Embed Size (px)
Citation preview

DENGUE IN CHILDREN
-Dr.Apoorva.E PG,DCMS

EPIDEMIOLOGY
• Dengue is the most rapidly spreading mosquito-borne viral disease in the world
• Increase in incidence by over 30-fold in the last 50 years
• Currently endemic in all continents except Europe

ETIOLOGYTHE VIRUS
• DEN- family flaviviridae genus flavivirus
• Has four distinct serotypes (DEN1 – 4)
• DEN-2 and DEN-3 cause severe disease
• Cleaved by host and viral proteases into 3 structural proteins and 7 nonstructural proteins(NS)
THE VECTOR
• Transmitted by infected Aedes mosquitoes
• Highly urbanized,
fresh water,
day feeding mosquito

THE HOST
• Humans are the primary host of the virus
• Severity depends upon factors like gender,secondary infection,age and chronic diseases (sickle cell anemia, asthma , DM)
• Vertical transmission and through infected blood products +
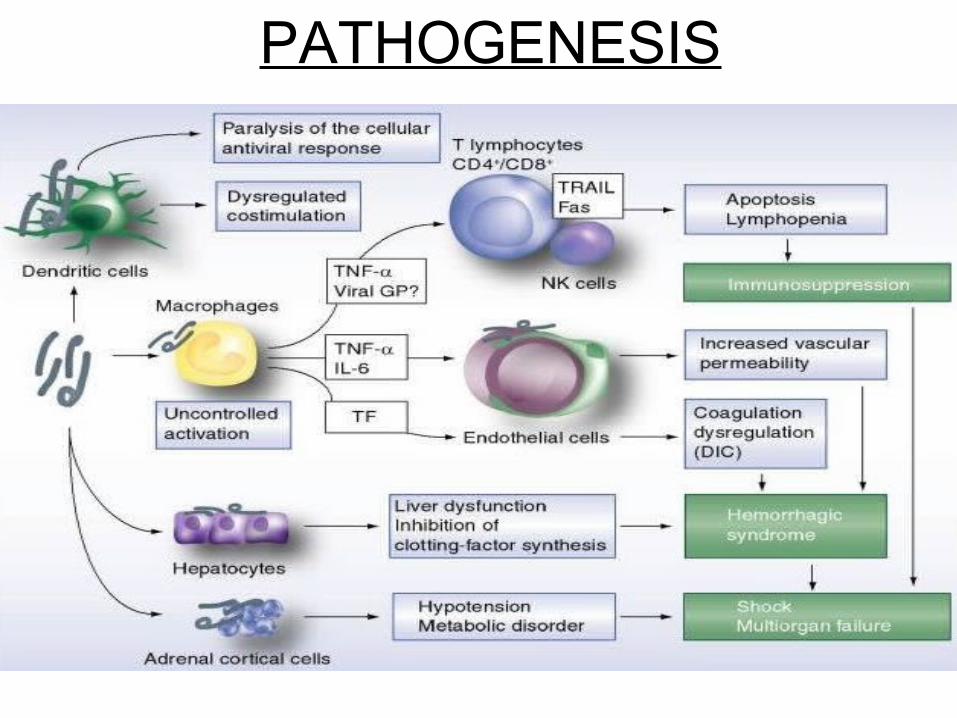
PATHOGENESIS

Capillary damage
Fluid leaks into extravascular spaces
Hemoconcentration Hypovolemia
Increased cardiac work Tissue hypoxia,metabolic acidosis

THROMBOCYTOPENIA
+
LIVER DAMAGE
+
DIC
DENGUE HAEMORRHAGIC FEVER

ANTIBODY DEPENDENT
ENHANCEMENT

• Specific antibodies start appearing around day 5 of illness.
• Infection with one serotype gives lifelong immunity to that type, but only short term protection against the other three.
• Secondary infection with DEN-2, DEN-3 is associated with dengue haemorrhagic fever.

