Embed Size (px)
Citation preview
CONTRACTED EYE SOCKET RECONSTRUCTION
Questions to be answered
• What is the eye socket?• What is the common causes for enucleation?• What is the contracture of socket?• What cause that?• how to prevent it?• Aims of surgery?• Types of surgery?• Types of implant?
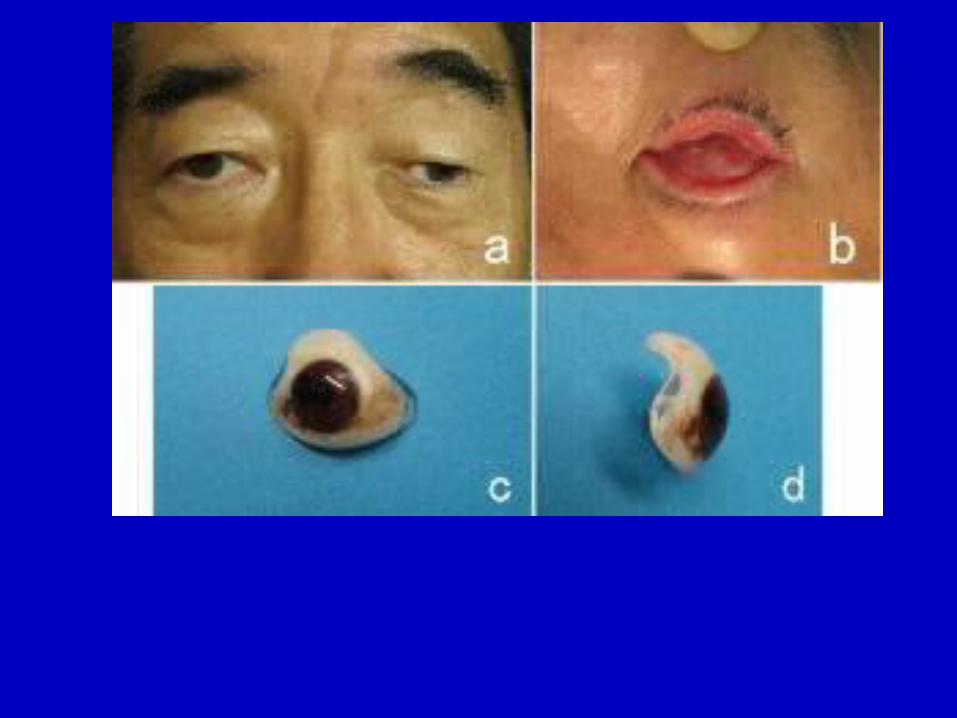
• Enucleation is the removal of the eye that leaves the eye muscles and remaining orbital contents intact.
• Exenteration – removal of the contents of the eye socket, including the eyeball, fat, muscles, and other adjacent structures of the eye.
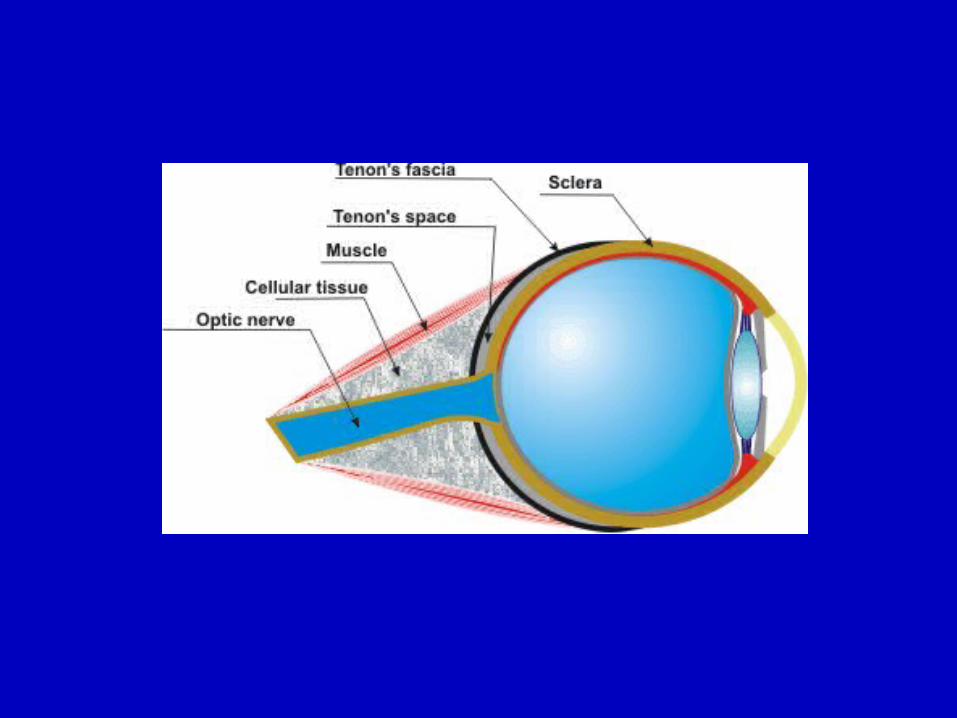
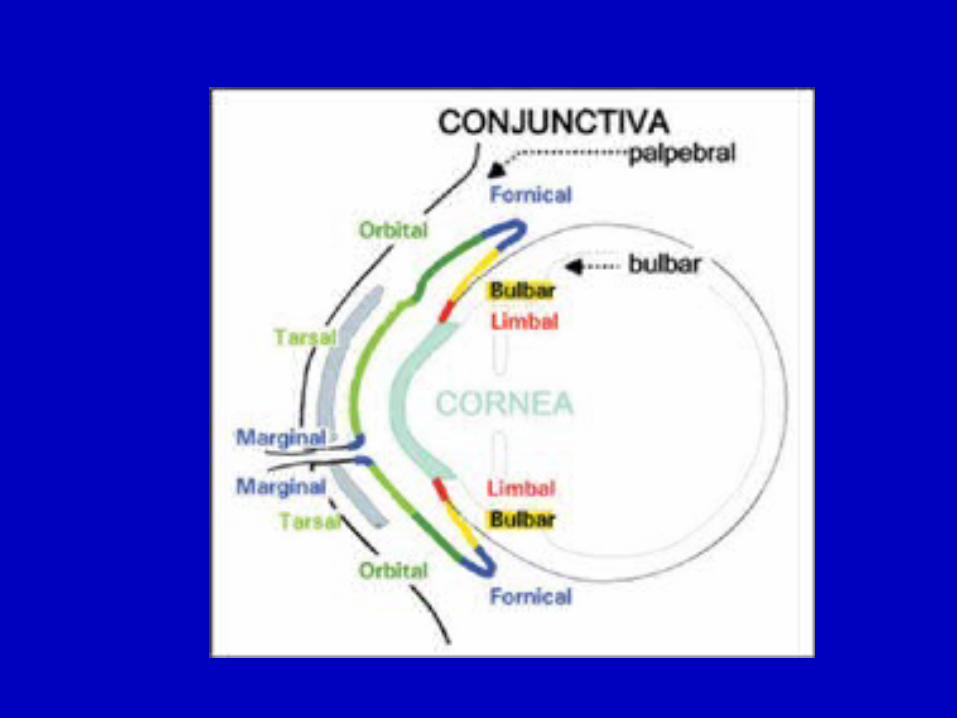
• Tenon's capsule thin membrane which envelops the eyeball from the optic nerve to the limbus, separating it from the orbital fat and forming a socket in which it moves, In front it adheres to the conjunctiva.
