Embed Size (px)
Citation preview
بسم هللا الرحمن الرحيم

Dr. Ahmed Abdallah Eisawy
MBBS M.Sc MD
• Adults: Do not eat or drink 8 hours before exam.
• Children: Do not eat or drink 4 hours before study or skip 1 meal.
• Necessary medications may be taken with a small amount of water only.
• No chewing gum.
• The choice of transducer for bowel assessment largely depends on the patient's body habitus and
the distance between the probe and the object of study.
For a regular scan of the abdomen: > abdominal transducer (2-5 MHz) For a detailed examination of the intestine: > A 2.5- to 5.0-MHz curvilinear probe is used for a
heavy patient, obese patients . > A 5.0- to 10.0-MHz linear transducer For average-size
and thin patients, which facilitates high-resolution sonography, is used for an average-size or thin patient and generally for assessment of superficial abnormalities.
• In patients with localized abdominal pain, the sonographic
examination can be started at the point of maximum tenderness.
• An area of interest is carefully analyzed with a high-resolution linear probe and graded compression sonography if possible.
• The compression resembles palpation of the abdomen. Gentle but adequate graded compression is applied to decrease the distance between the probe and the area of interest and to displace gas and fecal material.
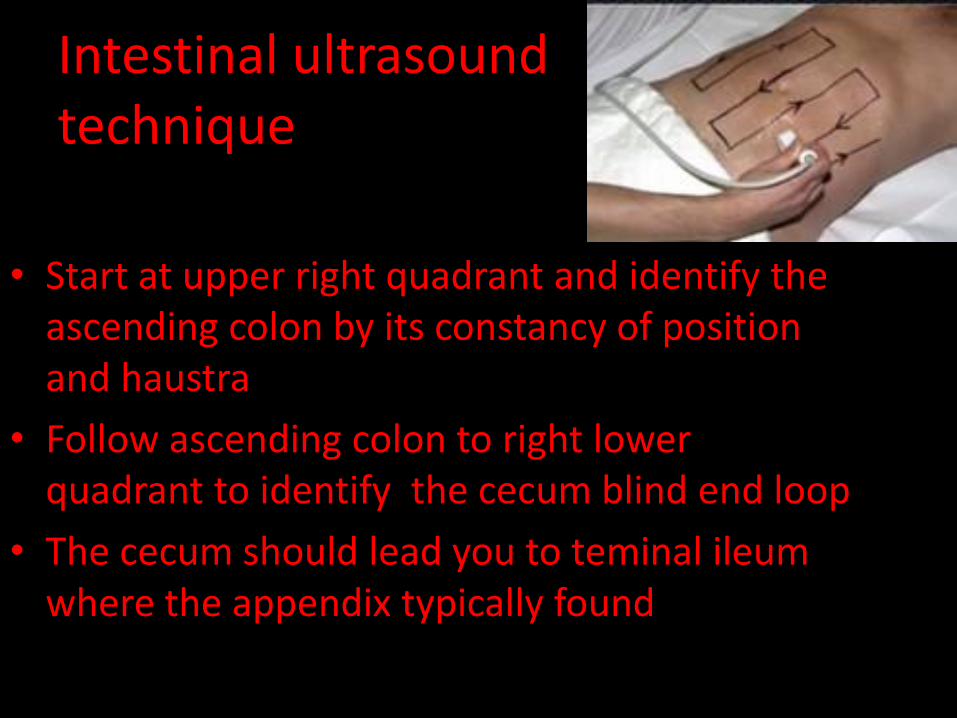
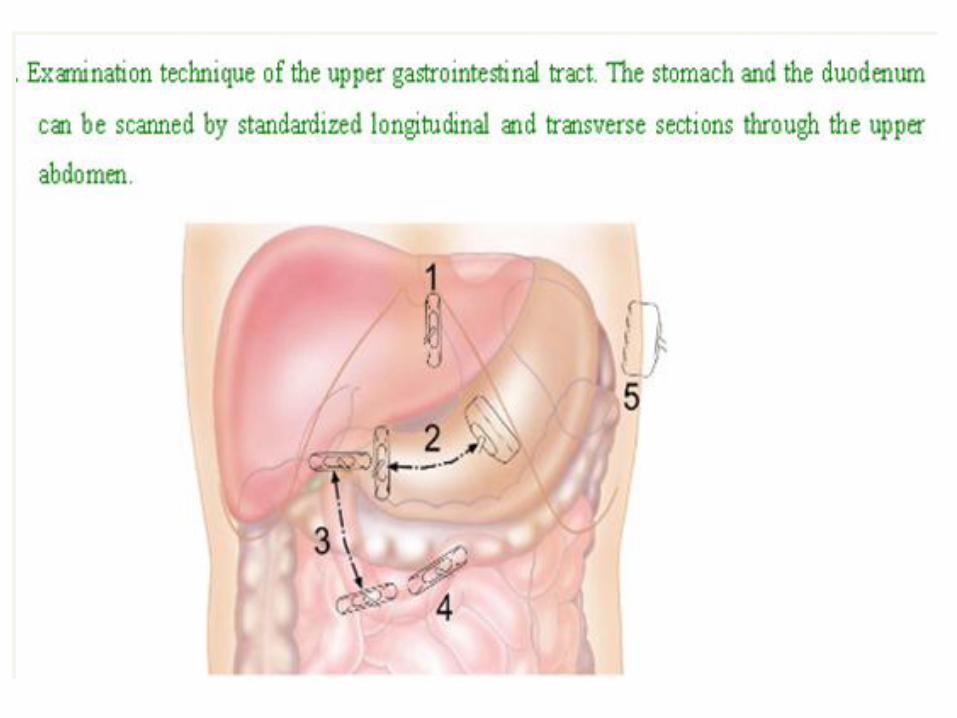
Intestinal ultrasound technique
• Start at upper right quadrant and identify the ascending colon by its constancy of position and haustra
• Follow ascending colon to right lower quadrant to identify the cecum blind end loop
• The cecum should lead you to teminal ileum where the appendix typically found
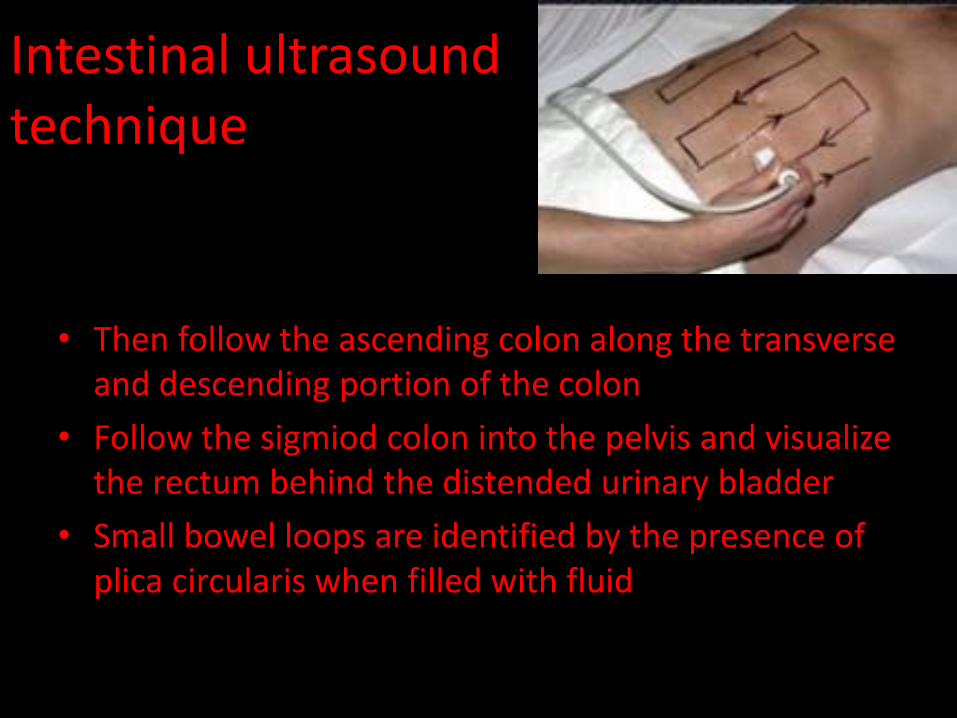
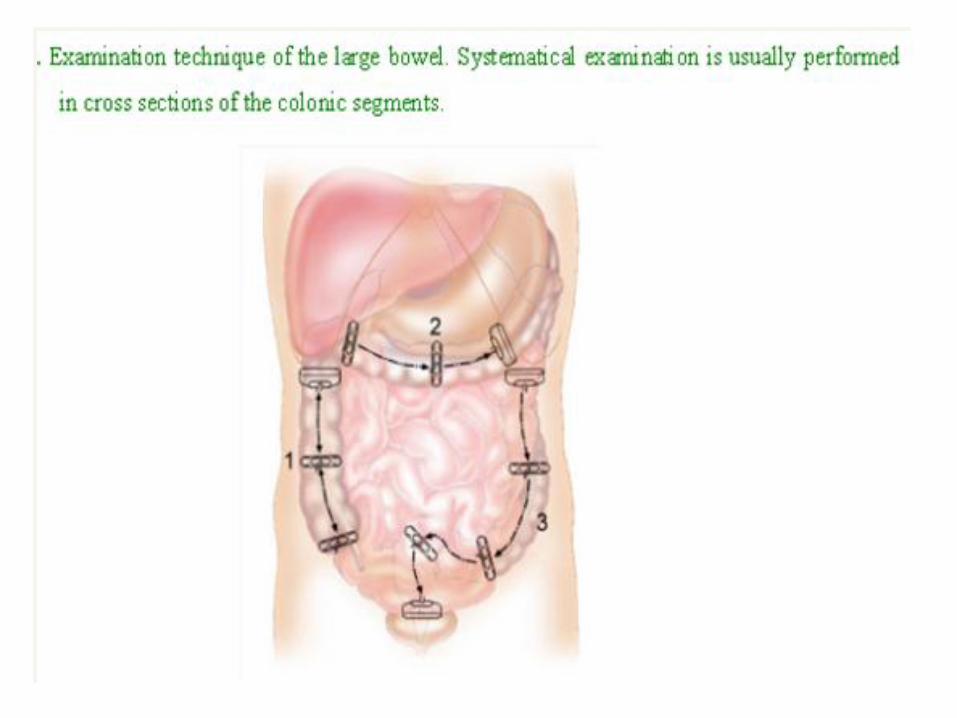
Intestinal ultrasound technique
• Then follow the ascending colon along the transverse and descending portion of the colon
• Follow the sigmiod colon into the pelvis and visualize the rectum behind the distended urinary bladder
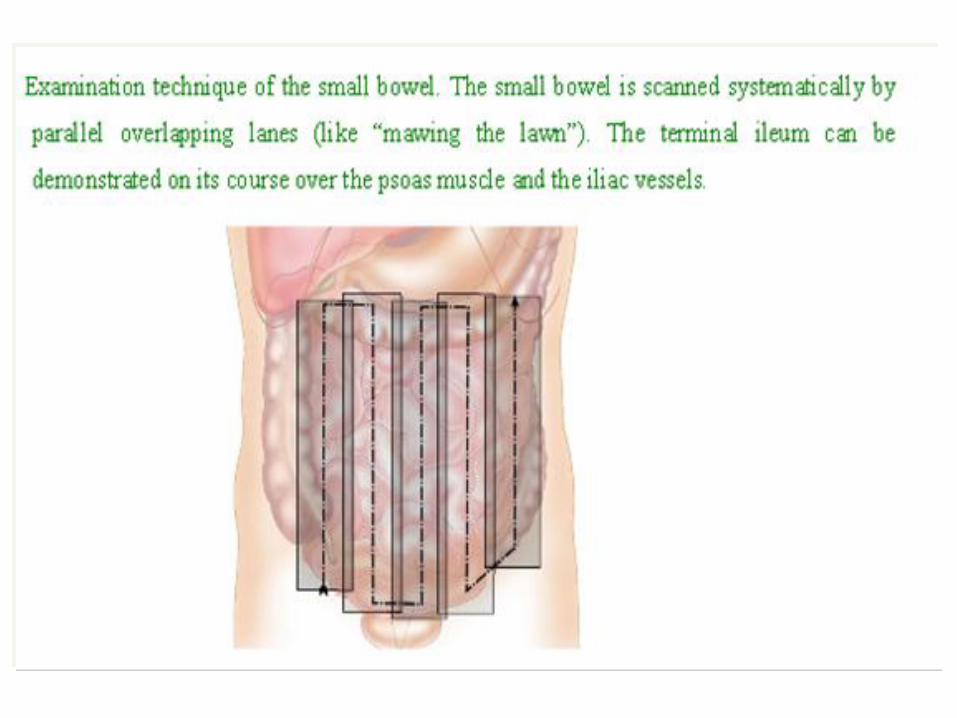
• Small bowel loops are identified by the presence of plica circularis when filled with fluid
overcoming
• Have the patient crossing their right leg over left as far as possible without rolling their hip off the table
• Push hard to compress air filled loops
• Adequate short acting analgesic agent like fentanyl
• Diseased states of intestine result in decrease peristalsis and bowel wall thickening resulting in decrease luminal gas content
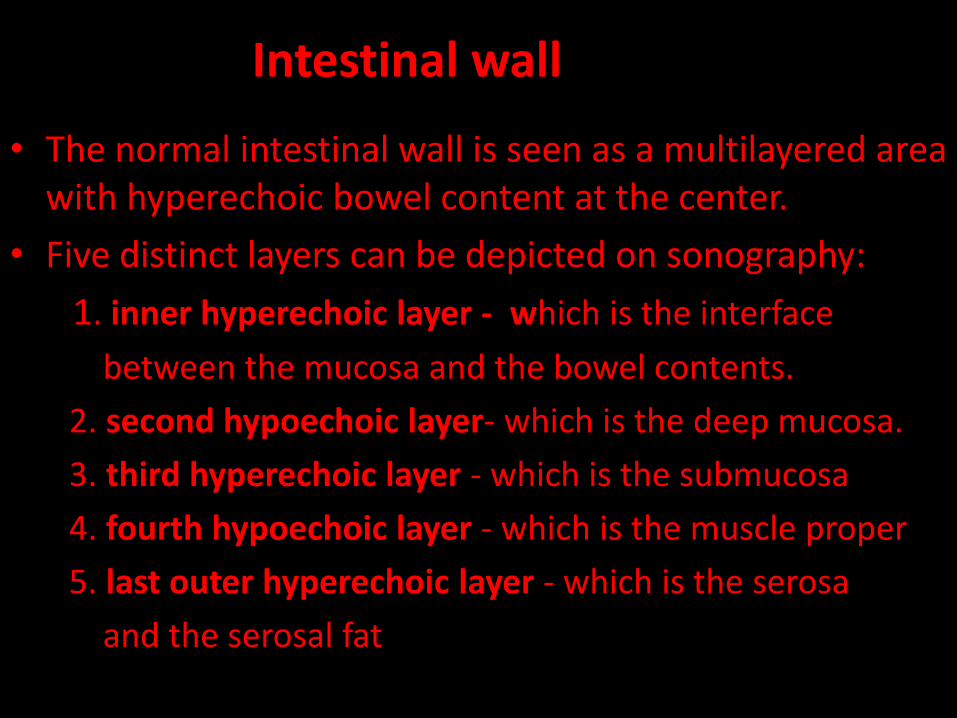
Intestinal wall
• The normal intestinal wall is seen as a multilayered area with hyperechoic bowel content at the center.
