Embed Size (px)
Citation preview

Fahad H. Al Hulaibi
Orthopedic Resident
NGH
DEVELOPMENTAL
DYSPLASIA OF THE HIP

Abnormal relationship between acetabulum & femoral head
resulting :
Dysplasia, possible subluxation &dislocation of the hip.
DEFINITION

most common orthopedic disorder in newborns
most common in left hips in females
bilateral in 20%
EPIDEMIOLOGY

1st born
Female ×5
Breach presentation 3%
Large baby
+ve family history 10%
Oligohydraminous.
RISK FACTORS
Cambpell’s

Initial instability
(maternal and fetal laxity, genetic laxity, and intrauterine and
postnatal malpositioning )
leads to dysplasia
leads to gradual dislocation
PATHOPHYSIOLOGY

Typically:
Antero-lateral of acetabulum
In CP patient:
Posterio-superior of acetabulum
WHERE IS THE DEFICIENCY

Torticollis in 8%
ASSOCIATED CONDITIONS
Cambpell’s


Metatarsus adductus (10%)
ASSOCIATED CONDITIONS

Spine anomaly
ASSOCIATED CONDITIONS

- Vital signs
- Wight
- Height
- HC
- Head to toe examination.
- Look for associated conditions. ( neck, spine, foot)
GENERAL EXAMINATION

Pt < 3 month
- Barlow test.
- Ortolani test.
- Galeazzi test.
Pt > 3 month
- Limitation in Abduction.
- LLD.
Pt > 1 year
- Pelvic obliquity.
- Lumbar lardosis.
- Trendelberg gait.
- Toe walking.
LOCAL EXAMINATION




after the femoral head begins to ossify 4-5 Month
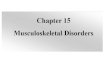
IMAGING

<25 >25

useful before femoral head ossification (<4 -6 mos)
ULTRASOUND


> 60
< 55

alpha angle
angle created by lines along the bony acetabulum and the ilium
normal is greater than 60°
beta angle
angle created by lines along the labrum and the ilium
normal is less than 55

ARTHROGRAM

Inverted labrum
Inverted limbus
Transverse acetabular ligament
Pulvinar
Thick ligamentous teres
Iliopsoas tendon contracture.
OBSTACLES THAT BLOCK REDUCTION

after reduction and hip spica
CT SCAN

Treatment

< 6 months & reducible hip
Success rate up to 95% ( C a m b p e l l )
PAVLIK HARNESS


Complication of pavlic harness: < 1%
1. AVN.
In extreme abduction
2. femoral nerve palsy
In hyper flexion
( C a m b p e l l )

When to say It’s failed Pavlic harness ?
3 to 4 weeks with no improvement

Pavlic harness failed
Patient 6-18 months
CLOSED REDUCTION, HIP ARTHROGRAM,
ADDUCTOR TENOTOMY + HIP SPICA

DDH > 2 yr with residual hip dysplasia
failure of closed reduction
Increased Acetabular index.
OPEN REDUCTION, PELVIC OSTEOTOMY
+_ FEMORAL SHORTENING

Femoral anteversion
Coxa valga
FEMORAL SHORTENING

PELVIC OSTEOTOMIES
Ost Age Coverage correction Hinge Contraindications
Salter 1-9 years Supero-
lateral
10-15 Symphysis • Posterior wall
deficiency
• Neurogenic hips
Pember-
Dega
18 mth All 10-40 Triradiate Coxa Magna
Double-
triple
8-15
years
Supero-
lateral
10-50 Symphysis
Open triradiate
Ganz Closed
triradiate
All 10-60
Most
Separate Open triradiate
Shelf Closed
triradiate
All - - Open triradiate
Chiari Closed
triradiate
All - - Open triradiate



COMPLICATIONS
Redislocation
Residual dysplasia
Lateralization
Stiffness
Impengement
Early OA
AVN

THANK YOU