Embed Size (px)
Citation preview
The optimal timing of initiation and duration of DAPT
Magdy El-MasryProf. of Cardiology
Tanta University
2015 Great Debate

? Single-antiplatelet therapy (SAPT) versus Dual-antiplatelet therapy (DAPT)
? Longer – versus shorter – duration DAPT
Answers to difficult questions in DAPT
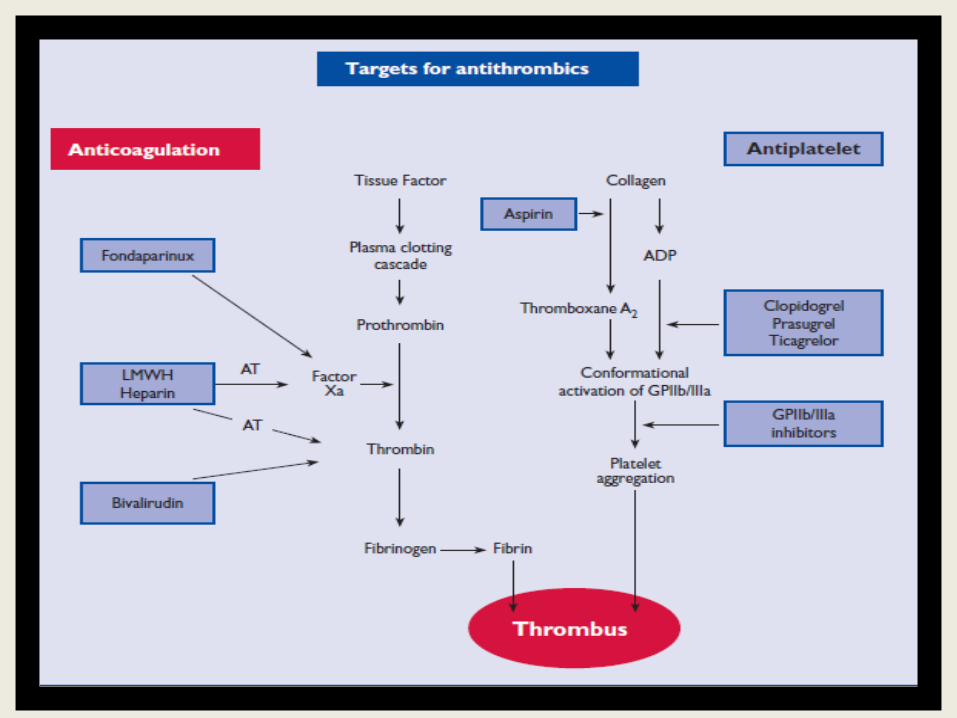
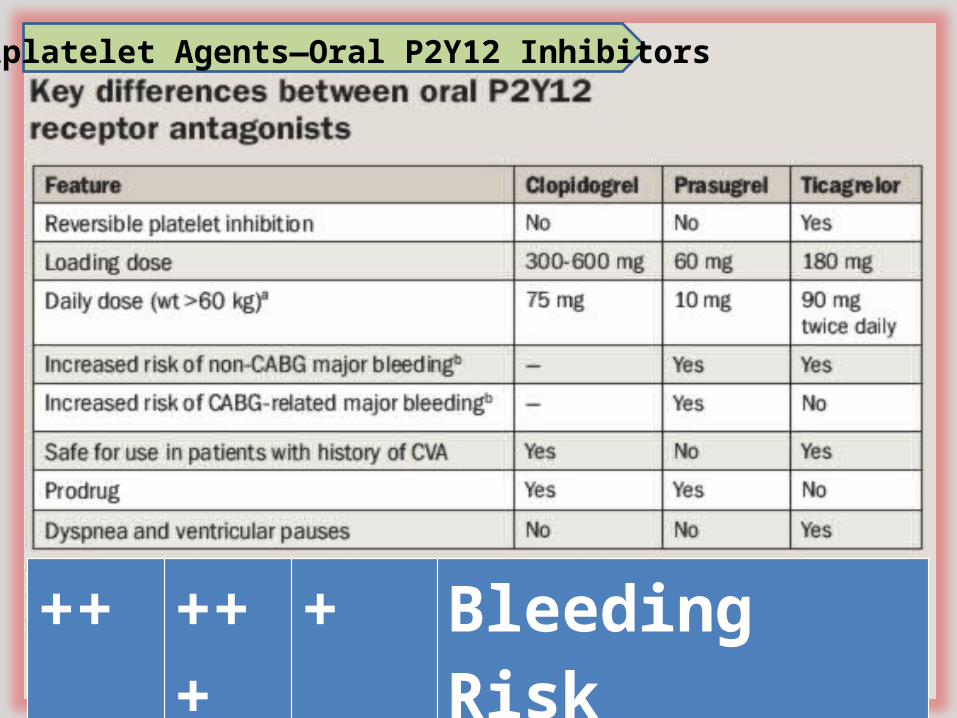
Antiplatelet Agents—Oral P2Y12 Inhibitors
++ +++
+ Bleeding Risk

