Embed Size (px)
DESCRIPTION
Causes of Hypomelanosis Leukoderma Hypomelanosis Amelanosis Depigmentation Pigmentary dilution Poliosis Vitiligo
Citation preview

DISORDERS OF HYPOPIGMENTATION


Leukoderma & Hypopigmentation
• They are general terms used to designate disorders characterized by lightening of the skin. They may be:
- Melanin-related result of ↓ epidermal melanin content. - Hemoglobin-related secondary to ↓ blood supply to the skin.

Hypomelanosis
Is a more specific term that denotes an absence or reduction of melanin within the skin; Cutaneous hypomelanosis is often classified into two groups:
• MELANOCYTOPENIC HYPOMELANOSIS; caused by a partial or total absence of epidermal &/or follicular melanocytes.
• MELANOPENIC HYPOMELANOSIS, in which the number of epidermal and/or follicular melanocytes is normal but the pigment cells fail to synthesize normal amounts of melanin and/or transfer it to surrounding keratinocytes.

Amelanosis
• Signifies the total absence of melanin.

Depigmentation
• Usually implies a total loss of skin color, most commonly due to disappearance of pre-existing melanin pigmentation, as in vitiligo.

Pigmentary dilution
• This term is used to describe a generalized lightening of the skin and hair, as in oculocutaneous albinism; this may be apparent only if affected individuals are compared with unaffected relatives.

Poliosis
• localized patch of white or gray hair.

Causes of Hypomelanosis
A. Genetic Hypomelanosis
B. Acquired Hypomelanosis

Genetic Hypomelanosis
1. Oculocutaneous albinism (OCA)
2. Ocular albinism With deafness
3. Albinoidism
4. Cross syndrome
5. Piebaldism
6. Waardenburg syndrome
7. Phenylketonuria (PKU)
8. Tuberous sclerosis (ash leaf macules)
9. Naevus depigmentosus
10.Hypomelanosis of Ito

Acquired HypomelanosisI-Inflammatory
1. Eczema
2. Atopic eczema
3. Pityriasis alba
4. Pityriasis rosea
5. Pityriasis lichenoides chronica (PLC)
6. Psoriasis
7. Parapsoriasis
8. Lupus erythematosus
9. Lichen planus
10.Lichen sclerosus
11.Lichen striatus
12.Scleroderma
13.Sarcoidosis
14.Bullous dermatoses

Acquired HypomelanosisII- Infections
1. Pityriasis versicolor
2. Leprosy
3. Syphilis
4. Pinta (Treponematoses)
5. Yaws
6. Onchocerciasis
7. Post Kala-Azar dermal leishmaniasis

Acquired HypomelanosisIII-Chemical factors
(occupational and therapeutic)
1. Phenol derivatives e.g. Monobenzylether of hydroquinone, Monomethylether of hydroquinone
2. Antimalarials: Chloroquine and hydroxychloroquine
3. Corticosteroids (topicals & intralesional)
4. Arsenic
5. Sulfhydryls
6. Azelaic acid

Acquired HypomelanosisIV- Physical factors
1. Thermal burns
2. Freezing
3. Lasers
4. UV radiation
5. Ionizing radiation,
6. Dermabrasion

Acquired HypomelanosisV-Endocrine factors
1. Hypopituitarism
2. Hypothyroidism
3. Addison’s disease

Acquired HypomelanosisVI-Nutritional factors
1. Chronic protein deficiency
a) Kwashiorkor
b) Malabsorption
c) Nephrosis
2. Pernicious anaemia (vit. B12↓)

Acquired HypomelanosisVII- Neoplasms
1. Halo naevus
2. Malignant melanoma
3. CTCL (hypopigmented MF & poikilodermatous MF)

Acquired HypomelanosisVIII- Miscellaneous
1. Poliosis
2. Canities
3. Idiopathic guttate hypomelanosis
4. Progressive Macular Hypomelanosis
5. Vitiligo
6. Vogt–Koyanagi–Harada syndrome
7. Vagabond’s Leukomelanoderma

Leukodermas without Hypomelanosis
1. Woronoff’s ring
2. Nevus anemicus
3. Cutaneous edema
4. Anemia
5. Angiospastic macules (Bier spots)

Vitiligo

Definition
• Latin vitilīgō skin eruption, appar. akin to vitium fault, defect.
• Vitiligo is an acquired pigmentary disorder of the skin and mucous membranes characterized by circumscribed depigmented macules and patches that result from a progressive loss of functional melanocytes that are selectively destroyed.

• Vitiligo affects 0.5-2% of the world population.
• The average age of onset is 20 years.
• The condition is frequently associated with disorders of autoimmune origin, with thyroid abnormalities being the most common.
Overview

Epidemiology of Vitiligo

INCIDENCE:
• Vitiligo is relatively common, with a rate of 0.5 -2% of the general population worldwide.
• Approximately 30% of vitiligo cases occur with a familial clustering of cases.
SEX:
• No statistically significant difference.
• The discrepancy has been attributed to an in reporting of cosmetic concerns by ♀ patients.
Epidemiology

AGE:
• The onset is most commonly observed in persons aged 10-30 years.
• The average age of onset for vitiligo is approximately 20 years.
• Vitiligo rarely is seen in infancy or old age. Nearly all cases of vitiligo are acquired relatively early in life.
• The age of onset is unlikely to vary between the sexes.
Epidemiology

Pathophysiology of Vitiligo

• Vitiligo is a multifactorial polygenic disorder with a complex pathogenesis. It is related to both genetic and nongenetic factors. Although several theories have been proposed about the pathogenesis of vitiligo, the precise cause remains unknown. Generally agreed upon principles are
An absence of functional melanocytes in vitiligo skin.
A loss of histochemically recognized melanocytes, owing to their destruction.
Pathophysiology