CLINICAL MANIFESTATIONS
• Multisystem disease with a wide clinical spectrum
• Incubation period – 4 to 10 days
• Illness begins abruptly following the IP,divided into three phases
FEBRILE CRITICAL RECOVERY

FEBRILE PHASE
• High grade fever lasting for 2-7 days
• Accompanied by facial flushing,rash,myalgia,arthralgia,headache,nausea,vomiting,anorexia,sore throat,injected pharynx and conjunctiva.
• Petechiae,epistaxis,gum bleed may be seen.

CRITICAL PHASE
• Usually occurs on days 3-6 of the illness
• Lasts for 24-48 hours
• Progressive leukopenia,increasing hematocrit levels,decrease in platelet count precede plasma leakage
Ascites Pleural effusion Shock
• Prolonged shock leads to DIC which leads to severe haemorrhage
-Decrease in hematocrit
-GI bleeding usually
• Organ hypoperfusion can lead to hepatitis,myocarditis,encephalitis

RECOVERY PHASE
• Reabsorption of the fluid from extravascular compartment occurs
• General well-being improves,appetite returns,hemodynamic status stabilizes,urine output becomes normal,GI symptoms abate
• Generalized pruritus,bradycardia ++


CLINICAL PROBLEMS ENCOUNTERED DURING
DIFFERENT PHASES

DENGUE CASE PROBABLE DENGUE (live in/travel to endemic area+fever+any of the following
two criteria : rash,nausea/vomiting,aches,positive tourniquet test,leukopenia,any warning sign)
WARNING SIGNS
NEGATIVE POSITIVE
DENGUE WITH SEVERE WARNING SIGNS DENGUE
DENGUE WITHOUT WARNING SIGNS

WARNING SIGNS
SEVERE DENGUE
FEVER OF 2-7 DAYS PLUS ANY OF THE FOLLOWING FEATURES :
1.EVIDENCE OF PLASMA LEAKAGE
2.SIGNIFICANT BLEEDING
3.ALTERED LEVEL OF CONSCIOUSNESS
4.SEVERE GI INVOLVEMENT
5.SEVERE ORGAN INVOLVEMENT

DENGUE SHOCK SYNDROME
COMPENSATED DECOMPENSATED
SHOCK SHOCK
(pulse pressure<20mmHg,
cold clammy extremities,
feeble rapid pulse)

DENGUE HAEMORRHAGIC FEVER

GRADING OF DENGUE FEVER

MANAGEMENT
• HISTORY – Time of fever onset,associated symptoms,warning signs,urine output,family or neighbourhood dengue
• PHYSICAL EXAMINATION – Assess hydration,hemodynamic status,tender abdomen,ascites,hepatomegaly,pleural efffusion,bleeding manifestations,mental state,tourniquet test

• INVESTIGATIONS – CBP with HCT,other organ function tests as indicated(USG,CXR,LFT,RFT,PT APTT INR,BLOOD GLUCOSE,SERUM ELECTROLYTES,ABG)
• SPECIFIC DIAGNOSTIC TESTS – NS1 Ag detection IgM IgG detection Viral isolation PCR to detect viral genome


DENGUE WITHOUT WARNING SIGNS - TREATMENT

DENGUE WITH WARNING SIGNS - TREATMENT

SEVERE DENGUE(COMPENSATED SHOCK) - TREATMENT


HYPOTENSIVE SHOCK - TREATMENT

DISCHARGE CRITERIA
• No fever for 48hours
• Improvement in general well-being,appetite,U/O,hemodynamic status
• Increasing platelet count
• Stable HCT without IVF

D/D
• CONDITIONS THAT MIMIC FEBRILE PHASE :
Influenza,
measles,
chikungunya,
scarlet fever,
meningococcal infection,
drug reactions,
G.E

• CONDITIONS THAT MIMIC CRITICAL PHASE :
Acute GE,
malaria,
viral hepatitis,
acute abdomen,
DKA,
lactic acidosis,
acute leukemia,
platelet disorders,
leptospirosis


THANK YOU !