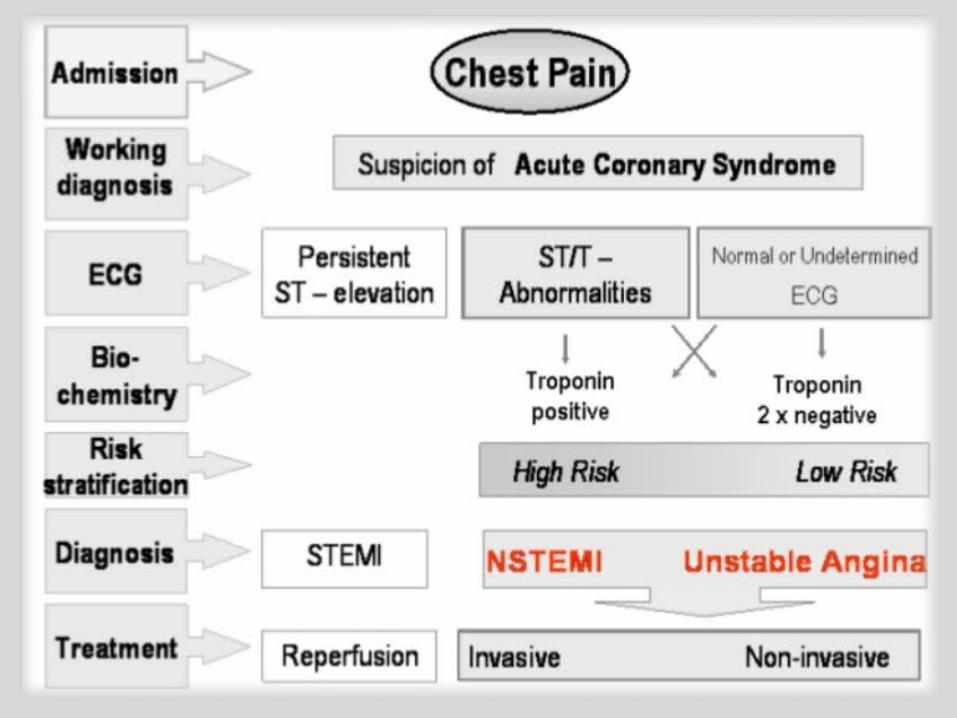
Spectrum of Coronary Artery Disease
AcuteCoronary Syndromes
StableCoronary Artery Disease


Moderate to high-risk NSTEACS as defined in PLATO: ≥2 of: (1) ischemic ST changes on ECG; (2) positive biomarkers;and (3) 1 of the following: 60 years of age or greater, previous MI or CABG, CAD > 50% stenosis in 2 vessels, previous ischemic stroke, diabetes,peripheral arterial disease, or chronic renal dysfunction.
Canadian Journal of Cardiology 29 (2013) 1334-1345
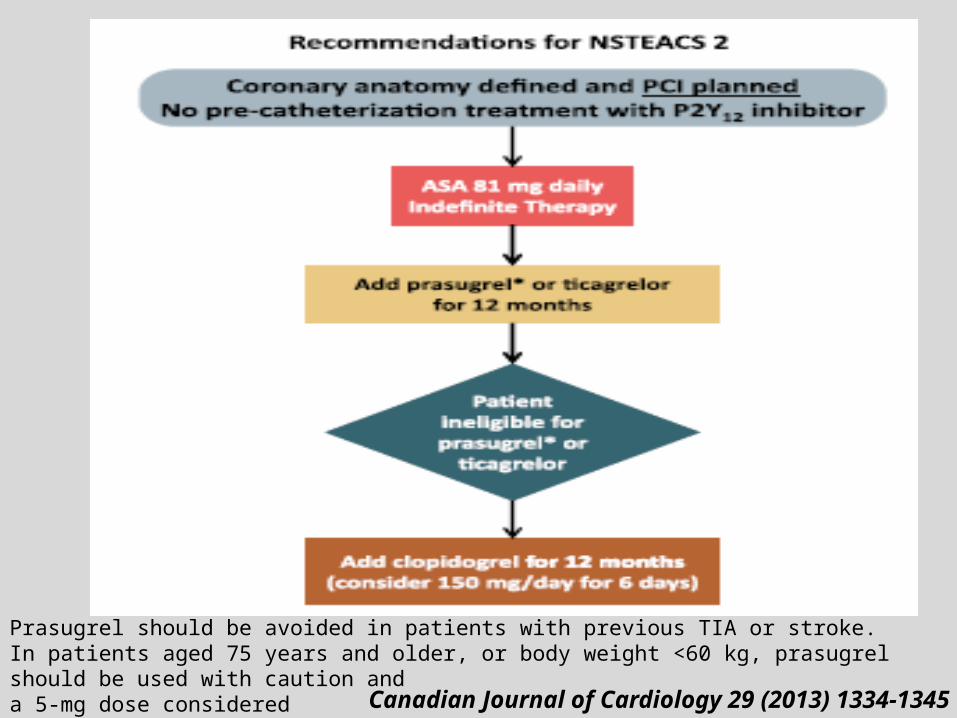
Canadian Journal of Cardiology 29 (2013) 1334-1345
Prasugrel should be avoided in patients with previous TIA or stroke. In patients aged 75 years and older, or body weight <60 kg, prasugrel should be used with caution and a 5-mg dose considered

Canadian Journal of Cardiology 29 (2013) 1334-1345
Prasugrel should be avoided in patients with previous TIA or stroke. In patients aged 75 years and older, or body weight <60 kg, prasugrel should be used with caution and a 5-mg dose considered

Canadian Journal of Cardiology 29 (2013) 1334-1345
Antiplatelet Therapy Post-CABG
? Single-antiplatelet therapy (SAPT)
? Dual-antiplatelet therapy (DAPT)

Management of SCAD patientsAngina relief Event prevention
• β-blockers and/or CCB
Ivabradine Long-acting nitrates Nicorandil Ranolazine Trimetazidine
• Lifestyle management• Control of risk factors
• Aspirin (if intolerance, consider clopidogrel)
• Statins• Consider ACE inhibitors or ARBs
Consider coronary angio → PCI or CABG
Short-acting nitrates, plus
1st line
2nd line
2013 ESC guidelines on the management of stable coronary artery disease.

