Embed Size (px)
Citation preview
BY
Professor of Internal MedicineZagazig University
2015
DR MONKEZ M YOUSIF
CPR
OBJECTIVES• Recognise cardiac arrest.
• How to perform chest compression and rescue breathing.
• Differentiate between shockable and
non- shockable rhythm.
• Understand Principal Drugs (Atropine–Adrenaline-
Amiodarone).
• Case presentations.

CASE 1
• You find a 72-year-old man lying unresponsive in
a restroom of a local airport. He is alone, and
you don't know how long he has been
unconscious. You speak loudly, trying to wake
him up, and you shake him; he continues to be
unresponsive.
What should be your sequential response in
this situation?
CASE 2
• A 56-year-old woman is found pulseless in her
room at a local hospital. The nurse calls "code
blue," and you are the first doctor responding.
• The nurse has started CPR, and the patient has a
patent I.V. line. After 2 minutes, the patient is still
pulseless. A defibrillator has now been brought to
the room.
What is the best intervention to take next in the
care of this patient?
What is CPR• Cardiopulmonary Resuscitation (CPR) consists of
chest compression and mouth-to-mouth respiration .
• CPR allows oxygenated blood to circulate to vital
organs such as the brain and heart.
• CPR can keep a person alive until more advanced
procedures (such as defibrillation - an electric shock
to the chest) can treat the cardiac arrest.
Cardio Pulmonary Resuscitation
• BLS – basic life support.
• ACLS – advanced cardiac life support.
Causes of Cardiac Arrest
8
Causes of cardiac arrest
Cardiac
Extracardiac
Primary lesion of cardiac muscle leading to the progressive decline of contractility, conductivity disorders, mechanical factors
All cases accompanied with hypoxia

9
Causes of circulation arrest
Cardiac• Ischemic heart disease • Arrhythmias of different
origin and character• Electrolytic disorders• Valvular disease• Cardiac tamponade• Pulmonary artery
