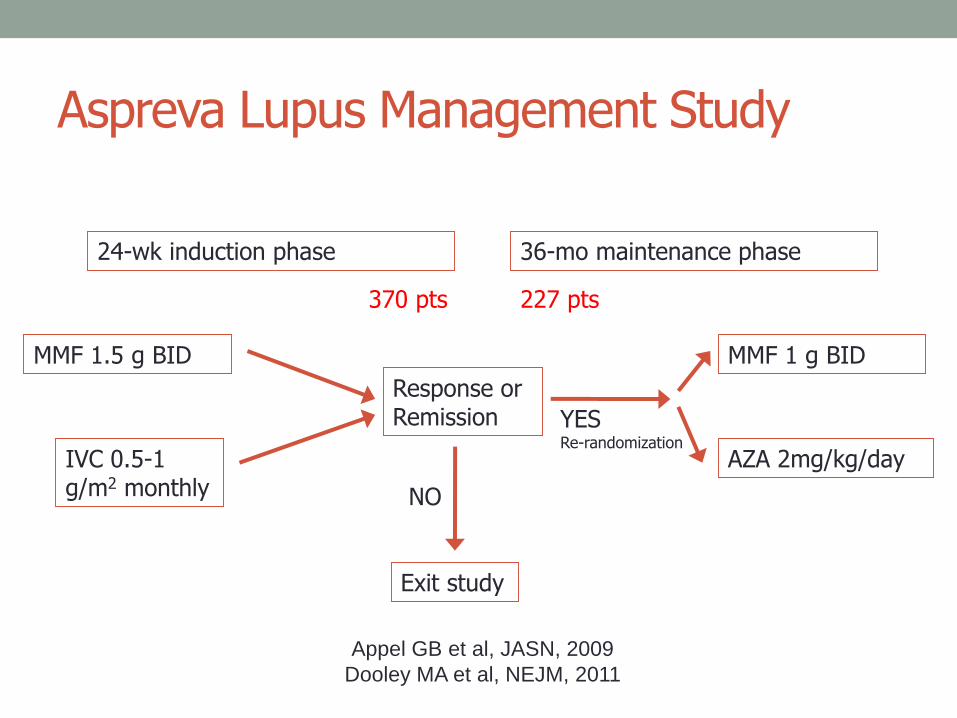
Aspreva Lupus Management Study
Appel GB et al, JASN, 2009
Dooley MA et al, NEJM, 2011
MMF 1.5 g BID
IVC 0.5-1 g/m2 monthly
Response or Remission
MMF 1 g BID
AZA 2mg/kg/day
Exit study
YESRe-randomization
NO
24-wk induction phase 36-mo maintenance phase
370 pts 227 pts
Primary endpoint: time to treatment failure
• Death
• ESRD
• Sustained doubling of serum creatinine
• Need for rescue therapy
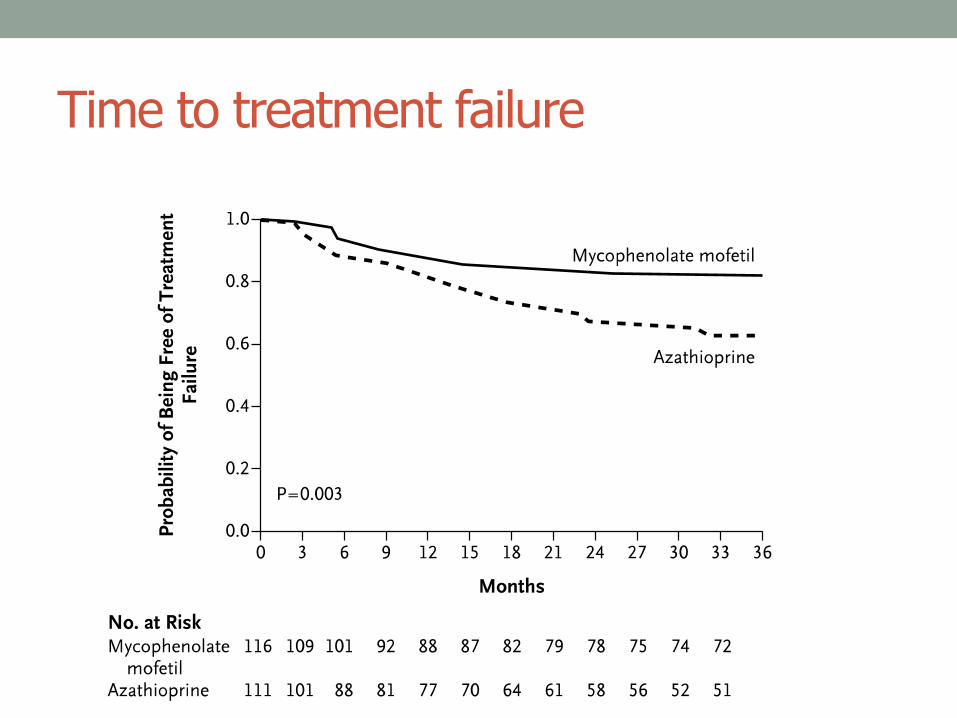