• levels of SCF (stem cell factor) in lesional vitiligo skin compared to non-lesional skin.
• levels of TNF-α and IL-1 in lesional vitiligo skin compared to non-lesional skin.
• In addition to the typical “absolute” type of vitiligo in which there are no DOPA-positive melanocytes “relative” types of vitiligo in which melanocytes remain within the lesions but have DOPA-positivity have been observed. It is possible that relative types of vitiligo are forerunners of the absolute type.
Pathophysiology

• There is increasing evidence that non-segmental and segmental forms of vitiligo do not have the same genetic influences and may be distinct entities. For non-segmental vitiligo, accumulated data strongly support an autoimmune etiology in genetically predisposed individuals.
• Melanocytes may be present in depigmented skin after years of onset & may still respond to therapy under appropriate stimulation.
Pathophysiology

GENETICS OF VITILIGO:• Both twin and family studies indicate the importance of genetic
factors in the development of vitiligo.• Vitiligo is characterized by;
1.Incomplete penetrance (with environmental influences)2.Multiple susceptibility loci.3.Genetic heterogeneity.
• The inheritance of vitiligo may involve genes associated with;
1.Biosynthesis of melanin.2.Response to oxidative stress.3.Regulation of autoimmunity.
• An association with HLA-B13 in the presence of antithyroid Abs.
Pathophysiology

• THEORIES REGARDING DESTRUCTION OF MELANOCYTES INCLUDE:
1.Autoimmune mechanisms.
2.Intrinsic defect of melanocytes mechanisms.
3.Oxidant-antioxidant mechanisms.
4.Neural mechanisms.
• “CONVERGENCE THEORY” has also been proposed that vitiligo results from a combination of several of the pathogenic mechanisms.
Pathophysiology


Pathophysiology

Pathophysiology

Pathophysiology

NEURAL THEORYBased on the following observations: • A neurochemical mediator released from nerve
endings destroys melanocytes or inhibits melanin production.
• Case reports describe patients afflicted with a nerve injury who also have vitiligo have hypo- or depigmentation in denervated areas.
• Segmental vitiligo frequently occurs in a dermatomal pattern.
• Sweating and vasoconstriction are in vitiliginous areas, implying an in adrenergic activity.
• Degenerative & regenerative autonomic nerves in depigmented patches.
• urinary excretion of homovanillic acid (HVA) and vanilmandelic acid (VMA) (neurometabolites) in active vitiligo has been documented in patients with vitiligo. This may be a secondary or primary phenomenon.
• Depigmentation in animal models with severed nerve fibres.
Pathophysiology

Clinical Features of Vitiligo

• Usually asymptomatic.
• Onset: usually insidious.
• Color: The MC form of vitiligo is totally amelanotic acquired chalk or milk-white or hypopigmented macules or patches surrounded by healthy skin. The lesions are not readily apparent in lightly pigmented individuals; however, they are easily distinguishable with a Wood lamp examination.
Clinical Features


• Shape: Round, oval, irregular or linear.
• Borders: Usually well demarcated may be convex as if the depigmenting process were “invading” the surrounding normally pigmented skin.
• Size: Range from mms to cms. Lesions enlarge centrifugally over time at an unpredictable rate (slow or rapid).
Clinical Features

• Site: Interestingly, it has a predilection for sites that are normally relatively hyperpigmented. Initial lesions occur most frequently on the hands, forearms, feet, and face, favoring a perioral and periocular (i.e. periorificial) distribution.
• The MC sites of vitiligo involvement are the face, neck, and scalp. Many of the MC sites of occurrence are areas subjected to repeated trauma pressure or friction esp. bony prominences, including the following:
1. Elbows2. Knees3. Dorsal ankles 4. Shins
• Involvement of the mucous membranes is frequently observed in the setting of generalized vitiligo.
• Vitiligo often occurs around body orifices such as the lips, anogenital, gingiva, areolas, and nipples.
Clinical Features
5. Extensor forearm6. Ventral wrists7. Dorsal hands8. Digital phalanges


• Vitiligo of the scalp usually appears as poliosis, but scattered white hairs due to involvement of individual follicles or even total depigmentation of all scalp hair may occur. Scalp involvement is the most frequent, followed by involvement of the eyebrows, pubic hair, and axillary hair, respectively.
Clinical Features

LEUKOTRICHIA:• Depigmented body hair in vitiliginous
macules. • May indicate a poor prognosis in regard to
repigmentation. • Spontaneous repigmentation of
depigmented hair in vitiligo does not occur as follicular melanocytes are often spared in vitiligo.
• It’s occurrence does not correlate with disease activity.
• Isolated early graying or whitening before 30 years of age has been suggested to represent a form of vitiligo.
Clinical Features

PSYCHOLOGICAL IMPACT
• Feelings of stress, embarrassment and self consciousness.
• Perception of discrimination.
• Low self steem.• Disturbed sexual
relationships.
Clinical Features

1. Trichrome vitiligo: has an intermediate zone of hypochromia located between the achromic center & the peripheral unaffected skin. The natural evolution of the hypopigmented areas is progression to full depigmentation & number of melanocytes is also intermediate in this zone. This results in 3 shades of color; brown, tan (fairly uniform hue), and white in the same patient.
2. Quadrichrome vitiligo: presence of 4th color (ie, dark brown) dt. perifollicular repigmentation.
3. Pentachrome vitiligo: with 5 shades of color (black, dark brown, medium brown [unaffected skin], tan and white) has also been described.
4. (Marginal) inflammatory vitiligo: results in erythematous raised border which is present from ‘onset of vitiligo (in rare cases) or which may appear several months or years after the initial onset. Mild pruritus may be present.
5. Blue vitiligo: results in blue coloration of vitiligo macules. This type has been observed in a patient with postinflammatory hyperpigmentation who then developed vitiligo.
6. Koebner phenomenon: is defined as the development of vitiligo in sites of specific trauma, such as a cut, burn, or abrasion. Minimum threshold injury is required for Koebner phenomenon to occur even friction from clothes. more common in progressive non-segmental vitiligo.
7. Vitiligo ponctué: “punctuated” an unusual clinical presentation of vitiligo, is characterized by multiple small (confetti-like), discrete amelanotic macules, sometimes superimposed upon a hyperpigmented macule.
Clinical Variants

