Embed Size (px)
DESCRIPTION
Ct & mr enterography
Citation preview


Introduction
• There was a time when small-bowel follow-through (SBFT) was the primary method of diagnosing diseases of the small bowel.
• Endoscopic methods for evaluating the small bowel, including ileocolonoscopy, capsule endoscopy, and double-balloon enteroscopy, offer distinct advantages for assessing superficial mucosal abnormalities and obtaining biopsies for histologic assessment. However, endoscopic evaluation is invasive and may be limited by bowel strictures, and techniques such as double-balloon enteroscopy and wireless capsule endoscopy require special equipment and expertise that are available only at large tertiary-care centers. Moreover, no endoscopic technique allows assessment of extraenteric abnormalities.

• In recent years, there has been renewed interest in small bowel imaging using a variety of techniques such as ultrasound(US), contrast enhanced ultrasound (CEUS), computed tomography (CT), magnetic resonance imaging (MRI), computed tomography enteroclysis/enterography (CTEc/CTEg) and magnetic resonance enteroclysis/enterography ( MREc/MREg) and the small bowel endoscopic methods.
• CT and MR enterography have proven superior to conventional barium examinations since they provide essential information about transmural and extramural involvements, and about the complications that may determine surgical treatment (obstruction, fistulas, abscesses).

CTE

Introduction
• CT enterography was first introduced by Raptopoulos et al in 1997 as a modification to ‘‘standard’’ abdomino-pelvic CT examination to specifically examine the small bowel in detail, notably to assess the extent and severity of Crohn’s disease.
• They combined neutral (low-density) oral contrast with ‘‘enteric phase’’ CT to optimise contrast resolution between mucosa and lumen, thereby maximising conspicuity of abnormalities arising from the small bowel wall.

• Several authors have subsequently described similar techniques, which are broadly categorised into:– CT enterography (where patients drink oral contrast) and
– CT enteroclysis (luminal contrast is introduced via a nasojejunal tube placed fluoroscopically prior to CT examination).
• Although superior jejunal distension is attained using enteroclysis, the convenience, efficiency and superior patient experience achieved with CT enterography make it the preferred technique at many institutions.

Technique
• The technique of CT enterography combines – small bowel distension with a neutral or low-density oral
contrast mixture and – abdomino-pelvic CT examination during the enteric phase
following administration of intravenous contrast.
• Patients drink approximately 1.5–2 l of oral contrast over 45–60 min.
• Patient compliance is central to the success of CT enterography, and supervision and encouragement during the drinking phase is recommended.
• Optimising luminal distension will facilitate rapid and efficient luminal navigation, enabling accurate detection and characterisation of abnormalities.

Luminal contrast and distension
• Neutral or low-density oral contrast media are a prerequisite for good-quality CT enterography because:
– they maximise contrast between the lumen and enhancing small bowel wall,
– facilitating assessment of mucosal thickening and wall stratification/enhancement patterns

Oral Contrast Agents
• Water
• Water–methylcellulose solution
• polyethylene glycol,
• commercially available low-density barium,
• 0.1% Volumen (Bracco, Milan, Italy) and
• Milk
• Positive oral contrast agents

• Water– inexpensive, well tolerated by patients, and effective for distending
the stomach, duodenum, and jejunum. – inadequate distension due to rapid reabsorption
• polyethylene glycol (PEG) electrolyte solution– Gastrointestinal side-effects
• Volumen; E-Z-EM, Westbury, NY• 0.1% w/v ultra-low-dose barium with • sorbitol, a nonabsorbable sugar alcohol
– promotes luminal distention and – limits resorption of water across the length of the small bowel.– The attenuation of low-concentration barium is only 20 HU. – Fewer side effects than are associated with PEG.– Unpleasant taste & loose bowel movements or diarrhea very soon
after the scan
• Milk– similar results as Volumen, – less expensive – freely available in Europe, – it may be deemed unpalatable by many patients when drunk in large
volumes.

• Positive oral contrast agents (containing iodine or barium) – not routinely used for CT enterography – they obscure mucosal enhancement, intraluminal haemorrhage
and assessment of subtle mural disease.– problematic in creating three-dimensional images if CT
angiography is concurrently being performed—for example, in the assessment of gastrointestinal blood loss.
• may be preferred for some clinical situations – establish fistula patency– exact site of mechanical obstruction– known serosal disease, – detection of some primary tumors, and – patients with an iodine allergy.

Optimal Volume
• Maglinte stated that a volume of less than 1.5L is unlikely to be sufficient to adequately distend the small bowel without active inflammation, and a subcentimetre mass could be missed; although,according to many authors, good-quality examinations can be achieved with smaller volumes.

• For the evaluation of the upper small intestine only, – patients drink a total of two 450-mL bottles of the agent, with a
10-minute interval between each bottle.– Water achieves the same results, is less expensive, and is better
tolerated by patients.
• For the evaluation of the complete small intestine,.– Patients are given three 450-mL bottles, each of which is
consumed at about 15-minute intervals. The last 150 to 200 mL is consumed just before the patient gets on the scanner.
• In small patients and patients with history of previous small bowel resection– smaller volumes of oral contrast may be sufficient, judged
mainly by patient tolerance.

Recommended protocol
• Avoid solid food for at least 6 h prior to examination to decrease the possibility of mischaracterising solid food residue as true luminal pathology.
• Patients can liberally drink clear fluids to maintain hydration prior to examination.
• Outside the scanner room, patients are then encouraged to drink the oral contrast.

Intravenous Contrast
• In addition, intravenous contrast is an essential component of CT enterography.
• It enables evaluation of:– wall thickening,
– mucosal enhancement,
– the supplying and draining blood vessels, and
– the presence or absence of GI bleeding.
• 100 to 125 mL of intravenous contrast at a rate of 3 to 5 mL/sec, initiating the scan acquisition after a 60-second delay.

• Maximal small bowel enhancement on MDCT has been reported by Schindera et al to be 50 s after administration of intravenous contrast or 14 s after aortic peak enhancement.
• Therefore administer contrast intravenously during this enteric phase.
• The enteric phase is similar to the pancreatic phase; therefore, CT enterography also optimises demonstration of most pancreatic neoplasms.
• This is particularly relevant for clinicians, given that symptoms of pancreatic tumour can mimic luminal disease.
• However, lack of portal venous phase imaging is rarely a problem for patients undergoing CT enterography because subtle liver metastases are rarely the target of imaging in this patient group.

Alternatively…
• Acquisition of both arterial and venous phase images at 30s and 60s respectively.
• The arterial phase images are critical for:– appreciating subtle bowel wall for mucosal hyperenhacement– engorgement of the adjacent vasa recta, all of which are
important signs of bowel inflammation.
• The venous phase images are important not only for – evaluating the bowel, but also the – other parenchymal organs of the abdomen (i.e., liver, spleen,
etc.), – the extraenteric manifestations of Crohn’s disease, – the venous mesenteric vasculature, and – hypovascular bowel tumors.

• Images are acquired with thin collimation, with acquisition of 0.625-0.75 mm slices, which are then reconstructed into 3-5 mm axial slices for routine interpretation.
• Coronal and sagittal multiplanar reconstructions are directly created at the CT scanner following the acquisition of the axial source images.
• At the same time, isotropic 0.5-0.75 mm images are used for 3-D post-processing.

3-D TECHNIQUE
• two separate sets of 3-D reconstructions:– Maximum intensity projection (MIP) imaging
• Effective for evaluation of the mesenteric vasculature• Not only the main aortic branch vessels, but also tiny mesenteric
branches which are typically not readily visualized on the axial source images.
• Areas of bowel hyperemia and mesenteric vascular engorgement (i.e., “comb sign”, opacification of the vasa recta) are also easily identified using this technique;
– Volume rendering (VR)• most useful in displaying the entirety of the small bowel, and
illustrating the relationship of adjacent small bowel loops, subtle areas of bowel wall thickening, abnormal mucosal enhancement, and extra-enteric manifestations of Crohn’s disease

Certain medications may be helpful but are optional.
• Metoclopramide (10 mg)
– given orally 75 minutes before the CT scan
– stimulates gastric emptying.
• Glucagon (1 mg) OR Buscopan (20mg)
– administered intravenously immediately prior to scanning
– decrease small bowel peristalsis.

Precautions
• To avoid intravenous contrast-induced nephropathy, – limit the use in frail and diabetic patients. – consider reducing the volume of intravenous contrast, – ensure patients are well hydrated before the examination and – monitor renal function closely afterwards.
• A large volume of oral contrast is contraindicated – who are fluid-restricted owing to clinical conditions such as
renal or heart failure.
• Following CT enterography examination, patients are encouraged to remain in the radiology department for approximately 45 min because they reasonably frequently experience severe, albeit short-lived, diarrhoea.

Variations to the basic protocol -Multiphase Scan
• In patients where active gastrointestinal bleeding is suspected (and endoscopic work-up is negative) a multiphase scan protocol can be used to identify sites of occult gastrointestinal bleeding.
• This protocol would frequently include pre-contrast, arterial, venous and delayed phase CT examinations of the abdomen and pelvis.
• Rarely, this can be used in emergency situations to identify the site of bleeding.
• However, the radiation burden is approximately three times higher, and therefore potential radiation risks should be balanced against patient benefit.

Indications for CT Enterography

LOW-DOSE CT TECHNIQUE
• peak incidence of Crohn’s disease is in patients between the ages of 20-40 years;
• a sizeable percentage of cases are diagnosed in children (15%); and
• the disease has a mild female predominance
i.e. radiation sensitive population,

Dose-reduction Techniques
• These include– automated tube current modulation, which alters the
tube current (mAs) based on the patient’s size and density;
– automated tube potential modulation, which alters the scanner’s tube potential (kVp) based on the patient’s size and density; and
– iterative reconstruction, an alternative to traditional filtered back projection reconstruction techniques, which allows the acquisition and reconstruction of diagnostic quality images at far lower radiation doses

The Future
• CT enterography will continue to be incorporated into wider clinical measures of Crohn’s disease, particularly given the promise that objective CT findings such as mural hyperenhancement can be quantitated.
• Continuing technical developments in CT image reconstruction will substantially reduce the radiation dose at CT enterography, which is already the same or less than routine abdominal CT.

• The use of dual-source CT systems will permit wider use of low-energy CT scanning, which will – increase the conspicuity of hypervascular
inflammation and – permit further radiation dose reduction.

Low-Dose 18F-FDG PET/CT Enterography• Low-dose 18F-FDG PET/CTE, compared with CTE,
may improve the detection and grading of active inflammation in patients with Crohn disease.
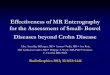
CTE demonstrates mural thickening and mucosal enhancement in loop of ileum (arrow) involved with Crohn disease. Corresponding 18F-FDG uptake is seen on PET. Excellent anatomic registration of PET and CTE findings on PET/CTE

PET/CTE also may reveal clinically significant findings, such as enterocolic fistula, not evident on PET or CTE alone.
Axial CTE image (A) demonstrates thickened loop of ileum (white arrow) in pelvis and unremarkable adjacent loop of sigmoid colon (black arrow). No fistula was appreciated on CTE. Corresponding 18F-FDG PET image (B) reveals increased tracer uptake in ileum (arrow) consistent with active Crohn disease; however, anatomic detail is insufficient to suggest enterocolic fistula. Fused PET/CTE image (C) clearly demonstrates 18F-FDG uptake (arrow) bridging ileum and sigmoid colon, with focal uptake present in wall of sigmoid colon. PET/CTE diagnosis of enterocolic fistula was confirmed at surgery.

MRE

Technique
• A combination of good bowel distention and ultrafast MRI sequences is required to obtain diagnostic small-bowel images.

Contrast Media Usedfor MR Enterography
• The first MR enterography studies were performed without oral contrast (Shoenut et al. 1993, 1994).
• One study that compares MR enteroclysis with MRI without oral contrast has found that the reliability for luminal findings increases when luminal contrast is given (Wiarda et al. 2009).

Good Contrast Agent
• Important features of a good contrast agent are:
– high contrast resolution between the bowel wall and the small bowel lumen and
– homogeneous signal intensity of the lumen.

Classification
• Contrast media can be classified according to how they appear on T1- and T2-weighted images.
• Negative contrast agents give low signal intensity on T1- and T2-weighted images (“dark lumen”), whereas positive contrast agents produce high signal intensity on T1- and T2-weighted images (“bright lumen”).
• Biphasic contrast agents give high signal intensity on one sequence and low signal intensity on the opposite sequence.