thromboembolism• Ruptured aneurysm of aorta• Hypertrophic obstructive CM
Extracardiac• Airway obstruction• Acute respiratory failure• Shock• Embolisms of different origin• Drug overdose• Electrocution• Poisoning
Cardiac Arrest
• Brain damage begins 4 - 6 minutes after
cardiac arrest
• Brain damage becomes irreversible in
8 - 10 minutes
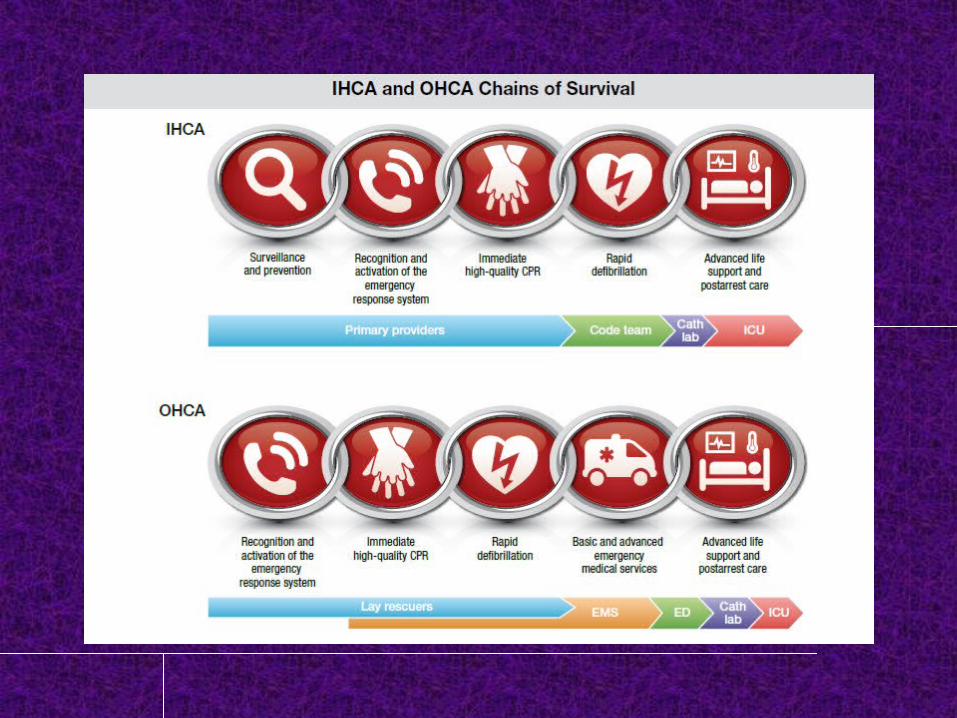
Chain of Survival for OHCA
Andrew H. Travers et al. Circulation. 2010;122:S676-S684
1. Immediate recognition and activation 2. Early CPR 3. Rapid defibrillation 4. Effective advanced life support 5. Integrated post-cardiac arrest care
Basic life support (BLS)
Implies that no equipment is employed other than a protective device.
Consists of chest compression mouth-to-mouth respiration and
Steps of CPR (3 Cs)1) Check
• Scene• Injuries• Consciousness
2) Call• EMS
3) Care• C-A-B-D
CHECKEstablish Unresponsiveness
• Tap victim on shoulder and ask “Are you OK?”
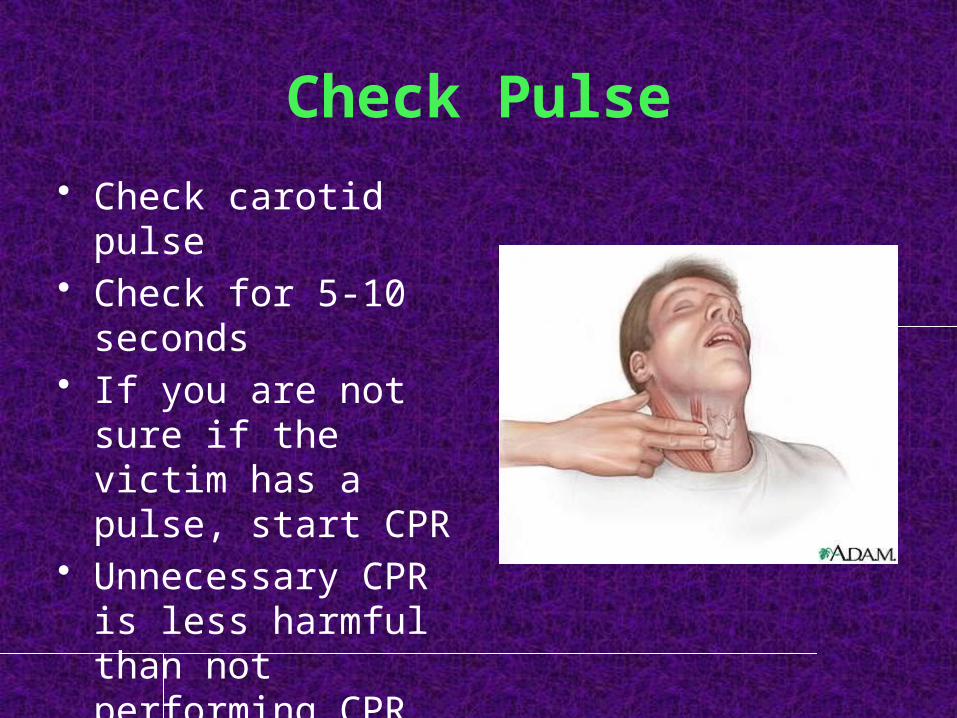
Check Pulse• Check carotid pulse• Check for 5-10
seconds• If you are not sure if
the victim has a pulse, start CPR
• Unnecessary CPR is less harmful than not performing CPR that is needed
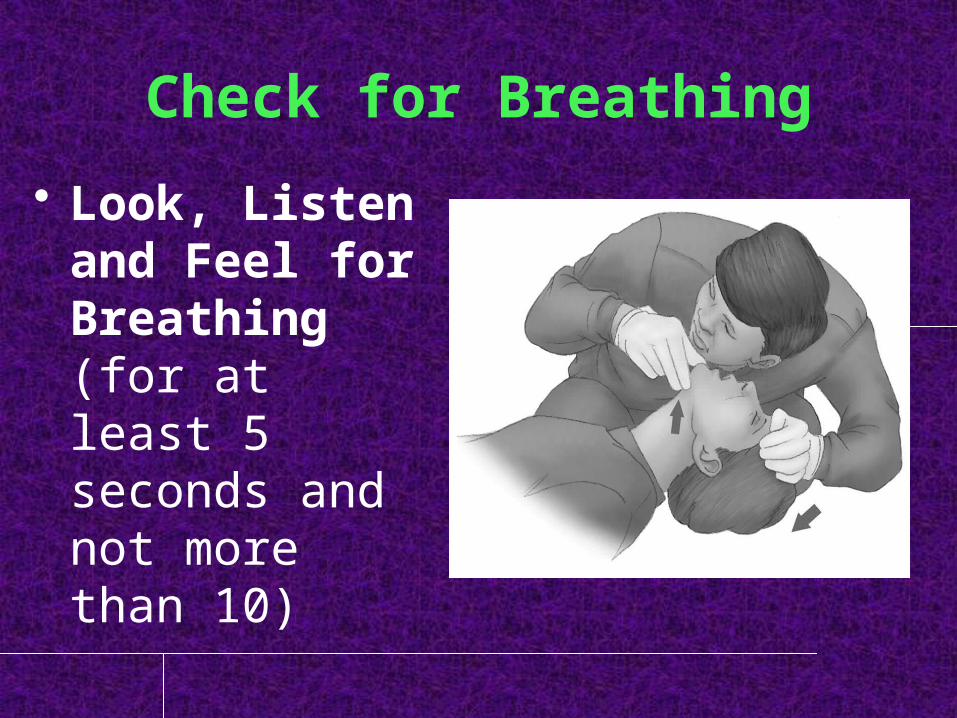
Check for Breathing• Look, Listen
and Feel for Breathing (for at least 5 seconds and not more than 10)
CALLActivate EMS
• If victim is unresponsive, activate EMS immediately
• Instruct a bystander to call• If you are alone, you must activate EMS before performing any other step• If unresponsive & victim is breathing, place in recovery position
Patient unresponsive with no breathingStart CPR
C-A-B-D
CARE

CAREHand Placement for Chest Compression• Place the heel of one
hand in the center of the victim’s bare chest between the nipples
• Put the heel of your other hand on the top of your first hand
• Straighten your arms and position your shoulders directly over your hands
