Embed Size (px)
Citation preview

11.2.2005
Dr. Uday C Ghoshal MD, DNB, DM, FACG, Rome Foundation Fellow
Professor, Department of Gastroenterology, SGPGI, Lucknow, India
PanelistsDr. M.L. Thakur, Dr. A. Chaudhary, Dr. S.A. Zargar, Dr. S.K.Sinha, Dr. Ashish
Kumar Jha, Dr. K. Mohandas, Dr. Sandeep Nijhawan

• Corrosive ingestion: A major public health issue1
• Age: Common in children (80%), accidental
• Adult: Commonly suicidal, often life-threatening
Type of ingestion2
• Western country: Most common substance is alkali
• India: Acids commoner (HCl & H2SO4, easy access)
Introduction
1.Bull World Health Organ 2009; 87: 950-954 2. Zargar SA et al, Gastroenterology 1989;97:702-707

Male, 30 y• H/O ingestion of toilet cleaning acid 6 hrs ago presented with
– Oropharygeal pain
– Increased salivation
– Dysphagia
– Odynophagia
• No history of
– Chest pain
– Epigastric pain
– Vomiting or hematemesis
• Examination
– Oral and pharyngeal mucosal burns
– Systemic examination: WNL
Case Scenario 1

Relationship between perioral & esophageal injury?
A. Such perioral injury is usually associated with severe esophageal injury
B. Such situation is related to less severe internal injury
C. There is no relationship between these two
D. Don;t know

Most commonly ingested caustic substances?
Lye: broad term used for strong alkali
Class Types Commercially available forms
Acids Sulfuric acid Batteries, industrial cleaning agents, metal plating
Oxalic acid Paint thinners, strippers, metal cleaners
Hydrochloric acid Solvents, metal cleaners, toilet and drain cleaners, antirust compounds
Alkali Sodium hydroxide Drain cleaners, home soap manufacturing
Potassium hydroxide Oven cleaners, washing powders
Sodium carbonate Soap manufacturing, fruit drying on farms
Ammonia Commercial ammonia Ammonium hydroxide
Household cleaners, household cleaners
Detergent, bleach Sodium hypochloriteSodium polyphosphate
Household bleach, cleaners, industrial detergents

Differences between alkalis and acids?
Zargar et al, Gastroenterology,1989;97:702-7
Marks IN et al, The natural history of corrosive gastritis: Am J Dig Dis 1963;8:509-24
Alkalis Acids
Ph >7 <7
Amount that can be ingested
Larger as these are tasteless and odorless
Lesser as odor is pungent and taste noxious
Depth of injury Deeper due to liquefactive necrosis and direct extension
Limited due to formation of a coagulum layer
Associated gastric injury More common Less common
Acids "lick oesophagus and bite the pyloric antrum", whereas the opposite situation results from alkaline ingestion

Zargar et alGastroenterology
1989
Broor et alGut1993
Broor et alGIE
1995
Poddar et alGIE
2001
Kochhar et alGIE
2002
Number 41 52 21 54 29
M:F 2:1 3:2 1:1 3:1 1:1
Acid 41 32 11 34 12
Alkali 0 14 10 20 17
Mean age(Years)
26 26.4 21.6 4.8± 3.4 29.3 ± 8.6
Indian studies

Caustic exposure
Necrosis
Ulceration
Fibrosis
Stricture
Carcinoma
Seconds
24-72 hours
14-21 days
Weeks-years
Decades
Perforation
Consequences of caustic injury over time?

Corrosive injury: clinical spectrum?
Zargar et al,Gastroenterology:1989;97,702-7
Clinical features Number of patients (n=41)
Oropharyngeal 30
Pain 30
Salivation 15
Laryngeal edema 2
Esophageal 27
Dysphagia 23
Odynophagia 14
Chest pain 7
Gastric 17
Epigastric pain 10
Vomiting 14
Retching 9
Hoarseness & stridor: Suggest laryngeal & epiglottic invovementDysphagia & odynophagia: Suggest esophageal involvementEpigastric pain & bleeding: Gastric involvement

Issues
• Acute management
• Gastric lavage and emesis
• Neutralization by acid or alkali
• Nasogastric tube placement
• Role of PPIs and H2 blockers
• Role of endoscopy
• Management algorithm
Case Scenario 1

