Embed Size (px)
DESCRIPTION
CRRT Therapy Overview CRRT day 2013, Cairo, Egypt organized by Scribe. www.scribeofegypt.com
Citation preview

Dr. Michel HelmyMarketing Manager – Acute TherapiesSouth East Europe, Middle East & Africa
CRRT Workshop
CRRTTherapy Overview I
CRRTCRRTTherapy Overview ITherapy Overview I

© 2012 – Michel Helmy 2
Continuous Renal Replacement Therapy
Also known as “slow CContinuous RRenal RReplacement TTherapy”.
DefinitionDefinition
“Any extracorporeal blood purification therapy intended to substitute for impaired renal function over an extended period of time and applied for or
aimed at being applied for 24 hours/day24 hours/day.”
R. Bellomo, C Ronco and R. Mehta, Nomenclature for Continuous Renal Replacement Therapies, AJKD, Vol 28, November 1996

© 2008, Gambro 3
Renal Replacement – Why?
Removal ofwaste products
(solutes)
Removalof fluid
Regulationelectrolytes
(solutes)
Regulationacid-basebalance(solutes)

© 2012 – Michel Helmy 4
Removal ofwaste products
(solutes)
Removalof fluid
RegulationElectrolytes
(solutes)
Regulationacid-basebalance(solutes)
Prevent furtherkidney damage
RenalRecovery
Hemodynamicallysafe
Why Continuous Renal Replacement?

© 2012 – Michel Helmy 5
Day of treatment
0
20
40
60
80
100
120
140
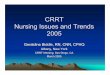
1 2 3 4 5 6 7 8 9 10 11 12 13 14
BUN (mg %)
CRRT IHD
Comparison between HD and CRRT
During iHD, serum levels of uremic toxins fall quickly but increase again quickly after the treatment. This saw-tooth urea profile cause significant changes in the serum osmolality –especially in the first treatment- and can result in a disequilibrium syndrome and additional fluid shift into the extra-vascular space.
In CRRT, the serum urea levels fall more slowly but continuously and can be maintained at a constant low level so disequilibrium syndrome can be avoided.

© 2012 – Michel Helmy
Why Choose CRRT?
• Slow, gentle and continuous• Well tolerated by hemodynamically unstable patient
• Prevent further damage to kidney tissue
• Promote healing and renal recovery
• Regulates electrolytes, acid-base balance
• Removes large amounts of fluid and waste products over time• Allow other supportive measures, i.e., nutrition
CRRT closely mimics the native kidney.
Bellomo, Ronco. Continous hemofiltration in the intensive care unit. Crit Care, 2000; 4(6)

© 2012 – Michel Helmy 7
Therapy Indications
WH0 ? … is our patientWH0 ?WH0 ? … is our patient

© 2012 – Michel Helmy 8
Indications for CRRT in the ICU(General Principals)
AEIOU
Bruce A. Molitoris. Critical Care Nephrology 2005. 151-154
Each illness that will be mentioned fits in at least one of these 5 principles, but mostly more. Sometimes an illness will cover all of them.
Acidosis (Diseases with metabolic acidosis due to acid-base imbalance)E.g. in ARF, ARDS, Sepsis
Electrolytes Imbalance (diseases with Electrolyte imbalance)E.g. in ARF, ARDS, Sepsis, MOF
Intoxications (water soluble toxins)E..g in Rhabdomyolysis
Overload (Fluid management in diseases with volume overload)E.g. in CHF, ARDS, Burns
Uraemia (ARF)

© 2012 – Michel Helmy 9
Clinical Indications .
Renal Indications• ARF with oliguria or anuria
• Azotemia (a medical condition characterized by abnormal levels of urea, creatinine, various body waste compounds, and other nitrogen-rich compounds in the blood as a result of insufficient filtering of the blood by the kidneys)
• Volume overload• Tumor lysis syndrome• Sepsis• Cerebral edema
Non-renal Indications• Drug overdose• Metabolic disorders (Lactic acidosis)
• Crush Injuries / Rhabdomyolosis(Myocyte “muscle” Necrosis)
Disintegration of striated/skeletal muscle Muscular cell components, myoglobin, released into circulation Resulting in electrolyte imbalance, hypovolemia, met. acidosis, coagulopathies, myoglobinuric RF
• Sepsis• ARDS• Fluid overload (e.g. 2ndry to CHF)
• Bellomo, Ronco. Continous hemofiltration in the intensive care unit. Crit Care, 2000; 4(6)• Schetz. Kidney International. 1999; 56:72. 88 – 94• Meyer, M. 2000 RRT; Critical Care Clin. 16 (1). 29