Time to treatment failure
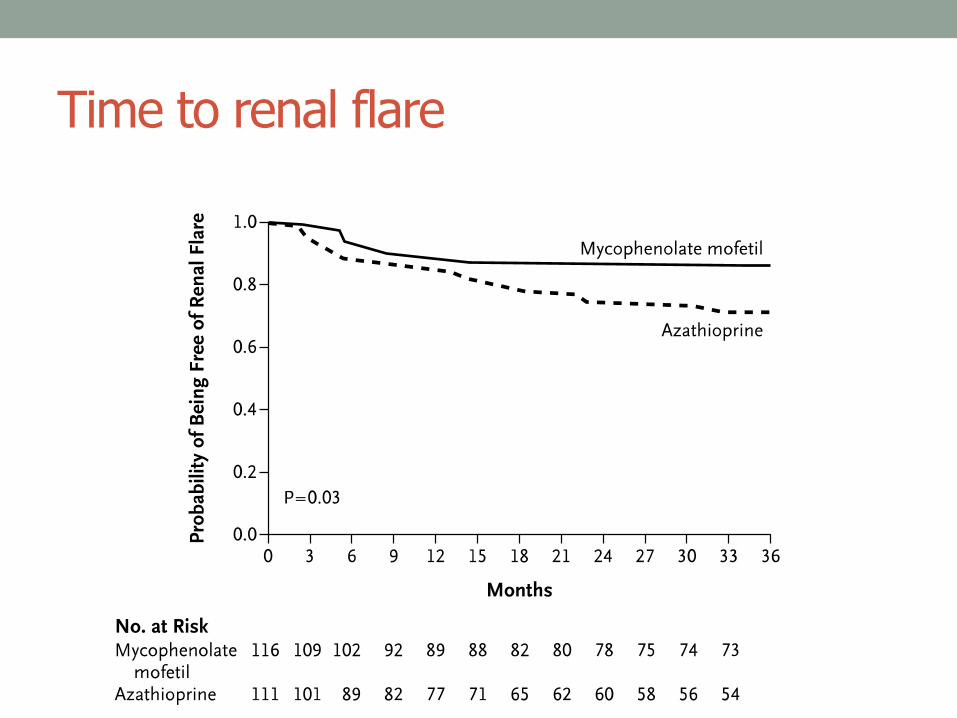
Time to renal flare
ALMS Conclusions
• Induction therapy
• NIH protocol IV CYC and MMF have similar efficacy and toxicity
• MMF may be superior in African-ancestry pts
• Maintenance therapy
• In pts who have achieved a renal response with induction therapy,
MMF is superior to AZA for maintenance therapy
• None of the tested therapies helped >60% patients
SYSTEMIC SCLEROSISSmall vessel vasculopathy
Pathological fibrosis
