Embed Size (px)
Citation preview
Dental sequalae of Pulpitis DC DC with
pulpitisDefensive reaction-Periapical Granuloma or Periapical cyst
Bone reaction-Osteomyelitis
Soft tissue reaction-Cellulitis
Blood reaction-Septicemia
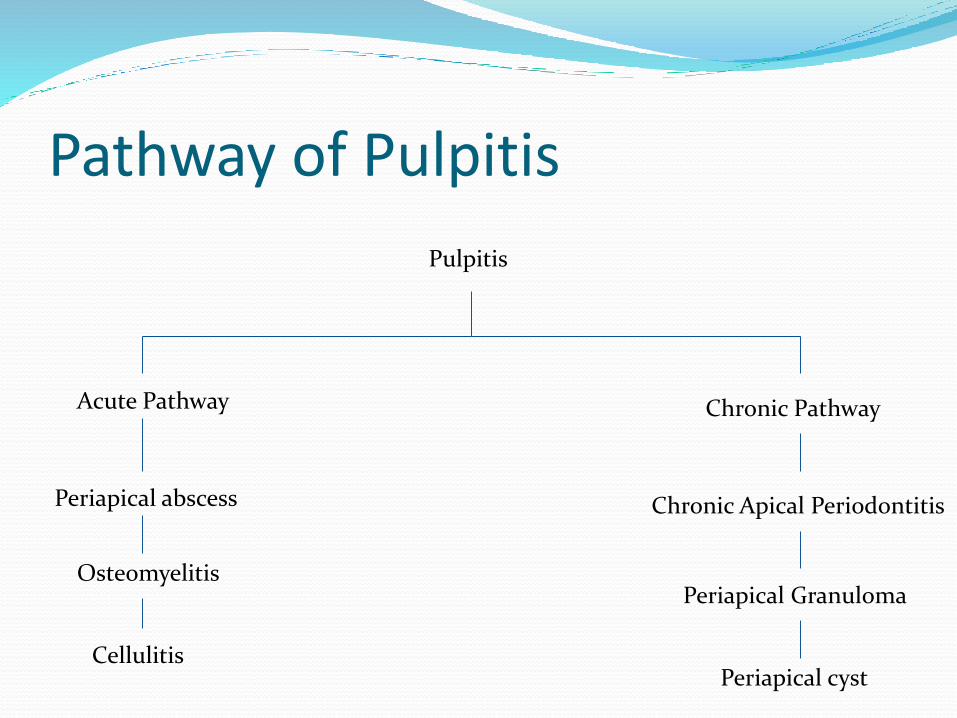
Pathway of Pulpitis
Pulpitis
Acute Pathway
Periapical abscess
Osteomyelitis
Cellulitis
Chronic Pathway
Chronic Apical Periodontitis
Periapical Granuloma
Periapical cyst
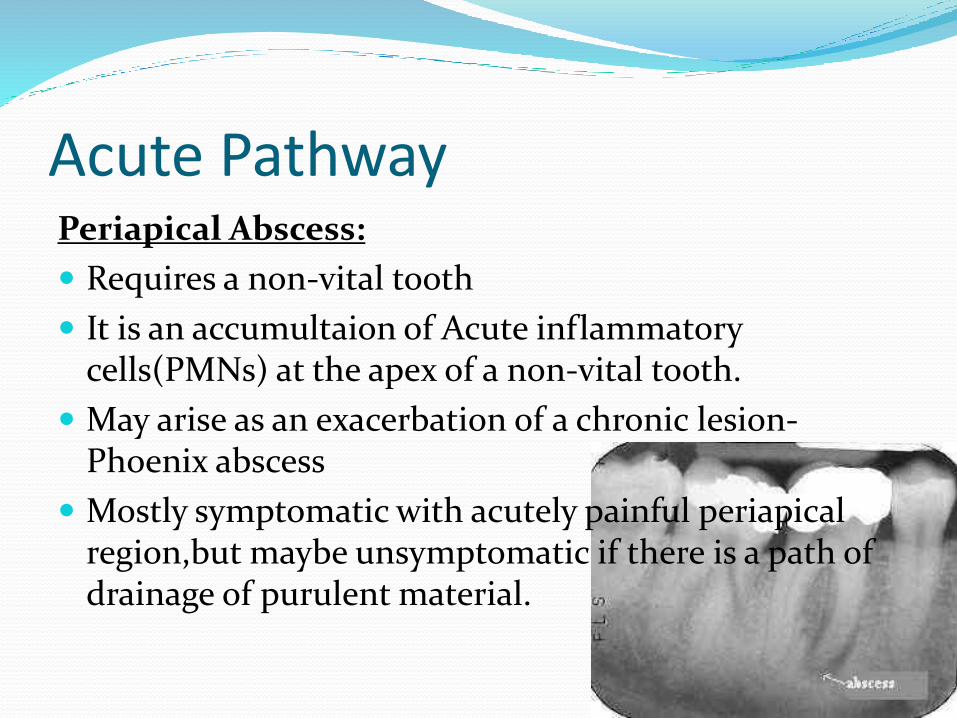
Acute PathwayPeriapical Abscess
Requires a non-vital tooth
It is an accumultaion of Acute inflammatory cells(PMNs) at the apex of a non-vital tooth
May arise as an exacerbation of a chronic lesion-Phoenix abscess
Mostly symptomatic with acutely painful periapicalregionbut maybe unsymptomatic if there is a path of drainage of purulent material
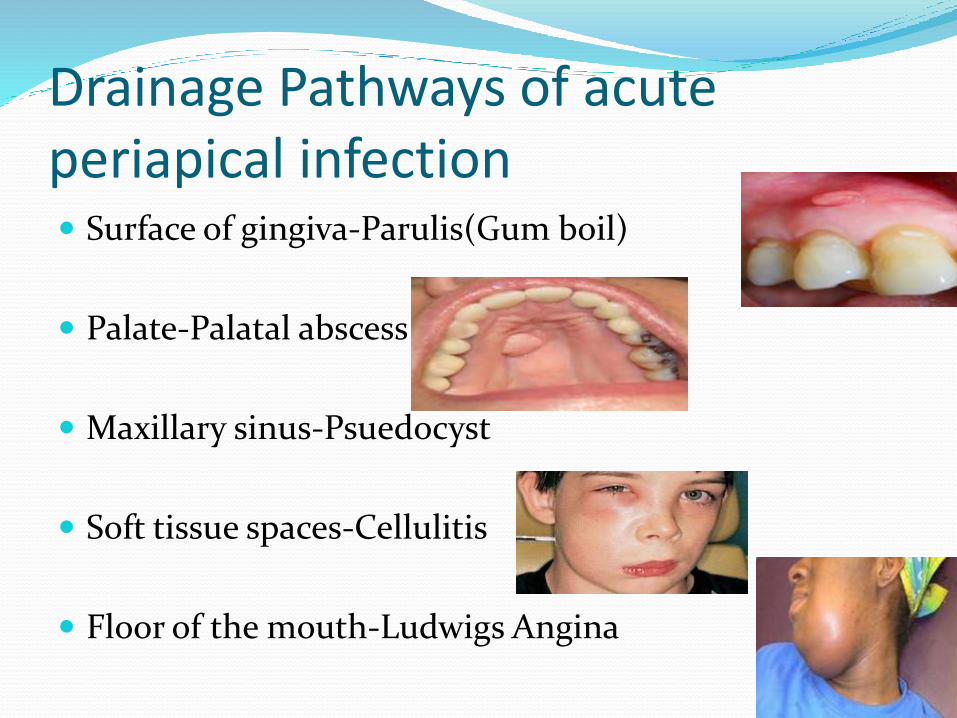
Drainage Pathways of acute periapical infection Surface of gingiva-Parulis(Gum boil)
Palate-Palatal abscess
Maxillary sinus-Psuedocyst
Soft tissue spaces-Cellulitis
Floor of the mouth-Ludwigs Angina
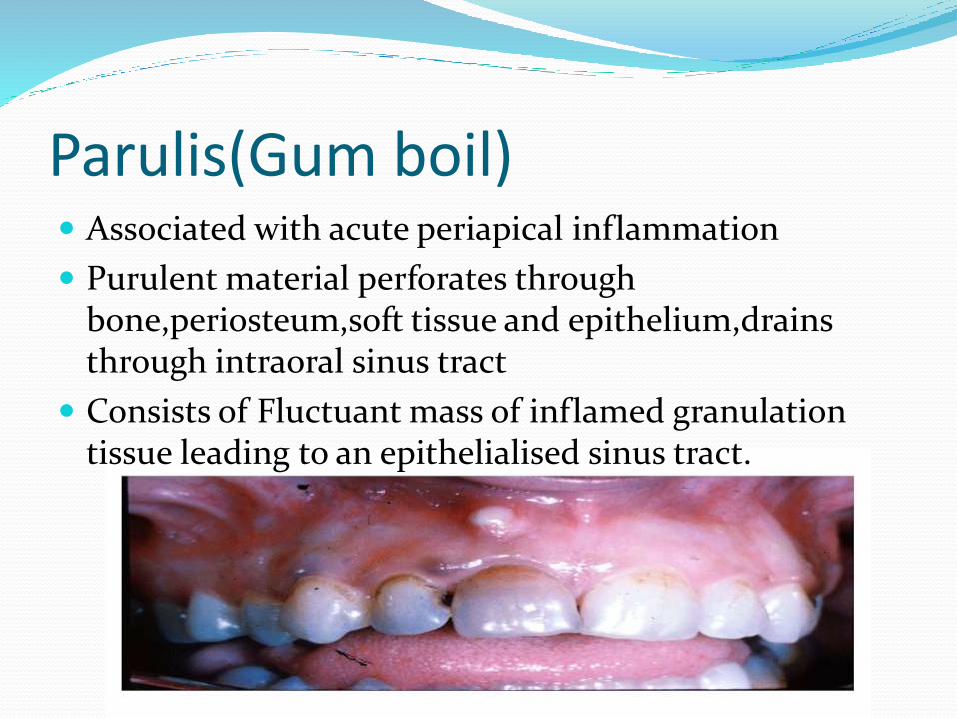
Parulis(Gum boil) Associated with acute periapical inflammation
Purulent material perforates through boneperiosteumsoft tissue and epitheliumdrainsthrough intraoral sinus tract
Consists of Fluctuant mass of inflamed granulation tissue leading to an epithelialised sinus tract
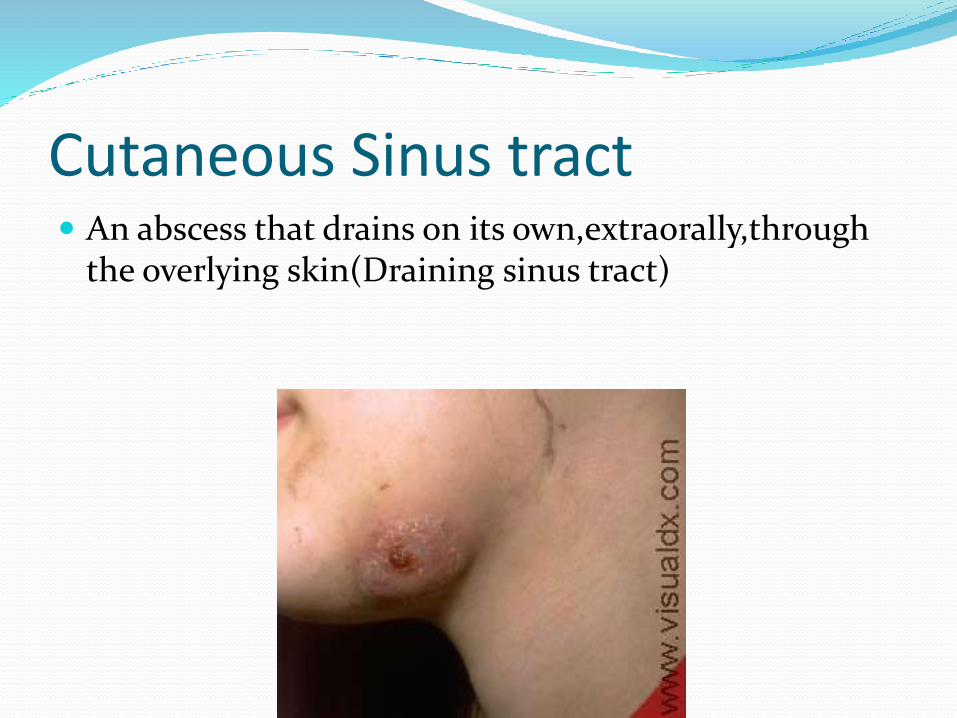
Cutaneous Sinus tract An abscess that drains on its ownextraorallythrough
the overlying skin(Draining sinus tract)
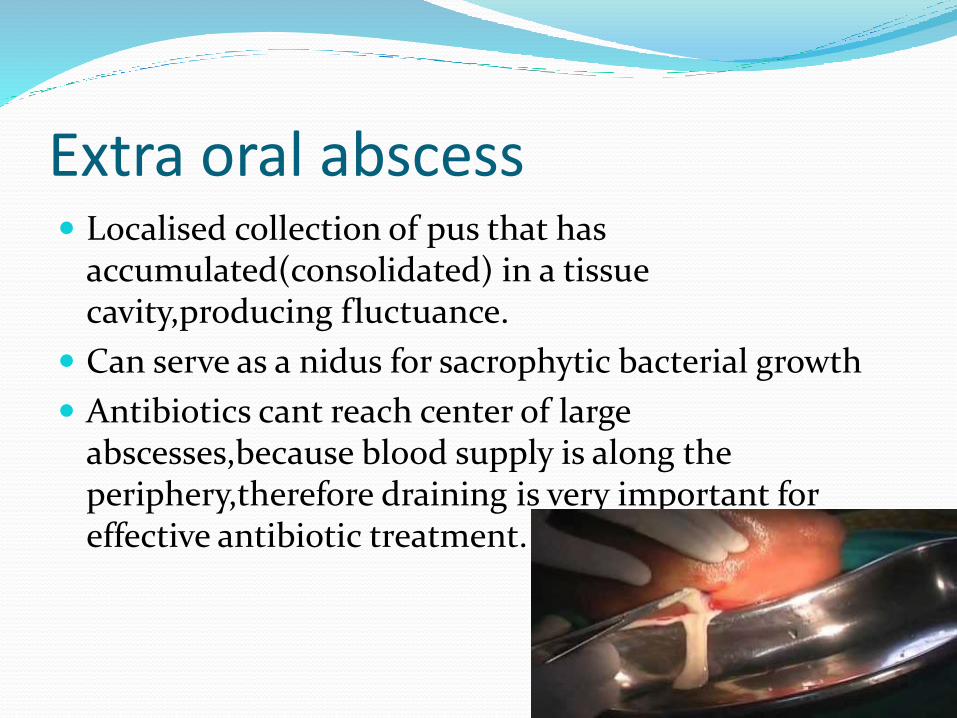
Extra oral abscess Localised collection of pus that has
accumulated(consolidated) in a tissue cavityproducing fluctuance
Can serve as a nidus for sacrophytic bacterial growth
Antibiotics cant reach center of large abscessesbecause blood supply is along the peripherytherefore draining is very important for effective antibiotic treatment
Cellulitis Diffuse spread of an acute inflammatory process
through the fascial planes of soft tissueproducingerythemaoedemawarmth and pain
It is a board-likediffusehard swelling
Trismus is a common secondary to cellulitis due to loss of function of muscles of mastication
Requires immediate antibiotics and drain placement
Ludwigs angina Aggressiverapidly spreading cellulitis involving
multiple anatomic spacessubmentalsublingualsubmandibular
Produces massive swelling of the neck that may extend close to the clavicles and cause airway obstruction(bullneck)
Causes elevation of the floor of the mouth and protrusion of tomgue(woody tongue)
Can be fatal due to airway obstructionmust establish an airwaydrain and give IV antibiotics
Cavernous sinus thrombosis Maybe associated with spread of infection from
maxillary teeth(classic canine space infection)
It is the formation of a blood clot within the cavernous sinus
Life threatening infection cause the cavernous sinus holds the pituitary gland and sella turcicaCranialnerves-346
Proliferative Periostitis Form of chronic osteomyelitis with proliferative
periostitis
Periosteal reaction in which layers of reactive vital bone are formedproducing cortical expansion(onion skinning) The periosteum is not destroyedbut lifted upwhen bone is formed beneath its layers
Chronic focal sclerosingosteomyelitis AKA Condensing osteitis Localised area of bone sclerosis associated with apices
of non-vital teeth
Most frequent in children and young adults involving mandibular molarspremolars
No cortical expansion
Differential diagnosisOsseous Dysplasia and idiopathic osseosclerosis
Osteomyelitis Bacterial infection of bone secondary to
A)Odontogenic infection
B)Traumatic injury
C)Necrotising Ulcerative GingivitisNoma or cancrumoris
Predisposition to decreased vascularity of bone-PagetrsquosOsteopetrosisflorid cemento-osseous dysplasia
Chronic PathwayPeriapical granuloma
It is a misnomerit is not a granulomatous reaction
Mass of chronically inflamed granulation tissue at apex of non-vital teethdesigned to wall off bacterial invasion at apex
Associated with chronic apical periodontitis
Periapical cyst AKA apical periodontal cystradicular cyst
Inflammatory odontogenic cystinduced by cell rests of malassez(Hertwigs Epithelial Root Sheath remnants) proliferation
Radiolucency at periapex of non-vital teeth
To differentiate from a granulomait must be tested histologically
Management of apical lesions Non-surgical management Periapical lesions develop as
sequelae to pulp disease They often occur without any episode of acute pain and are discovered on routine radiographic examination It is accepted that all inflammatory periapicallesions should be initially treated with conservative nonsurgical procedures
Methods1The conservative root canal treatment
2decompression technique3active nonsurgical decompression technique4aspiration-irrigation technique
5 method using calcium hydroxide6 Lesion Sterilization and Repair Therapy and7the Apexum procedure
Case selectionThe current philosophy in the management of periapical lesions includes the initial use of nonsurgical methods When this treatment approach is not successful a surgical approach may be adoptedThe following factors must be considered while deciding on the management approach
Diagnosis of the lesionMany bone destroying lesions closely resemble endodontically related periapicallesions on radiographs Some of these nonendodontic lesions include ameloblastoma central fibroma giant cell lesions fibrous dysplasia central hemangioma primary malignancies metastatic neoplasms and inflammatory bone diseases
Proximity of the periapical lesion to adjacent vital teethWhen in proximity to a vital toothadopting a surgical approach may result in injury to the blood vessels and nerves of the adjacent teeth thereby compromising their vitality
Encroachment on anatomical structuresSurgery increases the risk of damage to the anatomic structures such as mental foramen inferior alveolar nerve Also the aspirationndashirrigation technique a nonsurgical method is not recommended where adjacent tissue spaces or sinus cavities are involved
Patient cooperation
Considerable pain or discomfort can be experienced by the patient during or after a surgical procedure A nonsurgical approach would be recommended for apprehensive and uncooperative patients
Obstructions in the root canal system
Ledges calcified canals separated instruments may prevent access to the apical foramen and may warrant a surgical approach in managing periapical lesions related to such teeth
Time involved for treatment
Enhanced healing kinetics are observed after performing apical surgery in teeth with periapical lesions
Cases refractory to nonsurgical management methods
Inflammatory apical true cysts and the presence of cholesterol crystals have been suggested as possible causes that prevent healing of periapical lesionsSurgery is recommended for such cases
METHODS FOR NONSURGICAL MANAGMENT OF PERIAPICAL LESIONS Conservative root canal treatment without adjunctive therapy
Instrumentation should be carried 1 mm beyond the apical foramen when a periapical lesion is evident on a radiograph This may cause transitory inflammation and ulceration of the epithelial lining resulting in resolution of the cyst
Decompression technique
The decompression technique involves placement of a drain into the lesion regular irrigation periodic length adjustment and maintenance of the drain for various periods of time
Active nonsurgical decompression technique
This technique uses the Endo-eze vacuum system to create a negative pressure which results in the decompression of large periapical lesions The high-volume suction aspirator is connected to a micro 22-gauge needle which is inserted in the root canal and activated for 20 minutes creating a negative pressure which results in aspiration of the exudate When the drainage partially stops the access cavity is closed with temporary cement which helps in maintaining bacterial control
Aspiration and irrigation technique
Hoen et al suggested aspiration of the cystic fluid from the periapcial lesion using a buccal palatal approach In this technique an 18-gauge needle attached to a 20 ml syringe is used to penetrate the buccal mucosa and aspirate the cystic fluid A second syringe filled with saline is then used to rinse the bony lesion The new needle is inserted through the buccal wound and passed out through the palatal tissue creating a pathway for the escape of the irrigant
Aspiration through the root canal technique
In this technique aspiration of the cystic fluid is done through the root canal by passing the aspirating needle through the apical foramen This technique eliminates the creation of buccal and palatal wounds as in the traditional aspirationndashirrigation technique This minimizes the discomfort that the patient may experience
However it is advisable not to use either aspirationndashirrigation or aspiration through the root canal techniques where adjacent tissue spaces or sinus cavities are involved when there is no fluid aspiration from the lesion or in infected periapicallesions
Method using calcium hydroxide
Calcium hydroxide is a widely used material in endodontic treatment because of its bactericidal effectsIt is thought to create favorable conditions for periapical repair and stimulate hard tissue formationSouza et al suggested that the action of calcium hydroxide beyond the apex may be four-fold (a) anti-inflammatory activity (b) neutralization of acid products (c) activation of the alkaline phosphatase and (d) antibacterial action
Lesion sterilization and repair therapy
lsquoLesion Sterilization and Tissue Repair (LSTR)rsquo therapy that uses a triple antibiotic paste of ciprofloxacin metronidazole and minocycline for disinfection of oral infectious lesions including dentinal pulpal and periradicular lesions Repair of damaged tissues can be expected if lesions are disinfectedMetronidazole is the first choice because it has a wide antibacterial spectrum against anaerobesHowever some bacteria are resistant to metronidazole and hence ciprofloxacin and minocycline are added to the mix
Apexum procedure
Surgical removal of the periapical chronically inflamed tissue allows a fresh blood clot to form thereby converting a chronic inflammatory lesion into a new granulation tissue where healing might proceed much fasterThe Apexumprocedure uses two sequential rotary devices the Apexum NiTi Ablator and Apexum PGA Ablator (Apexum Ltd Or Yehuda Israel) designed to extend beyond the apex and mince the periapical tissues on rotation in a low-speed handpiece followed by washing out the minced tissue
Surgical management of Apical lesions Apical lesions maybe managed surgically to reduce
healing and recovery time
Indicated for emergency cases
Incision and drainagewith antibiotic therapy of the lesionfollowed by RCT with apisectomy is the usual modality of surgical treatment of apical lesions
Medical Management of apical lesions Antibiotic therapy is used to treat minor apical
lesionsin order to relieve the symptomsThis enables easier surgical or non0surgical management of the lesionThus medical management of apical lesions is used in conjunction with Surgical or non surgical management of apical lesions
Cellulitis-Cefazolin 1g iv Q8H7-10 days or cloxacillin500-1000mg po Q6H7-10 days
Acute osteomyelitis-Cefazolin 2g iv Q8H
Ludwigs angina-Clindamycin 600mg iv Q8H2-3 weeks
References J Conserv Dent 2010 Oct-Dec 13(4) 240-
245doi 1041030972070773384PMCID PMC3010029Nonsurgical management of periapical lesions Marina Fernandes and Ida de Ataide
Manual in maxillofacial surgery for senior house officers-Dental 2cmcvellore
DrVikram PerakathBDS
Pathway of Pulpitis
Pulpitis
Acute Pathway
Periapical abscess
Osteomyelitis
Cellulitis
Chronic Pathway
Chronic Apical Periodontitis
Periapical Granuloma
Periapical cyst
Acute PathwayPeriapical Abscess
Requires a non-vital tooth
It is an accumultaion of Acute inflammatory cells(PMNs) at the apex of a non-vital tooth
May arise as an exacerbation of a chronic lesion-Phoenix abscess
Mostly symptomatic with acutely painful periapicalregionbut maybe unsymptomatic if there is a path of drainage of purulent material
Drainage Pathways of acute periapical infection Surface of gingiva-Parulis(Gum boil)
Palate-Palatal abscess
Maxillary sinus-Psuedocyst
Soft tissue spaces-Cellulitis
Floor of the mouth-Ludwigs Angina
Parulis(Gum boil) Associated with acute periapical inflammation
Purulent material perforates through boneperiosteumsoft tissue and epitheliumdrainsthrough intraoral sinus tract
Consists of Fluctuant mass of inflamed granulation tissue leading to an epithelialised sinus tract
Cutaneous Sinus tract An abscess that drains on its ownextraorallythrough
the overlying skin(Draining sinus tract)
Extra oral abscess Localised collection of pus that has
accumulated(consolidated) in a tissue cavityproducing fluctuance
Can serve as a nidus for sacrophytic bacterial growth
Antibiotics cant reach center of large abscessesbecause blood supply is along the peripherytherefore draining is very important for effective antibiotic treatment
Cellulitis Diffuse spread of an acute inflammatory process
through the fascial planes of soft tissueproducingerythemaoedemawarmth and pain
It is a board-likediffusehard swelling
Trismus is a common secondary to cellulitis due to loss of function of muscles of mastication
Requires immediate antibiotics and drain placement
Ludwigs angina Aggressiverapidly spreading cellulitis involving
multiple anatomic spacessubmentalsublingualsubmandibular
Produces massive swelling of the neck that may extend close to the clavicles and cause airway obstruction(bullneck)
Causes elevation of the floor of the mouth and protrusion of tomgue(woody tongue)
Can be fatal due to airway obstructionmust establish an airwaydrain and give IV antibiotics
Cavernous sinus thrombosis Maybe associated with spread of infection from
maxillary teeth(classic canine space infection)
It is the formation of a blood clot within the cavernous sinus
Life threatening infection cause the cavernous sinus holds the pituitary gland and sella turcicaCranialnerves-346
Proliferative Periostitis Form of chronic osteomyelitis with proliferative
periostitis
Periosteal reaction in which layers of reactive vital bone are formedproducing cortical expansion(onion skinning) The periosteum is not destroyedbut lifted upwhen bone is formed beneath its layers
Chronic focal sclerosingosteomyelitis AKA Condensing osteitis Localised area of bone sclerosis associated with apices
of non-vital teeth
Most frequent in children and young adults involving mandibular molarspremolars
No cortical expansion
Differential diagnosisOsseous Dysplasia and idiopathic osseosclerosis
Osteomyelitis Bacterial infection of bone secondary to
A)Odontogenic infection
B)Traumatic injury
C)Necrotising Ulcerative GingivitisNoma or cancrumoris
Predisposition to decreased vascularity of bone-PagetrsquosOsteopetrosisflorid cemento-osseous dysplasia
Chronic PathwayPeriapical granuloma
It is a misnomerit is not a granulomatous reaction
Mass of chronically inflamed granulation tissue at apex of non-vital teethdesigned to wall off bacterial invasion at apex
Associated with chronic apical periodontitis
Periapical cyst AKA apical periodontal cystradicular cyst
Inflammatory odontogenic cystinduced by cell rests of malassez(Hertwigs Epithelial Root Sheath remnants) proliferation
Radiolucency at periapex of non-vital teeth
To differentiate from a granulomait must be tested histologically
Management of apical lesions Non-surgical management Periapical lesions develop as
sequelae to pulp disease They often occur without any episode of acute pain and are discovered on routine radiographic examination It is accepted that all inflammatory periapicallesions should be initially treated with conservative nonsurgical procedures
Methods1The conservative root canal treatment
2decompression technique3active nonsurgical decompression technique4aspiration-irrigation technique
5 method using calcium hydroxide6 Lesion Sterilization and Repair Therapy and7the Apexum procedure
Case selectionThe current philosophy in the management of periapical lesions includes the initial use of nonsurgical methods When this treatment approach is not successful a surgical approach may be adoptedThe following factors must be considered while deciding on the management approach
Diagnosis of the lesionMany bone destroying lesions closely resemble endodontically related periapicallesions on radiographs Some of these nonendodontic lesions include ameloblastoma central fibroma giant cell lesions fibrous dysplasia central hemangioma primary malignancies metastatic neoplasms and inflammatory bone diseases
Proximity of the periapical lesion to adjacent vital teethWhen in proximity to a vital toothadopting a surgical approach may result in injury to the blood vessels and nerves of the adjacent teeth thereby compromising their vitality
Encroachment on anatomical structuresSurgery increases the risk of damage to the anatomic structures such as mental foramen inferior alveolar nerve Also the aspirationndashirrigation technique a nonsurgical method is not recommended where adjacent tissue spaces or sinus cavities are involved
Patient cooperation
Considerable pain or discomfort can be experienced by the patient during or after a surgical procedure A nonsurgical approach would be recommended for apprehensive and uncooperative patients
Obstructions in the root canal system
Ledges calcified canals separated instruments may prevent access to the apical foramen and may warrant a surgical approach in managing periapical lesions related to such teeth
Time involved for treatment
Enhanced healing kinetics are observed after performing apical surgery in teeth with periapical lesions
Cases refractory to nonsurgical management methods
Inflammatory apical true cysts and the presence of cholesterol crystals have been suggested as possible causes that prevent healing of periapical lesionsSurgery is recommended for such cases
METHODS FOR NONSURGICAL MANAGMENT OF PERIAPICAL LESIONS Conservative root canal treatment without adjunctive therapy
Instrumentation should be carried 1 mm beyond the apical foramen when a periapical lesion is evident on a radiograph This may cause transitory inflammation and ulceration of the epithelial lining resulting in resolution of the cyst
Decompression technique
The decompression technique involves placement of a drain into the lesion regular irrigation periodic length adjustment and maintenance of the drain for various periods of time
Active nonsurgical decompression technique
This technique uses the Endo-eze vacuum system to create a negative pressure which results in the decompression of large periapical lesions The high-volume suction aspirator is connected to a micro 22-gauge needle which is inserted in the root canal and activated for 20 minutes creating a negative pressure which results in aspiration of the exudate When the drainage partially stops the access cavity is closed with temporary cement which helps in maintaining bacterial control
Aspiration and irrigation technique
Hoen et al suggested aspiration of the cystic fluid from the periapcial lesion using a buccal palatal approach In this technique an 18-gauge needle attached to a 20 ml syringe is used to penetrate the buccal mucosa and aspirate the cystic fluid A second syringe filled with saline is then used to rinse the bony lesion The new needle is inserted through the buccal wound and passed out through the palatal tissue creating a pathway for the escape of the irrigant
Aspiration through the root canal technique
In this technique aspiration of the cystic fluid is done through the root canal by passing the aspirating needle through the apical foramen This technique eliminates the creation of buccal and palatal wounds as in the traditional aspirationndashirrigation technique This minimizes the discomfort that the patient may experience
However it is advisable not to use either aspirationndashirrigation or aspiration through the root canal techniques where adjacent tissue spaces or sinus cavities are involved when there is no fluid aspiration from the lesion or in infected periapicallesions
Method using calcium hydroxide
Calcium hydroxide is a widely used material in endodontic treatment because of its bactericidal effectsIt is thought to create favorable conditions for periapical repair and stimulate hard tissue formationSouza et al suggested that the action of calcium hydroxide beyond the apex may be four-fold (a) anti-inflammatory activity (b) neutralization of acid products (c) activation of the alkaline phosphatase and (d) antibacterial action
Lesion sterilization and repair therapy
lsquoLesion Sterilization and Tissue Repair (LSTR)rsquo therapy that uses a triple antibiotic paste of ciprofloxacin metronidazole and minocycline for disinfection of oral infectious lesions including dentinal pulpal and periradicular lesions Repair of damaged tissues can be expected if lesions are disinfectedMetronidazole is the first choice because it has a wide antibacterial spectrum against anaerobesHowever some bacteria are resistant to metronidazole and hence ciprofloxacin and minocycline are added to the mix
Apexum procedure
Surgical removal of the periapical chronically inflamed tissue allows a fresh blood clot to form thereby converting a chronic inflammatory lesion into a new granulation tissue where healing might proceed much fasterThe Apexumprocedure uses two sequential rotary devices the Apexum NiTi Ablator and Apexum PGA Ablator (Apexum Ltd Or Yehuda Israel) designed to extend beyond the apex and mince the periapical tissues on rotation in a low-speed handpiece followed by washing out the minced tissue
Surgical management of Apical lesions Apical lesions maybe managed surgically to reduce
healing and recovery time
Indicated for emergency cases
Incision and drainagewith antibiotic therapy of the lesionfollowed by RCT with apisectomy is the usual modality of surgical treatment of apical lesions
Medical Management of apical lesions Antibiotic therapy is used to treat minor apical
