Embed Size (px)
DESCRIPTION
Citation preview

Mental Health Problems of Older Adults
Dr. Peter Brown RN, DNE, BA Hons,
MA, PhD, FRCNA, ACMHN
Associate Professor
Acting Head, School of Health
Charles Darwin University

Mental Health Problems in Old Age
1. Mental health problems which occur at a
younger age and carry over into old age
2. Mental health problems occurring in old
age, eg. delirium, dementia, depression
3. Old age, people 65 years and over

DeliriumDSM IV-TR
• a) Disturbed consciousness, reduced ability
to focus, sustain, shift attention
• b) Change in cognition or perceptual
disturbance
• c) Develops over a short period of time &
fluctuates over the day

Delirium
DSM IV (Cont’d)
d) History, physical examination, lab findings:
- related to a general medical
condition; or
- symptoms related to
substance intoxication; or
- medication use

Delirium in Older Adults
Introduction - results of systematic review• Often overlooked & misdiagnosed• Poorly recognised by nurses• Nurses perform superficial mental status
assessments• Documentation of patients’ cognitive status is
seldom accurate
(Steis & Flick, 2008)

Delirium
• Confusion may be obvious or not so obvious (‘Quiet’ confusion)
• Acute confusion (Delirium)
• Chronic confusion (Dementia)
• Acute on chronic (Delirium on Dementia)
eg. Older person with dementia experiences
a urinary tract infection

Delirium
Why does it occur in older adults? Disruptions to neurological pathways &
neurotransmitter systems; Medications interfere with cholinergic
neurotransmission Pathophysiology is not well understood;

Disruptions to neurological pathways & neurotransmitter systems

Delirium: Predisposing factors
• Age 70 years & over• Pre-existing cognitive impairment• Severe medical illness; infection• Depression (subjective confusion)• Abnormal sodium levels • Visual impairment• 3 or more medications• Surgical procedures

Delirium
Medications • 25% -31% of all medication
use over 65 years of age
• 60-90% community elderly
use medication
• Over 50% take more than
one medication
• On average 2-4 medications

Delirium
Environmental Causes
- Restraints
- Unfamiliar environment
- Sensory deprivation
- Sensory overload
- Sleep deprivation

ASSESSMENT: HOW TO RECOGNISE DELIRIUM
• Obtain an accurate history
• Ongoing assessment to check variability
• Abbreviated Mental Test (AMT)
• Confusion Assessment Method (CAM)
- When – Day 1, 6 and after discharge
- Patients considered at high risk
- All patients over 75
- Sudden change in behaviour or cognition

DELIRIUM DEMENTIA
ONSET acute usually insidious
DURATION usually < 1 month at least 1 month usually much longer
ORIENTATION faulty, at least for a time; may be correct in mild tendency to mistake cases unfamiliar with familiar
THINKING disorganised impoverished (thinking is reduced)
MEMORY recent impaired both recent and remote impaired
ATTENTION invariably disturbed, may be intact hard to direct or sustain
AWARENESS always reduced, tends to usually intact fluctuate during daytime & be worse at night
ALERTNESS increased or decreased normal or decreased
PERCEPTION misinterpretations often present misinterpretations often absent
SLEEP/WAKE- always usually normal for age FULNESS

Nursing Management
1) Environment – as quiet as possible, reduce stimulation; safety; not too restrictive; night light
2) Physical needs – adequate nutrition and fluids; oral hygiene; care of skin & oral hygiene; bowels; observations; comfort needs
3) Non-pharmacological strategies

Nursing Management
3) Protective needs – over-activity; injury; exhaustion; impulsivity; aggression; observation; specialling; reduce restraints
4) Orientation needs – reality orientation; clocks & calendars; providing information; speak in clear voice; identify self & context, others & the person by name; glasses & hearing aids; personal mementos; sustained nursing interactions (at least 10 minutes);

Delirium: Management
Patients experiencing severe behavioural &/or emotional symptoms
- one on one nursing
- encourage family members attendance
- consistent staff members
- specialised delirium rooms
- expert psychiatric consultation
- caution with antipsychotic medication

