Embed Size (px)
Citation preview

Is Map one of the causes of Crohn’s Disease?
A review of papers from 10th International Colloquium on Paratuberculosis
Peter Mullowney

The Public Health Perspective Carol Nacy
2

American Academy of MicrobiologyColloquium, June 2006; Publication June 2007
Question the Colloquium addressed is whether MAP has evolved to infect human gastrointestinal tissue and whether once there it can cause disease.
28 participants met for 3 days to discuss and debate a number of questions surrounding MAP and human disease
Participants included microbiologists, human geneticists, immunologists, molecular biologists, food microbiologists, diagnostics developers, veterinarians, public health officials, gastroenterologists and patients.
Nacy, (2009) 3

MAP Research in 2006Facts that DID NOT support existence of a link between MAP and CD:• Dairy farmers and others who may have greater exposure to MAP than the
general population did not experience higher rates of CD in one study• There are some dissimilarities in the clinical and pathological presentation
of CD and Johne’s disease• Cell-mediated immune responses to MAP or MAP antigens have not been
demonstrated in CD patients.• No systematic studies, but CD has not been reported to worsen with
progressive immunocompromise, such as happens with M. tuberculosis infections (exacerbated by HIV or anti-TNFα therapy)
• In a controlled clinical trial, CD patients undergoing 6 months of antibiotic therapy did not maintain a sustained response to the drugs and the relapse rate after 2 years was similar in treated and control groups.
Nacy, (2009) 4

MAP Research in 2009 ( a few examples)
Facts that DID NOT support existence of a link between MAP and CD:
Jones 2005, by questionnaire 2897 dairy farmers were surveyed“ The prevalence of Crohn’s disease was found to be similar to that reported in
other studies in the United Kingdom and showed no association with bovine paratuberculosis”
• Singh et. Al. Sharing of Indian Bison Type MAP between goatherds endemic for Johne’s Disease and their animal attendants.– Demonstrated that prolonged exposure to MAP-infected goats can result
in infected humans– MAP was isolated from 28/40 goatherders with CD symptoms– Longer the contact the more likely the goatherder was to acquire MAP– Prolonged contact may override any genetic resistance to MAP.
Nacy, (2009) 5

Singh,(2009) 6

Singh,(2009) 7

MAP Research in 2009 ( a few examples)
Facts that DID NOT support existence of a link between MAP and CD:
Cell mediated immune responses to MAP or MAP antigens have not been demonstrated in CD
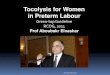
• Olsen et. Al, CD4 T cells from intestinal biopsies of Crohn’s Disease patients react to MAP.– Isolated T cells from biopsies of CD,UC, and control patients– T cells of CD patients proliferated to MAP Ags > UC T cells– 28 T cell clones were created from T cells of 4 CD patients– All clones responded to MAP, some also to other Mycobacteria– T cell clones produced IFNγ and IL17 to MAP stimulation
Nacy, (2009) 8

Olsen, (2009) 9

Proliferation of T-cell clones from two different CD patients
Olsen, (2009) 10

Cytokine production from T-cell clones in response to MAP
Olsen, (2009) 11

MAP Research in 2009Confirmatory studies reported at this meeting (and at this
session)Viable MAP has been identified in milk, cheese, and now muscle
tissues of Johne’s Diseased cattle:• Alonso-Hearn, et. Al, Isolation of MAP from muscle tissue of
naturally infected cattle.– 47 cows slaughtered for JD (17) or other reasons(30)– 66% had MAP in GI tissues– MAP was cultured from diaphragm tissues of 6 animals (19%)– Possible that infected meat may be a source of exposure for humans.
Nacy, (2009) 12

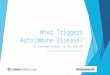
Paratuberculosis-zoonotic potential
1. Similarity between the clinical signs of Crohn’s disease in humans and those found in animals with Johne’s disease (Greenstein et al., 2003)
2. Detection of Map in feces, intestinal tissues and peripheral blood of patients with Crohn’s disease (Juste et al., 2008).
3. Association between Map DNA in blood and humoral immune responses in Crohn’s disease patients (Juste et al., 2008)
4. Anti-Map antibiotic therapy resulting in reduction of bacteremia and remission, or substantial improvement in disease condition in many patients (Borody et al., 2007)
Johne’s disease pathology
http://www.crohns.org/map_food/photo.htm
Alonso-Hearn, (2009) 13

