Embed Size (px)
Citation preview

NOTE:
To change
the image
on this
slide,
select the
picture
and delete
it. Then
click the
Pictures
icon in the
placeholde
r to insert
your own
image.
Amr Hassan, M.D. Associate professor of Neurology - Cairo
University
CRANIAL NERVES


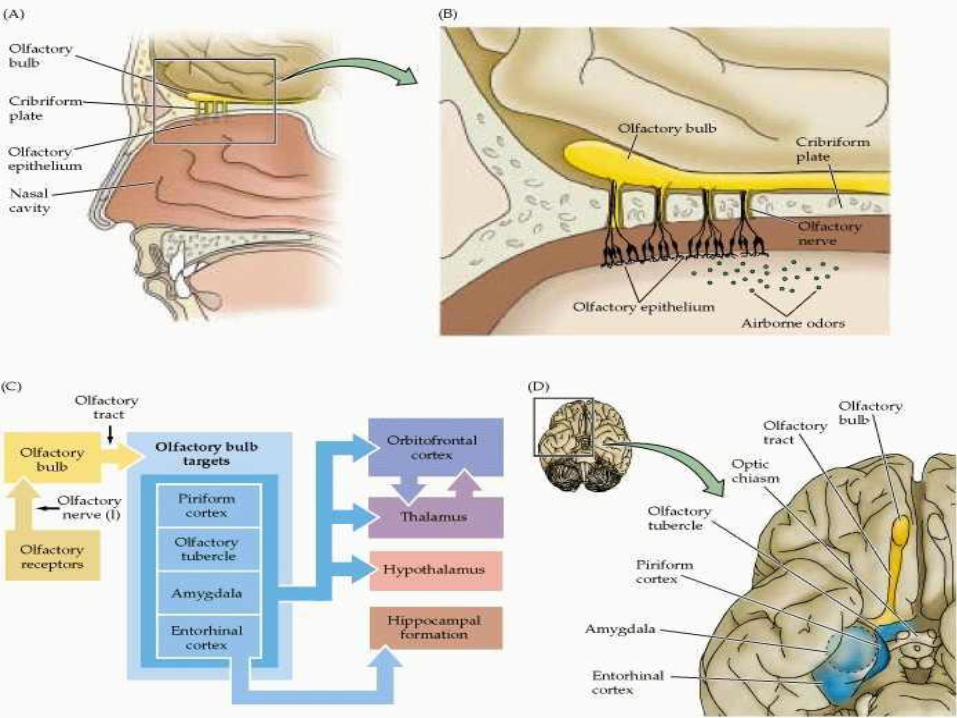
olfactory nerve Pathway of smell :
From the receptors in the olfactory mucosa the fibers of
the olfactory nerve pierce the cribriform plate of the
ethmoid bone and run in the olfactory groove to relay in
the olfactory bulb. A new set of fibers travels in the
olfactory tract to terminate in the olfactory sensory area
in the uncus of the temporal lobe of both sides
olfactory nerve

olfactory nerve lesion Unilateral anosmia Bilateral anosmia
a) Traumatic: fracture cribriform plate.
b) Inflammatory: basal meningitis
c) Neoplastic e.g.olfactory groove
meningioma
a) E.N.T. causes as common
cold.
b) Congenital.
c) Hysterical.
2. Parosmia: Perverted sense of smell. usually unpleasant. Commonest cause
is Post-traumatic.
3. Olfactory hallucinations: Perception of smell usually unpleasant, in the
absence of stimulus. It is due to an irritative lesion in or near the uncus.

The olfactory
system consists
of the olfactory
epithelium, bulbs
and tracts along
with olfactory
areas of the brain
collectively
known as the
rhinencephalon.


