Embed Size (px)
Citation preview
Controversies in Brain DeathMartin SmithConsultant & Honorary ProfessorThe National Hospital for Neurology & NeurosurgeryUniversity College London Hospitals
Medical Physics and Biomedical EngineeringUniversity College London
• the concept of brain death
• whole brain or brainstem death
• how to prove irreversibility
• one or two neurological examinations
• ancillary tests
• brain death as a construct to facilitate organ donation
Controversies
• prior to development of life-supporting therapies in in the 1950s death was a unitary phenomenon– following cessation of one of the three ‘vital’ functions critical to life,
both of the others ceased within minutes
• inability to restore or support vital functions made the diagnosis of death straightforward– its determination was not always accurate
History of brain death
• developments in critical care in the 1950s– somatic function sustained by mechanical ventilation long after cessation
of brain function– patients did not fulfil historical criteria for death, i.e. absence of all vital
signs
History of brain death
• developments in critical care in the 1950s– somatic function sustained by mechanical ventilation long after cessation
of brain function– patients did not fulfil historical criteria for death, i.e. absence of all vital
signs
• Mollaret and Goulon – 1959– 23 unconscious patients with brainstem areflexia
and absence of spontaneous respiration– ‘le coma dépassé’ - a state beyond coma
History of brain death
• no call to formalise diagnosis of brain death until 1967 – 107 heart transplants were carried out in 1968 using organs from beating
heart donors in 24 different countries despite there being no mechanism to confirm death prior to donation