lesionsin order to relieve the symptomsThis enables easier surgical or non0surgical management of the lesionThus medical management of apical lesions is used in conjunction with Surgical or non surgical management of apical lesions
Cellulitis-Cefazolin 1g iv Q8H7-10 days or cloxacillin500-1000mg po Q6H7-10 days
Acute osteomyelitis-Cefazolin 2g iv Q8H
Ludwigs angina-Clindamycin 600mg iv Q8H2-3 weeks
References J Conserv Dent 2010 Oct-Dec 13(4) 240-
245doi 1041030972070773384PMCID PMC3010029Nonsurgical management of periapical lesions Marina Fernandes and Ida de Ataide
Manual in maxillofacial surgery for senior house officers-Dental 2cmcvellore
DrVikram PerakathBDS
Acute PathwayPeriapical Abscess
Requires a non-vital tooth
It is an accumultaion of Acute inflammatory cells(PMNs) at the apex of a non-vital tooth
May arise as an exacerbation of a chronic lesion-Phoenix abscess
Mostly symptomatic with acutely painful periapicalregionbut maybe unsymptomatic if there is a path of drainage of purulent material
Drainage Pathways of acute periapical infection Surface of gingiva-Parulis(Gum boil)
Palate-Palatal abscess
Maxillary sinus-Psuedocyst
Soft tissue spaces-Cellulitis
Floor of the mouth-Ludwigs Angina
Parulis(Gum boil) Associated with acute periapical inflammation
Purulent material perforates through boneperiosteumsoft tissue and epitheliumdrainsthrough intraoral sinus tract
Consists of Fluctuant mass of inflamed granulation tissue leading to an epithelialised sinus tract
Cutaneous Sinus tract An abscess that drains on its ownextraorallythrough
the overlying skin(Draining sinus tract)
Extra oral abscess Localised collection of pus that has
accumulated(consolidated) in a tissue cavityproducing fluctuance
Can serve as a nidus for sacrophytic bacterial growth
Antibiotics cant reach center of large abscessesbecause blood supply is along the peripherytherefore draining is very important for effective antibiotic treatment
Cellulitis Diffuse spread of an acute inflammatory process
through the fascial planes of soft tissueproducingerythemaoedemawarmth and pain
It is a board-likediffusehard swelling
Trismus is a common secondary to cellulitis due to loss of function of muscles of mastication
Requires immediate antibiotics and drain placement
Ludwigs angina Aggressiverapidly spreading cellulitis involving
multiple anatomic spacessubmentalsublingualsubmandibular
Produces massive swelling of the neck that may extend close to the clavicles and cause airway obstruction(bullneck)
Causes elevation of the floor of the mouth and protrusion of tomgue(woody tongue)
Can be fatal due to airway obstructionmust establish an airwaydrain and give IV antibiotics
Cavernous sinus thrombosis Maybe associated with spread of infection from
maxillary teeth(classic canine space infection)
It is the formation of a blood clot within the cavernous sinus
Life threatening infection cause the cavernous sinus holds the pituitary gland and sella turcicaCranialnerves-346
Proliferative Periostitis Form of chronic osteomyelitis with proliferative
periostitis
Periosteal reaction in which layers of reactive vital bone are formedproducing cortical expansion(onion skinning) The periosteum is not destroyedbut lifted upwhen bone is formed beneath its layers
Chronic focal sclerosingosteomyelitis AKA Condensing osteitis Localised area of bone sclerosis associated with apices
of non-vital teeth
Most frequent in children and young adults involving mandibular molarspremolars
No cortical expansion
Differential diagnosisOsseous Dysplasia and idiopathic osseosclerosis
Osteomyelitis Bacterial infection of bone secondary to
A)Odontogenic infection
B)Traumatic injury
C)Necrotising Ulcerative GingivitisNoma or cancrumoris
Predisposition to decreased vascularity of bone-PagetrsquosOsteopetrosisflorid cemento-osseous dysplasia
Chronic PathwayPeriapical granuloma
It is a misnomerit is not a granulomatous reaction
Mass of chronically inflamed granulation tissue at apex of non-vital teethdesigned to wall off bacterial invasion at apex
Associated with chronic apical periodontitis
Periapical cyst AKA apical periodontal cystradicular cyst
Inflammatory odontogenic cystinduced by cell rests of malassez(Hertwigs Epithelial Root Sheath remnants) proliferation
Radiolucency at periapex of non-vital teeth
To differentiate from a granulomait must be tested histologically
Management of apical lesions Non-surgical management Periapical lesions develop as
sequelae to pulp disease They often occur without any episode of acute pain and are discovered on routine radiographic examination It is accepted that all inflammatory periapicallesions should be initially treated with conservative nonsurgical procedures
Methods1The conservative root canal treatment
2decompression technique3active nonsurgical decompression technique4aspiration-irrigation technique
5 method using calcium hydroxide6 Lesion Sterilization and Repair Therapy and7the Apexum procedure
Case selectionThe current philosophy in the management of periapical lesions includes the initial use of nonsurgical methods When this treatment approach is not successful a surgical approach may be adoptedThe following factors must be considered while deciding on the management approach
Diagnosis of the lesionMany bone destroying lesions closely resemble endodontically related periapicallesions on radiographs Some of these nonendodontic lesions include ameloblastoma central fibroma giant cell lesions fibrous dysplasia central hemangioma primary malignancies metastatic neoplasms and inflammatory bone diseases
Proximity of the periapical lesion to adjacent vital teethWhen in proximity to a vital toothadopting a surgical approach may result in injury to the blood vessels and nerves of the adjacent teeth thereby compromising their vitality
Encroachment on anatomical structuresSurgery increases the risk of damage to the anatomic structures such as mental foramen inferior alveolar nerve Also the aspirationndashirrigation technique a nonsurgical method is not recommended where adjacent tissue spaces or sinus cavities are involved
Patient cooperation
Considerable pain or discomfort can be experienced by the patient during or after a surgical procedure A nonsurgical approach would be recommended for apprehensive and uncooperative patients
Obstructions in the root canal system
Ledges calcified canals separated instruments may prevent access to the apical foramen and may warrant a surgical approach in managing periapical lesions related to such teeth
Time involved for treatment
Enhanced healing kinetics are observed after performing apical surgery in teeth with periapical lesions
Cases refractory to nonsurgical management methods
Inflammatory apical true cysts and the presence of cholesterol crystals have been suggested as possible causes that prevent healing of periapical lesionsSurgery is recommended for such cases
METHODS FOR NONSURGICAL MANAGMENT OF PERIAPICAL LESIONS Conservative root canal treatment without adjunctive therapy
Instrumentation should be carried 1 mm beyond the apical foramen when a periapical lesion is evident on a radiograph This may cause transitory inflammation and ulceration of the epithelial lining resulting in resolution of the cyst
Decompression technique
The decompression technique involves placement of a drain into the lesion regular irrigation periodic length adjustment and maintenance of the drain for various periods of time
Active nonsurgical decompression technique
This technique uses the Endo-eze vacuum system to create a negative pressure which results in the decompression of large periapical lesions The high-volume suction aspirator is connected to a micro 22-gauge needle which is inserted in the root canal and activated for 20 minutes creating a negative pressure which results in aspiration of the exudate When the drainage partially stops the access cavity is closed with temporary cement which helps in maintaining bacterial control
Aspiration and irrigation technique
Hoen et al suggested aspiration of the cystic fluid from the periapcial lesion using a buccal palatal approach In this technique an 18-gauge needle attached to a 20 ml syringe is used to penetrate the buccal mucosa and aspirate the cystic fluid A second syringe filled with saline is then used to rinse the bony lesion The new needle is inserted through the buccal wound and passed out through the palatal tissue creating a pathway for the escape of the irrigant
Aspiration through the root canal technique
In this technique aspiration of the cystic fluid is done through the root canal by passing the aspirating needle through the apical foramen This technique eliminates the creation of buccal and palatal wounds as in the traditional aspirationndashirrigation technique This minimizes the discomfort that the patient may experience
However it is advisable not to use either aspirationndashirrigation or aspiration through the root canal techniques where adjacent tissue spaces or sinus cavities are involved when there is no fluid aspiration from the lesion or in infected periapicallesions
Method using calcium hydroxide
Calcium hydroxide is a widely used material in endodontic treatment because of its bactericidal effectsIt is thought to create favorable conditions for periapical repair and stimulate hard tissue formationSouza et al suggested that the action of calcium hydroxide beyond the apex may be four-fold (a) anti-inflammatory activity (b) neutralization of acid products (c) activation of the alkaline phosphatase and (d) antibacterial action
Lesion sterilization and repair therapy
lsquoLesion Sterilization and Tissue Repair (LSTR)rsquo therapy that uses a triple antibiotic paste of ciprofloxacin metronidazole and minocycline for disinfection of oral infectious lesions including dentinal pulpal and periradicular lesions Repair of damaged tissues can be expected if lesions are disinfectedMetronidazole is the first choice because it has a wide antibacterial spectrum against anaerobesHowever some bacteria are resistant to metronidazole and hence ciprofloxacin and minocycline are added to the mix
Apexum procedure
Surgical removal of the periapical chronically inflamed tissue allows a fresh blood clot to form thereby converting a chronic inflammatory lesion into a new granulation tissue where healing might proceed much fasterThe Apexumprocedure uses two sequential rotary devices the Apexum NiTi Ablator and Apexum PGA Ablator (Apexum Ltd Or Yehuda Israel) designed to extend beyond the apex and mince the periapical tissues on rotation in a low-speed handpiece followed by washing out the minced tissue
Surgical management of Apical lesions Apical lesions maybe managed surgically to reduce
healing and recovery time
Indicated for emergency cases
Incision and drainagewith antibiotic therapy of the lesionfollowed by RCT with apisectomy is the usual modality of surgical treatment of apical lesions
Medical Management of apical lesions Antibiotic therapy is used to treat minor apical
lesionsin order to relieve the symptomsThis enables easier surgical or non0surgical management of the lesionThus medical management of apical lesions is used in conjunction with Surgical or non surgical management of apical lesions
Cellulitis-Cefazolin 1g iv Q8H7-10 days or cloxacillin500-1000mg po Q6H7-10 days
Acute osteomyelitis-Cefazolin 2g iv Q8H
Ludwigs angina-Clindamycin 600mg iv Q8H2-3 weeks
References J Conserv Dent 2010 Oct-Dec 13(4) 240-
245doi 1041030972070773384PMCID PMC3010029Nonsurgical management of periapical lesions Marina Fernandes and Ida de Ataide
Manual in maxillofacial surgery for senior house officers-Dental 2cmcvellore
DrVikram PerakathBDS
Drainage Pathways of acute periapical infection Surface of gingiva-Parulis(Gum boil)
Palate-Palatal abscess
Maxillary sinus-Psuedocyst
Soft tissue spaces-Cellulitis
Floor of the mouth-Ludwigs Angina
Parulis(Gum boil) Associated with acute periapical inflammation
Purulent material perforates through boneperiosteumsoft tissue and epitheliumdrainsthrough intraoral sinus tract
Consists of Fluctuant mass of inflamed granulation tissue leading to an epithelialised sinus tract
Cutaneous Sinus tract An abscess that drains on its ownextraorallythrough
the overlying skin(Draining sinus tract)
Extra oral abscess Localised collection of pus that has
accumulated(consolidated) in a tissue cavityproducing fluctuance
Can serve as a nidus for sacrophytic bacterial growth
Antibiotics cant reach center of large abscessesbecause blood supply is along the peripherytherefore draining is very important for effective antibiotic treatment
Cellulitis Diffuse spread of an acute inflammatory process
through the fascial planes of soft tissueproducingerythemaoedemawarmth and pain
It is a board-likediffusehard swelling
Trismus is a common secondary to cellulitis due to loss of function of muscles of mastication
Requires immediate antibiotics and drain placement
Ludwigs angina Aggressiverapidly spreading cellulitis involving
multiple anatomic spacessubmentalsublingualsubmandibular
Produces massive swelling of the neck that may extend close to the clavicles and cause airway obstruction(bullneck)
Causes elevation of the floor of the mouth and protrusion of tomgue(woody tongue)
Can be fatal due to airway obstructionmust establish an airwaydrain and give IV antibiotics
Cavernous sinus thrombosis Maybe associated with spread of infection from
maxillary teeth(classic canine space infection)
It is the formation of a blood clot within the cavernous sinus
Life threatening infection cause the cavernous sinus holds the pituitary gland and sella turcicaCranialnerves-346
Proliferative Periostitis Form of chronic osteomyelitis with proliferative
periostitis
Periosteal reaction in which layers of reactive vital bone are formedproducing cortical expansion(onion skinning) The periosteum is not destroyedbut lifted upwhen bone is formed beneath its layers
Chronic focal sclerosingosteomyelitis AKA Condensing osteitis Localised area of bone sclerosis associated with apices
of non-vital teeth
Most frequent in children and young adults involving mandibular molarspremolars
No cortical expansion
Differential diagnosisOsseous Dysplasia and idiopathic osseosclerosis
Osteomyelitis Bacterial infection of bone secondary to
A)Odontogenic infection
B)Traumatic injury
C)Necrotising Ulcerative GingivitisNoma or cancrumoris
Predisposition to decreased vascularity of bone-PagetrsquosOsteopetrosisflorid cemento-osseous dysplasia
Chronic PathwayPeriapical granuloma
It is a misnomerit is not a granulomatous reaction
Mass of chronically inflamed granulation tissue at apex of non-vital teethdesigned to wall off bacterial invasion at apex
Associated with chronic apical periodontitis
Periapical cyst AKA apical periodontal cystradicular cyst
Inflammatory odontogenic cystinduced by cell rests of malassez(Hertwigs Epithelial Root Sheath remnants) proliferation
Radiolucency at periapex of non-vital teeth
To differentiate from a granulomait must be tested histologically
Management of apical lesions Non-surgical management Periapical lesions develop as
sequelae to pulp disease They often occur without any episode of acute pain and are discovered on routine radiographic examination It is accepted that all inflammatory periapicallesions should be initially treated with conservative nonsurgical procedures
Methods1The conservative root canal treatment
2decompression technique3active nonsurgical decompression technique4aspiration-irrigation technique
5 method using calcium hydroxide6 Lesion Sterilization and Repair Therapy and7the Apexum procedure
Case selectionThe current philosophy in the management of periapical lesions includes the initial use of nonsurgical methods When this treatment approach is not successful a surgical approach may be adoptedThe following factors must be considered while deciding on the management approach
Diagnosis of the lesionMany bone destroying lesions closely resemble endodontically related periapicallesions on radiographs Some of these nonendodontic lesions include ameloblastoma central fibroma giant cell lesions fibrous dysplasia central hemangioma primary malignancies metastatic neoplasms and inflammatory bone diseases
Proximity of the periapical lesion to adjacent vital teethWhen in proximity to a vital toothadopting a surgical approach may result in injury to the blood vessels and nerves of the adjacent teeth thereby compromising their vitality
Encroachment on anatomical structuresSurgery increases the risk of damage to the anatomic structures such as mental foramen inferior alveolar nerve Also the aspirationndashirrigation technique a nonsurgical method is not recommended where adjacent tissue spaces or sinus cavities are involved
Patient cooperation
Considerable pain or discomfort can be experienced by the patient during or after a surgical procedure A nonsurgical approach would be recommended for apprehensive and uncooperative patients
Obstructions in the root canal system
Ledges calcified canals separated instruments may prevent access to the apical foramen and may warrant a surgical approach in managing periapical lesions related to such teeth
Time involved for treatment
Enhanced healing kinetics are observed after performing apical surgery in teeth with periapical lesions
Cases refractory to nonsurgical management methods
Inflammatory apical true cysts and the presence of cholesterol crystals have been suggested as possible causes that prevent healing of periapical lesionsSurgery is recommended for such cases
METHODS FOR NONSURGICAL MANAGMENT OF PERIAPICAL LESIONS Conservative root canal treatment without adjunctive therapy
Instrumentation should be carried 1 mm beyond the apical foramen when a periapical lesion is evident on a radiograph This may cause transitory inflammation and ulceration of the epithelial lining resulting in resolution of the cyst
Decompression technique
The decompression technique involves placement of a drain into the lesion regular irrigation periodic length adjustment and maintenance of the drain for various periods of time
Active nonsurgical decompression technique
This technique uses the Endo-eze vacuum system to create a negative pressure which results in the decompression of large periapical lesions The high-volume suction aspirator is connected to a micro 22-gauge needle which is inserted in the root canal and activated for 20 minutes creating a negative pressure which results in aspiration of the exudate When the drainage partially stops the access cavity is closed with temporary cement which helps in maintaining bacterial control
Aspiration and irrigation technique
Hoen et al suggested aspiration of the cystic fluid from the periapcial lesion using a buccal palatal approach In this technique an 18-gauge needle attached to a 20 ml syringe is used to penetrate the buccal mucosa and aspirate the cystic fluid A second syringe filled with saline is then used to rinse the bony lesion The new needle is inserted through the buccal wound and passed out through the palatal tissue creating a pathway for the escape of the irrigant
Aspiration through the root canal technique
In this technique aspiration of the cystic fluid is done through the root canal by passing the aspirating needle through the apical foramen This technique eliminates the creation of buccal and palatal wounds as in the traditional aspirationndashirrigation technique This minimizes the discomfort that the patient may experience
However it is advisable not to use either aspirationndashirrigation or aspiration through the root canal techniques where adjacent tissue spaces or sinus cavities are involved when there is no fluid aspiration from the lesion or in infected periapicallesions
Method using calcium hydroxide
Calcium hydroxide is a widely used material in endodontic treatment because of its bactericidal effectsIt is thought to create favorable conditions for periapical repair and stimulate hard tissue formationSouza et al suggested that the action of calcium hydroxide beyond the apex may be four-fold (a) anti-inflammatory activity (b) neutralization of acid products (c) activation of the alkaline phosphatase and (d) antibacterial action
Lesion sterilization and repair therapy
lsquoLesion Sterilization and Tissue Repair (LSTR)rsquo therapy that uses a triple antibiotic paste of ciprofloxacin metronidazole and minocycline for disinfection of oral infectious lesions including dentinal pulpal and periradicular lesions Repair of damaged tissues can be expected if lesions are disinfectedMetronidazole is the first choice because it has a wide antibacterial spectrum against anaerobesHowever some bacteria are resistant to metronidazole and hence ciprofloxacin and minocycline are added to the mix
Apexum procedure
Surgical removal of the periapical chronically inflamed tissue allows a fresh blood clot to form thereby converting a chronic inflammatory lesion into a new granulation tissue where healing might proceed much fasterThe Apexumprocedure uses two sequential rotary devices the Apexum NiTi Ablator and Apexum PGA Ablator (Apexum Ltd Or Yehuda Israel) designed to extend beyond the apex and mince the periapical tissues on rotation in a low-speed handpiece followed by washing out the minced tissue
Surgical management of Apical lesions Apical lesions maybe managed surgically to reduce
healing and recovery time
Indicated for emergency cases
Incision and drainagewith antibiotic therapy of the lesionfollowed by RCT with apisectomy is the usual modality of surgical treatment of apical lesions
Medical Management of apical lesions Antibiotic therapy is used to treat minor apical
lesionsin order to relieve the symptomsThis enables easier surgical or non0surgical management of the lesionThus medical management of apical lesions is used in conjunction with Surgical or non surgical management of apical lesions
Cellulitis-Cefazolin 1g iv Q8H7-10 days or cloxacillin500-1000mg po Q6H7-10 days
Acute osteomyelitis-Cefazolin 2g iv Q8H
Ludwigs angina-Clindamycin 600mg iv Q8H2-3 weeks
References J Conserv Dent 2010 Oct-Dec 13(4) 240-