1. Trichrome vitiligo: has an intermediate zone of hypochromia located between the achromic center & the peripheral unaffected skin. The natural evolution of the hypopigmented areas is progression to full depigmentation & number of melanocytes is also intermediate in this zone. This results in 3 shades of color; brown, tan (fairly uniform hue), and white in the same patient.
2. Quadrichrome vitiligo: presence of 4th color (ie, dark brown) dt. perifollicular repigmentation.
3. Pentachrome vitiligo: with 5 shades of color (black, dark brown, medium brown [unaffected skin], tan and white) has also been described.
4. (Marginal) inflammatory vitiligo: results in erythematous raised border which is present from ‘onset of vitiligo (in rare cases) or which may appear several months or years after the initial onset. Mild pruritus may be present.
5. Blue vitiligo: results in blue coloration of vitiligo macules. This type has been observed in a patient with postinflammatory hyperpigmentation who then developed vitiligo.
6. Koebner phenomenon: is defined as the development of vitiligo in sites of specific trauma, such as a cut, burn, or abrasion. Minimum threshold injury is required for Koebner phenomenon to occur even friction from clothes. more common in progressive non-segmental vitiligo.
7. Vitiligo ponctué: “punctuated” an unusual clinical presentation of vitiligo, is characterized by multiple small (confetti-like), discrete amelanotic macules, sometimes superimposed upon a hyperpigmented macule.
Clinical Variants

1. Trichrome vitiligo: has an intermediate zone of hypochromia located between the achromic center & the peripheral unaffected skin. The natural evolution of the hypopigmented areas is progression to full depigmentation & number of melanocytes is also intermediate in this zone. This results in 3 shades of color; brown, tan (fairly uniform hue), and white in the same patient.
2. Quadrichrome vitiligo: presence of 4th color (ie, dark brown) dt. perifollicular repigmentation.
3. Pentachrome vitiligo: with 5 shades of color (black, dark brown, medium brown [unaffected skin], tan and white) has also been described.
4. (Marginal) inflammatory vitiligo: results in erythematous raised border which is present from ‘onset of vitiligo (in rare cases) or which may appear several months or years after the initial onset. Mild pruritus may be present.
5. Blue vitiligo: results in blue coloration of vitiligo macules. This type has been observed in a patient with postinflammatory hyperpigmentation who then developed vitiligo.
6. Koebner phenomenon: is defined as the development of vitiligo in sites of specific trauma, such as a cut, burn, or abrasion. Minimum threshold injury is required for Koebner phenomenon to occur even friction from clothes. more common in progressive non-segmental vitiligo.
7. Vitiligo ponctué: “punctuated” an unusual clinical presentation of vitiligo, is characterized by multiple small (confetti-like), discrete amelanotic macules, sometimes superimposed upon a hyperpigmented macule.
Clinical Variants

1. Trichrome vitiligo: has an intermediate zone of hypochromia located between the achromic center & the peripheral unaffected skin. The natural evolution of the hypopigmented areas is progression to full depigmentation & number of melanocytes is also intermediate in this zone. This results in 3 shades of color; brown, tan (fairly uniform hue), and white in the same patient.
2. Quadrichrome vitiligo: presence of 4th color (ie, dark brown) dt. perifollicular repigmentation.
3. Pentachrome vitiligo: with 5 shades of color (black, dark brown, medium brown [unaffected skin], tan and white) has also been described.
4. (Marginal) inflammatory vitiligo: results in erythematous raised border which is present from ‘onset of vitiligo (in rare cases) or which may appear several months or years after the initial onset. Mild pruritus may be present.
5. Blue vitiligo: results in blue coloration of vitiligo macules. This type has been observed in a patient with postinflammatory hyperpigmentation who then developed vitiligo.
6. Koebner phenomenon: is defined as the development of vitiligo in sites of specific trauma, such as a cut, burn, or abrasion. Minimum threshold injury is required for Koebner phenomenon to occur even friction from clothes. more common in progressive non-segmental vitiligo.
7. Vitiligo ponctué: “punctuated” an unusual clinical presentation of vitiligo, is characterized by multiple small (confetti-like), discrete amelanotic macules, sometimes superimposed upon a hyperpigmented macule.
Clinical Variants

1. Trichrome vitiligo: has an intermediate zone of hypochromia located between the achromic center & the peripheral unaffected skin. The natural evolution of the hypopigmented areas is progression to full depigmentation & number of melanocytes is also intermediate in this zone. This results in 3 shades of color; brown, tan (fairly uniform hue), and white in the same patient.
2. Quadrichrome vitiligo: presence of 4th color (ie, dark brown) dt. perifollicular repigmentation.
3. Pentachrome vitiligo: with 5 shades of color (black, dark brown, medium brown [unaffected skin], tan and white) has also been described.
4. (Marginal) inflammatory vitiligo: results in erythematous raised border which is present from ‘onset of vitiligo (in rare cases) or which may appear several months or years after the initial onset. Mild pruritus may be present.
5. Blue vitiligo: results in blue coloration of vitiligo macules. This type has been observed in a patient with postinflammatory hyperpigmentation who then developed vitiligo.
6. Koebner phenomenon: is defined as the development of vitiligo in sites of specific trauma, such as a cut, burn, or abrasion. Minimum threshold injury is required for Koebner phenomenon to occur even friction from clothes. more common in progressive non-segmental vitiligo.
7. Vitiligo ponctué: “punctuated” an unusual clinical presentation of vitiligo, is characterized by multiple small (confetti-like), discrete amelanotic macules, sometimes superimposed upon a hyperpigmented macule.
Clinical Variants