History of brain death
• ad hoc committee of the Harvard Medical School– 1968 - first widely accepted standard
• brain stem function fundamental to state of irreversible coma– Mohandas and Chou (1971)
• UK guidelines– Report from the Conference of the Medical Royal Colleges and their
Faculties (1976 & 1979)
• more than 80 countries had accepted a brain-based determination of death by the turn of the 21st century– many enacted this medical practice into national laws
History of brain death
• initially accepted as a medical and legal standard in the absence of a rigorous philosophical justification– vigorous debate about the definition of death continues within
academia– no impact on determination of death at the bedside
• ‘alive’ and ‘dead’ are the only two possible states for an organism– infers that transition from one to the other is instantaneous– death marks the transition between the two
• death of an organism as a whole is a process and not an event at a single moment in time
The concept of (brain) death
• need for consensus in common terminology to support clarity and precision in the language used in death determination
Words matter

Brain dead woman gives birth to miracle baby after doctors keep her alive on a ventilator for seven weeks - then allow her to pass away
The baby born after 107 days inside his dead mum hooked up to ventilator
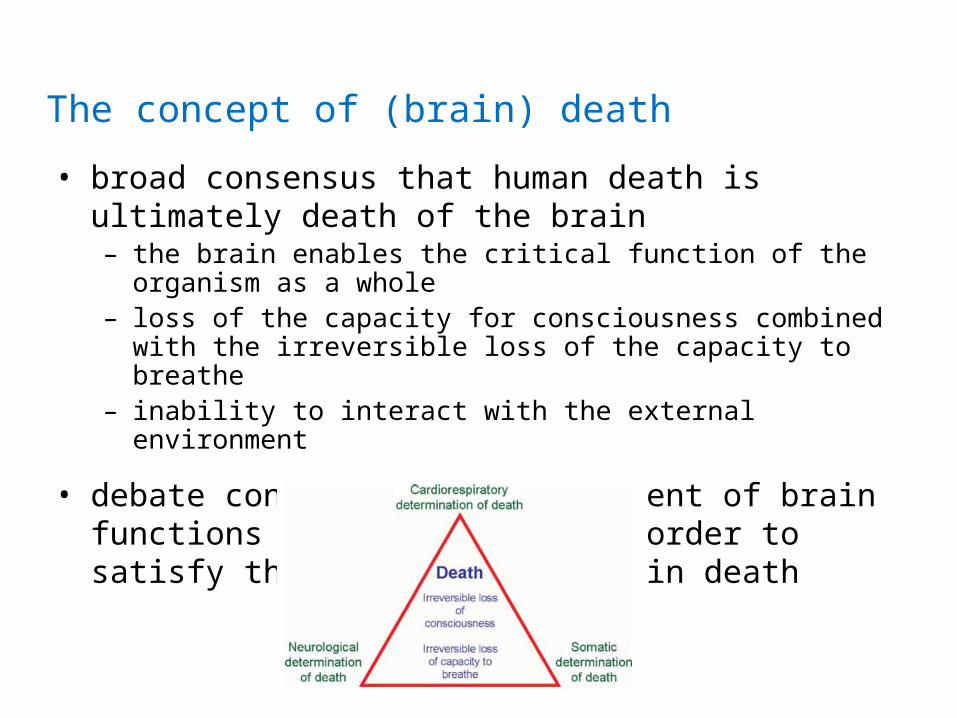
• broad consensus that human death is ultimately death of the brain– the brain enables the critical function of the organism as a whole– loss of the capacity for consciousness combined with the irreversible
loss of the capacity to breathe– inability to interact with the external environment