245doi 1041030972070773384PMCID PMC3010029Nonsurgical management of periapical lesions Marina Fernandes and Ida de Ataide
Manual in maxillofacial surgery for senior house officers-Dental 2cmcvellore
DrVikram PerakathBDS
Parulis(Gum boil) Associated with acute periapical inflammation
Purulent material perforates through boneperiosteumsoft tissue and epitheliumdrainsthrough intraoral sinus tract
Consists of Fluctuant mass of inflamed granulation tissue leading to an epithelialised sinus tract
Cutaneous Sinus tract An abscess that drains on its ownextraorallythrough
the overlying skin(Draining sinus tract)
Extra oral abscess Localised collection of pus that has
accumulated(consolidated) in a tissue cavityproducing fluctuance
Can serve as a nidus for sacrophytic bacterial growth
Antibiotics cant reach center of large abscessesbecause blood supply is along the peripherytherefore draining is very important for effective antibiotic treatment
Cellulitis Diffuse spread of an acute inflammatory process
through the fascial planes of soft tissueproducingerythemaoedemawarmth and pain
It is a board-likediffusehard swelling
Trismus is a common secondary to cellulitis due to loss of function of muscles of mastication
Requires immediate antibiotics and drain placement
Ludwigs angina Aggressiverapidly spreading cellulitis involving
multiple anatomic spacessubmentalsublingualsubmandibular
Produces massive swelling of the neck that may extend close to the clavicles and cause airway obstruction(bullneck)
Causes elevation of the floor of the mouth and protrusion of tomgue(woody tongue)
Can be fatal due to airway obstructionmust establish an airwaydrain and give IV antibiotics
Cavernous sinus thrombosis Maybe associated with spread of infection from
maxillary teeth(classic canine space infection)
It is the formation of a blood clot within the cavernous sinus
Life threatening infection cause the cavernous sinus holds the pituitary gland and sella turcicaCranialnerves-346
Proliferative Periostitis Form of chronic osteomyelitis with proliferative
periostitis
Periosteal reaction in which layers of reactive vital bone are formedproducing cortical expansion(onion skinning) The periosteum is not destroyedbut lifted upwhen bone is formed beneath its layers
Chronic focal sclerosingosteomyelitis AKA Condensing osteitis Localised area of bone sclerosis associated with apices
of non-vital teeth
Most frequent in children and young adults involving mandibular molarspremolars
No cortical expansion
Differential diagnosisOsseous Dysplasia and idiopathic osseosclerosis
Osteomyelitis Bacterial infection of bone secondary to
A)Odontogenic infection
B)Traumatic injury
C)Necrotising Ulcerative GingivitisNoma or cancrumoris
Predisposition to decreased vascularity of bone-PagetrsquosOsteopetrosisflorid cemento-osseous dysplasia
Chronic PathwayPeriapical granuloma
It is a misnomerit is not a granulomatous reaction
Mass of chronically inflamed granulation tissue at apex of non-vital teethdesigned to wall off bacterial invasion at apex
Associated with chronic apical periodontitis
Periapical cyst AKA apical periodontal cystradicular cyst
Inflammatory odontogenic cystinduced by cell rests of malassez(Hertwigs Epithelial Root Sheath remnants) proliferation
Radiolucency at periapex of non-vital teeth
To differentiate from a granulomait must be tested histologically
Management of apical lesions Non-surgical management Periapical lesions develop as
sequelae to pulp disease They often occur without any episode of acute pain and are discovered on routine radiographic examination It is accepted that all inflammatory periapicallesions should be initially treated with conservative nonsurgical procedures
Methods1The conservative root canal treatment
2decompression technique3active nonsurgical decompression technique4aspiration-irrigation technique
5 method using calcium hydroxide6 Lesion Sterilization and Repair Therapy and7the Apexum procedure
Case selectionThe current philosophy in the management of periapical lesions includes the initial use of nonsurgical methods When this treatment approach is not successful a surgical approach may be adoptedThe following factors must be considered while deciding on the management approach
Diagnosis of the lesionMany bone destroying lesions closely resemble endodontically related periapicallesions on radiographs Some of these nonendodontic lesions include ameloblastoma central fibroma giant cell lesions fibrous dysplasia central hemangioma primary malignancies metastatic neoplasms and inflammatory bone diseases
Proximity of the periapical lesion to adjacent vital teethWhen in proximity to a vital toothadopting a surgical approach may result in injury to the blood vessels and nerves of the adjacent teeth thereby compromising their vitality
Encroachment on anatomical structuresSurgery increases the risk of damage to the anatomic structures such as mental foramen inferior alveolar nerve Also the aspirationndashirrigation technique a nonsurgical method is not recommended where adjacent tissue spaces or sinus cavities are involved
Patient cooperation
Considerable pain or discomfort can be experienced by the patient during or after a surgical procedure A nonsurgical approach would be recommended for apprehensive and uncooperative patients
Obstructions in the root canal system
Ledges calcified canals separated instruments may prevent access to the apical foramen and may warrant a surgical approach in managing periapical lesions related to such teeth
Time involved for treatment
Enhanced healing kinetics are observed after performing apical surgery in teeth with periapical lesions
Cases refractory to nonsurgical management methods
Inflammatory apical true cysts and the presence of cholesterol crystals have been suggested as possible causes that prevent healing of periapical lesionsSurgery is recommended for such cases
METHODS FOR NONSURGICAL MANAGMENT OF PERIAPICAL LESIONS Conservative root canal treatment without adjunctive therapy
Instrumentation should be carried 1 mm beyond the apical foramen when a periapical lesion is evident on a radiograph This may cause transitory inflammation and ulceration of the epithelial lining resulting in resolution of the cyst
Decompression technique
The decompression technique involves placement of a drain into the lesion regular irrigation periodic length adjustment and maintenance of the drain for various periods of time
Active nonsurgical decompression technique
This technique uses the Endo-eze vacuum system to create a negative pressure which results in the decompression of large periapical lesions The high-volume suction aspirator is connected to a micro 22-gauge needle which is inserted in the root canal and activated for 20 minutes creating a negative pressure which results in aspiration of the exudate When the drainage partially stops the access cavity is closed with temporary cement which helps in maintaining bacterial control
Aspiration and irrigation technique
Hoen et al suggested aspiration of the cystic fluid from the periapcial lesion using a buccal palatal approach In this technique an 18-gauge needle attached to a 20 ml syringe is used to penetrate the buccal mucosa and aspirate the cystic fluid A second syringe filled with saline is then used to rinse the bony lesion The new needle is inserted through the buccal wound and passed out through the palatal tissue creating a pathway for the escape of the irrigant
Aspiration through the root canal technique
In this technique aspiration of the cystic fluid is done through the root canal by passing the aspirating needle through the apical foramen This technique eliminates the creation of buccal and palatal wounds as in the traditional aspirationndashirrigation technique This minimizes the discomfort that the patient may experience
However it is advisable not to use either aspirationndashirrigation or aspiration through the root canal techniques where adjacent tissue spaces or sinus cavities are involved when there is no fluid aspiration from the lesion or in infected periapicallesions
Method using calcium hydroxide
Calcium hydroxide is a widely used material in endodontic treatment because of its bactericidal effectsIt is thought to create favorable conditions for periapical repair and stimulate hard tissue formationSouza et al suggested that the action of calcium hydroxide beyond the apex may be four-fold (a) anti-inflammatory activity (b) neutralization of acid products (c) activation of the alkaline phosphatase and (d) antibacterial action
Lesion sterilization and repair therapy
lsquoLesion Sterilization and Tissue Repair (LSTR)rsquo therapy that uses a triple antibiotic paste of ciprofloxacin metronidazole and minocycline for disinfection of oral infectious lesions including dentinal pulpal and periradicular lesions Repair of damaged tissues can be expected if lesions are disinfectedMetronidazole is the first choice because it has a wide antibacterial spectrum against anaerobesHowever some bacteria are resistant to metronidazole and hence ciprofloxacin and minocycline are added to the mix
Apexum procedure
Surgical removal of the periapical chronically inflamed tissue allows a fresh blood clot to form thereby converting a chronic inflammatory lesion into a new granulation tissue where healing might proceed much fasterThe Apexumprocedure uses two sequential rotary devices the Apexum NiTi Ablator and Apexum PGA Ablator (Apexum Ltd Or Yehuda Israel) designed to extend beyond the apex and mince the periapical tissues on rotation in a low-speed handpiece followed by washing out the minced tissue
Surgical management of Apical lesions Apical lesions maybe managed surgically to reduce
healing and recovery time
Indicated for emergency cases
Incision and drainagewith antibiotic therapy of the lesionfollowed by RCT with apisectomy is the usual modality of surgical treatment of apical lesions
Medical Management of apical lesions Antibiotic therapy is used to treat minor apical
lesionsin order to relieve the symptomsThis enables easier surgical or non0surgical management of the lesionThus medical management of apical lesions is used in conjunction with Surgical or non surgical management of apical lesions
Cellulitis-Cefazolin 1g iv Q8H7-10 days or cloxacillin500-1000mg po Q6H7-10 days
Acute osteomyelitis-Cefazolin 2g iv Q8H
Ludwigs angina-Clindamycin 600mg iv Q8H2-3 weeks
References J Conserv Dent 2010 Oct-Dec 13(4) 240-
245doi 1041030972070773384PMCID PMC3010029Nonsurgical management of periapical lesions Marina Fernandes and Ida de Ataide
Manual in maxillofacial surgery for senior house officers-Dental 2cmcvellore
DrVikram PerakathBDS
Cutaneous Sinus tract An abscess that drains on its ownextraorallythrough
the overlying skin(Draining sinus tract)
Extra oral abscess Localised collection of pus that has
accumulated(consolidated) in a tissue cavityproducing fluctuance
Can serve as a nidus for sacrophytic bacterial growth
Antibiotics cant reach center of large abscessesbecause blood supply is along the peripherytherefore draining is very important for effective antibiotic treatment
Cellulitis Diffuse spread of an acute inflammatory process
through the fascial planes of soft tissueproducingerythemaoedemawarmth and pain
It is a board-likediffusehard swelling
Trismus is a common secondary to cellulitis due to loss of function of muscles of mastication
Requires immediate antibiotics and drain placement
Ludwigs angina Aggressiverapidly spreading cellulitis involving
multiple anatomic spacessubmentalsublingualsubmandibular
Produces massive swelling of the neck that may extend close to the clavicles and cause airway obstruction(bullneck)
Causes elevation of the floor of the mouth and protrusion of tomgue(woody tongue)
Can be fatal due to airway obstructionmust establish an airwaydrain and give IV antibiotics
Cavernous sinus thrombosis Maybe associated with spread of infection from
maxillary teeth(classic canine space infection)
It is the formation of a blood clot within the cavernous sinus
Life threatening infection cause the cavernous sinus holds the pituitary gland and sella turcicaCranialnerves-346
Proliferative Periostitis Form of chronic osteomyelitis with proliferative
periostitis
Periosteal reaction in which layers of reactive vital bone are formedproducing cortical expansion(onion skinning) The periosteum is not destroyedbut lifted upwhen bone is formed beneath its layers
Chronic focal sclerosingosteomyelitis AKA Condensing osteitis Localised area of bone sclerosis associated with apices
of non-vital teeth
Most frequent in children and young adults involving mandibular molarspremolars
No cortical expansion
Differential diagnosisOsseous Dysplasia and idiopathic osseosclerosis
Osteomyelitis Bacterial infection of bone secondary to
A)Odontogenic infection
B)Traumatic injury
C)Necrotising Ulcerative GingivitisNoma or cancrumoris
Predisposition to decreased vascularity of bone-PagetrsquosOsteopetrosisflorid cemento-osseous dysplasia
Chronic PathwayPeriapical granuloma
It is a misnomerit is not a granulomatous reaction
Mass of chronically inflamed granulation tissue at apex of non-vital teethdesigned to wall off bacterial invasion at apex
Associated with chronic apical periodontitis
Periapical cyst AKA apical periodontal cystradicular cyst
Inflammatory odontogenic cystinduced by cell rests of malassez(Hertwigs Epithelial Root Sheath remnants) proliferation
Radiolucency at periapex of non-vital teeth
To differentiate from a granulomait must be tested histologically
Management of apical lesions Non-surgical management Periapical lesions develop as
sequelae to pulp disease They often occur without any episode of acute pain and are discovered on routine radiographic examination It is accepted that all inflammatory periapicallesions should be initially treated with conservative nonsurgical procedures
Methods1The conservative root canal treatment
2decompression technique3active nonsurgical decompression technique4aspiration-irrigation technique
5 method using calcium hydroxide6 Lesion Sterilization and Repair Therapy and7the Apexum procedure
Case selectionThe current philosophy in the management of periapical lesions includes the initial use of nonsurgical methods When this treatment approach is not successful a surgical approach may be adoptedThe following factors must be considered while deciding on the management approach
Diagnosis of the lesionMany bone destroying lesions closely resemble endodontically related periapicallesions on radiographs Some of these nonendodontic lesions include ameloblastoma central fibroma giant cell lesions fibrous dysplasia central hemangioma primary malignancies metastatic neoplasms and inflammatory bone diseases
Proximity of the periapical lesion to adjacent vital teethWhen in proximity to a vital toothadopting a surgical approach may result in injury to the blood vessels and nerves of the adjacent teeth thereby compromising their vitality
Encroachment on anatomical structuresSurgery increases the risk of damage to the anatomic structures such as mental foramen inferior alveolar nerve Also the aspirationndashirrigation technique a nonsurgical method is not recommended where adjacent tissue spaces or sinus cavities are involved
Patient cooperation
Considerable pain or discomfort can be experienced by the patient during or after a surgical procedure A nonsurgical approach would be recommended for apprehensive and uncooperative patients
Obstructions in the root canal system
Ledges calcified canals separated instruments may prevent access to the apical foramen and may warrant a surgical approach in managing periapical lesions related to such teeth
Time involved for treatment
Enhanced healing kinetics are observed after performing apical surgery in teeth with periapical lesions
Cases refractory to nonsurgical management methods
Inflammatory apical true cysts and the presence of cholesterol crystals have been suggested as possible causes that prevent healing of periapical lesionsSurgery is recommended for such cases
METHODS FOR NONSURGICAL MANAGMENT OF PERIAPICAL LESIONS Conservative root canal treatment without adjunctive therapy
Instrumentation should be carried 1 mm beyond the apical foramen when a periapical lesion is evident on a radiograph This may cause transitory inflammation and ulceration of the epithelial lining resulting in resolution of the cyst
Decompression technique
The decompression technique involves placement of a drain into the lesion regular irrigation periodic length adjustment and maintenance of the drain for various periods of time
Active nonsurgical decompression technique
This technique uses the Endo-eze vacuum system to create a negative pressure which results in the decompression of large periapical lesions The high-volume suction aspirator is connected to a micro 22-gauge needle which is inserted in the root canal and activated for 20 minutes creating a negative pressure which results in aspiration of the exudate When the drainage partially stops the access cavity is closed with temporary cement which helps in maintaining bacterial control
Aspiration and irrigation technique
Hoen et al suggested aspiration of the cystic fluid from the periapcial lesion using a buccal palatal approach In this technique an 18-gauge needle attached to a 20 ml syringe is used to penetrate the buccal mucosa and aspirate the cystic fluid A second syringe filled with saline is then used to rinse the bony lesion The new needle is inserted through the buccal wound and passed out through the palatal tissue creating a pathway for the escape of the irrigant
Aspiration through the root canal technique
In this technique aspiration of the cystic fluid is done through the root canal by passing the aspirating needle through the apical foramen This technique eliminates the creation of buccal and palatal wounds as in the traditional aspirationndashirrigation technique This minimizes the discomfort that the patient may experience
However it is advisable not to use either aspirationndashirrigation or aspiration through the root canal techniques where adjacent tissue spaces or sinus cavities are involved when there is no fluid aspiration from the lesion or in infected periapicallesions
Method using calcium hydroxide
Calcium hydroxide is a widely used material in endodontic treatment because of its bactericidal effectsIt is thought to create favorable conditions for periapical repair and stimulate hard tissue formationSouza et al suggested that the action of calcium hydroxide beyond the apex may be four-fold (a) anti-inflammatory activity (b) neutralization of acid products (c) activation of the alkaline phosphatase and (d) antibacterial action
Lesion sterilization and repair therapy
lsquoLesion Sterilization and Tissue Repair (LSTR)rsquo therapy that uses a triple antibiotic paste of ciprofloxacin metronidazole and minocycline for disinfection of oral infectious lesions including dentinal pulpal and periradicular lesions Repair of damaged tissues can be expected if lesions are disinfectedMetronidazole is the first choice because it has a wide antibacterial spectrum against anaerobesHowever some bacteria are resistant to metronidazole and hence ciprofloxacin and minocycline are added to the mix
Apexum procedure
Surgical removal of the periapical chronically inflamed tissue allows a fresh blood clot to form thereby converting a chronic inflammatory lesion into a new granulation tissue where healing might proceed much fasterThe Apexumprocedure uses two sequential rotary devices the Apexum NiTi Ablator and Apexum PGA Ablator (Apexum Ltd Or Yehuda Israel) designed to extend beyond the apex and mince the periapical tissues on rotation in a low-speed handpiece followed by washing out the minced tissue
Surgical management of Apical lesions Apical lesions maybe managed surgically to reduce
healing and recovery time
Indicated for emergency cases
Incision and drainagewith antibiotic therapy of the lesionfollowed by RCT with apisectomy is the usual modality of surgical treatment of apical lesions
Medical Management of apical lesions Antibiotic therapy is used to treat minor apical
lesionsin order to relieve the symptomsThis enables easier surgical or non0surgical management of the lesionThus medical management of apical lesions is used in conjunction with Surgical or non surgical management of apical lesions
Cellulitis-Cefazolin 1g iv Q8H7-10 days or cloxacillin500-1000mg po Q6H7-10 days
Acute osteomyelitis-Cefazolin 2g iv Q8H
Ludwigs angina-Clindamycin 600mg iv Q8H2-3 weeks
References J Conserv Dent 2010 Oct-Dec 13(4) 240-
245doi 1041030972070773384PMCID PMC3010029Nonsurgical management of periapical lesions Marina Fernandes and Ida de Ataide
Manual in maxillofacial surgery for senior house officers-Dental 2cmcvellore
DrVikram PerakathBDS
Extra oral abscess Localised collection of pus that has
accumulated(consolidated) in a tissue cavityproducing fluctuance
Can serve as a nidus for sacrophytic bacterial growth
Antibiotics cant reach center of large abscessesbecause blood supply is along the peripherytherefore draining is very important for effective antibiotic treatment
Cellulitis Diffuse spread of an acute inflammatory process
through the fascial planes of soft tissueproducingerythemaoedemawarmth and pain
It is a board-likediffusehard swelling
Trismus is a common secondary to cellulitis due to loss of function of muscles of mastication
Requires immediate antibiotics and drain placement
Ludwigs angina Aggressiverapidly spreading cellulitis involving
multiple anatomic spacessubmentalsublingualsubmandibular
Produces massive swelling of the neck that may extend close to the clavicles and cause airway obstruction(bullneck)
Causes elevation of the floor of the mouth and protrusion of tomgue(woody tongue)
Can be fatal due to airway obstructionmust establish an airwaydrain and give IV antibiotics
Cavernous sinus thrombosis Maybe associated with spread of infection from
maxillary teeth(classic canine space infection)
It is the formation of a blood clot within the cavernous sinus