Lesions of the olfactory nerve Anosmia
Unilateral : traumatic, inflammatory
neoplastic: Foster-Kennedy syndrome
• Bilateral : ENT, Hereditary, Hysterical • Parasomia NB: Olfactory hallucination is due to central olfactory dysfunction
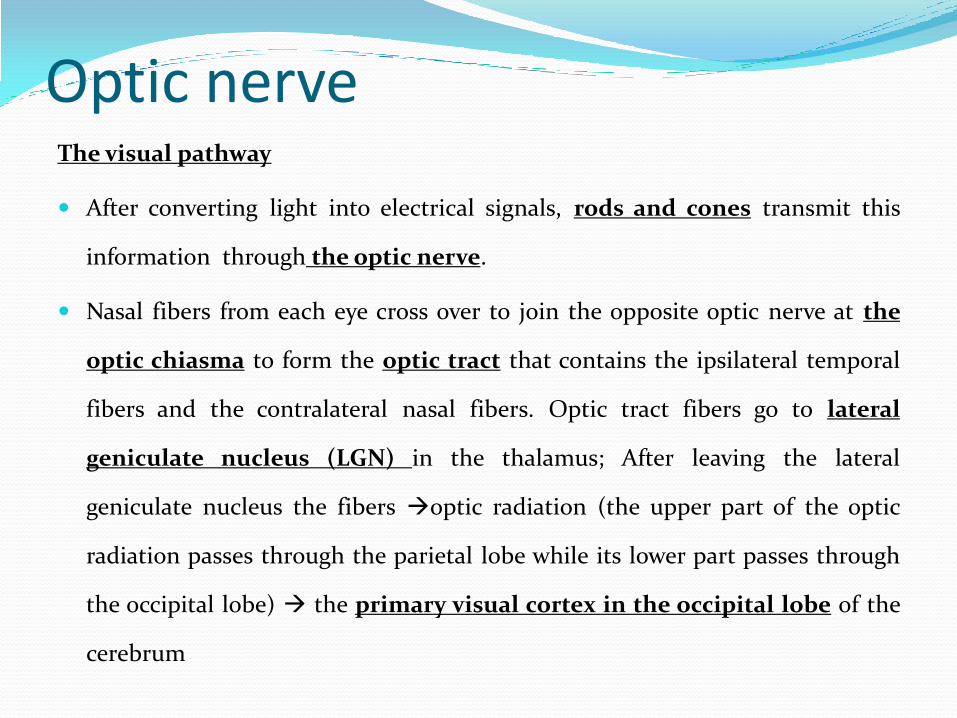
Optic nerve The visual pathway
After converting light into electrical signals, rods and cones transmit this
information through the optic nerve.
Nasal fibers from each eye cross over to join the opposite optic nerve at the
optic chiasma to form the optic tract that contains the ipsilateral temporal
fibers and the contralateral nasal fibers. Optic tract fibers go to lateral
geniculate nucleus (LGN) in the thalamus; After leaving the lateral
geniculate nucleus the fibers optic radiation (the upper part of the optic
radiation passes through the parietal lobe while its lower part passes through
the occipital lobe) the primary visual cortex in the occipital lobe of the
cerebrum

Site of lesion Resulting deficit Explanation
1 The optic nerve Total loss of vision
2 The optic chiasm Bitemporal hemianopia A loss of vision in the temporal halves of both visual
fields because the chiasm carries crossing nasal fibers
from both eyes.
3 The optic tract Contralateral hemianopia Complete loss of vision in the opposite half of the
visual field (e.g. the nasal half of the field of the right
eye and the temporal half of the field of the left eye.
4 Lower optic radiation (temporal lobe)
Upper contralateral quadrantic anopia
A loss of vision in the upper quadrant of the opposite
half of the visual field of both eyes.
5 Upper optic radiation (parietal lobe)
Lower contralateral quadrantic anopia
A loss of vision in the lower quadrant of the opposite
half of the visual field of both eyes.
6 The visual cortex Contralateral hemianopia with macular sparing
Intact macular vision due to its double blood supply.



Monocular blindness

Bitemporal hemianopia

Contralateral homonymous hemianopia


Oculomotor nerve Anatomy
The oculomotor nerve originates from 3 nuclei motor neurons arise from the
oculomotor nucleus, parasympathetic fibers arise from Edinger-Westphal and
Perlia nuclei in the midbrain.
The nerve passes through the superior orbital fissure to reach the orbit.
The motor component of the nerve divides into a superior and inferior division:
The superior division supplies the levator palpebrae superioris and superior rectus
muscles.
The inferior division supplies the medial rectus, inferior rectus and inferior oblique
muscles.
The parasympathetic component of the oculomotor nerve travels with inferior
division to innervate the ciliary muscle and the constrictor pupillae muscle