UGI endoscopy following corrosive ingestion
A. Such perioral injury is usually associated with severe esophageal injury
B. Such situation is related to less severe internal injury
C.There is no relationship between these two
D.Don;t know

• Priority Airway, Breathing and Circulation (ABC)
• In unstable airway Intubation under fiberoptic laryngoscopy Tracheostomy may be required
• Gastric lavage Contraindicated
• Milk & water As antidotes or to dilute corrosive is not proven
• pH neutralization Not recommended (fear of exothermic reaction, which may increase the damage)
Corticosteroids: In patients with respiratory involvement, who should also receive broad spectrum antibiotics
Acute management?

• Routine use of NG tube: not recommended
• Best approach: NG tube placement should be individualized
Nasogastric tube
Advantage: Disadvantage:
Helpful to ensure patency of esophageal lumen
Itself leads to long stricture
Providing a lumen for dilatation of tight stricture
Nidus for infection
Worsening of gastroesophageal reflux
Delay in mucosal healing
Ramasamy K et al, J Clin Gastroenterol 2003; 37: 119-124
Kochhar R et al, Gastrointest Endosc 2009; 70: 874-880

• Efficacy of PPI and H2 blockers in minimizing esophageal injury by suppressing acid reflux: Not proven
• Cakal et al (Turkey)• Prospective cohort study• 13 patients (>18 years age)• May 2010 and June 2010
• Mucosal damage graded with Zargar grading• Given IV Omeprazole 80mg followed be 8mg/hr for 72 hours• Repeat UGIE after 72 hours and endoscopic healing was compared
Role of PPIs & H2 blockers?
Cakal B et al. Dis Esophagus 2013; 26: 22-26

Investigations in acute phase: CXR/AXR?

Investigations in acute phase: CT Scan?
Grade Features
Grade 1 No definite swelling of esophageal wall
Grade 2Edematous wall thickening without periesophageal soft tissue involvement
Grade 3
Edematous wall thickening with periesophageal soft tissue infiltration plus well-demarcated tissue interface
Grade 4
Edematous wall thickening with periesophageal soft tissue infiltration plus blurring of tissue interface or localized fluid collection around the esophagus or descending aorta
Contini S. World J Gastroenterol 2013 ; 19: 3918-30

A.Should be avoided as it does not have much
clinical utility
B.Should be done only during a period between 4
days and 7 days after ingestion
C.Should be done within 4 days
D.It only helps in prediction of prognosis but not
treatment
Endoscopy immediately following corrosive ingestion

• Cornerstone for diagnosis
• Usual recommendation1: within first 12-48 h
• Relatively safe and reliable up to 96 h2
(gentle insufflation and great caution are mandatory)
• Adequate sedation (general anaesthesia in children) is compulsory
• Endotracheal intubation: Strictly required for respiratory distress
• Contraindications: Perforation, severe supra-glottic or epiglottic burn
Endoscopy
1.Poley JW et al, Gastrointest Endosc 2004; 60: 372-3772. Previtera C et al, Pediatr Emerg Care 1990;6: 176-178
3. Tiryaki T et al, Pediatr Surg Int 2005; 21: 78-80

Endoscopic classification: Zargar’s classification
Zargar SA et al, Gastrointestinal Endosc 1991; 37: 165-169
Grade Features0 Normal
1 Superficial mucosal edema & erythema
2 Mucosal & submucosal ulceration
2 A Superficial ulceration, erosion, exudate
2 B Deep discrete or circumferential ulcer
3 Transmural ulceration with necrosis
3 A Focal necrosis
3 B Extensive necrosis
4 Perforation

Degree of injury
Number(total 81)
Complications Need for surgery
DeathsEarly Late
Grade 0 7 0 0 0 0
Grade 1 10 0 0 0 0
Grade 2a 19 0 0 0 0
Grade 2b 14 Minor bleed: 2 Stricture:10 0 0
Grade 3 31 Major bleed: 6Minor bleed: 3Perforation: 3Tracheo-esophageal fistula: 1
Stricture: 26
25-67% 4
Corrosive injury: grading and prognosis
Zargar SA et al, Gastrointestinal Endosc 1991; 37: 165-169