Positive Oral Contrast Agents
• Paramagnetic substances based on gadolinium-chelate, ferrous or manganese ions.
• An increase in signal intensity at T1-weighted sequences (appearing as bright lumen) is caused by the paramagnetic effect that causes a reduction in the T1 relaxation time.
• There is no effect on T2 relaxation time in the concentrations used in clinical practice, so on T2-weighted images the signal intensity is also high because of the high water content of the contrast agent.

• Wall thickening is demonstrated well by positive oral contrast agents.
• A limitation of positive oral contrast agents is that the luminal high signal intensity at T1-weighted sequences may interfere with the enhancement of the bowel wall after the administration of intravenous contrast.

• Gadopentate dimeglumine (Magnevist Enteral, Schering AG, Berlin, Germany)– 1.0 mmol/L gadolinium-DTPA with – 15 g/L mannitol
• to reduce water reabsorption in the bowel
– Mild side effects (flatulence, diarrhea, and thin stools) occur in 11% of patients. These are caused by the addition of the mannitol.
• Ferric ammonium citrate– mixture of granular and crystalline powders based on iron salt with
paramagnetic effects, and has to be dissolved in water (600–1,200 mg in 600 mL).
– Some patients (15%) report minor gastrointestinal side effects
• natural substances– milk, green tea, and blueberry juice appear bright on MR because the
contents of these substances shorten the T1 relaxation time. – Limitation of these positive contrast agents is that their signal intensity is not
constant through the gastrointestinal tract.

Negative Oral Contrast Agents
• Superparamagnetic substances that are based on iron
• They act by inducing local field inhomogeneties, thus resulting in shortening T1 and T2 relaxation time.
• The signal intensity on both T1- and T2-weighted images is thus much lower (“dark lumen” appearance).

• These local field inhomogenities could hypothetically lead to an underestimation of bowel wall thickness.
• The hypointense bowel wall is visualized due to the negative contrast in the bowel lumen and the high signal intensity of the mesenteric fat.
• The pathologic bowel wall is hyperintense after contrast injection and the lumen remains hypointense.
• Fat suppression is recommended to suppress the high signal intensity of the mesenteric fat for optimal contrast after intravenous contrast injection.

• Ferumoxsil (Lumirem; Laboratoires Guerbet, Paris, France) contains
– superparamagnetic particles of iron oxide coated in a layer of silicone that prevents it from being absorbed by the small bowel.
• Side effects include mostly minor gastrointestinal symptoms

Biphasic Oral Contrast Agents
• now the most widely used
• have low signal intensity on T1-weighted images and high signal intensity on T2-weighted images.
• On T1-weighted images, the contrast between the enhancing bowel wall and the dark lumen is optimized.

• These agents include:– water,
– methylcellulose,
– mannitol (2.5%),
– mannitol (2.5%) with locust bean gum (0.2%),
– sorbitol (2%),
– VoLumen (EZ-E-M, Westbury, NY), and
– polyethylene glycol (used as a cathartic agent for colonoscopy)

• Optimal contrast agents (eg, mannitol, locust bean gum, and polyethylene glycol) are hyperosmolar to prevent their absorption across the intestinal mucosa and thereby maximize luminal distention, in contradistinction to less effective agents such as water and methylcellulose.

Note!!!
• It should be noted that most, if not all, hyperosmolar oral contrast agents may cause gastrointestinal side effects — notably, diarrhea. This often occurs within 1 hour of ingestion, and all patients should be warned of this possibility before undergoing the study, so that they may plan the timing and method of their travel home from the hospital.

• Water has been used as a luminal contrast agent, as it has several advantages:
– it is widely available, cheap, and safe.
• A disadvantage is that it is rapidly absorbed, often before it reaches the terminal ileum.
• Therefore, various additives have been proposed to diminish intestinal absorption.

• Mannitol is an osmotic agent that can be added, but can also cause osmotic effects such as diarrhea and cramping.
• Nonosmotic agents such as locust bean gum (a thickening agent extracted from the seeds of the European carob tree) can also be used or in combination with mannitol.

• Polyethylene glycol solution (PEG), often used as a bowel cleansing agent, is a poorly absorbed carbohydrate that retains fluid in the bowel lumen.
• PEG binds water molecules preventing their rapid absorption.
• As a secondary effect, it promotes peristalsis and leads to the evacuation of bowel contents several hours after ingestion.
• Good distension has been achieved with the administration of 600mL; increasing the dosage did not improve distension.
• Similar to mannitol, PEG can cause side effects such as cramping and diarrhea.
• PEG is less appreciated by patients because of its salty taste.

• Barium sulfate, often used in conventional fluoroscopic exams, can be used as biphasic contrast agent.
• The signal intensity depends on the concentration.
• The advantage of barium sulfate is the high safety and low cost. It is also widely available.
• The taste is a drawback for the use of barium sulfate. Gastrointestinal side effects have been reported

Enteric contrast agents for MR imaging.

Technique
• A specific protocol for MR enterography requires that the patient fast for 6 hours before the procedure. – decreases the amount of food residue and debris in
the intestinal lumen that can be mistaken for mass lesions or polyps.
• Unless contraindicated, patients also follow a low-residue diet for the preceding 5 days. – promotes reduction of fecal matter in the colon,
which facilitates transit of the small-bowel contrast agent because fecal material can delay transit times in the small bowel.

• It is advised to aim for a total of 1.5 L, some patients cannot tolerate this volume, and adequate results may still be achieved with as little as 500 mL.
• An oral suspension that contains 20 mg of metoclopramide is given with the first aliquot to promote gastric emptying.
• Just before imaging, patients are asked to drink another 200 mL of contrast material to opacifythe stomach and duodenum.

Precaution!!!
• Colonoscopy with electrocoagulation should not be performed directly after an MR enterography with a mannitol solution. This as methane and hydrogen are formed when mannitol dissociates.

Rectal contrast administration
• Some authors have advocated concomitant administration of a warm rectal enema to improve the depiction of the entire colon and the distension of the terminal ileum.
• However it is not routinely performed, but when required, 1-1.5 l of warm saline can be administered via the rectum, depending on the patient tolerance.
• Antegrade colonic filling is also possible and well tolerated, although it does not provide an optimal colonic distension.

An Alternative!!!
• Two-step techniques have also been described in which the patients drink:
– 2 l of PEG solution 2-4 h before the examination, and then
– 1.2-2 l of solution, 45 min before the examination.

Imaging Timing
• Although rapid transit to the right colon (<20 minutes) in seen in some patients, most patients require a delay of at least 40–60 minutes from contrast material ingestion to imaging
• Some advocate imaging patients twice (eg, after 20 minutes to best visualize the distended jejunum and then at 45 minutes for evaluation of the ileum),

Intravenous Contrast Agents
• Detection of active inflammation can be improved by the administration of intravenous contrast, especially in patients with CD.
• A study with dynamic MRI has shown that the mean peak enhancement in patients with active CD is after 39 s (±19 s) (Florie et al. 2006).
• Administer Gadolinium (0.1 mL/kg) and start with the postcontrast series after 60 s.
• In patients with renal impairment (low glomerular filtration rate) or pregnancy, the usage of intravenous contrast is contraindicated.

Anti-Spasmolytic Agents
• To prevent blurring or artifacts due to peristalsis
• N-butyl scopolamine bromide (Buscopan, Boehringer, Ingelheim, Germany)– Not approved for this use by the FDA
– lower costs
• Glucagon– aperistalsis has been reported to be significantly
longer
• intravenously just before the contrast-enhanced sequence

Technique
• 1.5-T imagers
• Large-gradient body coils are necessary for adequate resolution and a sufficiently large field of view.
• fast imaging techniques
• Performed in breath-holds (usually between 15 and 25s)
• For breath-holds over 15 s, hyperventilation directly prior to the sequence is advised.
• Good explanation of the procedure and length of the breathhold is mandatory.

Patient position
• Prone imaging– compression of the bowel loops resulting in better loop separation and can
give some reduced scan coverage due to a smaller bowel cavity in the coronal plane, which in turn reduces the length of breath hold required, resulting in improved patient compliance.
– It has also been shown to improve small bowel distention.
• Supine position– more comfortable, especially in older individuals.– normally required in patients with stomas and abdominal wall fistulas, or in
those who cannot lie prone.
• In a study that investigated this subject, prone scanning position did lead to improved small bowel distension but not to improved lesion detection (Cronin et al. 2008).

Imaging Protocol
• An initial thick-slab (50 mm) T2-weighted MR cholangiopancreatographicsequence (HASTE) helps to determine whether the oral contrast agent has reached the ileocecal junction.
• Once the contrast material reaches the ileocecal junction, an IV injection of 1 mg of glucagon is administered to minimize bowel peristalsis.
• If bowel obstruction is observed on thick slab HASTE images, MR fluoroscopy of the affected segment may be performed to assess for inflammatory adhesions or strictures before injection of antiperistaltic drugs.

Half-Fourier Single Shot RARE (HASTE)
• Performed in the axial and coronal plane images with a strong T2-weighting short acquisition times (less than 1 s per slice), breathing artifacts are minimal.
• Normal bowel wall has low signal intensity on HASTE sequences, an increased signal intensity can be seen in edematous lesions (inflammation).
• sensitive to intraluminal flow-void artifacts.– because of peristaltic motion,
– limited by spasmolytic drugs
• used for measuring wall thickness,– because it is not sensitive to the chemical shift
artifact.
• performed using fat suppression.– To differentiate between Fat and edema
(intramural edema of the bowel wall is indicative of inflammation)

Balanced Steady-State Free Precession (True-FISP)
• (true Fast Imaging with Steady-state Precession; True-FISP)
• More complex in generation of tissue contrast.
• This tissue contrast comes from both T1 and T2 in a ratio, namely the T2/T1 ratio.
• A higher ratio corresponds with higher signal intensity.
• At 1.5 T, the bowel wall has an intermediate to low signal intensity and fluids have a high signal intensity.
• provide high contrast between the bowel wall, lumen, and mesentery.
• Flow-void (motion) artifacts are not so common
• The most common artifact in the true-FISP sequence is the black boundary artifact, due to chemical shift.– however, fat suppression helps in reducing
the effects of this artifact

Balanced Steady-State Free Precession (True-FISP)
Black boundary artifact Not seen with fat saturation

T1-Weighted Sequences
• Contrast-enhanced T1-weighted gradient echo sequences with fat suppression– to assess whether there are areas of increased
enhancement
• either two-dimensional (2D) or three-dimensional (3D).
• Commonly used is the 3D T1w interpolated volume imaging sequence (3D VIBE: Volumetric Interpolated Breath-Hold Examination or comparable sequences)
• To reduce the acquisition time, small flip angles and short TR (repetition time) are used.
• recommend a precontrast coronal series and coronal and axial postcontrast series to optimal assess the bowel wall enhancement.
• 3D ultrafast gradient echo sequences are sensitive to bowel peristalsis, so spasmolytic drugs are advised.– an additional 10 mg of hyoscine butylbromide or 0.2 mg of
glucagon prior to gadolinium-based contrast material injection (0.2 mg/kg).

Coronal True FISP image: normal bowel. The ‘black boundary’ artefact may be confused with bowel wall thickening (arrows)
Coronal T1 fat-saturated post-contrast image: normal bowelwall shows mild homogeneous enhancement
Coronal fat-saturated HASTE image: normal bowel. Intraluminal flow voids (arrow) are seen, as this sequence is sensitive to fluidmotion


• The imaging plane in these sequences is
– aligned parallel to the bowel segments
• to allow detailed visualization of mucosal irregularitiesand
– aligned perpendicular to the bowel
• to provide accurate visualization of transmural ulcers, fistulas, sinus tracts, and periintestinal abnormalities.
• The total in room time of the examination is approximately 30 - 45 min.