SCAD
Medical Elective PCIElective CABG
Single-antiplatelet therapy (SAPT) Dual-antiplatelet therapy (DAPT)
Aspirin (Indefinite Therapy)If aspirin intolerant :
Clopidogrel (Indefinite Therapy)
Aspirin plus Clopidogrel BMS : 1 month DES : 6-12 months
The Balance between Anti-ischemic Efficacy and Bleeding Risk of Antithrombotic Therapy
in PC I
Thus, the thousand dollar question is : Where is the sweet spot between ischaemia and bleeding?
What is the optimal duration of DAPT
after PCI?

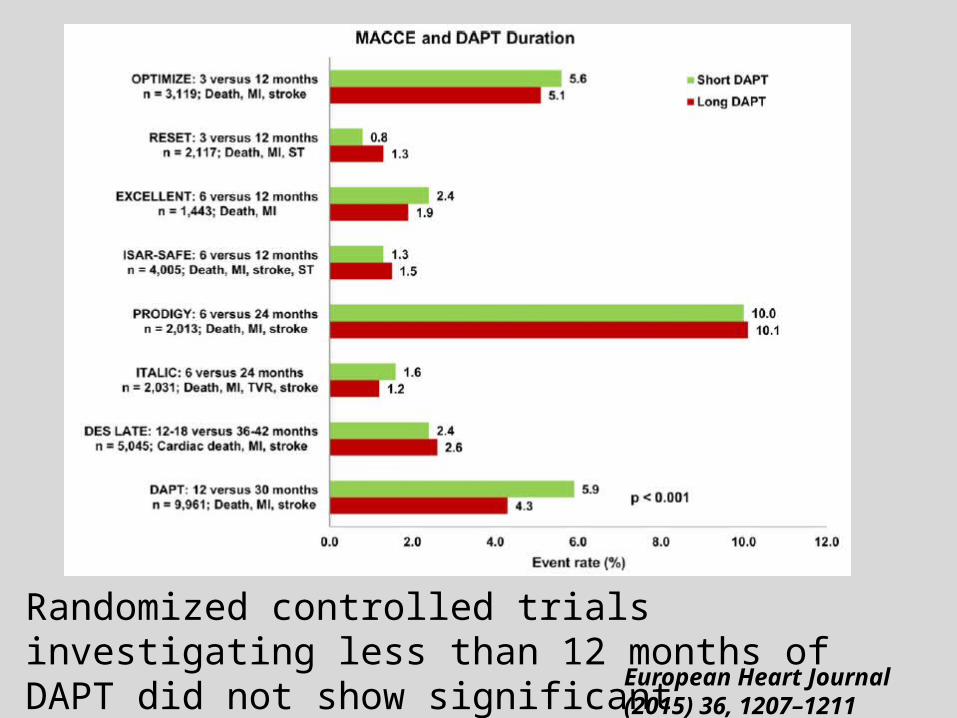
Randomized controlled trials investigating less than 12 months of DAPT did not show significant differences in their composite endpointscompared with 12 months or prolonged DAPT.
European Heart Journal (2015) 36, 1207–1211

Rates of bleeding are consistently higher for prolonged DAPT, reaching statistical significance in some studies
European Heart Journal (2015) 36, 1207–1211

The appropriate duration of DAPT for patients following placement of a DES remains controversial.
The “Will this trial change my practice?” sessions at PCR 2015
Will this trial change my practice? The Dual Antiplatelet Therapy (DAPT) study – 12 or 30 months of dual
antiplatelet therapy after drug-eluting stents
Should the DAPT study shift the standard of care from 12 months to 30 months in patients who receive a DES?
Does the increased risk of bleeding essentially offset the benefits?
To whom would you recommend continued DAPT? In whom would you avoid it?

A call for individualised medicine(precision medicine or personalized medicine)
How long should DAPT be continued ? 3, 6, 12, 24, 30 months
The therapeutic sweet spot between reduced ischaemia and increased bleeding markedly differs between patients.


Pharmacogenomics : Determining the right drug in the right dosage at the right time for
each and every patient
Pers
onal
ized
Trea
tmen
t:
Dre
am o
r Rea
lity?
Thromb Haemost 2015; 113: 37–52
Pharmacogenomics

Ischemic RiskBleeding Risk
Balanced Benefit/Risk Ratio
Tailoring antiplatelet therapy : a step toward individualized therapy to improve clinical outcome?

Proposed duration of dual antiplatelet therapy after DES (based on individual risk)
European Heart Journal (2015) 36, 1207–1211

Long-term risk factors for stent thrombosis after PCI
Pharmacological factors
Patientcharacteristics
Proceduralfactors
-Premature discontinuationof DAPT
-Slow metabolizers of the antiplatelet
pro-drug
-Diabetes-ACS
-LV dysfunction-Malignancy
-Stent type-Stent undersizing-Incomplete stent
expansion-Incomplete apposition
-Greater stent length-Side branch stenting
-Overlapping stents-Small vessel calibre
European Heart Journal (2015) 36, 1207–1211