Delirium: Management
1. Discharge planning & follow-up
- Patient & family education
- Follow-up, professional monitoring & treatment
- Post-delirium counselling
2. Staff education

Dementia
Dementia is a syndrome (has lots of symptoms) which is acquired (genetic or age-related), chronic (lasts months or years), global (not just memory problems), impairment of higher brain function (frontal, parietal & temporal lobe involvement) in an alert patient (looks okay) which interferes with the ability to cope with daily living

DEMENTIA
Types:• Alzheimer’s (53%)
• Vascular dementia (17%)
• Alzheimer’s and Vascular dementia
(19%)
• Parkinson’s disease (10%)
• Diffuse Lewy Body Disease (up to
30%)
• Fronto-temporal dementia (up to 10%)

DEMENTIA (con’t)
Dementia facts
1. 2001 – 210,000 60 yrs & over - mod. To severe dementia
2. Nos. are expected to increase by 65% by
year 2040 (460,000)
2. Prevalence of mod.-severe
4% for 60+; 16% for 80+; 24% for 85+

ALZHEIMER’S DISEASE
DSM IV
(1) multiple cognitive deficits (eg. memory
loss)
(2) 1 or more of following:
* aphasia – difficulty taking in info
* apraxia – inability to carry out purposive
activities
* agnosia – inability to recognise ‘things’

ALZHEIMER’S DISEASE (con’t)
(3) (1) & (2) cause significant impairment in
social & occupational functioning
(4) gradual onset & continuing cog. decline
(5) not due to other CNS condition or
systematic condition
(6) doesn’t occur during course of delirium
(7) not another Axis I disorder, eg. depression

Alzheimer’s disease (con’t)
Levels
1. Mild
- 2 to 4 yrs; lack spontaneity;
- 120,000; most at home
- poor decision making; memory changes
- repetitious
- blame others when things go wrong

ALZHEIMER’s DISEASE (con’t)
2. Moderate
- 4-7 yrs from onset; 2 to 10 years
- forgets to eat; wanders; forgets names
- neglects personal hygiene
- forgetful of recent events
- easily frustrated
- just over half live in community

ALZHEIMER’S DISEASE (cont’d)
3. Severe
- 7-10 yrs from onset; 3 or more years
- dependent on care; unable to feed
- unable to recognise others
- wanders
- aggressive

ALZHEIMER’S DISEASE (con’t)
** Exact cause is unknown
1. Genetic:
- non-identical twins - 8% risk
- identical twins - 43%
- Down’s syndrome >35 yrs of age
- Chromosome 14 & 21 (early onset, familial)
- Chromosome 19 - late onset

ALZHEIMER’S DISEASE (con’t)
Risk factors
1. Increasing age - prevalence doubles every 5 years (eg. 60-64 - .7%; 65-69 – 1.4% etc)
2. Family history - increased risk 2-4 fold
3. Sex - women at greater risk than men
4. Head trauma - increases risk
5. Education - lower level of greater risk

ALZHEIMER’S DISEASE (con’t)
Histologic features
1. Neurofibrillary tangles
- consist of protein tau - found inside nerve
cells (resembles pairs of threads wound
around each other in a helix)

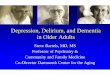
Plaques and Tangles

ALZHEIMER’S DISEASE (con’t)
2. Senile plaques - deposits of amyloid protein in the spaces between nerve cells - swollen nerve terminals - found in hippocampus & cerebral cortex3. Neuronal loss/synaptic loss - 90% in hippocampus - correlated with number of tangles & duration & severity of AD

Shrinkage of Hippocampus

ALZHEIMER’S DISEASE (con’t)
Neuroimaging in AD
1. CT - increased ventricular size & cortical
atrophy
2. MRI - hippocampal atrophy
3. SPECT - temporoparietal hypofusion
4. PET - temporoparietal & frontal
hypometabolism (glucose)

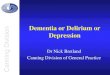
Positron Emission Tomography (PET) of a person with Alzheimer’s disease