1. Trichrome vitiligo: has an intermediate zone of hypochromia located between the achromic center & the peripheral unaffected skin. The natural evolution of the hypopigmented areas is progression to full depigmentation & number of melanocytes is also intermediate in this zone. This results in 3 shades of color; brown, tan (fairly uniform hue), and white in the same patient.
2. Quadrichrome vitiligo: presence of 4th color (ie, dark brown) dt. perifollicular repigmentation.
3. Pentachrome vitiligo: with 5 shades of color (black, dark brown, medium brown [unaffected skin], tan and white) has also been described.
4. (Marginal) inflammatory vitiligo: results in erythematous raised border which is present from ‘onset of vitiligo (in rare cases) or which may appear several months or years after the initial onset. Mild pruritus may be present.
5. Blue vitiligo: results in blue coloration of vitiligo macules. This type has been observed in a patient with postinflammatory hyperpigmentation who then developed vitiligo.
6. Koebner phenomenon: is defined as the development of vitiligo in sites of specific trauma, such as a cut, burn, or abrasion. Minimum threshold injury is required for Koebner phenomenon to occur even friction from clothes. more common in progressive non-segmental vitiligo.
7. Vitiligo ponctué: “punctuated” an unusual clinical presentation of vitiligo, is characterized by multiple small (confetti-like), discrete amelanotic macules, sometimes superimposed upon a hyperpigmented macule.
Clinical Variants

1. Trichrome vitiligo: has an intermediate zone of hypochromia located between the achromic center & the peripheral unaffected skin. The natural evolution of the hypopigmented areas is progression to full depigmentation & number of melanocytes is also intermediate in this zone. This results in 3 shades of color; brown, tan (fairly uniform hue), and white in the same patient.
2. Quadrichrome vitiligo: presence of 4th color (ie, dark brown) dt. perifollicular repigmentation.
3. Pentachrome vitiligo: with 5 shades of color (black, dark brown, medium brown [unaffected skin], tan and white) has also been described.
4. (Marginal) inflammatory vitiligo: results in erythematous raised border which is present from ‘onset of vitiligo (in rare cases) or which may appear several months or years after the initial onset. Mild pruritus may be present.
5. Blue vitiligo: results in blue coloration of vitiligo macules. This type has been observed in a patient with postinflammatory hyperpigmentation who then developed vitiligo.
6. Koebner phenomenon: is defined as the development of vitiligo in sites of specific trauma, such as a cut, burn, or abrasion. Minimum threshold injury is required for Koebner phenomenon to occur even friction from clothes. more common in progressive non-segmental vitiligo.
7. Vitiligo ponctué: “punctuated” an unusual clinical presentation of vitiligo, is characterized by multiple small (confetti-like), discrete amelanotic macules, sometimes superimposed upon a hyperpigmented macule.
Clinical Variants

1. Trichrome vitiligo: has an intermediate zone of hypochromia located between the achromic center & the peripheral unaffected skin. The natural evolution of the hypopigmented areas is progression to full depigmentation & number of melanocytes is also intermediate in this zone. This results in 3 shades of color; brown, tan (fairly uniform hue), and white in the same patient.
2. Quadrichrome vitiligo: presence of 4th color (ie, dark brown) dt. perifollicular repigmentation.
3. Pentachrome vitiligo: with 5 shades of color (black, dark brown, medium brown [unaffected skin], tan and white) has also been described.
4. (Marginal) inflammatory vitiligo: results in erythematous raised border which is present from ‘onset of vitiligo (in rare cases) or which may appear several months or years after the initial onset. Mild pruritus may be present.
5. Blue vitiligo: results in blue coloration of vitiligo macules. This type has been observed in a patient with postinflammatory hyperpigmentation who then developed vitiligo.
6. Koebner phenomenon: is defined as the development of vitiligo in sites of specific trauma, such as a cut, burn, or abrasion. Minimum threshold injury is required for Koebner phenomenon to occur even friction from clothes. more common in progressive non-segmental vitiligo.
7. Vitiligo ponctué: “punctuated” an unusual clinical presentation of vitiligo, is characterized by multiple small (confetti-like), discrete amelanotic macules, sometimes superimposed upon a hyperpigmented macule.
Clinical Variants

VITILIGO
Localized
Focal Segmental Mucosal
Generalized
Acrofacial Vulgaris Mixed
Universal
Classifications of Vitiligo “By Distribution”

Classifications of Vitiligo “By Distribution”
I. LOCALIZED VITILIGO “3”1.Focal: characterized by one or more macules in one area but not clearly
in a segmental distribution, MC in the distribution of the trigeminal nerve.
2.Segmental/ Unilateral.3.Mucosal: Mucous membranes alone are affected.
II. GENERALIZED VITILIGO “3”• Generalized vitiligo implies more than one general area of involvement.
Macules are usually found on both sides of the trunk, either symmetrically or asymmetrically arrayed. It represents 90% of vitiligo patients.
1.Acrofacial: distal extremities and face (periorificial areas).2.Vulgaris: scattered patches that are widely distributed.3.Mixed: Acrofacial and vulgaris vitiligo occur in combination, or
segmental and acrofacial vitiligo and/or vulgaris involvement are noted in combination.
III.UNIVERSAL VITILIGO• This is complete or nearly complete depigmentation. It is often associated
with multiple endocrinopathy syndrome.