Life threatening infection cause the cavernous sinus holds the pituitary gland and sella turcicaCranialnerves-346
Proliferative Periostitis Form of chronic osteomyelitis with proliferative
periostitis
Periosteal reaction in which layers of reactive vital bone are formedproducing cortical expansion(onion skinning) The periosteum is not destroyedbut lifted upwhen bone is formed beneath its layers
Chronic focal sclerosingosteomyelitis AKA Condensing osteitis Localised area of bone sclerosis associated with apices
of non-vital teeth
Most frequent in children and young adults involving mandibular molarspremolars
No cortical expansion
Differential diagnosisOsseous Dysplasia and idiopathic osseosclerosis
Osteomyelitis Bacterial infection of bone secondary to
A)Odontogenic infection
B)Traumatic injury
C)Necrotising Ulcerative GingivitisNoma or cancrumoris
Predisposition to decreased vascularity of bone-PagetrsquosOsteopetrosisflorid cemento-osseous dysplasia
Chronic PathwayPeriapical granuloma
It is a misnomerit is not a granulomatous reaction
Mass of chronically inflamed granulation tissue at apex of non-vital teethdesigned to wall off bacterial invasion at apex
Associated with chronic apical periodontitis
Periapical cyst AKA apical periodontal cystradicular cyst
Inflammatory odontogenic cystinduced by cell rests of malassez(Hertwigs Epithelial Root Sheath remnants) proliferation
Radiolucency at periapex of non-vital teeth
To differentiate from a granulomait must be tested histologically
Management of apical lesions Non-surgical management Periapical lesions develop as
sequelae to pulp disease They often occur without any episode of acute pain and are discovered on routine radiographic examination It is accepted that all inflammatory periapicallesions should be initially treated with conservative nonsurgical procedures
Methods1The conservative root canal treatment
2decompression technique3active nonsurgical decompression technique4aspiration-irrigation technique
5 method using calcium hydroxide6 Lesion Sterilization and Repair Therapy and7the Apexum procedure
Case selectionThe current philosophy in the management of periapical lesions includes the initial use of nonsurgical methods When this treatment approach is not successful a surgical approach may be adoptedThe following factors must be considered while deciding on the management approach
Diagnosis of the lesionMany bone destroying lesions closely resemble endodontically related periapicallesions on radiographs Some of these nonendodontic lesions include ameloblastoma central fibroma giant cell lesions fibrous dysplasia central hemangioma primary malignancies metastatic neoplasms and inflammatory bone diseases
Proximity of the periapical lesion to adjacent vital teethWhen in proximity to a vital toothadopting a surgical approach may result in injury to the blood vessels and nerves of the adjacent teeth thereby compromising their vitality
Encroachment on anatomical structuresSurgery increases the risk of damage to the anatomic structures such as mental foramen inferior alveolar nerve Also the aspirationndashirrigation technique a nonsurgical method is not recommended where adjacent tissue spaces or sinus cavities are involved
Patient cooperation
Considerable pain or discomfort can be experienced by the patient during or after a surgical procedure A nonsurgical approach would be recommended for apprehensive and uncooperative patients
Obstructions in the root canal system
Ledges calcified canals separated instruments may prevent access to the apical foramen and may warrant a surgical approach in managing periapical lesions related to such teeth
Time involved for treatment
Enhanced healing kinetics are observed after performing apical surgery in teeth with periapical lesions
Cases refractory to nonsurgical management methods
Inflammatory apical true cysts and the presence of cholesterol crystals have been suggested as possible causes that prevent healing of periapical lesionsSurgery is recommended for such cases
METHODS FOR NONSURGICAL MANAGMENT OF PERIAPICAL LESIONS Conservative root canal treatment without adjunctive therapy
Instrumentation should be carried 1 mm beyond the apical foramen when a periapical lesion is evident on a radiograph This may cause transitory inflammation and ulceration of the epithelial lining resulting in resolution of the cyst
Decompression technique
The decompression technique involves placement of a drain into the lesion regular irrigation periodic length adjustment and maintenance of the drain for various periods of time
Active nonsurgical decompression technique
This technique uses the Endo-eze vacuum system to create a negative pressure which results in the decompression of large periapical lesions The high-volume suction aspirator is connected to a micro 22-gauge needle which is inserted in the root canal and activated for 20 minutes creating a negative pressure which results in aspiration of the exudate When the drainage partially stops the access cavity is closed with temporary cement which helps in maintaining bacterial control
Aspiration and irrigation technique
Hoen et al suggested aspiration of the cystic fluid from the periapcial lesion using a buccal palatal approach In this technique an 18-gauge needle attached to a 20 ml syringe is used to penetrate the buccal mucosa and aspirate the cystic fluid A second syringe filled with saline is then used to rinse the bony lesion The new needle is inserted through the buccal wound and passed out through the palatal tissue creating a pathway for the escape of the irrigant
Aspiration through the root canal technique
In this technique aspiration of the cystic fluid is done through the root canal by passing the aspirating needle through the apical foramen This technique eliminates the creation of buccal and palatal wounds as in the traditional aspirationndashirrigation technique This minimizes the discomfort that the patient may experience
However it is advisable not to use either aspirationndashirrigation or aspiration through the root canal techniques where adjacent tissue spaces or sinus cavities are involved when there is no fluid aspiration from the lesion or in infected periapicallesions
Method using calcium hydroxide
Calcium hydroxide is a widely used material in endodontic treatment because of its bactericidal effectsIt is thought to create favorable conditions for periapical repair and stimulate hard tissue formationSouza et al suggested that the action of calcium hydroxide beyond the apex may be four-fold (a) anti-inflammatory activity (b) neutralization of acid products (c) activation of the alkaline phosphatase and (d) antibacterial action
Lesion sterilization and repair therapy
lsquoLesion Sterilization and Tissue Repair (LSTR)rsquo therapy that uses a triple antibiotic paste of ciprofloxacin metronidazole and minocycline for disinfection of oral infectious lesions including dentinal pulpal and periradicular lesions Repair of damaged tissues can be expected if lesions are disinfectedMetronidazole is the first choice because it has a wide antibacterial spectrum against anaerobesHowever some bacteria are resistant to metronidazole and hence ciprofloxacin and minocycline are added to the mix
Apexum procedure
Surgical removal of the periapical chronically inflamed tissue allows a fresh blood clot to form thereby converting a chronic inflammatory lesion into a new granulation tissue where healing might proceed much fasterThe Apexumprocedure uses two sequential rotary devices the Apexum NiTi Ablator and Apexum PGA Ablator (Apexum Ltd Or Yehuda Israel) designed to extend beyond the apex and mince the periapical tissues on rotation in a low-speed handpiece followed by washing out the minced tissue
Surgical management of Apical lesions Apical lesions maybe managed surgically to reduce
healing and recovery time
Indicated for emergency cases
Incision and drainagewith antibiotic therapy of the lesionfollowed by RCT with apisectomy is the usual modality of surgical treatment of apical lesions
Medical Management of apical lesions Antibiotic therapy is used to treat minor apical
lesionsin order to relieve the symptomsThis enables easier surgical or non0surgical management of the lesionThus medical management of apical lesions is used in conjunction with Surgical or non surgical management of apical lesions
Cellulitis-Cefazolin 1g iv Q8H7-10 days or cloxacillin500-1000mg po Q6H7-10 days
Acute osteomyelitis-Cefazolin 2g iv Q8H
Ludwigs angina-Clindamycin 600mg iv Q8H2-3 weeks
References J Conserv Dent 2010 Oct-Dec 13(4) 240-
245doi 1041030972070773384PMCID PMC3010029Nonsurgical management of periapical lesions Marina Fernandes and Ida de Ataide
Manual in maxillofacial surgery for senior house officers-Dental 2cmcvellore
DrVikram PerakathBDS
Cellulitis Diffuse spread of an acute inflammatory process
through the fascial planes of soft tissueproducingerythemaoedemawarmth and pain
It is a board-likediffusehard swelling
Trismus is a common secondary to cellulitis due to loss of function of muscles of mastication
Requires immediate antibiotics and drain placement
Ludwigs angina Aggressiverapidly spreading cellulitis involving
multiple anatomic spacessubmentalsublingualsubmandibular
Produces massive swelling of the neck that may extend close to the clavicles and cause airway obstruction(bullneck)
Causes elevation of the floor of the mouth and protrusion of tomgue(woody tongue)
Can be fatal due to airway obstructionmust establish an airwaydrain and give IV antibiotics
Cavernous sinus thrombosis Maybe associated with spread of infection from
maxillary teeth(classic canine space infection)
It is the formation of a blood clot within the cavernous sinus
Life threatening infection cause the cavernous sinus holds the pituitary gland and sella turcicaCranialnerves-346
Proliferative Periostitis Form of chronic osteomyelitis with proliferative
periostitis
Periosteal reaction in which layers of reactive vital bone are formedproducing cortical expansion(onion skinning) The periosteum is not destroyedbut lifted upwhen bone is formed beneath its layers
Chronic focal sclerosingosteomyelitis AKA Condensing osteitis Localised area of bone sclerosis associated with apices
of non-vital teeth
Most frequent in children and young adults involving mandibular molarspremolars
No cortical expansion
Differential diagnosisOsseous Dysplasia and idiopathic osseosclerosis
Osteomyelitis Bacterial infection of bone secondary to
A)Odontogenic infection
B)Traumatic injury
C)Necrotising Ulcerative GingivitisNoma or cancrumoris
Predisposition to decreased vascularity of bone-PagetrsquosOsteopetrosisflorid cemento-osseous dysplasia
Chronic PathwayPeriapical granuloma
It is a misnomerit is not a granulomatous reaction
Mass of chronically inflamed granulation tissue at apex of non-vital teethdesigned to wall off bacterial invasion at apex
Associated with chronic apical periodontitis
Periapical cyst AKA apical periodontal cystradicular cyst
Inflammatory odontogenic cystinduced by cell rests of malassez(Hertwigs Epithelial Root Sheath remnants) proliferation
Radiolucency at periapex of non-vital teeth
To differentiate from a granulomait must be tested histologically
Management of apical lesions Non-surgical management Periapical lesions develop as
sequelae to pulp disease They often occur without any episode of acute pain and are discovered on routine radiographic examination It is accepted that all inflammatory periapicallesions should be initially treated with conservative nonsurgical procedures
Methods1The conservative root canal treatment
2decompression technique3active nonsurgical decompression technique4aspiration-irrigation technique
5 method using calcium hydroxide6 Lesion Sterilization and Repair Therapy and7the Apexum procedure
Case selectionThe current philosophy in the management of periapical lesions includes the initial use of nonsurgical methods When this treatment approach is not successful a surgical approach may be adoptedThe following factors must be considered while deciding on the management approach
Diagnosis of the lesionMany bone destroying lesions closely resemble endodontically related periapicallesions on radiographs Some of these nonendodontic lesions include ameloblastoma central fibroma giant cell lesions fibrous dysplasia central hemangioma primary malignancies metastatic neoplasms and inflammatory bone diseases
Proximity of the periapical lesion to adjacent vital teethWhen in proximity to a vital toothadopting a surgical approach may result in injury to the blood vessels and nerves of the adjacent teeth thereby compromising their vitality
Encroachment on anatomical structuresSurgery increases the risk of damage to the anatomic structures such as mental foramen inferior alveolar nerve Also the aspirationndashirrigation technique a nonsurgical method is not recommended where adjacent tissue spaces or sinus cavities are involved
Patient cooperation
Considerable pain or discomfort can be experienced by the patient during or after a surgical procedure A nonsurgical approach would be recommended for apprehensive and uncooperative patients
Obstructions in the root canal system
Ledges calcified canals separated instruments may prevent access to the apical foramen and may warrant a surgical approach in managing periapical lesions related to such teeth
Time involved for treatment
Enhanced healing kinetics are observed after performing apical surgery in teeth with periapical lesions
Cases refractory to nonsurgical management methods
Inflammatory apical true cysts and the presence of cholesterol crystals have been suggested as possible causes that prevent healing of periapical lesionsSurgery is recommended for such cases
METHODS FOR NONSURGICAL MANAGMENT OF PERIAPICAL LESIONS Conservative root canal treatment without adjunctive therapy
Instrumentation should be carried 1 mm beyond the apical foramen when a periapical lesion is evident on a radiograph This may cause transitory inflammation and ulceration of the epithelial lining resulting in resolution of the cyst
Decompression technique
The decompression technique involves placement of a drain into the lesion regular irrigation periodic length adjustment and maintenance of the drain for various periods of time
Active nonsurgical decompression technique
This technique uses the Endo-eze vacuum system to create a negative pressure which results in the decompression of large periapical lesions The high-volume suction aspirator is connected to a micro 22-gauge needle which is inserted in the root canal and activated for 20 minutes creating a negative pressure which results in aspiration of the exudate When the drainage partially stops the access cavity is closed with temporary cement which helps in maintaining bacterial control
Aspiration and irrigation technique
Hoen et al suggested aspiration of the cystic fluid from the periapcial lesion using a buccal palatal approach In this technique an 18-gauge needle attached to a 20 ml syringe is used to penetrate the buccal mucosa and aspirate the cystic fluid A second syringe filled with saline is then used to rinse the bony lesion The new needle is inserted through the buccal wound and passed out through the palatal tissue creating a pathway for the escape of the irrigant
Aspiration through the root canal technique
In this technique aspiration of the cystic fluid is done through the root canal by passing the aspirating needle through the apical foramen This technique eliminates the creation of buccal and palatal wounds as in the traditional aspirationndashirrigation technique This minimizes the discomfort that the patient may experience
However it is advisable not to use either aspirationndashirrigation or aspiration through the root canal techniques where adjacent tissue spaces or sinus cavities are involved when there is no fluid aspiration from the lesion or in infected periapicallesions
Method using calcium hydroxide
Calcium hydroxide is a widely used material in endodontic treatment because of its bactericidal effectsIt is thought to create favorable conditions for periapical repair and stimulate hard tissue formationSouza et al suggested that the action of calcium hydroxide beyond the apex may be four-fold (a) anti-inflammatory activity (b) neutralization of acid products (c) activation of the alkaline phosphatase and (d) antibacterial action
Lesion sterilization and repair therapy
lsquoLesion Sterilization and Tissue Repair (LSTR)rsquo therapy that uses a triple antibiotic paste of ciprofloxacin metronidazole and minocycline for disinfection of oral infectious lesions including dentinal pulpal and periradicular lesions Repair of damaged tissues can be expected if lesions are disinfectedMetronidazole is the first choice because it has a wide antibacterial spectrum against anaerobesHowever some bacteria are resistant to metronidazole and hence ciprofloxacin and minocycline are added to the mix
Apexum procedure
Surgical removal of the periapical chronically inflamed tissue allows a fresh blood clot to form thereby converting a chronic inflammatory lesion into a new granulation tissue where healing might proceed much fasterThe Apexumprocedure uses two sequential rotary devices the Apexum NiTi Ablator and Apexum PGA Ablator (Apexum Ltd Or Yehuda Israel) designed to extend beyond the apex and mince the periapical tissues on rotation in a low-speed handpiece followed by washing out the minced tissue
Surgical management of Apical lesions Apical lesions maybe managed surgically to reduce
healing and recovery time
Indicated for emergency cases
Incision and drainagewith antibiotic therapy of the lesionfollowed by RCT with apisectomy is the usual modality of surgical treatment of apical lesions
Medical Management of apical lesions Antibiotic therapy is used to treat minor apical
lesionsin order to relieve the symptomsThis enables easier surgical or non0surgical management of the lesionThus medical management of apical lesions is used in conjunction with Surgical or non surgical management of apical lesions
Cellulitis-Cefazolin 1g iv Q8H7-10 days or cloxacillin500-1000mg po Q6H7-10 days
Acute osteomyelitis-Cefazolin 2g iv Q8H
Ludwigs angina-Clindamycin 600mg iv Q8H2-3 weeks
References J Conserv Dent 2010 Oct-Dec 13(4) 240-
245doi 1041030972070773384PMCID PMC3010029Nonsurgical management of periapical lesions Marina Fernandes and Ida de Ataide
Manual in maxillofacial surgery for senior house officers-Dental 2cmcvellore
DrVikram PerakathBDS
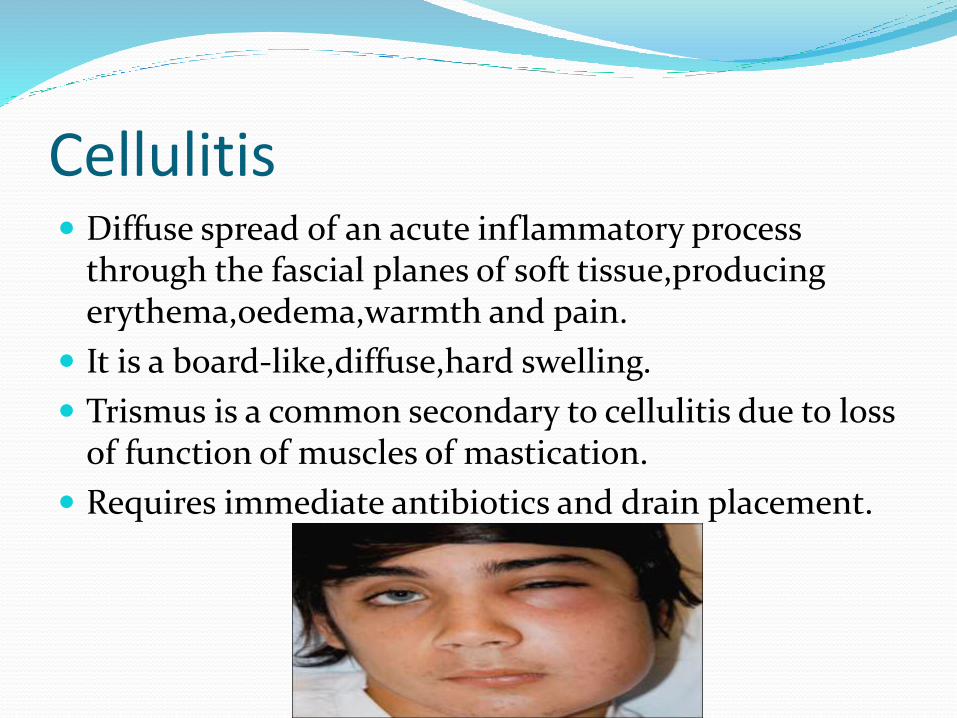
Ludwigs angina Aggressiverapidly spreading cellulitis involving
multiple anatomic spacessubmentalsublingualsubmandibular
Produces massive swelling of the neck that may extend close to the clavicles and cause airway obstruction(bullneck)
Causes elevation of the floor of the mouth and protrusion of tomgue(woody tongue)
Can be fatal due to airway obstructionmust establish an airwaydrain and give IV antibiotics
Cavernous sinus thrombosis Maybe associated with spread of infection from
maxillary teeth(classic canine space infection)
It is the formation of a blood clot within the cavernous sinus
Life threatening infection cause the cavernous sinus holds the pituitary gland and sella turcicaCranialnerves-346
Proliferative Periostitis Form of chronic osteomyelitis with proliferative
periostitis
Periosteal reaction in which layers of reactive vital bone are formedproducing cortical expansion(onion skinning) The periosteum is not destroyedbut lifted upwhen bone is formed beneath its layers
Chronic focal sclerosingosteomyelitis AKA Condensing osteitis Localised area of bone sclerosis associated with apices
of non-vital teeth
Most frequent in children and young adults involving mandibular molarspremolars
No cortical expansion
Differential diagnosisOsseous Dysplasia and idiopathic osseosclerosis
Osteomyelitis Bacterial infection of bone secondary to
A)Odontogenic infection
B)Traumatic injury
C)Necrotising Ulcerative GingivitisNoma or cancrumoris
Predisposition to decreased vascularity of bone-PagetrsquosOsteopetrosisflorid cemento-osseous dysplasia
Chronic PathwayPeriapical granuloma
It is a misnomerit is not a granulomatous reaction
Mass of chronically inflamed granulation tissue at apex of non-vital teethdesigned to wall off bacterial invasion at apex
Associated with chronic apical periodontitis
Periapical cyst AKA apical periodontal cystradicular cyst
Inflammatory odontogenic cystinduced by cell rests of malassez(Hertwigs Epithelial Root Sheath remnants) proliferation
Radiolucency at periapex of non-vital teeth
To differentiate from a granulomait must be tested histologically
Management of apical lesions Non-surgical management Periapical lesions develop as
sequelae to pulp disease They often occur without any episode of acute pain and are discovered on routine radiographic examination It is accepted that all inflammatory periapicallesions should be initially treated with conservative nonsurgical procedures
Methods1The conservative root canal treatment
2decompression technique3active nonsurgical decompression technique4aspiration-irrigation technique
5 method using calcium hydroxide6 Lesion Sterilization and Repair Therapy and7the Apexum procedure
Case selectionThe current philosophy in the management of periapical lesions includes the initial use of nonsurgical methods When this treatment approach is not successful a surgical approach may be adoptedThe following factors must be considered while deciding on the management approach
Diagnosis of the lesionMany bone destroying lesions closely resemble endodontically related periapicallesions on radiographs Some of these nonendodontic lesions include ameloblastoma central fibroma giant cell lesions fibrous dysplasia central hemangioma primary malignancies metastatic neoplasms and inflammatory bone diseases
Proximity of the periapical lesion to adjacent vital teethWhen in proximity to a vital toothadopting a surgical approach may result in injury to the blood vessels and nerves of the adjacent teeth thereby compromising their vitality