Pharmacologicalfactors
Patientcharacteristics
Proceduralfactors
-Prolonged DAPT-Concomitant use
of OAC
-Age-History of bleeding
-Low body weight-ACS
-Thrombocytopenia-GI disease
-Impaired kidney function-Liver disease
-Cerebrovascular accident-Malignancy
Short-term riskfactors:
-Femoral access,-Large sheath size
-No vascularclosure device
Long-term riskfactors:
-Unknown
Long-term risk factors for bleeding after PCI
European Heart Journal (2015) 36, 1207–1211
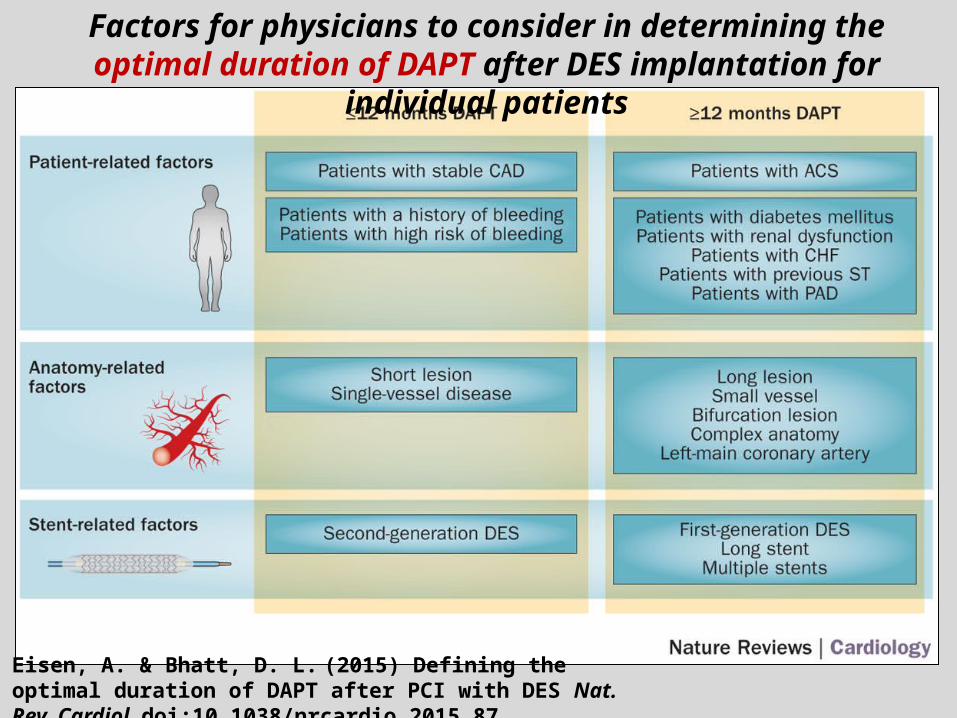
Factors for physicians to consider in determining the optimal duration of DAPT after DES implantation for individual patients
Eisen, A. & Bhatt, D. L. (2015) Defining the optimal duration of DAPT after PCI with DES Nat. Rev. Cardiol. doi:10.1038/nrcardio.2015.87
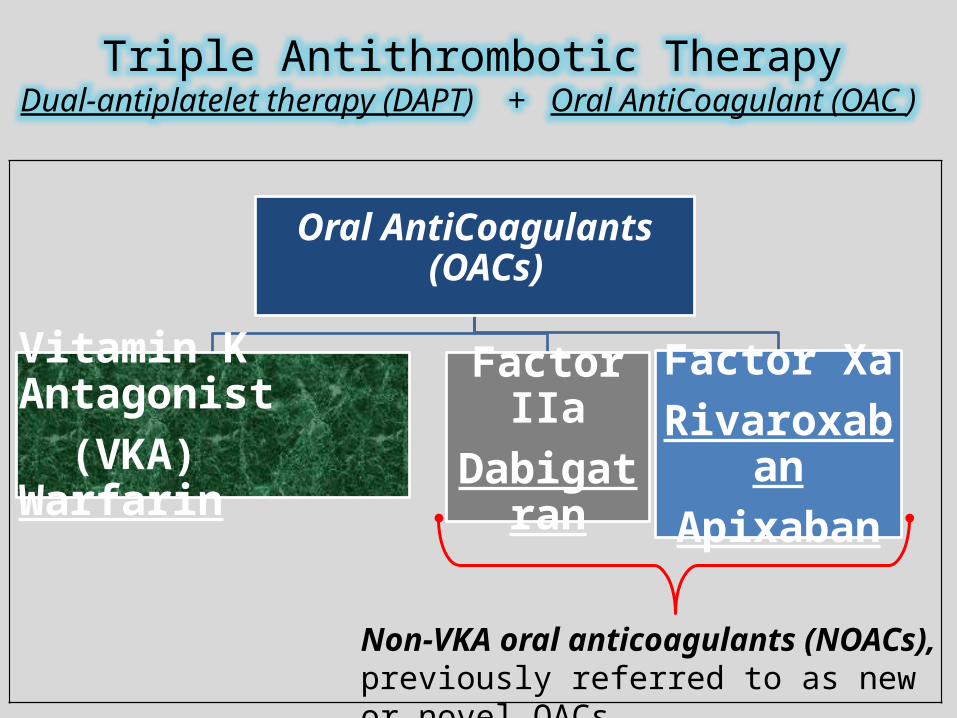
Triple Antithrombotic TherapyDual-antiplatelet therapy (DAPT) + Oral AntiCoagulant (OAC )
Oral AntiCoagulants (OACs)
Vitamin K Antagonist(VKA )Warfarin
Factor IIaDabigatran
Factor XaRivaroxaban
Apixaban
Non-VKA oral anticoagulants (NOACs), previously referred to as new or novel OACs

Triple Antithrombotic TherapyRisky but sometimes necessary
Dual-antiplatelet therapy (DAPT):Oral AntiCoagulant (OAC):