• After enucleation orbital implant iserted to the Tenon's capsule in order to keep the orbital size and to keep eye animation .

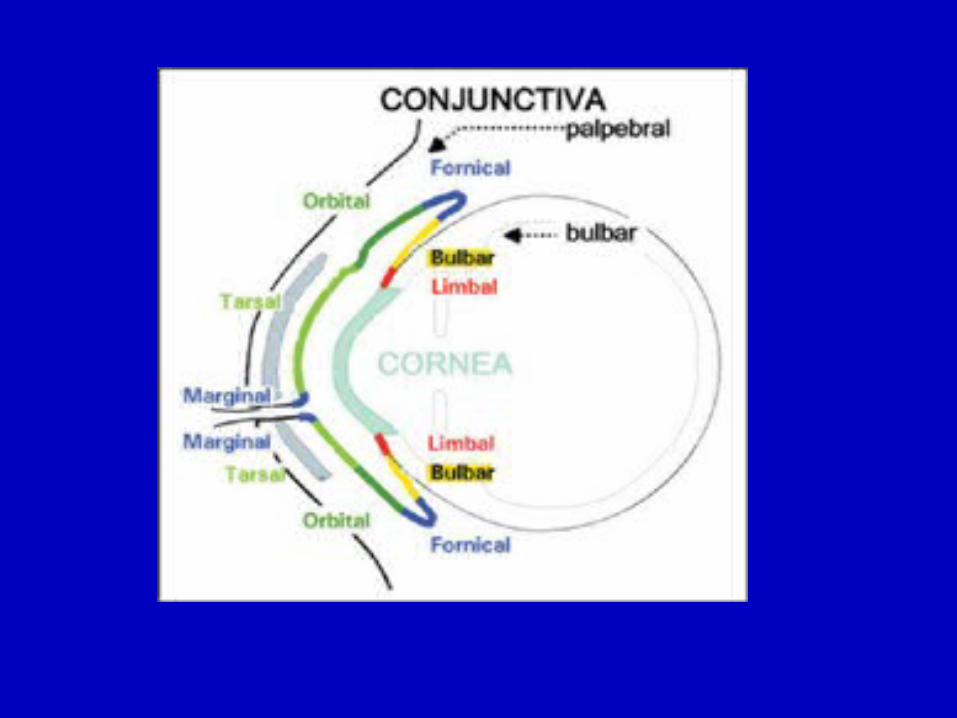
The term Eye socket is refer to:• Eyelids• Conjunctival fornices• Orbital structures(bony cavity and soft tissues)
Common causes requiring socket reconstruction
• Congenital (anophthalmia ,microphthalmia)• Trauma• Tumour• scarring
contracture of socket
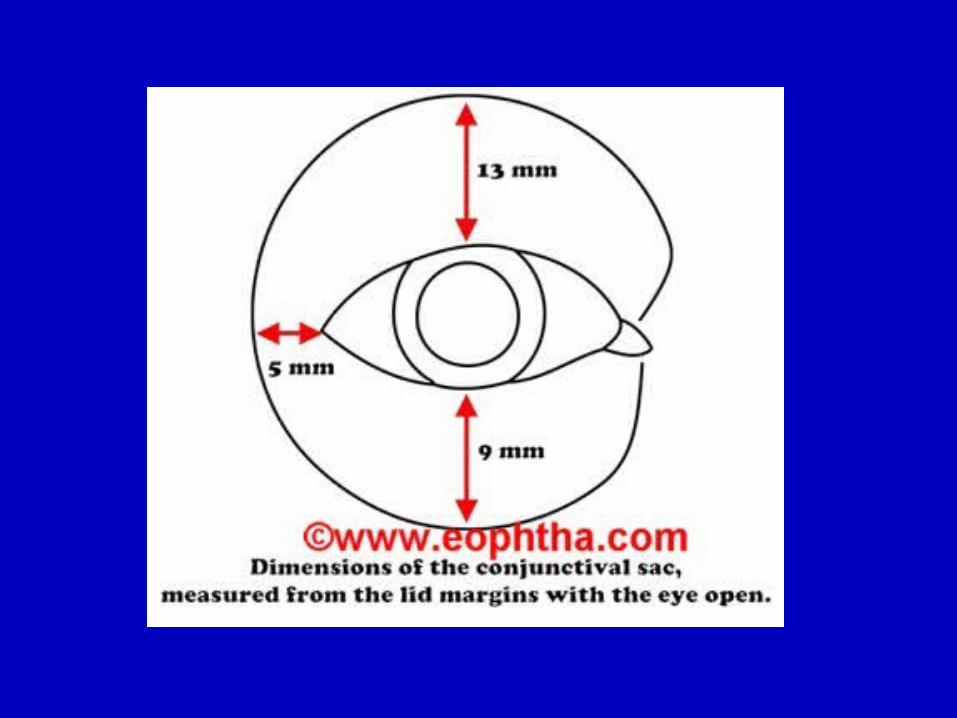
It refer to :• extensive loss of conjunctiva surface area • deep scar formation • shrinkage of orbital fat• conjunctiva fornices contracture.
Causes of contracture of socket
• irradiation of the socket as after enucleation in some cases of retinoblastoma.
• severe socket infections.• faulty or non wearing of the artificial eye.• keloid like mass formation in the socket.• tissue loss due to injury.• scarring of the conjunctiva due to various