Management algorithm

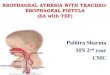
25 Y male
• H/O ingestion of corrosive 4 months ago
• Dysphagia for solids X 1 month
• No history of vomiting or hematemesis
• Examination: WNL
• UGIE: Stricture at 25 cm, scope could not
be negotiated beyond
• Barium swallow: Shown
Case Scenario 2

Incidence of stricture:1,2
•Overall- 26%-55%•Grade 2B- 71%•Grade 3- 100%
•Time period- 80% strictures within 8 week2
(but can occur as early as 3 week to as late as after 1 year)
•Ingestion of powerful caustic substances (e.g. NaOH): Severe, long-standing strictures Dramatically altered esophageal motility
Corrosive stricture
1.Zargar SA et al, Gastrointestinal Endosc 1991; 37: 165-1692.Kay M et al, Curr Opin Pediatr 2009; 21: 651-654

• Timely evaluation & dilatation: central role in achieving better
outcome
• Dilatation should be avoided from 5-21 d (high risk of perforation)
• More number of sessions needed than non corrosive strictures
• Target: At regular intervals until a lumen size of 15 mm with
complete amelioration of dysphagia (adequate dilatation)
• Afterwards, dilation repeated whenever dysphagia recurs
• Perforation rate: 0.4-32%
Endoscopic dilatation for corrosive stricture: When & how?
Doğan Y et al, Clin Pediatr (Phila) 2006; 45: 435-438Panieri E et al, Pediatr Surg Int 1998; 13: 336-340

Dilators
• There are several different types: of dilators, including –Mercury-filled, rubber Maloney dilators–Wire-guided rigid Savary-Gilliard dilators–Balloon dilators that can either be through-the-sco
pe (TTS) or wire guided –Savary bougies: More reliable than balloon
dilators in consolidated and fibrotic strictures (such as old caustic stenosis or long, tortuous strictures)

Predictors of refractory corrosive stricture?
• Long stricture• Complex stricture • Delayed initiation of treatment• Dilation with balloon rather than with SG dilator• Thick esophageal wall on CT scan or EUS

Dilation: Early or late?
Costini S et al, Dig Liver Dis. 2009;41:263-268

Role of EUS & CT in prediction of outcome of corrosive esophageal injury
Chiu MH et al, Am J Gastroenterol 2004; 99: 851-854

How to augment result of endoscopic dilation?
• Nd-YAG LASER• Intra-lesional injection with various substances• Prosthesis placement• Endoscopic stricture incision

• Utility of corticosteroid: controversial
• Meta-analysis: No benefit for stricture prevention
• Systemic administration of steroids: ineffective(especially in grade 3
corrosive injury)
• Intra-lesional triamcinolone injections have been proposed to
prevent strictures, but optimal dose, frequency, and best application
techniques are still to be defined
• Triamcinolone: prevents cross-linking of collagen
Role of steroids in prevention & management of corrosive stricture
Systematic pooled analysis of 50 years of human data: 1956-2006.Clin Toxicol (Phila) 2007
Siersema PD et al, Gastrointest Endosc 2009; 70:1000-1012

Methods:
•N:71 (mean age 42.39 yrs; range, 13-78 yrs) with benign esophageal
strictures (corrosive 29, peptic 14, anastomotic 19, radiation-induced 9)
•All were managed: Endoscopic dilation (by using over-the-wire polyvinyl
dilators) & intra lesional triamcinolone injection
•At each session – 4 injections (4 quadrants) at proximal margin of stricture
and another 4 injections into strictured segment

• Intervals, & frequency of dilations and Periodic dilation index (number of dilations required/per month) were calculated before and after injections
Results: Mean number of sessions of injection: 1.4 (0.62)
Intra lesional triamcinolone augment the effects of dilation in benignesophageal strictures
Before injection After injection
Mean duration of treatment (month) 10.9 (range 1-120) 8.1(range 3-30)
Mean number of dilatation required 9.67(range 1-70) 3.8(range 1-16)
Periodic dilatation index 1.24(range 0.13-3.16) 0.5(range 0-2)

Periodic dilation index (dilation needed/mo) in relation to etiology of benign stricture
Kochhar R. Gastrointest Endosc 2002;56:829-34.