Continuing DAPT + OAC
Bleeding risk
Discontinuing OAC
Stroke risk
Discontinuing DAPT
Stent thrombosis
risk
Triple Antithrombotic Therapyin AF patients with ACS/PCI
Issues for Mr. X
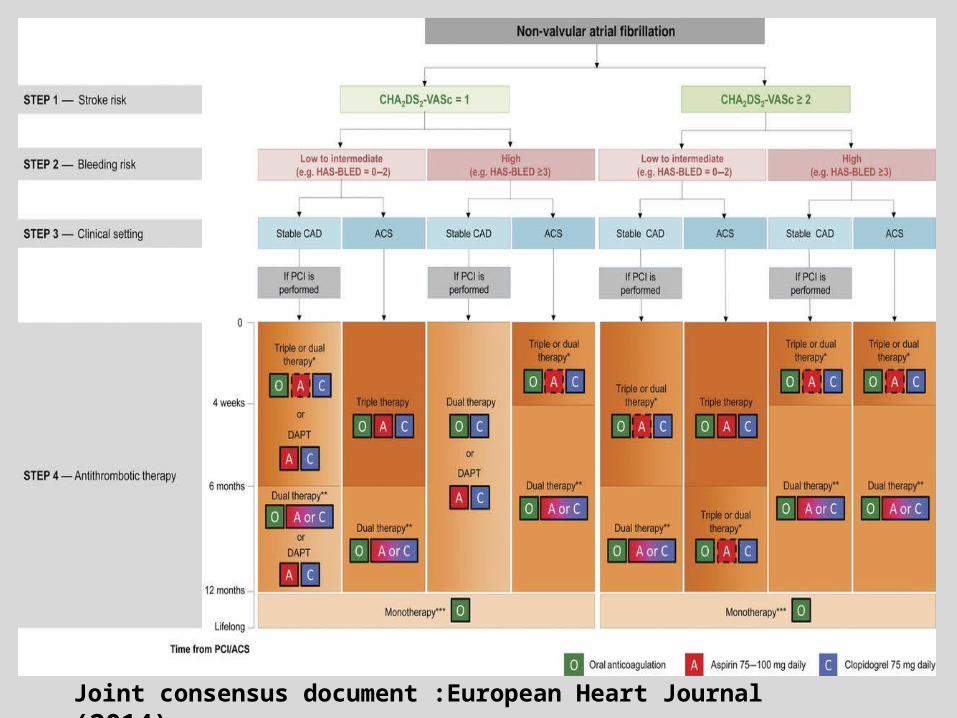
Joint consensus document :European Heart Journal (2014)

Clinical settingElective PCI in stable CAD
ACS (either STEMI or NSTEMI )
Stroke riskCHA2DS2-VASc score
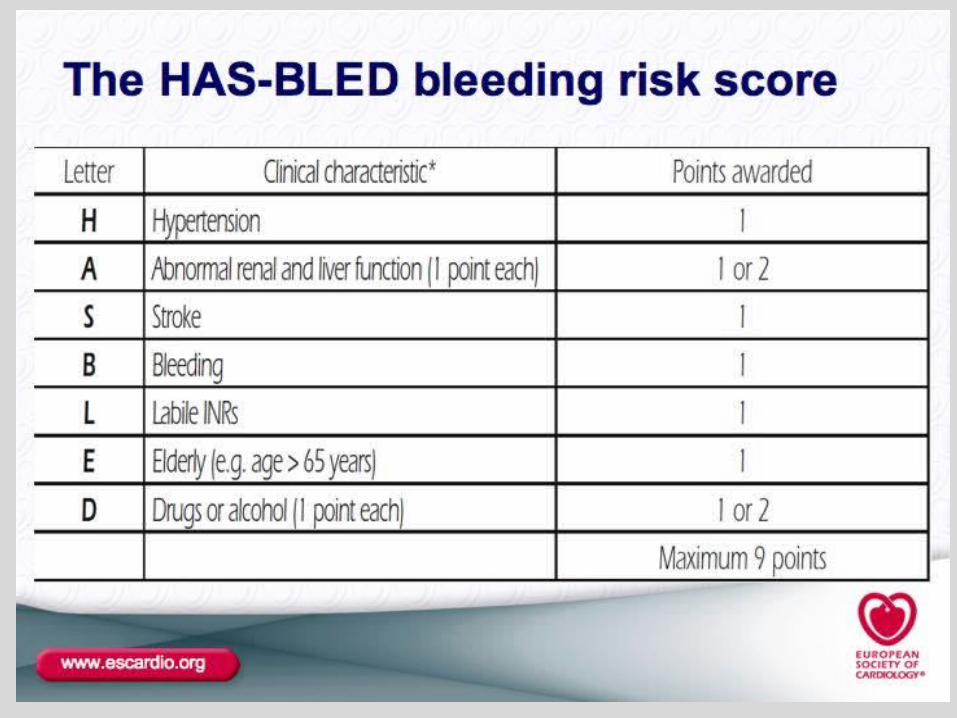
Bleeding riskHAS-BLED score
Antithrombotic therapy Triple(OAC+DAPT) , dual(OAC+SAPT) , mono(OAC)
Antithrombotic management in NVAF patients with ACS/PCI