factors(allergy for ex.)
Main compliants
The main presenting complaint :• story of a gradually increasing difficulty in
retaining the prostheses.• the patients are not satisfied with the
cosmetic appearance.
Preoperative assessment
the contracted sockets should be examined clinically and microbiologically.
History :In every case, mode, circumstances and duration of the eye loss, and subsequent problems with the prostheses .
The socket should be examined for fibrous bands, condition of the various fornices and the state of the conjunctiva.
• Never forget to Assess the prosthesis shape and size .
• Look for orbital implant exposure.

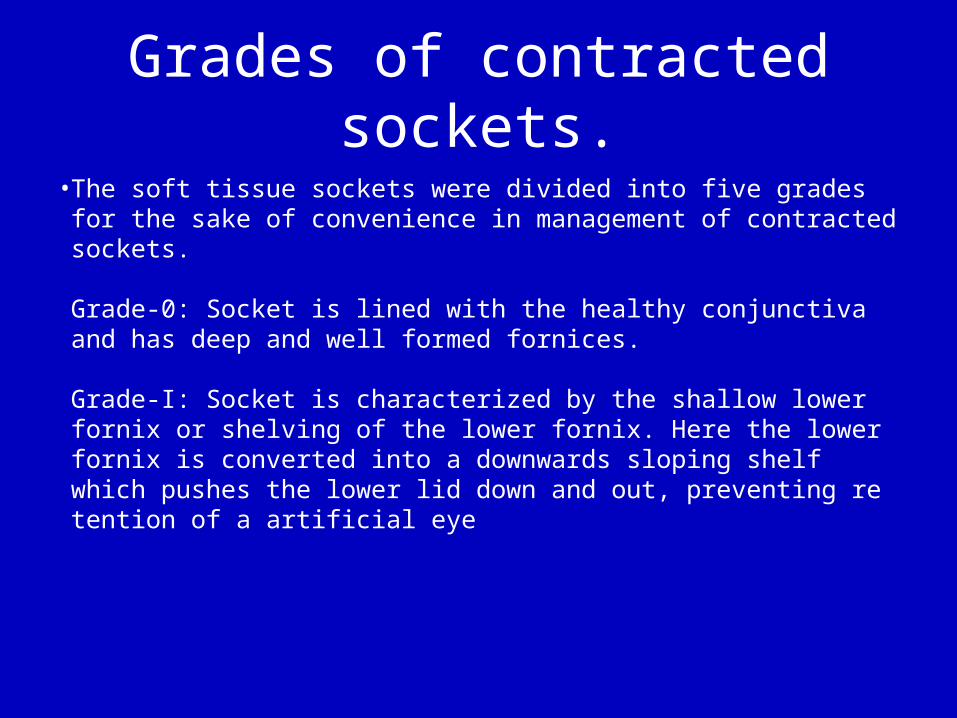
Grades of contracted sockets.• The soft tissue sockets were divided into five grades for the sake of
convenience in management of contracted sockets.
