Embed Size (px)
Citation preview

© 2010. Clinical Horizons, Inc. All Rights Reserved
Crossing the Quality Chasm: A New Health System for the 21st Century
Key Points Summary and 2008 Implications
December 18, 2008 Joanne Bohn, MBA

© 2010. Clinical Horizons, Inc. All Rights Reserved
Summary Note on Briefing
Charts titled “Validation… ” are provided as trends and industry references to support preceding slides
and the future trends that unfolded after the IOM concepts were published in 2001

© 2010. Clinical Horizons, Inc. All Rights Reserved
Outline
• Book Overview
• Key Points
• Strategic Implications in 2008

© 2010. Clinical Horizons, Inc. All Rights Reserved
Report Overview • Crossing the Quality Chasm: A New Health System for the 21st
Century… was the 2nd report and study in the “Quality Chasm Series” issued by the Committee on Quality of Health Care in America (launched 1998) and followed their landmark report “To Err Is Human: Building a Safer Health System”.
• Strategies are proposed for progressing toward the learning organization model for a national patient-centered care system. It denotes “…how the healthcare delivery system can be redesigned to innovate & improve care.”
• The study was funded collectively by: – Howard Hughes Medical Institute – Kellogg Foundation – Healthcare Financing Administration – Commonwealth Fund – Robert Wood Johnson Foundation – California Healthcare Foundation – AHRQ

© 2010. Clinical Horizons, Inc. All Rights Reserved
Quality Chasm Series of Literature by the IOM
1999 2001 2003 2005
Identification of quality problems in
patient care
Identification of a framework for redesign of the US healthcare
system (6 aims for improvement)
Expansion of redesign process in the 2001 framework
Application of the framework in the mental health / substance abuse (M/
SU) sector of the industry
Discussion of underlying causes of ADEs and CPOE noted as top IT intervention
2006

© 2010. Clinical Horizons, Inc. All Rights Reserved
Key Points

© 2010. Clinical Horizons, Inc. All Rights Reserved
The Framework: Six Aims of High-Quality Health Care
1. Safety1- Avoid injuries to patients 2. Effective-
Provide services based on scientific
knowledge to all who can benefit
3. Patient-Centered- Provide care that is
respectful & responsive to individual patient needs &
preferences 4. Timely- Reduce waits & delays for those receiving &
Giving care
5. Efficient- Eliminate waste including
ideas, equipment, supplies & energy
6. Equitable- Providing consistent quality
of care regardless of gender, ethnicity, location or
socioeconomic status

© 2010. Clinical Horizons, Inc. All Rights Reserved
Validation #1: December 11, 2008 Joint Commission Report- Sentinel Event Alert
Title: Safely Implementing Health Information and Converging Technologies
“United States Pharmacopeia MEDMARX database includes 176,409 medication error records for 2006, of which 1.25 percent resulted in harm. Of those medication error records, 43,372, or approximately 25 percent, involved some aspect of computer
technology as at least one cause of the error.”1
13 Suggested Actions by the Joint Commission for Mitigating Risk of Errors Related to HIT Implementations
Source; “Sentinel Event Alert- Safely Implementing Health Information and Converging Technologies”. Joint Commission Report. Issue 42, 12/11/08.

© 2010. Clinical Horizons, Inc. All Rights Reserved
1. Examine workflow processes and procedures prior to HIT implementation
2.Actively involve clinicians and staff who will Use/be affected by the HIT (full life cycle)
3.Assess HIT needs; require IT staff to interact with users outside their facility; reduce interfaces
4.Continuously monitor HIT for problems; address resultant workarounds/incomplete error reporting early
5.Provide training program for all types of clinicians and staff with refresher courses; focus on benefits
7. Prior to taking a technology live, ensure all guidelines /standardized order sets are developed & tested
8. Develop a graduated system of safety alerts to aid Clinicians in determining urgency and relevancy
9.Mitigate harmful drug orders by requiring dept/pharm review & signoff on orders created outside parameters
10.Provide an environment that protects staff involved In data entry from undue distractions when using HIT
11.Post implementation, continue to reassess/enhance safety effectiveness and error-detection capability
Validation #1, ctd: Joint Commission Report 12/11/08 - Sentinel Event Alert- 13 Suggested Actions
6.Create and communicate policies specifying staff authorizations and responsibilities
12.Post-implementation, continually monitor/report errors, near misses or close calls caused by HIT
13.Re-evaluate applicability of security and confidentiality protocols as more medical devices interface with the IT network