• Five distinct layers can be depicted on sonography:
1. inner hyperechoic layer - which is the interface
between the mucosa and the bowel contents.
2. second hypoechoic layer- which is the deep mucosa.
3. third hyperechoic layer - which is the submucosa
4. fourth hypoechoic layer - which is the muscle proper
5. last outer hyperechoic layer - which is the serosa
and the serosal fat
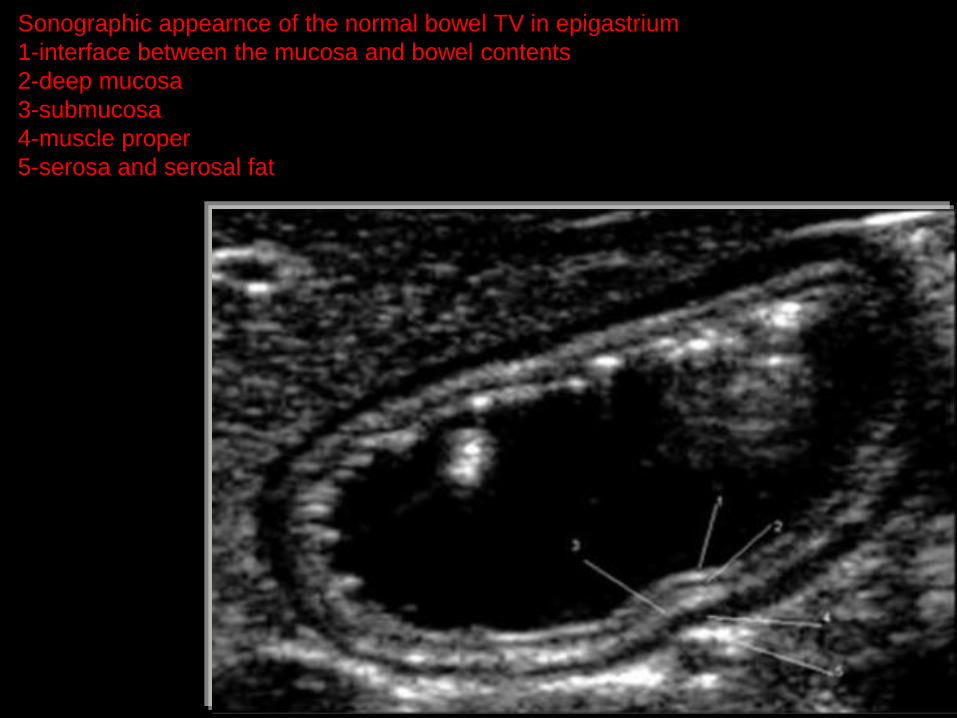
Sonographic appearnce of the normal bowel TV in epigastrium
1-interface between the mucosa and bowel contents
2-deep mucosa
3-submucosa
4-muscle proper
5-serosa and serosal fat
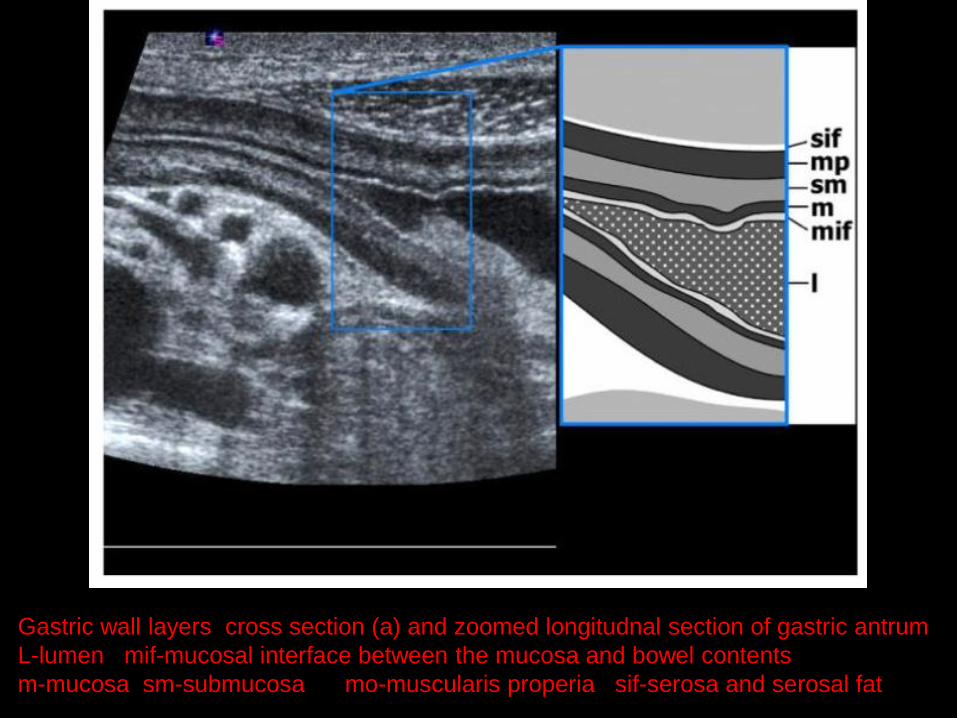
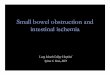
Gastric wall layers cross section (a) and zoomed longitudnal section of gastric antrum
L-lumen mif-mucosal interface between the mucosa and bowel contents
m-mucosa sm-submucosa mo-muscularis properia sif-serosa and serosal fat
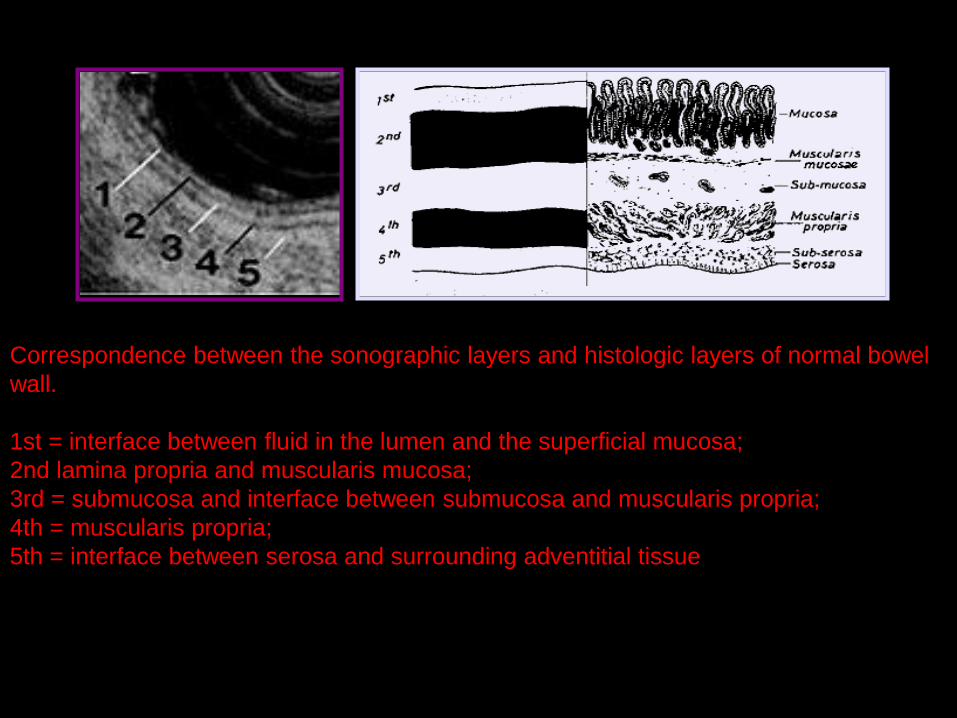
Correspondence between the sonographic layers and histologic layers of normal bowel
wall.
1st = interface between fluid in the lumen and the superficial mucosa;
2nd lamina propria and muscularis mucosa;
3rd = submucosa and interface between submucosa and muscularis propria;
4th = muscularis propria;
5th = interface between serosa and surrounding adventitial tissue
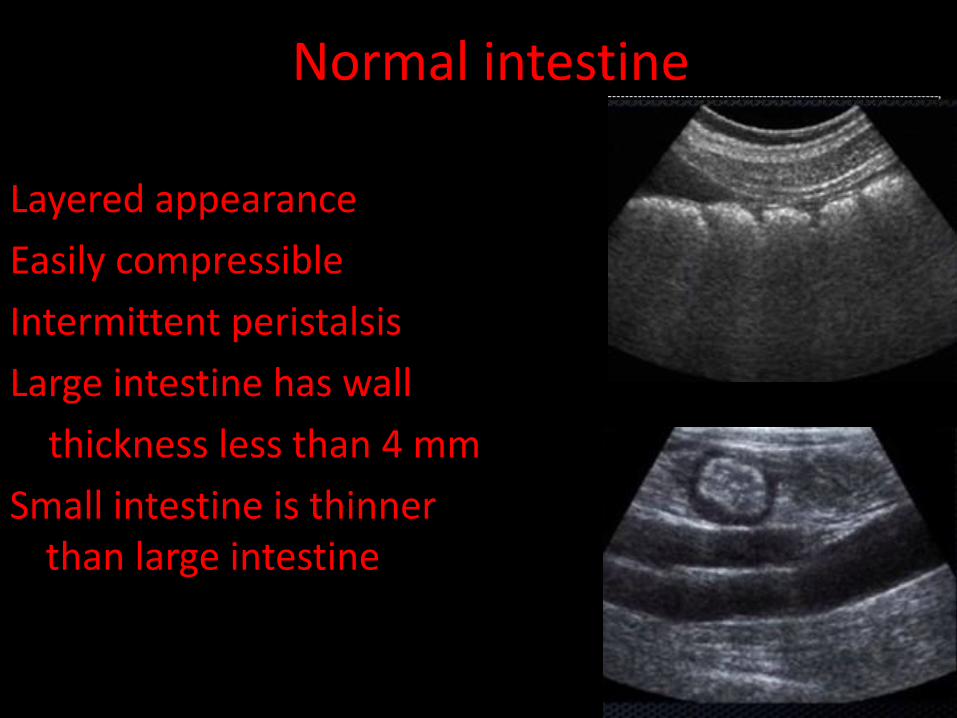
Normal intestine
Layered appearance
Easily compressible
Intermittent peristalsis
Large intestine has wall
thickness less than 4 mm
Small intestine is thinner than large intestine
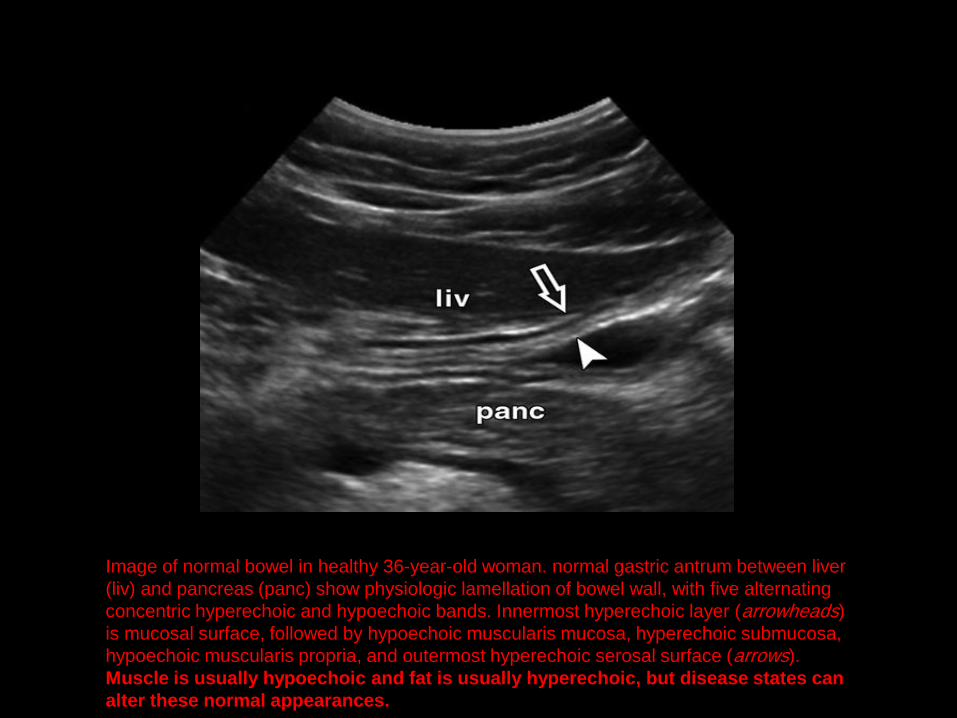
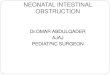
Image of normal bowel in healthy 36-year-old woman. normal gastric antrum between liver
(liv) and pancreas (panc) show physiologic lamellation of bowel wall, with five alternating
concentric hyperechoic and hypoechoic bands. Innermost hyperechoic layer (arrowheads)
is mucosal surface, followed by hypoechoic muscularis mucosa, hyperechoic submucosa,
hypoechoic muscularis propria, and outermost hyperechoic serosal surface (arrows).
Muscle is usually hypoechoic and fat is usually hyperechoic, but disease states can
alter these normal appearances.