Grade-0: Socket is lined with the healthy conjunctiva and has deep and well formed fornices.
Grade-I: Socket is characterized by the shallow lower fornix or shelving of the lower fornix. Here the lower fornix is converted into a downwards sloping shelf which pushes the lower lid down and out, preventing re tention of a artificial eye
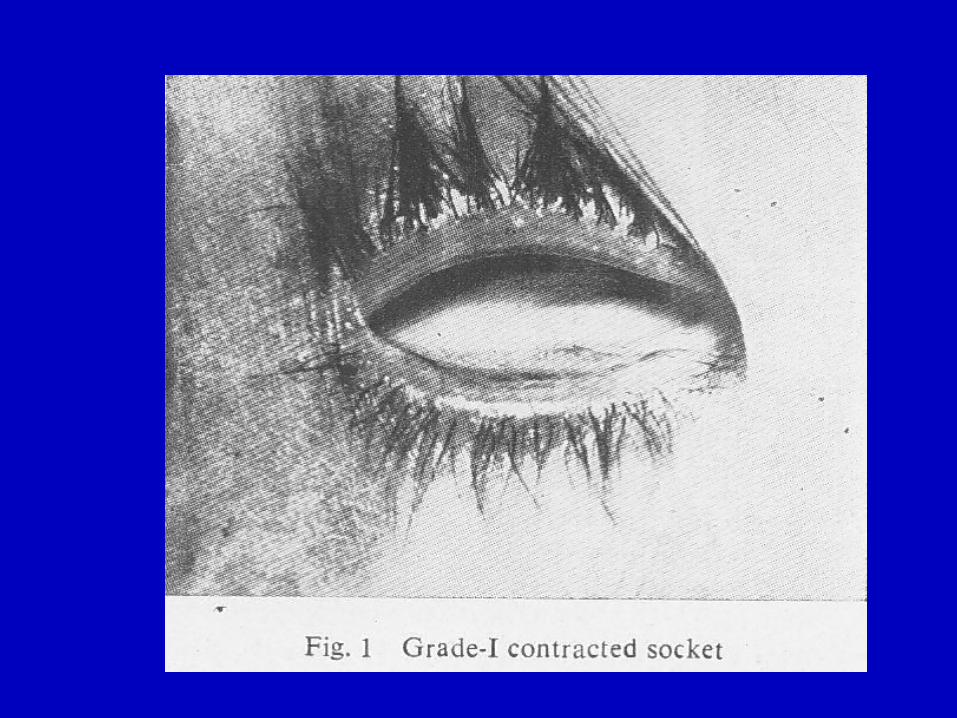
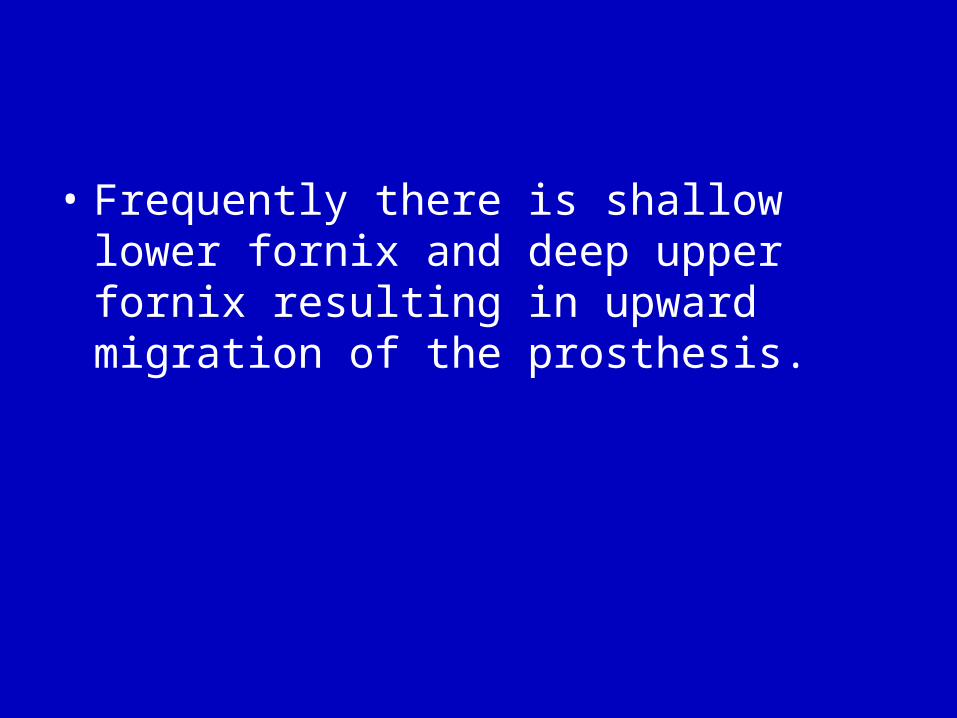
• Frequently there is shallow lower fornix and deep upper fornix resulting in upward migration of the prosthesis.