Pitfalls
• suboptimal distention of bowel loops can be encountered more commonly. – Early mural changes of Crohn disease may be
overlooked in areas of collapsed bowel segments. – Partial strictures may also not be identified because of
inadequate distention of the bowel.
• Artifacts due to peristalsis or flow voids are more prominent on HASTE sequences. – Intraluminal food debris may simulate filling defects
or polyps; a low-residue diet and fasting before examination help in reducing these artifacts.
• Previous surgery, particularly stricturoplasty, may mimic tumors with a shouldered margin or fibrotic strictures. – Observation of these segments in all three planes
helps in distinguishing stricturoplasties from tumorsbecause stricturoplasties typically have a lobulated or bi- or trifoliate appearance. Coronal HASTE image with fat
saturation (4-mm thickness) shows linear filling defect in bowel lumen (arrow) due to peristalsis

NEW SEQUENCES AND TECHNIQUES

Diffusion-Weighted Imaging (DWI)
• DWI at MR enterography has been researched recently in one small study of 11 patients for detection of active CD (Oto et al. 2009).
• In patients with active CD, ADC values are decreased, indicating diffusion restriction.
• The sensitivity for detecting inflammation with DWI was 95% and specificity 82%.
• More studies have to be performed to test the reproducibility of these data and the relevance in comparison with other MR findings.
• Hence it is suggested that DWI may have a role in imaging of patients for:– whom IV contrast administration is
contraindicated or – who cannot tolerate oral
preparation.

Cine Imaging / MR fluoroscopy
• to obtain information about peristalsis and bowel motion.
• allow both qualitative and quantitative assessment of bowel motility.
• The most common indication is the diagnosis of adhesions, which are visualized by fixation of bowel loops and lack of normal peristalsis.
• This is best seen on true-FISP images• a frame rate of 0.5–2 sections per second along
the long axis of the affected segments.

Magnetization Transfer Imaging
• role in imaging of fibrosis in Crohn disease
• Magnetization transfer imaging reflects the transfer of energy from protons in free water molecules to those associated with large molecules such as collagen.
• Fibrotic tissues therefore have a high magnetization transfer effect.
• An in vivo study of nine patients with ileal Crohndisease showed the magnetization transfer ratio was highest in patients with a stricturing disease phenotype, supporting the use of MRI to image enteric fibrosis

Future Prospects of MR Enterography
• Research now is focused on: – creating abdominal 3 T protocols, – studying perfusion and diffusion and – obtaining more insight into the role of MRI in determining disease
activity in CD.
• New techniques are being developed to assess bowel wall enhancement in a more objective manner. With the creation of so-called T1-maps, the absolute T1-value can be calculated and therefore the absolute contrast enhancement.
• Recently, more research is being performed on dynamic contrast-enhanced MRI (DCE-MRI) in CD. Mural hemodynamic parameters derived from DCEMRI were reported to be correlated with disease chronicity and microvessel density was inversely related to mural blood flow (Taylor et al. 2009).

ENTEROGRAPHY INTERPRETATION: HOW TO REVIEW AND AVOID PITFALLS

Reading Technique
• Careful luminal navigation from the gastro-oesophageal junction to the anus, or vice versa.
• Can take several minutes (up to 15 min in some patients) and can be thwarted by poor luminal distension or collapse, particularly when there is minimal intra-abdominal fat separating loops.
• Use of a multiplanar review will improve accuracy of both luminal navigation and interpretation

• first distinguish abnormal from normal segments.
– differential contrast enhancement is a cardinal sign of many small bowel pathologies.
– hyperenhancing mass
– focus of wall thickening.

• The jejunum occasionally is collapsed at enterography, which can be a normal finding in the minority of cases, but the ileum almost always is distended adequately.
• the enteric phase of enhancement the jejunum enhances more than the ileum.
• This should not be mistaken for pathology.
Normal CT enterography. Coronal CT enterography image showing normal jejunal(short arrows) and ileal (long arrrows) loops. Note the prominent mucosal pattern inthe proximal jejunal loops.

• Furthermore, collapsed bowel loops appear to enhance more than the distended loops in the same segment.
• In the non-distended loops, other signs of disease must be used to diagnose pathological processes, including associated changes in the adjacent small bowel mesentery such as hypervascularity, fat stranding or lymphadenopathy.
Collapsed small bowel. Axial CT enterographyimage showing a collapsed small bowel mimicking pathology (long arrow) compared with a normal fluid-filled loop (short arrow). Note the absence of any associated changes.

• Focal small bowel spasm is frequently encountered, despite the use of Buscopan, and can mimic short strictures.
• Identification of similar areas of spasm, lack of mucosal hyperenhancementand absence of mesenteric abnormality helps to distinguish spasm from true pathology
Small bowel spasm. Axial CT enterography image showing two areas of focal small bowel spasm mimicking pathology (arrows). Note the absence of any associated changes.

• Repeat scanning through the section of interest is often useful to distinguish stricture from a collapsed loop, but clearly the dose of ionising radiation imparted by CT makes this less applicable than during MRI enterography.
• As noted above, multiplanar reformatting when reporting CT enterography has been shown to increase diagnostic confidence and sensitivity.

Characterisation of small bowel pathology
• Interpretation of small bowel abnormalities can be divided into:
– Luminal (Wall, Fold and Mucosal) changes
– Extra Enteric changes
– Colonic abnormalities

Characterisation of small bowel pathology
• Interpretation of small bowel abnormalities can be divided into:
– Luminal (Wall, Fold and Mucosal) changes
– Extra Enteric changes
– Colonic abnormalities

Intestinal ulcers
• An aphthous ulcer may be seen on high-resolution MR images as a nidus of high signal surrounded by a rim of moderate signal intensity.
• The presence of aphthous ulcers provides strong evidence for Crohn disease in the appropriate clinical setting.
• Aphthous ulcers are also seen in other conditions such as infections, tuberculosis, and ischemic enteritis, but aphthousulcers are encountered less commonly in these entities than in Crohn disease.
Axial FIESTA images show mural thickening of the terminal ileum with submucosal edema and irregular mucosal surface with some focalulcerations (white arrows).

• Advanced inflammation in Crohn disease manifests as deep ulcerations and a cobblestone mucosal appearance.
• Deep transmural ulcers manifest as linear, high-signal-intensity protrusions into the bowel wall on fast imaging with steady-state precession (FISP) and HASTE sequences.
• True FISP images have a black boundary artifact that may mask smaller transmuralulcers. Coronal true fast imaging with steady-state
precession image obtained with fat saturation shows thickened, inflamed segments of ileum with deep ulcers seen as high-contrast protrusions within bowel wall (arrow).

• Axial HASTE image shows good bowel distention, a short terminal ileal stricture, wall thickening, and a deep rose thorn ulcer (arrow), findings that are infrequently seen at enterography

• Early and superficial ulceration is not well demonstrated even with full luminal distention at MR imaging or CT, and well-performed conventional fluoroscopy still holds an advantage
MR enterogram shows no ulceration in an asymmetrically thickened terminal ilealsegment (arrowhead) lying adjacent to the transverse colon (arrow).
Image from a small bowel follow-through study clearly shows ulceration in the terminal ileal segment..

Wall thickening
• Although this feature is not entirely specific for Crohn disease, any thickening of the small bowel wall greater than 3 mm should be considered abnormal.
• In patients with small bowel Crohn disease, wall thickness usually ranges between 5 and 10 mm.
• The black border artifact seen on true FISP images can complicate the assessment of bowel wall thickness. Bowel wall thickness is more accurately assessed with a HASTE sequence

Fold Pattern
• Three main alterations in fold pattern are recognized:
– the picket fence pattern of diffusely thickened folds,
– a reduction in or distortion of folds due to ulceration, and
– cobblestoning.

(a) picket fence pattern of diffusely thickened folds,
• 47-year-old man with proven Crohn disease.
• Coronal HASTE image shows nodular (arrow), thickened, and asymmetric folds in distal ileum (arrowhead).

(a) picket fence pattern of diffusely thickened folds,
Small bowel Crohn disease in a 66-year-old man who had previously undergone right hemicolectomy and presented with recurrent symptoms. Axial (a) and coronal (b) HASTE images show a small volume of free fluid between small bowel mesenteries (arrows), but no loculation, encapsulation, or mass effect as would be expected with an abscess. There is a “picket fence” pattern of fold thickening in the neoterminal ileum, along with wall thickening (arrowheads).

(b) reduction in or distortion of folds due to ulceration
Distortion or blunting of the mucosal folds and thickening of the valvulae conniventes. (A) Coronal SSFSE image shows thickening and blunting of valvulae conniventes of the terminal ileum with a pseudopolypoid appearance (white arrows in (A).(B) Endoscopic view shows mucosal ulcers and edema (black arrows) in the terminal ileum.

(c) Cobblestoning
• It manifests as sharply demarcated patchy areas of both high and moderate signal intensity within an affected bowel wall segment caused by longitudinal and transverse ulceration, producing a cobblestone pattern.
• This finding is best appreciated on true FISP images, which are less sensitive to intraluminal flow void.
• Although cobblestoning is best seen in well-distended bowel at MR enteroclysis, it can also be identified on good-quality MR enterograms.
• The mesenteric border is preferentially affected in Crohn disease

Stricture
• defined as functionally significant if there is upstream bowel dilatation greater than 3 cm, or
• as nonfunctional if there is a greater than 10% narrowing in the bowel lumen compared with normal adjacent bowel in the absence of dilatation.
• In Crohn disease, strictures are invariably associated with a segment of thick-walled bowel, whereas adhesive strictures do not demonstrate this finding.
• However, in isolation, a stricture with wall thickening does imply an extensive differential diagnosis, which includes infections, radiation enteritis, or neutropenic enteritis in immunocompromised patients (in the latter two conditions, an appropriate antecedent history would be expected) and malignancies such as carcinoid tumors and lymphoma.

Acute Wall Edema
• Higher than normal wall T2 signal intensity, best seen as longitudinal intermediate signal intensity (within what is normally hypointense bowel wall) affecting the thickened bowel wall on fat-saturated HASTE images, may be related to mucosal or submucosal edema and has been shown to correlate with independent indexes of Crohn disease activity.
• Axial HASTE image shows higher than normal wall signal intensity (arrowhead).
• Axial fat-saturated HASTE image shows apparent wall edema from active inflammation in the defunctioned segment (arrowhead)

• In a histology matched study, the mural signal intensity on T2-weighted images was compared with cerebro-spinal fluid (CSF) signal intensity.
• The ratio of these signal intensities (T2 mural/CSF) was positively correlated with histology (a higher ratio denotes a more inflamed bowel wall)(Punwani et
al. 2009).

• This may allow differentiation from fibrotic wall thickening, which usually has low to moderate T2 signal intensity on true FISP and HASTE images.
• However, the absence of wall hyperintensitydoes not exclude active disease, whereas the presence of high signal intensity can result from intramural fat deposition, found in chronic strictures.

Chronicity and Wall Fat
• Fatty infiltration of the bowel wall may occur in chronic IBD, and both the small bowel and colon may be affected.
• Notably, however, intramural fat deposition is a nonspecific finding that can be seen not only in other causes of chronic bowel inflammation, but also in the setting of obesity, steroid use, and diabetes.

• Generally, fat-saturated and non-fat-saturated T2-weighted HASTE sequences are required to differentiate fat from wall edema, with the latter demonstrating persistent high signal intensity with both sequences, whereas fat saturation will reduce wall signal intensity that is due to fat.
• Gradient-echo (FISP) sequences demonstrate chemical shift artifact in the presence of intramural fat.
Intramural fat in a patient with chronic ileal Crohn disease. (a) HASTE image shows focal midilealwall thickening with associated linear intramural high signal intensity (arrow). (b) Gradient-echo FISP image shows chemical shift artifact as a thin black stripe in the corresponding location (arrow), a finding that confirms the presence of intramural fat rather than edema.

Patterns of Wall Enhancement
• Mural enhancement is best assessed by comparing
(a) abnormal bowel with adjacent normal loops, or
(b) bowel loops that are at a similar distance from the center of the field of view to mitigate for field inhomogeneity, which may otherwise influence the apparent level of enhancement

Enhancement pattern
• Small bowel wall enhancement patterns have been divided into:
1. ‘‘target’’ appearance,
2. homogeneous mild
3. homogenous hyperenhancement
4. heterogeneous and
5. diminished.

1. Target/stratified/layered appearance with stratification of the layers of the small bowel wall (mural stratification) is generally found with benign conditions — for example, vasculitis, Crohn’s disease, venous thrombosis with associated bowel oedema or ischaemia and intramural haemorrhage.
Coronal VIBE image shows stratified contrast enhancement, with avid enhancement of the mucosa (arrowheads) relative to the submucosaand muscular layers (arrows), findings that help confirm active Crohn disease.