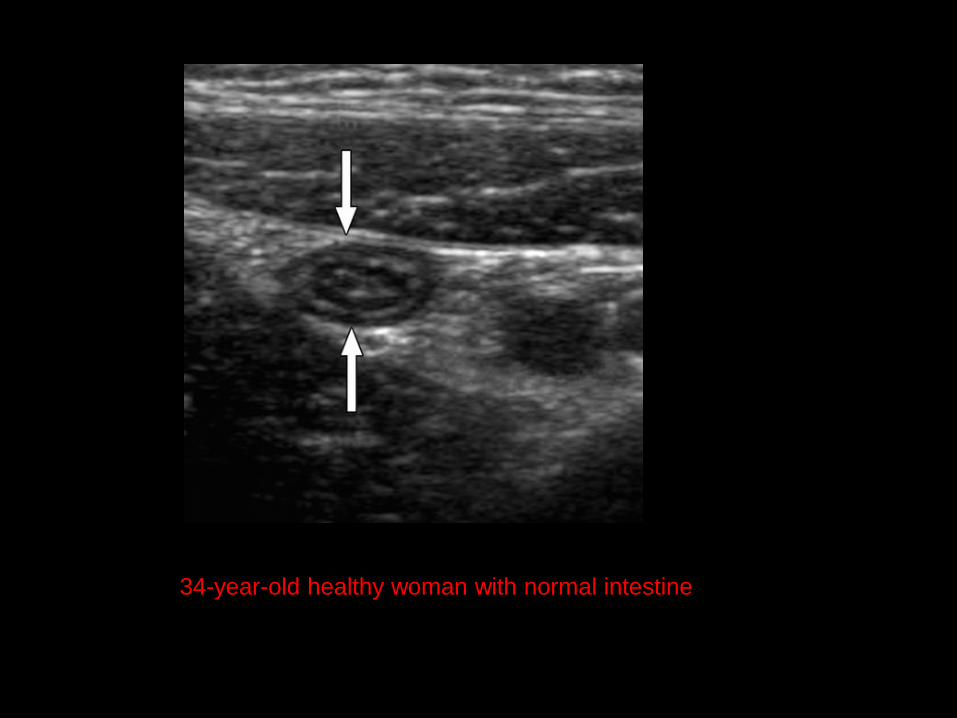
34-year-old healthy woman with normal intestine
• This pattern allows to distinguish bowel from adjacent structures
• Disruption of the pattern aids the diagnosis of bowel pathology
• Masses may transgress the layers
• Edema may expand certain layers or obscure the margins
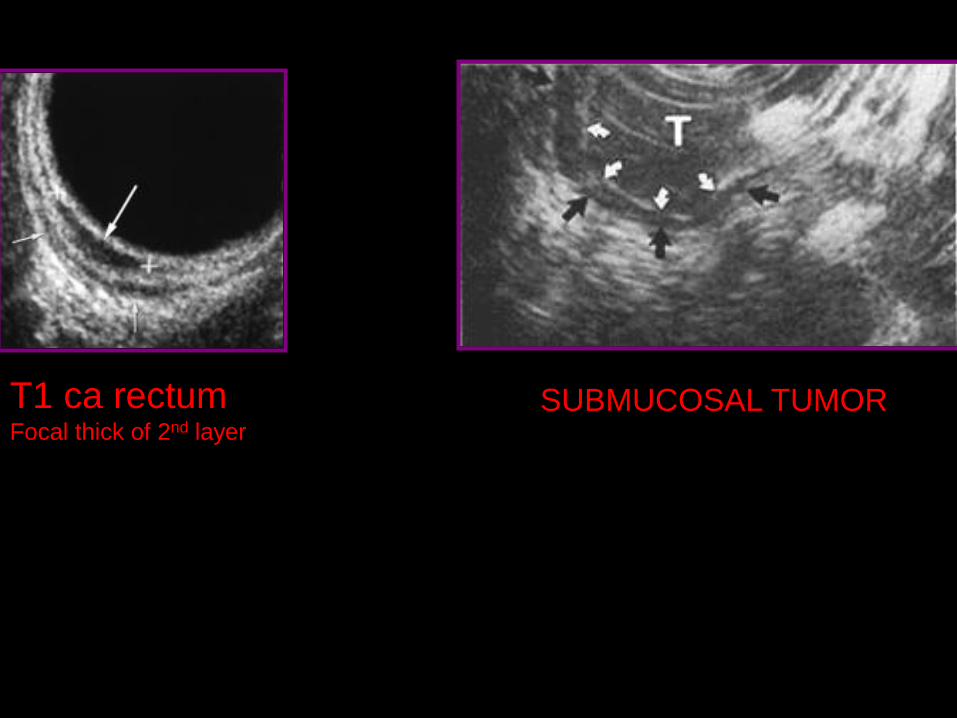
T1 ca rectum
Focal thick of 2nd layer
SUBMUCOSAL TUMOR
Non IR
Non invasive
No contrast media
Bowel wall layers
Extramural components
Expertise
Technical difficulties:gas
distention
Advantages
Limitations
Ultrasonography
Special technique
• Doppler Vascularity
• Dynamic Imaging
• Compression
• Valsalva Maneuver
• Focused Scanning
• Transvaginal Imaging
Doppler Vascularity
• increased vascularity in inflammatory and infectious diseases.
• Hyperemia, both of bowel wall and adjacent mesentery, is in inflammatory bowel disease.
• diminished vascularity is sign of ischemia
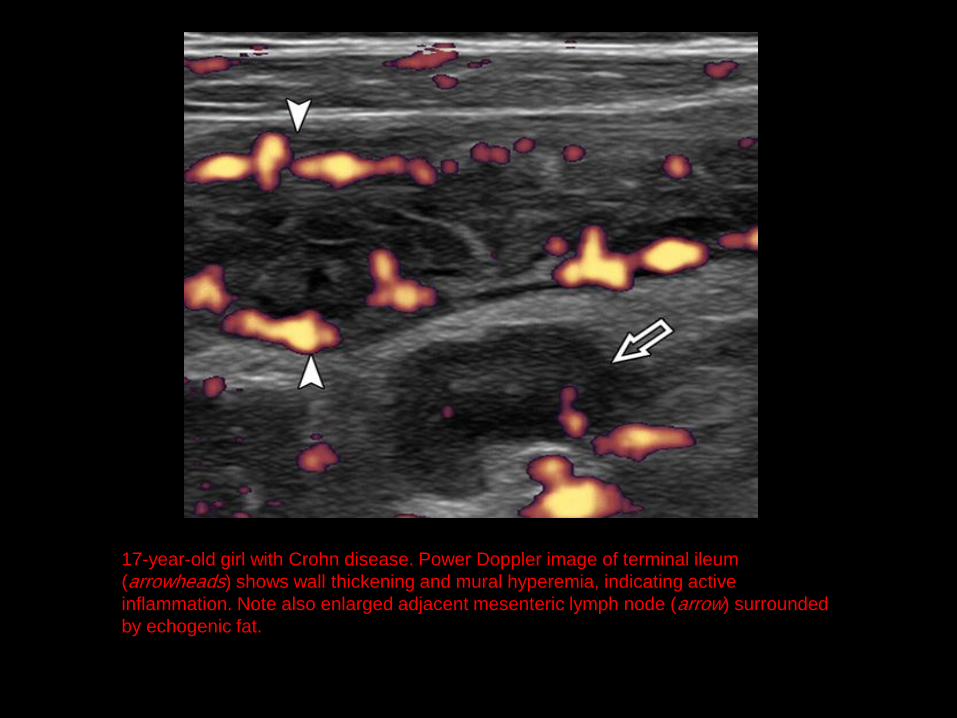
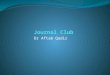
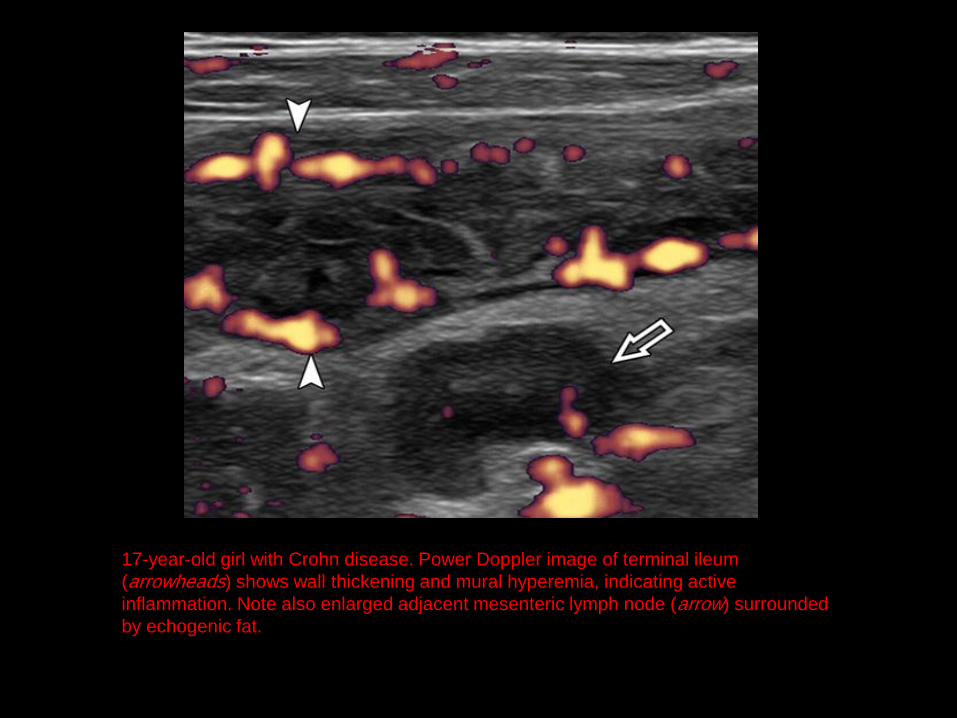
17-year-old girl with Crohn disease. Power Doppler image of terminal ileum
(arrowheads) shows wall thickening and mural hyperemia, indicating active
inflammation. Note also enlarged adjacent mesenteric lymph node (arrow) surrounded
by echogenic fat.
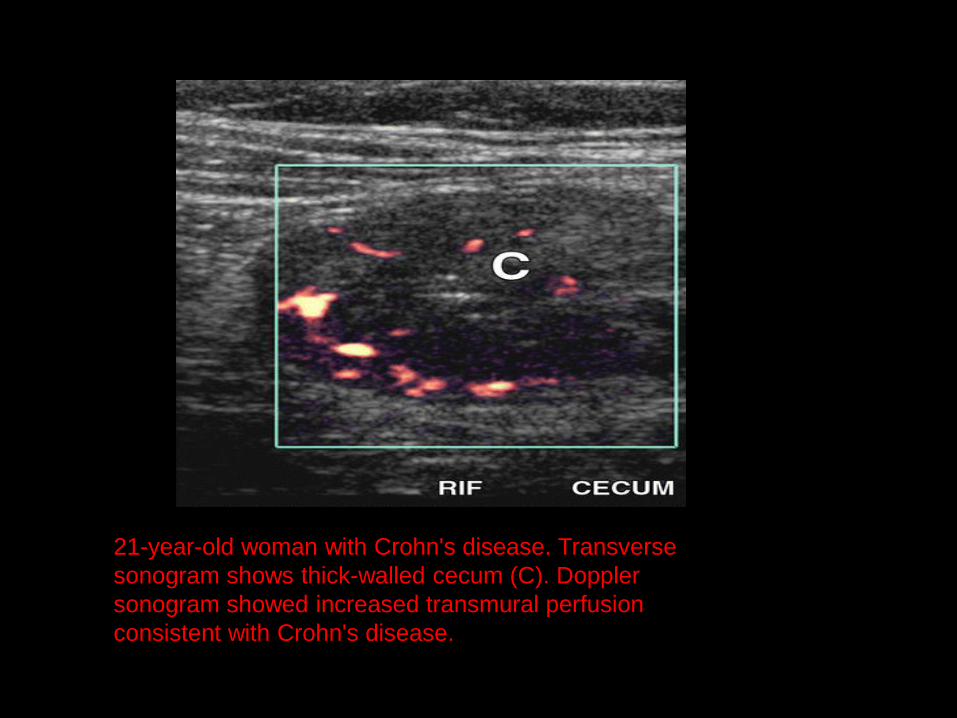
21-year-old woman with Crohn's disease. Transverse
sonogram shows thick-walled cecum (C). Doppler
sonogram showed increased transmural perfusion
consistent with Crohn's disease.
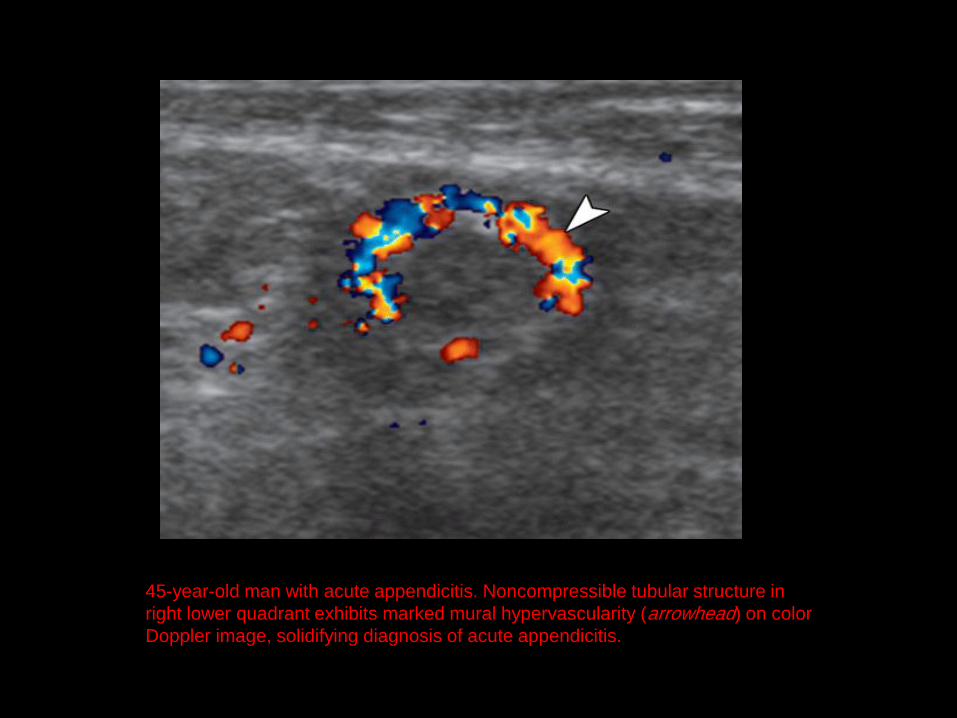
45-year-old man with acute appendicitis. Noncompressible tubular structure in
right lower quadrant exhibits marked mural hypervascularity (arrowhead) on color
Doppler image, solidifying diagnosis of acute appendicitis.
1. Peristalsis
2. Compression
3. Valsalva Maneuver
Dynamic Imaging
Real-time imaging is a unique strength of ultrasound Cine clips
Peristalsis
• impair peristalsis
small-bowel obstruction
Ischemia
enteritis
infiltrative processes
Compression
• Healthy bowel can be compressed and shifted by transducer pressure.