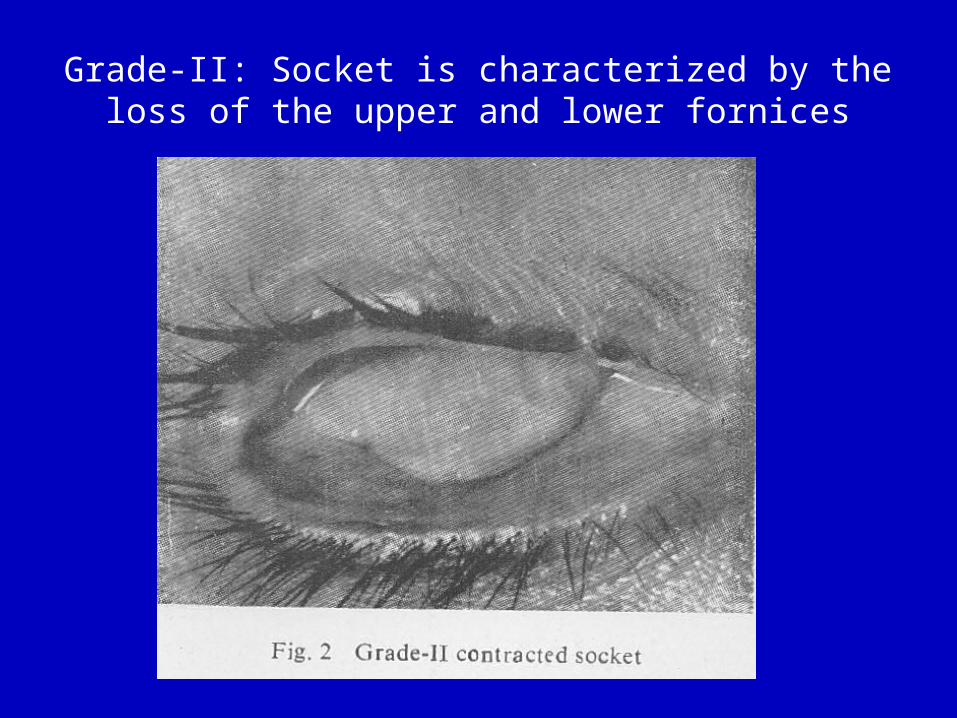
Grade-II: Socket is characterized by the loss of the upper and lower fornices
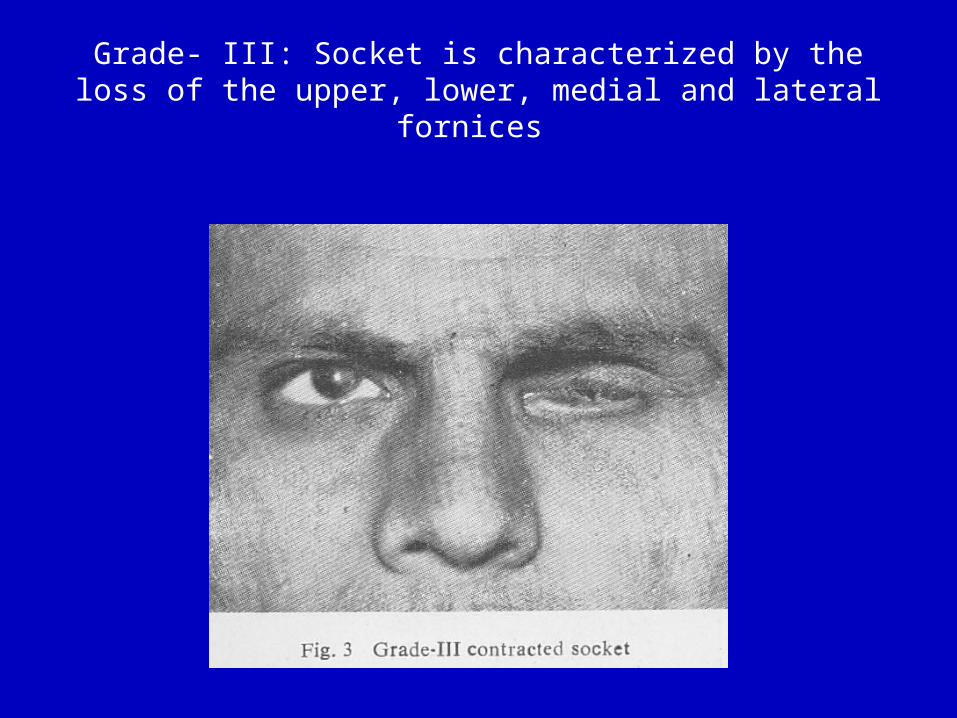
Grade- III: Socket is characterized by the loss of the upper, lower, medial and lateral fornices
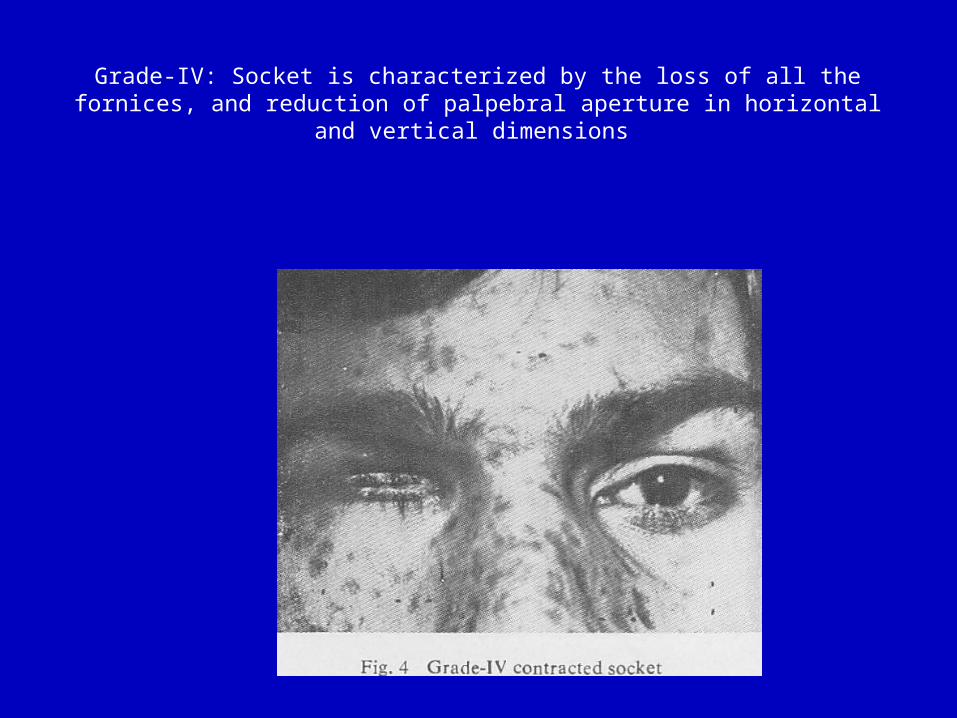
Grade-IV: Socket is characterized by the loss of all the fornices, and reduction of palpebral aperture in horizontal and vertical dimensions
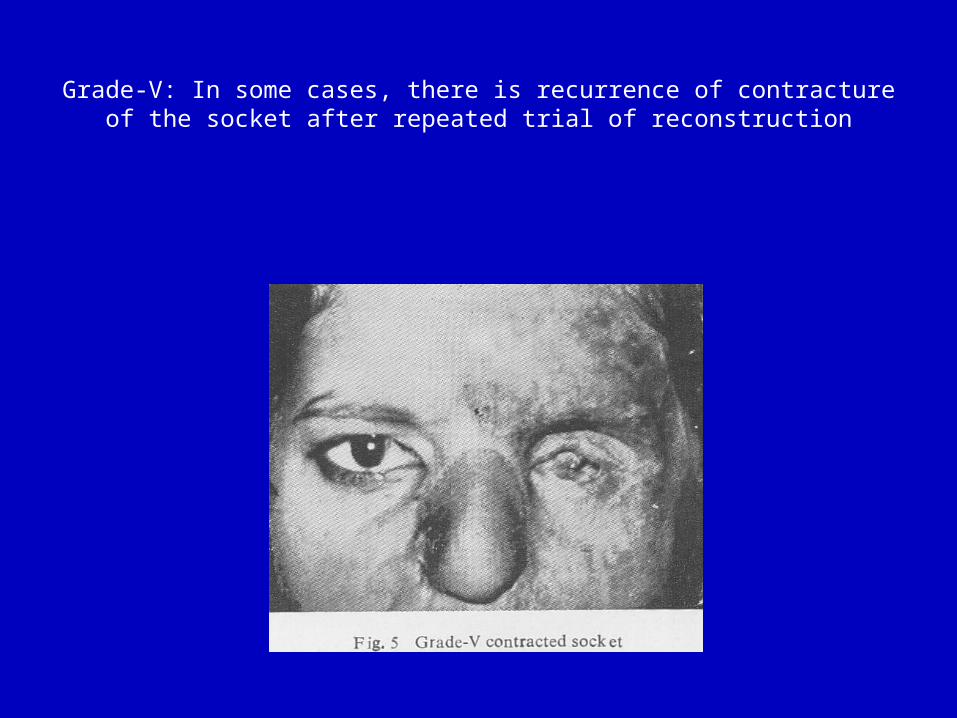
Grade-V: In some cases, there is recur rence of contracture of the socket after re peated trial of reconstruction
Aims of reconstruction
• To establish stable fornices by increasing the surface area by (hard palate ,oral mucosal,skin graft) and if necessary by increasing size by orbital implant.
• The ocular prostheses should be light and take its support from infraorbital rim not from the lids.
Prevention
• By use of conformer made by ocularist placed inside orbit to help support the growth of eye socket and bones in the face.
• the conformer used during healing for about 6 weeks then ocular shell prosthesis used there after.