Different types of mural stratification
Soft tissue density mural thickening of the terminal ileum representing inflammatory infiltrate in a 34-year-old male with newly diagnosed active Crohn’s disease.
Fluid density mural thickening of the distal ileum representing submucosal oedema in a 62-year-old female with recurrent Crohn’s disease.
Fat density muralthickening of the terminal ileum in a 62-year-old female, representing chronic active inflammation

2. If wall enhancement is homogeneous and mild (i.e. similar to muscle), chronic inflammatory conditions should be considered, particularly those producing fibrosiswithin the small bowel wall (for example Crohn’s disease, ischaemia and radiation)
Coronal contrast-enhanced T1-weighted fatsuppressedimage of a patient with no history of surgery, but with similar symptoms, show thickening and stenosis of the terminal ileum with homogeneous contrast enhancement (arrows), compatible with chronic stenosis.

3. Homogeneous hyperenhancementrepresents transmuralinflammation is commonly seen with active Crohn’s disease, and is frequently associated with increased density in the surrounding mesenteric fat.
• Indeed, it has been roposed by Bodily et al that a cut off of 109HU can be used with reasonable accuracy
Gadolinium-enhanced image shows diffuse hyperenhancement relative to normal adjacent bowel (arrowheads), a finding that further confirms active disease.

4. Heterogeneous enhancement is seen in small bowel neoplasms, including gastrointestinal stromal tumours, adenocarcinomas, metastases and peritoneal deposits.
5. Decreased enhancement is typical of bowel ischaemia, and usually precedes the development of intramural gas and subsequent perforation.

• In addition, the absolute level of bowel wall enhancement has been suggested as a marker for disease activity.
• The peak signal intensity of mucosal enhancement has been shown to have good correlation with the Crohn disease activity index.

Active Crohn disease. Dynamic axial contrast-enhanced three-dimensional gradient-echo MR images (left to right, top to bottom) show progressive rapid bowel wall enhancement within the first 70 seconds after injection of contrast material.

Length of small bowel involvement
• For the purpose of differential diagnosis, the length of small bowel involvement can be divided into three:– focal (5 cm)
• neoplasms, endometriosis, small bowel diverticulitis, foreign body perforations, small bowel ulcers (secondary to non-steroidal anti-inflammatory drugs) and occasionally granulomatous processes like tuberculosis and Crohn’s disease
– segmental (6–40 cm)• intramural haemorrhage, Crohn’s disease, lymphoma, infectious enteritis and
ischaemia, particularly due to superior mesenteric artery (SMA) embolus or superior mesenteric vein (SMV) thrombosis.
• In a patient with previous malignancy and segmental involvement, previous radiotherapy should be considered
– diffuse (40 cm)• hypoalbuminaemia, low-flow intestinal ischaemia, vasculitis, graft vs host
disease and infectious enteritis

Mural thickening and symmetry

Location of pathology within the small bowel wall
• The mucosa is seen to be predominantly affected in inflammatory conditions like Crohn’s disease, tuberculosis and neoplasms such as adenocarcinoma.
• The predominant abnormality is seen in the submucosa in conditions like intramural haemorrhage, vasculitis, ischaemia, hypoalbuminaemia and angio-oedema.
• The serosa is predominantly involved in metastases, endometriosis, carcinoid and other inflammatory conditions in the peritoneum.

Pseudosacculation-Pseudodiverticulum Formation
• Pseudosacculations are a consequence of relative sparing of the antimesenteric border within an affected bowel segment.
• Fibrosis and shortening of the diseased mesenteric wall lead to apparent dilatation of the opposing normal bowel wall.
• Because all three bowel wall layers form the sacculation (in contrast to colonic diverticular disease), such a finding may also be referred to as a pseudodiverticulum .
• Abnormal bowel segments frequently demonstrate other features of chronic Crohn disease, such as fibrofattyinfiltration of the wall, wall thickening, and fat wrapping.

Multiple pseudodiverticula in a 33-year-old woman. US demonstrated thickened right iliac fossa bowel loops. (a) Coronal HASTE image shows pseudosacculation produced by asymmetric thickening of the terminal ilealmesenteric border. (b) Coronal fat-saturated HASTE image shows intermediate-signal-intensity mesenteric edema (arrows) tracking from the bowel segment shown in a, a finding that is appreciated only with fat saturation. (c) Gadolinium-enhanced image shows diffuse hyperenhancement relative to normal adjacent bowel (arrowheads), a finding that further confirms active disease.

Characterisation of small bowel pathology
• Interpretation of small bowel abnormalities can be divided into:
– Luminal (Wall, Fold and Mucosal) changes
– Extra Enteric changes
– Colonic abnormalities

Extra-enteric Assessment
• One of the major advantages of CT and other cross- sectional techniques is their ability to visualise the extraluminal soft tissues.
• It is therefore important to carefully evaluate the structures beyond the bowel wall.

Mesenteric Blood Vessels
• Patency or otherwise of mesenteric blood vessels should be assessed to exclude a vascular pathology such as arterial embolus or venous thrombosis.

Comb Sign
• corresponds to increased mesenteric vascularity. • identified as short low-signal-intensity parallel
lines on true FISP images, oriented perpendicular to the longitudinal axis of the affected bowel wall.
• On contrast material–enhanced VIBE images, the comb sign is seen as high-signal-intensity parallel lines due to contrast enhancement of the vasculature.
• The presence of the comb sign may suggest active disease.


Mesenteric Edema
• Mesenteric edema is present in some (but not all) patients with advanced active disease, and it tracks along the adjacent mesentery from an inflamed bowel loop.
• Seen particularly on fat-suppressed sequences.
• There is typically accompanying bowel wall edema and hyperenhancement, findings that are commensurate with active disease.
Coronal fat-saturated HASTE image shows intermediate-signal-intensity mesenteric edema (arrows), a finding that is appreciated only with fat saturation.

Fat Wrapping
• Increased mesenteric fat producing a mass effect and manifests as anatomic displacement of mesenteric vessels or surrounding abdominal viscera.
• Frequently asymmetric, preferentially involving the mesenteric border of the bowel, although there is often fibrofatty proliferation encircling involved bowel loops.
• Fat wrapping usually occurs in patients with long-standing, established transmural inflammation, and it is a very specific sign for Crohn disease (its presence may help in narrowing the differential diagnosis for small bowel disease).
Sequela of chronic Crohn’s related bowel inflammation. Twenty-seven year-old male with Crohn’s disease. Axial images demonstrate diffuse fat depositionin the wall of the rectosigmoid colon (A, B), as well as marked fibrofatty proliferation (“creeping fat”) (B) surrounding the rectum.

Lymph Nodes
• Better on T2-weighted FISP images.
• Small-volume lymph nodes can be seen adjacent to normal bowel segments and to those affected by active and inactive Crohn disease.
• However, hyperenhancement, enlargement, and edema of lymph nodes seen with fat-saturated VIBE & FISP sequences are highly suggestive of active Crohn disease in patients in whom this diagnosis has been established.

• FISP image shows a distended terminal ileum (arrow) but no focal thickening. Arrowheads indicate lymph nodes.
• HASTE image clearly delineates a thickened terminal ileum (arrow) but not lymph nodes. • VIBE image shows abnormal enhancement of the ileal wall (arrow) and lymph nodes
(arrowheads).

Mesenteric lymphadenopathy in a patient with Crohn disease. Coronal HASTE (a) andbalanced SSFP (b) MR images show mesenteric adenopathy (arrowheads), which is
much more conspicuous in b

• Nodes typically lie along the vascular supply of an affected disease segment (eg, ileocolicvessels in terminal ileal disease) but may be spatially remote from the segment.
• Enhancement, when present, is usually homogeneous.

• Nonenhancing nodes in the presence of adjacent bowel wall thickening and nodal edema may indicate an alternative diagnosis to Crohn disease.
• Necrotic caseatingnodes are present in tuberculosis and, more rarely, in histoplasmosis MR image shows central nonenhancement (arrows),
a finding that suggests necrosis (confirmed at CT), and a pattern of nodal change (arrowheads) that is atypical for Crohn disease. Results of laparoscopic lymph node biopsy confirmed histoplasmosis

Fistulas and Sinuses
• Up to 1/3 of Crohn’s patients develop a fistula within the first ten years after exhibiting symptoms of Crohn’s disease.
• While the perianal region is the most common site of fistula formation, fistulas can develop anywhere in the abdomen, including enteroenteric, coloenteric, colocolic, rectovaginal, enterocutaneous, and enterovesicular fistulas.
• Deep transmural ulcers may ultimately communicate with an adjacent epithelial surface and so become fistulas.

• In the most obvious cases, an enhancing tract can be traced, clearly identifying the presence of a fistula.
• Fistulas that are visible at MR enterography typically manifest as high-signal-intensity tracts on T2-weighted images and enhance avidly following gadolinium-based contrast material administration.

• Coronal HASTE image again shows the ileum (arrow) in proximity to the sigmoid colon (arrowhead).
• Coronal fat-saturated HASTE image shows a high-signal-intensity tract (straight arrow) connecting the ileum (curved arrow) and the colon (arrowhead).

• 32-year-old man in treatment for known Crohn disease.
• Coronal true fast imaging with steadystateprecession image obtained with fat saturation shows ileoilealfistula (arrow).
• Note that fistula does not contain any fluid or air within patent lumen but appears isointense.

• A sinus is defined as a blind-ending tract that arises from bowel but does not reach another epithelium-lined surface.
• Sinuses also manifest as high-signal-intensity tracts on T2-weighted images and appear similar to fistulas, sometimes in association with abscesses.

Enterocutaneous Fistulas
• Imaging with the patient supine is recommended to mitigate against the field inhomogenity if such fistulas are suspected clinically.
• Conventional techniques such as fistulographymay still have an important problem-solving role in difficult cases involving the abdominal wall.

37-year-old woman with known Crohn disease and previous ileorectal anastomosis.A, Axial true fast imaging with steady-state precession image shows large enterocutaneousfistula (arrow) containing high-signal enteral contrast material and surrounding inflammation.B, Intraoperative photograph shows fistula opening in bowel wall (arrow) and marked mural thickening (arrowhead)

• However, in many cases a discrete tract will not be identified, and the presence of a fistula must be surmised by secondary signs.
• In particular, the presence of ectopic gas in the midst of bowel loops, tethering and spiculation of adjacent bowel loops, and soft tissue stranding and density in the midst of tethered bowel loops can be seen in the presence “complex fistulizing” Crohn’s disease.

• However, in many cases a discrete tract will not be identified, and the presence of a fistula must be surmised by secondary signs.
• In particular, the presence of ectopic gas in the midst of bowel loops, tethering and spiculation of adjacent bowel loops, and soft tissue stranding and density in the midst of tethered bowel loops can be seen in the presence “complex fistulizing” Crohn’s disease.

• However, in many cases a discrete tract will not be identified, and the presence of a fistula must be surmised by secondary signs.
• In particular, the presence of ectopic gas in the midst of bowel loops, tethering and spiculation of adjacent bowel loops, and soft tissue stranding and density in the midst of tethered bowel loops can be seen in the presence “complex fistulizing” Crohn’s disease.

• Incipient or early fistulas manifest as linear areas of moderate signal intensity arising from the bowel wall.
• These fistulas may be difficult to visualize because of partial volume averaging and the lower spatial resolution of MRI.
• Multiplanar imaging of the bowel is useful for a complete assessment and avoidance of missed sinuses.
Coronal true FISP image obtained with fat saturation shows active inflammation in distal ileum. Small linear projections (arrows) are seen arising from bowel; these findings are indicative of incipient fistulas or sinuses.

• Ectopic gas in other locations, including the bladder and subcutaneous soft tissues, should also raise concern for a fistula, and should not automatically be assumed to be secondary to a foleycatheter or soft tissue injections.
Coronal CT enterograms reveal that the irregularly shaped fistula (arrowheads) coursesanterior to a bowel loop (arrows) and extends to the urinary bladder. Air is seen within the bladder, a finding that is consistent with fistula.

A 22-year-old female with Crohn’s disease and persistent pelvic pain. An abnormally thickened loop of distal ileum is present in the pelvis (a–d, chevron). Note the wide-mouthed fistulous connection (a–d, small arrows) with the left ovary (a–d, arrowheads), which has become enlarged with an intra-ovarian phlegmon (c, asterisk) as a sequela of long-standing Crohn’s disease. There is also tethering of this diseased bowel to adjacent small bowel loops in the pelvis (a–d, large arrows), but no severe, active inflammation is identified on fatsaturated T2W images (a–d).

