CORNEAL SURGERY
CORNEAL SURGERY
SHREESAGAR.B.V44247TH term
Corneal Physiology
Transparent, dome shaped, outermost layer that covers the front
of the eye.Provides greatest amount refractive power to the
eye.Avascular, relies on atmosphere for oxygen and aqueous humor
for its nutritional needs.Corneal surface is kept smooth by
constant moistening action of tears.
Layers of Cornea1 Epithelium (55m).Stratified squamous
epithelium,5-6 layersIt maintains stromal dehydration.2 Bowmans
Membrane(12m):acellular,collagen fibrils,resistant and do not
regenerate3 Stroma (470m)Collagen fibers arrangement are
responsible for corneal strength, optical characters.90%thickness.4
Duas Membrane5 Descemets Membrane: highly resistant and
regenerates.6 Endothelium (5m)It contains single layer of polygonal
cells.
3
Corneal surgery
Corneal refractive surgeryIt is of two types:>Flap surgery:
-Automated Lamellar Keratoplasty -LASIK >Surface surgery: -PRK
-LASEK -epi LASIK
FLAP SURGERYALK The surgeon uses a instrument called a
microkeratome to cut a thin flap of the corneal tissue.The flap is
then lifted like a hinged door and target corneal tissue is removed
from microkeratome and flap is replaced
LASIKLamellar assisted in situ keratomileusisMicrokeratome or
femtosecond laserProcedure is similar to ALKThe corneal tissue here
is removed through excimer laser
LASIK
Advantages:Pain free recovery.Quick restoration of
eyesight.Better result for severe short sight.
Disadvantages:Dry eyes.Halos, starburst.Loss of contrast
sensitivity. Thick corneal flap (100-180 microns).
SURFACE PROCEDURESIt differs from flap method wherein only the
epithelium of the corneal epithelium is ablated rather than the
partial thickness of the stroma.
PRK-Photo Refractive KeratectomyIt is a outpatient procedure
performed with local anesthetic eye drops.it is atype of refractive
surgery which reshapes the cornea by removing microscopic amount of
tissue.Done using excimer laser.Used to correct mild to moderate
Myopia.Hyperopia.Astigmatism.Advantages:Highly accurate for
myopia.80% patients have 20/20 visionDisadvantages:Mild discomfort
including minor eye irritation.Dry eyes.
LASEKLaser assisted sub epithelium keratomileusisEpithelium is
kept intact here.The surgeon uses an alcohol solution to loosen
then lift a thin layer of the epithelium with a trephine blade.
Advantages:No flap complications.Causes less dry eyes than
LASIK.Finer trephine blade is used instead of microkeratome.Good
for patient with thin cornea.Disadvantages:May cause more pain and
discomfort than LASIK.Dry eyes.Longer recovery time than LASIK.
Epi-lasikSimilar to LASEK.Epi-keratome is used rather than a
trephine blade and alcohol
Epi-LasikAdvantages:Less complications to corneal
nerves.Disadvantages:Dry eyes.Poor night vision.
Newer techniques:C-TEN(Customised Transepithelial No-touch
surgery)
CORNEAL TRANSPLANT SURGERYIt is a corneal grafting procedure
called KERATOPLASTY.The procedure involves replacing the damaged
recepients corneal tissue by clear donor corneal
tissue.Types:Lamellar KeratoplastyPenetrating Keratoplasty
indicationsOptical: to improve visual acuity in conditions such
as pseudophakic bullous keratopathy,keratoconus,corneal
degeneration etc.Tectonic/Reconstuctive: to preserve corneal
anatomy in cases of thinning of stroma and as in descemetoceles or
reconstruction of eye as after corneal perforation.Therapeutic: to
remove inflamed corneal tissue unresponsive to drugs.Cosmetic: to
improve patients appearance.
Donor corneaThe donor cornea is removed within 6 hours of death
and stored under sterile conditions.Evaluation:biomicroscopic
examination of whole globe is done before considering the media
storage.Corneal transplants are rarely a failure,as it is
avascular.
Methods of preservationShort term: 48 hours,whole globe is
preserved at 4c in moist chamber.Intermediate term:2 weeks,in MK
media(Mc-Carey Kaufman) or Optisol mediumLong term:35 days,by organ
culture method
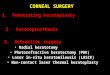
Surgery technique
A-Normal cornea
B-Penetrating Keratoplasty
C-Deep Anterior Lamellar Keratoplasty
D-Descemets Stripping Automated Endothelial Keratoplasty
E-Descemets Membrane Endothelial Keratoplasty
Possible complications of surgeryGraft RejectionWound Separation
Loose suturesAstigmatism InfectionSecondary glaucomaIris
prolapseFlat anterior chamber
Signs of graft rejection
R S
V
PRednessSensitivity to lightVision ChangesPain
A loose suture may give a foreign body sensation.Wound
separation may lead to prolapse ,infection many complications
secondarily.ASTIGMATISM: it can occur as a result of distorted
shape of the graft(oblong shaped). it is usually treated by
contacts or spectacles.
After surgeryFollowing surgery, your eye most likely will be
red, irritated, and sensitive to light. You may experience
increased tearing and a slight discharge.Discomfort can be
controlled with medication eye drops.
Eye drops are used to reduce inflammation and graft
rejection.Activities are restrained to prevent any blow to eye.Your
eye will be covered with a patch the day of surgeryYour surgeon
most likely will remove the patch at your follow-up appointment the
next day. You must wear the patch and shield over your eye while
sleeping or showering
Vision after surgeyVision usually is blurred after surgery. It
gradually improves as healing takes place. As the eye heals and the
sutures are removed, the shape of the cornea changesTherefore, your
surgeon usually will wait between 3 and 12 months before
prescribing a new lens for your glassesIf needed, a contact lens
may be prescribed.
Penetrating keratoplasty
THANK YOUTHANK YOU