Embed Size (px)
Citation preview
© The Wellesley Institutewww.wellesleyinstitute.com
Driving Health Equity Into Action: Policy Change and Community Mobilization to Address the
Social Determinants of Health
Bob GardnerRyerson University
Promoting Health Equity ConferenceFebruary 12, 2011
© The Wellesley Institutewww.wellesleyinstitute.com
• health disparities are pervasive and damaging → importance of health equity
• will set out how these disparities can be addressed through comprehensive health equity strategy
• acting on health equity within the health system• building equity into all planning and delivery• targeting some programs and resources for equity impact• aligning equity with key system drivers • embedding equity in performance management and service delivery
• and well beyond healthcare -- tackling the underlying roots of health inequality in the wider social determinants of health• through community-based innovation, cross-sectoral collaborations and
fundamental social and policy change to reduce inequality• community and political mobilization to demand and drive the necessary policy
changes
Outline
2
© The Wellesley Institutewww.wellesleyinstitute.com
The Challenge = Health Disparities in Ontario
• there is a clear gradient in health in which people with lower income, education or other indicators of social inequality and exclusion tend to have poorer health
• + major differences between women and men• the gap between the health status of the best off
and most disadvantaged can be huge – and damaging
• in addition, there are systemic disparities in access to and quality of care within the health care system
3
© The Wellesley Institutewww.wellesleyinstitute.com 4
© The Wellesley Institutewww.wellesleyinstitute.com 5
© The Wellesley Institutewww.wellesleyinstitute.com 6
© The Wellesley Institutewww.wellesleyinstitute.com
Impact of Disparities
inequality in how long people live• difference btwn life expectancy of top and bottom
income decile = 7.4 years for men and 4.5 for women• more sophisticated analyses add the pronounced
gradient in morbidity to mortality → taking account of quality of life and developing data on health adjusted life expectancy
• even higher disparities btwn top and bottom = 11.4 years for men and 9.7 for women
Statistics Canada Health Reports Dec 09
7
8www.welleseyinstitute.com
Foundations of Health Disparities Roots Lie in Social Determinants of Health
•clear research consensus that roots of health disparities lie in broader social and economic inequality and exclusion
•impact of inadequate early childhood development, poverty, precarious employment, social exclusion, inadequate housing and decaying social safety nets on health outcomes is well established here and internationally
•real problem is differential access to these determinants – many analysts are focusing more specifically on social determinants of health inequalities
© The Wellesley Institutewww.wellesleyinstitute.com
SDoH As a Complex Problem
•Determinants interact and intersect with each other•In constantly changing and dynamic system•In fact, through multiple interacting and inter-dependent economic, social and health systems•Determinants have a reinforcing and cumulative effect on individual and population health
9
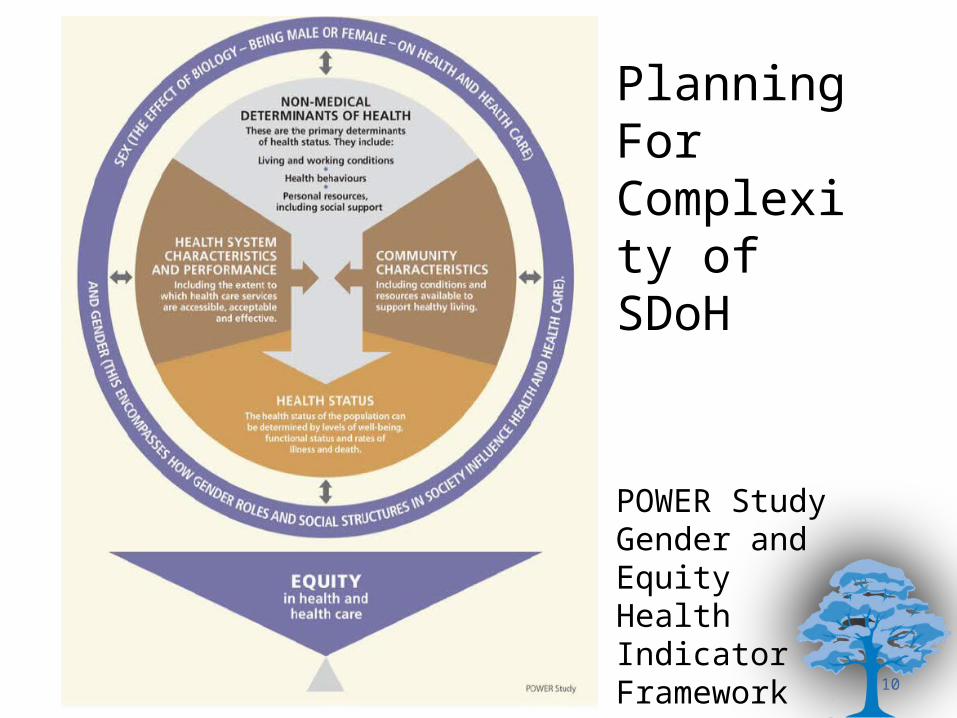
Planning For Complexity of SDoH
POWER StudyGender andEquityHealth IndicatorFramework
10
© The Wellesley Institutewww.wellesleyinstitute.com
Health Equity = Reducing Unfair Differences
• Health disparities or inequities are differences in health outcomes that are avoidable, unfair and systematically related to social inequality and disadvantage
• This concept:• is clear, understandable and actionable• identifies the problem that policies will try to solve• is also tied to widely accepted notions of fairness and social justice
• The goal of health equity strategy is to reduce or eliminate socially and institutionally structured health inequalities and differential outcomes
• A positive and forward-looking definition = equal opportunities for good health
• Equity is a broad goal, including diversity in background, culture, race and identity