Small Fistulas
Enterocolic fistula in a 36-year-old woman who presented with clinical relapse after undergoing right hemicolectomy for Crohn disease. (a) Coronal HASTE image shows a thickened ileum (arrowhead) a few centimeters from an
ileocolic anastomosis. Arrows indicate the path of the transverse colon. (b) Image from a subsequent small bowel follow-through study shows a fistula (arrow) from the
ileum to the transverse colon. In hindsight, the fistula was visible at MR enterography. Fistulization can be difficult to appreciate, and dynamic imaging with compression (eg, a small bowel follow-through study) has advantages in some doubtful cases.

Abscess
• An abscess is a well-defined, encapsulated collection of pus.
• Abscesses do not conform to normal peritoneal reflections (unlike free fluid) but do have the signal intensity characteristics of fluid (ie, high signal intensity on T2-weighted images, low signal intensity on T1-weighted images), and their rim often enhances strongly.
Abscess in a 29-year-old man with known Crohn disease who presented with clinical relapse. Coronal gadolinium-enhanced VIBE image shows a high-signal-intensity fluid collection 2 cm in diameter with intense wall enhancement (arrowheads), a finding that is consistent with an abscess. The abscess responded to intravenous antibiotic therapy.

• MR enterography is very sensitive for the detection of abscesses, but unlike CT, MR imaging may fail to help detect small volumes of gas within an abscess.
• The detection of any intraabdominal abscess is important because the use of anti–tumor necrosis factor agents such as infliximab is contraindicated in the presence of intra-abdominal abscess.

• Reactive loculated peritoneal fluid is occasionally seen in patients with severe nutritional failure, in patients with long-segment inflammation, or as a normal physiologic finding in young women with Crohn disease.
• It may mimic abscess, but it will not demonstrate an enhancing wall or adjacent peritoneal thickening, and it will have uniform high signal intensity.
Axial HASTE images show a small volume of free fluid between small bowel mesenteries (arrows), but no loculation, encapsulation, or mass effect as would be expected with an abscess.

Characterisation of small bowel pathology
• Interpretation of small bowel abnormalities can be divided into:
– Luminal (Wall, Fold and Mucosal) changes
– Extra Enteric changes
– Colonic abnormalities

Colonic Abnormalities
• This technique is specifically aimed at maximizing detection of small bowel disease and hence colonic distention may not be optimimal.
• Lack of prior laxative bowel preparation can sometimes interfere with the assessment of mucosal hyperenhancement, since colonic fecalresidue can be hyperintense with T1-weighted sequences, and underdistention or collapse may cause difficulty in accurately measuring wall thickness.

Crohn colitis. • Axial three-dimensional
gradient-echo MR image obtained with intravenous contrast material shows mucosal hyperenhancement and wall thickening in the colon (arrows), findings consistent with active inflammation.
• In this case, adequate colonic visualization was achieved because of antegrade filling.

Decision Making!!!
Choice of Small Bowel Imaging Technique: General Considerations

The Radiation Issue
• It is now clear that access to multidetector computed tomography (MDCT) has led to an increase in population radiation exposure.
• The benefits of MDCT are also well known.• However, patients with small bowel pathology, particularly those
with Crohn’s disease, frequently undergo multiple studies over the course of their disease, especially during acute episodes or when complications arise (Desmond et al. 2008). This can result in significant radiation accumulation;
• Nuclear medicine studies and barium examinations carry a lower but not insignificant radiation burden. Many individuals with small bowel disease are young, so where possible radiation-free imaging is preferable .
• For this reason, small bowel MRI and ultrasound examinations are advantageous, where clinically appropriate.

Invasive Investigations: BowelPreparation and Tubes
• Cathartic bowel preparation is unpopular with patients (Jensch et al. 2008), but may be an important aspect of barium examinations of the small bowel, WCE, and DBE.
• Purgation is not always necessary prior to CT, nuclear medicine, or MRI studies, depending on the indication and clinician preference, but the bowel distension agent may be a laxative, for example polyethylene glycol (PEG), or have a significant laxative side-effect (e.g., mannitol) (Lauenstein et al. 2003).

• Nasojejunal intubation without sedation for enteroclysis is tolerated but unpopular with both patients and most radiologists.
• Tube placement by less experienced operators or in more difficult cases may result in higher screening times, imparting a significant radiation dose and thereby increasing the radiation dose in a CTE procedure or negating the benefit of using MRI to avoid radiation.

• While sedoanesthesia makes the procedure more comfortable for patients, it requires additional monitoring and staff to prevent complications and has implications for the patient following the procedure.
• MR enteroclysis examinations also result in significantly more discomfort and abdominal pain following the procedure than enterography.

Acute vs. Elective Evaluation
• While similar out of hours access may be available for ultrasound and CT, the same is not always true for other modalities, particularly MRI.
• In acutely unwell patients, a MDCT scan is quicker and needs fewer breath-holds than MRI, improving patient compliance in what is often a difficult clinical situation.
• In severely ill patients, the length of examination and limited access for clinical assessment during the scan may render MRI completely inappropriate.
• Even in an elective outpatient setting, limited access of MRI may restrict its usage.

Capacity and Hardware
• Access to high-quality body surface coils and adequate field strength scanners (1.5 T or higher) are essential.
• Need for balancing ever increasing MRI service demands for other clinical indications.

Disease Stage
• Aphthous ulcers, the earliest manifestation of Crohn’s disease, are best demonstrated radiologically with traditional barium studies.
• Patients presenting with advanced stages need a cross-sectional imaging.

Extra Enteric Assessment
• A clear benefit of cross-sectional imaging over barium examinations and endoscopy

SMALL BOWEL ASSESSMENT: HEAD-TO-HEAD COMPARISON – GENERAL CONSIDERATIONS

Radiology or Endoscopy?
• An obvious advantage of endoscopic techniques is direct visualization of the enteric mucosa and the ability to detect subtle lesions beyond the resolution of radiological investigations, including telangectasias, mucosal hyperaemia (the earliest visible sign of Crohn’s disease), and aphthous ulcers.
• Other endoscopic possibilities include various interventions biopsy, polypectomy, ablation of vascular malformations, and tattooing to aid identification of pathology for laparoscopic resection.

• Disadvantages would include:– Often long– Sedation or anaesthesia– Significant learning curve– interventional tools is more limited– Expensive eqipments– Limited expertise– Risk of retension/obstruction (WCE)– Difficult anatomical location (WCE)– Proximal lesions may be missed due to rapid transit (WCE)– Limited battery life (WCE)– Information beyond the bowel - nil

• Overall, radiology and endoscopy are not mutually exclusive but frequently complimentary in such cases.

Enterography or Enteroclysis
• While enteroclysis is inherently invasive, usually unpopular with patients and incurs additional financial cost and radiation exposure, distension is undoubtedly superior, particularly in the jejunum.
• There is, therefore, a reasonable argument that the superior quality of enteroclysis justifies its invasiveness in the first diagnosis of polyposis syndromes and CD, with enterography more suited to follow-up of patients with established disease.

• Enterography is, however, highly advantageous in a paediatric population and in other patients where nasojejunal intubation is unsuitable or not tolerated.
• It is also less time-consuming

Advantages of MRI
• lack of ionizing radiation • high tissue contrast resolution. • ability to provide accurate anatomic detail; • depict extraintestinal abnormalities; and • facilitate distinction between phlegmon, abscesses,
and mesenteric lymphadenopathy.• MR fluoroscopy can also be performed to assess
stricture and obstruction.• perfusion MRI to assess for recurrent inflammation and
fibrosis• high-resolution MRI in the detection of early ulceration

Limitations of MRE
• still somewhat limited expertise and availability
• Longer time (30 min vs 30 sec)
• Sedation for very young children and for patients with claustrophobia
• Absolute contraindications to MRE (pacemaker, implants…..)

MRE v/s VCE
• Three studies concluded that both MRE and VCE identified diseased small bowel;
• However, VCE was better at identifying small aphthous lesions and often identified more lesions.
• MRE is insensitive to early mild disease restricted to the mucosa.

MRE vs SBFT/conventional enteroclysis
• full agreement in revealing, localizing, and estimating the length of bowel involved.
• MRE (with MR-enteroclysis) was poor at detecting superficial ulcers but performed well in identifying deep ulcers and stenosis.

MRE vs CTE
• No radiation risks• MRE more accurately describe the submucosal
pathology of transmural Crohn’s disease.• ability to differentiate inflammation from fibrosis
within the submucosa of the bowel wall and in the peri-enteric tissues.
• MRE can show extra-intestinal disease (including bowel obstruction, abscesses, webs, tethering, and fistulae) with less dependence on enteroclysis-level bowel distension as is necessary for optimal CT.

• Adv of CT:
– availability and a slight cost differential
• Although the overall cost-benefit balance is a key measure that remains incompletely evaluated.
– Acute situations – critically ill

MRE vs PET or PET/CT
• With regards to the use of PET or PET-CT in the evaluation of CD, the sensitivity in the detection of active inflammation ranges between 73% and 90% when compared with clinical, endoscopic or biological markers of disease activity.
• Using PET alone, there is poor disease localisation, and specificity can sometimes be low, as other pathological or physiological processes may lead to increased bowel fluorodeoxyglucose (FDG) uptake.
• The main disadvantage of PET-CT is the use of ionising radiation; this is clearly not ideal in young patients who may require repeated imaging.
• It is also more time consuming to perform than CT or MRI alone. • Hence for these reasons, PET-CT is not routinely used in the
assessment of patients with CD.


……..in summary
• Multimodality tailored assessment is the rule rather than the exception in small bowel imaging , particularly for difficult cases.

Clinical Role of Enterography

Charts illustrate the spectrum of indications of enterography

Crohn disease
• Crohn disease has a worldwide distribution but is more prevalent in Europe and North America .
• The peak incidence of Crohn disease is in adolescents and young adults between 15 and 25 years old; a second shallow peak is seen in the 50- to 80-year-old age group.
• Disease is distributed equally between the sexes, although isolated colonic disease is more common in women than men.
• Older patients tend to have localized enteritis, whereas jejunoileitis is more common in younger patients

• The current view is that the diagnosis of Crohn disease is established by a non strictly defined combination of clinical presentation; endoscopic appearance; radiology, histology, and surgical findings; and, more recently, serology results.
• The varied behaviour and clinical progression of Crohn disease have led to its subtyping by various investigators on the basis of inflammatory activity, clinical indexes, and histopathology results.

Diagnosis of Crohn Disease and Assessment of Inflammatory Activity
• Crohn’s disease can involve any portion of the gastrointestinal tract from the mouth to the anus, although the small bowel is the most commonly affected portion of the bowel, particularly the distal and terminal ileum.
Thirty-eight-year-old male with Crohn’s disease. Coronal volume rendered image demonstrates thickening and mucosal hyperemia of the terminal ileum, a classic appearance and location for acute Crohn’s related inflammation;

Classification of Crohn Disease
• Classification by clinical or laboratory data has not been entirely reproducible.
• Maglinte and colleagues proposed an imaging-basedclassification of Crohn disease, which they surmise could provide useful information when used in combination with clinical and laboratory data.
• They classify Crohn disease into four broad groups: – active inflammatory, – perforating and fistulating, – fibrostenotic, and – reparative and regenerative subtypes.
• The imaging findings in these subtypes are based on the detection of ulceration, fistulas, bowel edema, strictures, and extraintestinal abnormalities.

Active Inflammatory Disease
• This subtype of disease is characterized by:
– inflammation with superficial and deep ulcers,
– transmural inflammation with granuloma formation, and
– mural thickening.

• Several enterographic findings are associated with increased disease activity, including
(a) wall thickening greater than 4 mm,
(b) intramural and mesenteric edema,
(c) mucosal hyperemia,
(d) wall enhancement (and enhancement pattern),
(e) vascular engorgement, and
(f) inflammatory mesenteric lymph nodes (often with hyperenhancement)

(a) Active distal ileal Crohn’s disease in a 36-year-old male. Coronal CT enterography image showing mural thickening and mucosal hyperenhancement (long arrows). Compare the normalenhancement of the unaffected small bowel (short arrow). (b) Enlarged vasa recta involving the actively inflamed neoterminal ileum producing a comb sign (arrows). Note the presence of enlarged mesenteric lymph nodes.

Perforating And Fistulating Disease
• transmural ulceration and fistula formation,

Fibrostenotic Disease
• This subtype of disease is characterized by bowel obstruction.
• A fixed narrowing of the affected segment without any significant bowel wall thickening or inflammation is typically seen.
• MR fluoroscopy may also show fixity of the affected segment with proximal dilatation of the bowel.