Oculomotor nerve

External ophthalmoplegia:
Paralysis of Levator palpebrae superioris ptosis
Paralysis of superior rectus muscles, medial rectus, inferior rectus and inferior oblique muscles eye is deviated out and down (due to unopposed action of lateral rectus (supplied by Cr N VI) and superior oblique (supplied by Cr N IV).
Internal ophthalmoplegia :
Paralysis of constrictor pupillae muscle. mydriasis (dilated fixed pupil).
Oculomotor nerve lesion

Lesions of the oculomotor nerve
External ophthalmoplegia
Internal ophthalmoplegia
NB:
compression: early mydriasis and lost light reflex
infarction: pupillary reflex intact

Extraocular muscle movement



Ptosis
Partial Complete


Block the action of frontalis to differentiate between partial and complete ptosis.

The pupil
Constrictor pupillae muscle (parasympathetic supply)
Dilator pupillae (sympathetic supply)

Reflex Light Accommodation
Stimulus Light (torch). Near vision.
Receptor Rods and cones in retina. Rods and cones in retina.
Afferent Ipsilat. optic nerve. Ipsilat. optic nerve.
Center Midbrain: Ipsilat. pretectal nucleus EW nucleus on
both sides.
Occipital cortex.
Efferent Oculomotor nerve on both sides (parasympathetic
fibers) to ciliary ganglion then to constrictor papillae
through short ciliary nerves.
Oculomotor nerve on both sides ( parasympathetic fibers)
to ciliary ganglion constrictor papillae + ciliary muscle
to contact to increase refractive power of lens.
Oculomotor nerve on both sides ( motor fibers) Medial
recti on both sides convergence.
Response Miosis (Constriction of the pupils). 1. Convergence of the eyes due to contraction of both
medial recti muscles.
2. Miosis (constriction of the pupils) due to contraction
of the constrictor pupillae muscles.
3. Accommodation (increased refractive power of the
lens) due to contraction of ciliary muscles.



Accomodation reflex
Convergence
Miosis
Increase refractive
power of lens

Pupillary reflexes

Trochlear nerve
The trochlear nerve has only a somatic motor component which
innervates the superior oblique muscle of the contralateral orbit.
The nucleus of this nerve lies in the lower part of the midbrain.
The trochlear nerve supplies the superior oblique muscle which
turn the eye inwards & downwards (Thus help reading and
descending the stairs).



The Abducent Nerve The nucleus of this nerve lies in the lower part of the pons.
The nerve runs a long intracranial course to supply the lateral
rectus muscle which moves the eye outwards (laterally).
Lesion:
It is the most commonly affected ocular nerve because of its
long course.
Diplopia only when the patient looks outwards, towards the
paralysed side due to limitation of movement of the affected eye
on looking outwards.


Abducent nerve palsy Trochlear nerve palsy
Torticollis

Trigeminal nerve
main 4The trigeminal nerve has
nuclei. 1st 3rd are sensory while the
4th one is motor:.
•Spinal nucleus lies in medulla
oblongata
•Main sensory nucleus lies in pons
•Mesencephalic nucleus lies in midbrain
•Motor nucleus lies in pons .


It leaves the brain stem through the middle cerebellar peduncle form trigeminal ganglion, this ganglion lies in a depression in the floor of the middle
cranial fossa.

Ophthalmic nerve: which enter
the cranial cavity through the
superior orbital fissure. It receive
sensation from GREEN area.
Maxillary nerve: which enter the
cranial cavity through the
foramen rotundum. It receive
sensation from RED area.
Mandibular nerve: which enter the cranial cavity through the foramen ovale. It receive sensation from BLUE area.


Trigeminal nerve functions Functions: 2 functions
The motor function:
The motor fibers start in the motor nucleus in the pons. The fibers emerge from the pons & pass laterally below the trigeminal ganglion to join the mandibular branch of the nerve which leaves the cranial cavity through the foramen ovale. It supplies 7 muscles:
The muscles of mastication: temporalis, masseter, lateral & medial pterygoids.
Three other muscles: anterior belly of digastric, mylohyoid and tensor palati.