• debate continues over the extent of brain functions that must cease in order to satisfy the definition of brain death
The concept of (brain) death
• whole brain death– an individual who has sustained irreversible cessation of all functions
of entire brain is dead– irreversible loss of all intracranial neurological functions not
confirmed during clinical determination of whole brain death– some functions, such as hypothalamic-pituitary responses, can be
maintained
• brainstem death– key components of consciousness and respiratory control reside in the
brainstem– does not require confirmation that all brain functions have ceased but
that none of those functions that might persist should indicate any form of consciousness
Brainstem vs. whole brain death
• the clinical determination of whole brain and brainstem death is the same but role of confirmatory investigations different
• little practical relevance– death is not a single event but a process– biological death of the whole human organism cannot be proven
during the diagnosis of brain death– point of irreversibility
Brainstem vs. whole brain death
Clinical determination of brain death
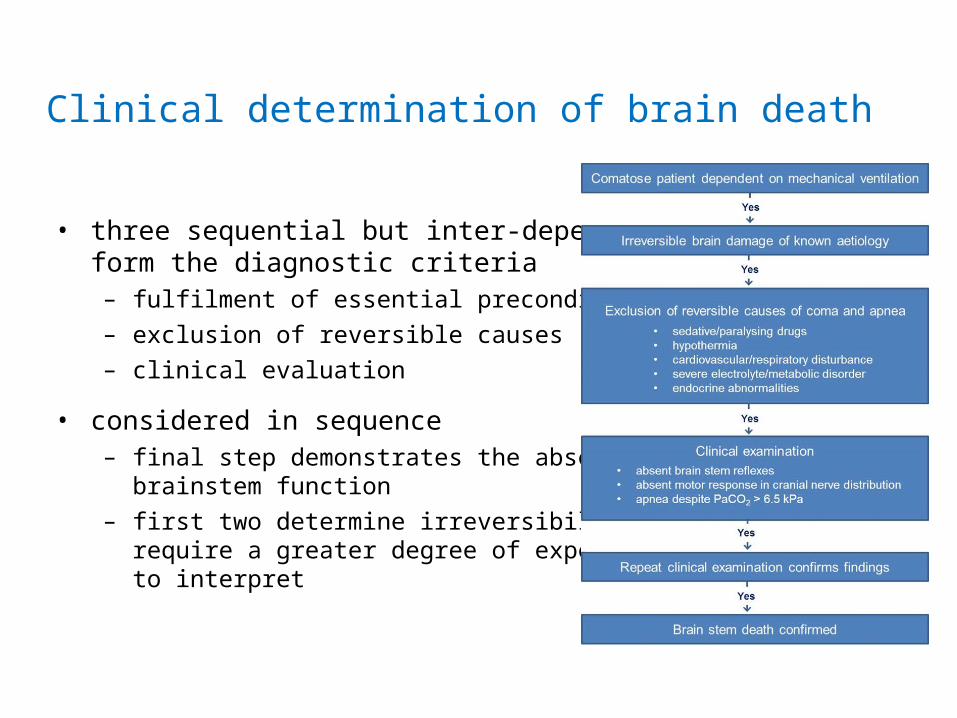
• three sequential but inter-dependent stepsform the diagnostic criteria
– fulfilment of essential preconditions– exclusion of reversible causes – clinical evaluation
• considered in sequence– final step demonstrates the absence of
brainstem function– first two determine irreversibility and
require a greater degree of expertise to interpret
• patient’s comatose condition and dependence on mechanical ventilation due to irreversible brain damage of known aetiology– irreversibility might be obvious within a relatively short period of
time, e.g. after severe TBI, ICH, stroke– may take longer to establish diagnosis and be confident of