Single-photon emission computerised tomography

ALZHEIMER’S DISEASE (con’t)
2 or more diseases2 or more diseases
1. Early onset
- more aphasia, apraxia, agnosia,
more rapid rate of progress; family history
2. Late onset
- more muscle rigidity, gait disorder

ALZHEIMER’S DISEASE (con’t)
Neuropsychological deficits in AD
1. Memory - encoding & retention; for
visuospatial skills
2. Visuospatial functioning
3. Word store; comprehension; reading
4. Problem solving; Flexibility; Awareness
5. Praxis; Anosognosia (lack of awareness of illness

ALZHEIMER’S DISEASE (con’t)
Behavioural Symptoms1. Personality change; depression
2. Wandering; suspiciousness; delusions
3. Hallucinations; disruption of sleep/wake
cycle
4. Inappropriate behaviour, sexual disinhibition
5. Controlling emotions

VASCULAR DEMENTIA
DSM IV-R
1. As for AD (1), (2), (3)
2. Focal neurological signs & symptoms
or laboratory evidence
3. Stepwise deteriorating course with
patchy distribution of deficits

Vascular dementia: Clinical features
1. Second most common cause of dementia
2.Gait disturbance; unsteadiness & falls

Vascular dementia: Clinical Features
3. Urinary frequency & urgency
4.Depression, emotional lability
5. Psychomotor slowing
6. Abnormal executive functioning

VASCULAR DEMENTIA (con’t)
1. 25% of patients with cerebrovascular disease develop demented
2. Cognitive impairment & dementia depend on:
a. extent of area of infarction
b. location of lesions, their bilaterality
& volume rather than their cause

VASCULAR DEMENTIA (con’t)
Aetiology
1. Occlusion of major cerebral artery
2. Minor multiple infarctions
3. Small vessel disease - white matter
4. Perfusion disturbances - cardiac arrest
5. Cerebral haemorrhage

DEMENTIA (con’t)DEMENTIAEarly warning signs1. MemoryMemory - recalling data, recall events, losing items, repetitive questioning2. Cognitive problems Cognitive problems - problems with complex activities, difficulty recognising familiar people & objects, language problems

DEMENTIA (con’t)
3. Behavioural changes Behavioural changes - withdrawal &/or inertia; inflexible attitude; irritability;
reduced planning & decision making
4. Specific incidents Specific incidents - confusion while on holiday; inability to recognise familiar faces; neglect of long-established behaviours

DEMENTIA (con’t)
Diagnostic process for dementia
1. Serious cognitive loss or normal ageing?
2. Is the cognitive loss psychiatric in origin?
3. Is it attributed to delirium?
4. Does it affect more than one part of the brain?
5. If dementia - what is the underlying condition?

DEMENTIA (con’t)
Challenging Behaviours Related to Dementia
* Wandering
* Sleep disturbances
* Eating disorders
* Agitation; Aggression
* Sexual inappropriateness
* Other?

LEWY BODY DISEASE
A syndrome in which Parkinsonism overlaps with features of Alzheimer’s disease & psychiatric phenomena. Brain pathology shows Lewy bodies identical to those in Parkinson’s Disease but scattered throughout the cortex

Lewy Body

COGNITIVE SYNDROMES ASSOCIATED WITH LB DISEASE
Lewy body variant of AD/SD of the LB type
1. Onset after 65 yrs of age
2.Mild extrapyramidal signs; unexplained falls; hallucinations
4.Dementia precedes or accompanies motor
symptoms
5. Neuroleptic sensitivity

Drug Therapy and Dementia
Drug Therapy
1. Age-related decline
2. Favourite drugs
3. Low initial dose; incremental increase
5. Hypnotics for night wandering
6.Neuroleptics
7.Anti-depressants (?); Review regularly

The Carer: The ‘Second Patient’
* primary carer, eg. wife, adult daughter
* physical, social & financial burdens;
depressive disorders (up to 30%)
* need to be vigilant about their health
* Alzheimer’s Association
* respite, day care