بت و بت : سوف الفرق واحدة خدودها مدورين و التانية شفايفها بيضاويين

Trigeminal nerve functions The sensory function:
Fibers carrying pain and temperature sensations from
the 3 divisions run downwards to relay in the spinal
nucleus in the lower part of the medulla on the same side.
In this nucleus:
The face is represented upside down i.e. ophthalmic
fibers end in the lower part of the nucleus while the
mandibular fibers end in its upper part.

Trigeminal nerve functions The peripheral part of the face is represented in the inner
part of the nucleus and the central part of the face is
represented in its outer part.
Fibers carrying proprioceptive sensations from the 3 divisions
run upwards and relay in the mesencephalic nucleus in the
midbrain, on the same side . Fibres carrying touch from the 3
divisions pass directly to the main sensory nucleus in the pons
on the same side.


Lesions of the trigeminal nerve Loss of sensations on the same side of the face (sparing
the angle of the mandible that supplied by C2).
Weakness of the muscles of mastication on the same side of the lesion.
Deviation of the jaw to the affected side due to the unopposed action of the pterygoid muscles of the healthy side.

Trigeminal Neuralgia Definition: Paroxysmal pain along distribution of trigeminal nerve. Clinical picture: Pain is brief (Seconds to 1-2 minutes) and paroxysmal, occur in Several attacks, Stabbing or Shocklike and is typically Severe. One (Single) or more branches of the trigeminal nerve (usually maxillary or mandibular) are involved. Pain is unilateral (rarely bilateral). Trigger points Various triggers may commonly precipitate a pain attack. Light touch or vibration is the most provocative. Activities such as shaving, laughing, brushing teeth and face washing. Pain provokes brief muscle Spasm of the facial muscles, thus producing the tic. Investigations: MRI brain to exclude an uncommon mass lesion or aberrant vessel compressing the nerve roots. Treatment: Medical: Carbamazepine (Tegretol) is the drug of choice. B. Surgical

Motor affection: Weakness of muscles of mastication on the same side of the
lesion
Deviation of the jaw to the affected side
Reflex affection Ipsilateral loss of corneal and conjunctival refelx.
Ipsilateral loss of palatal refelx.
Lost jaw reflex
Exaggerated jaw reflex BILATERAL UMNL ABOVE THE PONS.


Facial nerve
The facial nerve is a mixed nerve, as it contains motor,
sensory and autonomic fibers.
Anatomy of the motor part:The motor nucleus of the
facial nerve is located in the pons.The upper part of the
nucleus is bilaterally supplied from the pyramidal tracts
of both sides, while its lower part is unilaterally supplied
from the pyramidal tract of the opposite side only.

Facial nerve From the nucleus, the motor fibres pass through the
cerebello pontine angle in close proximity to Cr.N. V & VIII
then enter through the internal auditory meatus, into
the facial canal where it becomes adherent to its sensory and
autonomic parts.
It then leaves the canal through the stylomastoid foramen,
passes through the parotid gland to divide into its terminal
branches that supply the following muscles.

Facial nerve Muscles of expression Other muscles
1. Frontalis
2. Oricularis oculi
3. Orbicularis oris
4. Buccinator
5. Retractor anguli
1. Platysma.
2. Stapedius
3. Posterior belly of the
digastric muscle.
4. Stylohyoid.