33-year-old woman with known Crohndisease and previous ileocolic resection.A, Coronal true fast imaging with steady-stateprecession image obtained with fat saturation shows thickened neoterminal ileum (arrow). Note dark submucosal band and relative lack of inflammation.This band was proven to be fibrotic stricturesecondary to chronic Crohn disease.B, Photograph of resected specimen shows fibrotic stricture (arrow).

• Chronic fibrotic strictures are typically hypointense on both T1- and T2- weighted sequences, whereas acute inflammatory strictures due to acute inflammatory edema show the target sign.
• Fibrotic strictures may show minor, inhomogeneous enhancement without any evidence of edema or surrounding mesenteric inflammation or hyperemia.
• Asymmetric bowel fibrosis and shortening secondary to ulceration of the mesenteric side of the bowel lead to the formation of pseudosacculations on the other side.
• The ability of tissue contrast differentiation on MRI is particularly suited to distinguish between a fibrotic stricture that may require surgical intervention and an acute inflammatory stricture that may benefit from medical treatment.

Fibrostenotic Crohn disease. Axial balanced SSFP MR images without (a) and with (b) fat suppression show low-signal-intensity duodenal wall thickening (arrows) and proximal obstruction.

Reparative or Regenerative Disease
• This subtype is characterized by mucosal atrophy and the presence of regenerative polyps.
• Luminal narrowing may be seen, but usually there are no signs of inflammation or obstruction.
• Mucosal denudation with focal areas of sparing is seen on imaging.
• Typically, reparative polyps do not show significant hyperemia or mural edema.
• Extensive filiform polyposis may be seen in chronic Crohn disease as multiple filling defects extending into the lumen without an obstructive element or significant enhancement.
Wall thickening mainly at the expense of the submucosa (white curved arrow), which appears hypointense on the axial T2 fat-suppressed image, reflecting fat hypertrophy and fibrosis in the setting of the regenerative---reparative subtype.The serosa (blue arrow) and mucosa appear hyperintense producing the halo sign.

Complications
• Segments affected by Crohn disease are at increased risk of developing adenocarcinoma, and the risk of colorectal cancer in patients with Crohn colitis is 4–20 times higher than that of the healthy population.
• Furthermore, segments of bowel that are not functioning have a higher risk for developing cancer.
71-year-old woman with known Crohndisease. Coronal true fast imaging with steady-state precession image obtained with fat saturation shows large mass arising from jejunum (arrow) with adjacent lymphadenopathy. Pathology results showed that mass was adenocarcinoma arising from segment affected by Crohn disease.

• Carcinomas usually present as stricture lesions that may be difficult to differentiate from benign fibrotic strictures.
• Neoplastic lesions tend to have longer strictures and may occur in noninflamed segments of bowel.
• Although reactive nodes are commonly noted in patients with active Crohn’s disease, large nodes (> 2 cm) should raise the possibility of an underlying malignancy.
• Any fixed site of narrowing (whether inflammatory or fibrotic) should be treated as a site of suspicion until proven otherwise, even if a discrete soft tissue mass is not identified.
• Moreover, asymmetric wall thickening and irregularity should not automatically be assumed to simply represent a site of active inflammation, particular if mural stratification of the wall is not seen.
• Bowel cancer must be suspected when bowel obstruction in Crohn disease does not respond to conventional treatment.

• In a series by Soyer et al, four different patternswere seen with Crohn’s related small bowel adenocarcinomas:
1. focal soft tissue mass;
2. short severe stenosis;
3. long stenosis with wall irregularity; and
4. irregular circumferential wall thickening of a bowel loop.

Lymphoma has been reported to present as multifocal areas of increased nodularity and strictures on barium examinations.
• Fifty-one-year-old female with a history of Crohn’s disease.
• Axial image demonstrates nodular soft tissue thickening (arrows) surrounding an aneurysmally dilated loop of bowel in the right abdomen.
• This was found to represent B-cell lymphoma following surgical resection.

Clinical applications of MRE in Crohn’s disease
• Evaluation of the extent of small bowel disease at diagnosis
• Evaluation of disease burden in symptomatic patients to direct therapeutic management
• Evaluation of fibro-stenotic disease, which may respond better to surgery than to escalation of medical therapy
• Confirmation of clinical remission and consideration for escalation of medical therapy if there is persistent submucosal disease despite clinical remission
• Evaluation of intra-abdominal complications, including fistulae, tethering, stenosis, and abscesses
• Evaluation of perianal disease

Enterography Beyond Crohn’s

Enterography Beyond Crohn’s
• Small Bowel Obstruction• Occult GI bleed• Ulcerative colitis• Small bowel Neoplasms
– Primary (benign, malignant) & Secondary
• Inflammatory conditions• Infectious conditions• Diverticular disease• Systemic sclerosis• Bowel duplication• Familial Mediterranean disease• Incidental findings

Small-Bowel Obstruction
• The diagnosis of small-bowel obstruction at enterography is based on:
– the identification of dilated loops of bowel proximal to the level of obstruction,
– a distinct transition point, and
– a normal-caliber or collapsed distal bowel segment.

• Abdominal CT has been shown to have high sensitivity for detection of acute high-grade small bowel obstructions, and because of its widespread availability, it is routinely used in clinical practice. MR imaging also has been shown to be useful for detecting bowel obstructions in acute settings and differentiating malignant from benign causes.
• However, conventional cross-sectional imaging methods (CT, MR imaging) may fail to depict a cause in a substantial number of patients with symptoms of intermittent low-grade small-bowel obstruction.

• Studies have shown that CT/MR enteroclysis is superior to abdominal CT/MR for detection of transition points because of its improved distention.
• MR enteroclysis provides improved distentionof the small bowel and may demonstrate subtle transition points or an obstruction that may not be visible at imaging with more routine methods, including enterography.

Low-grade obstruction caused by adhesions. (a) Axial MR enterographic image shows a distorted small-bowel loop (arrow) in the right lower quadrant, without obstruction. (b) Axial image from follow-up MR enteroclysis with improved bowel distention (arrowhead) shows a persistent focal transition point (arrow) indicative of a proximal obstruction. These findings are suggestive of an adhesion, the presence of which was confirmed at laparoscopy.

• However, functional cine MR as part of an MR enterography examination depicts physiological peristalsis and normal bowel motion within the abdomen, including “visceral slide,” which is the normal movement of bowel loops relative to each other (Lienemann et al. 2000).

Postoperative Adhesions
• The most common cause of small-bowel obstructions.
• Adhesive ileal obstruction in a 30-year-old woman with a history of appendectomy and recurrent low-grade bowel obstruction.
• MR enterography was performed after the administration of 1 L of an oral contrast agent.
• Coronal FISP image from MR enterography demonstrates ileal loop dilatation (curved arrow), a transition point (straight arrow), and normal distal caliber (arrowhead).
• No mass, bowel wall thickening, stricture, or other specific cause of obstruction was identified.
• These findings were suggestive of an obstruction due to bowel adhesion, which was later confirmed at laparotomy.

• Other possible causes of small-bowel obstruction include:
– inflammatory diseases,
– benign and malignant tumors,
– intussusception,
– strangulated hernia,
– volvulus, and
– radiation-induced enteritis.

Brunner gland hamartoma in a 58-year-old woman with GI tract bleeding and recurrent low-grade bowel obstruction. Initial MR enterographic sequences were applied after administration of 500 mL of an oral contrast agent.
(a) Axial FISP image from MR enterography shows jejunalintussusception (arrowheads) and narrowing with resultant obstruction (arrow). (b) Coronal FISP image from MR enterography shows the lead point for intussusception: a multicystic lesion (arrowheads). (c) Photograph shows the resected jejunal lesion. The diagnosis at histopathologic analysis was Brunner gland hamartoma. (Scale is in millimeters.)

Occult Gastrointestinal Bleeding
• Bleeding from the upper GI tract/colon, if it is reachable by endoscope, is well evaluated.
• Gastrointestinal bleeding from the small intestine is less common but is difficult to diagnose by endoscopy or conventional imaging.

Multi-phase CTE
• Scanning is performed from the diaphragm to the symphysis pubis during each of 3 phases, with scanning initiated when a region-of interest attenuation threshold in the aorta is reached.
• During the arterial phase (bolus-triggered) , vascular ectasias such as AVMs and their early draining veins are seen.
• The enteric phase (20 seconds after trigger), often highlights enhancing tumors, with
• The delayed images (70 seconds after trigger) showing that iodinated contrast is accumulating in the small-bowel lumen, indicating active bleeding.

Active bleeding at multiphase CT enterography. (A) Arterial, (B) enteric, and (C) delayed phase images show progressive focal contrast accumulation (arrows in A, B, and C) in an ileal angiodysplasia confirmed at intraoperative endoscopy. (C) Additional focus (arrows) of contrast on delayed image is also presumed to be active bleeding.

• CT enterography misses some lesions, such as flat arteriovenous malformations that may be seen on capsule endoscopy.
• On the other hand, CT can show active extravasation of contrast into the bowel lumen.
• CT enterography shows promise as a complementary study to capsule endoscopy in this setting.

A heart transplant recipient who presented with abdominal pain and gastrointestinal bleeding. (A and B) CT shows (A) an intramural small bowel hematoma and (B) a partial small bowel obstruction. (B) In the more caudal section, note the high-attenuation mural hematoma and the narrowed lumen, which caused the bowel obstruction.

Ulcerative Colitis
• Because enterography is less sensitive than endoscopy and principally allows evaluation of the small bowel, it is not used for the diagnosis or staging of ulcerative colitis

Active ulcerative colitis with “backwash” ileitis in a 28-year-old woman who presented with intermittent nausea, vomiting, fever, and chills. (a) CT enterogram shows a patulous ileocecal valve (arrows), as well as mural hyperenhancement in the cecal wall (arrowhead).(b) Transverse CT enterographic images demonstrate pseudopolyps as enhancing tags arising from the luminal mural surface.

Mural stratification, dilatation of the vasa recta, colonic wall thickening, and inflammatory pseudopolyps are seen in both
ulcerative colitis and Crohn colitis
Ulcerative Colitis Crohn’s Colitis
Crohn colitis in a 43-yearold woman. CT enterogramdemonstrates Crohn colitis as mural stratification with intramural edema, bowel wall thickening (arrows),and dilatation of the vasa recta (arrowheads).
Coronal reformatted CT enterographic images demonstrate mural hyperenhancement in the colonic wall and pseudopolyps as enhancingtags arising from the luminal mural surface.

• When these findings occur in the right colon and terminal ileum, Crohn disease is more likely.
• In addition, extraenteric complications such as fistulas, abscesses, or discontinuous colonic or small bowel inflammation support the diagnosis of Crohn disease.
• Because of the sensitivity of enterography for Crohn disease, the principal role of this modality in patients with suspected ulcerative colitis is to help exclude findings of Crohn disease such as small bowel inflammation.

Small-Bowel Neoplasms
• As at CT, differentiation between benign and malignant small-bowel lesions at MR imaging may prove difficult, particularly when lesions are small.
• Factors they found to be associated with malignancy were:– the presence of a long, solitary, non-pedunculated
lesion;
– mesenteric fat infiltration; and
– mesenteric lymph node enlargement.

• An advantage of MR imaging over CT for the detection of small-bowel masses is the ability of MR imaging to generate images with different gradations of luminal contrast agents.
• The use of biphasic enteric contrast agents at MR imaging further helps in the detection of subtle masses.

Benign Tumors
• Adenomas – most common asymptomatic benign tumors of the small
bowel
– most often seen in the duodenum.
– may have malignant potential.
– The tumors appear as well-defined sessile or pedunculatedsoft-tissue masses that are surrounded by clear fat planes.
– They show homogeneous moderate enhancement after the administration of an intravenous contrast medium.
– Adenomas may protrude into the small-bowel lumen without obstructing it

Lipomas
• Most are seen in the distal small bowel.
• They commonly arise in the submucosa and manifest with intussusception or bleeding.
• They display high signal intensity on T1- and T2-weighted MR images, with loss of signal intensity when fat suppression is used.
Jejunal intussusception due to a lipoma in a 63-year-old woman. Axial gadolinium-enhanced T1-weighted fat-suppressed 3D VIBE image from MR enterography shows intussusception of a proximal small-bowel segment. The lead point (arrow) is an ovoid lesion with low internal signal intensity, a finding suggestive of a lipoma. The diagnosis was confirmed at pathologic analysis.