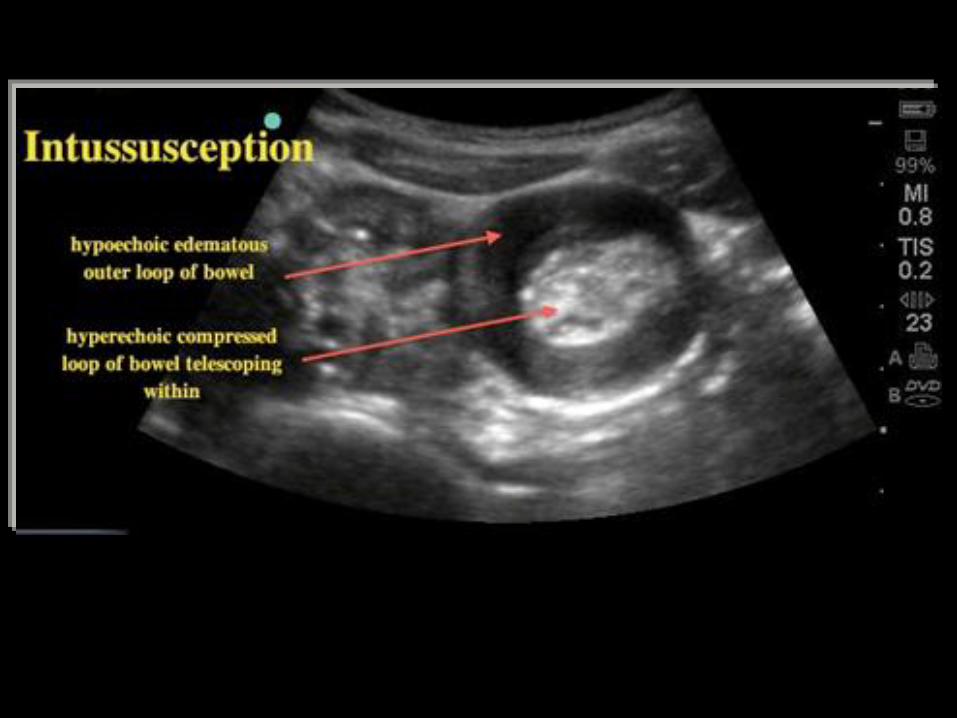
• lack of normal compressibility in appendicitis, intussusception
• The graded-compression technique enables isolation of abnormal bowel loops by pushing away adjacent mobile bowel.
•
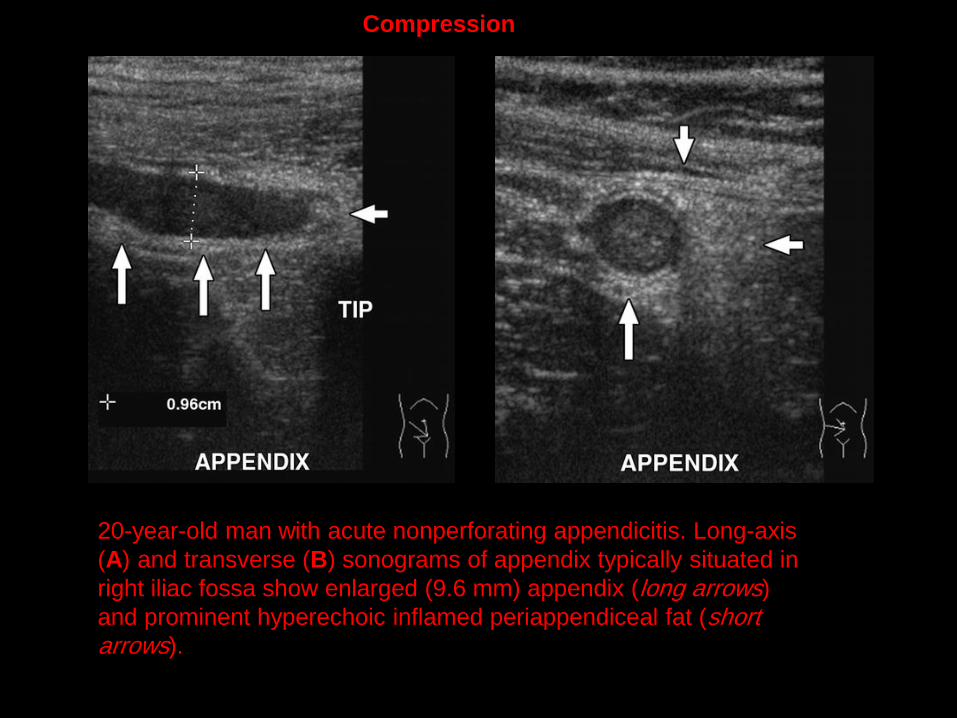
20-year-old man with acute nonperforating appendicitis. Long-axis
(A) and transverse (B) sonograms of appendix typically situated in
right iliac fossa show enlarged (9.6 mm) appendix (long arrows)
and prominent hyperechoic inflamed periappendiceal fat (short arrows).
Compression
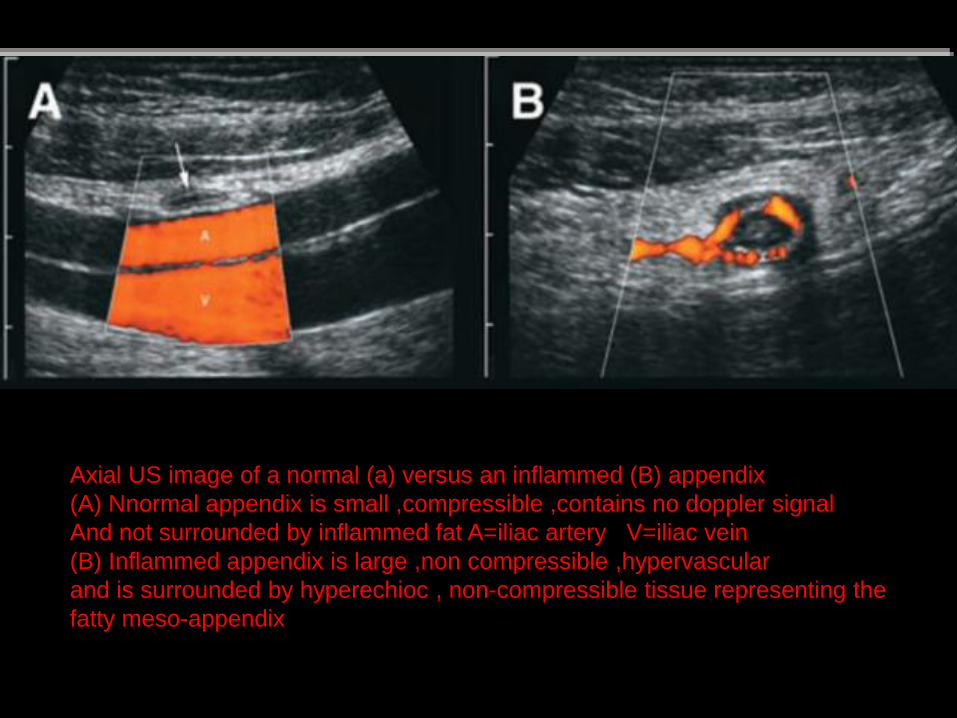
Axial US image of a normal (a) versus an inflammed (B) appendix
(A) Nnormal appendix is small ,compressible ,contains no doppler signal
And not surrounded by inflammed fat A=iliac artery V=iliac vein
(B) Inflammed appendix is large ,non compressible ,hypervascular
and is surrounded by hyperechioc , non-compressible tissue representing the
fatty meso-appendix
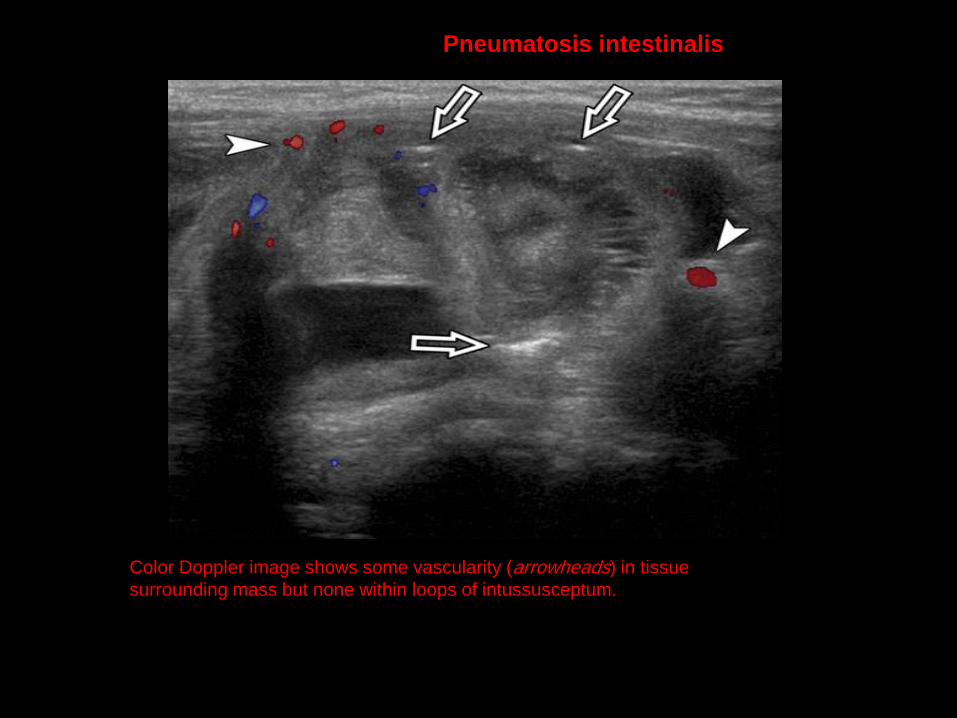
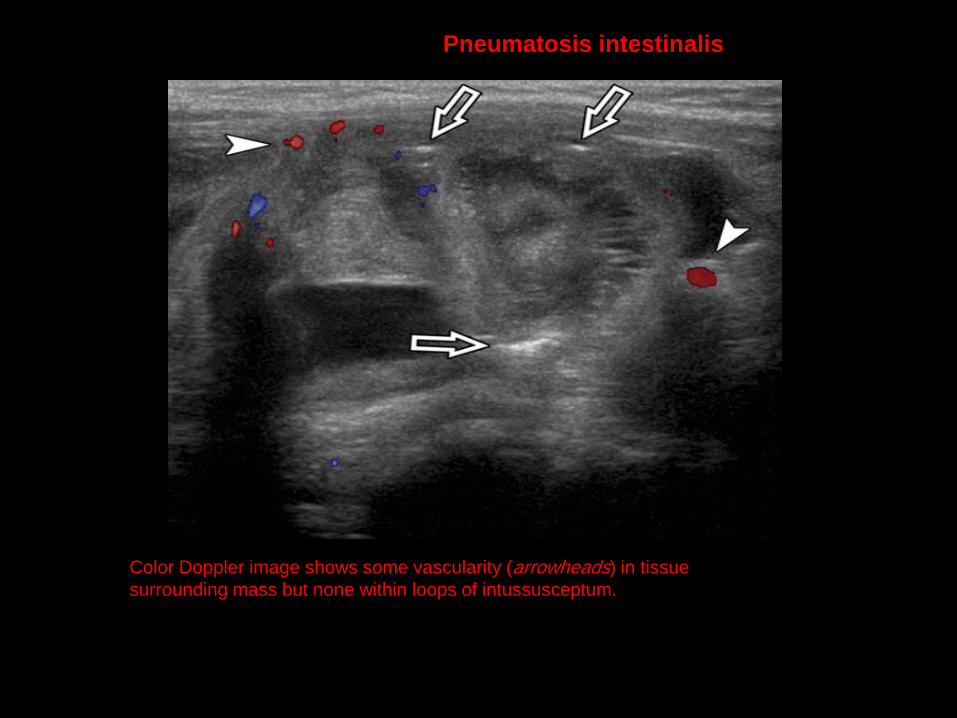
Color Doppler image shows some vascularity (arrowheads) in tissue
surrounding mass but none within loops of intussusceptum.