•Stylohyoid
•Post. Belly of diagastric
•Stapidus
•platysma

بس بس


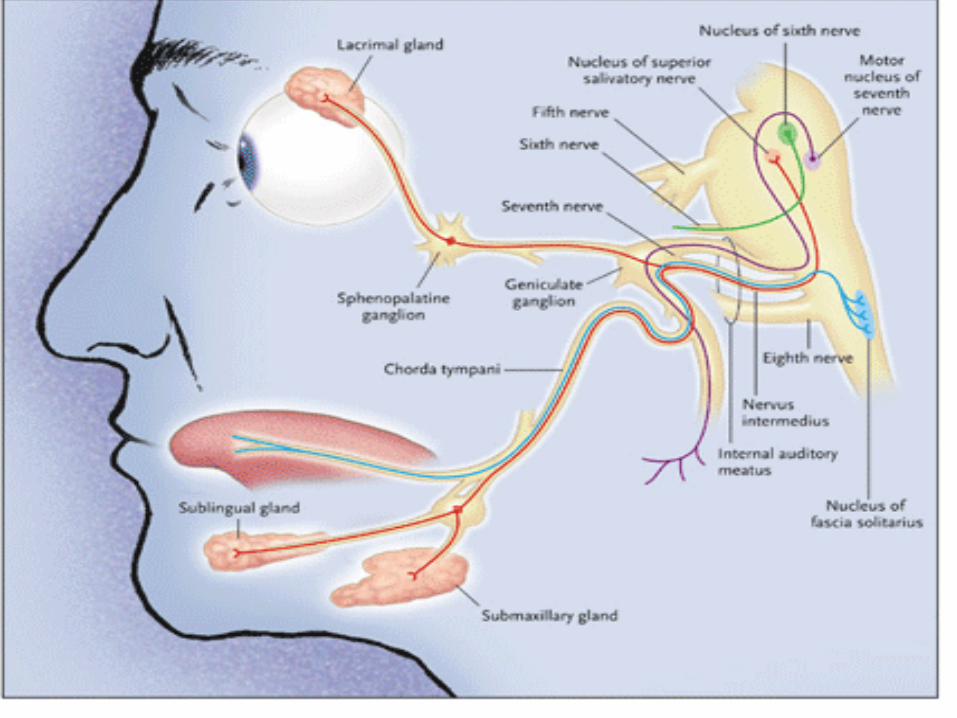
Facial nerve Anatomy of the sensory and autonomic parts: In the facial canal lies the
geniculate ganglion, which contains unipolar cells. The process of these cells
divides in a T-shaped manner into a peripheral branch and a central branch.
1. The peripheral branch runs laterally and divides into the greater superficial
petrosal nerve and the chorda tympani.
a. The greater superficial petrosal (GSP) nerve passes forwards to
relay in the sphenopalatine ganglion where a new set of fibres gives
autonomic supply to the lacrimal gland.
b. The chorda tympani leaves the facial nerve before the stylomastoid foramen, to
supply the submaxillary and sublingual salivary glands and to carry taste
sensations from the anterior 2/3 of the tongue.

The central branch passes centrally, joins the motor part of the nerve,
then enters the cranial cavity through the internal auditory meatus as
the nervus intermediusenters the brain stem terminate in the
solitary nucleus in the medulla. A new set of fibers passes from the
nucleus to the opposite side and runs upwards to terminate in the
lower part of the ;cortical sensory area, where taste sensation from
the anterior 2/3of the tongue is perceived.
Facial nerve

U.M.N.L L.M.N.L
Affecting Δ tract above facial nucleus. Affecting the facial motor nucleus or the nerve
itself.
Paralysis of the muscles of lower half of the
face on the opposite side of the lesion
(supplied from the opposite ∆ tract only)
leading to:
a. Obliteration of the naso-labial fold.
b. Dropping of the angle of the mouth
with dribbling of saliva.
c. Accumulation of food behind the cheek
d. Inability to blow the cheek.
e. Inability to show the teeth properly.
Paralysis of the muscles of the upper & lower
halves of the face on the same side of the lesion
leading to:
a e and in addition:
f. Inability to raise the eyebrows with absence
of wrinkles of the forehead.
g. Inability to close the eye, when the pt.
attempts to close his eye the eyeball rolls
upwards (Bell's phenomenon).
Paralysis involves the voluntary movement;
it spares the emotional & associative
movements (which are supplied by extra ∆
fibers).
Paralysis affects voluntary, emotional &
associative movements.
There is associated hemiplegia on the
same side of the facial paralysis.
If there is hemiplegia, it is on the opposite side
of the facial paralysis (crossed hemiplegia).