© The Wellesley Institutewww.wellesleyinstitute.com
12
Think Big, But Get Going• the point of all this analysis is to be able to identify policy and program
changes needed to reduce health disparities
• but health disparities can seem so overwhelming and their underlying social determinants so intractable → can be paralyzing
• think big and think strategically, but get going• make best judgment from evidence and experience• identify actionable and manageable initiatives that can make a difference• experiment and innovate --- learn lessons and adjust• gradually build up coherent sets of policy and program actions – and keep
evaluating
• need to start somewhere – and focus today is on 1. building equity into health system2. and the wider context of addressing the social determinants of health through
community action and policy change
© The Wellesley Institutewww.wellesleyinstitute.com
• even though roots of health disparities lie in far wider social and economic inequality
• how the health system is organized and how services and care are delivered is still crucial to tackling health disparities
• consistent theme in WHO, EU and all the major international reports and in the many countries that have developed comprehensive multi-sectoral strategies to reduce health disparities
• in all of them, transforming the health system is an indispensable element, including:• reducing barriers to equitable access to high quality care• targeted interventions to improve the health of the poorest, fastest• up-stream investments in primary and preventative care directed to most
vulnerable• delivering a full continuum of services in coordinated way at
community/local level
Equity Into Health System: Why
13
© The Wellesley Institutewww.wellesleyinstitute.com
1. it’s in the health system that the most disadvantaged in SDoH terms end up sicker and needing care
• equitable healthcare and support can help to mediate the harshest impact of the wider social determinants of health on health disadvantaged populations and communities
2. in addition, there are systemic disparities in access and quality of healthcare that need to be addressed
• people lower down the social hierarchy can have poorer access to health services, even though they may have more complex needs and require more care
• unless we address inequitable access and quality, healthcare and community support services could make overall disparities even worse
Equity Into Health System: Why II
14

© The Wellesley Institutewww.wellesleyinstitute.com
• goal is to ensure equitable access to high quality healthcare regardless of social position
• can do this through a three pronged strategy:1. building health equity into all health planning and delivery
• doesn’t mean all programs are all about equity• but all take equity into account in planning their services and outreach
2. aligning equity with system drivers and embedding it in provider organizations and performance management
3. targeting some resources or programs specifically to addressing disadvantaged populations or key access barriers
• looking for investments and interventions that will have the highest impact on reducing health disparities or enhancing the opportunities for good health of the most vulnerable
Equity Into Health System: How
15
© The Wellesley Institutewww.wellesleyinstitute.com
Equity Into Health System: How IIwhile health disparities are pervasive and deep-rooted, they can be changed through policy and program actioncomprehensive strategy developed in 2008 for Toronto Central LHINmany recommendations have been acted onother LHINs are also prioritizing and moving to address health disparities
16
© The Wellesley Institutewww.wellesleyinstitute.com
Start From The Community• goal is to reduce health disparities and speak to needs of most
vulnerable communities – who will define?• can’t just be ‘experts’, planners or professionals
• have to build community into core planning and priority setting• not as occasional community engagement• but to identify equity needs and priorities• and to evaluate how we are doing