prognosis after hypoxic brain injury. e.g. cardiac arrest, severe cardiorespiratory insufficiency
Preconditions
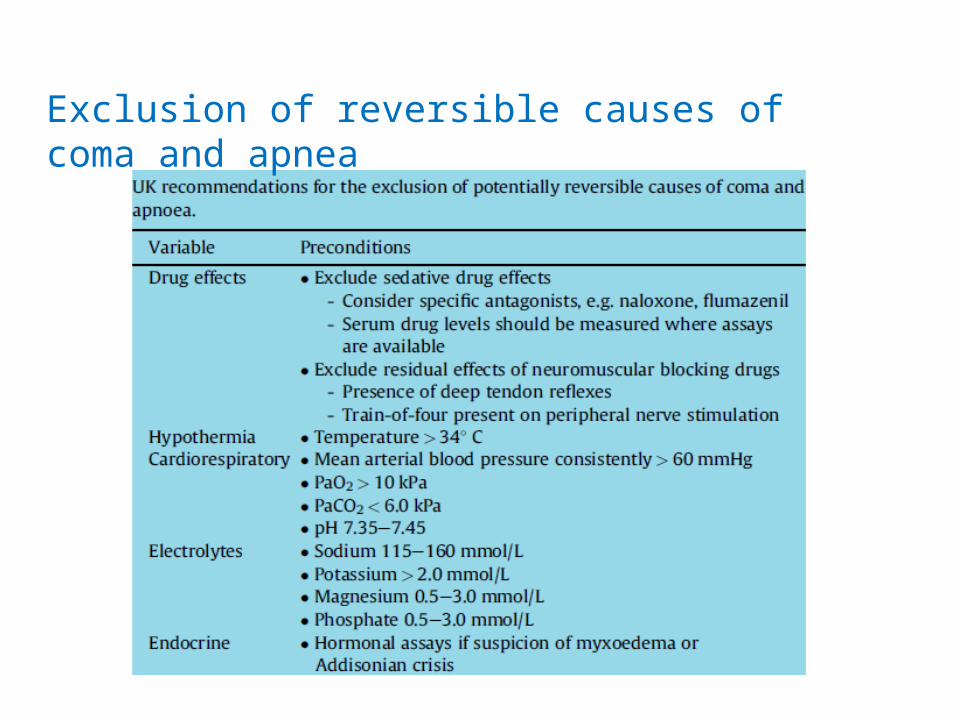
Exclusion of reversible causes of coma and apnea
Crit Care Med 2011; 39: 1538-42
Confounding effects of hypothermia
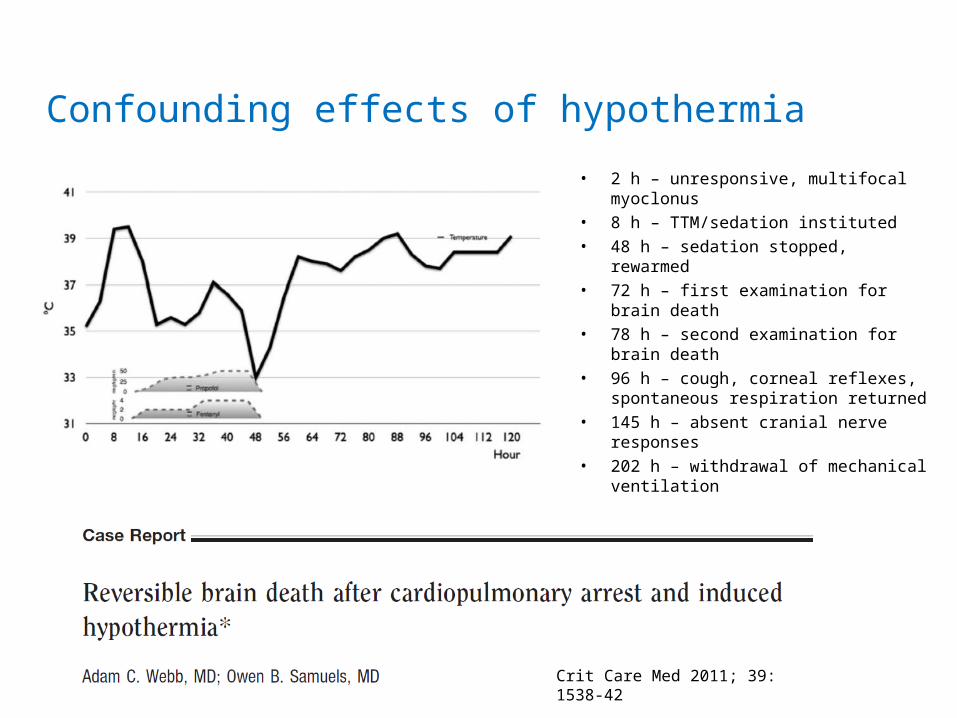
• 2 h – unresponsive, multifocal myoclonus• 8 h – TTM/sedation instituted• 48 h – sedation stopped, rewarmed• 72 h – first examination for brain death• 78 h – second examination for brain death• 96 h – cough, corneal reflexes,
spontaneous respiration returned• 145 h – absent cranial nerve responses• 202 h – withdrawal of mechanical
ventilation
Crit Care Med 2011; 39: 1538-42
Confounding effects of hypothermia
• there is no ‘reversible’ brain death
• ‘false positive’ brain death determination always results from examination inadequacies– hypothermia slows metabolism of depressant and neuromuscular
blocking drugs– all brain death guidelines require reversible causes to be excluded– protocols should mandate a delay between rewarming and
determination of brain death
Confounding effects of hypothermia
• practice guidelines generally mandate two sequential and independent examinations
• large study confirmed that a second examination added nothing to the first but delayed the declaration of death
• some jurisdictions now require only one examination– not universally accepted
One or two examinations?
• clinical diagnosis is sufficient for the determination of brain death in many jurisdictions– no published reports of recovery after a diagnosis of brain death using
established criteria– not possible if preconditions for testing are not met or comprehensive
examination is not possible