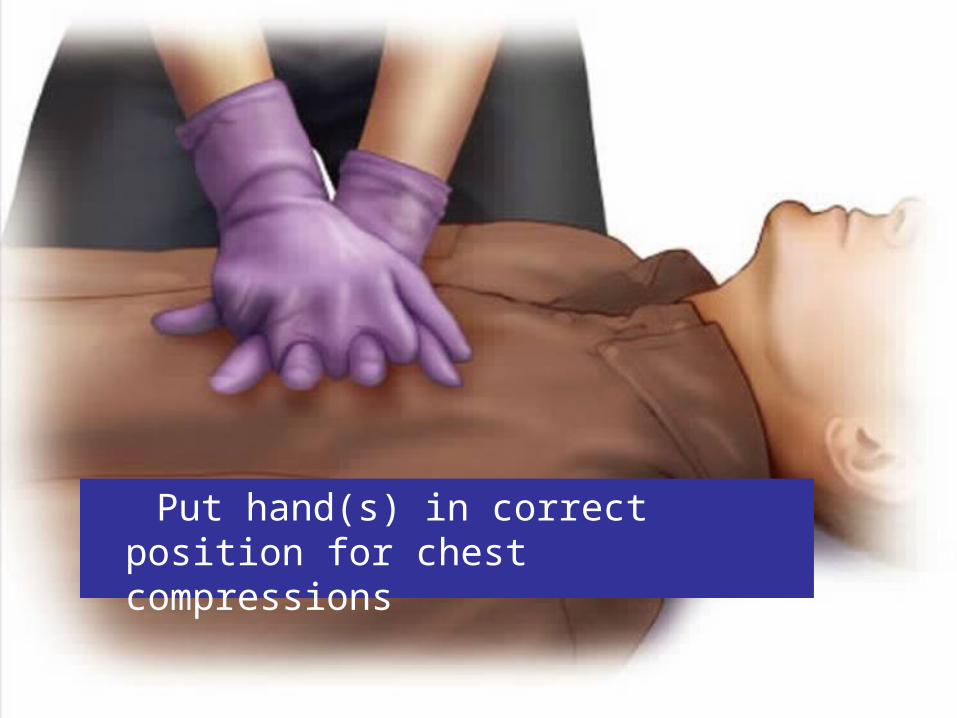
Put hand(s) in correct position for chest compressions
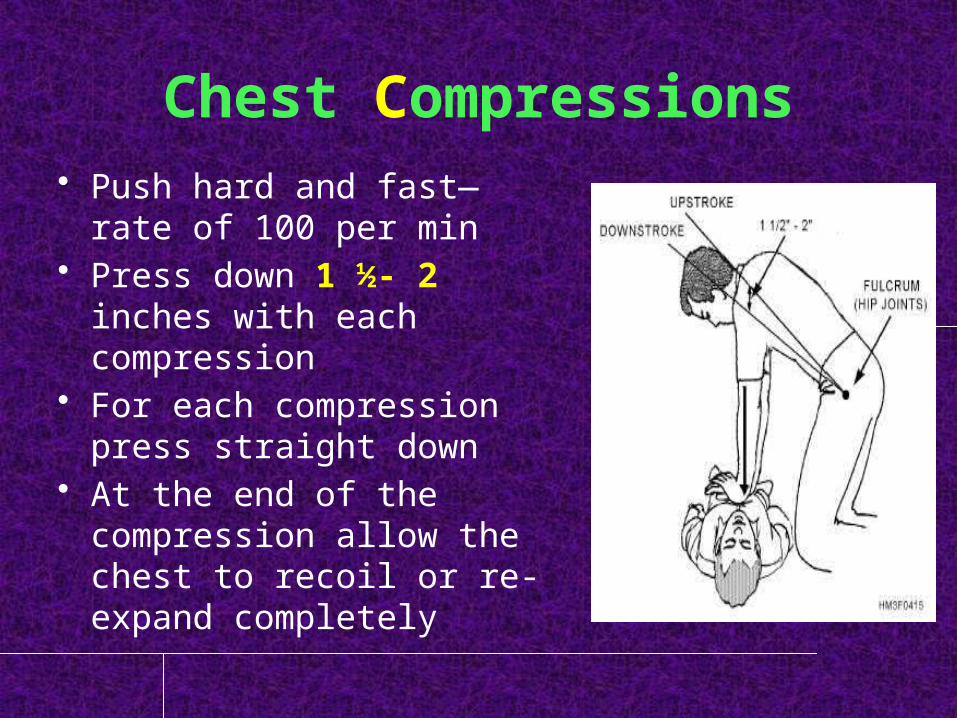
Chest Compressions• Push hard and fast—rate
of 100 per min• Press down 1 ½- 2 inches
with each compression• For each compression
press straight down• At the end of the
compression allow the chest to recoil or re-expand completely
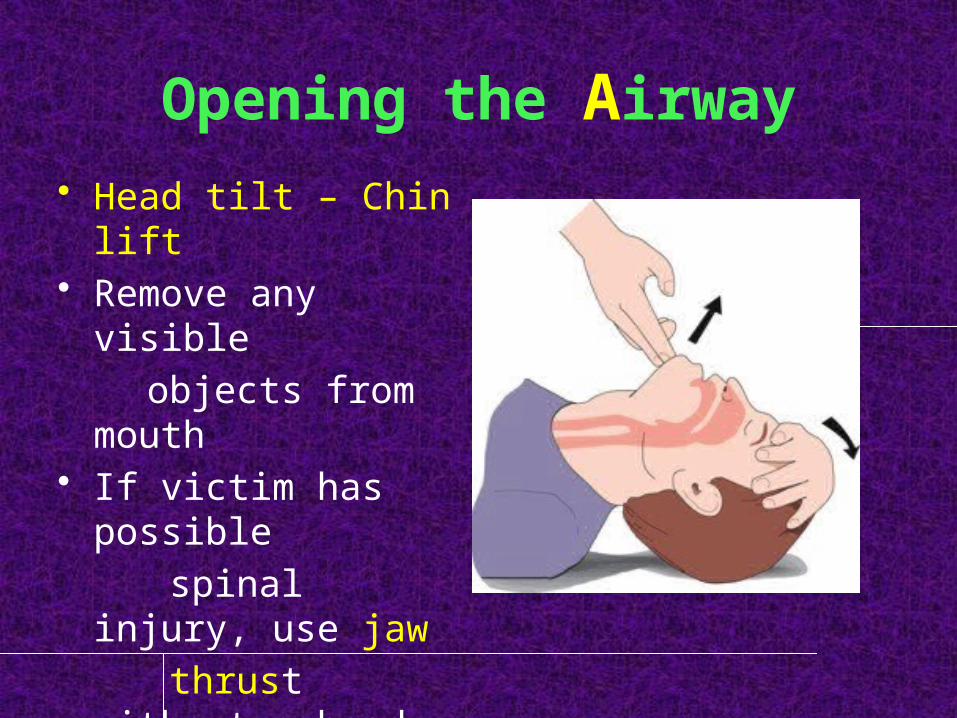
Opening the Airway• Head tilt – Chin lift• Remove any visible objects from mouth• If victim has possible spinal injury, use jaw thrust without a head
tilt
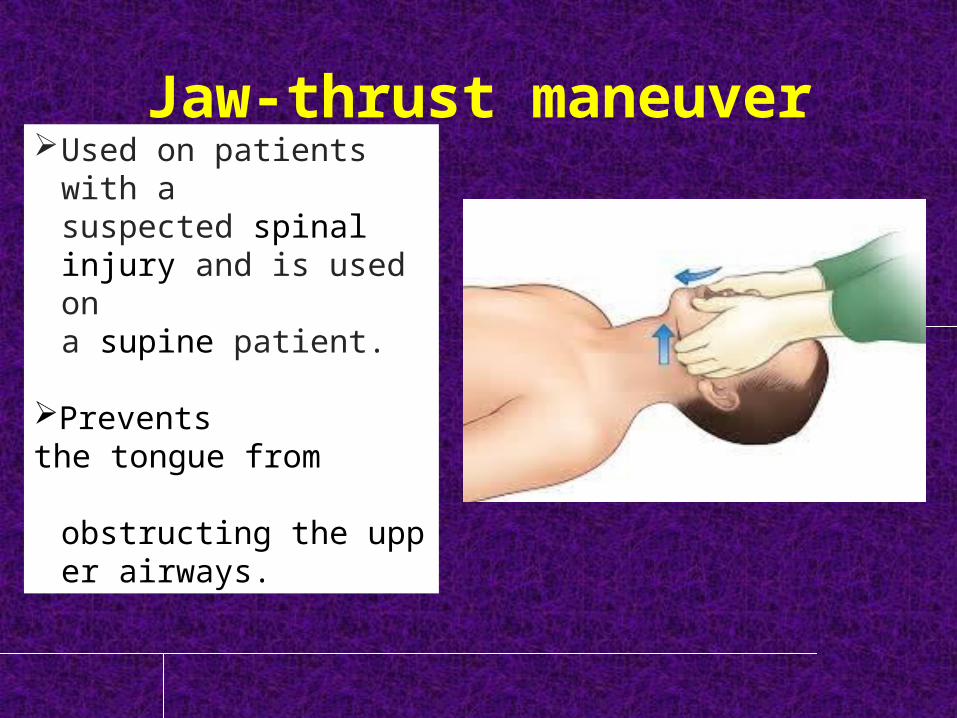
Jaw-thrust maneuver
Used on patients with a suspected spinal injury and is used on a supine patient.
Prevents the tongue from obstructing the upper
airways.

Give 2 Breaths• Pinch the nose closed with
your thumb and index finger• Take a regular breath and
seal your lips around the victim’s mouth, creating an airtight seal
• Slowly breath air into victim’s mouth until victim’s chest rises
• Remove your mouth to let the air come out
• Repeat one more breath
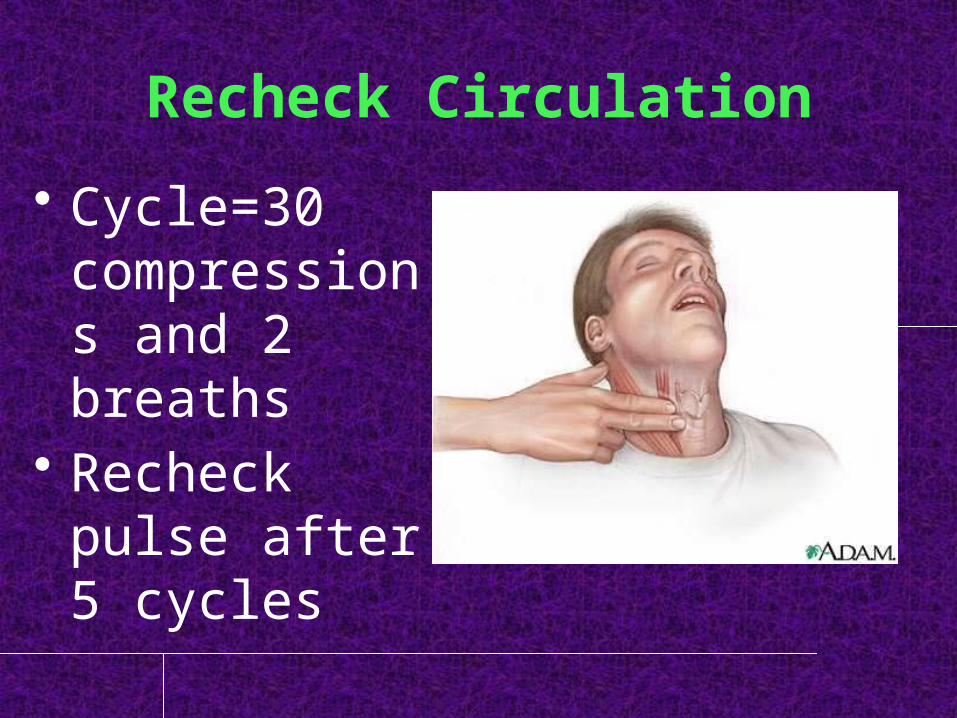
Recheck Circulation• Cycle=30
compressions and 2 breaths
• Recheck pulse after 5 cycles
During CPR
• Push hard & fast (100-120/min)
• Compressions to relaxation ration 50:50
• Ensure full chest recoil
During CPR• Avoid hyperventilation• Secure airway & confirm placement• Rotate compressors every 2min with
rhythm checks• After an advanced airway is placed,
rescuers no longer deliver “cycles” of CPR. Give continuous chest compressions without pause for breaths. Give 6-8 breaths/min. check every 2min.
CPR Pushing on the Chest
• Sometimes you may hear a cracking sound.
• The sound is caused by cartilage or ribs cracking.
• Even if this occurs the damage is not serious.
• The risk of delaying CPR or not doing CPR is far greater than the risk of a broken rib.