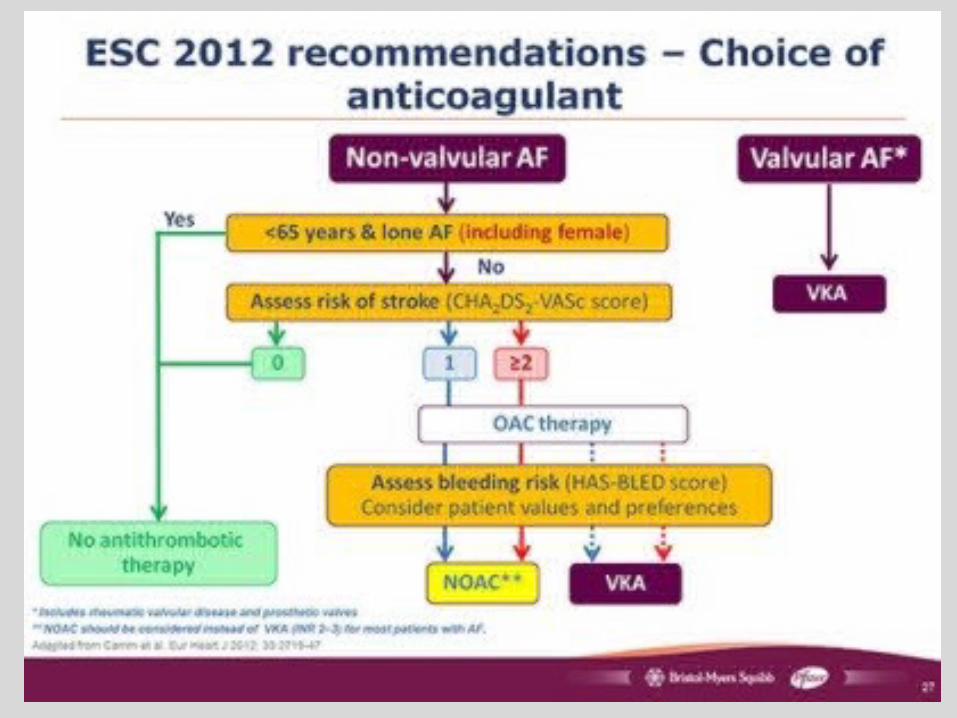
Non-valvular AF : Stroke risk
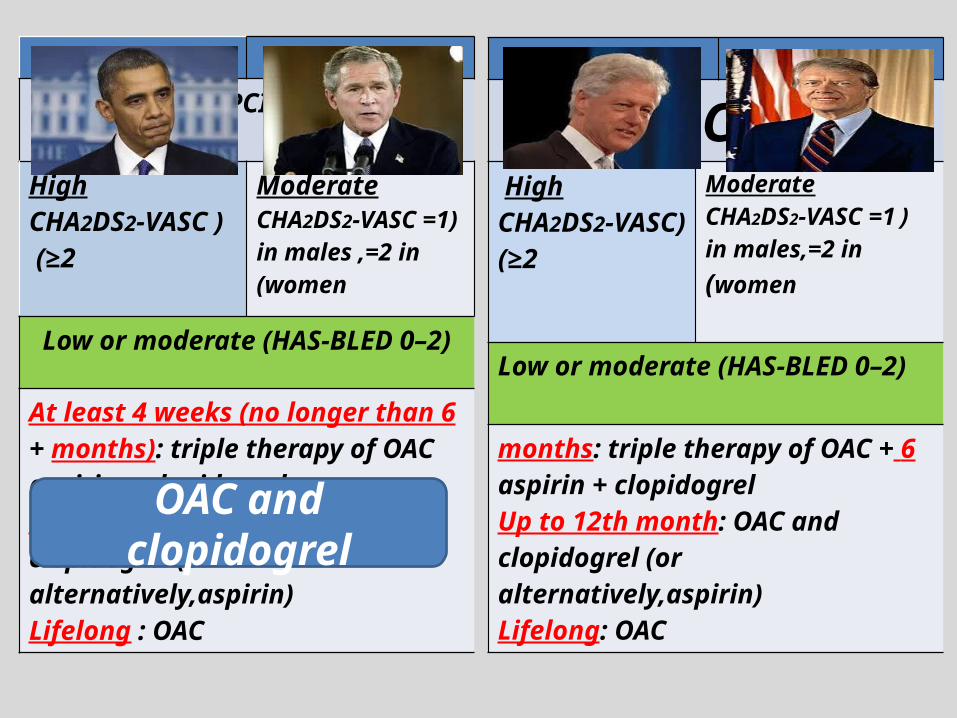
Elective PCI in SCAD
High( CHA2DS2-VASC
≥2 )
Moderate(CHA2DS2-VASC =1
in males ,=2 in women)
Low or moderate (HAS-BLED 0–2)
At least 4 weeks (no longer than 6 months): triple therapy of OAC+
aspirin + clopidogrelUp to 12th month: OAC and clopidogrel (or alternatively,aspirin)Lifelong : OAC
ACSHigh
(CHA2DS2-VASC ≥2)
Moderate(CHA2DS2-VASC =1 in
males,=2 in women)
Low or moderate (HAS-BLED 0–2)
6 months: triple therapy of OAC + aspirin + clopidogrelUp to 12th month: OAC and clopidogrel (or alternatively,aspirin)Lifelong: OAC
OAC and clopidogrel
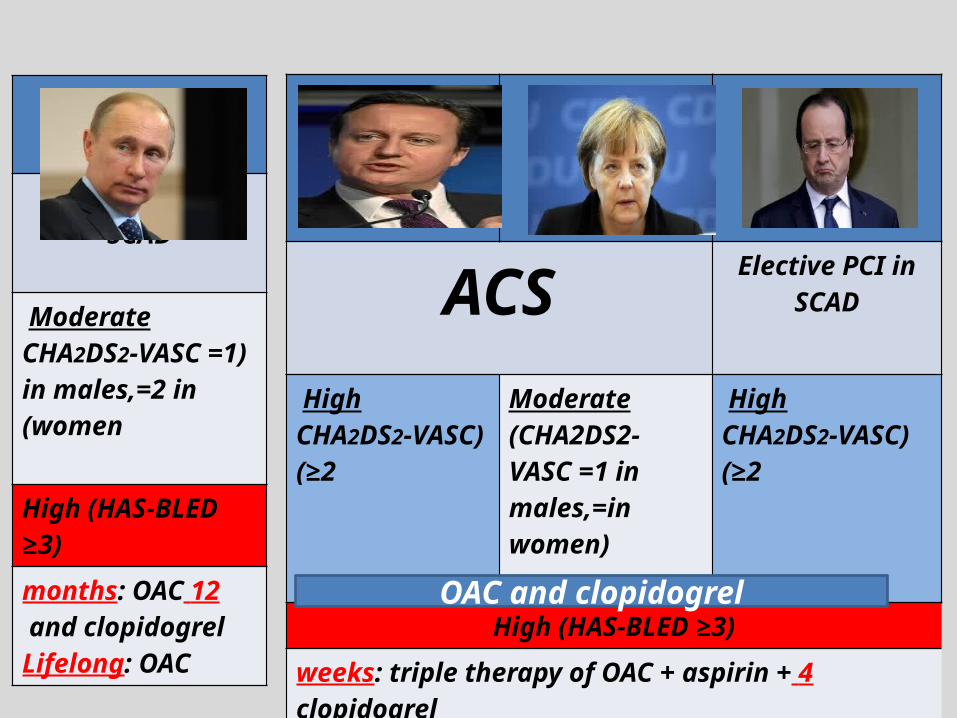
Elective PCI in SCAD
Moderate (CHA2DS2-VASC =1 in
males,=2 in women)
High (HAS-BLED ≥3)
12 months: OAC and clopidogrel
Lifelong: OAC
ACS Elective PCI in SCAD
High (CHA2DS2-VASC
≥2)
Moderate (CHA2DS2-VASC =1 in males,=in women)
High (CHA2DS2-VASC
≥2)
High (HAS-BLED ≥3)
4 weeks: triple therapy of OAC + aspirin + clopidogrelUp to 12th month: OAC and clopidogrel (or alternatively,aspirin)Lifelong: OAC
OAC and clopidogrel