SEGMENTAL:• This type manifests as one or more macules in a dermatomal or
quasidermatomal pattern. • Onset early in life. occurs more commonly seen in children than
adults (~30% versus ~10%).• More than ½ the patients with segmental vitiligo have patches of
white hair or poliosis.• This type of vitiligo is not associated with thyroid or other
autoimmune disorders. • Lesions usually stop abruptly at midline doesn't cross it. rapidly
spreads in affected area.• The course of segmental vitiligo can arrest, & depigmented patches
can persist unchanged for the life of the patient (Stable).
NON-SEGMENTAL:• This type includes all types of vitiligo, except segmental vitiligo.• It is strongly associated with autoimmunity or inflammation such
as halo naevi and thyroid antibodies more than segmental vitiligo. • Patients with non-segmental vitiligo were also more likely to have a
family history of vitiligo or autoimmunity.
Two distinct forms of vitiligo

1. Thyroid disorders, most common & usually occur after the onset of vitiligo. Mainly in non-segmental vitiligo: a. Hashimoto thyroiditisb. Graves disease
2. Other endocrinopathies, such as a. Addison diseaseb. diabetes mellitus; c. Autoimmune Polyglandular Syndrome / APECED (autoimmune polyendocrinopathy–candidiasis–ectodermal dystrophy) syndrome. In this genetic, autoAb cause destruction of endocrine cells.
Autoimmune diseases associated with vitiligo
3. Pernicious anemia;4. Rheumatoid
arthritis,5. Inflammatory Bowel
Disease (IBD)Dermatological disorders:6. Halo nevus7. Alopecia areata (AA)8. Lupus
erythematosus,9. Psoriasis; 10.lichen sclerosus


Course of Vitiligo

• Unpredictable.• It becomes more extensive by the appearance of new
depigmented macules, enlargement of pre-existing lesions, or both processes.
• The natural course of the disease is usually one of slow progression, but it may stabilize for a long period of time or spread rapidly.
• Total body involvement that develops within a few weeks or even a few days may occur.
• Some degree of sun-induced or spontaneous repigmentation isnot uncommon in vitiligo, but complete and stable spontaneous repigmentation is rare.
Course

Investigations of Vitiligo

• Diagnosis of vitiligo generally is made on the basis of clinical findings.
• Vitiligo is diagnosed by means of inspection with a Wood’s lamp.
Investigations





• If signs or symptoms of associated autoimmune diseases occur, appropriate tests should be performed e.g. 1.Thyrotropin testing is the most cost-effective screening
test for thyroid disease. 2.Serum antithyroglobulin 3.Antithyroid peroxidase antibodies (Anti TPO) which
regarded as a sensitive and specific marker of autoimmune thyroid antibodies.
4.Antinuclear antibody (ANA) screening is also helpful. 5.CBC with indices helps rule out anemia. 6.Fasting blood glucose (FBG) : for Screening for
diabetes.7.Glycosylated hemoglobin (HbA1c)
Investigations

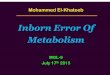
Histopathology

Vitiligo, 10x, stained for melanin. Note that melanin (tiny, dark spots) is absent on the basal layer of the epidermis although it is
preserved around the hair follicle.




• Biopsy is occasionally helpful for differentiating vitiligo from other hypopigmentary disorders.
• Complete absence of melanocytes in association with a total loss of epidermal pigmentation.
• Superficial perivascular and perifollicular lymphocytic infiltrates may be observed at the margin of vitiliginous lesions, consistent with a cell-mediated process destroying melanocytes.
• Degenerative changes have been documented in keratinocytes & melanocytes in border lesions & adjacent skin.
• Other documented changes include increased numbers of Langerhans cells, epidermal vacuolization, and thickening of the basement membrane.
• Loss of pigment and melanocytes in the epidermis is highlighted by Fontana-Masson staining and immunohistochemistry testing.
Histopathology

Treatment of Vitiligo

• THE AIMS OF VITILIGO TREATMENT ARE;
1. Repigmentation.
2. Stabilization of the depigmentation process.
3. To prevent complications.
• No single therapy for vitiligo produces predictably good results in all patients; the response to therapy is highly variable so treatment must be individualized, and patients should be made aware of the risks associated with therapy. The choice of therapy depends on the extent, location, and activity of disease as well as the patient’s age, skin type, and motivation to undergo treatment.
• Combination therapy may produce higher rates of repigmentation compared to traditional monotherapies.
Treatment

• Period of at least 2–3 months is required to determine whether a particular treatment is effective.
• The areas of the body that typically have the best response to medical therapy are the face, neck, mid extremities and trunk, while the distal extremities and lips are the most resistant to treatment consider camouflage.
Treatment
• Sunscreens (sun protection factor of 15 or higher is best) should be given to all patients with vitiligo to minimize risk of sunburn or repeated solar damage to depigmented skin.
• Tanning of surrounding normal skin exaggerates appearance of vitiligo this is prevented by sun protection.

• During medical therapy, pigment cells arise and proliferate from the following 3 sources:
1. The pilosebaceous unit, which provides the highest number of cells, migrating from the ORS toward the epidermis (vertical migration) When the hairs within an area of vitiligo are depigmented, this pattern is not observed.
2. Spared epidermal melanocytes not affected during depigmentation
3. The border of lesions, migrating up to 2-4 mm from the edge (horizontal migration)
Treatment

1. Phototherapy
2. Laser therapy
3. Corticosteroids
4. Topical calcineurin inhibitors (TCIs)
5. Vitamin D analogs
6. Depigmentation therapy
7. Surgical therapies
8. Micropigmentation
9. Pseudocatalase with narrowband UVB
10.Systemic antioxidant therapy
11.Dermabrasion followed by topical 5-fluorouracil and NB-UVB
12.Topical prostaglandins
Lines of Treatment

1. Narrow-band UV-B phototherapy (NB-UVB).
2. Focused microphototherapy.
3. Psoralen photochemotherapy (PUVA).
4. Khellin plus UVA (KUVA).
I. Phototherapy

1. NARROW-BAND UV-B PHOTOTHERAPY (NB-UVB): • Is widely used and produces good clinical
results & considered first choice of therapy for adults and children with generalized vitiligo especially if it involves ≥20% of the body surface area.
• Narrow-band fluorescent tubes with an emission spectrum of 310-313 nm & a maximum wavelength of 311 nm.
• Initial assessment of the MED in a vitiliginous area that is normally not sun exposed (e.g. buttocks, lower back or abdomen) is recommended. Since intense erythema may induce the Koebner phenomenon and worsening of the disease.
I. Phototherapy