Encroachment on anatomical structuresSurgery increases the risk of damage to the anatomic structures such as mental foramen inferior alveolar nerve Also the aspirationndashirrigation technique a nonsurgical method is not recommended where adjacent tissue spaces or sinus cavities are involved
Patient cooperation
Considerable pain or discomfort can be experienced by the patient during or after a surgical procedure A nonsurgical approach would be recommended for apprehensive and uncooperative patients
Obstructions in the root canal system
Ledges calcified canals separated instruments may prevent access to the apical foramen and may warrant a surgical approach in managing periapical lesions related to such teeth
Time involved for treatment
Enhanced healing kinetics are observed after performing apical surgery in teeth with periapical lesions
Cases refractory to nonsurgical management methods
Inflammatory apical true cysts and the presence of cholesterol crystals have been suggested as possible causes that prevent healing of periapical lesionsSurgery is recommended for such cases
METHODS FOR NONSURGICAL MANAGMENT OF PERIAPICAL LESIONS Conservative root canal treatment without adjunctive therapy
Instrumentation should be carried 1 mm beyond the apical foramen when a periapical lesion is evident on a radiograph This may cause transitory inflammation and ulceration of the epithelial lining resulting in resolution of the cyst
Decompression technique
The decompression technique involves placement of a drain into the lesion regular irrigation periodic length adjustment and maintenance of the drain for various periods of time
Active nonsurgical decompression technique
This technique uses the Endo-eze vacuum system to create a negative pressure which results in the decompression of large periapical lesions The high-volume suction aspirator is connected to a micro 22-gauge needle which is inserted in the root canal and activated for 20 minutes creating a negative pressure which results in aspiration of the exudate When the drainage partially stops the access cavity is closed with temporary cement which helps in maintaining bacterial control
Aspiration and irrigation technique
Hoen et al suggested aspiration of the cystic fluid from the periapcial lesion using a buccal palatal approach In this technique an 18-gauge needle attached to a 20 ml syringe is used to penetrate the buccal mucosa and aspirate the cystic fluid A second syringe filled with saline is then used to rinse the bony lesion The new needle is inserted through the buccal wound and passed out through the palatal tissue creating a pathway for the escape of the irrigant
Aspiration through the root canal technique
In this technique aspiration of the cystic fluid is done through the root canal by passing the aspirating needle through the apical foramen This technique eliminates the creation of buccal and palatal wounds as in the traditional aspirationndashirrigation technique This minimizes the discomfort that the patient may experience
However it is advisable not to use either aspirationndashirrigation or aspiration through the root canal techniques where adjacent tissue spaces or sinus cavities are involved when there is no fluid aspiration from the lesion or in infected periapicallesions
Method using calcium hydroxide
Calcium hydroxide is a widely used material in endodontic treatment because of its bactericidal effectsIt is thought to create favorable conditions for periapical repair and stimulate hard tissue formationSouza et al suggested that the action of calcium hydroxide beyond the apex may be four-fold (a) anti-inflammatory activity (b) neutralization of acid products (c) activation of the alkaline phosphatase and (d) antibacterial action
Lesion sterilization and repair therapy
lsquoLesion Sterilization and Tissue Repair (LSTR)rsquo therapy that uses a triple antibiotic paste of ciprofloxacin metronidazole and minocycline for disinfection of oral infectious lesions including dentinal pulpal and periradicular lesions Repair of damaged tissues can be expected if lesions are disinfectedMetronidazole is the first choice because it has a wide antibacterial spectrum against anaerobesHowever some bacteria are resistant to metronidazole and hence ciprofloxacin and minocycline are added to the mix
Apexum procedure
Surgical removal of the periapical chronically inflamed tissue allows a fresh blood clot to form thereby converting a chronic inflammatory lesion into a new granulation tissue where healing might proceed much fasterThe Apexumprocedure uses two sequential rotary devices the Apexum NiTi Ablator and Apexum PGA Ablator (Apexum Ltd Or Yehuda Israel) designed to extend beyond the apex and mince the periapical tissues on rotation in a low-speed handpiece followed by washing out the minced tissue
Surgical management of Apical lesions Apical lesions maybe managed surgically to reduce
healing and recovery time
Indicated for emergency cases
Incision and drainagewith antibiotic therapy of the lesionfollowed by RCT with apisectomy is the usual modality of surgical treatment of apical lesions
Medical Management of apical lesions Antibiotic therapy is used to treat minor apical
lesionsin order to relieve the symptomsThis enables easier surgical or non0surgical management of the lesionThus medical management of apical lesions is used in conjunction with Surgical or non surgical management of apical lesions
Cellulitis-Cefazolin 1g iv Q8H7-10 days or cloxacillin500-1000mg po Q6H7-10 days
Acute osteomyelitis-Cefazolin 2g iv Q8H
Ludwigs angina-Clindamycin 600mg iv Q8H2-3 weeks
References J Conserv Dent 2010 Oct-Dec 13(4) 240-
245doi 1041030972070773384PMCID PMC3010029Nonsurgical management of periapical lesions Marina Fernandes and Ida de Ataide
Manual in maxillofacial surgery for senior house officers-Dental 2cmcvellore
DrVikram PerakathBDS
Cavernous sinus thrombosis Maybe associated with spread of infection from
maxillary teeth(classic canine space infection)
It is the formation of a blood clot within the cavernous sinus
Life threatening infection cause the cavernous sinus holds the pituitary gland and sella turcicaCranialnerves-346
Proliferative Periostitis Form of chronic osteomyelitis with proliferative
periostitis
Periosteal reaction in which layers of reactive vital bone are formedproducing cortical expansion(onion skinning) The periosteum is not destroyedbut lifted upwhen bone is formed beneath its layers
Chronic focal sclerosingosteomyelitis AKA Condensing osteitis Localised area of bone sclerosis associated with apices
of non-vital teeth
Most frequent in children and young adults involving mandibular molarspremolars
No cortical expansion
Differential diagnosisOsseous Dysplasia and idiopathic osseosclerosis
Osteomyelitis Bacterial infection of bone secondary to
A)Odontogenic infection
B)Traumatic injury
C)Necrotising Ulcerative GingivitisNoma or cancrumoris
Predisposition to decreased vascularity of bone-PagetrsquosOsteopetrosisflorid cemento-osseous dysplasia
Chronic PathwayPeriapical granuloma
It is a misnomerit is not a granulomatous reaction
Mass of chronically inflamed granulation tissue at apex of non-vital teethdesigned to wall off bacterial invasion at apex
Associated with chronic apical periodontitis
Periapical cyst AKA apical periodontal cystradicular cyst
Inflammatory odontogenic cystinduced by cell rests of malassez(Hertwigs Epithelial Root Sheath remnants) proliferation
Radiolucency at periapex of non-vital teeth
To differentiate from a granulomait must be tested histologically
Management of apical lesions Non-surgical management Periapical lesions develop as
sequelae to pulp disease They often occur without any episode of acute pain and are discovered on routine radiographic examination It is accepted that all inflammatory periapicallesions should be initially treated with conservative nonsurgical procedures
Methods1The conservative root canal treatment
2decompression technique3active nonsurgical decompression technique4aspiration-irrigation technique
5 method using calcium hydroxide6 Lesion Sterilization and Repair Therapy and7the Apexum procedure
Case selectionThe current philosophy in the management of periapical lesions includes the initial use of nonsurgical methods When this treatment approach is not successful a surgical approach may be adoptedThe following factors must be considered while deciding on the management approach
Diagnosis of the lesionMany bone destroying lesions closely resemble endodontically related periapicallesions on radiographs Some of these nonendodontic lesions include ameloblastoma central fibroma giant cell lesions fibrous dysplasia central hemangioma primary malignancies metastatic neoplasms and inflammatory bone diseases
Proximity of the periapical lesion to adjacent vital teethWhen in proximity to a vital toothadopting a surgical approach may result in injury to the blood vessels and nerves of the adjacent teeth thereby compromising their vitality
Encroachment on anatomical structuresSurgery increases the risk of damage to the anatomic structures such as mental foramen inferior alveolar nerve Also the aspirationndashirrigation technique a nonsurgical method is not recommended where adjacent tissue spaces or sinus cavities are involved
Patient cooperation
Considerable pain or discomfort can be experienced by the patient during or after a surgical procedure A nonsurgical approach would be recommended for apprehensive and uncooperative patients
Obstructions in the root canal system
Ledges calcified canals separated instruments may prevent access to the apical foramen and may warrant a surgical approach in managing periapical lesions related to such teeth
Time involved for treatment
Enhanced healing kinetics are observed after performing apical surgery in teeth with periapical lesions
Cases refractory to nonsurgical management methods
Inflammatory apical true cysts and the presence of cholesterol crystals have been suggested as possible causes that prevent healing of periapical lesionsSurgery is recommended for such cases
METHODS FOR NONSURGICAL MANAGMENT OF PERIAPICAL LESIONS Conservative root canal treatment without adjunctive therapy
Instrumentation should be carried 1 mm beyond the apical foramen when a periapical lesion is evident on a radiograph This may cause transitory inflammation and ulceration of the epithelial lining resulting in resolution of the cyst
Decompression technique
The decompression technique involves placement of a drain into the lesion regular irrigation periodic length adjustment and maintenance of the drain for various periods of time
Active nonsurgical decompression technique
This technique uses the Endo-eze vacuum system to create a negative pressure which results in the decompression of large periapical lesions The high-volume suction aspirator is connected to a micro 22-gauge needle which is inserted in the root canal and activated for 20 minutes creating a negative pressure which results in aspiration of the exudate When the drainage partially stops the access cavity is closed with temporary cement which helps in maintaining bacterial control
Aspiration and irrigation technique
Hoen et al suggested aspiration of the cystic fluid from the periapcial lesion using a buccal palatal approach In this technique an 18-gauge needle attached to a 20 ml syringe is used to penetrate the buccal mucosa and aspirate the cystic fluid A second syringe filled with saline is then used to rinse the bony lesion The new needle is inserted through the buccal wound and passed out through the palatal tissue creating a pathway for the escape of the irrigant
Aspiration through the root canal technique
In this technique aspiration of the cystic fluid is done through the root canal by passing the aspirating needle through the apical foramen This technique eliminates the creation of buccal and palatal wounds as in the traditional aspirationndashirrigation technique This minimizes the discomfort that the patient may experience
However it is advisable not to use either aspirationndashirrigation or aspiration through the root canal techniques where adjacent tissue spaces or sinus cavities are involved when there is no fluid aspiration from the lesion or in infected periapicallesions
Method using calcium hydroxide
Calcium hydroxide is a widely used material in endodontic treatment because of its bactericidal effectsIt is thought to create favorable conditions for periapical repair and stimulate hard tissue formationSouza et al suggested that the action of calcium hydroxide beyond the apex may be four-fold (a) anti-inflammatory activity (b) neutralization of acid products (c) activation of the alkaline phosphatase and (d) antibacterial action
Lesion sterilization and repair therapy
lsquoLesion Sterilization and Tissue Repair (LSTR)rsquo therapy that uses a triple antibiotic paste of ciprofloxacin metronidazole and minocycline for disinfection of oral infectious lesions including dentinal pulpal and periradicular lesions Repair of damaged tissues can be expected if lesions are disinfectedMetronidazole is the first choice because it has a wide antibacterial spectrum against anaerobesHowever some bacteria are resistant to metronidazole and hence ciprofloxacin and minocycline are added to the mix
Apexum procedure
Surgical removal of the periapical chronically inflamed tissue allows a fresh blood clot to form thereby converting a chronic inflammatory lesion into a new granulation tissue where healing might proceed much fasterThe Apexumprocedure uses two sequential rotary devices the Apexum NiTi Ablator and Apexum PGA Ablator (Apexum Ltd Or Yehuda Israel) designed to extend beyond the apex and mince the periapical tissues on rotation in a low-speed handpiece followed by washing out the minced tissue
Surgical management of Apical lesions Apical lesions maybe managed surgically to reduce
healing and recovery time
Indicated for emergency cases
Incision and drainagewith antibiotic therapy of the lesionfollowed by RCT with apisectomy is the usual modality of surgical treatment of apical lesions
Medical Management of apical lesions Antibiotic therapy is used to treat minor apical
lesionsin order to relieve the symptomsThis enables easier surgical or non0surgical management of the lesionThus medical management of apical lesions is used in conjunction with Surgical or non surgical management of apical lesions
Cellulitis-Cefazolin 1g iv Q8H7-10 days or cloxacillin500-1000mg po Q6H7-10 days
Acute osteomyelitis-Cefazolin 2g iv Q8H
Ludwigs angina-Clindamycin 600mg iv Q8H2-3 weeks
References J Conserv Dent 2010 Oct-Dec 13(4) 240-
245doi 1041030972070773384PMCID PMC3010029Nonsurgical management of periapical lesions Marina Fernandes and Ida de Ataide
Manual in maxillofacial surgery for senior house officers-Dental 2cmcvellore
DrVikram PerakathBDS
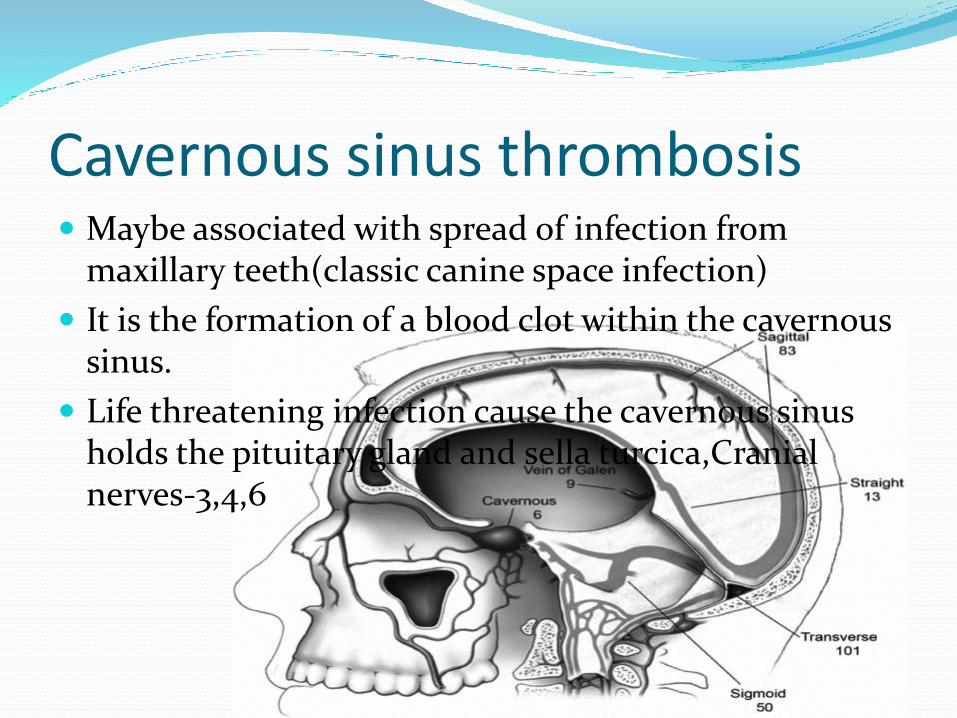
Proliferative Periostitis Form of chronic osteomyelitis with proliferative
periostitis
Periosteal reaction in which layers of reactive vital bone are formedproducing cortical expansion(onion skinning) The periosteum is not destroyedbut lifted upwhen bone is formed beneath its layers
Chronic focal sclerosingosteomyelitis AKA Condensing osteitis Localised area of bone sclerosis associated with apices
of non-vital teeth
Most frequent in children and young adults involving mandibular molarspremolars
No cortical expansion
Differential diagnosisOsseous Dysplasia and idiopathic osseosclerosis
Osteomyelitis Bacterial infection of bone secondary to
A)Odontogenic infection
B)Traumatic injury
C)Necrotising Ulcerative GingivitisNoma or cancrumoris
Predisposition to decreased vascularity of bone-PagetrsquosOsteopetrosisflorid cemento-osseous dysplasia
Chronic PathwayPeriapical granuloma
It is a misnomerit is not a granulomatous reaction
Mass of chronically inflamed granulation tissue at apex of non-vital teethdesigned to wall off bacterial invasion at apex
Associated with chronic apical periodontitis
Periapical cyst AKA apical periodontal cystradicular cyst
Inflammatory odontogenic cystinduced by cell rests of malassez(Hertwigs Epithelial Root Sheath remnants) proliferation
Radiolucency at periapex of non-vital teeth
To differentiate from a granulomait must be tested histologically
Management of apical lesions Non-surgical management Periapical lesions develop as
sequelae to pulp disease They often occur without any episode of acute pain and are discovered on routine radiographic examination It is accepted that all inflammatory periapicallesions should be initially treated with conservative nonsurgical procedures
Methods1The conservative root canal treatment
2decompression technique3active nonsurgical decompression technique4aspiration-irrigation technique
5 method using calcium hydroxide6 Lesion Sterilization and Repair Therapy and7the Apexum procedure
Case selectionThe current philosophy in the management of periapical lesions includes the initial use of nonsurgical methods When this treatment approach is not successful a surgical approach may be adoptedThe following factors must be considered while deciding on the management approach
Diagnosis of the lesionMany bone destroying lesions closely resemble endodontically related periapicallesions on radiographs Some of these nonendodontic lesions include ameloblastoma central fibroma giant cell lesions fibrous dysplasia central hemangioma primary malignancies metastatic neoplasms and inflammatory bone diseases
Proximity of the periapical lesion to adjacent vital teethWhen in proximity to a vital toothadopting a surgical approach may result in injury to the blood vessels and nerves of the adjacent teeth thereby compromising their vitality
Encroachment on anatomical structuresSurgery increases the risk of damage to the anatomic structures such as mental foramen inferior alveolar nerve Also the aspirationndashirrigation technique a nonsurgical method is not recommended where adjacent tissue spaces or sinus cavities are involved
Patient cooperation
Considerable pain or discomfort can be experienced by the patient during or after a surgical procedure A nonsurgical approach would be recommended for apprehensive and uncooperative patients
Obstructions in the root canal system
Ledges calcified canals separated instruments may prevent access to the apical foramen and may warrant a surgical approach in managing periapical lesions related to such teeth
Time involved for treatment
Enhanced healing kinetics are observed after performing apical surgery in teeth with periapical lesions
Cases refractory to nonsurgical management methods
Inflammatory apical true cysts and the presence of cholesterol crystals have been suggested as possible causes that prevent healing of periapical lesionsSurgery is recommended for such cases
METHODS FOR NONSURGICAL MANAGMENT OF PERIAPICAL LESIONS Conservative root canal treatment without adjunctive therapy
Instrumentation should be carried 1 mm beyond the apical foramen when a periapical lesion is evident on a radiograph This may cause transitory inflammation and ulceration of the epithelial lining resulting in resolution of the cyst
Decompression technique
The decompression technique involves placement of a drain into the lesion regular irrigation periodic length adjustment and maintenance of the drain for various periods of time
Active nonsurgical decompression technique
This technique uses the Endo-eze vacuum system to create a negative pressure which results in the decompression of large periapical lesions The high-volume suction aspirator is connected to a micro 22-gauge needle which is inserted in the root canal and activated for 20 minutes creating a negative pressure which results in aspiration of the exudate When the drainage partially stops the access cavity is closed with temporary cement which helps in maintaining bacterial control
Aspiration and irrigation technique
Hoen et al suggested aspiration of the cystic fluid from the periapcial lesion using a buccal palatal approach In this technique an 18-gauge needle attached to a 20 ml syringe is used to penetrate the buccal mucosa and aspirate the cystic fluid A second syringe filled with saline is then used to rinse the bony lesion The new needle is inserted through the buccal wound and passed out through the palatal tissue creating a pathway for the escape of the irrigant
Aspiration through the root canal technique
In this technique aspiration of the cystic fluid is done through the root canal by passing the aspirating needle through the apical foramen This technique eliminates the creation of buccal and palatal wounds as in the traditional aspirationndashirrigation technique This minimizes the discomfort that the patient may experience
However it is advisable not to use either aspirationndashirrigation or aspiration through the root canal techniques where adjacent tissue spaces or sinus cavities are involved when there is no fluid aspiration from the lesion or in infected periapicallesions
Method using calcium hydroxide
Calcium hydroxide is a widely used material in endodontic treatment because of its bactericidal effectsIt is thought to create favorable conditions for periapical repair and stimulate hard tissue formationSouza et al suggested that the action of calcium hydroxide beyond the apex may be four-fold (a) anti-inflammatory activity (b) neutralization of acid products (c) activation of the alkaline phosphatase and (d) antibacterial action
Lesion sterilization and repair therapy
lsquoLesion Sterilization and Tissue Repair (LSTR)rsquo therapy that uses a triple antibiotic paste of ciprofloxacin metronidazole and minocycline for disinfection of oral infectious lesions including dentinal pulpal and periradicular lesions Repair of damaged tissues can be expected if lesions are disinfectedMetronidazole is the first choice because it has a wide antibacterial spectrum against anaerobesHowever some bacteria are resistant to metronidazole and hence ciprofloxacin and minocycline are added to the mix
Apexum procedure