Autoimmunity
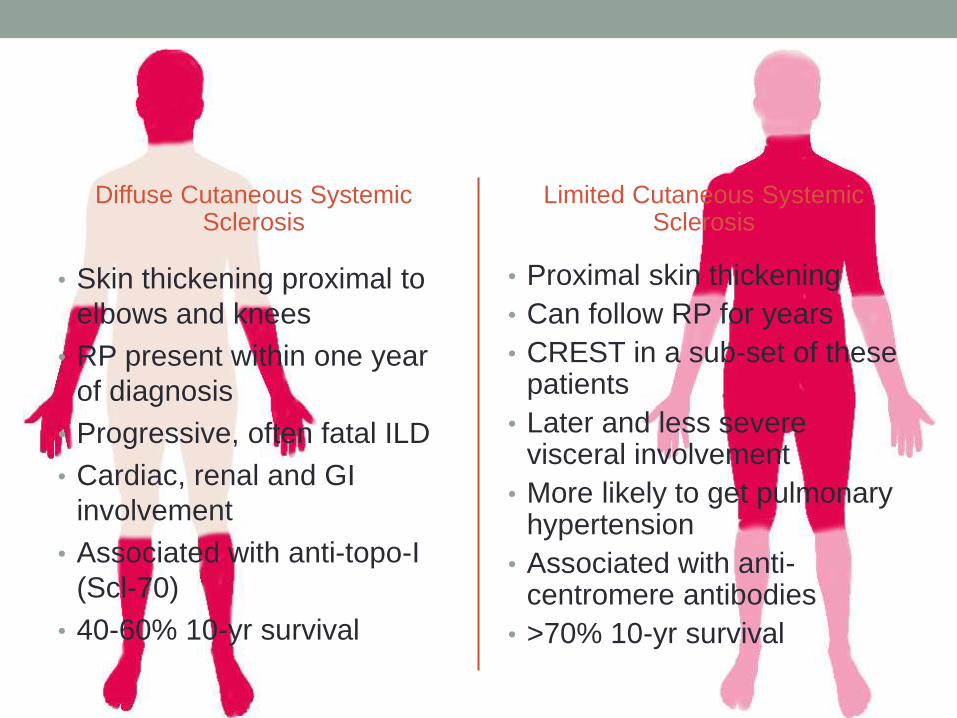
Diffuse Cutaneous Systemic Sclerosis
• Skin thickening proximal to
elbows and knees
• RP present within one year
of diagnosis
• Progressive, often fatal ILD
• Cardiac, renal and GI
involvement
• Associated with anti-topo-I
(Scl-70)
• 40-60% 10-yr survival
Limited Cutaneous Systemic Sclerosis
• Proximal skin thickening
• Can follow RP for years
• CREST in a sub-set of these patients
• Later and less severe visceral involvement