NARROW-BAND UV-B PHOTOTHERAPY (NB-UVB): • The UVB doses have to be more carefully than in other
disorders, because of the photosensitivity.• The initial exposure is 70% of the MED in lesional skin,
and subsequent doses are chosen according to the response in vitiligo areas, i.e. the goal is to induce a barely perceptible erythema. This minimal erythema is the only useful parameter for determining dosage increments. The starting dose ranges from 100 to 250 mJ/cm2, which is in increments of 10–20% at each subsequent exposure. The objective of the dose increments is to achieve a minimally perceptible erythema within the lesions.
• Treatment frequency is 2-3 times weekly, but never on consecutive days for sufficiently long period.
• Effective as monotherapy without the addition of exogenous photosensitizers
• It is as effective as PUVA but had fewer side effects.
I. Phototherapy

SHORT-TERM ADVERSE EFFECTS OF NB-UVBi) Intense Erythema ii) Pruritus iii) Xerosisiv) Occasional Blisteringv) frequency of recurrent HSV.
LONG-TERM SIDE EFFECTS OF NB-UVBi) Photoaging ii) Cutaneous carcinogenesis (carcinogenic potential seems to be lower than that of PUVA).
I. Phototherapy

THE ADVANTAGES OF NARROW-BAND UV-B OVER PUVA INCLUDE:
1. Shorter treatment times
2. No drug costs
3. No adverse GI effects (e.g. nausea)
4. phototoxic reactions
5. No need for subsequent photoprotection.
6. Can be safely used in children, pregnant or lactating ♀, individuals with hepatic or kidney dysfunction.
7. Produces less accentuation of the contrast between depigmented and normally pigmented skin.
I. Phototherapy

2. FOCUSED MICROPHOTOTHERAPY:
• Targeting only the specific small lesions.
• A directed beam of broadband or narrowband UVB is used with a fiber optic system to direct radiation to specific areas of skin.
I. Phototherapy

3. PSORALEN PHOTOCHEMOTHERAPY (PUVA):
• Involves the use of photosensitizers psoralens combined with UV-A light.
THE PSORALENS COMMONLY USED:
a. 8-methoxypsoralen (8-MOP, methoxsalen) most commonly used.
b. 5-methoxypsoralen (5-MOP),
c. Trimethylpsoralen (TMP/ Trioxsalen).
I. Phototherapy

• The best results from PUVA can be obtained on the face, trunk, and proximal parts of the extremities.
• 2-3 treatments per week for many months or even years to achieve a satisfactory result before repigmentation from perifollicular openings merges to produce confluent repigmentation.
• If treatment is discontinued, reversal of acquired repigmentation may occur unless the lesion has completely repigmented. Completely repigmented areas can be stable for a decade or more without relapse
• The total number of PUVA treatments required is 50-300.
• Recommend that vitiligo patients receive a maximum cumulative UVA dose of 1000 J/cm2 and a maximum number of 300 treatments.
• If there is no response after 4–5 months or approximately 30–40 treatments, PUVA should be terminated.
I. Phototherapy

TOPICAL PUVA: • Cream and solution of 8-
methoxypsoralen (0.1-0.3% concentration).
• It is applied 30 minutes prior to UV-A radiation (usually 0.1-0.3 J/cm2 UV-A) exposure. It should be applied once or twice a week.
• TMP and 5 MOP can also be used for topical PUVA but are more phototoxic than 8 MOP.
I. Phototherapy

SYSTEMIC PUVA:a) 8-MOP: 0.4–0.6 mg/kg. the initial dose of UVA is usually 0.5–
1.0 J/cm2, which is gradually until minimal asymptomatic erythema of the involved skin occurs. To the risk of the Koebner phenomenon, significant erythema (phototoxicity) is avoided.Inhibits mitosis by covalently binding to pyrimidine bases in DNA when photoactivated by UV-A.
b) 5-MOP: has about the same response rate as 8-MOP in repigmenting vitiligo, but a lower incidence of adverse effects, including reduced phototoxicity as well as less nausea and vomiting.
c) TMP: Because of weaker phototoxicity, it is preferred to 8 MOP for treatment with sunlight as the radiation source.
I. Phototherapy

SIDE EFFECTS OF PUVA:
1. PUVA-induced cutaneous carcinomas.
2. High risk of phototoxicity (e.g. blistering, koebnerization) from topical psoralen formulations.
3. Treatments stimulate the pigmentation of normal skin, which will intensify the contrast between normal and vitiliginous skin. (Application of sunscreen to the surrounding uninvolved skin prior to application of the topical psoralen can reduce hyperpigmented rims).
I. Phototherapy

4. KHELLIN PLUS UVA (KUVA): • Oral khellin as the photosensitizer [at a dose of 100
mg 2 hours before treatment] plus UVA or• Topical khellin [4-5% ointment] plus UVA
ADVANTAGES:a) Relatively low risk of phototoxicity. b) Safe for home treatment or treatment with natural sunlight. c) lower mutagenic activity than psoralens.
DISADVANTAGES:a) It requires a longer duration of treatment than oral PUVA or monochromatic excimer light (MEL) 308 nm.b) It requires a higher UVA doses than oral PUVA or monochromatic excimer light (MEL) 308 nm. c) Hepatic toxicity.
I. Phototherapy