© 2010. Clinical Horizons, Inc. All Rights Reserved
Validation #2: Obama-Biden Health Plan
Provide Quality, Affordable & Portable Health Coverage For All
Modernizing The U.S. Health Care System To Lower Costs & Improve Quality
Promoting Prevention & Strengthening Public Health
Establish New Public Health Plan
New National Health Insurance Exchange
New Tax Credits for Families and Small Businesses
Expand eligibility For Medicare & SCHIP
Employer’s Have Option Of “Play or Pay” Model
Guarantee Eligibility To All Americans
$10B/Yr Investment In HIT
Require Health Plans to Utilize Proven Disease Mgmt Programs
Hospitals & Health Plans Increase Transparency
Allow Safe Drug Imports; Incr. Payer Competition
Establish Independent Inst. on Comparative Effectiveness
Strengthen Anti-trust Laws/Reduce Malpractice
Increase Focus on Worksite Interventions
Strengthen School-based Health Screening Programs
Expand Funding for Public Health Workforce Training
Increase Funding to Expand Community -based Preventive Interventions
Realign Public Policy; Invest in Workforce Recruitment; Develop National Public Health Strategy
Source: http://www.barackobama.com/pdf/issues/HealthCareFullPlan.pdf

© 2010. Clinical Horizons, Inc. All Rights Reserved
Underlying Factors for Inadequate Care Across Entire US Healthcare System
Growing complexity of science and technology
Increase in chronic conditions
Poorly organized delivery system
Constraints on exploiting the revolution in information technology

© 2010. Clinical Horizons, Inc. All Rights Reserved
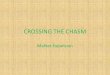
Validation #3: NIH Increase in Total Research Funding 1992-2007
Source: http://www.nih.gov/about/almanac/appropriations/part2.htm
Funding trend tracks with “growing increase in science and technology”

© 2010. Clinical Horizons, Inc. All Rights Reserved
Validation #3, ctd: Increase in Chronic Conditions (i.e. Diabetes)
Source: "Diabetes is surging worldwide."By Marc Santora of The New York Times. 6/11/06 (figures from International Diabetes Federation)
Source: http://www.cdc.gov/diabetes/statistics/prev/national/tablepersons.htm , http://www.diabetes.org/uedocuments/NationaldiabetesFactSheetRev.pdf

© 2010. Clinical Horizons, Inc. All Rights Reserved
Validation #4: Increase in Uninsured (Care Gap Expanding)
Source: US Census Bureau, Income, Poverty, and Health Insurance Coverage in the United States: 2006. Data released August 2007. Table 6. People With or Without Health Insurance Coverage by Selected Characteristics: 2005 and 2006. Link: http://www.census.gov/hhes/www/hlthins/hlthin06/p60no233_table6.pdf
Increasing care gap tracks with “poorly organized delivery system”

© 2010. Clinical Horizons, Inc. All Rights Reserved
Ten Rules to Guide Redesign of the Health Care System
1. Care Based on Continuous Healing Relationships- Patients should have access to care 24/7 and in many forms
2. Customization Based on Patient Needs & Values- System meets most common needs & capable of fulfilling unique preferences
3. Patient As the Source of Control2- Patients receive adequate information to make Informed choices about healthcare decisions
4. Shared Knowledge & Free Flow of Info- Patients have open access to their medical info and communication with their clinician
5. Evidence-based decision making- Patients receive care based on best available scientific knowledge with no variation
6. Safety as a System Property- Patients should be safe from injury by the care system; which should strive to prevent & mitigate errors
7. The Need for Transparency- Patients should have access to care 24/7 and in many forms
8. Anticipation of Needs- The health system should anticipate patient needs rather than reacting to them
9. Continuous Decrease in Waste- The health system will not waste resources or patient time
10. Cooperation Among Clinicians- Clinicians & institutions should collaborate & Coordinate to ensure coordination of care

© 2010. Clinical Horizons, Inc. All Rights Reserved
Five Elements for Improving the Delivery System to Ameliorate Outcomes
1. Evidence-based, Planned Care
2. Reorganization of Practices to Provide Improved Delivery
of Care
3. Systematic Attention To Patients Need For
Information & Behavioral Change
5. Ready Access to Necessary Clinical
Expertise
4. Supportive Information Systems
National Patient Outcomes

© 2010. Clinical Horizons, Inc. All Rights Reserved
Three Focus Areas for Accomplishing the Six Aims
6 Aims for Improving Quality of Care
1. Need for improved organization of the delivery system3
2. Improving accessibility & usefulness of clinical evidence
3. Need for changes to the environment of payment4

© 2010. Clinical Horizons, Inc. All Rights Reserved
Validation #5: Transition from Inpatient to Outpatient Services (1981-2005)
Change in surgical service mix supporting the need for evaluation and reform in the US care delivery model
Source: http://www.aha.org/aha/research-and-trends/chartbook/2007chartbook.html
Avalere Health analysis of American Hospital Association Annual Survey data, 2005, for community hospitals.