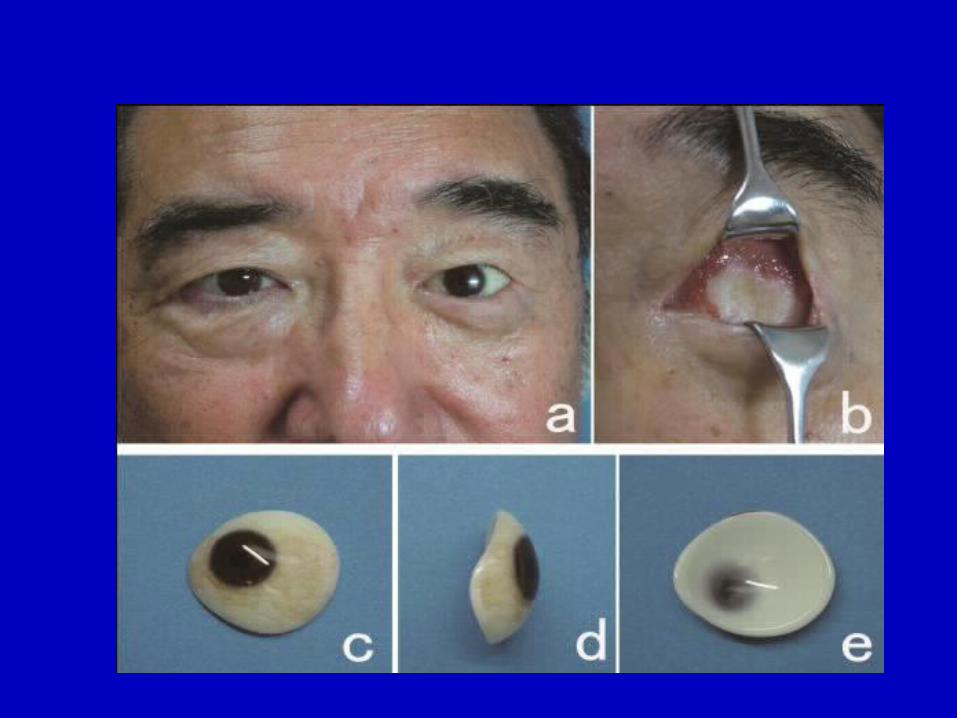
Types of ocular prosthesis
• Spherical or oval• Stock or custom made• Porous or non porous• Chemical make up• Presence or absence of motility post.
Surgical principle• First : obtain adequate palpepral aperture size
(canthoplasty may be needed in grade3,4,5)• Second : create adequate fornixes (lower,upper,lateral)
insicion central in grade 2 while it can be at inferior position in grade 1.
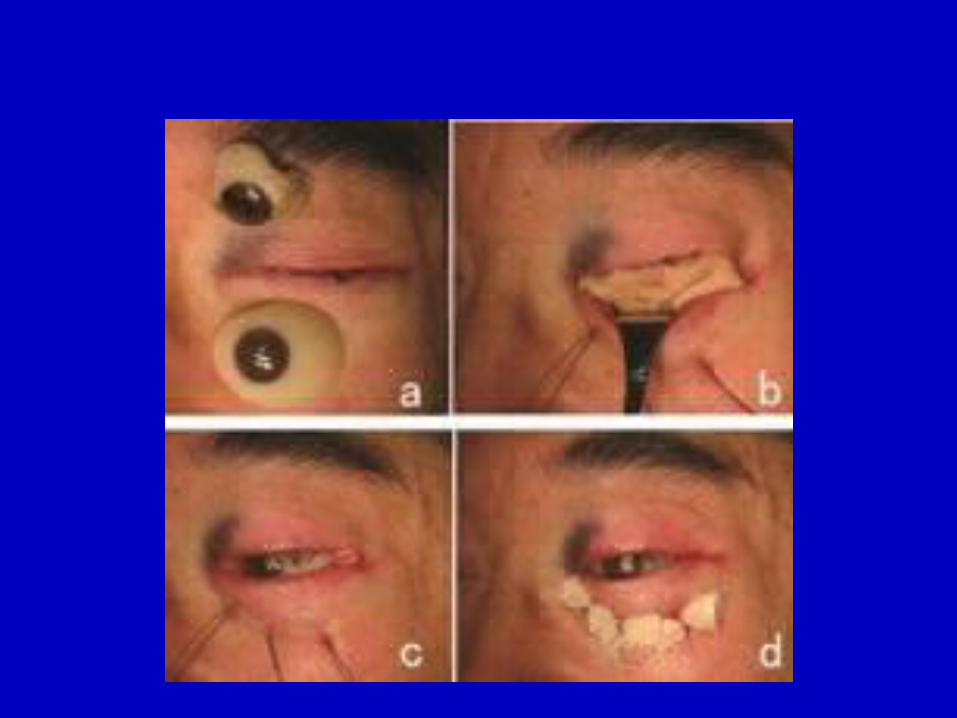
• Third : perfect lining of the created fornix (hard palate ,oral mucosal,skin graft ,amniotic membrane)
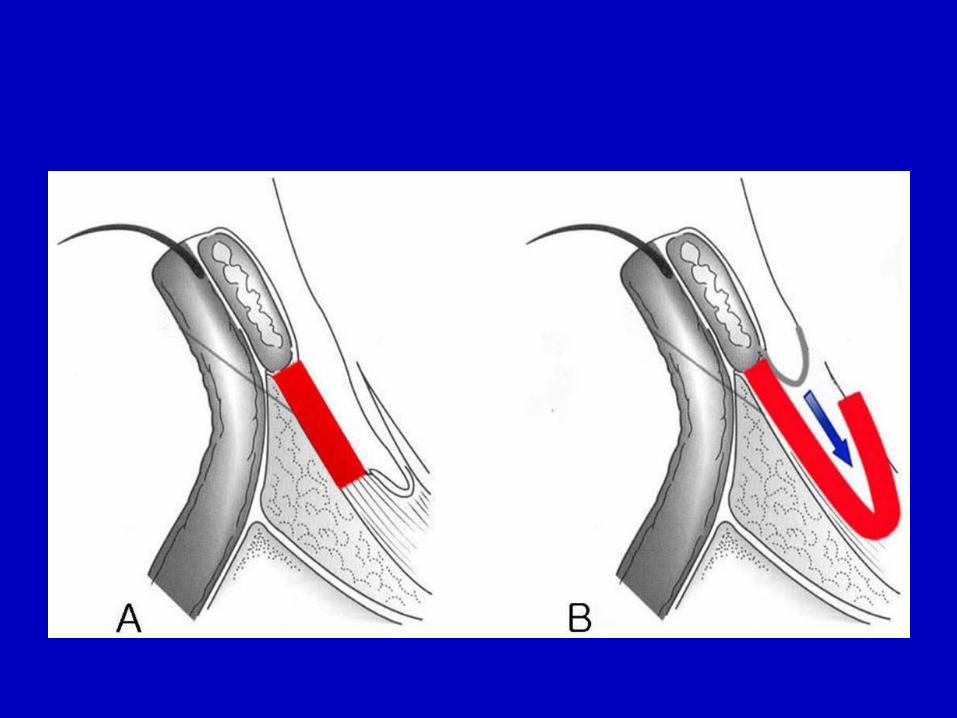
• Fourth be sure that the fornix created supported by orbital bony rim to create a stable and deep lower fornix, the lower edge of the graft should be sutured to the inferior orbital bone rim using anchor sutures .