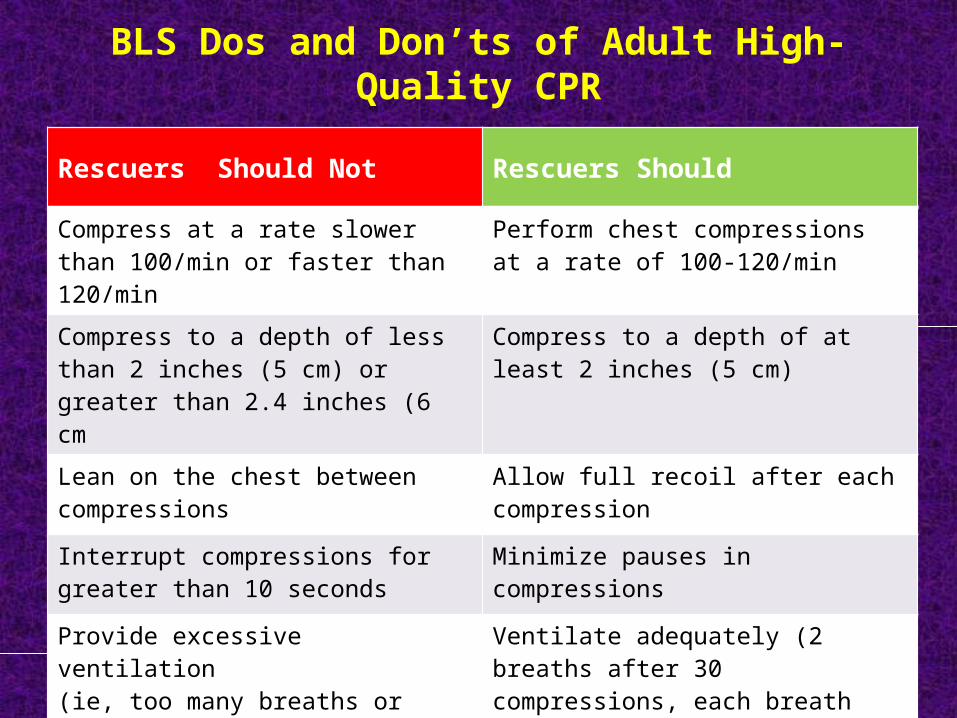
BLS Dos and Don’ts of Adult High-Quality CPR
Rescuers Should Not Rescuers Should
Compress at a rate slower than 100/min or faster than 120/min
Perform chest compressions at a rate of 100-120/min
Compress to a depth of less than 2 inches (5 cm) or greater than 2.4 inches (6 cm
Compress to a depth of at least 2 inches (5 cm)
Lean on the chest between compressions
Allow full recoil after each compression
Interrupt compressions for greater than 10 seconds
Minimize pauses in compressions
Provide excessive ventilation(ie, too many breaths or breaths with excessive force)
Ventilate adequately (2 breaths after 30 compressions, each breathdelivered over 1 second, each causing chest rise)
When to Stop CPR• Victim is revived• Replaced by another
equally trained person or physician assumes responsibility
• Exhaustion• Scene becomes unsafe• Physician direction to
stop
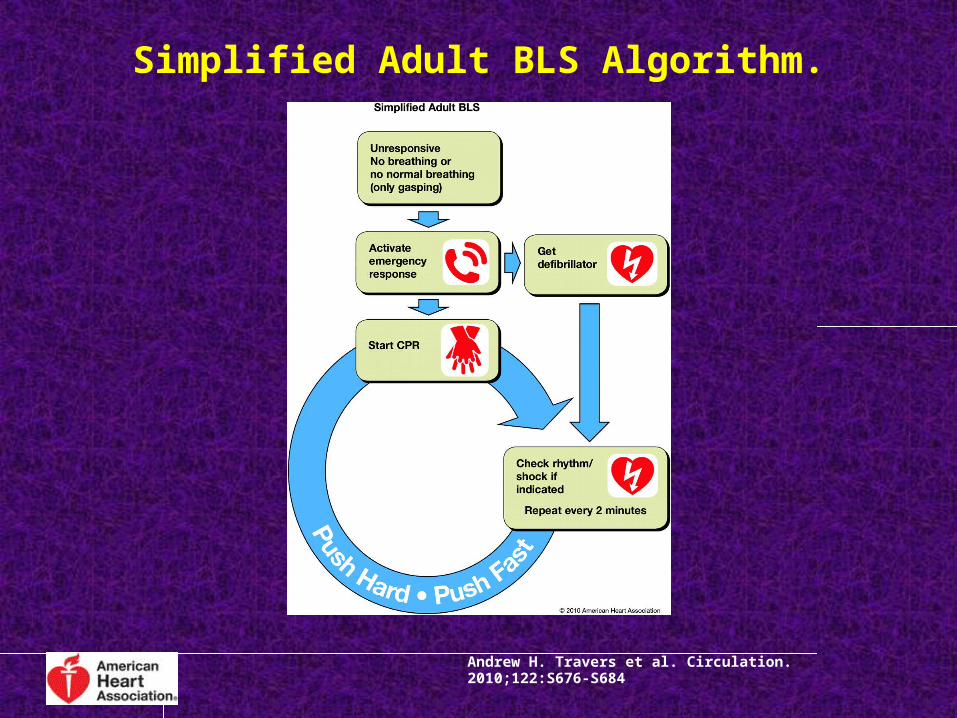
Simplified Adult BLS Algorithm.
Andrew H. Travers et al. Circulation. 2010;122:S676-S684
In Hospital Resuscitation
• In hospital resuscitation differs in ;
- location (monitored),
- training of the first responder,
- number of responders,
- equipment available and
- resuscitation team.
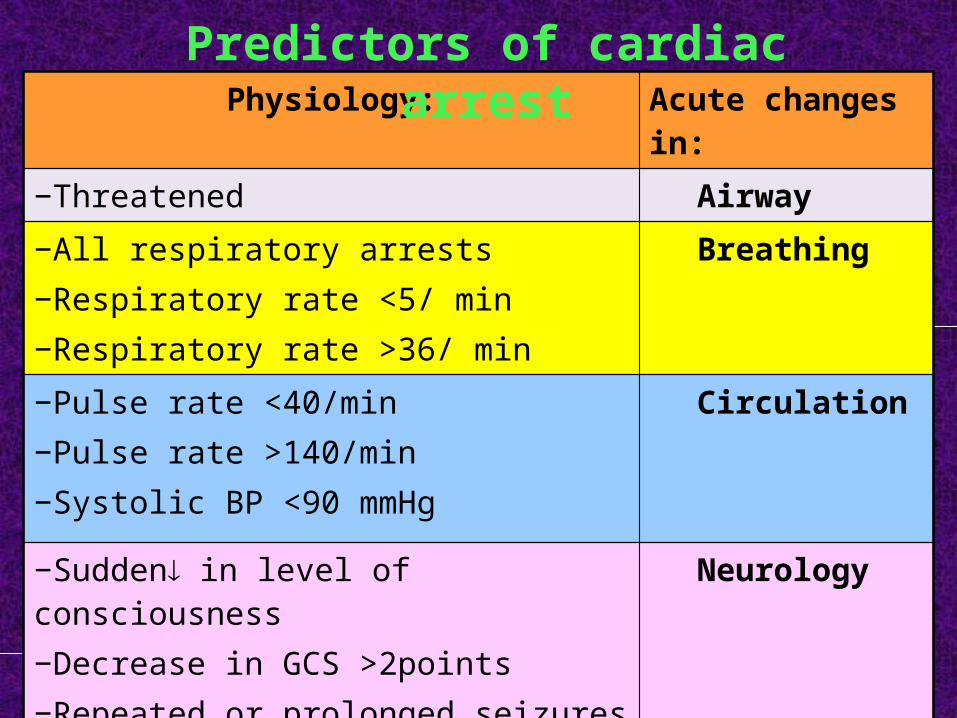
Physiology: Acute changes in:−Threatened Airway−All respiratory arrests−Respiratory rate <5/ min −Respiratory rate >36/ min
Breathing
−Pulse rate <40/min−Pulse rate >140/min−Systolic BP <90 mmHg
Circulation
−Sudden in level of consciousness−Decrease in GCS >2points−Repeated or prolonged seizures
Neurology
−Any patient - causing concern who does not fit the above criteria
Other
Predictors of cardiac arrest
Sequence for collapsed patient in a hospital
1) Ensure personal safety:– Your personal safety and that of resuscitation
team members is the first priority. – Check that the patient’s surroundings are safe. – Put on gloves as soon as possible, eye
protection and face mask may be necessary.