For PCI, BMS may be considered to minimize duration of DAPT Class IIb C
After coronary revascularization in patients with CHA2DS2-VASc score ≥2, it may be reasonable to use clopidogrel concurrently with oral anticoagulants but without aspirin Class IIb B

The balance of bleeding and ischaemic events in surgical patients after
stenting.
Continuing DAPT
Bleeding risk
Discontinuing DAPT
Stent thrombosis risk
Issues for Mr. X
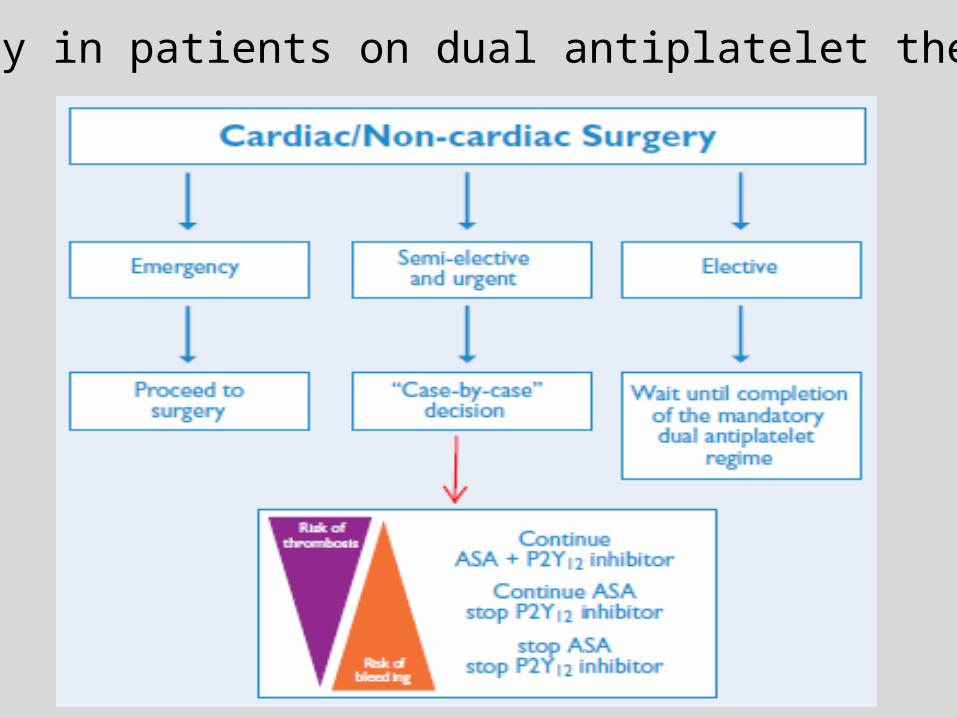
Surgery in patients on dual antiplatelet therapy
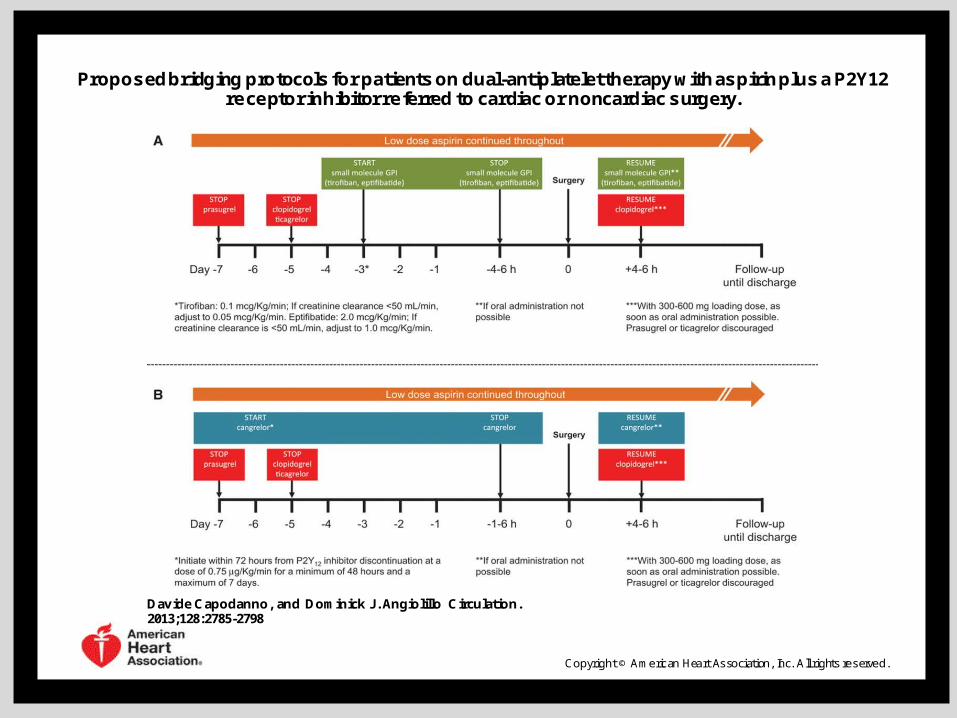
Proposed bridging protocols for patients on dual-antiplatelet therapy with aspirin plus a P2Y12 receptor inhibitor referred to cardiac or noncardiac surgery.
Davide Capodanno, and Dominick J. Angiolillo Circulation. 2013;128:2785-2798
Copyright © American Heart Association, Inc. All rights reserved.