Pneumatosis intestinalis
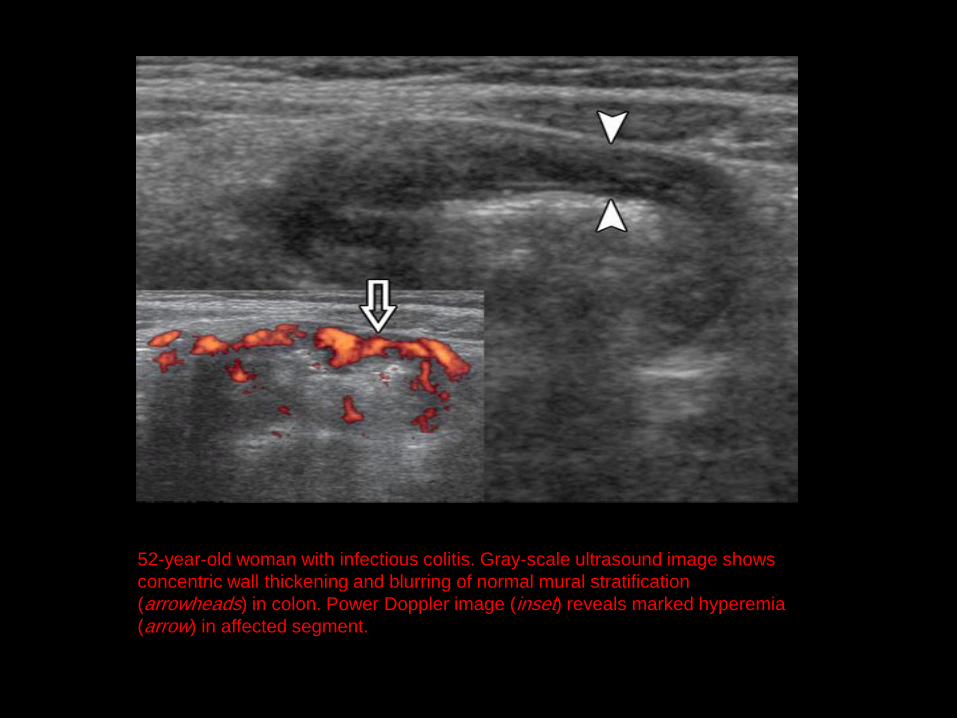
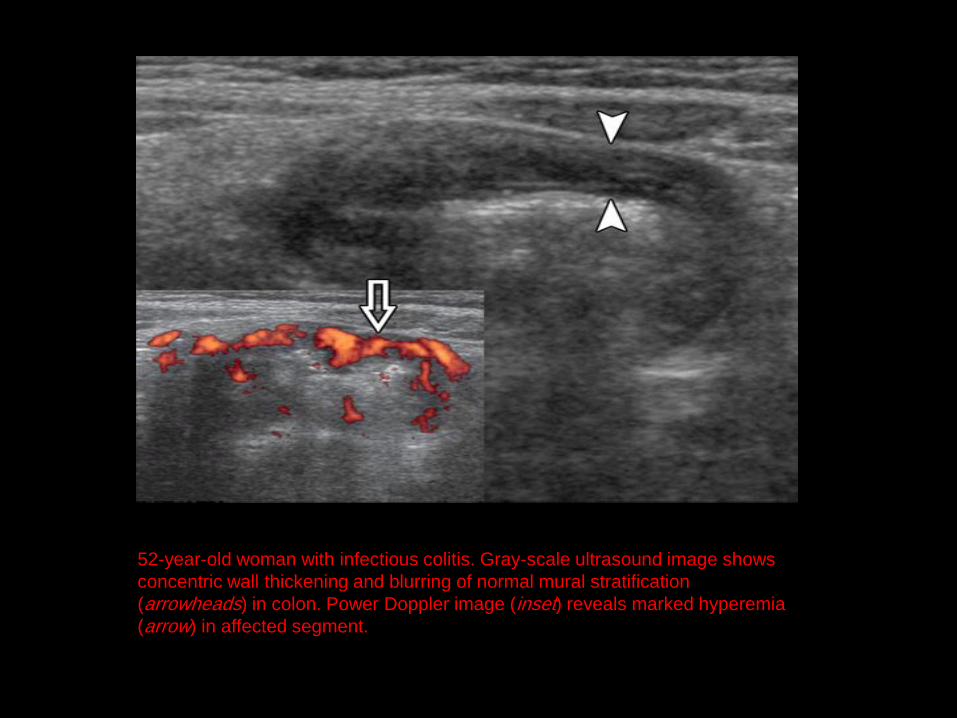
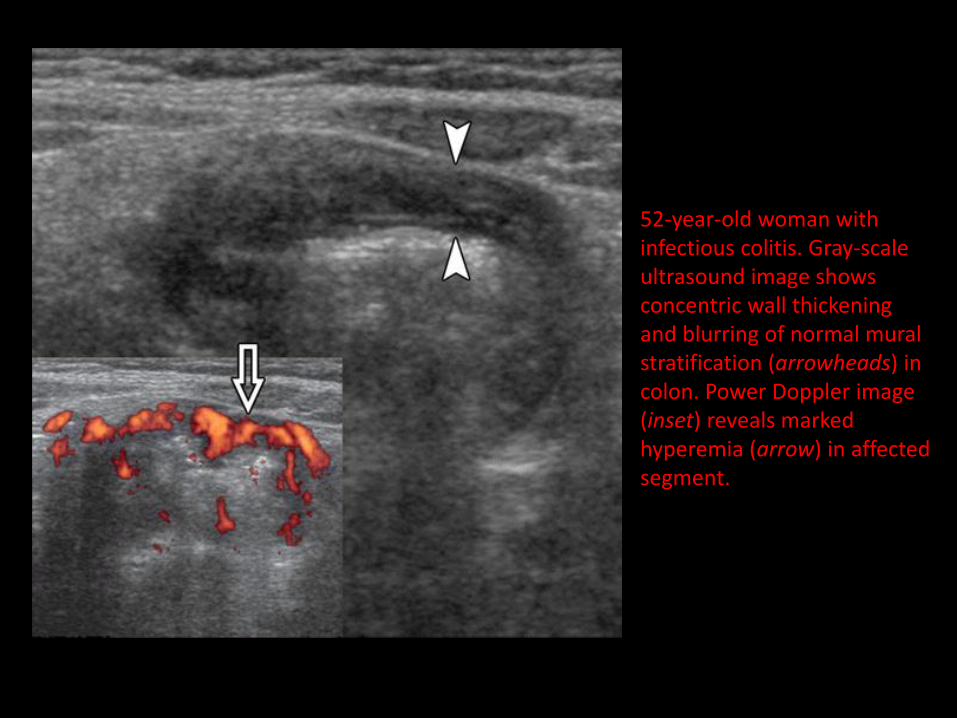
52-year-old woman with infectious colitis. Gray-scale ultrasound image shows
concentric wall thickening and blurring of normal mural stratification
(arrowheads) in colon. Power Doppler image (inset) reveals marked hyperemia
(arrow) in affected segment.
Valsalva Maneuver
• Hernias of bowel, mesentery, and omentum
• direct observation while the patient coughs or “bears down” to increase intraabdominal pressure
• Such maneuvers may reveal an intermittent hernia, show contiguity of a mass with the intraperitoneal space
• allow better depiction of the hernia sac or abdominal wall defect, and show reducibility .
• High-frequency linear transducers (≥ 7 MHz) are most appropriate for this evaluation.
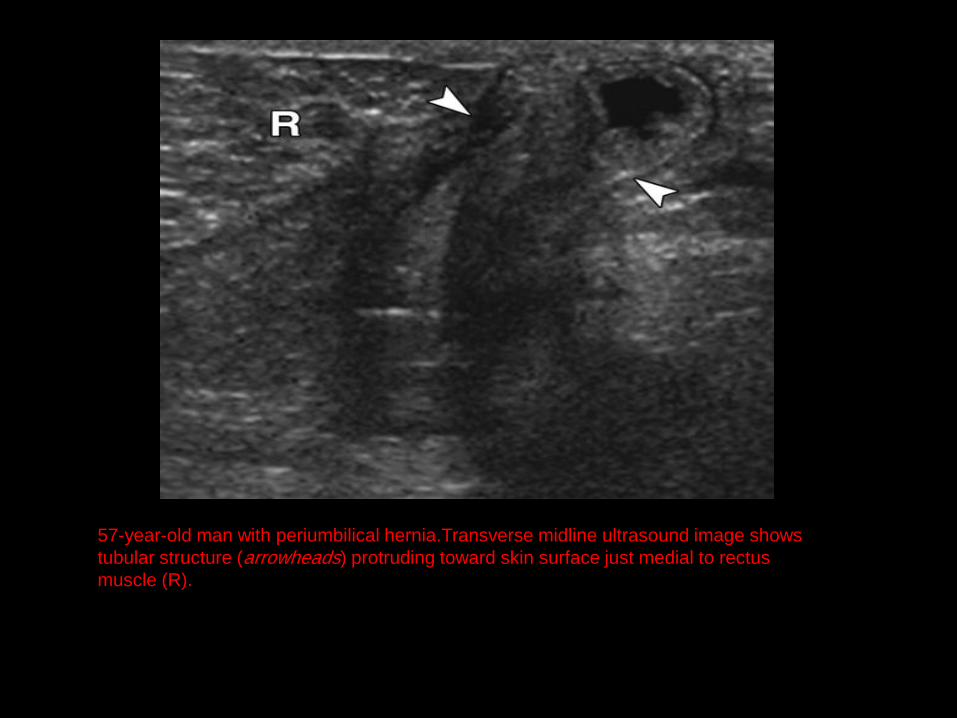
57-year-old man with periumbilical hernia.Transverse midline ultrasound image shows
tubular structure (arrowheads) protruding toward skin surface just medial to rectus
muscle (R).

57-year-old man with periumbilical hernia.Ultrasound image shows
bulge changes and enlarges (arrowheads) with Valsalva maneuver,
compatible with hernia. Some peristalsis was appreciable in real
time, confirming bowel content in hernia sac.
Focused Scanning
• extremely useful, particularly if the patient is able to localize the symptoms.
• superficial lesions, high-frequency linear transducers may be most appropriate (7–10 MHz)
• high-frequency linear transducers for detailed assessment of bowel wall and mesentery
• lower-frequency curved-array imaging (3–8 MHz) to evaluate the complete deep extent of lesions.
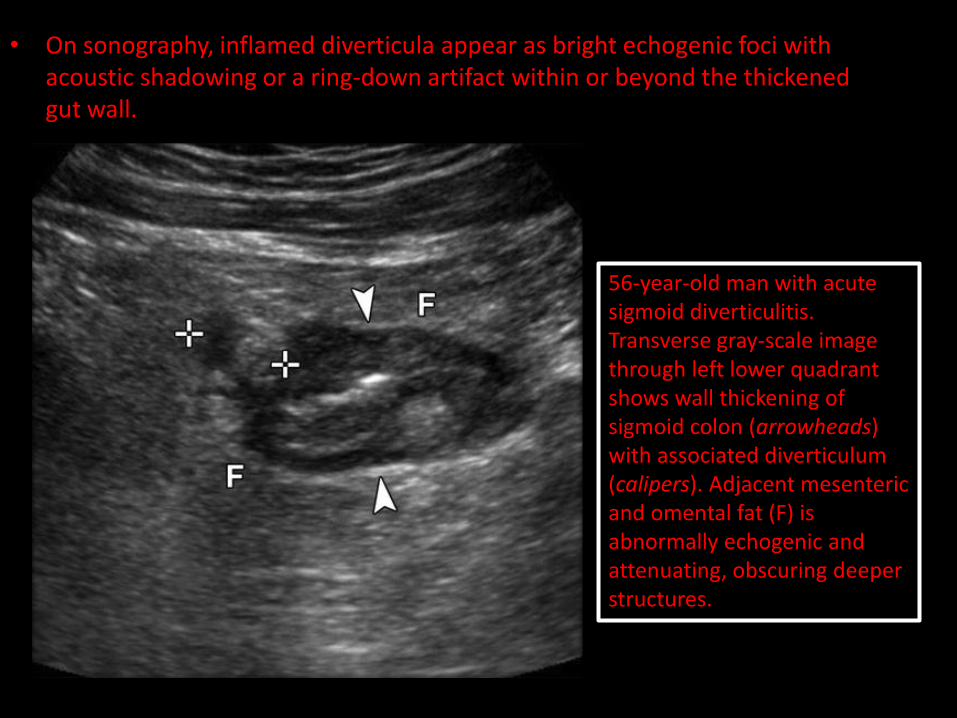
• On sonography, inflamed diverticula appear as bright echogenic foci with acoustic shadowing or a ring-down artifact within or beyond the thickened gut wall.
56-year-old man with acute sigmoid diverticulitis. Transverse gray-scale image through left lower quadrant shows wall thickening of sigmoid colon (arrowheads) with associated diverticulum (calipers). Adjacent mesenteric and omental fat (F) is abnormally echogenic and attenuating, obscuring deeper structures.
Transvaginal Imaging
• Deeply positioned appendixes may be best visualized transvaginally
• terminal ileitis
• sigmoid or rectal inflammation
• pelvic masses or abscesses,
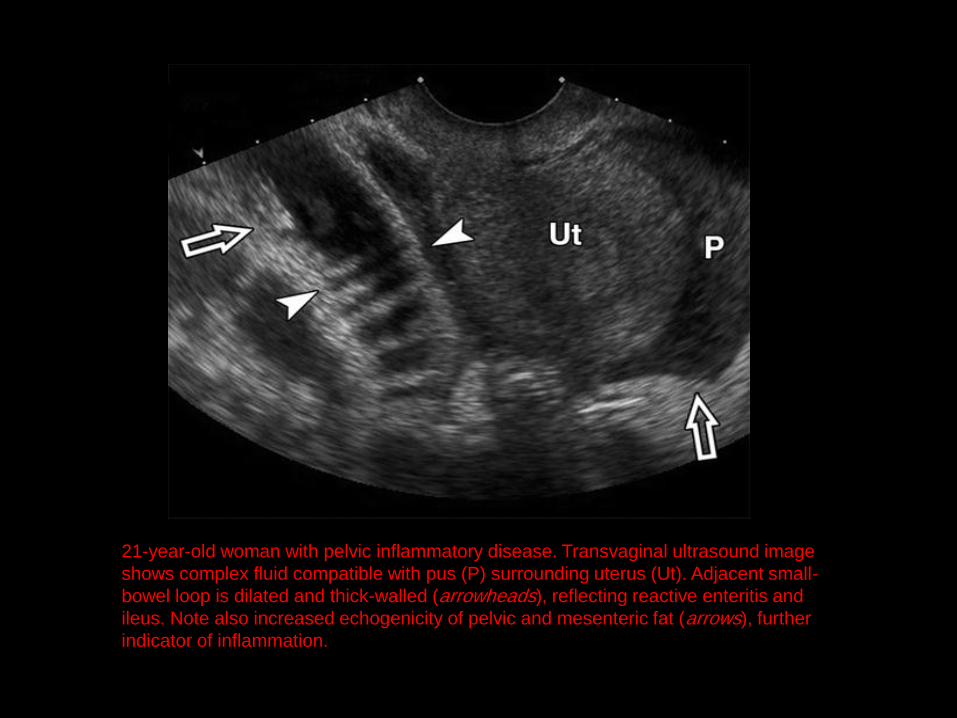
21-year-old woman with pelvic inflammatory disease. Transvaginal ultrasound image
shows complex fluid compatible with pus (P) surrounding uterus (Ut). Adjacent small-
bowel loop is dilated and thick-walled (arrowheads), reflecting reactive enteritis and
ileus. Note also increased echogenicity of pelvic and mesenteric fat (arrows), further
indicator of inflammation.
Factors which decrease the reliability of sonographic evaluation
• operator dependent technique
• the presence of overlying bowel gas
• obesity of the patient.
Mesentery and Omentum
• Abnormally echogenic fat ( this extraluminal finding) may be the most conspicuous finding in bowel disease
• “Creeping fat” characteristic of inflammatory bowel.
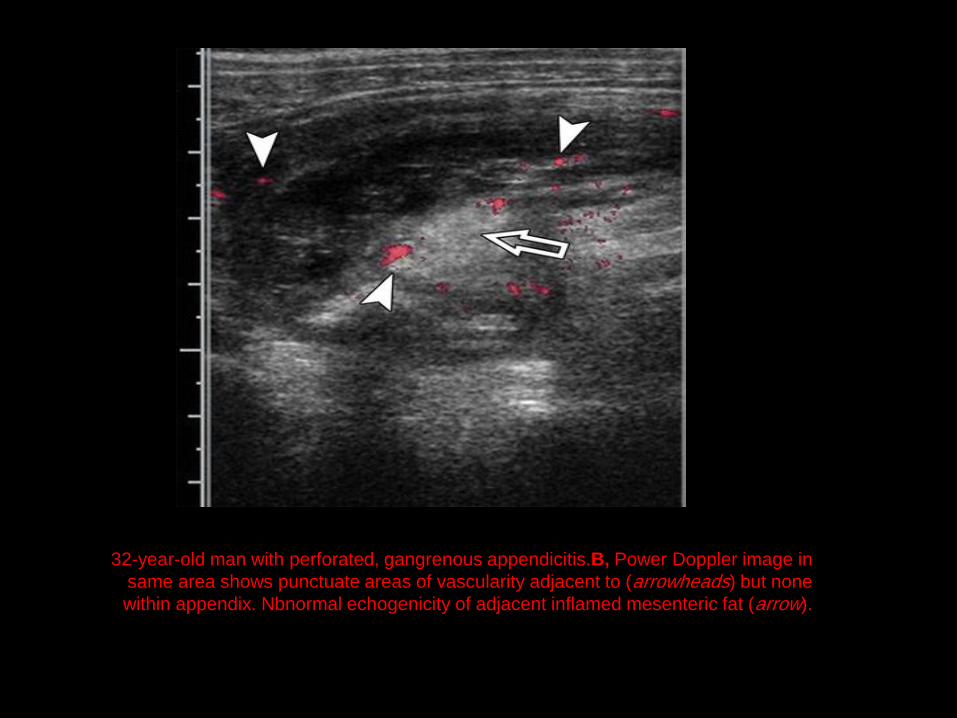
32-year-old man with perforated, gangrenous appendicitis.B, Power Doppler image in
same area shows punctuate areas of vascularity adjacent to (arrowheads) but none
within appendix. Nbnormal echogenicity of adjacent inflamed mesenteric fat (arrow).