2) Check the patient for a response: If you see a patient collapse or apparently unconscious, -shout for help -assess response by gently shaking the victim and ask loudly, "Are you OK?“
3) If he has a pulse or signs of life: ABCDE
4) If he has no pulse or signs of life:call the resuscitation team and start CPR immediately
5) If he is not breathing and has a pulse ( respiratory arrest): keep ventilation and check for a circulation / 10 breath.
6) If the patient has a monitored and witnessed cardiac arrest:– Confirm cardiac arrest and shout for help.
– Give precordial thump if the rhythm VF/ VT
or defibrillator is not to hand immediately, and
start CPR.
– Success if done 10 sec of VF
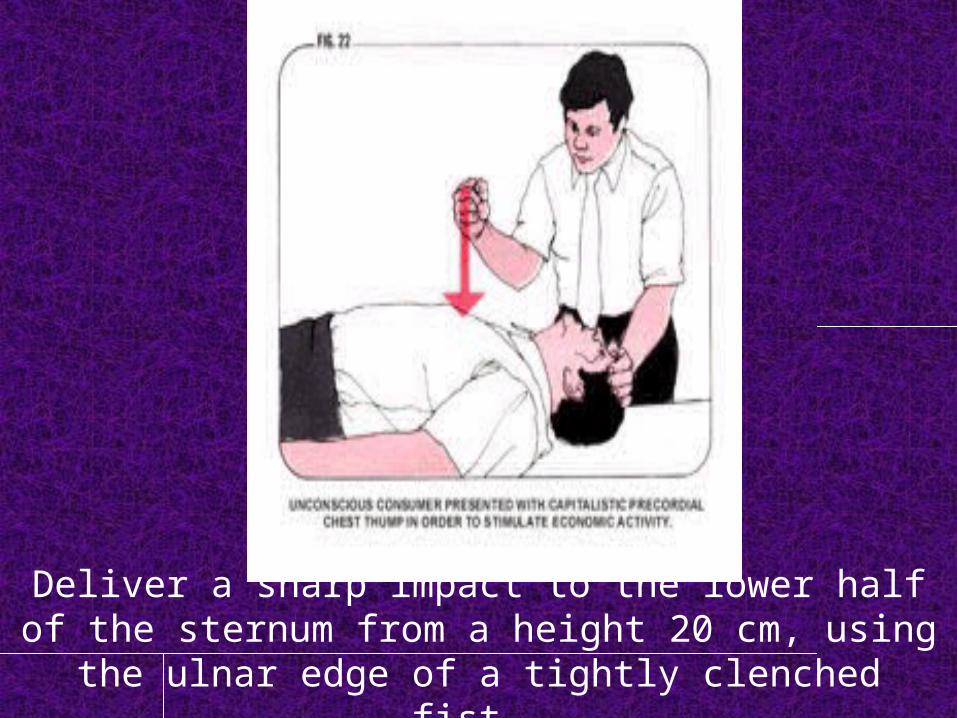
Deliver a sharp impact to the lower half of the sternum from a height 20 cm, using the ulnar edge of a tightly clenched fist.

ABCDE
Airway (A): Airway obstruction hypoxia, and risk damage to
brain, kidneys, heart, cardiac arrest and even death.
Signs of obstruction: stridor, wheeze, gurgling,
snoring..TTT: Airway clearance Airway opening maneuvers, suction,
Insertion of an oropharyngeal or nasopharyngeal airway
Tracheal intubation.
Use high concentration oxygen with sufficient flow (>10
L/ min.).

Oropharyngeal
Laryngeal mask
Tracheal tubes
Nasopharyngeal airway
Breathing (B):Diagnose and treat immediately life- threatening condition,
- acute severe asthma, - pulmonary edema, - tension pneumothorax, - massive hemothorax.
Look, listen and feel for general signs of respiratory distress;
- sweating, central cyanosis, - use of accessory ms of resp, abd breathing. - resp rate, depth, JVP, record oxygen saturation %,
TTT: give oxygen, use bag-mask or pocket mask ventilation if rate and depth of breathing is inadequate.
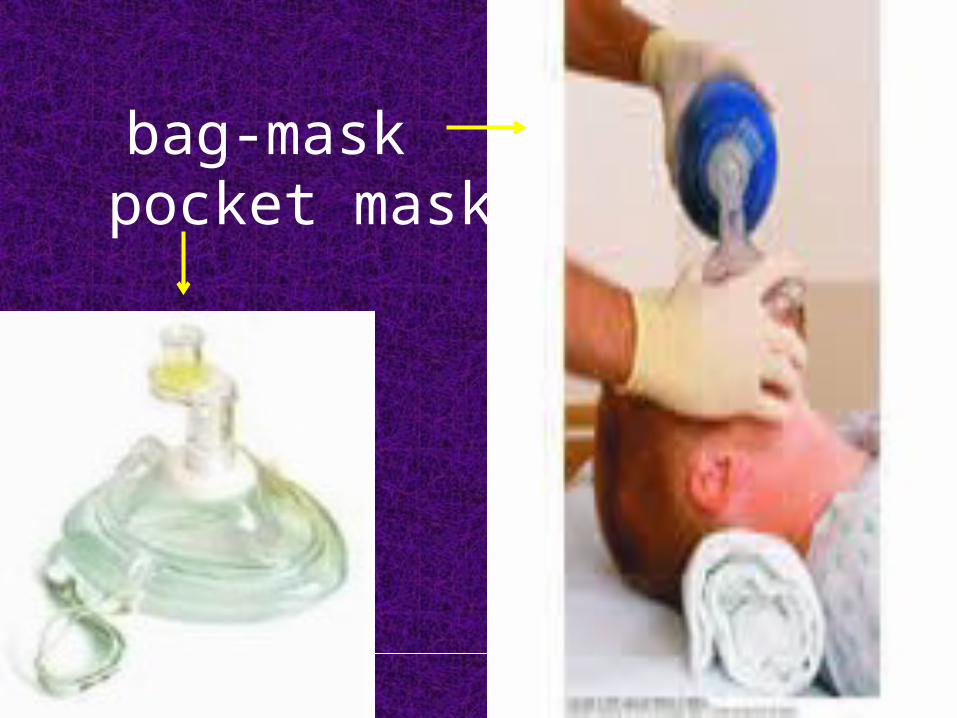
bag-mask pocket mask
Circulation (C) :Look for color and temperature of the handAssess state of veins, peripheral and central
pulseMeasure BP, auscultate the heart.Look for signs of poor cardiac output
(reduced conscious level and oliguria)Treat urgently life threatening conditions,
• cardiac tamponade, massive or continued hge, septicemic shock.
Insert IV cannula, give fluids, reassess HR and BP/5min. 12-lead ECG monitoring
Disability (D):• Common causes of unconsciousness include
− profound hypoxia, − hypercapnea, − cerebral hypo perfusion or − recent administration of sedatives or
analgesics.• Exclude or treat hypoxia and hypotension• Check drug chart and give antagonist• Measure bl gl and give glucose if<50mg/dl.• Rapid initial assessment of conscious level using
Glasgow coma scale• Nurse unconscious patients in lateral position if their
airway is not protected.