Surgical removal of the periapical chronically inflamed tissue allows a fresh blood clot to form thereby converting a chronic inflammatory lesion into a new granulation tissue where healing might proceed much fasterThe Apexumprocedure uses two sequential rotary devices the Apexum NiTi Ablator and Apexum PGA Ablator (Apexum Ltd Or Yehuda Israel) designed to extend beyond the apex and mince the periapical tissues on rotation in a low-speed handpiece followed by washing out the minced tissue
Surgical management of Apical lesions Apical lesions maybe managed surgically to reduce
healing and recovery time
Indicated for emergency cases
Incision and drainagewith antibiotic therapy of the lesionfollowed by RCT with apisectomy is the usual modality of surgical treatment of apical lesions
Medical Management of apical lesions Antibiotic therapy is used to treat minor apical
lesionsin order to relieve the symptomsThis enables easier surgical or non0surgical management of the lesionThus medical management of apical lesions is used in conjunction with Surgical or non surgical management of apical lesions
Cellulitis-Cefazolin 1g iv Q8H7-10 days or cloxacillin500-1000mg po Q6H7-10 days
Acute osteomyelitis-Cefazolin 2g iv Q8H
Ludwigs angina-Clindamycin 600mg iv Q8H2-3 weeks
References J Conserv Dent 2010 Oct-Dec 13(4) 240-
245doi 1041030972070773384PMCID PMC3010029Nonsurgical management of periapical lesions Marina Fernandes and Ida de Ataide
Manual in maxillofacial surgery for senior house officers-Dental 2cmcvellore
DrVikram PerakathBDS
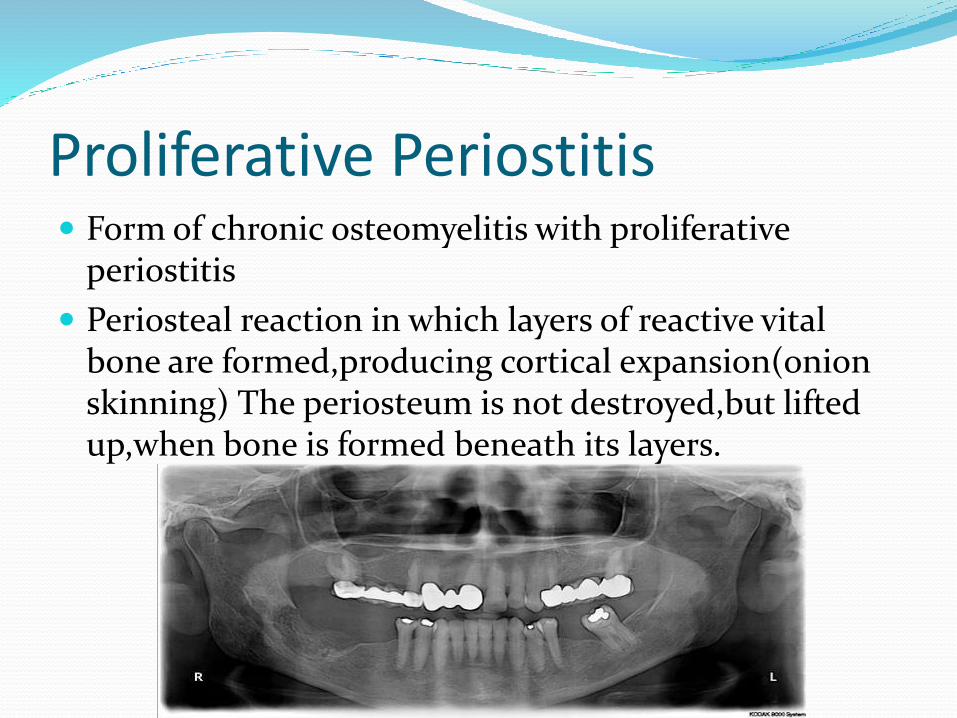
Chronic focal sclerosingosteomyelitis AKA Condensing osteitis Localised area of bone sclerosis associated with apices
of non-vital teeth
Most frequent in children and young adults involving mandibular molarspremolars
No cortical expansion
Differential diagnosisOsseous Dysplasia and idiopathic osseosclerosis
Osteomyelitis Bacterial infection of bone secondary to
A)Odontogenic infection
B)Traumatic injury
C)Necrotising Ulcerative GingivitisNoma or cancrumoris
Predisposition to decreased vascularity of bone-PagetrsquosOsteopetrosisflorid cemento-osseous dysplasia
Chronic PathwayPeriapical granuloma
It is a misnomerit is not a granulomatous reaction
Mass of chronically inflamed granulation tissue at apex of non-vital teethdesigned to wall off bacterial invasion at apex
Associated with chronic apical periodontitis
Periapical cyst AKA apical periodontal cystradicular cyst
Inflammatory odontogenic cystinduced by cell rests of malassez(Hertwigs Epithelial Root Sheath remnants) proliferation
Radiolucency at periapex of non-vital teeth
To differentiate from a granulomait must be tested histologically
Management of apical lesions Non-surgical management Periapical lesions develop as
sequelae to pulp disease They often occur without any episode of acute pain and are discovered on routine radiographic examination It is accepted that all inflammatory periapicallesions should be initially treated with conservative nonsurgical procedures
Methods1The conservative root canal treatment
2decompression technique3active nonsurgical decompression technique4aspiration-irrigation technique
5 method using calcium hydroxide6 Lesion Sterilization and Repair Therapy and7the Apexum procedure
Case selectionThe current philosophy in the management of periapical lesions includes the initial use of nonsurgical methods When this treatment approach is not successful a surgical approach may be adoptedThe following factors must be considered while deciding on the management approach
Diagnosis of the lesionMany bone destroying lesions closely resemble endodontically related periapicallesions on radiographs Some of these nonendodontic lesions include ameloblastoma central fibroma giant cell lesions fibrous dysplasia central hemangioma primary malignancies metastatic neoplasms and inflammatory bone diseases
Proximity of the periapical lesion to adjacent vital teethWhen in proximity to a vital toothadopting a surgical approach may result in injury to the blood vessels and nerves of the adjacent teeth thereby compromising their vitality
Encroachment on anatomical structuresSurgery increases the risk of damage to the anatomic structures such as mental foramen inferior alveolar nerve Also the aspirationndashirrigation technique a nonsurgical method is not recommended where adjacent tissue spaces or sinus cavities are involved
Patient cooperation
Considerable pain or discomfort can be experienced by the patient during or after a surgical procedure A nonsurgical approach would be recommended for apprehensive and uncooperative patients
Obstructions in the root canal system
Ledges calcified canals separated instruments may prevent access to the apical foramen and may warrant a surgical approach in managing periapical lesions related to such teeth
Time involved for treatment
Enhanced healing kinetics are observed after performing apical surgery in teeth with periapical lesions
Cases refractory to nonsurgical management methods
Inflammatory apical true cysts and the presence of cholesterol crystals have been suggested as possible causes that prevent healing of periapical lesionsSurgery is recommended for such cases
METHODS FOR NONSURGICAL MANAGMENT OF PERIAPICAL LESIONS Conservative root canal treatment without adjunctive therapy
Instrumentation should be carried 1 mm beyond the apical foramen when a periapical lesion is evident on a radiograph This may cause transitory inflammation and ulceration of the epithelial lining resulting in resolution of the cyst
Decompression technique
The decompression technique involves placement of a drain into the lesion regular irrigation periodic length adjustment and maintenance of the drain for various periods of time
Active nonsurgical decompression technique
This technique uses the Endo-eze vacuum system to create a negative pressure which results in the decompression of large periapical lesions The high-volume suction aspirator is connected to a micro 22-gauge needle which is inserted in the root canal and activated for 20 minutes creating a negative pressure which results in aspiration of the exudate When the drainage partially stops the access cavity is closed with temporary cement which helps in maintaining bacterial control
Aspiration and irrigation technique
Hoen et al suggested aspiration of the cystic fluid from the periapcial lesion using a buccal palatal approach In this technique an 18-gauge needle attached to a 20 ml syringe is used to penetrate the buccal mucosa and aspirate the cystic fluid A second syringe filled with saline is then used to rinse the bony lesion The new needle is inserted through the buccal wound and passed out through the palatal tissue creating a pathway for the escape of the irrigant
Aspiration through the root canal technique
In this technique aspiration of the cystic fluid is done through the root canal by passing the aspirating needle through the apical foramen This technique eliminates the creation of buccal and palatal wounds as in the traditional aspirationndashirrigation technique This minimizes the discomfort that the patient may experience
However it is advisable not to use either aspirationndashirrigation or aspiration through the root canal techniques where adjacent tissue spaces or sinus cavities are involved when there is no fluid aspiration from the lesion or in infected periapicallesions
Method using calcium hydroxide
Calcium hydroxide is a widely used material in endodontic treatment because of its bactericidal effectsIt is thought to create favorable conditions for periapical repair and stimulate hard tissue formationSouza et al suggested that the action of calcium hydroxide beyond the apex may be four-fold (a) anti-inflammatory activity (b) neutralization of acid products (c) activation of the alkaline phosphatase and (d) antibacterial action
Lesion sterilization and repair therapy
lsquoLesion Sterilization and Tissue Repair (LSTR)rsquo therapy that uses a triple antibiotic paste of ciprofloxacin metronidazole and minocycline for disinfection of oral infectious lesions including dentinal pulpal and periradicular lesions Repair of damaged tissues can be expected if lesions are disinfectedMetronidazole is the first choice because it has a wide antibacterial spectrum against anaerobesHowever some bacteria are resistant to metronidazole and hence ciprofloxacin and minocycline are added to the mix
Apexum procedure
Surgical removal of the periapical chronically inflamed tissue allows a fresh blood clot to form thereby converting a chronic inflammatory lesion into a new granulation tissue where healing might proceed much fasterThe Apexumprocedure uses two sequential rotary devices the Apexum NiTi Ablator and Apexum PGA Ablator (Apexum Ltd Or Yehuda Israel) designed to extend beyond the apex and mince the periapical tissues on rotation in a low-speed handpiece followed by washing out the minced tissue
Surgical management of Apical lesions Apical lesions maybe managed surgically to reduce
healing and recovery time
Indicated for emergency cases
Incision and drainagewith antibiotic therapy of the lesionfollowed by RCT with apisectomy is the usual modality of surgical treatment of apical lesions
Medical Management of apical lesions Antibiotic therapy is used to treat minor apical
lesionsin order to relieve the symptomsThis enables easier surgical or non0surgical management of the lesionThus medical management of apical lesions is used in conjunction with Surgical or non surgical management of apical lesions
Cellulitis-Cefazolin 1g iv Q8H7-10 days or cloxacillin500-1000mg po Q6H7-10 days
Acute osteomyelitis-Cefazolin 2g iv Q8H
Ludwigs angina-Clindamycin 600mg iv Q8H2-3 weeks
References J Conserv Dent 2010 Oct-Dec 13(4) 240-
245doi 1041030972070773384PMCID PMC3010029Nonsurgical management of periapical lesions Marina Fernandes and Ida de Ataide
Manual in maxillofacial surgery for senior house officers-Dental 2cmcvellore
DrVikram PerakathBDS
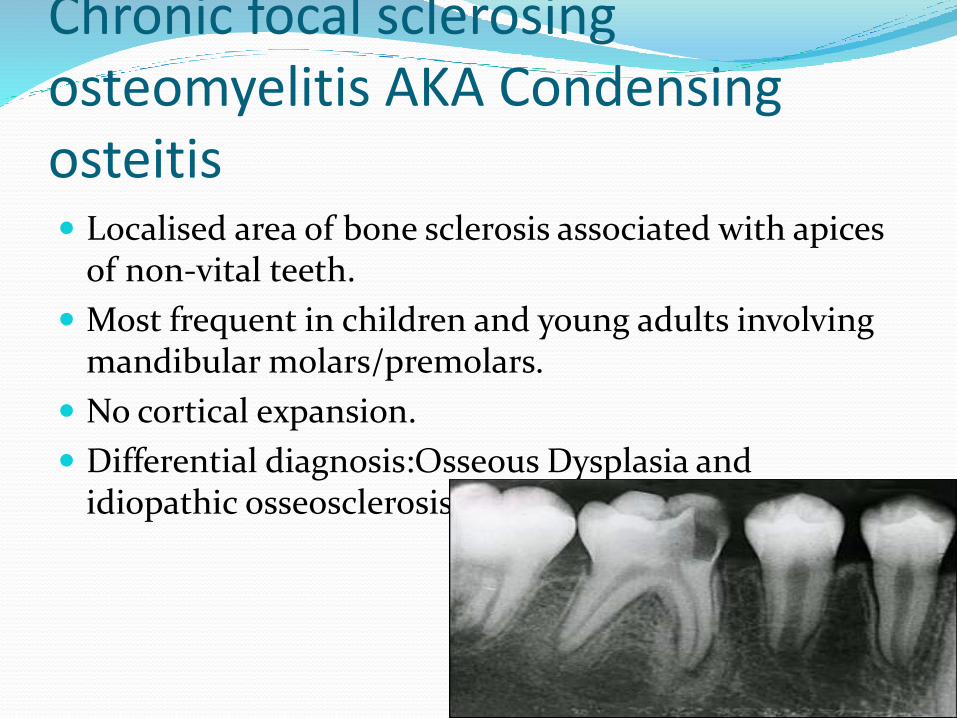
Osteomyelitis Bacterial infection of bone secondary to
A)Odontogenic infection
B)Traumatic injury
C)Necrotising Ulcerative GingivitisNoma or cancrumoris
Predisposition to decreased vascularity of bone-PagetrsquosOsteopetrosisflorid cemento-osseous dysplasia
Chronic PathwayPeriapical granuloma
It is a misnomerit is not a granulomatous reaction
Mass of chronically inflamed granulation tissue at apex of non-vital teethdesigned to wall off bacterial invasion at apex
Associated with chronic apical periodontitis
Periapical cyst AKA apical periodontal cystradicular cyst
Inflammatory odontogenic cystinduced by cell rests of malassez(Hertwigs Epithelial Root Sheath remnants) proliferation
Radiolucency at periapex of non-vital teeth
To differentiate from a granulomait must be tested histologically
Management of apical lesions Non-surgical management Periapical lesions develop as
sequelae to pulp disease They often occur without any episode of acute pain and are discovered on routine radiographic examination It is accepted that all inflammatory periapicallesions should be initially treated with conservative nonsurgical procedures
Methods1The conservative root canal treatment
2decompression technique3active nonsurgical decompression technique4aspiration-irrigation technique
5 method using calcium hydroxide6 Lesion Sterilization and Repair Therapy and7the Apexum procedure
Case selectionThe current philosophy in the management of periapical lesions includes the initial use of nonsurgical methods When this treatment approach is not successful a surgical approach may be adoptedThe following factors must be considered while deciding on the management approach
Diagnosis of the lesionMany bone destroying lesions closely resemble endodontically related periapicallesions on radiographs Some of these nonendodontic lesions include ameloblastoma central fibroma giant cell lesions fibrous dysplasia central hemangioma primary malignancies metastatic neoplasms and inflammatory bone diseases
Proximity of the periapical lesion to adjacent vital teethWhen in proximity to a vital toothadopting a surgical approach may result in injury to the blood vessels and nerves of the adjacent teeth thereby compromising their vitality
Encroachment on anatomical structuresSurgery increases the risk of damage to the anatomic structures such as mental foramen inferior alveolar nerve Also the aspirationndashirrigation technique a nonsurgical method is not recommended where adjacent tissue spaces or sinus cavities are involved
Patient cooperation
Considerable pain or discomfort can be experienced by the patient during or after a surgical procedure A nonsurgical approach would be recommended for apprehensive and uncooperative patients
Obstructions in the root canal system
Ledges calcified canals separated instruments may prevent access to the apical foramen and may warrant a surgical approach in managing periapical lesions related to such teeth
Time involved for treatment
Enhanced healing kinetics are observed after performing apical surgery in teeth with periapical lesions
Cases refractory to nonsurgical management methods
Inflammatory apical true cysts and the presence of cholesterol crystals have been suggested as possible causes that prevent healing of periapical lesionsSurgery is recommended for such cases
METHODS FOR NONSURGICAL MANAGMENT OF PERIAPICAL LESIONS Conservative root canal treatment without adjunctive therapy
Instrumentation should be carried 1 mm beyond the apical foramen when a periapical lesion is evident on a radiograph This may cause transitory inflammation and ulceration of the epithelial lining resulting in resolution of the cyst
Decompression technique
The decompression technique involves placement of a drain into the lesion regular irrigation periodic length adjustment and maintenance of the drain for various periods of time
Active nonsurgical decompression technique
This technique uses the Endo-eze vacuum system to create a negative pressure which results in the decompression of large periapical lesions The high-volume suction aspirator is connected to a micro 22-gauge needle which is inserted in the root canal and activated for 20 minutes creating a negative pressure which results in aspiration of the exudate When the drainage partially stops the access cavity is closed with temporary cement which helps in maintaining bacterial control
Aspiration and irrigation technique
Hoen et al suggested aspiration of the cystic fluid from the periapcial lesion using a buccal palatal approach In this technique an 18-gauge needle attached to a 20 ml syringe is used to penetrate the buccal mucosa and aspirate the cystic fluid A second syringe filled with saline is then used to rinse the bony lesion The new needle is inserted through the buccal wound and passed out through the palatal tissue creating a pathway for the escape of the irrigant
Aspiration through the root canal technique
In this technique aspiration of the cystic fluid is done through the root canal by passing the aspirating needle through the apical foramen This technique eliminates the creation of buccal and palatal wounds as in the traditional aspirationndashirrigation technique This minimizes the discomfort that the patient may experience
However it is advisable not to use either aspirationndashirrigation or aspiration through the root canal techniques where adjacent tissue spaces or sinus cavities are involved when there is no fluid aspiration from the lesion or in infected periapicallesions
Method using calcium hydroxide
Calcium hydroxide is a widely used material in endodontic treatment because of its bactericidal effectsIt is thought to create favorable conditions for periapical repair and stimulate hard tissue formationSouza et al suggested that the action of calcium hydroxide beyond the apex may be four-fold (a) anti-inflammatory activity (b) neutralization of acid products (c) activation of the alkaline phosphatase and (d) antibacterial action
Lesion sterilization and repair therapy
lsquoLesion Sterilization and Tissue Repair (LSTR)rsquo therapy that uses a triple antibiotic paste of ciprofloxacin metronidazole and minocycline for disinfection of oral infectious lesions including dentinal pulpal and periradicular lesions Repair of damaged tissues can be expected if lesions are disinfectedMetronidazole is the first choice because it has a wide antibacterial spectrum against anaerobesHowever some bacteria are resistant to metronidazole and hence ciprofloxacin and minocycline are added to the mix
Apexum procedure
Surgical removal of the periapical chronically inflamed tissue allows a fresh blood clot to form thereby converting a chronic inflammatory lesion into a new granulation tissue where healing might proceed much fasterThe Apexumprocedure uses two sequential rotary devices the Apexum NiTi Ablator and Apexum PGA Ablator (Apexum Ltd Or Yehuda Israel) designed to extend beyond the apex and mince the periapical tissues on rotation in a low-speed handpiece followed by washing out the minced tissue
Surgical management of Apical lesions Apical lesions maybe managed surgically to reduce
healing and recovery time
Indicated for emergency cases
Incision and drainagewith antibiotic therapy of the lesionfollowed by RCT with apisectomy is the usual modality of surgical treatment of apical lesions
Medical Management of apical lesions Antibiotic therapy is used to treat minor apical
lesionsin order to relieve the symptomsThis enables easier surgical or non0surgical management of the lesionThus medical management of apical lesions is used in conjunction with Surgical or non surgical management of apical lesions
Cellulitis-Cefazolin 1g iv Q8H7-10 days or cloxacillin500-1000mg po Q6H7-10 days
Acute osteomyelitis-Cefazolin 2g iv Q8H
Ludwigs angina-Clindamycin 600mg iv Q8H2-3 weeks
References J Conserv Dent 2010 Oct-Dec 13(4) 240-
245doi 1041030972070773384PMCID PMC3010029Nonsurgical management of periapical lesions Marina Fernandes and Ida de Ataide
Manual in maxillofacial surgery for senior house officers-Dental 2cmcvellore
DrVikram PerakathBDS
Chronic PathwayPeriapical granuloma
It is a misnomerit is not a granulomatous reaction
Mass of chronically inflamed granulation tissue at apex of non-vital teethdesigned to wall off bacterial invasion at apex
Associated with chronic apical periodontitis
Periapical cyst AKA apical periodontal cystradicular cyst
Inflammatory odontogenic cystinduced by cell rests of malassez(Hertwigs Epithelial Root Sheath remnants) proliferation
Radiolucency at periapex of non-vital teeth
To differentiate from a granulomait must be tested histologically
Management of apical lesions Non-surgical management Periapical lesions develop as
sequelae to pulp disease They often occur without any episode of acute pain and are discovered on routine radiographic examination It is accepted that all inflammatory periapicallesions should be initially treated with conservative nonsurgical procedures
Methods1The conservative root canal treatment
2decompression technique3active nonsurgical decompression technique4aspiration-irrigation technique
5 method using calcium hydroxide6 Lesion Sterilization and Repair Therapy and7the Apexum procedure
Case selectionThe current philosophy in the management of periapical lesions includes the initial use of nonsurgical methods When this treatment approach is not successful a surgical approach may be adoptedThe following factors must be considered while deciding on the management approach
Diagnosis of the lesionMany bone destroying lesions closely resemble endodontically related periapicallesions on radiographs Some of these nonendodontic lesions include ameloblastoma central fibroma giant cell lesions fibrous dysplasia central hemangioma primary malignancies metastatic neoplasms and inflammatory bone diseases
Proximity of the periapical lesion to adjacent vital teethWhen in proximity to a vital toothadopting a surgical approach may result in injury to the blood vessels and nerves of the adjacent teeth thereby compromising their vitality
Encroachment on anatomical structuresSurgery increases the risk of damage to the anatomic structures such as mental foramen inferior alveolar nerve Also the aspirationndashirrigation technique a nonsurgical method is not recommended where adjacent tissue spaces or sinus cavities are involved
Patient cooperation
Considerable pain or discomfort can be experienced by the patient during or after a surgical procedure A nonsurgical approach would be recommended for apprehensive and uncooperative patients
Obstructions in the root canal system
Ledges calcified canals separated instruments may prevent access to the apical foramen and may warrant a surgical approach in managing periapical lesions related to such teeth
Time involved for treatment
Enhanced healing kinetics are observed after performing apical surgery in teeth with periapical lesions
Cases refractory to nonsurgical management methods
Inflammatory apical true cysts and the presence of cholesterol crystals have been suggested as possible causes that prevent healing of periapical lesionsSurgery is recommended for such cases
METHODS FOR NONSURGICAL MANAGMENT OF PERIAPICAL LESIONS Conservative root canal treatment without adjunctive therapy
Instrumentation should be carried 1 mm beyond the apical foramen when a periapical lesion is evident on a radiograph This may cause transitory inflammation and ulceration of the epithelial lining resulting in resolution of the cyst
Decompression technique
The decompression technique involves placement of a drain into the lesion regular irrigation periodic length adjustment and maintenance of the drain for various periods of time
Active nonsurgical decompression technique
This technique uses the Endo-eze vacuum system to create a negative pressure which results in the decompression of large periapical lesions The high-volume suction aspirator is connected to a micro 22-gauge needle which is inserted in the root canal and activated for 20 minutes creating a negative pressure which results in aspiration of the exudate When the drainage partially stops the access cavity is closed with temporary cement which helps in maintaining bacterial control