Upper motor neurone Facial nerve lesion

Site
of lesion
Facial
muscles
Taste
sensation.
Salivation
lacrimation
Other
Features
Causes
Nuclear
Lesion
Paralysed Intact Intact Hemiplegia
on opposite
side
Vascular:
Vertebro-basilar insuf.
Millard-Gubler
syndrome.
Infective:
Encephalitis.
Poliomyelitis.
Neoplastic:
Astrocytoma
Glioma
Demyelinating: M.S.
Cerebello-
Pontine Angle
Lesion:
Paralysed ↓ ↓ Cr.n.
V,VIII
palsies on
same side
Infective:
Basal meningitis.
Neoplastic:
Acoustic neuroma.
Meningioma
Facial Canal
Lesion:
Paralysed ↓ if chorda
tympani is
involved.
Lacrimation
↓ If the
GSP nerve
is involved.
Salivation↓
if chorda
tympani is
involved.
Traumatic:
Fracture base.
Infective:
Otitis media.
Herpes zoster.
Neoplastic:
Facial neuroma.
Bell's palsy.
Extracranial
Facial Lesion:
After its exit
from the
stylomastoid
foramen.
Paralysed Intact Intact Intact Neuropathy:
Diabetic
Myasthenia.
Myopathy:
Facioscapulo-humeral.
Myotonia Atrophica.
Neoplastic:
Invasion by a tumour
e.g. from parotid.

Bell’s palsy
Definition: It is an acute paralysis of the facial nerve near the stylomastoid foramen (i.e. LMN). It is usually unilateral, may be recurrent & sometimes runs in families.
Aetiology: Many causes have been suggested:
1. Exposure to air drafts usually precedes the onset; this may lead to ischaemia, oedema & compression of the nerve at the stylomastoid foramen.
2. It may be 2ry to a neurotropic virus e.g. Herpes zoster.
3. It may be autoimmune, as evidenced by high levels of immunoglobulins in the patient's serum.

Bell’s palsy
Clinical Picture:
The onset is usually acute with pain behind the ear One or two days later, there is complete
paralysis of the facial muscles on the affected side of L.M.N. nature.
Treatment :
1. Medical:
a) Oral steroids
b) Protection of the exposed cornea.
2. Physiotherapy:
3. Surgical:
a) Decompression of the facial nerve.
b) Facial nerve grafting.
Fig. 30: A patient with Lt 7th nerve palsy


Prognosis:
Full recovery occurs in about 80% of the cases, 15% experience some kind of
permanent nerve damage and 5% remain with severe sequelae.
Poor prognostic factors:
- Complete palsy or severe degeneration (electrophysiology).
- No signs of recovery by three weeks.
- Age >60.
- Severe pain.
- Ramsay Hunt's syndrome (herpes zoster virus).
- Associated with either hypertension, diabetes, or pregnancy.
Bell’s palsy
Those with axonal degeneration may not show any re-innervation for three months and recovery may be partial or not at all.
Synkinesis is often seen e.g. blinking causes the angle of the mouth to contract.
Also aberrant parasympathetic re-innervation may cause symptoms such as gustatory lacrimation ('crocodile tears').
Bell’s palsy

The Vestibulo-Cochlear Nerve This nerve is composed of 2 divisions: 1. Vestibular. 2. Cochlear
1. Vestibular branch:
Fibers originating from the semicircular canal, utricle & saccule in the inner ear join the
cochlear division in the internal auditory canal (see fig. 31).
They then pass in the cerebello-pontine angle to enter the brain stem where they relay in the
vestibular nuclei in the brain stem. New fibres take 3 pathways to:
1. The archicerebellum, concerned with equilibrium.
2. The medial longitudinal bundle, concerned with the synchronous movements of the eyes,
head & neck.
3. The cerebral cortex, concerned with the perception of the sense of vertigo.
Lesion of the vestibular division results in:
1. Vertigo. 2. Ipsilateral incoordination. 3. Spontaneous nystagmus.

The Vestibulo-Cochlear Nerve 2. Cochlear nerve:
Fibers originating from the ganglion cells of the cochlea pass centrally from the inner ear through the internal auditory canal where they are joined by the vestibular division. They then pass through the cerebello pontine angle to enter the brain stem, where they relay in the cochlear nucleus (in the lower pons) lateral lemniscus medial geniculate bodies (M.G.B.) auditory sensory area in the temporal lobes (see fig. 31).
Lesion:
Tinnitus, in irritative lesions.
Deafness, in destructive lesions.


Vertigo Definition: It is the sense of rotation of the body in steady
surroundings or the reverse that is usually aggravated by
movements of the head and it persists in all positions: sitting,
standing or supine.It is usually associated with autonomic
manifestations in the form of nausea, vomiting, pallor and
bradycardia.
N.B. Vertigo should be differentiated from dizziness, giddiness
and light headedness where the unsteadiness is not associated
with a sense of rotation.