• ancillary tests– optional in most countries– may reduce element of uncertainty and minimize period of
observation if clinical testing not possiblee.g. extensive maxillofacial injuries, inability to exclude primary metabolic derangement or residual sedation, high cervical cord injury
Ancillary tests
• demonstration of loss of electrical activity of the brain– EEG– evoked potentials
• confirmation of the absence of intracerebral blood flow– TCD– cerebral angiography– CT angiography– thallium scan
Ancillary tests
• role of EEG a source of debate since the early days of the description of brain death- non-reliance on EEG supported by the original description of
brainstem death and (lack of) EEG correlates by Mohandas and Chou
• patient who is brainstem dead may exhibit residual cortical electrical activity– EEG activity in 3.5% of patients with brainstem areflexia and apnea– dead brainstem always leads to asystole irrespective of EEG findings– waiting for inevitable onset of isoelectric EEG merely prolongs the
determination of death
• scalp EEG– may be isoelectric even in the presence of viable neurons in deep structures– affected by hypothermia and sedation
EEG
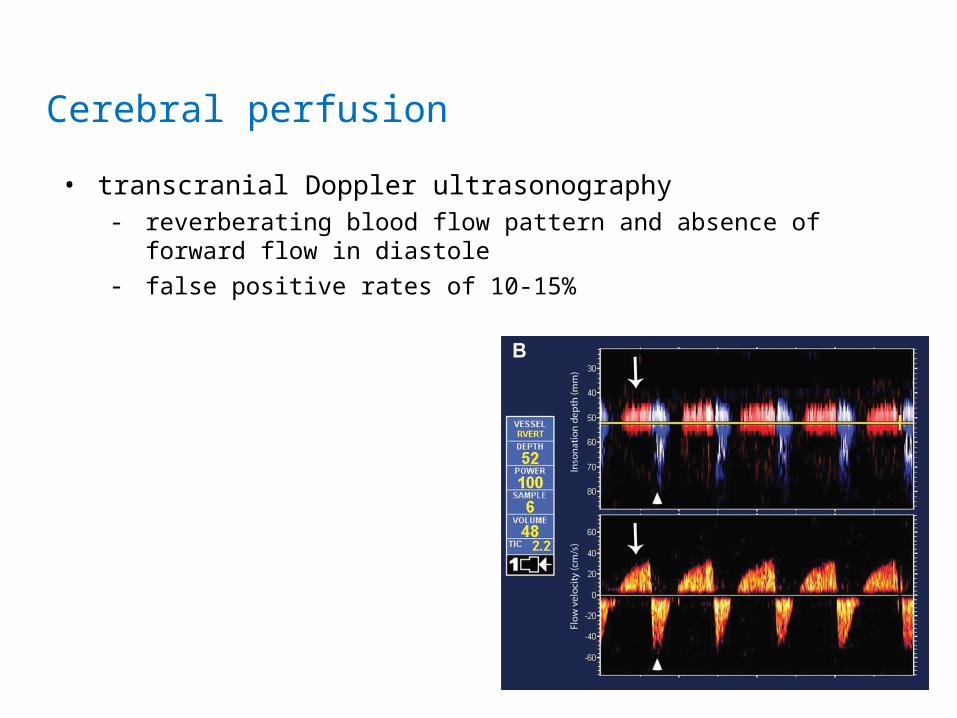
• transcranial Doppler ultrasonography- reverberating blood flow pattern and absence of forward flow in diastole- false positive rates of 10-15%
Cerebral perfusion
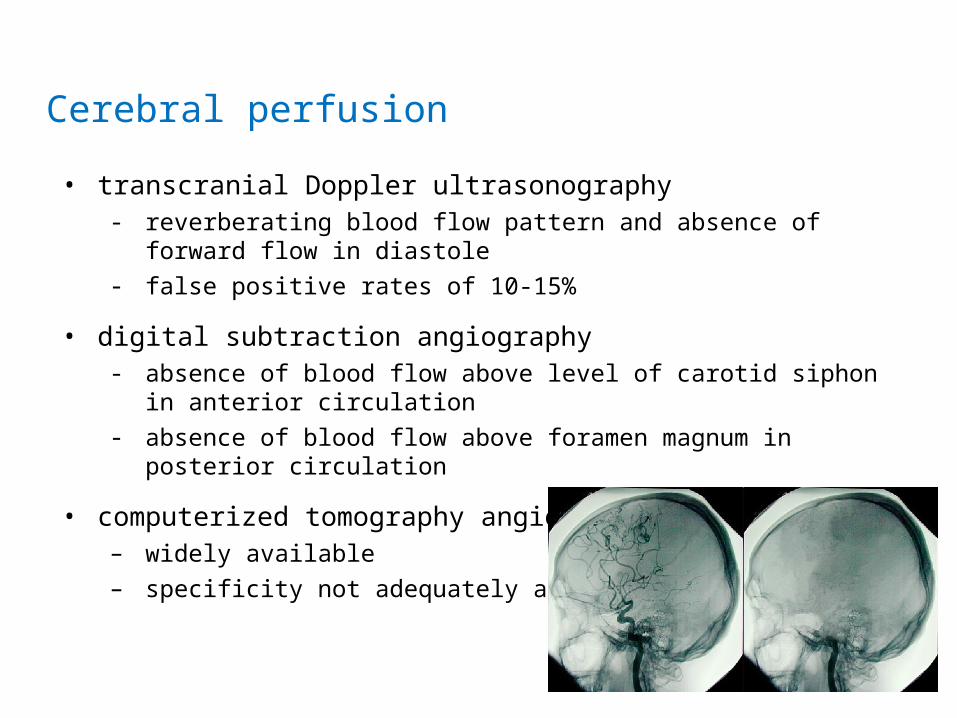
• transcranial Doppler ultrasonography- reverberating blood flow pattern and absence of forward flow in diastole- false positive rates of 10-15%
• digital subtraction angiography- absence of blood flow above level of carotid siphon in anterior circulation- absence of blood flow above foramen magnum in posterior circulation