Aspiration and irrigation technique
Hoen et al suggested aspiration of the cystic fluid from the periapcial lesion using a buccal palatal approach In this technique an 18-gauge needle attached to a 20 ml syringe is used to penetrate the buccal mucosa and aspirate the cystic fluid A second syringe filled with saline is then used to rinse the bony lesion The new needle is inserted through the buccal wound and passed out through the palatal tissue creating a pathway for the escape of the irrigant
Aspiration through the root canal technique
In this technique aspiration of the cystic fluid is done through the root canal by passing the aspirating needle through the apical foramen This technique eliminates the creation of buccal and palatal wounds as in the traditional aspirationndashirrigation technique This minimizes the discomfort that the patient may experience
However it is advisable not to use either aspirationndashirrigation or aspiration through the root canal techniques where adjacent tissue spaces or sinus cavities are involved when there is no fluid aspiration from the lesion or in infected periapicallesions
Method using calcium hydroxide
Calcium hydroxide is a widely used material in endodontic treatment because of its bactericidal effectsIt is thought to create favorable conditions for periapical repair and stimulate hard tissue formationSouza et al suggested that the action of calcium hydroxide beyond the apex may be four-fold (a) anti-inflammatory activity (b) neutralization of acid products (c) activation of the alkaline phosphatase and (d) antibacterial action
Lesion sterilization and repair therapy
lsquoLesion Sterilization and Tissue Repair (LSTR)rsquo therapy that uses a triple antibiotic paste of ciprofloxacin metronidazole and minocycline for disinfection of oral infectious lesions including dentinal pulpal and periradicular lesions Repair of damaged tissues can be expected if lesions are disinfectedMetronidazole is the first choice because it has a wide antibacterial spectrum against anaerobesHowever some bacteria are resistant to metronidazole and hence ciprofloxacin and minocycline are added to the mix
Apexum procedure
Surgical removal of the periapical chronically inflamed tissue allows a fresh blood clot to form thereby converting a chronic inflammatory lesion into a new granulation tissue where healing might proceed much fasterThe Apexumprocedure uses two sequential rotary devices the Apexum NiTi Ablator and Apexum PGA Ablator (Apexum Ltd Or Yehuda Israel) designed to extend beyond the apex and mince the periapical tissues on rotation in a low-speed handpiece followed by washing out the minced tissue
Surgical management of Apical lesions Apical lesions maybe managed surgically to reduce
healing and recovery time
Indicated for emergency cases
Incision and drainagewith antibiotic therapy of the lesionfollowed by RCT with apisectomy is the usual modality of surgical treatment of apical lesions
Medical Management of apical lesions Antibiotic therapy is used to treat minor apical
lesionsin order to relieve the symptomsThis enables easier surgical or non0surgical management of the lesionThus medical management of apical lesions is used in conjunction with Surgical or non surgical management of apical lesions
Cellulitis-Cefazolin 1g iv Q8H7-10 days or cloxacillin500-1000mg po Q6H7-10 days
Acute osteomyelitis-Cefazolin 2g iv Q8H
Ludwigs angina-Clindamycin 600mg iv Q8H2-3 weeks
References J Conserv Dent 2010 Oct-Dec 13(4) 240-
245doi 1041030972070773384PMCID PMC3010029Nonsurgical management of periapical lesions Marina Fernandes and Ida de Ataide
Manual in maxillofacial surgery for senior house officers-Dental 2cmcvellore
DrVikram PerakathBDS
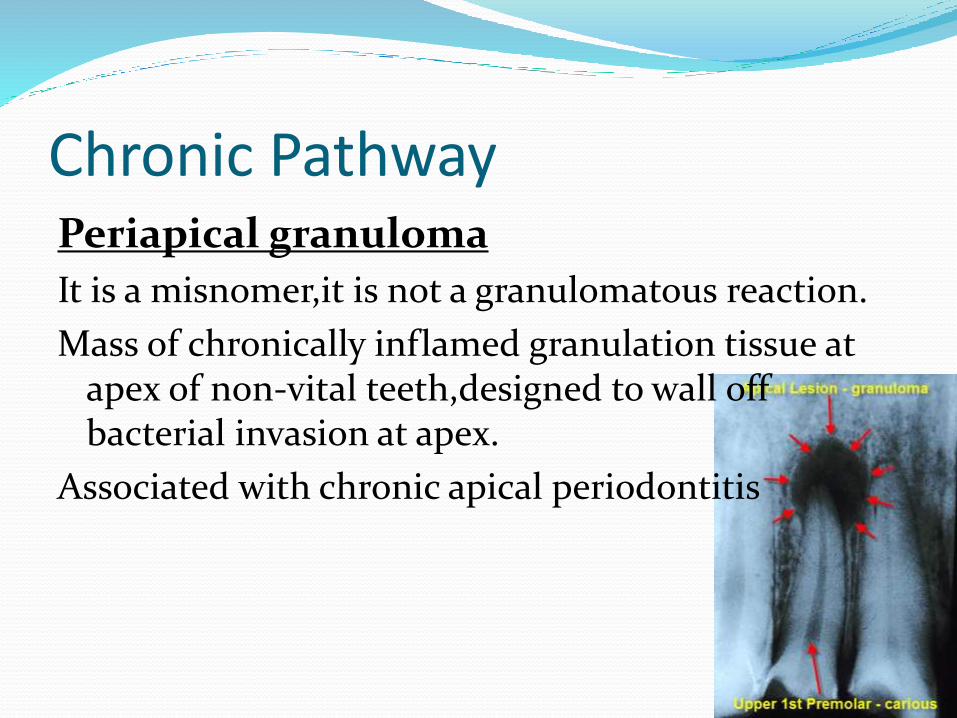
Periapical cyst AKA apical periodontal cystradicular cyst
Inflammatory odontogenic cystinduced by cell rests of malassez(Hertwigs Epithelial Root Sheath remnants) proliferation
Radiolucency at periapex of non-vital teeth
To differentiate from a granulomait must be tested histologically
Management of apical lesions Non-surgical management Periapical lesions develop as
sequelae to pulp disease They often occur without any episode of acute pain and are discovered on routine radiographic examination It is accepted that all inflammatory periapicallesions should be initially treated with conservative nonsurgical procedures
Methods1The conservative root canal treatment
2decompression technique3active nonsurgical decompression technique4aspiration-irrigation technique
5 method using calcium hydroxide6 Lesion Sterilization and Repair Therapy and7the Apexum procedure
Case selectionThe current philosophy in the management of periapical lesions includes the initial use of nonsurgical methods When this treatment approach is not successful a surgical approach may be adoptedThe following factors must be considered while deciding on the management approach
Diagnosis of the lesionMany bone destroying lesions closely resemble endodontically related periapicallesions on radiographs Some of these nonendodontic lesions include ameloblastoma central fibroma giant cell lesions fibrous dysplasia central hemangioma primary malignancies metastatic neoplasms and inflammatory bone diseases
Proximity of the periapical lesion to adjacent vital teethWhen in proximity to a vital toothadopting a surgical approach may result in injury to the blood vessels and nerves of the adjacent teeth thereby compromising their vitality
Encroachment on anatomical structuresSurgery increases the risk of damage to the anatomic structures such as mental foramen inferior alveolar nerve Also the aspirationndashirrigation technique a nonsurgical method is not recommended where adjacent tissue spaces or sinus cavities are involved
Patient cooperation
Considerable pain or discomfort can be experienced by the patient during or after a surgical procedure A nonsurgical approach would be recommended for apprehensive and uncooperative patients
Obstructions in the root canal system
Ledges calcified canals separated instruments may prevent access to the apical foramen and may warrant a surgical approach in managing periapical lesions related to such teeth
Time involved for treatment
Enhanced healing kinetics are observed after performing apical surgery in teeth with periapical lesions
Cases refractory to nonsurgical management methods
Inflammatory apical true cysts and the presence of cholesterol crystals have been suggested as possible causes that prevent healing of periapical lesionsSurgery is recommended for such cases
METHODS FOR NONSURGICAL MANAGMENT OF PERIAPICAL LESIONS Conservative root canal treatment without adjunctive therapy
Instrumentation should be carried 1 mm beyond the apical foramen when a periapical lesion is evident on a radiograph This may cause transitory inflammation and ulceration of the epithelial lining resulting in resolution of the cyst
Decompression technique
The decompression technique involves placement of a drain into the lesion regular irrigation periodic length adjustment and maintenance of the drain for various periods of time
Active nonsurgical decompression technique
This technique uses the Endo-eze vacuum system to create a negative pressure which results in the decompression of large periapical lesions The high-volume suction aspirator is connected to a micro 22-gauge needle which is inserted in the root canal and activated for 20 minutes creating a negative pressure which results in aspiration of the exudate When the drainage partially stops the access cavity is closed with temporary cement which helps in maintaining bacterial control
Aspiration and irrigation technique
Hoen et al suggested aspiration of the cystic fluid from the periapcial lesion using a buccal palatal approach In this technique an 18-gauge needle attached to a 20 ml syringe is used to penetrate the buccal mucosa and aspirate the cystic fluid A second syringe filled with saline is then used to rinse the bony lesion The new needle is inserted through the buccal wound and passed out through the palatal tissue creating a pathway for the escape of the irrigant
Aspiration through the root canal technique
In this technique aspiration of the cystic fluid is done through the root canal by passing the aspirating needle through the apical foramen This technique eliminates the creation of buccal and palatal wounds as in the traditional aspirationndashirrigation technique This minimizes the discomfort that the patient may experience
However it is advisable not to use either aspirationndashirrigation or aspiration through the root canal techniques where adjacent tissue spaces or sinus cavities are involved when there is no fluid aspiration from the lesion or in infected periapicallesions
Method using calcium hydroxide
Calcium hydroxide is a widely used material in endodontic treatment because of its bactericidal effectsIt is thought to create favorable conditions for periapical repair and stimulate hard tissue formationSouza et al suggested that the action of calcium hydroxide beyond the apex may be four-fold (a) anti-inflammatory activity (b) neutralization of acid products (c) activation of the alkaline phosphatase and (d) antibacterial action
Lesion sterilization and repair therapy
lsquoLesion Sterilization and Tissue Repair (LSTR)rsquo therapy that uses a triple antibiotic paste of ciprofloxacin metronidazole and minocycline for disinfection of oral infectious lesions including dentinal pulpal and periradicular lesions Repair of damaged tissues can be expected if lesions are disinfectedMetronidazole is the first choice because it has a wide antibacterial spectrum against anaerobesHowever some bacteria are resistant to metronidazole and hence ciprofloxacin and minocycline are added to the mix
Apexum procedure
Surgical removal of the periapical chronically inflamed tissue allows a fresh blood clot to form thereby converting a chronic inflammatory lesion into a new granulation tissue where healing might proceed much fasterThe Apexumprocedure uses two sequential rotary devices the Apexum NiTi Ablator and Apexum PGA Ablator (Apexum Ltd Or Yehuda Israel) designed to extend beyond the apex and mince the periapical tissues on rotation in a low-speed handpiece followed by washing out the minced tissue
Surgical management of Apical lesions Apical lesions maybe managed surgically to reduce
healing and recovery time
Indicated for emergency cases
Incision and drainagewith antibiotic therapy of the lesionfollowed by RCT with apisectomy is the usual modality of surgical treatment of apical lesions
Medical Management of apical lesions Antibiotic therapy is used to treat minor apical
lesionsin order to relieve the symptomsThis enables easier surgical or non0surgical management of the lesionThus medical management of apical lesions is used in conjunction with Surgical or non surgical management of apical lesions
Cellulitis-Cefazolin 1g iv Q8H7-10 days or cloxacillin500-1000mg po Q6H7-10 days
Acute osteomyelitis-Cefazolin 2g iv Q8H
Ludwigs angina-Clindamycin 600mg iv Q8H2-3 weeks
References J Conserv Dent 2010 Oct-Dec 13(4) 240-
245doi 1041030972070773384PMCID PMC3010029Nonsurgical management of periapical lesions Marina Fernandes and Ida de Ataide
Manual in maxillofacial surgery for senior house officers-Dental 2cmcvellore
DrVikram PerakathBDS
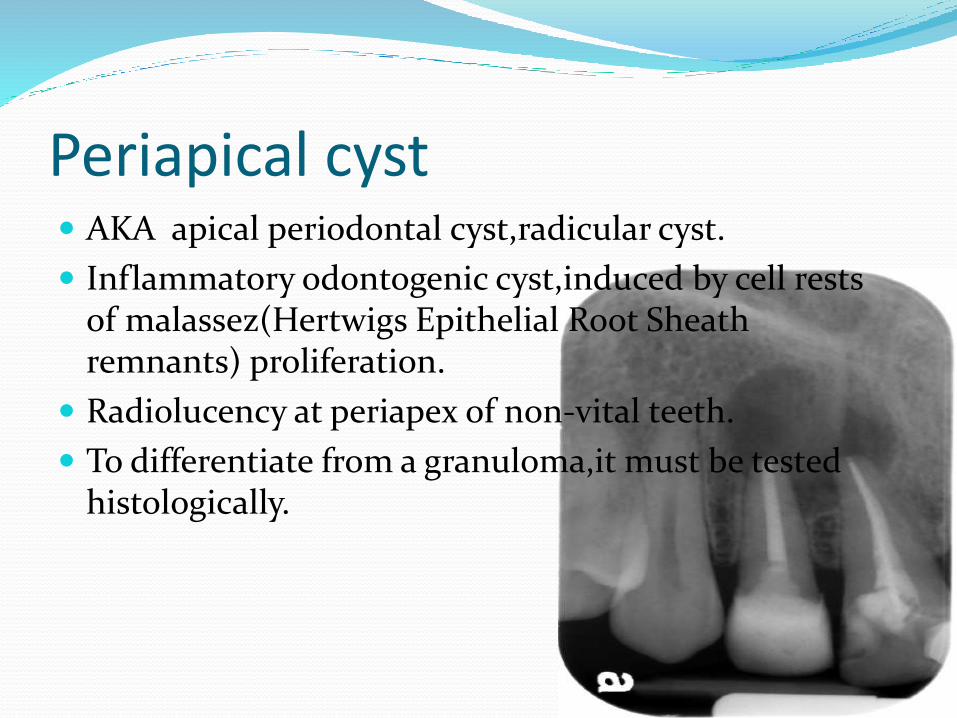
Management of apical lesions Non-surgical management Periapical lesions develop as
sequelae to pulp disease They often occur without any episode of acute pain and are discovered on routine radiographic examination It is accepted that all inflammatory periapicallesions should be initially treated with conservative nonsurgical procedures
Methods1The conservative root canal treatment
2decompression technique3active nonsurgical decompression technique4aspiration-irrigation technique
5 method using calcium hydroxide6 Lesion Sterilization and Repair Therapy and7the Apexum procedure
Case selectionThe current philosophy in the management of periapical lesions includes the initial use of nonsurgical methods When this treatment approach is not successful a surgical approach may be adoptedThe following factors must be considered while deciding on the management approach
Diagnosis of the lesionMany bone destroying lesions closely resemble endodontically related periapicallesions on radiographs Some of these nonendodontic lesions include ameloblastoma central fibroma giant cell lesions fibrous dysplasia central hemangioma primary malignancies metastatic neoplasms and inflammatory bone diseases
Proximity of the periapical lesion to adjacent vital teethWhen in proximity to a vital toothadopting a surgical approach may result in injury to the blood vessels and nerves of the adjacent teeth thereby compromising their vitality
Encroachment on anatomical structuresSurgery increases the risk of damage to the anatomic structures such as mental foramen inferior alveolar nerve Also the aspirationndashirrigation technique a nonsurgical method is not recommended where adjacent tissue spaces or sinus cavities are involved
Patient cooperation
Considerable pain or discomfort can be experienced by the patient during or after a surgical procedure A nonsurgical approach would be recommended for apprehensive and uncooperative patients
Obstructions in the root canal system
Ledges calcified canals separated instruments may prevent access to the apical foramen and may warrant a surgical approach in managing periapical lesions related to such teeth
Time involved for treatment
Enhanced healing kinetics are observed after performing apical surgery in teeth with periapical lesions
Cases refractory to nonsurgical management methods
Inflammatory apical true cysts and the presence of cholesterol crystals have been suggested as possible causes that prevent healing of periapical lesionsSurgery is recommended for such cases
METHODS FOR NONSURGICAL MANAGMENT OF PERIAPICAL LESIONS Conservative root canal treatment without adjunctive therapy
Instrumentation should be carried 1 mm beyond the apical foramen when a periapical lesion is evident on a radiograph This may cause transitory inflammation and ulceration of the epithelial lining resulting in resolution of the cyst
Decompression technique
The decompression technique involves placement of a drain into the lesion regular irrigation periodic length adjustment and maintenance of the drain for various periods of time
Active nonsurgical decompression technique
This technique uses the Endo-eze vacuum system to create a negative pressure which results in the decompression of large periapical lesions The high-volume suction aspirator is connected to a micro 22-gauge needle which is inserted in the root canal and activated for 20 minutes creating a negative pressure which results in aspiration of the exudate When the drainage partially stops the access cavity is closed with temporary cement which helps in maintaining bacterial control
Aspiration and irrigation technique
Hoen et al suggested aspiration of the cystic fluid from the periapcial lesion using a buccal palatal approach In this technique an 18-gauge needle attached to a 20 ml syringe is used to penetrate the buccal mucosa and aspirate the cystic fluid A second syringe filled with saline is then used to rinse the bony lesion The new needle is inserted through the buccal wound and passed out through the palatal tissue creating a pathway for the escape of the irrigant
Aspiration through the root canal technique
In this technique aspiration of the cystic fluid is done through the root canal by passing the aspirating needle through the apical foramen This technique eliminates the creation of buccal and palatal wounds as in the traditional aspirationndashirrigation technique This minimizes the discomfort that the patient may experience
However it is advisable not to use either aspirationndashirrigation or aspiration through the root canal techniques where adjacent tissue spaces or sinus cavities are involved when there is no fluid aspiration from the lesion or in infected periapicallesions
Method using calcium hydroxide
Calcium hydroxide is a widely used material in endodontic treatment because of its bactericidal effectsIt is thought to create favorable conditions for periapical repair and stimulate hard tissue formationSouza et al suggested that the action of calcium hydroxide beyond the apex may be four-fold (a) anti-inflammatory activity (b) neutralization of acid products (c) activation of the alkaline phosphatase and (d) antibacterial action
Lesion sterilization and repair therapy
lsquoLesion Sterilization and Tissue Repair (LSTR)rsquo therapy that uses a triple antibiotic paste of ciprofloxacin metronidazole and minocycline for disinfection of oral infectious lesions including dentinal pulpal and periradicular lesions Repair of damaged tissues can be expected if lesions are disinfectedMetronidazole is the first choice because it has a wide antibacterial spectrum against anaerobesHowever some bacteria are resistant to metronidazole and hence ciprofloxacin and minocycline are added to the mix
Apexum procedure
Surgical removal of the periapical chronically inflamed tissue allows a fresh blood clot to form thereby converting a chronic inflammatory lesion into a new granulation tissue where healing might proceed much fasterThe Apexumprocedure uses two sequential rotary devices the Apexum NiTi Ablator and Apexum PGA Ablator (Apexum Ltd Or Yehuda Israel) designed to extend beyond the apex and mince the periapical tissues on rotation in a low-speed handpiece followed by washing out the minced tissue
Surgical management of Apical lesions Apical lesions maybe managed surgically to reduce
healing and recovery time
Indicated for emergency cases
Incision and drainagewith antibiotic therapy of the lesionfollowed by RCT with apisectomy is the usual modality of surgical treatment of apical lesions
Medical Management of apical lesions Antibiotic therapy is used to treat minor apical
lesionsin order to relieve the symptomsThis enables easier surgical or non0surgical management of the lesionThus medical management of apical lesions is used in conjunction with Surgical or non surgical management of apical lesions
Cellulitis-Cefazolin 1g iv Q8H7-10 days or cloxacillin500-1000mg po Q6H7-10 days
Acute osteomyelitis-Cefazolin 2g iv Q8H
Ludwigs angina-Clindamycin 600mg iv Q8H2-3 weeks
References J Conserv Dent 2010 Oct-Dec 13(4) 240-
245doi 1041030972070773384PMCID PMC3010029Nonsurgical management of periapical lesions Marina Fernandes and Ida de Ataide
Manual in maxillofacial surgery for senior house officers-Dental 2cmcvellore
DrVikram PerakathBDS
Case selectionThe current philosophy in the management of periapical lesions includes the initial use of nonsurgical methods When this treatment approach is not successful a surgical approach may be adoptedThe following factors must be considered while deciding on the management approach
Diagnosis of the lesionMany bone destroying lesions closely resemble endodontically related periapicallesions on radiographs Some of these nonendodontic lesions include ameloblastoma central fibroma giant cell lesions fibrous dysplasia central hemangioma primary malignancies metastatic neoplasms and inflammatory bone diseases
Proximity of the periapical lesion to adjacent vital teethWhen in proximity to a vital toothadopting a surgical approach may result in injury to the blood vessels and nerves of the adjacent teeth thereby compromising their vitality
Encroachment on anatomical structuresSurgery increases the risk of damage to the anatomic structures such as mental foramen inferior alveolar nerve Also the aspirationndashirrigation technique a nonsurgical method is not recommended where adjacent tissue spaces or sinus cavities are involved
Patient cooperation
Considerable pain or discomfort can be experienced by the patient during or after a surgical procedure A nonsurgical approach would be recommended for apprehensive and uncooperative patients
Obstructions in the root canal system
Ledges calcified canals separated instruments may prevent access to the apical foramen and may warrant a surgical approach in managing periapical lesions related to such teeth
Time involved for treatment
Enhanced healing kinetics are observed after performing apical surgery in teeth with periapical lesions
Cases refractory to nonsurgical management methods
Inflammatory apical true cysts and the presence of cholesterol crystals have been suggested as possible causes that prevent healing of periapical lesionsSurgery is recommended for such cases
METHODS FOR NONSURGICAL MANAGMENT OF PERIAPICAL LESIONS Conservative root canal treatment without adjunctive therapy
Instrumentation should be carried 1 mm beyond the apical foramen when a periapical lesion is evident on a radiograph This may cause transitory inflammation and ulceration of the epithelial lining resulting in resolution of the cyst
Decompression technique
The decompression technique involves placement of a drain into the lesion regular irrigation periodic length adjustment and maintenance of the drain for various periods of time
Active nonsurgical decompression technique
This technique uses the Endo-eze vacuum system to create a negative pressure which results in the decompression of large periapical lesions The high-volume suction aspirator is connected to a micro 22-gauge needle which is inserted in the root canal and activated for 20 minutes creating a negative pressure which results in aspiration of the exudate When the drainage partially stops the access cavity is closed with temporary cement which helps in maintaining bacterial control
Aspiration and irrigation technique
Hoen et al suggested aspiration of the cystic fluid from the periapcial lesion using a buccal palatal approach In this technique an 18-gauge needle attached to a 20 ml syringe is used to penetrate the buccal mucosa and aspirate the cystic fluid A second syringe filled with saline is then used to rinse the bony lesion The new needle is inserted through the buccal wound and passed out through the palatal tissue creating a pathway for the escape of the irrigant