Vertigo
Causes:
Table 8: causes of vertigo.
Labyrinthine Peripheral nerve Brain stem
Physiological: sea
sickness, car sickness.
Pathological:
labyrinthitis, Meniere's
disease, otosclerosis.
Cerebello-pontine angle
lesion as acoustic
neuroma.
Vestibular neuritis.
Vertebro-basilar artery
insufficiency.
Posterior inferior cerebellar
artery occlusion.
M.S.
Treatment: Treatment of the cause and medical.treatment for vertigo

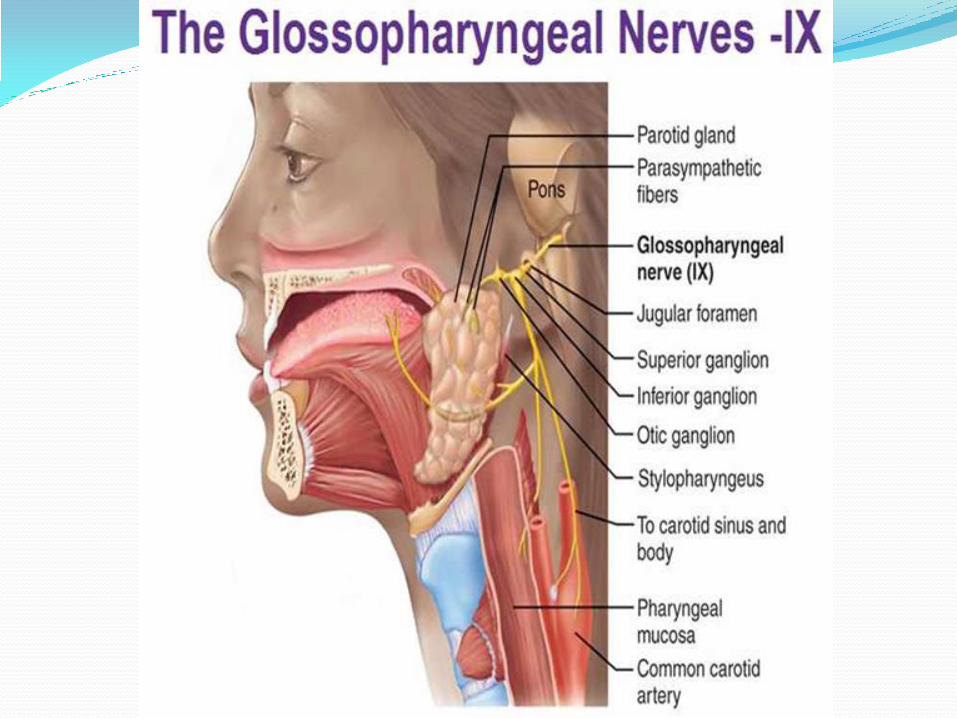
IX. The Glossopharyngeal Nerve This is a mixed nerve carrying motor, sensory &
autonomic (parasympathetic) fibers.
Motor fibers: supplying stylopharyngeus and constrictors of the pharynx.
Sensory fibers: receive general sensations from the posterior ⅓ of tongue, pharynx & tonsils and taste sensation from the posterior ⅓ of tongue.
Autonomic fibers: Parasympathetic fibers to the parotid gland (see fig. 32).

Lesion:
Ipsilateral loss of taste & general sensations from the posterior ⅓ of the tongue.
Ipsilateral loss of the pharyngeal reflex (afferent Cr.N. 9, efferent Cr.N.10).
IX. The Glossopharyngeal Nerve

The Vagus Nerve
This is a mixed nerve carrying motor, sensory & autonomic (parasympathetic) fibers (see fig. 33).
Anatomy:
1. Motor fibers: to the soft palate, pharynx & larynx.
2. Sensory fibers: from - The skin over the external auditory meatus.
- The thoracic & abdominal viscera.
3. Autonomic fibers: Parasympathetic fibers to the heart (inhibitory), the G.I.T. & the bronchial tree (secretory & motor).
Lesion:
1. True Bulbar Palsy:
- Bulbar symptoms: Dysphagia, dysarthria, dysphonia & nasal regurge.
- Ipsilateral loss of palatal & pharyngeal reflexes.
2. Dysautonomia: Tachycardia & constipation. `