EXCIMER LASER
II. Laser therapy

EXCIMER LASER• It produces monochromatic rays at 308 nm close to that of NB-UVB to treat limited (<30%
BSA), localized stable patches of vitiligo.• Twice weekly for an average of 24-48 sessions with the repigmentation rate depending on
total number of sessions, not frequency.
ADVANTAGES:1. Efficacious, 2. Safe 3. Well-tolerated
DISADVANTAGES:4. Expensive. 5. Erythema 6. (Rarely) blistering.
• Combination treatment with 0.1% tacrolimus ointment plus the 308-nm excimer laser is superior to 308-nm excimer laser monotherapy for the treatment of UV-resistant cases.
• Segmental vitiligo has a better repigmentation response with excimer laser treatment used at earlier stages of the disease.
II. Laser therapy

A. SYSTEMIC CORTICOSTEROIDS
B.TOPICAL CORTICOSTEROIDS
C. INTRALESIONAL CORTICOSTEROIDS
III.Corticosteroids

A. SYSTEMIC STEROIDS: • Side-effects associated with long-term use of daily
systemic corticosteroids contraindicate their common use.
• Prednisone has been used esp. to arrest rapidly progressive vitiligo, without inducing repigmentation.
• Steroids have been reported anecdotally to achieve success when given in:
a. Oral mini-pulsed (OMP) therapy (2.5-5 mg of dexamethasone on two consecutive days per week).
b.High-dose pulsed therapy
c. Low daily oral dose
III.Corticosteroids

B. TOPICAL STEROIDS: • Is often chosen first to treat localized vitiligo because it is
easy and convenient for both doctors and patients to maintain the treatment.
• The results of therapy have been reported as moderately successful, with either class 1 (superpotent) or class 2–3 (high-potency) particularly in patients with localized vitiligo and/or an inflammatory component to their vitiligo, even if the inflammation is subclinical.
• To minimize side effects, class 1 corticosteroids can be used as follow: In 6–8-week cycles. On a twice-weekly basis. Alternating with topical tacrolimus. Alternating with a less potent topical corticosteroid.
III.Corticosteroids

• Treatment should be discontinued if there’s no visible improvement after 2 m.
• In addition, these agents modify the body's immune response to diverse stimuli.
• These drugs’re used to stop spread of vitiligo & accomplish repigmentation.
EXAMPLES FOR TOPICAL STEROID AGENTS:
1.Hydrocortisone topical: An adrenocorticosteroid derivative suitable for application to skin or external mucous membranes. Has mineralocorticoid and glucocorticoid effects.
2.Triamcinolone topical: medium potency topical steroid.
3.Clobetasol Propionate: Class I superpotent
topical steroid.
III.Corticosteroids

C. INTRALESIONAL CORTICOSTEROIDS:
• Should be avoided because of the pain associated with injection and the risk of cutaneous atrophy that occurs in approximately one-third of vitiligo patients.
III.Corticosteroids

• Effective alternative therapy for vitiligo, particularly when the disease involves the head and neck.
• Act as Immunomodulators that suppress the activity of the immune system.
• Drugs of this class are more expensive than topical corticosteroids
• Combination treatment: Better results superior to monotherapy suggesting a synergistic effect1.Sun exposure.2.308-nm excimer laser 3.Narrow-band UV-B 4.Corticosteroids5.Microdermabrasion
IV. Topical calcineurin inhibitors (TCIs)


AGENTS:
1.Tacrolimus (0.03-0.1% ointment) Can be used in patients as young as 2 years old.Applied twice daily.
2.Pimecrolimus (1% cream) Originally approved for AD.More Expensive than tacrolimus.
IV. Topical calcineurin inhibitors (TCIs)

• Originally approved for psoriasis.• They target the local immune response and act on
specific T-cell activation. They do this by inhibition of the transition of T cells (early to late G1 phase) and inhibition of the expression of various proinflammatory cytokines that encode TNFα and IFγ.
• These vitamin D3 compounds influence melanocyte maturation and differentiation, in addition to up-regulating melanogenesis through pathways that are activated by specific ligand receptors (eg, endothelin receptor and c-kit).
• The combination of topical calcipotriene and narrow-band UV-B or PUVA results in improvement appreciably better than that achieved with monotherapy.
V. Vitamin D analogs

AGENTS:
1.Calcipotriene (calcipotriol) 0.005% Synthetic vitamin D-3 analog that regulates skin cell production and development. Has immunosuppressive effects on lymphoid cells.
2.Tacalcitol excessive skin cell turnover.
V. Vitamin D analogs

• In widespread & progressive vitiligo (BSA > 50%) with only a few areas of normally pigmented skin in exposed sites & repigmentation do not produce satisfactory results.
• The patients must be carefully chosen, i.e. adults who recognize that their appearance will be altered significantly and who understand that procedure generally results in permanent depigmentation & requires lifelong strict photoprotection (e.g. sunscreens, clothing, umbrellas).
• Depigmentation may be chemical or physical.•
VI. Depigmentation therapy

CHEMICAL DEPIGMENTATION:1.Monobenzyl ether of
hydroquinone (MBEH) (20%), the only FDA approved for depigmentation. The MC used agent is applied once to twice daily to the affected areas for 9–12 months or longer.
2.Monomethyl ether of hydroquinone (20%) cream can be used as analternative to MBEH. S.E. include contact dermatitis, exogenous ochronosis and leukomelanoderma en confetti.
VI. Depigmentation therapy

PHYSICAL DEPIGMENTATION:1.Q-switched lasers:
Q-switched ruby laser therapy was reported to achieve faster depigmentation than that achieved with a bleaching agent, and this laser has also been used in combination with topical 4-methoxyphenol to induce depigmentation. Q-switched alexandrite laser has also been described
2.Cryotherapy.
VI. Depigmentation therapy

• Autologous transplantation.
• Surgical treatment for vitiligo can be considered in two main categories:
A.Grafting of melanocyte-rich tissue (tissue grafting)
B.Grafting of melanocyte cells (cellular grafting).
• Limited to stable vitiligo.
• Segmental vitiligo has been shown as the most stable form, responding well to surgical interventions.
VII. Surgical therapies