Rabeprazole ------------- PARIET
Pantoprazole -----------CONTROLOC
Omeprazole --------------LOSEC
Lansoprazole -----------LANZOR
Esomeprazole ---------NEXIUM
(Circ Cardiovasc Qual Outcomes. 2015)
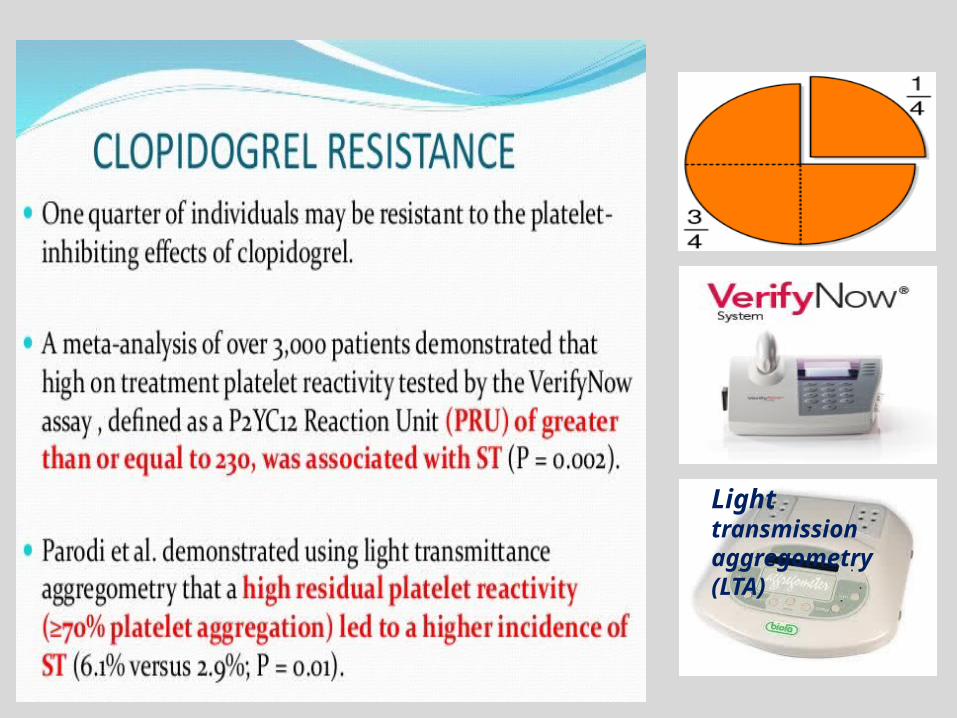
Light transmission aggregometry (LTA)
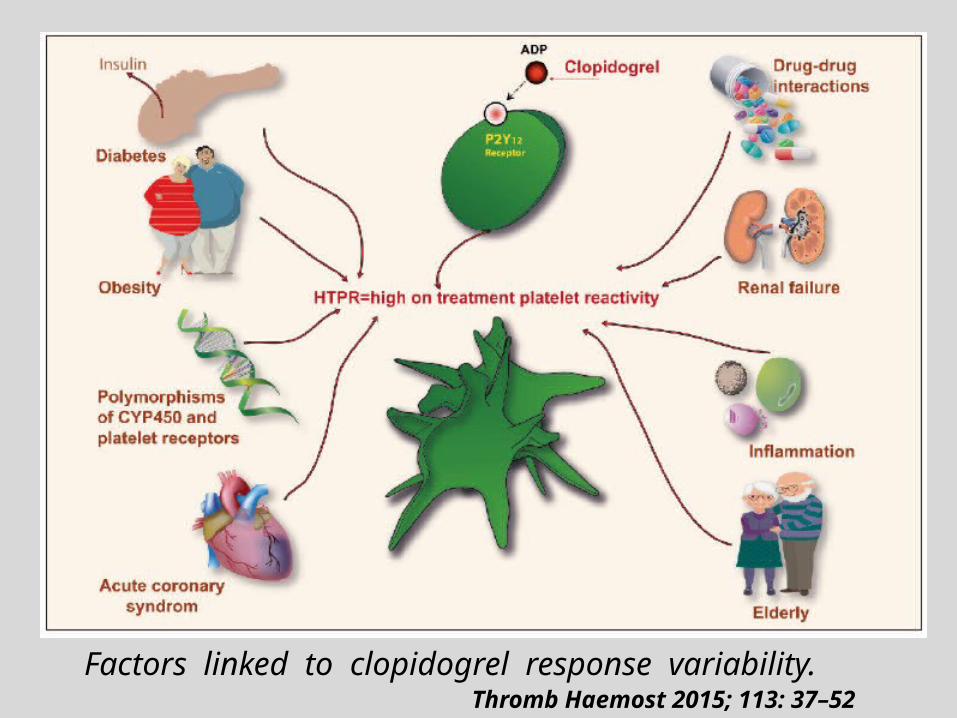
Factors linked to clopidogrel response variability. Thromb Haemost 2015; 113: 37–52

A proposed algorithm for personalised antiplatelet treatment with P2Y12
receptor blockers

*The PREDICT score might be
used when ticagrelor or
prasugrel are not available or
contraindicated.