© 2010. Clinical Horizons, Inc. All Rights Reserved
Validation #6: Change in Community Hospital ED Services Capacity and Use 3
Increasing reliance for treatment by various demographic segments through ED services coupled with closings of ED departments 91-01
Source: http://www.aha.org/aha/research-and-trends/chartbook/2007chartbook.html

© 2010. Clinical Horizons, Inc. All Rights Reserved
Validation #7: Change in Family Health Insurance Premiums and Federal Poverty Level
SOURCE: Kaiser Family Foundation. http://facts.kff.org/chart.aspx?ch=157
Acceleration of family premiums over federal poverty level. Evidence of need for change in the delivery system and payment reform

© 2010. Clinical Horizons, Inc. All Rights Reserved
Validation #8: 2008 Payment Reform Options Summary on a Project of the Bipartisan Policy Center Funded Through the RWJF
SOURCE: “Financing the U.S. Health System: Issues and Options for Change.” Bipartisan Policy Center Report. 6/08.
1: Continue Current Financing Structure Redirect revenue funds to better use
Economic Implications: No clear way to improve funds utilization and recoup increased spending
Health System Implications: Increase in health programs coupled with further erosion of employer-based coverage
and potential for continued increase in uninsured workforce
2: Rollback High-Income Tax Cuts Use revenue generated from expiring tax cuts
Economic Implications: Greatest impact on high-income tax payers; may reduce national productivity
Health System Implications: Effect a “one-time” adjustment in tax revenue and no real impact on healthcare spending or cost containment
3: Reform the Health Benefit Tax Exclusion Limit/eliminate employer premiums from employees’ TI
Economic Implications: High-income employees absorb tax increase; employers reduce non-wage costs
Health System Implications: Altering nature of coverage limiting health benefit tax exclusion may change
price sensitivity and/or population cost awareness
4: Institute a Play-or-Pay Model Employers pay for employee insurance or a tax equal to
cost of alternative source coverage for workers Economic Implications: Expands pool of employers
contributing to health financing
Health System Implications: Dependent on design; it may increase employer-sponsored coverage
5: Implement a Value-Added Tax Replace Medicare payroll tax with a value-added tax on manufacturers/sellers of goods and services
Economic Implications: Flat tax on consumption, encourage more savings than other options, and spreads burden of healthcare across entire population
Health System Implications: No direct connection to reform, but could increase public awareness of system cost

© 2010. Clinical Horizons, Inc. All Rights Reserved
Six Dimensions of Patient-centered Care
Respect for patient’s values, preferences, and expressed needs
Coordination and integration of care
Information, communication, and
education
Physical comfort Emotional support- Relieving fear and
anxiety
Involvement of family and friends

© 2010. Clinical Horizons, Inc. All Rights Reserved
Model Progression: Stages of Development
Stage 2 Loosely structured multidisciplinary teams focused around physician
specialization
Stage 3 Gravitation toward a patient-centered system. Team practices increase and
adoption of HIT accelerates
Highly adaptive system thriving on collaborative relations that continuously
increases system efficiency through innovation and quality improvement
Learning Organization
Stage 4
Stage 1 Highly fragmented
delivery system
Organized Chaos

© 2010. Clinical Horizons, Inc. All Rights Reserved
Validation #9: NCQA PCMH Model as an Organizational Transformation Project
Source: NCQA Jan. 2008 Presentation (Phyllis Torda) http://www.nrhi.org/downloads/PPC-PCMHJan2008.pdf
Focus on physician directed practice, strengthening care coordination across the care continuum and for all stages of a patient’s care needs

© 2010. Clinical Horizons, Inc. All Rights Reserved
Six Domains of Health Information Technology
Clinical Care
Administrative and Financial
Transactions Public Health Professional
Education Research
Consumer Health
4 Domains can be viewed as stand alone but also strategically supporting consumer health and clinical care5

© 2010. Clinical Horizons, Inc. All Rights Reserved
Other Topics Discussed
• Applying Evidence to Health Care Delivery
• Aligning Payment Policies with Quality Improvement
• Preparing the Workforce
Clinical Education and Training
Regulation of the Professions
Legal Liability Issues
Research Agenda for the Future Care Workforce