• computerized tomography angiography – widely available– specificity not adequately assessed
Cerebral perfusion
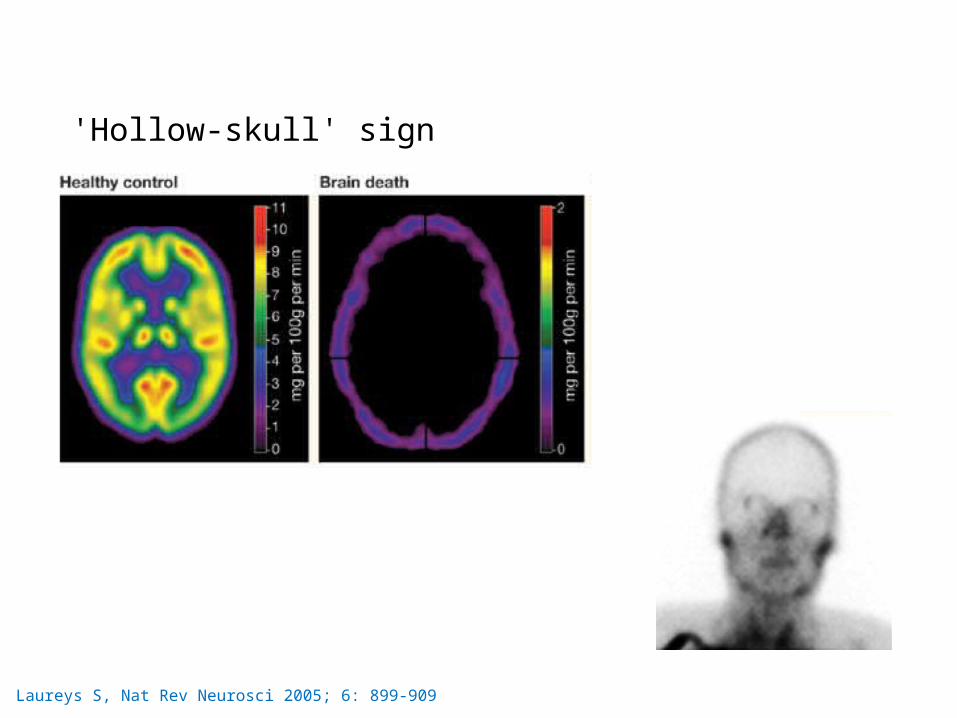
Laureys S, Nat Rev Neurosci 2005; 6: 899-909
'Hollow-skull' sign
Confirmatory tests are residua from earlier days of refining comatose states. A comprehensive clinical examination, when performed by skilled
examiners, should have perfect diagnostic accuracy.
• brain dead patients are ideal multi-organ donors– inescapable relationship between brain death practices and the
development of organ donation and transplantation
• a person should be declared (brain) dead because it is in their best interests for their death to be confirmed– withdrawal of treatment (including mechanical ventilation) which
cannot conceivably be of benefit to them
Brain death and organ donation
• major international differences
• survey of brain death protocols in leading neurology departments in the US showed a shocking lack of standardization
– apnea test not required in one
The need for standardization
• major international differences
• survey of brain death protocols in leading neurology departments in the US showed a shocking lack of standardization
– apnea test not required in one
• need for greater uniformity is obvious– national /international standards
The need for standardization
• the concept of brain death is clear
• the difference between whole brain and brainstem formulations is overstated
• proving irreversibility requires clinical acumen and experience
• the clinical diagnosis is robust, one examination is sufficient and ancillary tests are not strictly necessary
• the diagnosis of brain death is in an individual’s best interests irrespective of whether or not they become an organ donor
There should be no controversy

THANK YOU!