SELECTION CRITERIA: “6”
1. Stable disease for at least 6-12 months (Spontaneous repigmentation indicates vitiligo inactivity)
2. Unsatisfactory response to medical therapy
3. Absence of the Koebner phenomenon
4. A positive minigrafting test (retention/spread of pigment at the recipient site and no koebnerization at the donor site after 2–3 months), disclosing repigmentation at 4-5 minigrafts, which, to date, is the most accurate evidence of vitiligo stability
5. No tendency for scar or keloid formation,
6. Age > 12 years
VII. Surgical therapies

• Uppermost layer of affected skin is usually removed under local anaesthesia in an outpatient setting. Techniques to remove the skin include:
1. Cryotherapy
2. Dermabrasion
3. Shave biopsy
4. Punch biopsy
5. Laser therapy
VII. Surgical therapies

BASIC METHODS FOR REPIGMENTATION SURGERY HAVE BEEN DESCRIBED, AS FOLLOWS: “6”
1. Punch Minigrafting
2. Noncultured epidermal cell suspensions
3. Thin dermoepidermal grafts
4. Suction epidermal grafting
5. Cultured epidermis with melanocytes or cultured melanocyte suspensions
6. Grafting of individual hairs
VII. Surgical therapies

1. Punch Minigrafting: the simplest technique. Small Punch donor grafts (1–2 mm) are inserted into the incision of recipient sites separated from each other by 5–8 mm and held in place by a pressure dressing. The graft heals readily and begins to show repigmentation within 4-6 weeks. The cosmetic result is excellent.
VII. Surgical therapies


POTENTIAL IMMEDIATE COMPLICATIONS OF MINIATURE PUNCH GRAFTING: 1. Loss of graft tissue2. Infection MID- TO LONG-TERM COMPLICATIONS:3. Persistent vitiligo 4. Hyperpigmentation5. Colour matching6. Graft rejection7. Peripheral depigmentation (halo effect)8. Keloid and hypertrophic scar at the donor or graft site
(cosmetically insensitive areas are chosen). 9. Cobblestone appearance (more common with larger punch
biopsies)
VII. Surgical therapies

2. Noncultured epidermal cell suspensions:
• After the achromic epidermis is removed, an epidermal suspension with melanocytes and keratinocytes previously prepared by trypsinization of normally pigmented donor skin is spread onto the denuded area and immediately covered with nonadherent dressings.
• Using noncultured epidermal cellular grafts, especially in segmental vitiligo, piebaldism, and halo nevi.
• Color mismatches were common, and generalized vitiligo did not repigment quite as well.
VII. Surgical therapies


3. Thin dermoepidermal grafts:
• The depigmented epidermis is removed by superficial dermabrasion, including the papillary dermis, and very thin dermoepidermal sheets harvested with dermatome (skin graft knife) are grafted onto the denuded skin.
VII. Surgical therapies

4. Suction epidermal grafting:
• Epidermal grafts can be obtained by vacuum suction, usually with -150 mm Hg.
• The recipient site can be prepared by suction, freezing, or dermabrasion of the sites 24 hours before grafting.
• The depigmented blister roof is discarded, and the epidermal donor graft is placed on the vitiliginous areas.
• Advantages of suction blister epidermal grafting are the absence of scarring at the donor site and the possibility of reusing this area. However, failure of the graft to take and koebnerization may occur.
VII. Surgical therapies

5. Cultured epidermis with melanocytes or cultured melanocyte suspensions:
• Depigmented skin is removed using liquid nitrogen, superficial dermabrasion, thermosurgery, or CO2 lasers.
• Very thin sheets of cultured epidermis are grafted or suspensions are spread onto the denuded surface.
VII. Surgical therapies
• Grafting of cultured autologous melanocytes is an expensive technique that requires specialized laboratory expertise; grafts consist of pure melanocytes or melanocytes admixed with keratinocytes.
• Involves mitogens to enhance cell growth.

6. Grafting of individual hairs
VII. Surgical therapies

• Permanent dermal Micropigmentation to camouflage recalcitrant areas of vitiligo.
• Tattooing can be used to repigment depigmented skin in dark-skinned individuals.
• Non-allergenic iron oxide pigment / dihydroxyacetone preparations.
• In areas with poor rate of repigmentation e.g. the lips, nipples and distal fingers.
• The color may not match perfectly with the normal surrounding skin.
• The result is immediate and can represent a dramatic aesthetic improvement.
• The color may fade slightly over a period of years.
VIII. Micropigmentation


• The rationale for this treatment is based on the hypothesis that accumulation of hydrogen peroxide leads to pathogenic inactivation of catalase (Its functions include catalyzing the decomposition of H2O2 to H2O and O2) in the skin of patients with vitiligo.
• Topical pseudocatalase and calcium twice daily plus UVB twice weekly, with may induce repigmentation at 2–4 months.
IX. Pseudocatalase with narrowband UVB

• The rationale for this approach rests on the hypothesis that vitiligo results from a deficiency of natural antioxidant mechanisms.
EXAMPLES:1. Selenium
2. Methionine
3. Tocopherols (Vit. E)
4. Ascorbic acid (Vit. C)
5. Ubiquinone (Coenzyme Q)
X. Systemic antioxidant therapy

• Erbium: YAG laser ablation of vitiligo lesions followed by topical application of 5-fluorouracil and NB-UVB therapy twice weekly for 4 months.
XI. Dermabrasion followed by topical 5-FU & NB-UVB

• Prostaglandin E2
• Prostaglandin analogues eg. Latanoprost
XII. Topical prostaglandins

Guidelines for the Management of VitiligoThe European Dermatology Forum Consensus


References
• Dr. Angelo Smith M.D WHPL
• Mohammad Jafferany Ajyad general hospital Makkah.
• Bolognia 3rd ed.
• http://www.edoj.org
• http://www.e-ijd.org
• http://www.medscape.com

THANK YOU