Aspiration through the root canal technique
In this technique aspiration of the cystic fluid is done through the root canal by passing the aspirating needle through the apical foramen This technique eliminates the creation of buccal and palatal wounds as in the traditional aspirationndashirrigation technique This minimizes the discomfort that the patient may experience
However it is advisable not to use either aspirationndashirrigation or aspiration through the root canal techniques where adjacent tissue spaces or sinus cavities are involved when there is no fluid aspiration from the lesion or in infected periapicallesions
Method using calcium hydroxide
Calcium hydroxide is a widely used material in endodontic treatment because of its bactericidal effectsIt is thought to create favorable conditions for periapical repair and stimulate hard tissue formationSouza et al suggested that the action of calcium hydroxide beyond the apex may be four-fold (a) anti-inflammatory activity (b) neutralization of acid products (c) activation of the alkaline phosphatase and (d) antibacterial action
Lesion sterilization and repair therapy
lsquoLesion Sterilization and Tissue Repair (LSTR)rsquo therapy that uses a triple antibiotic paste of ciprofloxacin metronidazole and minocycline for disinfection of oral infectious lesions including dentinal pulpal and periradicular lesions Repair of damaged tissues can be expected if lesions are disinfectedMetronidazole is the first choice because it has a wide antibacterial spectrum against anaerobesHowever some bacteria are resistant to metronidazole and hence ciprofloxacin and minocycline are added to the mix
Apexum procedure
Surgical removal of the periapical chronically inflamed tissue allows a fresh blood clot to form thereby converting a chronic inflammatory lesion into a new granulation tissue where healing might proceed much fasterThe Apexumprocedure uses two sequential rotary devices the Apexum NiTi Ablator and Apexum PGA Ablator (Apexum Ltd Or Yehuda Israel) designed to extend beyond the apex and mince the periapical tissues on rotation in a low-speed handpiece followed by washing out the minced tissue
Surgical management of Apical lesions Apical lesions maybe managed surgically to reduce
healing and recovery time
Indicated for emergency cases
Incision and drainagewith antibiotic therapy of the lesionfollowed by RCT with apisectomy is the usual modality of surgical treatment of apical lesions
Medical Management of apical lesions Antibiotic therapy is used to treat minor apical
lesionsin order to relieve the symptomsThis enables easier surgical or non0surgical management of the lesionThus medical management of apical lesions is used in conjunction with Surgical or non surgical management of apical lesions
Cellulitis-Cefazolin 1g iv Q8H7-10 days or cloxacillin500-1000mg po Q6H7-10 days
Acute osteomyelitis-Cefazolin 2g iv Q8H
Ludwigs angina-Clindamycin 600mg iv Q8H2-3 weeks
References J Conserv Dent 2010 Oct-Dec 13(4) 240-
245doi 1041030972070773384PMCID PMC3010029Nonsurgical management of periapical lesions Marina Fernandes and Ida de Ataide
Manual in maxillofacial surgery for senior house officers-Dental 2cmcvellore
DrVikram PerakathBDS
Patient cooperation
Considerable pain or discomfort can be experienced by the patient during or after a surgical procedure A nonsurgical approach would be recommended for apprehensive and uncooperative patients
Obstructions in the root canal system
Ledges calcified canals separated instruments may prevent access to the apical foramen and may warrant a surgical approach in managing periapical lesions related to such teeth
Time involved for treatment
Enhanced healing kinetics are observed after performing apical surgery in teeth with periapical lesions
Cases refractory to nonsurgical management methods
Inflammatory apical true cysts and the presence of cholesterol crystals have been suggested as possible causes that prevent healing of periapical lesionsSurgery is recommended for such cases
METHODS FOR NONSURGICAL MANAGMENT OF PERIAPICAL LESIONS Conservative root canal treatment without adjunctive therapy
Instrumentation should be carried 1 mm beyond the apical foramen when a periapical lesion is evident on a radiograph This may cause transitory inflammation and ulceration of the epithelial lining resulting in resolution of the cyst
Decompression technique
The decompression technique involves placement of a drain into the lesion regular irrigation periodic length adjustment and maintenance of the drain for various periods of time
Active nonsurgical decompression technique
This technique uses the Endo-eze vacuum system to create a negative pressure which results in the decompression of large periapical lesions The high-volume suction aspirator is connected to a micro 22-gauge needle which is inserted in the root canal and activated for 20 minutes creating a negative pressure which results in aspiration of the exudate When the drainage partially stops the access cavity is closed with temporary cement which helps in maintaining bacterial control
Aspiration and irrigation technique
Hoen et al suggested aspiration of the cystic fluid from the periapcial lesion using a buccal palatal approach In this technique an 18-gauge needle attached to a 20 ml syringe is used to penetrate the buccal mucosa and aspirate the cystic fluid A second syringe filled with saline is then used to rinse the bony lesion The new needle is inserted through the buccal wound and passed out through the palatal tissue creating a pathway for the escape of the irrigant
Aspiration through the root canal technique
In this technique aspiration of the cystic fluid is done through the root canal by passing the aspirating needle through the apical foramen This technique eliminates the creation of buccal and palatal wounds as in the traditional aspirationndashirrigation technique This minimizes the discomfort that the patient may experience
However it is advisable not to use either aspirationndashirrigation or aspiration through the root canal techniques where adjacent tissue spaces or sinus cavities are involved when there is no fluid aspiration from the lesion or in infected periapicallesions
Method using calcium hydroxide
Calcium hydroxide is a widely used material in endodontic treatment because of its bactericidal effectsIt is thought to create favorable conditions for periapical repair and stimulate hard tissue formationSouza et al suggested that the action of calcium hydroxide beyond the apex may be four-fold (a) anti-inflammatory activity (b) neutralization of acid products (c) activation of the alkaline phosphatase and (d) antibacterial action
Lesion sterilization and repair therapy
lsquoLesion Sterilization and Tissue Repair (LSTR)rsquo therapy that uses a triple antibiotic paste of ciprofloxacin metronidazole and minocycline for disinfection of oral infectious lesions including dentinal pulpal and periradicular lesions Repair of damaged tissues can be expected if lesions are disinfectedMetronidazole is the first choice because it has a wide antibacterial spectrum against anaerobesHowever some bacteria are resistant to metronidazole and hence ciprofloxacin and minocycline are added to the mix
Apexum procedure
Surgical removal of the periapical chronically inflamed tissue allows a fresh blood clot to form thereby converting a chronic inflammatory lesion into a new granulation tissue where healing might proceed much fasterThe Apexumprocedure uses two sequential rotary devices the Apexum NiTi Ablator and Apexum PGA Ablator (Apexum Ltd Or Yehuda Israel) designed to extend beyond the apex and mince the periapical tissues on rotation in a low-speed handpiece followed by washing out the minced tissue
Surgical management of Apical lesions Apical lesions maybe managed surgically to reduce
healing and recovery time
Indicated for emergency cases
Incision and drainagewith antibiotic therapy of the lesionfollowed by RCT with apisectomy is the usual modality of surgical treatment of apical lesions
Medical Management of apical lesions Antibiotic therapy is used to treat minor apical
lesionsin order to relieve the symptomsThis enables easier surgical or non0surgical management of the lesionThus medical management of apical lesions is used in conjunction with Surgical or non surgical management of apical lesions
Cellulitis-Cefazolin 1g iv Q8H7-10 days or cloxacillin500-1000mg po Q6H7-10 days
Acute osteomyelitis-Cefazolin 2g iv Q8H
Ludwigs angina-Clindamycin 600mg iv Q8H2-3 weeks
References J Conserv Dent 2010 Oct-Dec 13(4) 240-
245doi 1041030972070773384PMCID PMC3010029Nonsurgical management of periapical lesions Marina Fernandes and Ida de Ataide
Manual in maxillofacial surgery for senior house officers-Dental 2cmcvellore
DrVikram PerakathBDS
METHODS FOR NONSURGICAL MANAGMENT OF PERIAPICAL LESIONS Conservative root canal treatment without adjunctive therapy
Instrumentation should be carried 1 mm beyond the apical foramen when a periapical lesion is evident on a radiograph This may cause transitory inflammation and ulceration of the epithelial lining resulting in resolution of the cyst
Decompression technique
The decompression technique involves placement of a drain into the lesion regular irrigation periodic length adjustment and maintenance of the drain for various periods of time
Active nonsurgical decompression technique
This technique uses the Endo-eze vacuum system to create a negative pressure which results in the decompression of large periapical lesions The high-volume suction aspirator is connected to a micro 22-gauge needle which is inserted in the root canal and activated for 20 minutes creating a negative pressure which results in aspiration of the exudate When the drainage partially stops the access cavity is closed with temporary cement which helps in maintaining bacterial control
Aspiration and irrigation technique
Hoen et al suggested aspiration of the cystic fluid from the periapcial lesion using a buccal palatal approach In this technique an 18-gauge needle attached to a 20 ml syringe is used to penetrate the buccal mucosa and aspirate the cystic fluid A second syringe filled with saline is then used to rinse the bony lesion The new needle is inserted through the buccal wound and passed out through the palatal tissue creating a pathway for the escape of the irrigant
Aspiration through the root canal technique
In this technique aspiration of the cystic fluid is done through the root canal by passing the aspirating needle through the apical foramen This technique eliminates the creation of buccal and palatal wounds as in the traditional aspirationndashirrigation technique This minimizes the discomfort that the patient may experience
However it is advisable not to use either aspirationndashirrigation or aspiration through the root canal techniques where adjacent tissue spaces or sinus cavities are involved when there is no fluid aspiration from the lesion or in infected periapicallesions
Method using calcium hydroxide
Calcium hydroxide is a widely used material in endodontic treatment because of its bactericidal effectsIt is thought to create favorable conditions for periapical repair and stimulate hard tissue formationSouza et al suggested that the action of calcium hydroxide beyond the apex may be four-fold (a) anti-inflammatory activity (b) neutralization of acid products (c) activation of the alkaline phosphatase and (d) antibacterial action
Lesion sterilization and repair therapy
lsquoLesion Sterilization and Tissue Repair (LSTR)rsquo therapy that uses a triple antibiotic paste of ciprofloxacin metronidazole and minocycline for disinfection of oral infectious lesions including dentinal pulpal and periradicular lesions Repair of damaged tissues can be expected if lesions are disinfectedMetronidazole is the first choice because it has a wide antibacterial spectrum against anaerobesHowever some bacteria are resistant to metronidazole and hence ciprofloxacin and minocycline are added to the mix
Apexum procedure
Surgical removal of the periapical chronically inflamed tissue allows a fresh blood clot to form thereby converting a chronic inflammatory lesion into a new granulation tissue where healing might proceed much fasterThe Apexumprocedure uses two sequential rotary devices the Apexum NiTi Ablator and Apexum PGA Ablator (Apexum Ltd Or Yehuda Israel) designed to extend beyond the apex and mince the periapical tissues on rotation in a low-speed handpiece followed by washing out the minced tissue
Surgical management of Apical lesions Apical lesions maybe managed surgically to reduce
healing and recovery time
Indicated for emergency cases
Incision and drainagewith antibiotic therapy of the lesionfollowed by RCT with apisectomy is the usual modality of surgical treatment of apical lesions
Medical Management of apical lesions Antibiotic therapy is used to treat minor apical
lesionsin order to relieve the symptomsThis enables easier surgical or non0surgical management of the lesionThus medical management of apical lesions is used in conjunction with Surgical or non surgical management of apical lesions
Cellulitis-Cefazolin 1g iv Q8H7-10 days or cloxacillin500-1000mg po Q6H7-10 days
Acute osteomyelitis-Cefazolin 2g iv Q8H
Ludwigs angina-Clindamycin 600mg iv Q8H2-3 weeks
References J Conserv Dent 2010 Oct-Dec 13(4) 240-
245doi 1041030972070773384PMCID PMC3010029Nonsurgical management of periapical lesions Marina Fernandes and Ida de Ataide
Manual in maxillofacial surgery for senior house officers-Dental 2cmcvellore
DrVikram PerakathBDS
Aspiration and irrigation technique
Hoen et al suggested aspiration of the cystic fluid from the periapcial lesion using a buccal palatal approach In this technique an 18-gauge needle attached to a 20 ml syringe is used to penetrate the buccal mucosa and aspirate the cystic fluid A second syringe filled with saline is then used to rinse the bony lesion The new needle is inserted through the buccal wound and passed out through the palatal tissue creating a pathway for the escape of the irrigant
Aspiration through the root canal technique
In this technique aspiration of the cystic fluid is done through the root canal by passing the aspirating needle through the apical foramen This technique eliminates the creation of buccal and palatal wounds as in the traditional aspirationndashirrigation technique This minimizes the discomfort that the patient may experience
However it is advisable not to use either aspirationndashirrigation or aspiration through the root canal techniques where adjacent tissue spaces or sinus cavities are involved when there is no fluid aspiration from the lesion or in infected periapicallesions
Method using calcium hydroxide
Calcium hydroxide is a widely used material in endodontic treatment because of its bactericidal effectsIt is thought to create favorable conditions for periapical repair and stimulate hard tissue formationSouza et al suggested that the action of calcium hydroxide beyond the apex may be four-fold (a) anti-inflammatory activity (b) neutralization of acid products (c) activation of the alkaline phosphatase and (d) antibacterial action
Lesion sterilization and repair therapy
lsquoLesion Sterilization and Tissue Repair (LSTR)rsquo therapy that uses a triple antibiotic paste of ciprofloxacin metronidazole and minocycline for disinfection of oral infectious lesions including dentinal pulpal and periradicular lesions Repair of damaged tissues can be expected if lesions are disinfectedMetronidazole is the first choice because it has a wide antibacterial spectrum against anaerobesHowever some bacteria are resistant to metronidazole and hence ciprofloxacin and minocycline are added to the mix
Apexum procedure
Surgical removal of the periapical chronically inflamed tissue allows a fresh blood clot to form thereby converting a chronic inflammatory lesion into a new granulation tissue where healing might proceed much fasterThe Apexumprocedure uses two sequential rotary devices the Apexum NiTi Ablator and Apexum PGA Ablator (Apexum Ltd Or Yehuda Israel) designed to extend beyond the apex and mince the periapical tissues on rotation in a low-speed handpiece followed by washing out the minced tissue
Surgical management of Apical lesions Apical lesions maybe managed surgically to reduce
healing and recovery time
Indicated for emergency cases
Incision and drainagewith antibiotic therapy of the lesionfollowed by RCT with apisectomy is the usual modality of surgical treatment of apical lesions
Medical Management of apical lesions Antibiotic therapy is used to treat minor apical
lesionsin order to relieve the symptomsThis enables easier surgical or non0surgical management of the lesionThus medical management of apical lesions is used in conjunction with Surgical or non surgical management of apical lesions
Cellulitis-Cefazolin 1g iv Q8H7-10 days or cloxacillin500-1000mg po Q6H7-10 days
Acute osteomyelitis-Cefazolin 2g iv Q8H
Ludwigs angina-Clindamycin 600mg iv Q8H2-3 weeks
References J Conserv Dent 2010 Oct-Dec 13(4) 240-
245doi 1041030972070773384PMCID PMC3010029Nonsurgical management of periapical lesions Marina Fernandes and Ida de Ataide
Manual in maxillofacial surgery for senior house officers-Dental 2cmcvellore
DrVikram PerakathBDS
Method using calcium hydroxide
Calcium hydroxide is a widely used material in endodontic treatment because of its bactericidal effectsIt is thought to create favorable conditions for periapical repair and stimulate hard tissue formationSouza et al suggested that the action of calcium hydroxide beyond the apex may be four-fold (a) anti-inflammatory activity (b) neutralization of acid products (c) activation of the alkaline phosphatase and (d) antibacterial action
Lesion sterilization and repair therapy
lsquoLesion Sterilization and Tissue Repair (LSTR)rsquo therapy that uses a triple antibiotic paste of ciprofloxacin metronidazole and minocycline for disinfection of oral infectious lesions including dentinal pulpal and periradicular lesions Repair of damaged tissues can be expected if lesions are disinfectedMetronidazole is the first choice because it has a wide antibacterial spectrum against anaerobesHowever some bacteria are resistant to metronidazole and hence ciprofloxacin and minocycline are added to the mix
Apexum procedure
Surgical removal of the periapical chronically inflamed tissue allows a fresh blood clot to form thereby converting a chronic inflammatory lesion into a new granulation tissue where healing might proceed much fasterThe Apexumprocedure uses two sequential rotary devices the Apexum NiTi Ablator and Apexum PGA Ablator (Apexum Ltd Or Yehuda Israel) designed to extend beyond the apex and mince the periapical tissues on rotation in a low-speed handpiece followed by washing out the minced tissue
Surgical management of Apical lesions Apical lesions maybe managed surgically to reduce
healing and recovery time
Indicated for emergency cases
Incision and drainagewith antibiotic therapy of the lesionfollowed by RCT with apisectomy is the usual modality of surgical treatment of apical lesions
Medical Management of apical lesions Antibiotic therapy is used to treat minor apical
lesionsin order to relieve the symptomsThis enables easier surgical or non0surgical management of the lesionThus medical management of apical lesions is used in conjunction with Surgical or non surgical management of apical lesions
Cellulitis-Cefazolin 1g iv Q8H7-10 days or cloxacillin500-1000mg po Q6H7-10 days
Acute osteomyelitis-Cefazolin 2g iv Q8H
Ludwigs angina-Clindamycin 600mg iv Q8H2-3 weeks
References J Conserv Dent 2010 Oct-Dec 13(4) 240-
245doi 1041030972070773384PMCID PMC3010029Nonsurgical management of periapical lesions Marina Fernandes and Ida de Ataide
Manual in maxillofacial surgery for senior house officers-Dental 2cmcvellore
DrVikram PerakathBDS
Surgical management of Apical lesions Apical lesions maybe managed surgically to reduce
healing and recovery time
Indicated for emergency cases
Incision and drainagewith antibiotic therapy of the lesionfollowed by RCT with apisectomy is the usual modality of surgical treatment of apical lesions
Medical Management of apical lesions Antibiotic therapy is used to treat minor apical
lesionsin order to relieve the symptomsThis enables easier surgical or non0surgical management of the lesionThus medical management of apical lesions is used in conjunction with Surgical or non surgical management of apical lesions
Cellulitis-Cefazolin 1g iv Q8H7-10 days or cloxacillin500-1000mg po Q6H7-10 days
Acute osteomyelitis-Cefazolin 2g iv Q8H
Ludwigs angina-Clindamycin 600mg iv Q8H2-3 weeks
References J Conserv Dent 2010 Oct-Dec 13(4) 240-
245doi 1041030972070773384PMCID PMC3010029Nonsurgical management of periapical lesions Marina Fernandes and Ida de Ataide
Manual in maxillofacial surgery for senior house officers-Dental 2cmcvellore
DrVikram PerakathBDS
Medical Management of apical lesions Antibiotic therapy is used to treat minor apical
lesionsin order to relieve the symptomsThis enables easier surgical or non0surgical management of the lesionThus medical management of apical lesions is used in conjunction with Surgical or non surgical management of apical lesions
Cellulitis-Cefazolin 1g iv Q8H7-10 days or cloxacillin500-1000mg po Q6H7-10 days
Acute osteomyelitis-Cefazolin 2g iv Q8H
Ludwigs angina-Clindamycin 600mg iv Q8H2-3 weeks
References J Conserv Dent 2010 Oct-Dec 13(4) 240-
245doi 1041030972070773384PMCID PMC3010029Nonsurgical management of periapical lesions Marina Fernandes and Ida de Ataide
Manual in maxillofacial surgery for senior house officers-Dental 2cmcvellore
DrVikram PerakathBDS
References J Conserv Dent 2010 Oct-Dec 13(4) 240-
245doi 1041030972070773384PMCID PMC3010029Nonsurgical management of periapical lesions Marina Fernandes and Ida de Ataide
Manual in maxillofacial surgery for senior house officers-Dental 2cmcvellore
DrVikram PerakathBDS
DrVikram PerakathBDS