• More likely to get pulmonary hypertension
• Associated with anti-centromere antibodies
• >70% 10-yr survival
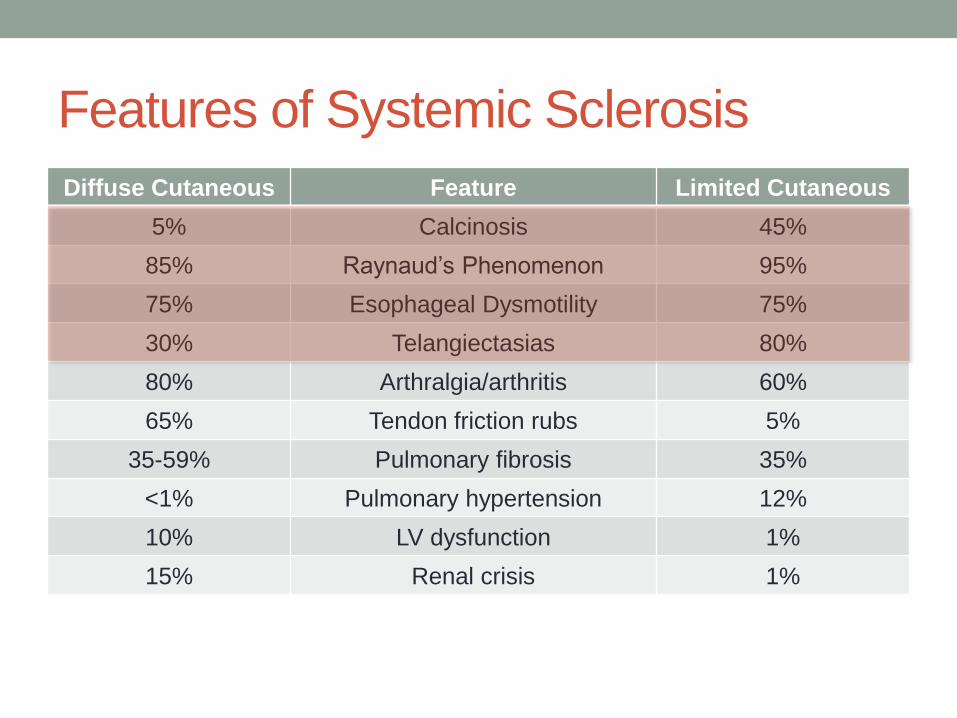
Features of Systemic Sclerosis
Diffuse Cutaneous Feature Limited Cutaneous
5% Calcinosis 45%
85% Raynaud’s Phenomenon 95%
75% Esophageal Dysmotility 75%
30% Telangiectasias 80%
80% Arthralgia/arthritis 60%
65% Tendon friction rubs 5%
35-59% Pulmonary fibrosis 35%
<1% Pulmonary hypertension 12%
10% LV dysfunction 1%