Dementia: Legal Issues
Legal Issues
* loss of capacity to consent treatment -
need to obtain permission to continue
treatment from carer or guardian
* assign enduring power of attorney early
in the illness
* alter Will early in illness

Dementia: Legal aspects
Driving
1. Mild dementia - ask to stop driving or
confine themselves to familiar routes
2. Mod. To Severe - ‘DO NOT DRIVE’
3. Dispute - refer to local RTA
4. If endanger others through work - drs,
engineers

Alzheimer’s Disease: Pharmacological
1. Cholinesterase boosters:
- Donepezil; Exelon; Rivastigmine;
Galantamine
2. Non-cholinesterase inhibitors:
- ginko biloba; vitamin E; NSAIs

Vascular Dementia:Treatment
• No drugs as such
• Treatment of stroke risk factors (eg.
smoking & hyperlipidemia; diabetes,
hypertension)
• Galantamine ( a memory enhancing drug)

Depression in Old Age
# Depression in older people is under-researched
# As common in old age as for other groups
# Complex interplay between vascular factors, physical illness, disability, socio-cultural risk factors (eg. Unemployment; divorce)

Depression in Old Age: Risk Factors
# Most common mental illness in older adults (40% of all new cases)
# Risk factors:1. Female gender2. Divorced or separated3. Low socioeconomic status4. Poor social supports5. History of depression

Depression in Old Age: Risk Factors (cont’d)
6. Physical illness
7. Pain & disability
8. Substance abuse
9. Medication
10. Personality
11. Grief

Depression in Old Age: Sequelae
Sequelae:Sequelae:
- unnecessary suffering
- excess physical & social disability
- exacerbation of co-existing illness
- earlier death (eg. Suicide)
- overuse of services

Depression in Old Age: Severe Depression
1. Major depressive disorder & Bipolar Depression
- feeling of despair; hopelessness; apathy
- delusional thinking; inability to
concentrate; suicidal thoughts
- sluggish digestion; constipation;
amenorrhoea; urinary retention;
anorexia; weight loss

Depression in Old Age: Moderate Depression (Dysthymia)
Dysthymia• Feelings of sadness; dejection; low self-
esteem; difficulties experiencing pleasure
• Psychomotor retardation; slowed speech; self-destructive behaviour
• Retarded thinking; difficulty thinking; sleep
disturbances; decreased libido; low energy levels

Depression in Old Age: PTSD
Post-traumatic Stress Disorder
- upsetting event
- fear, helplessness, horror
- event is persistently experienced
- avoidant of stimuli
- increased arousal
- many depressive symptoms

Depression in Older Adults
Depression in older adults
- Common in elderly living at home
- Common in nursing homes
- 60% inappropriately or inadequately
treated
- Associated with treatment refusal
- Treatable

Depression in Old Age: Assessment
Assessment Traps
- physical illness may cause identical features
- physical illness can trigger depression- response to physical illness seen as
a natural response but may need anti- depressants

Depression in Old Age: Assessment
Assessment Traps
- ‘pseudodementia’
- depression & dementia occurring
together
- assuming that the current picture has
been present for a long time/short time

Depression in Old Age: Assessment
Assessment: History
- look depressed’?
- decreased thought & movement
- ‘frozen’ face (expression-
less)
- ‘Omega’ sign (fixed,
furrowed forehead)

Depression In Old Age: Suicide
Assessment: Suicidal ideas
- don’t be afraid to ask about suicidal
thoughts
- look for the right moment to ask
- “Do you sometimes feel that life is not
worth living?”
- if the answer is “yes” try to explore

Depression in Old Age: Suicide
Assessment: Suicide
The following are not necessarily suicidal ideas:
- older people are prepared to talk about death in general
- content to go when time comes- inpatient for the time to come

Depression in Old Age: Treatments
• Antidepressants +++• ECT +++• CBT +++• Interpersonal psychotherapy ++• Psychodynamic psychotherapy ++• Reminiscence ++• Exercise ++

Nursing Management
• Observation (eg. for suicide)
• Safety issues
• Food and fluids
• Constipation
• Patient/Family education
• Medication