Overview of ultrasound
• Mural Thickening
• Intraluminal versus extraluminal
• Bowel obstruction
• Appendicitis
• Free air
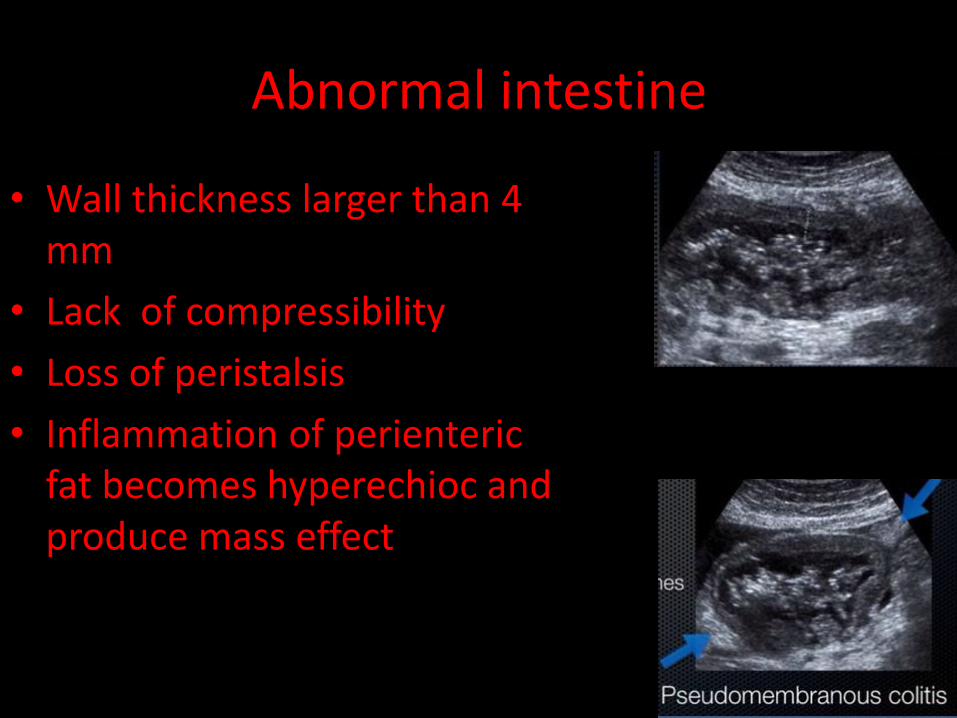
Abnormal intestine
• Wall thickness larger than 4 mm
• Lack of compressibility
• Loss of peristalsis
• Inflammation of perienteric fat becomes hyperechioc and produce mass effect
Mural Thickening
• Bowel wall thickening may be the most common and reliable sign of bowel disease
• Wall thickening is more typically
concentric in benign
eccentric in malignant conditions
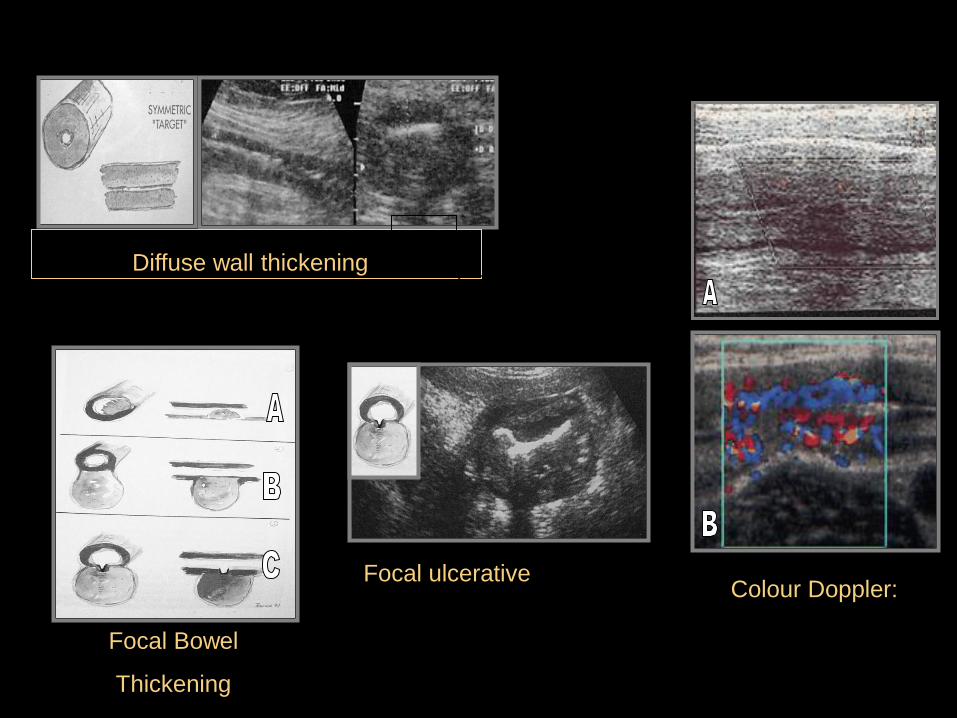
Diffuse wall thickening.
Focal Bowel
Thickening
Colour Doppler:
Activity in Crohn’s
Focal ulcerative Colonic
adenocarcinoma
Target
sign
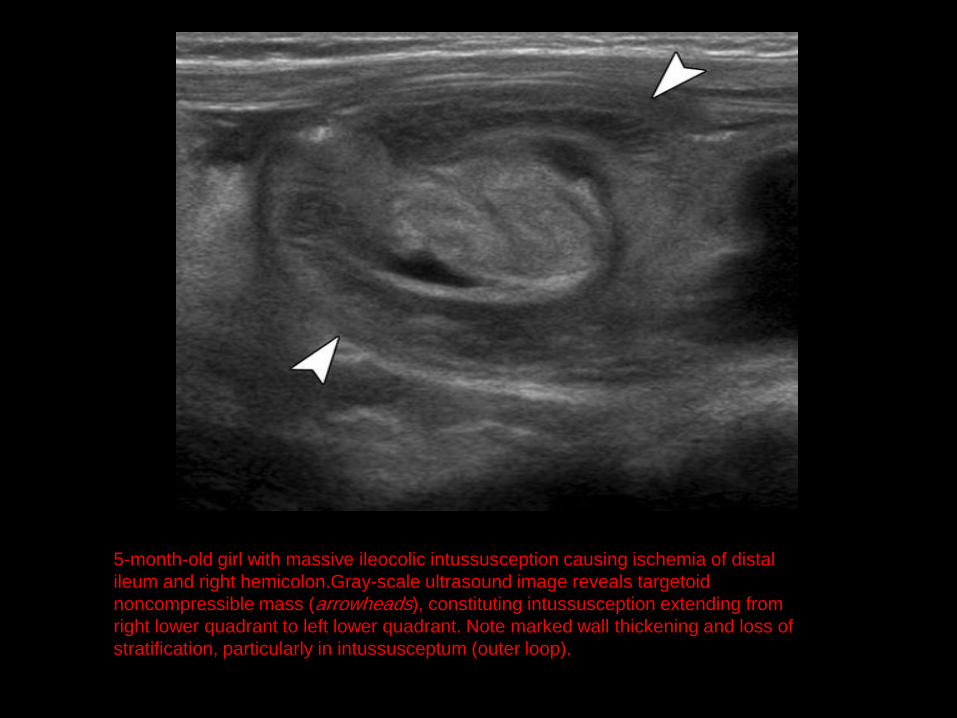
5-month-old girl with massive ileocolic intussusception causing ischemia of distal
ileum and right hemicolon.Gray-scale ultrasound image reveals targetoid
noncompressible mass (arrowheads), constituting intussusception extending from
right lower quadrant to left lower quadrant. Note marked wall thickening and loss of
stratification, particularly in intussusceptum (outer loop).
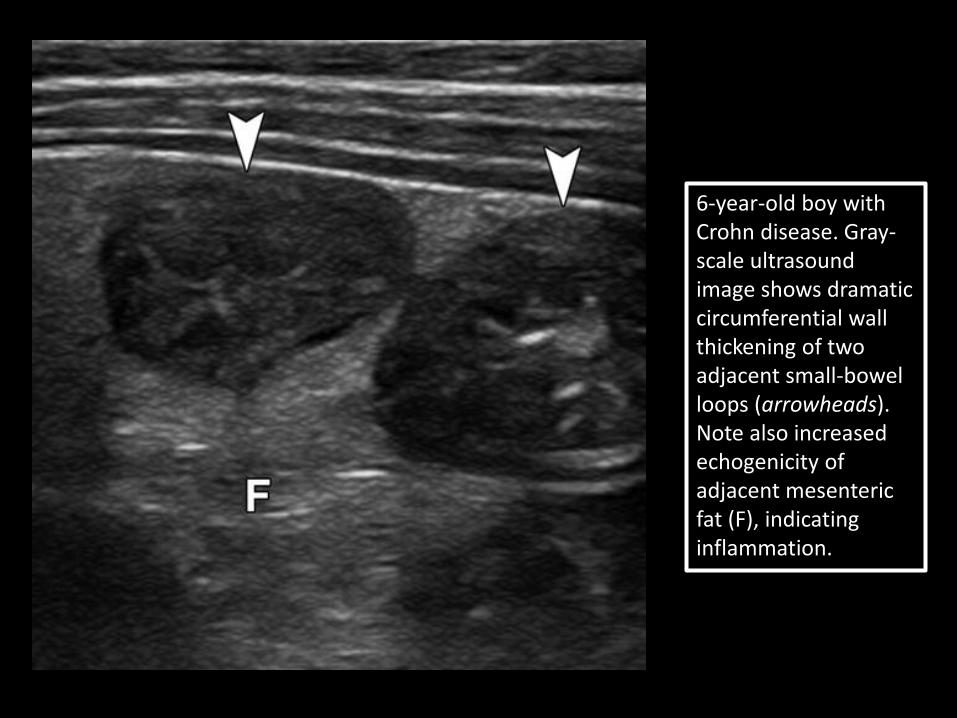
6-year-old boy with Crohn disease. Gray-scale ultrasound image shows dramatic circumferential wall thickening of two adjacent small-bowel loops (arrowheads). Note also increased echogenicity of adjacent mesenteric fat (F), indicating inflammation.
17-year-old girl with Crohn disease. Power Doppler image of terminal ileum
(arrowheads) shows wall thickening and mural hyperemia, indicating active
inflammation. Note also enlarged adjacent mesenteric lymph node (arrow) surrounded
by echogenic fat.
52-year-old woman with infectious colitis. Gray-scale ultrasound image shows
concentric wall thickening and blurring of normal mural stratification
(arrowheads) in colon. Power Doppler image (inset) reveals marked hyperemia
(arrow) in affected segment.

64-year-old woman with locally advanced colon cancer presenting as
palpable mass in right upper quadrant.A, Transverse ultrasound image
colonic wall thickening (arrowheads).
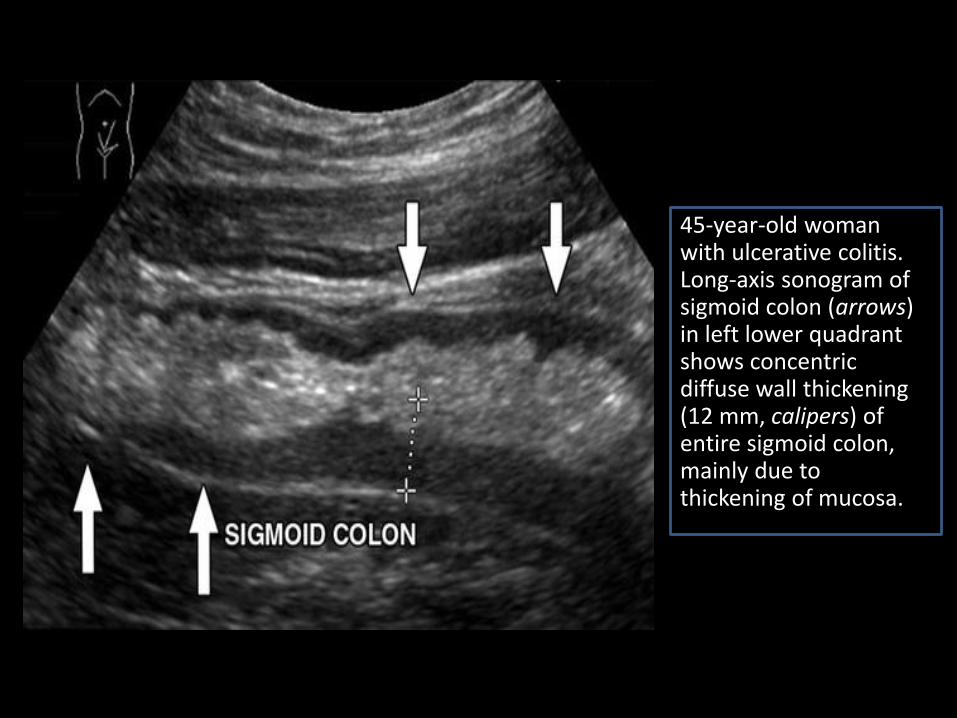
45-year-old woman with ulcerative colitis. Long-axis sonogram of sigmoid colon (arrows) in left lower quadrant shows concentric diffuse wall thickening (12 mm, calipers) of entire sigmoid colon, mainly due to thickening of mucosa.
52-year-old woman with infectious colitis. Gray-scale ultrasound image shows concentric wall thickening and blurring of normal mural stratification (arrowheads) in colon. Power Doppler image (inset) reveals marked hyperemia (arrow) in affected segment.