15% Renal crisis 1%

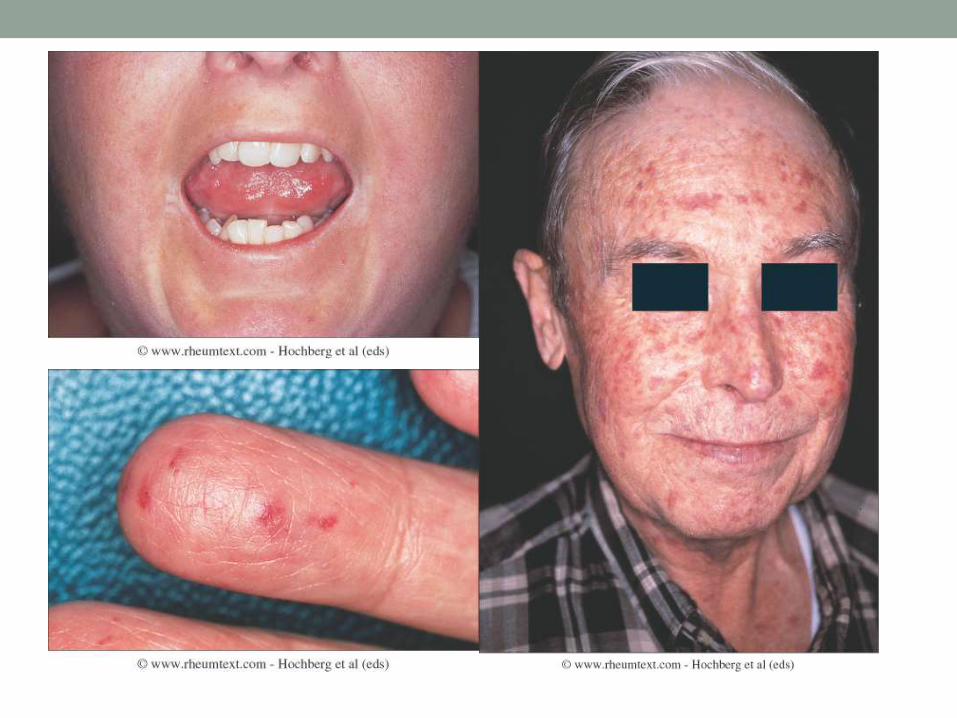
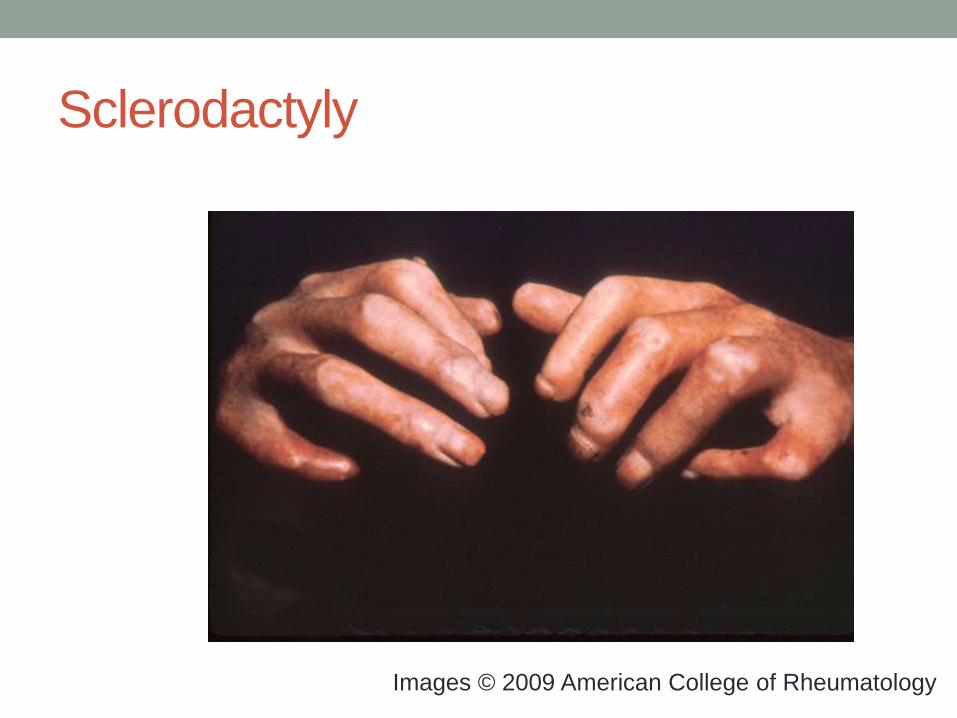
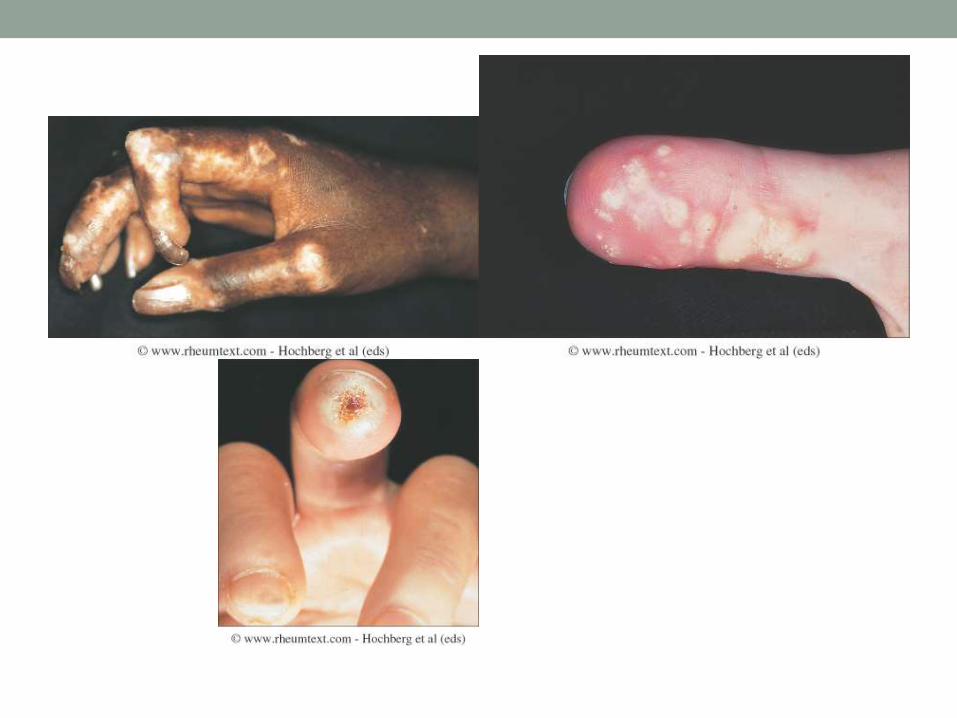
Sclerodactyly
Images © 2009 American College of Rheumatology
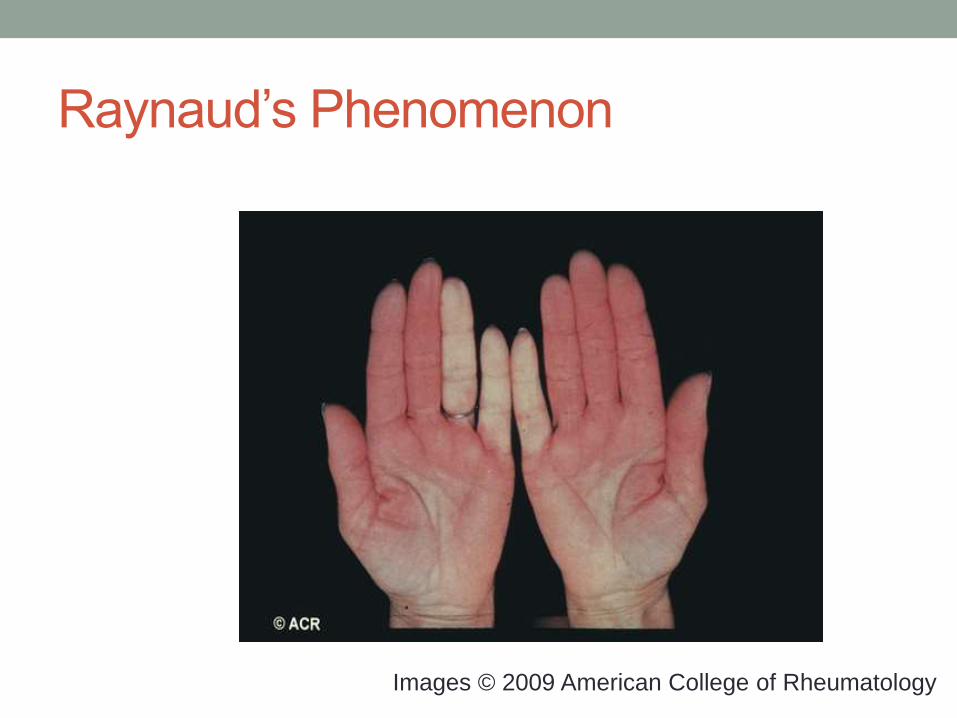
Raynaud’s Phenomenon
Images © 2009 American College of Rheumatology
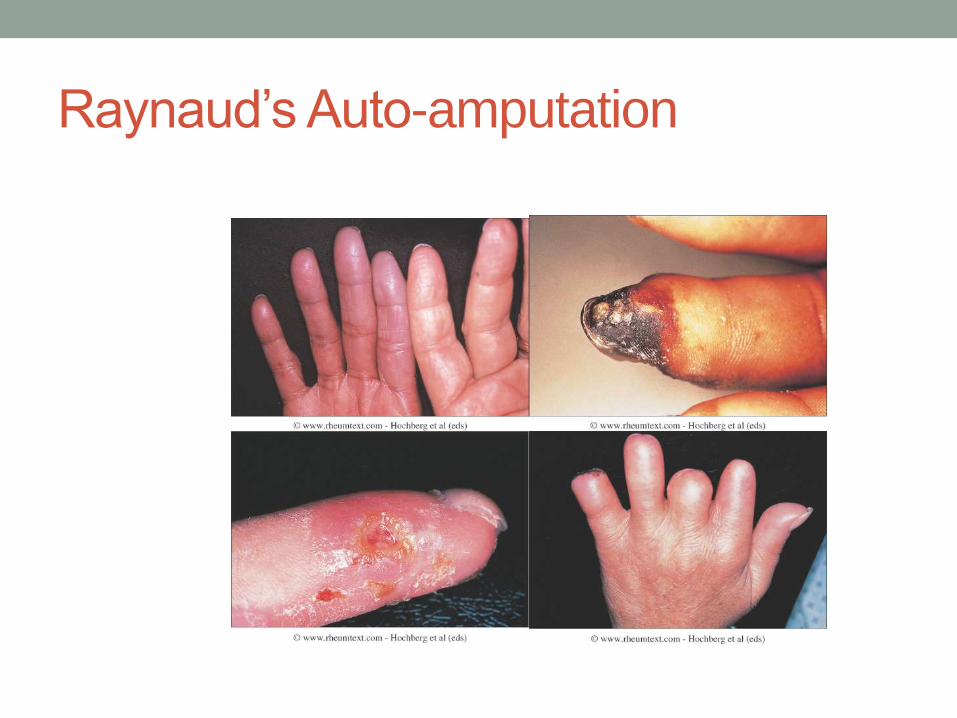
Raynaud’s Auto-amputation
Pulmonary Arterial Hypertension
• CTD-PAH accounts for 30% of all PAH worldwide