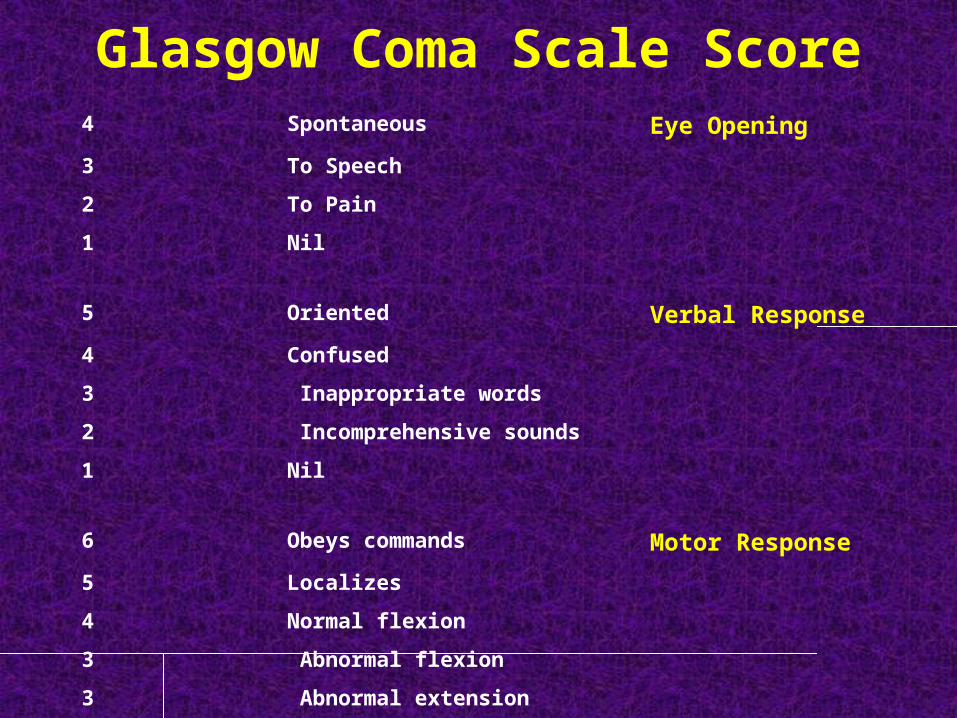
Glasgow Coma Scale Score4 Spontaneous Eye Opening3 To Speech2 To Pain1 Nil
5 Oriented Verbal Response4 Confused 3 Inappropriate words2 Incomprehensive sounds 1 Nil
6 Obeys commands Motor Response5 Localizes4 Normal flexion 3 Abnormal flexion 3 Abnormal extension 1 Nil
Exposure (E):• To examine the patient properly full exposure of
the body may be necessary. Respect the patient dignity and minimize heat loss.
• Additional information:-Take a full history-Review the patient notes and charts-Review the results of lab and radiology-Assess, treat and record response to treatment-Consider definitive treatment of underlying condition.
Problems with CPR Technique• CPR often ineffective because of poor technique
• Compressions not delivered steadily and constantly during resuscitation efforts
• Often compressions are too shallow, resulting in ineffective blood flow
• Compressions may be given at too fast a rate
Advanced Life SupportALS
Advanced Life SupportInterventions intended to achieve
1- Adequate ventilation,
2- Control cardiac arrhythmias,
3- Stabilize blood pressure and cardiac output
4- Restoration of spontaneous circulation
5- Protection of the central nervous system
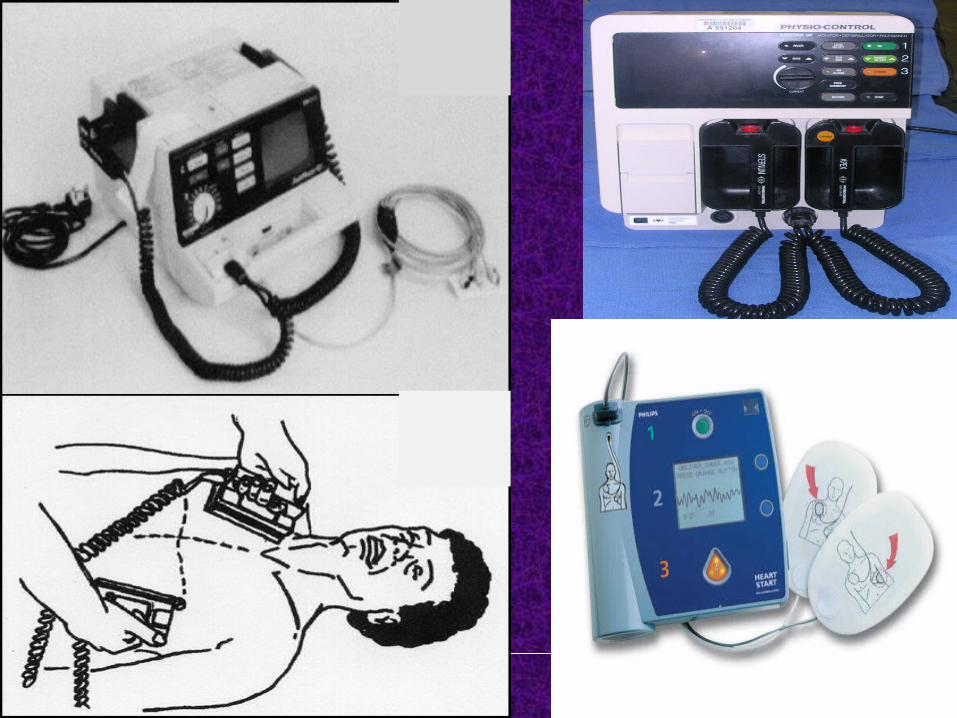
Advanced Life SupportThe activities carried out to achieve these goals include 1) Defibrillation / cardioversion and/or pacing,2) Anti-arrhythmic medications3) Intubation with an endotracheal tube, and 4) Insertion of an intravenous line.
Immediate defibrillation should precede intubation and insertion of an intravenous line; CPR should be carried out while the defibrillator is being charged.
Advanced life support algorithm:
Heart rhythms associated with CA are either:– Shockable rhythm
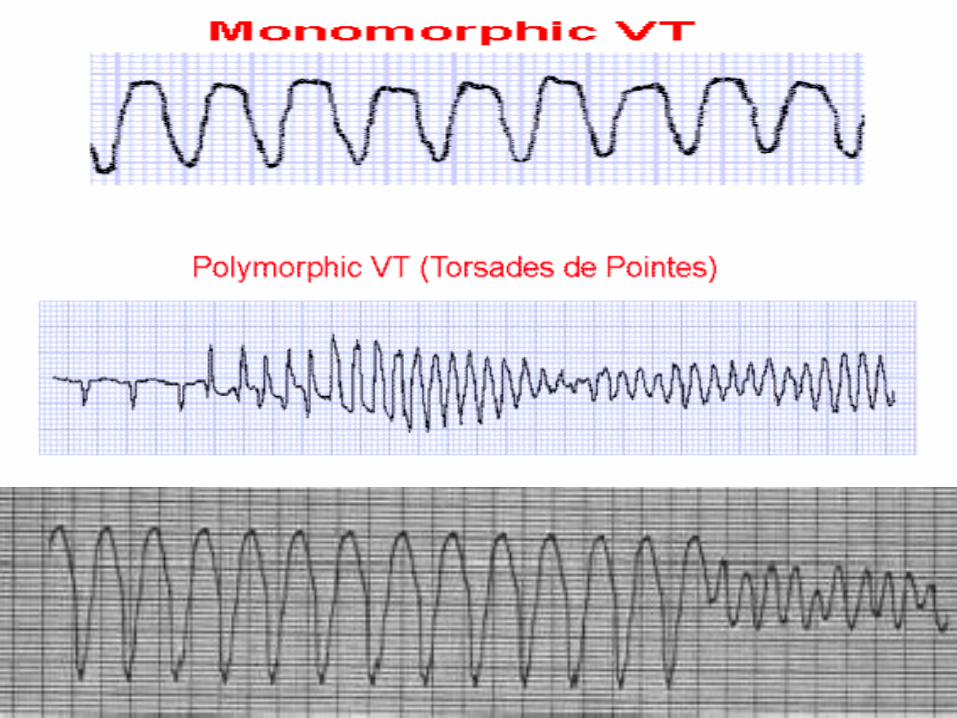
• VF • pulseless VT
– Non-shockable rhythm • Asystole • pulseless electrical activity PEA

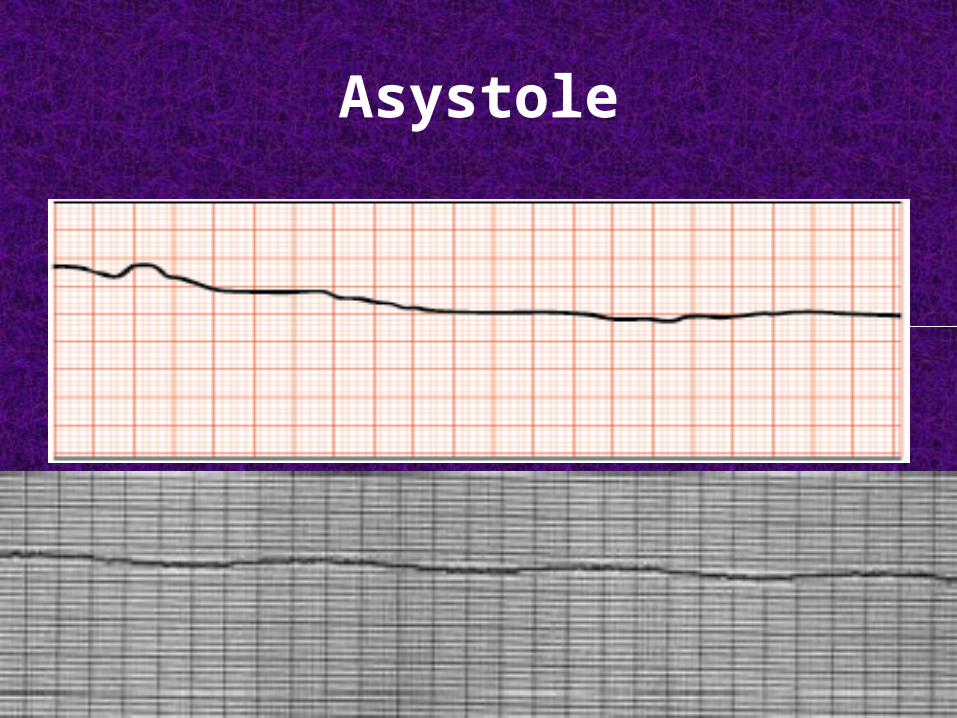
Asystole
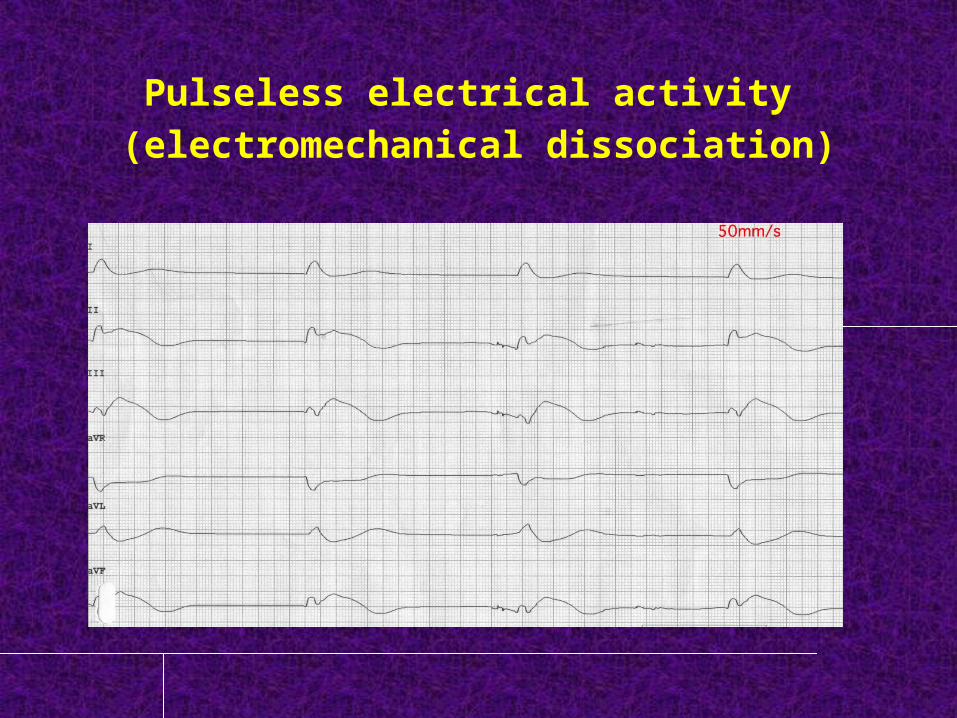