© 2010. Clinical Horizons, Inc. All Rights Reserved
Strategic Implications in 2008

© 2010. Clinical Horizons, Inc. All Rights Reserved
Implications for Healthcare Providers in 2008
Clinical Transformation: Bridging the Quality Gap- the adoption of HIT6 has and will continue to
serve as an enabler for quality improvements in our healthcare system
The Patient-centered Care Model- increased industry focus on consumer knowledge and consumerism7, need for reduction of errors, changes in medical staff education are all contributors to the transition toward this model
Following the “Ten Rules”- sharing of knowledge (consumers and clinicians), elimination of waste through quality improvement initiatives, and increasing collaborative networks of physicians and healthcare systems will continue to accelerate improvements in the following8: Access to care, Quality and costs of care, Management of chronic conditions for an ever changing population

© 2010. Clinical Horizons, Inc. All Rights Reserved
Implications for Healthcare Providers in 2008
Organizational Transformation: Bridging the Quality Gap- since 2001 the surge in adopting HIT has
supported increased collaboration among health systems, physicians, payers, and regulatory agencies
Demographic Changes and Increases in Chronic Conditions- These issues are driving healthcare workforce strategies for sustainment, education, and the dealing with the forecasted future shortage in clinician talent
Innovation in Our Payment System- at the national level this is needed to improve access to care and alleviate the burden of paying for uncompensated care9
Transition from Stage 1 to Stage 4 in Relation to HIT Adoption- Infusion of HIT systems that impact workflow and communications can initially increase and stress workforces; however as we advance through the learning curve processes are standardized, people adapt to changes, and we transition toward Stage 4, the learning organization plateau

© 2010. Clinical Horizons, Inc. All Rights Reserved
Reference Listing
1. Source; “Sentinel Event Alert- Safely Implementing Health Information and Converging Technologies”. Joint Commission Report. Issue 42, 12/11/08. http://www.jointcommission.org/SentinelEvents/SentinelEventAlert/sea_42.htm
2. “Hospital Quality Improvement: Strategies and Lessons Learned from U.S. Hospitals” Commonwealth Fund Study. 4/07. http://www.commonwealthfund.org/usr_doc/Silow-Carroll_hosp_quality_improve_strategies_lessons_1009.pdf?section=4039
3. “Managed Consumerism In Health Care”. Health Affairs. November/December 2005. Volume 24, No. 6. http://content.healthaffairs.org/cgi/reprint/24/6/1478
4. “Financing the U.S. Health System: Issues and Options for Change.” Bipartisan Policy Center report. June 2008 Authors: Meena Seshamani, MD, PhD (John Hopkins School of Medicine), Jeanne M. Lambrew, PhD (Center for American Progress), Joseph R. Antos, PhD (American Enterprise Institute). http://www.rwjf.org/files/research/financingjune2008.pdf
5. “Pay-for-Performance: Will the Latest Payment Trend Improve Care?” JAMA, February 21, 2007—Vol 297, No. 7. Meredith B. Rosenthal, PhD, R. Adams Dudley, MD, MBA http://www.bridgestoexcellence.org/Documents/JAMACommentary.pdf
6. “Health Information Technology in the United States: Where We Stand, 2008”. Robert Wood Johnson Foundation Study. 2008. http://www.rwjf.org/files/research/3297.31831.hitreport.pdf
7. “The ONC-Coordinated Federal Health IT Strategic Plan: 2008-2012”. 6/3/08 http://www.hhs.gov/healthit/resources/HITStrategicPlan.pdf
8. “CPOE Lessons Learned in Community Hospitals.” Massachusetts Technology Collaborative. 12/06 http://www.masstech.org/ehealth/CPOE_lessonslearned.pdf
9. “Can Incentives for Healthy Behavior Improve Health and Hold Down Medicaid Costs?” Center on Budget and Policy Priorities. By Pat Redmond, Judith Solomon, and Mark Lin. 6/1/07 http://www.cbpp.org/6-1-07health.pdf
10. US Dept of Health and Human Services (HHS) Strategic Plan 2007-2012: Chapter 2- Healthcare http://aspe.hhs.gov/hhsplan/2007/hhsplanpdf/hhsplanc2.pdf

© 2010. Clinical Horizons, Inc. All Rights Reserved
Thank You for Your Time
Author Contact Information: Email: [email protected] Website: http://www.clinicalhorizons.com
Phone: 502-645-5776