• Prevalence of PAH in SSc is 10-15%
• 80% 5-yr survival without PAH
• 10% 5-yr survival with PAH
• Risk factors
• Limited cutaneous form
• Raynaud’s for > 8 yr
• Anti-centromere or anti-nucleolar ANA (Scl-70 neg)
• DLCO < 60% without ILD
• FVC%/DLCO% ratio > 1.6
• Treatment is complicated – ETRA, PDE5i, prostanoids or
a combination of 2 or all 3
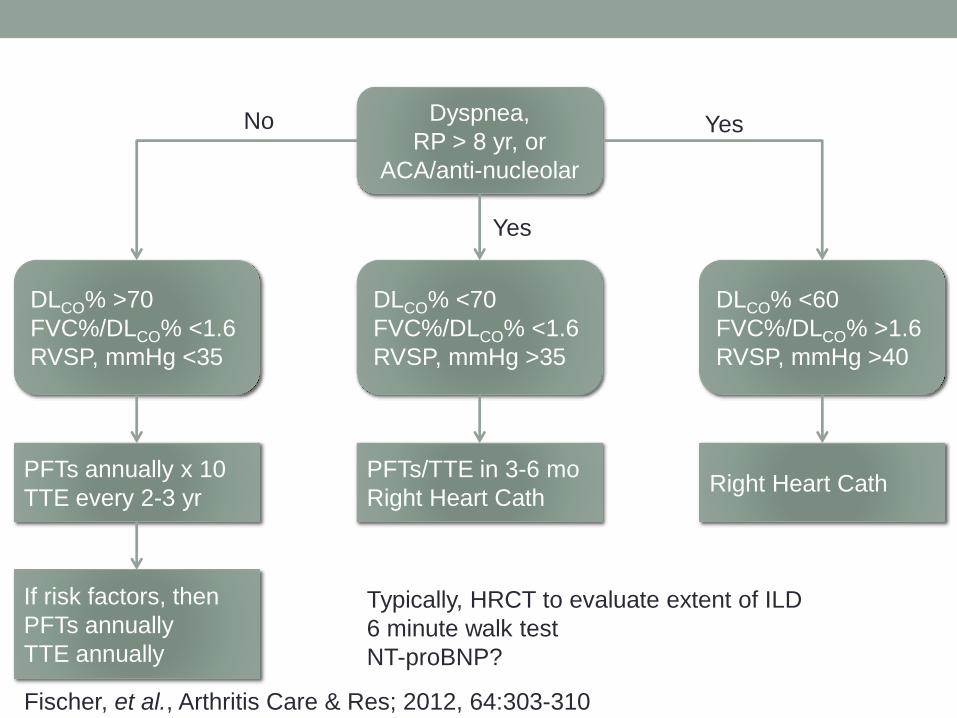
Dyspnea,
RP > 8 yr, or
ACA/anti-nucleolar
DLCO% <60
FVC%/DLCO% >1.6
RVSP, mmHg >40
DLCO% <70
FVC%/DLCO% <1.6
RVSP, mmHg >35
DLCO% >70
FVC%/DLCO% <1.6
RVSP, mmHg <35
PFTs annually x 10
TTE every 2-3 yr
If risk factors, then
PFTs annually
TTE annually
PFTs/TTE in 3-6 mo
Right Heart CathRight Heart Cath
No Yes
Yes
Typically, HRCT to evaluate extent of ILD
6 minute walk test
NT-proBNP?
Fischer, et al., Arthritis Care & Res; 2012, 64:303-310
Raynaud’s Phenomenon
• SSc patients have structural ischemia (fibrosis) as well as
functional ischemia (vasospasm)
• Keep warm, even in summer!