Small-bowel hemangiomas
• consist of either capillaries or cavernous vessels, most commonly manifest with acute or chronic GI tract bleeding.
• At MR imaging, small-bowel hemangiomasappear as submucosal polypoid tumors.
• It may be difficult to differentiate them from other vascular tumors or malformations on the basis of imaging criteria alone.
• Angiodysplasia usually appears as an avidly enhancing plaque or nodule with fading during the delayed phase

Peutz-Jeghers syndrome
• A genetic disorder with an autosomal dominant pattern of inheritance, is distinguished by multiple hamartomatous polyps throughout the GI tract, mostly in the small bowel, along with pigmented mucocutaneous lesions.
• The two main problems in the management of the GI tract lesions in patients with Peutz-Jegherssyndrome are the longterm cancer risk and polyp-related complications.

• It is now widely accepted that patients with the syndrome have increased risks for many cancers, including small-bowel cancers, with a lifetime incidence of malignancyapproaching 60%.
• Large Peutz-Jeghers polyps (>15 mm) in the small bowel commonly manifest at an early age with complications such as GI tract bleeding, anemia, and intussusception or obstruction.
• Hence the need for surveillance.
On a CT enterogram obtained in a 17-year-old boy who presented with signs of intestinal obstruction secondary to intussusception, multiple juvenile hamartomatous polyps(arrows) are visible within the ileum.

• Benign hamartomatous polyps are found throughout the small intestine, especially the jejunum, in patients with Peutz-Jeghers syndrome.
• FISP and gadolinium-enhanced fat-suppressed VIBE are the most useful MR imaging sequences for detecting small-bowel polyps.
• Polyps appear as hypointense filling defects on FISP images and typically show marked enhancement similar to that of the bowel wall mucosa after the intravenous administration of a gadolinium chelate.

Surveillance of polyps in a 27-year-old man with Peutz-Jeghers syndrome. (a) Coronal FISP image from MR enterography shows at least three low-signal-intensity polyps (arrows) in the small bowel. (b) Coronal gadolinium-enhanced T1-weighted fat-suppressed 3D VIBE image from MR enterography shows moderate to marked enhancement of the polyps (arrows).

Gastrointestinal Stromal Tumors
• The most commonly occurring mesenchymal neoplasm of the GI tract.
• The most frequent sites of GISTs are the stomach (60%) and the small bowel (30%).
• The tumors are usually solitary but have been reported to occur in multiples, particularly in the setting of type 1 neurofibromatosis
• GISTs in the small bowel most often originate from the muscularis propria and frequently involve the outer muscular layer of the bowel wall, exhibiting an exophyticgrowth pattern; less frequently, they arise intraluminally.
• Most (70%–80%) of the tumors are benign, but 20%–30% are malignant

• A GIST often manifests as an exoenteric, rounded mass that expands the small-bowel wall with a smooth, broadly pushing border; however, endoluminaldevelopment of the tumor is also possible.
• The tumor may show evidence of internal hemorrhage or necrosis, but satellite adenopathy is lacking.
• Small tumors usually enhance markedly.
• In lesions with extensive regions of hemorrhage or necrosis, cavities may form that communicate with the digestive lumen and contain air.
Gastrointestinal stromal tumor. CT enterogramshows an exoenteric gastrointestinal stromal tumor (arrows) of the duodenum.

Duodenal GIST in a 21-year-old man with type 1 neurofibromatosis. MR enterography was performed for small-bowel assessment after a small GIST was seen at gastroduodenal endoscopy. (a) Axial gadolinium-enhanced T1-weighted fat-suppressed 3D VIBE image from MR enterography shows a large (2-cm), well-delimited exophytic duodenal lesion (arrow). (b) Diffusion-weighted MR image obtained with b of 800 sec/mm2 optimally displays the high-signal-intensity lesion against a suppressed background.

• Leiomyomas are mesenchymal tumors that also may manifest with bleeding in the small bowel but, unlike GISTs, do not express the c-Kit protein.
• They are sharply defined spheroid or ovoid masses with a maximal diameter of 1–10 cm that usually enhance after the administration of an intravenous contrast medium
Leiomyoma in a 60-year-old woman referred for evaluation of unexplained GI tract bleeding and anemia. (a) Axial T2-weighted half-Fourier RARE image from MR enterography shows a round, homogeneous, exophytic ilealmass (arrow). (b) Photograph of the resected bowel segment shows a well-delimited extraluminal mass arising from the bowel wall. (Scale is in centimeters.)

Malignant Tumors
• Malignant tumors of the small bowel account for 1%–2% of all GI tract neoplasms and are usually misdiagnosed at initial presentation or diagnosed late in the disease process.
• An estimated 60%–70% of symptomatic small-bowel tumors prove to be malignant

Adenocarcinomas
• most common primary malignancies of the small bowel, accounting for 40% of malignancies in this part of the GI tract.
• They most often arise in the duodenum (50%), followed by the jejunum (30%) and ileum (20%).
• Adenocarcinomas typically involve a short segment of bowel, and they may lead to partial or complete bowel obstruction. Adenocarcinoma of the jejunum in a 33-year-
old man. CT enterogram demonstrates a bulky, heterogeneously enhancing mass (arrow) arising from the proximal jejunum (arrowhead).

• MR enterographic features of adenocarcinomas include:– annular and constricting lesions; – eccentric or circumferential wall thickening with irregular
borders; and – moderate, sometimes late enhancement after the
administration of intravenous contrast material.
• Lymph node enlargement is not as marked in the presence of adenocarcinomas as it is in the setting of lymphomas.
• Metastases from bowel adenocarcinomas to local lymph nodes, liver, peritoneal surfaces, and ovaries may be depicted at MR enterography

Pathologically proved jejunal adenocarcinoma in a 57-year-old man with abdominal pain andvomiting for 15 days. (a) Coronal T2-weighted half-Fourier RARE image from MR enterography shows alow-signal-intensity jejunal loop with irregular short-segment circumferential thickening and stenosis(arrow) and a dilated jejunal loop with some degree of ischemia proximal to the stenosed segment (arrowheads).(b) Coronal gadolinium-enhanced T1-weighted fat-suppressed 3D VIBE image from MR enterographyshows moderate enhancement of the lesion (arrow).

Carcinoid tumors
• second most common primary malignancies of the small bowel (33% of malignancies), after adenocarcinomas.
• They most often arise in the appendix (50%) and the distal ileum.
• Symptoms are often vague because carcinoid tumors are characteristically slow growing and may go unrecognized for many years. Only 10% of patients develop carcinoid syndrome.
• Carcinoid tumors of the small bowel may occur in multiples.

• Those occurring in the distal small bowel often involve the adjacent mesentery, stimulating considerable desmoplasia and fibrosis; the resultant angulation and kinking of the bowel often lead to obstruction and ischemia.
• Mesenteric carcinoid tumors have a maximal diameter of 2–4 cm, typically show signal isointense to that in muscle on T1- and T2-weighted images, and sometimes exhibit radiating spicule-like strands of tissue.
• Small-bowel carcinoid carcinoid tumors are likely to be small and difficult to detect.

• CT/MR enterographic appearances of carcinoid tumors of the small bowel vary and may include:
– an avidly enhancing, well-delimited submucosalmass, often in the distal ileum;
– multifocal enhancing polypoid lesions in a segmental distribution; and
– numerous tiny enhancing lesions in a carpetlikeconfiguration.

(a) submucosal carcinoid tumor (arrows) within a Meckel diverticulum. (b)carcinoid tumor (arrow) within the wall of the ileum. (c) mesenteric metastases from an ileal carcinoid tumor. Note the enhancing, star-shaped mesenteric nodule (arrowhead), with stranding of the mesentery and thickening of the adjacent small bowel wall (arrows). The segmental wall thickening may indicate either a carcinoid carpet lesion or segmental edema. (d) mesenteric carcinoid tumor (arrows) with hypervascular liver metastases (arrowheads).
Varied appearances of small bowelcarcinoid tumors

Histologically proved isolated ileal carcinoid tumor in a 71-year-old man with a history of synchronous renal and rectal cancers. (a) Axial gadolinium-enhanced T1-weighted fat-suppressed 3D VIBE image from MR enterography shows a single 1.5-cm markedly enhancing submucosal ileal nodule (arrow). (b, c) Coronal gadolinium-enhanced T1- weighted fat-suppressed 3D VIBE images from MR enterography show the submucosal ileal nodule (arrow in b) and a distant, spiculated, irregular mesenteric mass (arrowheads).

Lymphomas
• may arise as primary tumors of the small bowel or may represent secondary intestinal involvement in the setting of diffuse lymphomatous disease.
• Non-Hodgkin B-cell lymphoma, the most common histologic subtype found in the small bowel, is believed to arise from mucosa-associated lymphoid tissue.
• T-cell lymphomas of the small bowel are considerably less common and are associated with concomitant celiac disease.

• Small-bowel lymphomas have varied appearances at imaging, depending on their gross morphologic features; they may differ considerably in regard to their location, their size, the extent of their involvement of bowel, and their effect on luminal integrity. – an exoenteric mass or
– long segment of circumferential bowel wall thickening with adjacent lymphadenopathy or
– aneurysmal ulceration
• but without obstruction is suggestive of lymphoma as the primary diagnostic consideration.

Lymphoma in a 50-year-old man with abdominal pain. Coronal FISP (a) and gadolinium-enhanced T1-weighted fat-suppressed 3D VIBE (b) images from MR enterography demonstrate segmental homogeneous and circumferential bowel wall thickening with a pseudoaneurysmal pattern (arrow).

Burkitt-type lymphoma in a 19- year-old man with abdominal pain. (a) Coronal FISP image from MR enterography demonstrates segmental bowel wall thickening (arrows) with mesenteric adenopathy (arrowhead).(b) Axial diffusion-weighted image obtained with b of 800 sec/mm2 optimally depicts high signal- intensity abnormalities in the small-bowel wall (arrows) against a suppressed background.

Secondary neoplasms
• Secondary neoplasms that arise by means of intraperitoneal seeding may appear as small or large enhancing nodules along the serosal surface of the small bowel, mesentery, or omentum.
• Bowel metastases also may occur by direct extension from adjacent structures or by lymphatic spread.
• Hematogenous metastases to the intestine from extraenteric primary tumors are unusual, but melanoma, breast cancer, and lung cancer are the most common primary sources of such metastases.
• Metastases characteristically appear as mural nodules and may cause transient intussusception.

Metastases from stage IV melanoma in a 57-year-old man with abdominal pain.
Coronal gadolinium-enhanced T1- weighted fat-suppressed 3D VIBE image from MR enterography demonstrates numerous rounded subserosalintestinal lesions (arrows) that represent metastases.

INFLAMMATORY CONDITIONS

Bowel Ischemia and Vasculitis
• Bowel ischemia is a common but complex disorder with various primary causes and diverse clinical and imaging manifestations.
• Primary causes of insufficient blood flow to the intestine are numerous and include:– thromboembolism, – nonocclusive conditions (hypovolemia; hypotension; low cardiac
output status; and therapy with digoxin, a-adrenergic agonists, or b-receptor–blocking agents),
– bowel obstructions, – neoplasms, – abdominal inflammatory conditions, – chemotherapy- and radiation-induced enteropathies, and – vasculitides.

• Enterographic features of ischemia include:
– thickening of the bowel wall with or without the target sign,
– poor contrast enhancement of the bowel wall, and
– low-grade obstruction.

• Absence of enhancement or poor enhancement of the bowel wall appears to be the most specific finding.
• However, in some cases the ischemic segment shows prolonged enhancement due to abnormal perfusion (eg, delayed return of venous blood with resultant slowing of the arterial supply or arteriospasm).
• An additional sign of ischemia is the presence of ascites.
Intravenous contrast enables visualization of both viable segments, which are identified by brisk enhancement of the mucosa (left arrow) and ischemic segments, identified by the absence of enhancement of the bowel wall (right arrow).

Small-bowel ischemia in a 67-year-old woman with hypovolemic shock. Coronal FISP (a) and gadolinium-enhanced T1-weighted fat-suppressed 3D VIBE (b) images from MR enterography show a long segment of the proximal small bowel with a mildly thickened wall (arrows) that enhances in b. These findings are indicative of ischemia.