•Chemotherapeutic agent with DNA crosslinking activity
•Valuable in preventing strictures (either injected/ topically)
•Deleterious adverse effects (due to systemic absorption)
•Risk of secondary long term malignancy
•A recent systematic review: encouraging results in the long term
•Prospective studies are clearly mandatory to determine the most effective
concentration, duration and frequency of application
Mitomycin C for corrosive stricture
Berger M et al Eur J Pediatr Surg. 2012 Apr;22(2):109-16

•Introduction: • The topical application of Mitomycin C to the site of stricture: limited study
Systematic review in persistent esophageal stricture
Method and Results: •11 publications including 31 cases•Underlying cause of stricture: Caustic ingestion-19 (61.2%), esophageal surgery-7 (22.6%) and others-5 (16.2%)•Median age: 48 months (range 4 -276 months)
•In majority cases: Cotton soaked in solution applied endoscopically •Application: 1 to 12 times within intervals from 1 to 12 weeks
Mitomycin C in the therapy of recurrent esophageal strictures
Berger M et al Eur J Pediatr Surg. 2012 Apr;22(2):109-16

•Concentrations of Mitomycin C: Varied considerably (0.1-1 mg/Ml)•Mean follow-up- 22 months (range 6-60 months) Complete relief- 21 (67.7%) Partial relief- 6 (19.4%) No response- 4 •No adverse effects were reported
Conclusions:•The short-term results of topical Mitomycin C for refractory esophageal
stricture: Encouraging
•Prospective studies are mandatory to determine the optimal time points, dosage, and modalities of treatment before a recommendation
Mitomycin C in the therapy of recurrent esophageal strictures

Role of stents in corrosive stricture

• Design: Silicone rubber stent or Polyflex stents
• Helpful in preventing stricture formation, but efficacy < 50% with a
high migration rate (25%)
• Patient selection: challenging with concern of hyperplastic tissue • Home-made poly-tetra-fluoroethylene stents: 72% efficacy at 9-14
month, similar to home-made silicone stents
Corrosive stricture: prevention and management
Broto J et al, J Pediatr Gastroenterol Nutr 2003; 37: 203-206 Atabek C et al, J Pediatr Surg 2007; 42:636-640

• Success rate - 45% at 53 months• Migration rate - 10%• Significant hyperplastic tissue response
• Stent integrity & radial force maintained for 6-8 weeks (pH dependent)• Stent degradation occurs in 11-12 weeks (pH dependent)• No need for removal procedure
• Issues: Cost
Limited experience
Biodegradable stents (poly-L-lactide or polydioxanone)
Tokar JL et al , Gastrointest Endosc 2011; 74: 954-958 Repici A et al , Gastrointest Endosc 2010; 72: 927-934

Approved stents
Yim HB. Annals Palliative Medicine 2014; 3.

F, 30 y
• Consultation received from Surgical Gastroenterology for a patient with
dysphagia
• History of corrosive ingestion in an attempt for suicide 2 y ago
• Barium swallow then revealed long esophageal stricture with severe
gastric injury
• Underwent surgical management for the stricture with colon inter-
position
Case Scenario 3

Barium swallow and meal

A.Dilation with SG dilator is a safe option
B.TTS balloon is a safe option
C.Neither of these is safe
D.This is an absolute indication in which both
esophageal and gastric lesion should be
treated surgically
Endoscopic esophageal dilation in patients with co-existing cicatrizing gastric injury

F, 30 y
• Currently, recurrent dysphagia
• Esophagogastroduodenoscopy: Anastomotic stricture
• Examination: Poorly nourished, Pallor++
• Anemia- not responding to oral iron
• How to manage?
Case Scenario 3 (Contd.)
Work-upHb 7.4 Gm %MacrocyticNormal Iron profileMCV 112 FlS. Vitamin B12- 80 pg/ml
Follow-up

Late complication of corrosive ingestion: Esophageal cancer
• Incidence: 2-30% after 1-3 decades• Shortest time 1 y after ingestion• Some studies overestimated?• Both adenocarcinoma & squamous cell carcinoma• In strictured segement• Bypass surgery does not prevent• Endoscopic screening recommended

Conclusions
• Corrosive ingestion, particularly of acids, is common in India
• Early endoscopy is helpful in prognostication
• Acute management is important for outcome in severe injury
• Late outcome of esophageal stricture can be managed by endoscopic dilation
• There are novel methods to manage refractory stricture
• Surgical management play important role both in early and late stages