Pulseless electrical activity (electromechanical dissociation)
Treatment of shockable rhythm:
- If VF/VT is confirmed, follow the algorithm of European
Resuscitation Council ERC Guidelines for Resuscitation,
2010.
- Attempt defib. Give one chock of 150-200 biphasic or
360 j monophasic.
- Immediately resume CPR 30-2 without assessing the
rhythm or feeling the pulse for 2 min.
- If VF/VT persists give 2nd shock of 150-360 biphasic or
360 j monophasic. and resume CPR for 2 min
− If VF/VT persists give 3rd shock of 150-360 biphasic
or 360 j monophasic. resume CPR for 2 min.
− Pause briefly to check the monitor.
− If VF/VT persists give adrenaline 1 mg IV and
amiodarone 300 mg IV followed by 4th shock of 150-
360 biphasic or 360 j monophasic. resume CPR for 2
min.
− Pause briefly to check the monitor.
− Give adrenaline 1mg IV immediately before alternate
shocks ( every 3-5min).
Non-shockable rhythm – survival following CA with asystole or PEA, is
unlikely unless a reversible cause can be found and treated quickly and effectively.
• Treatment − Start CPR 30-2− Give adrenaline 1 mg IV as soon as I.V
access is achieved.− Continue CPR 30-2 until airway is secured,
then continue chest compression without pausing during ventilation.
− Recheck the rhythm after 2 min:

During CPR: consider potential causes or aggravating factors during CA.
6 H’sHypovolemiaHypoxiaHydrogen ion (acidosis)Hypo-/HyperkalemiaHypoglycemiaHypothermia
5 T’sToxinsTamponadeThrombosis (coronary or pulmonary)Tension PTxTrauma
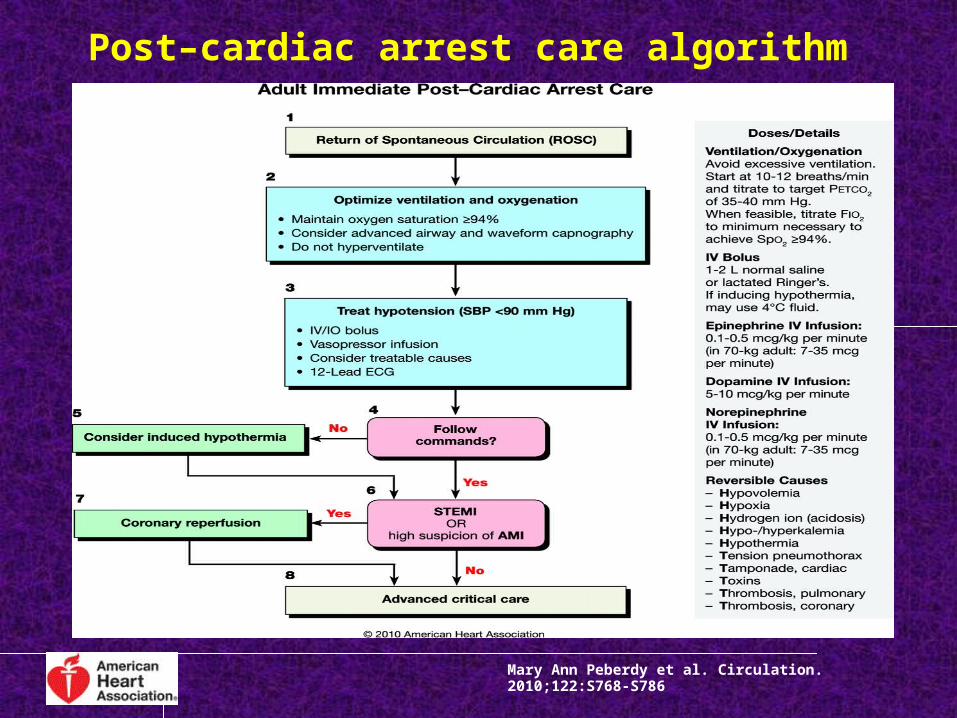
Post–cardiac arrest care algorithm
Mary Ann Peberdy et al. Circulation. 2010;122:S768-S786

CASE 1
• You find a 72-year-old man lying unresponsive in
a restroom of a local airport. He is alone, and
you don't know how long he has been
unconscious. You speak loudly, trying to wake
him up, and you shake him; he continues to be
unresponsive.
what should be your sequential response in
this situation?