• Fifth: the conformer used during healing for about 6 weeks then ocular shell prosthesis used there after.
• Sixth : central temporary tarsorrhaphy may be used.
Orbital implant exposure
• One of the most important aspect of eye socket reconstruction can present with or without socket contracture.
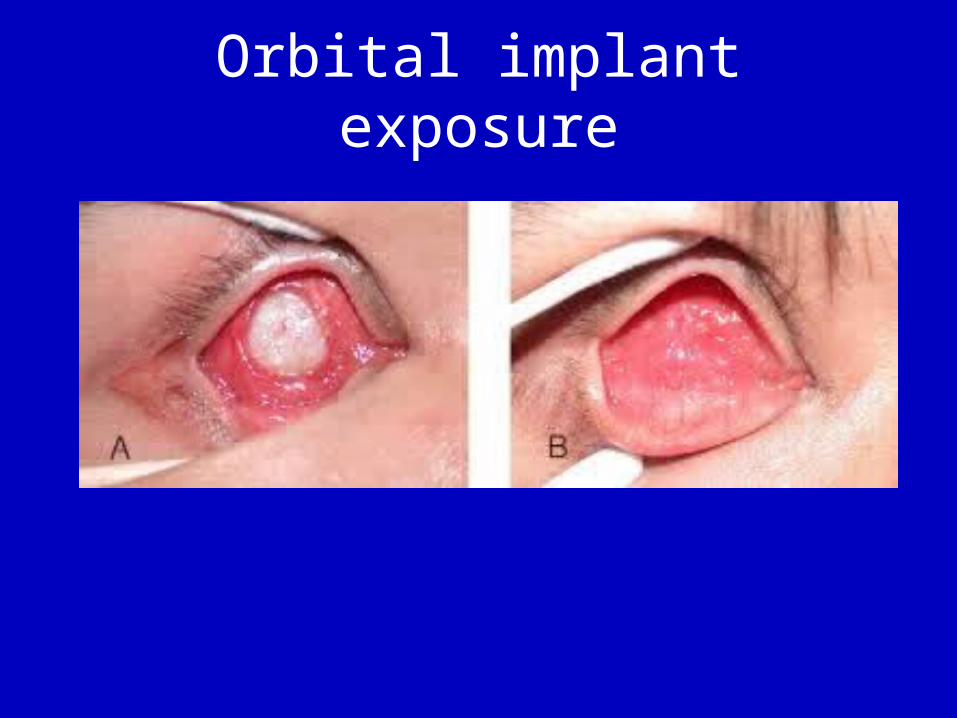
Orbital implant exposure

• Autogenous Derma-Fat Graft used usally in case of Exenteration and in cases of extrusion or implant exposure.
The extraocular muscles and conjunctiva is sutured into the border of the DFG
Thank you






![ReconstructionofTotalLowerEyelidDefectswith ...downloads.hindawi.com/journals/criopm/2012/927260.pdf · reconstruction of anophthalmic orbit with a contracted eye socket [7–9] and](https://img.pdfslide.net/doc/110x75/5f33462a25abc14195249f3b/reconstructionoftotallowereyeliddefectswith-reconstruction-of-anophthalmic-orbit.jpg)






