© 2012 – Michel Helmy 10
Clinical Indications .
Renal Replacement vs. Renal SupportRenal Replacements
• Life threatening indications:• Hyperkalemia(K>6.5 mmol/l)
• Acidemia(pH<7.1) due to metabolic acidosis• Pulmonary edema• Uremic complications (e.g. pericarditis)
• Solute control• Fluid removal• Regulation of acid-base• Regulation of electrolytes
Renal Support• Nutrition • Fluid removal in CHF• Cytokine manipulation (sepsis)• Cancer chemotherapy• Respiratory acidosis in ARDS• Fluid management in MOF
R.L. Metha. Blood Purification 2001; 19: 227-232

© 2012 – Michel Helmy 11
• Non-obstructive oliguria (urine output <200 mL/12 h) or anuria• Severe acidaemia (pH <7.1)because of metabolic acidosis• Azotaemia (urea >30 mmol/L)• Hyperkalaemia (K+ >6.5 mmol/L or rapidly rising K+ )• Suspected uremic organ involvement (pericarditis / encephalopathy / neuropathy
/ myopathy)• Progressive and uncontrolled severe dysnatremia (Na >180 or <115 mmol/L) • Uncontrolled hyperthermia• Clinically significant, diuretic-unresponsive organ edema (especially lungs)• Drug overdose with dialyzable toxin• Coagulopathy requiring the rapid administration of large amounts of blood
products in patients with or at risk of pulmonary edema / ARDS
The following is a proposed set of indications which can be used as triggers for initiating CRRT
R.Bellomo, C.Ronco. Critical Care 2000 – 4: 339-345

© 2012 – Michel Helmy 12
Indications generally used to start renal replacement therapy in standard clinical practice in patients with AKI
Biochemical indications• Refractory hyperkalaemia > 6.5 mmol/l
• serum urea > 30 mmol/l
• Refractory metabolic acidosis pH ≤ 7.1
• Refractory electrolyte abnormalities:
• hyponatraemia or hypernatraemia and hypercalcaemia
• Tumor lysis syndrome with hyperuricaemia and hyperphosphataemia
• Urea cycle defects, and organic acidurias resulting in hyperammonaemia, methymalonic acidaemia
Clinical indications• Urine output < 0.3 ml/kg for 24 h or absolute anuria for 12 h
• AKI with multiple organ failure
• Refractory volume overload
• End organ damage: pericarditis, encephalopathy, neuropathy, myopathy, uraemic bleeding
• Create intravascular space for plasma and other blood product infusions and nutrition
• Severe poisoning or drug overdose

© 2012 – Michel Helmy 13
Role of CRRT in ARF
Removal of toxins (urea, creatinine)Regulate electrolyte and water balanceRegulate acid-base balancePrevent further damage to the kidney tissuesPromote healing and renal recovery

© 2012 – Michel Helmy
Role of CRRT in CHF
Maintain 24/7 fluid balance (All CRRT therapies)• Reduce ascites and peripheral edema• Relieve Pulmonary edema
Normalize cardiac filling pressuresMaintain 24/7 Electrolyte and acid/base balance (CVVHD, CVVHDF)
• - Dialytic control of electrolytes• - Delivery of bicarbonate or lactate buffer
Possibly prevent further renal damage or prolong renal InsufficiencyPossibly reduce length of stay
Refractory Congestive Heart Failure: Overview and Application of Extracorporeal Ultrafiltration, Paul Blake and Emil P. Paganini, Advances in RRT, Vol 3, No2 (April), 1996: pp 166-173

© 2012 – Michel Helmy 15
Role of CRRT in Sepsis
Removal of middle to large molecule septic mediators by convection and adsorption including TNF-α, IL-1, IL-6 and IL-8 through:Removal of excess fluid and waste productsMaintenance of acid-base balanceImprove cardiovascular hemodynamic → removal of cardiodepressants (caused by inflammatory mediators)Thermoregulation
Bruce A. Molitoris. Critical Care Nephrology 2005. 28-34

© 2012 – Michel Helmy 16
Role of CRRT for RhabdomyolysisMaintain fluid, electrolyte, acid/base balance.Prevent further damage to kidney tissueRemoval of small to middle protein molecules - 17,000 Dalton through convection
• May cause nuisance BLD alarms
Example of reduction ofpigmentation In Ultra-Filtration fluid over 3 days of treatment

© 2012 – Michel Helmy 17
Role of CRRT in Intoxications
Removal of small molecules by Dialysis• Dialysate up to 4l/h• Optional replacement up to 500ml/h
Duration: depends on clearance of toxic medication