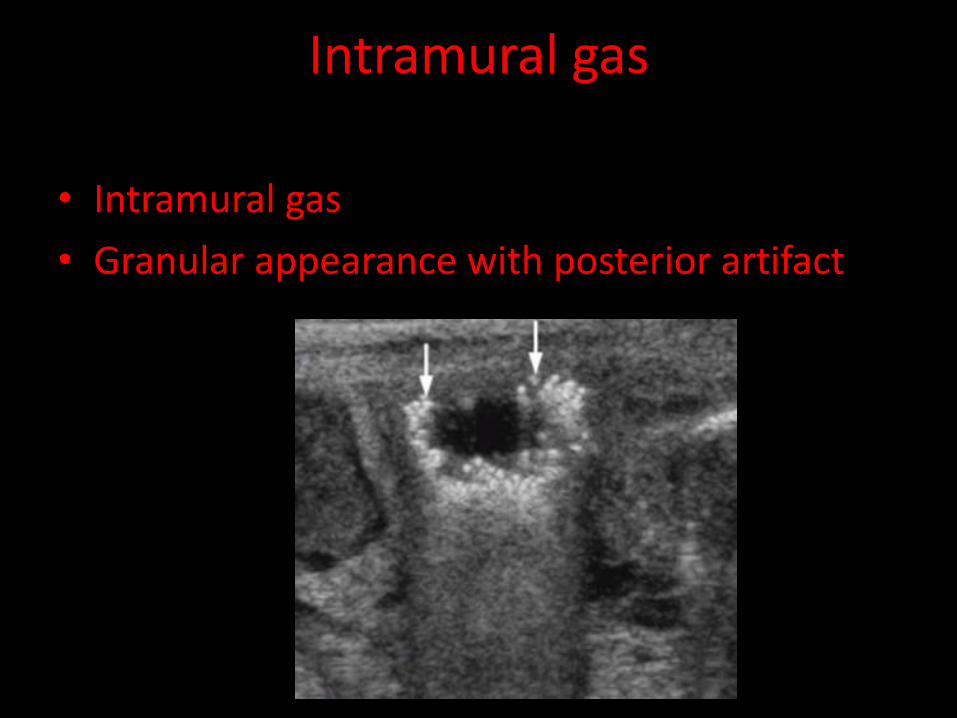
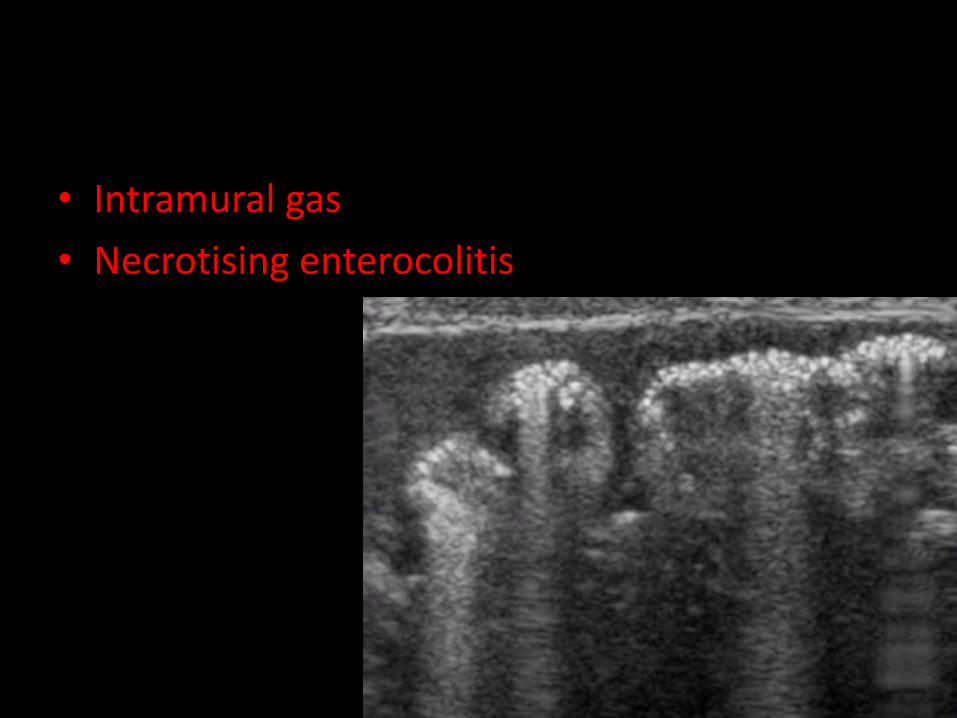
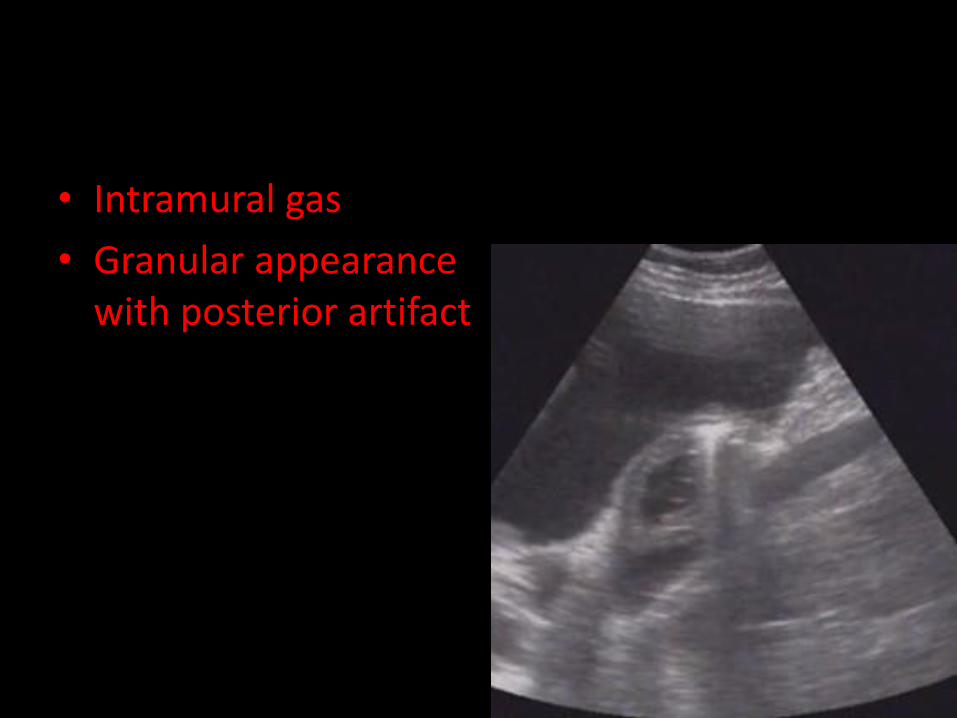
Intramural gas
• Intramural gas
• Granular appearance with posterior artifact
Color Doppler image shows some vascularity (arrowheads) in tissue
surrounding mass but none within loops of intussusceptum.
Pneumatosis intestinalis
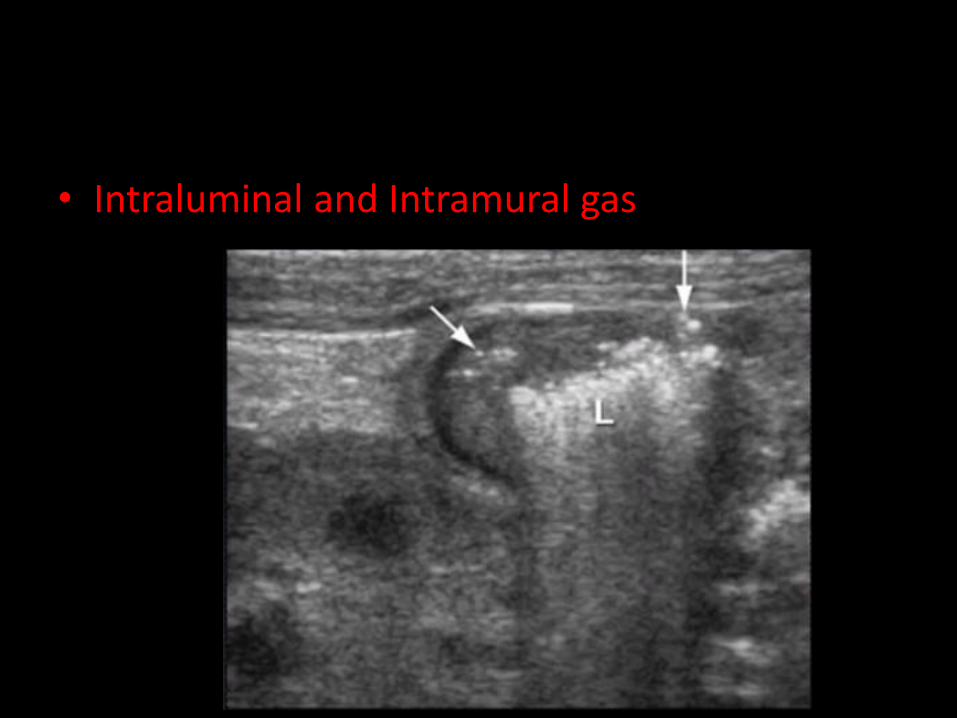
• Intraluminal and Intramural gas
• Intramural gas
• Necrotising enterocolitis
• Intramural gas
• Granular appearance with posterior artifact
Small bowel obstruction plain film can be inaccurate
• Ileus may resemble partial SBO
• Dilated small bowel loop can be filled with fluid instead of air and therfore radiologically invisible
• Proximal SBO may present with few dilated loops and be empty of air from repeated vomiting
• Closed loop obstruction occurs when bowel is obstructed at two different ends and therfore no gas trapped
• Plain film equivocal in 20-30 % of patient
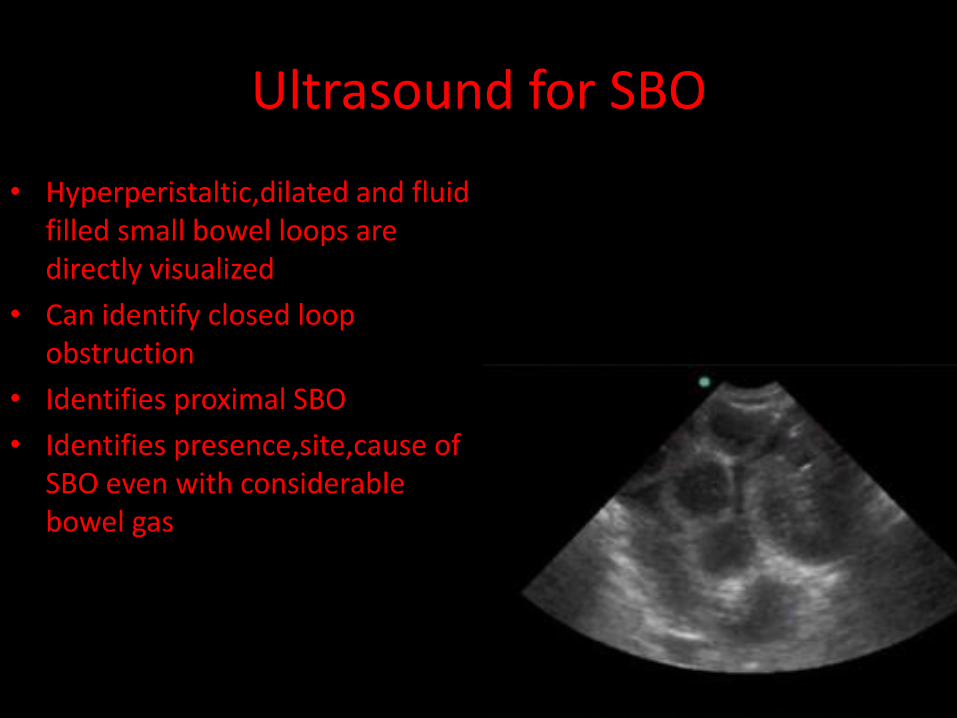
Ultrasound for SBO
• Hyperperistaltic,dilated and fluid filled small bowel loops are directly visualized
• Can identify closed loop obstruction
• Identifies proximal SBO
• Identifies presence,site,cause of SBO even with considerable bowel gas
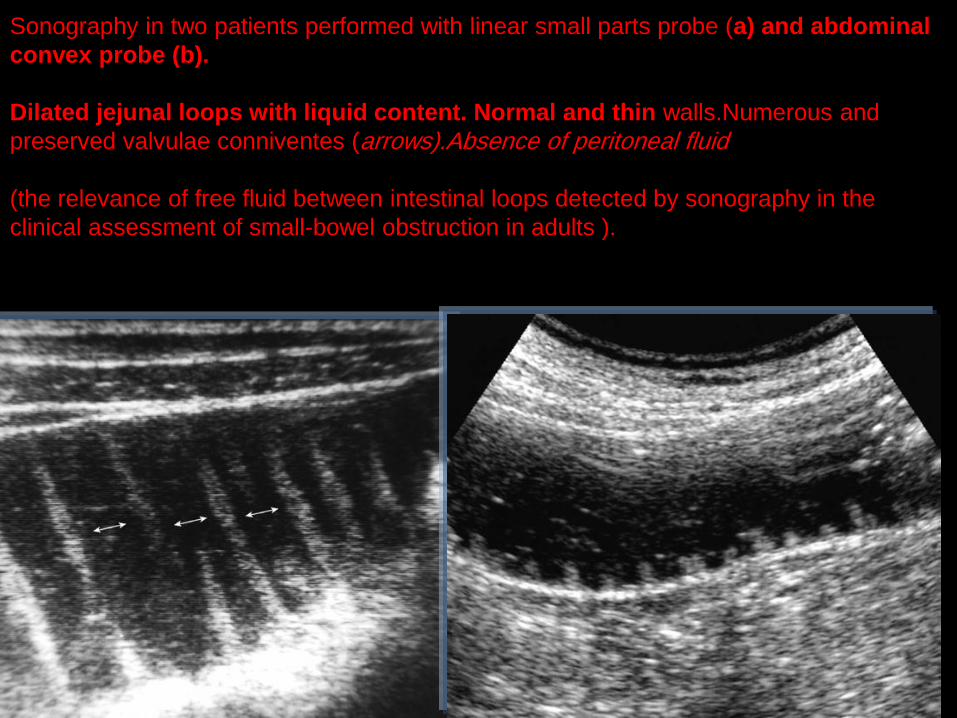
Sonography in two patients performed with linear small parts probe (a) and abdominal
convex probe (b).
Dilated jejunal loops with liquid content. Normal and thin walls.Numerous and
preserved valvulae conniventes (arrows).Absence of peritoneal fluid (the relevance of free fluid between intestinal loops detected by sonography in the
clinical assessment of small-bowel obstruction in adults ).