• The resuscitation of an adult victim of sudden
cardiac arrest should follow an orderly sequence,
no matter where the patient collapse occurs.
• This sequence is called the chain of survival.

CASE 2
• A 56-year-old woman is found pulseless in her room at a local hospital. The nurse calls "code blue," and you are the first doctor responding. The nurse has started CPR, and the patient has a patent I.V. line. After 2 minutes, the patient is still pulseless. A defibrillator has now been brought to the room.What is the best intervention to take next in the care of this patient?
• In the chain of survival, the importance of rapid access to defibrillation cannot be ignored.
• In a patient who is dying from a shockable rhythm, the chance of survival declines by 7% to 10% for every minute that defibrillation is delayed.
• Early defibrillation is so critical that if a defibrillator is immediately available, its use takes precedence over CPR in patients with pulseless VT or VF.
• If CPR is already in progress, it should be halted while defibrillation takes place.
Questions
1. Success of any resuscitation attempt is built on:
A. high quality CPR B. defibrillation when required by the patients ECG rhythm C. neither 1 or 2 D. both 1 and 2
1. Success of any resuscitation attempt is built on:
A. high quality CPR B. defibrillation when required by the patients ECG rhythm C. neither 1 or 2 D. both 1 and 2
2) The most important algorithm to know for adult resuscitation is:
A. Bradycardia B. PEA C. Tachycardia D. Cardiac Arrest
2) The most important algorithm to know for adult resuscitation is:
A. Bradycardia B. PEA C. Tachycardia D. Cardiac Arrest
3) The systematic approach with a person in cardiac arrest should include the BLS survey and the ACLS survey?
A. True B. False
3) The systematic approach with a person in cardiac arrest should include the BLS survey and the ACLS survey?
A. True B. False
4) While conducting the BLS Survey, you should do all of the following except:
A. check patient responsiveness
B. activate emergency response system
C. open the airway
D. get an AED
4) While conducting the BLS Survey, you should do all of the following except:
A. check patient responsiveness
B. activate emergency response system
C. open the airway
D. get an AED
5) According to new 2010 Guidelines for CPR, which of the following is in the correct order for the patient with sudden cardiac arrest?
A. open airway, provide ventilations, give 30 chest compressions, attach AED as soon as possible
B. give 30 compressions, open airway, provide ventilation, attach AED as soon as possible
C. open airway, check breathing, check pulse , attach AED as soon as possible
D. none of the above
5) According to new 2010 Guidelines for CPR, which of the following is in the correct order for the patient with sudden cardiac arrest?
A. open airway, provide ventilations, give 30 chest compressions, attach AED as soon as possible
B. give 30 compressions, open airway, provide ventilation, attach AED as soon as possible
C. open airway, check breathing, check pulse , attach AED as soon as possible
D. none of the above
6) After providing a shock with an AED you should:
A. Start CPR, beginning with chest compressions
B. check a pulse
C. give a rescue breath
D. let the AED reanalyze the rhythm
6) After providing a shock with an AED you should:
A. Start CPR, beginning with chest compressions
B. check a pulse
C. give a rescue breath
D. let the AED reanalyze the rhythm
7) During CPR with no advanced airway in place the compression-to-ventilation ratio is:
A. 5:1 B. 30:2 C. 10:1 D. 20:2
7) During CPR with no advanced airway in place the compression-to-ventilation ratio is:
A. 5:1 B. 30:2 C. 10:1 D. 20:2
8) During CPR after an advanced airway is in place, which of the following is true:
A. Breaths should be synchronized with the chest compressions.
B. The goal is 20 or greater breaths per minute C. Chest compressions should be stopped while giving
breaths. D. One breath every 6 to 8 seconds should be given
8) During CPR after an advanced airway is in place, which of the following is true:
A. Breaths should be synchronized with the chest compressions.
B. The goal is 20 or greater breaths per minute C. Chest compressions should be stopped while giving
breaths. D. One breath every 6 to 8 seconds should be given
9) The most important intervention with witnessed sudden cardiac arrest is:
A. early defibrillation
B. effective chest compressions
C. early activation of EMS
D. rapid use of resuscitation drugs
9) The most important intervention with witnessed sudden cardiac arrest is:
A. early defibrillation
B. effective chest compressions
C. early activation of EMS
D. rapid use of resuscitation drugs
1) Typically, suctioning attempts in ACLS situations should be:
A. 10 seconds or less B. 20 seconds or less C. 5 seconds or less D. no more than 30 seconds
1) Typically, suctioning attempts in ACLS situations should be:
A. 10 seconds or less B. 20 seconds or less C. 5 seconds or less D. no more than 30 seconds
Thank you
Please rate the lecture on the following items
Slightly disagree
Strongly disagree
Slightly agree
Strongly agree
Clear
Interesting
Easy to take notes from
Well organized
Relevant to the course
Please rate the lecture on the following items
Slightly disagree
Strongly disagree
Slightly agree
Strongly agree
Was enthusiastic
Was clearly audible
Seemed confident
Gave clear explanation
Encouraged participation
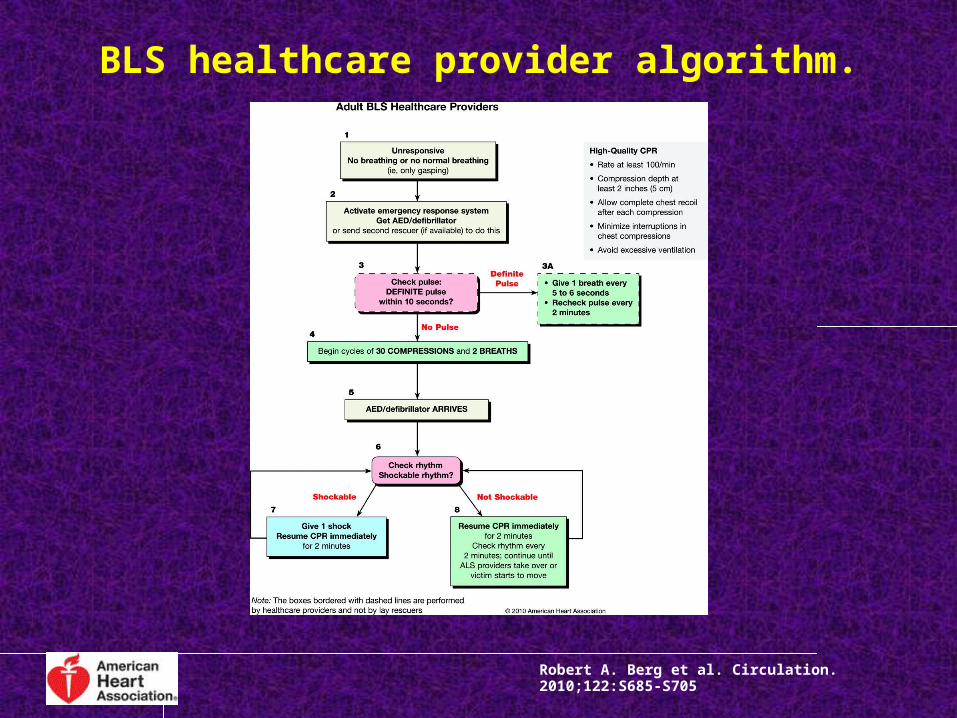
BLS healthcare provider algorithm.
Robert A. Berg et al. Circulation. 2010;122:S685-S705