• Extended-release calcium channel blockers
• ACEi, ARBs, SSRI possibly effective
• PDE5 inhibitors – true placebo not possible
• Endothelin receptor antagonists – may help ulcers but not
symptoms
• Topical nitrates – tolerance a problem
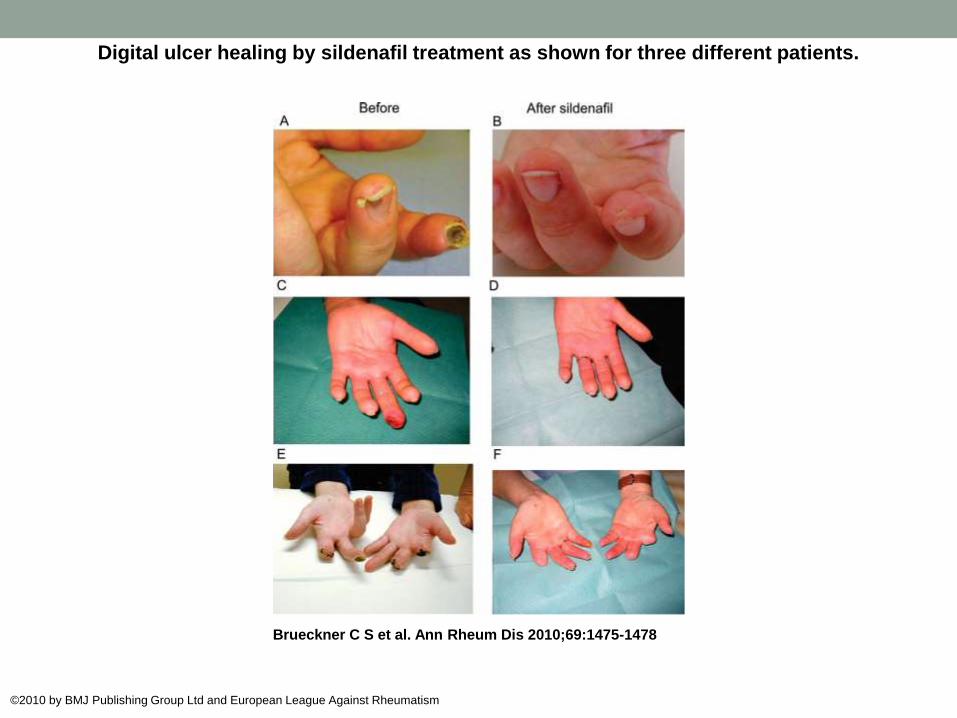
Digital ulcer healing by sildenafil treatment as shown for three different patients.
Brueckner C S et al. Ann Rheum Dis 2010;69:1475-1478
©2010 by BMJ Publishing Group Ltd and European League Against Rheumatism
MCTD
Mixed Connective Tissue Disease
• Patients with overlapping features of SLE, polymyositis
and scleroderma
• Associated with high titer U1-RNP antibody
• Not to be confused with “overlap” or “undifferentiated”
connective tissue disease
“Discovery” of MCTD
Rash
Arthritis
Serositis
ANA
SLE
Raynaud’s
Puffy Hands
Mild arthritis
Myositis
High Titer
anti-U1-RNP
MCTD – A New Disease?
• Original Description:
• Mild, highly steroid responsive
• Little, if any, renal, CNS, or pulmonary disease
• Not lupus (anti-Sm or anti-DNA excluded patients)
• But, 8 years later:
• 8 patients had died
• Many had moved toward systemic sclerosis features
• Association with anti-RNP not clear
• Anti-RNP is not unique to MCTD
• Many MCTD patients can fit criteria for RA, SLE, or SSc
• Risk of fitting clinical features to a syndrome based on serology
MCTD – Diagnostic Criteria
• Four competing criteria!
• Alarcón-Segovia, et al.
• Anti-U1-RNP at 1:1600 or greater (no clue what this is now), and
• Three or more clinical criteria
• Edema of the hands
• Raynaud’s phenomenon
• Acrosclerosis
• Myositis
• Synovitis
• 81.3% sensitive; 86.3% specific in anti-RNP+ patients
MCTD – Not Benign
• 11% developed glomerulonephritis
• 17% had neurological manifestations
• Pulmonary disease and esophageal dysmotility both seen
in two-thirds of patients
• Pulmonary HTN (often asymptomatic) seen in 23%,
including all 9 of 47 patients who died of MCTD related
causes
• Other studies
• ILD/PF seen in 20-65%
• PHT seen in 10-45%
• BAL has CD4+ T cell predominance
MCTD
• Not all anti-RNP is MCTD
• These patients may be better classified as
undifferentiated CTD
• Make sure to screen for lung disease.
QUESTIONS?