• Differentiation of bowel ischemia from infiltrative or neoplastic disease may be difficult on the basis of imaging appearances alone.
• In such cases, the clinical manifestations and clinical history (eg, a history of radiation therapy or other intervention) often enable an accurate diagnosis of ischemia.
• Bowel ischemia also may arise in the presence of a malignancy, particularly colonic carcinoma.

• Systemic vasculitides, such as systemic lupus erythematosus, polyarteritis nodosa, and Henoch-Schönlein purpura, rarely cause bowel ischemia.
• Mesenteric vasculitis usually involves a relatively long length of bowel and is nonsegmental in distribution.
• The finding of ischemic changes involving the duodenum is relatively specific for the presence of vasculitis; other causes of small-bowel ischemia typically involve the jejunum and ileum as well as the colon.

Treatment-induced Inflammation
• The frequency and severity of radiation therapy–induced enteritis depend on:– the radiation dose, – treatment volume, and – fractionation scale.
• Risk factors that predispose patients to chronic radiation therapy–related enteritis include:– hypertension, – atherosclerosis, – diabetes, – adhesions due to previous abdominal surgery, and – history of peritonitis.
• Radiation-induced enteropathy occurs in patients who receive a dose of more than 45 Gy to the pelvis.

• During the subacute phase (5–12 months after the completion of radiation therapy), severe endarteritis obliterans may develop, with resultant inflammatory thickening of loops of ileum within the pelvic radiation port.
• During the chronic phase (1–2 years after the completion of radiation therapy), these bowel loops may become fixed and angulated, with resultant stricture and obstruction.
• MR enterography may show narrowing of the bowel lumen secondary to mural thickening and bowel angulation due to adhesions and retraction of the mesentery; fistulas may also be observed.

Radiation therapy–induced enteropathy in a 42-year-old woman with low-grade bowel obstruction and weight loss 4 years after undergoing surgery and external-beam radiation therapy for uterine cervical cancer. (a) Axial T2-weighted half-Fourier RARE image from MR enterography depicts thickened pelvic small-bowel loops (arrows) and a recurrent nodule (arrowheads) in the bowel wall. (b) Axial gadolinium-enhanced T1-weighted fat-suppressed 3D VIBE image from MR enterography demonstrates thick-walled pelvic small-bowel loops with a stratified enhancement pattern (arrows) produced by the low-signal-intensity edematous submucosa between the enhancing mucosa and serosa.

• Chemotherapeutic agents also can induce enteropathy.
• Chemotherapy-induced enteritis appears as nonspecific focal or diffuse bowel wall thickening with or without the target sign.
• Regional mesenteric vessel engorgement and haziness also may be seen
Enteropathy in a 50-year-old man with diarrhea and abdominal pain while undergoing chemotherapy for esophageal adenocarcinoma.
Coronal gadolinium-enhanced T1- weighted fat-suppressed 3D VIBE image from MR enterography demonstrates wall
thickening and stratified enhancement of a distal ileal loop (arrow), findings suggestive of inflammatory active ileitis. Symptoms resolved after a change in the chemotherapeutic agent.

Celiac Disease
• Celiac disease is a gluten-sensitive enteropathy that affects the small intestine in genetically susceptible individuals.
• The symptoms of celiac disease are frequently nonspecific, and the differential diagnosis, which is based on clinical and radiologic manifestations, includes viral enteritis, giardiasis, Crohn disease, AIDS, and Whipple disease.
• Although a diagnosis of celiac disease is verified with biopsy of the small intestine, imaging findings are often suggestive of the diagnosis in adult patients with nonspecific intestinal disorders and a presumably low risk for celiac disease

• Celiac disease predominantly involves the duodenum and proximal jejunum, with the extent of involvement ranging from one or two segments to the entire small bowel.
• The radiologist should examine the folds attentively for signs of villous atrophy in the jejunum (seen as reversal of the normal jejunoileal fold pattern, with an increased number of ileal folds and a decreased number of jejunal folds) or dilatation of jejunalloops with absence of the valvulaeconniventes.
• Findings such as:– inflammatory thickening of the bowel
wall, – lymphadenopathy, and – mesenteric vascular engorgement
also may be seen in patients with celiac disease.
Celiac disease in a 23-year-old woman. Coronal FISP image from MR enterography shows an
increased number of folds in ileal loops (arrow).

• Complications of the disease may include:– nonobstructive intussusception
and – ulcerative jejunoileitis with
circumferential thickening of the bowel wall seen at enterography.
– Cavitary mesenteric lymph node syndrome, • which is characterized by fat-fluid
levels, and the development of lymphoma or carcinoma, are rare associated conditions.
• The latter should be suspected when previously asymptomatic patients with celiac disease develop recurrent diarrhea, abdominal pain, or both after initiating a gluten-free dietary regimen.
– increased risk for lymphoma and carcinoma of the bowel
A patient with sprue and an intussusception (arrow).

• Complications of the disease may include:– nonobstructive intussusception
and – ulcerative jejunoileitis with
circumferential thickening of the bowel wall seen at enterography.
– Cavitary mesenteric lymph node syndrome, • which is characterized by fat-fluid
levels, and the development of lymphoma or carcinoma, are rare associated conditions.
• The latter should be suspected when previously asymptomatic patients with celiac disease develop recurrent diarrhea, abdominal pain, or both after initiating a gluten-free dietary regimen.
– increased risk for lymphoma and carcinoma of the bowel
Coronal reformatted CT enterographicimage obtained in a patient with celiac disease and ulcerative jejunitis shows thickened bowel wall with mucosal hyperenhancement (arrows) in the jejunum.

• Complications of the disease may include:– nonobstructive intussusception
and – ulcerative jejunoileitis with
circumferential thickening of the bowel wall seen at enterography.
– Cavitary mesenteric lymph node syndrome, • which is characterized by fat-fluid
levels, and the development of lymphoma or carcinoma, are rare associated conditions.
• The latter should be suspected when previously asymptomatic patients with celiac disease develop recurrent diarrhea, abdominal pain, or both after initiating a gluten-free dietary regimen.
– increased risk for lymphoma and carcinoma of the bowel
A patient with sprue, mural masses, and lymphoma of the ileum (arrow

Infectious Processes
• Infectious processes are rarely detected initially at MR enterography.
• However, MR imaging may be useful for visualizing small-bowel abnormalities that occur in the setting of chronic infectiousdiseases such as tuberculosis, as well as for monitoring such abnormalities during treatment.
• The diagnosis of infectious enterocolitis, a common cause of acute diarrhea, abdominal pain, and fever, rarely requires MR enterography; however, ileitis may manifest on MR images as segmental circumferential wall thickening of the terminal ileum and cecum with moderate or marked enlargement of the mesenteric lymph nodes.
• Perforation and fistulation may be complicating factors in infectious terminal ileitis

• GI tract tuberculosis tends to involve the ileocecal region;– cecum and ascending colon > terminal ileum.
• Characteristic MR features of tuberculous enteritis include:– asymmetric thickening of the ileocecal valve and medial wall of
the cecum with – deformation and contraction of the cecum and extension to the
terminal ileum. – Massive adjacent lymph nodes with central areas of necrosis are
often seen.
• It may be difficult to differentiate small-bowel tuberculosis from Crohn disease in the absence of a clinical history of tuberculosis or a positive tuberculin skin test result

Bacterial infection in a 35-year-old man with AIDS, bowel obstruction, and a mesenteric mass seen at CT. (a) Coronal FISP image from MR enterography shows thickened small-bowel loops (arrow) and a mesenteric mass (arrowhead). (b) Coronal gadolinium-enhanced T1-weighted fat-suppressed 3D VIBE image from MR enterography depicts enhancing thickened small-bowel loops (arrow) and the partly necrotic mesenteric mass (arrowhead). Biopsy of the mass revealed Mycobacterium infection.

• Less common small-bowel infections include giardiasis, nontuberculous mycobacterial infection, and histoplasmosis.
• Such infections are more commonly seen in the setting of acquired immunodeficiency syndrome (AIDS).
• The associated MR imaging findings tend to be nonspecific; these include: – bowel wall thickening, – a stratified pattern of bowel enhancement, and – enlargement of adjacent lymph nodes.

Diverticular Disease
• Jejunoileal diverticulosis – results from herniation of the mucosa at sites of small-bowel
weakening. – predominantly on the mesenteric border of the jejunum and
less frequently on that of the ileum. – Multiple smooth, rounded outpouchings of variable size may be
seen, with a discrete “neck” or constriction at the base. – Most cases are asymptomatic, and the condition is often
overlooked at cross-sectional imaging. – Chronic symptoms of small-bowel diverticular disease include
nonspecific abdominal discomfort and malabsorption in the presence of bacterial overgrowth.
– The condition is conservatively managed.

Small-bowel diverticula in a 40-year-old man with chronic abdominal pain, nausea, and diarrhea. Coronal FISP images from MR enterography (a obtained in a section anterior to b) show at least three small-bowel diverticula (arrows).

• Diverticulitis
– Resulting from acute inflammation or perforation of a diverticulum.
– At radiologic imaging, it manifests as inflammatory infiltration of the mesenteric fat around one or more diverticula of the small bowel.
– Although CT is the more commonly used imaging modality, diverticulitis of the small bowel may be diagnosed at MR imaging.

Systemic Sclerosis
• Systemic sclerosis is a connective-tissue disorder involving the lungs, kidneys, heart, and GI tract.
• The small bowel is the second most common site of GI tract involvement, after the esophagus.
• Systemic sclerosis is characterized by smooth-muscle atrophy and fibrosis with deposition of collagen and other pathologic changes that result in decreased small-bowel motility with stasis, bacterial overgrowth, diarrhea, and malabsorption.
• Diffuse dilatation of the small bowel may be seen and is most prominent in the jejunum.

MR enterography may reveal the classic “hidebound sign,” an increased number of jejunal folds crowded together despite luminal distention, an appearance produced by
small-bowel fibrosis and contraction.
Systemic sclerosis in a 54-year-old woman with mild diarrhea. Coronal T2-weighted half- Fourier RARE (a) and gadolinium-enhanced T1-weighted fat-suppressed 3D VIBE (b) images from MR enterography show diffuse dilatation of the small bowel to the level of the cecum, without obstruction. Note the increased frequency of jejunal folds (arrow).

• In some patients, small-bowel sacculation may be seen as multiple wide-mouthed outpouchings containing all layers of the bowel; these features are due to asymmetric bowel wall fibrosis, especially in the jejunum.
• Other possible findings include intestinal pseudo obstruction, transient intussusception, and a benign form of pneumatosiscystoides intestinalis
Diffuse dilatation of small bowel in Scleroderma (arrowheads) shown at coronal HASTE. There is no wall thickening and folds are preserved. Note stasis of bowel content (asterisk) due to reduced peristalsis

Bowel Duplication
• Bowel duplications are uncommon congenital anomalies that appear on MR images as smoothly rounded, fluid-filled cystic or tubular structures with thin, slightly enhancing walls containing smooth muscle.
• These structures are either continuous with or located adjacent to the GI tract
Duodenal duplication cyst in a 32-year-old man with nonspecific abdominal pain. Coronal FISP image from MR
enterography shows a round, fluid-filled lesion in communication with the duodenum (arrow).

Familial Mediterranean fever • Rare autosomal
recessive disease that is characterized by attacks of fever and serosalinflammation.
• On MR enterography, enhancing bowel wall thickening of the jejunum and ileum is seen with especially serosal enhancement.

Incidental Findings
• In a series, the rate of potentially significant incidental findings not involving the small bowel was 3.5%.
• Incidental findings ranged from pancreatic and hepatic masses to endometrial cancer and extraentericcomplications of inflammatory bowel disease such as sacroilitis or primary sclerosing cholangitis .

Conclusion
• Enterography has already become the standard of care in small bowel imaging particularly in IBD.
• It clearly outperforms and will largely reduce fluoroscopic barium studies for evaluation of the small intestine to being problem-solving tools.
• Enterography will not replace visual optical endoscopy, nor will it replace capsule endoscopy, but will play an important role as a complement to capsule endoscopy.
• CT and MR enterography were similar in their capabilities to depict active inflammation, as well as extraenteric complications and other CD-associated findings, in the small bowel.
• Although MR imaging is costlier than SBFT and CT enterography, it can be repeated without subjecting the patient to additional ionizing radiation.
• Because CT and MR enterography are similar in their diagnostic abilities, it is proposed that MR enterography be used as a radiation-free alternative for evaluation of patients with chronic diseases, especially those who are young and may require repeated examinations.