• Small bowel obstruction
• Hyperperistalsis,thickened wall and free fluid

• Small bowel obstruction
• Hyperperistalsis,thickened wall and free fluid
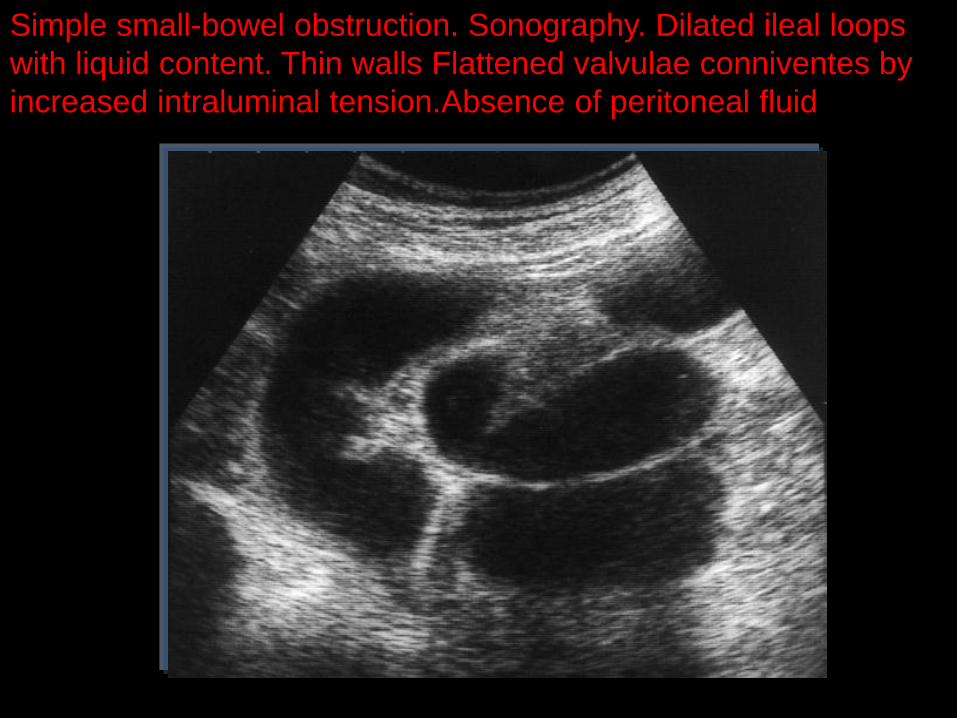
Simple small-bowel obstruction. Sonography. Dilated ileal loops
with liquid content. Thin walls Flattened valvulae conniventes by
increased intraluminal tension.Absence of peritoneal fluid
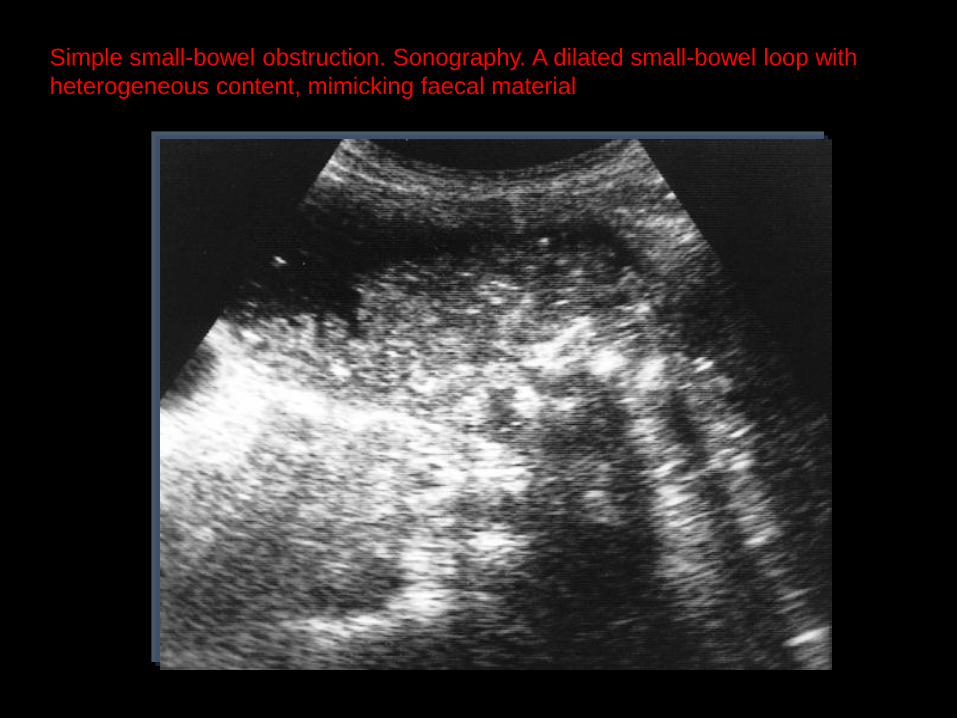
Simple small-bowel obstruction. Sonography. A dilated small-bowel loop with
heterogeneous content, mimicking faecal material
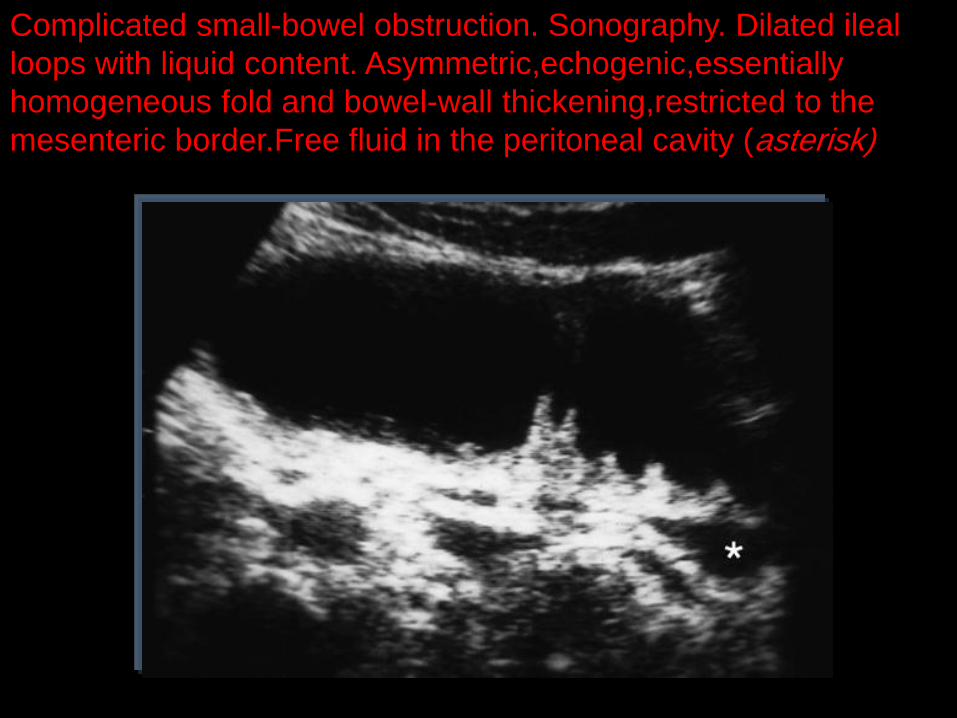
Complicated small-bowel obstruction. Sonography. Dilated ileal
loops with liquid content. Asymmetric,echogenic,essentially
homogeneous fold and bowel-wall thickening,restricted to the
mesenteric border.Free fluid in the peritoneal cavity (asterisk)
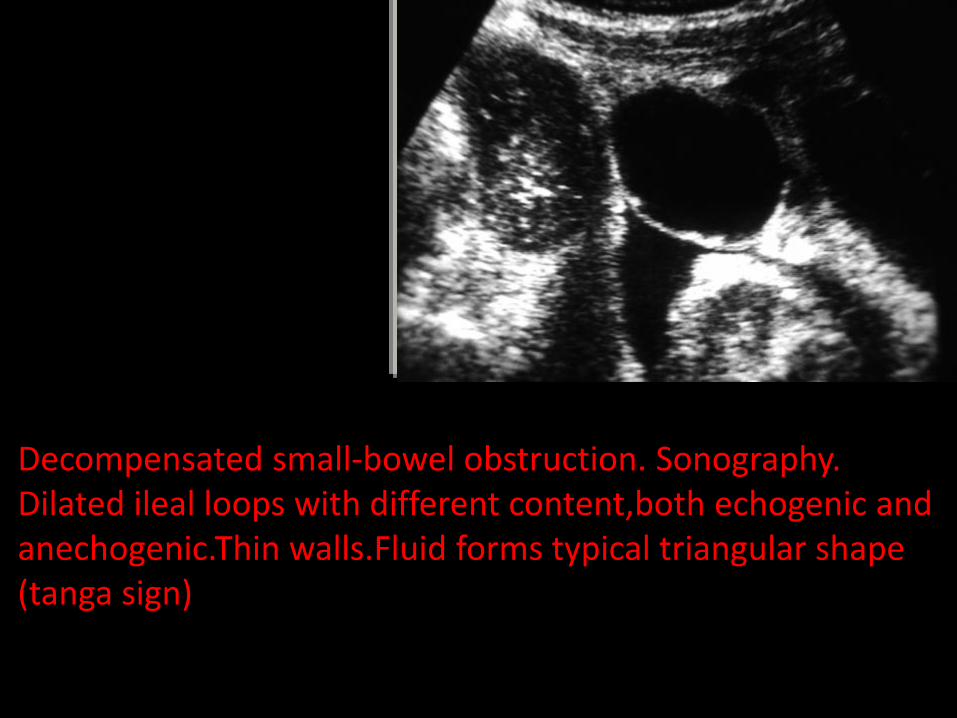
Decompensated small-bowel obstruction. Sonography. Dilated ileal loops with different content,both echogenic and anechogenic.Thin walls.Fluid forms typical triangular shape (tanga sign)
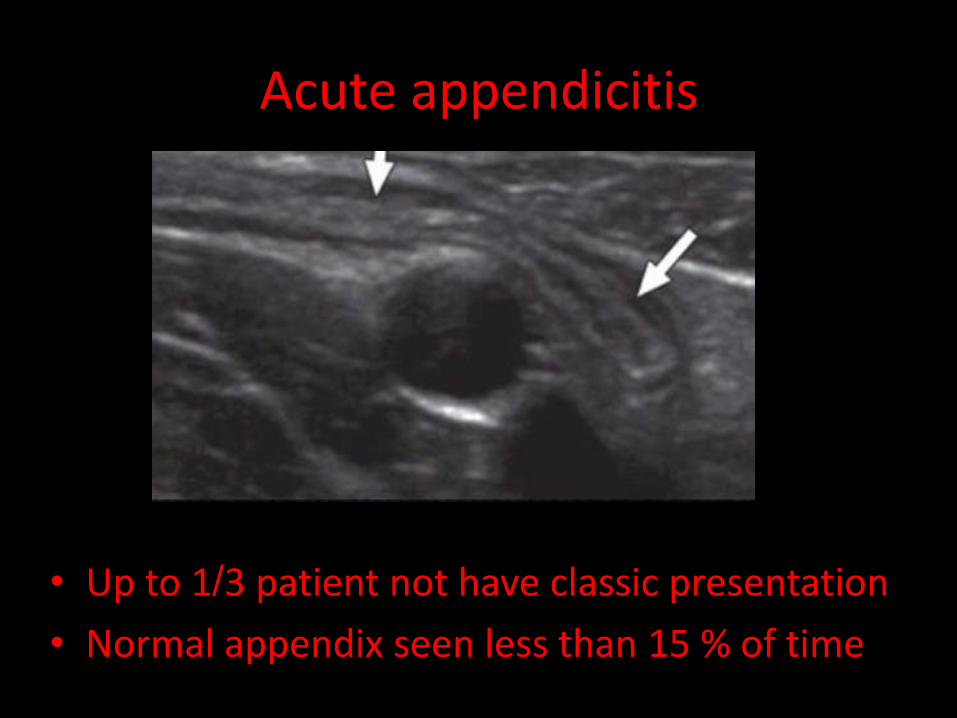
Acute appendicitis
• Up to 1/3 patient not have classic presentation
• Normal appendix seen less than 15 % of time
Acute appendicitis wait for it , wait for it , wait for it
• Non compressible tubular structure in RLO sandwitched between abdominal musculature and psoas
Wall No bigger than 6 mm when normal
Occasionally associated with appendicolith
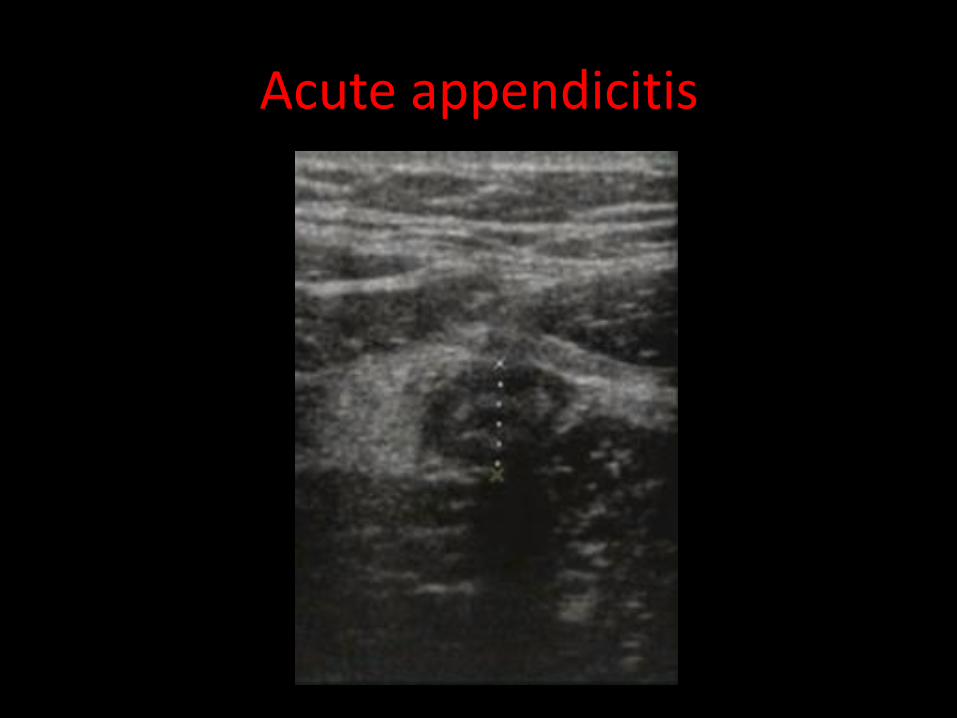
Acute appendicitis
Appendix not visualized
Acute appendicitis
Acute appendicitis
Acute appendicitis

Appendix with fecolith