MAP Research in 2009Genetic polymorphisms are associated with development of
Crohn’s Disease:• Juste, et. Al, Associations between CARD15 polymorphisms,
MAP DNA in blood and lactase persistence in a Crohn’s Disease case-control study in North-Spain.– Blood was collected from 150 CD patients and 65 blood donors– MAP was identified by PCR in blood of both CD patients and donors– T allele of lactase gene > CD patients than donors– The odds ratio of 2 alleles of CARD15 and MAP was >4– Genetic factors associated with CD
Nacy, (2009) 14

Empirical Clinical Observation:Tobacco use exacerbates Crohn’s disease and its
cessation results in clinical improvement.
HypothesisNicotine, or its structural analogs (Isoniazid,
nicotinic acid, nicotinamide, α & β nicotinamide adenine dinucleotide) will
modify MAP growth kinetics.
Greenstein, (2009)15

MAP Research in 2009There are antibiotics that can inhibit MAP growth in
vitro:• Greenstein, et. Al, Nicotinic and Salicylic acids and α
& β NAD cause dose-dependent enhancement, and INH and PAS cause dose-dependent inhibition of MAP.– Pure nicotine does not affect MAP growth– Structural nicotine analogues and antituberculars INH and
PAS inhibit MAP growth– Salicylic and nicotinic acids increase MAP growth– It is unclear why cessation of smoking improves Crohn’s
Disease.
Nacy, (2009) 16

Greenstein, (2009)17

Greenstein, (2009)18

Greenstein, (2009)
19

Conclusions:In the doses tested Nicotine has no effect
on the growth kinetics of MAP.
Nicotine’s structural analogs
Profoundly effect the growth kinetics of MAP.
Do not enhance growth of the M. tuberculosis complex.
Greenstein, (2009)20

Where are the Weapons of Mass Destruction - - - the MPTB? Herb Van
Kruiningen• Features of Crohn’s Disease that do not occur in Johne’s disease• It was for a time said that a total of 10 cultures of M paratuberculosis
had been recovered. Or --- 10 cultures recovered throughout the world in 27 years of attempts
• Collins 2000, conducted 3985 culture attempts with various selective media on 191 patients with IBD, 79 of which had Crohn’s disease … all were negative for M paratuberculosis.
• Naser 2000, reports on the isolation of M paratuberculosis in breast milk of 2 patients and not in 5 controls.
21

Bacteriologic CultureBull 2003, PCR detected IS900 in 14/33 in CD, 3/33 in controls.
“ However the isolation of M.avium subsp. Paratuberculosis from these positive MGIT cultures on solid medium or in axenic culture has not yet been achieved”.
Naser 2004, describes the isolation of viable MAP from the blood of 14/28 CD patients, 2/28 with ulcerative colitis and none from 15 non-IBD controls
Freeman 2005, repeats the work of Naser on 22 patients and is unable to culture MAP
Van Kruiningen, (2009)
22

Blood samples from 58 subjects were blindly coded and investigated by three independent laboratories for the presence of Mycobacterium avium subspecies paratuberculosis (MAP) using MGITpara specialized media and nested PCR. Consequently, viable MAP was detected in 22/40 (55%) IBD (11/20 CD and 11/20 UC) compared to 4/18 (22%) NIBD (P<0.009). At least two centers detected MAP in 41% IBD samples compared to none (0%) in NIBD (P<0.0001). No sample was positive by all three centers. Despite result variability between centers, the study strongly demonstrates that using MGITpara culture media and nested PCR are essential for successful detection of MAP in human blood. Overall, the study supports a mycobacterial role in CD pathogenesis.
23