Glossopharyngeal and vagus nerves
Deviation of the palate
Palatal reflex
Pharyngeal reflex
Swallowing water


Palatal deviation

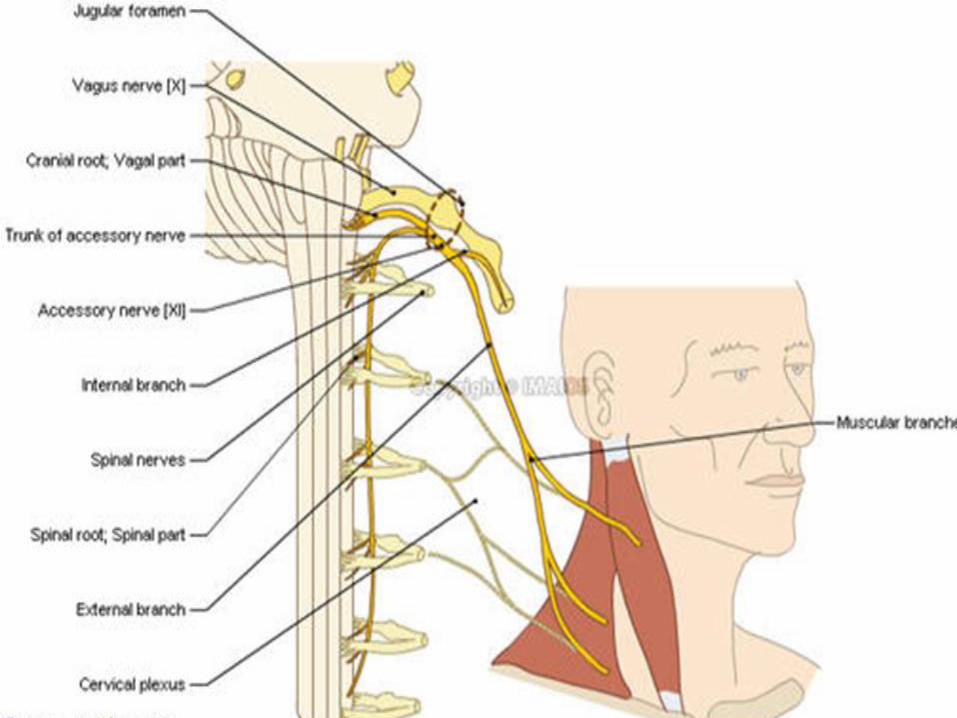
XI. The Accessory Nerve This nerve is purely motor & is formed of 2 parts.
Anatomy:
1. Cranial part: It arises in the medulla & runs with the vagus nerve to
share in the motor innervation of the soft palate & pharynx.
2. Spinal part: It arises from the A.H.C. of the upper five cervical
segments, ascends alongside the spinal cord and enters the cranial
cavity through the foramen magnum. It joins the cranial portion to exit
through the jugular foramen to supply the sternomastoid &
trapezius muscles (see fig. 34).
Lesion: Ipsilateral paralysis of the sternomastoid & trapezius muscles.
XII. The Hypoglossal Nerve This is a purely motor nerve which supplies the
intrinsic muscles of the tongue.
Anatomy: Its fibers arise from the cells of the hypoglossal nucleus in the medulla hypoglossal canal hypoglossal foramen intrinsic muscles of the tongue (see fig. 35).


Lesion:
Table 9: U.M.N. and L.M.N. hypoglossal nerve.
. U.M.N.L L.M.N.L.
Unilateral Deviation of the tongue to the
opposite side of the lesion.
No wasting or fasciculation.
Deviation of the tongue to the side of
the lesion.
Wasting and fasciculation.
Bilateral Inability to protrude the tongue
(spastic tongue)
No wasting or fasciculation.
Inability to protrude the tongue.
Wasting and fasciculation.
XII. The Hypoglossal Nerve

Inspect the tongue for: Deviation.
Wasting.
Fasiculations.
Abnormal movement
Evidence of systemic disease
Test for the power
The hypoglossal nerve


Thank you