MAP in early onset CD
140 patients: 2 – 16 yrs ageProspective samples no medicationOptimised DNA extractionControlled, MAP specific PCRLong term culture for MAP
(Kirkwood; Inflamm. Bowel Dis.2009)
Biopsy
PCR
PBMC
PCR
Biopsy
Culture
CD 39% 16% 40%
UC 32% 8% 0%
Non-IBD 15% 0% 0%
Bull, (2009)24

Paratuberculosis and Crohn's Disease: Already beyond reasonable doubt
Tim Bull
• “For MAP not to contribute to pathogenesis and merely to have a bystander role, it would be necessary to accept that despite its specific ability to cause chronic inflammation of the intestine in so many animals, including primates, it is somehow harmless to man.”(Herman –Taylor et al., J. Med Microbiol, 2002)
• “ The critical issue today is not whether MAP is associated with CD, but whether MAP causes CD or is only incidentally present, not an inciter or participant in the disease process.”(Nacy et al. American Society for Microbiology 2008)
Bull, (2009)25

MAP Reservoirs
MAP prevalence in wild and domestic animals is very high 70% MAP prevalence in US Dairy herds (USDA 2008)
CD prevalence is increasing in humans particularly paediatric CD (10 fold in 20 yrs: Phavaichitr 2003)850,000 CD cases in North America 50% are children.
Bull, (2009)26

MAP Reservoirs
Viable MAP is present in Soil (Whittington: Appl Environm Microbiol 2005)Water (Pickup: Appl Environm Microbiol 2006)Potable water (Mishina: Proc Natl Acad Sci USA 1996) Meat products (Aloso-Hearn: Foodborne Path Dis 2009) Dairy products (Shankar:Int. J. Infect.Dis. 2009)
CD clusters associated with Water Supplies (Van Kruininingen: Inflamm Bowel Dis. 2007)
Bull, (2009)27

MAP Transmission
MAP Transmission regularly occurs from animals to humans
Can MAP actively invade and persist in human gut epithelium?
Bull, (2009)28

MAP Infection into human gut is an active process
Human foetal ileum xenographed to SCID mice(Golan: J. Inf. Dis. 2009)
MAP M. smegmatis 3/9 donors 6/9 donors 9/9 donors Active Invasion Low Invasion Low Invasion Severe Inflammation Mild Inflammation No damage Epithelial damage No damage Bull, (2009)
29

MAP and HD5
HD5 expression is significantly reduced in the gut of CD patients.HD5 inhibits entry of MAP into human macrophage cell linesNOD2 mutation leads to HD5 depletion leads to MAP infection?
Bull, (2009)30

MAP Detection
“The association of MAP and Crohn’s disease, based on PCR or ELISA testing is well established”MAP +ve are 7 fold more likely in CD than Normals
10 – 40% presence of MAP in Non-STERILE and STERILE samples from Normals
MAP is chronically and actively invading humansBull, (2009)31

MAP culture and VNC phenotype
Viable Non-Culturable (lag) phase increases with repeated cycles of heat shock.
Bull, (2009)32

MAP culture and VNC phenotype
MAP infection into human macrophages leads to Viable Non-Culturable (VNC) phenotype.
Bull, (2009)33

MAP culture and VNC phenotype
MAP becomes Viable Non-Culturable (VNC) on intracellular entry
Some Crohn’s Disease therapies are inhibitory to culture
Immunotherapy (which aggravates MTB infection) does not promote MAP growth
Negative MAP culture is NOT necessarily indicative of Negative MAP infection
CD patients on some long term therapies may not be suitable for MAP culture studies
Bull, (2009)34

Summary
MAP can and does
Infect and persist in Crohn’s patients
Respond to anti-MAP therapeutics in Crohn’s patients
Exploit CD susceptibility gene defects to promote chronic persistence
Generate a Th17 biased immune dysregulation that COULD lead to Crohn’s Disease
Bull, (2009)35

Verdict
Viable chronic MAP infection is present in most patients with Crohn’s DiseaseMAP infection can cause the immune dysregulation
that is the major predisposing factor to the development of Crohn’s Disease
Bull, (2009)36

MAP
Incidental Pathogen or Public Health Threat?
Is this any longer the right question?
Nacy, (2009) 37