• how:• many hospital have community advisory panels• CHCs have community members on their boards • innovative methods of engagement – e.g. citizens’ assemblies or juries in
many countries• community-based research, needs assessment and evaluation
17
© The Wellesley Institutewww.wellesleyinstitute.com
And Start From a Solid Strategic Commitment
• need to make equity one of driving priorities for health system and reform• equity and a population health focus are among key principles enshrined in
new Excellent Care for All Act = opening and context
• need clear provincial strategy for equity: • implicit from MOHLTC, but promised ten year strategy has not been released• equity and population health are in public health standards• need strategic coherence across health system in approach to equity
• LHINs, CCACs, and other coordinating agencies need to prioritize equity – and many have
• cascading down to all providers prioritizing equity in their overall strategic plans and then into service delivery and resource allocation
18
© The Wellesley Institutewww.wellesleyinstitute.com
Align Equity With System Drivers
• ECFA Act and quality agenda • providers have to develop Quality Improvement Plans
• hospitals are reporting April 1• other providers will report in subsequent years• equity should be developed as one of dimensions to report on
• similarly, improving safety requires addressing equity barriers • inadequate interpretation services can lead to mid-diagnoses, people
not being able to follow medication, etc.• can also build equity into accreditation processes• provincial priorities – e.g. diabetes, wait times, mental health, ALCs – are
all sensitive to social conditions and will not be achieved unless planning/delivery takes equity into account
19
© The Wellesley Institutewww.wellesleyinstitute.com
Into Practice Through Equity-Focused Planning
• addressing health disparities in service delivery and planning requires a solid understanding of:• key barriers to equitable access to high quality care• the specific needs of health-disadvantaged populations• gaps in available services for these populations
• need to understand roots of disparities:• i.e. is the main problem language barriers, lack of coordination among
providers, sheer lack of services in particular neighbourhoods, etc.• which requires good local research and detailed information – speaks to
great potential of community-based research• involvement of local communities and stakeholders in planning and priority
setting is critical to understanding the real local problems
• requires an array of effective and practical equity-focused planning tools
20
© The Wellesley Institutewww.wellesleyinstitute.com
Health Equity Impact Assessment
• increasing attention to potential – from WHO, through most European strategies, PHAC, to MOHLTC and LHINs
• planning tool that analyzes potential impact of program or policy change on health disparities and/or health disadvantaged populations• can help to plan new services, policy development or other initiatives• can also be used to assess/realign existing programs• intended to be relatively easy-to-use tool • essentially prospective, helping plan forward
• piloted in Toronto in 2009 by MOHTLC, Toronto Central LHIN and WI• HEIA is being used in Toronto Central and other LHINs and providers across
the province • Toronto Central has required HEIA within recent funding application
processes for Aging at Home, and refreshing hospital equity plans
21
© The Wellesley Institutewww.wellesleyinstitute.com
Beyond Planning: Embed Equity in Targets and Incentives
• clear consensus from research and policy literature and consistent feature in comprehensive policies on health equity from other countries =• setting targets for reducing access barriers, improving
health outcomes of particular populations, etc• developing realistic and actionable indicators for service
delivery• closely monitoring progress against the targets and
indicators• disseminating the results widely for public scrutiny• tying funding and resource allocation to performance
22
© The Wellesley Institutewww.wellesleyinstitute.com
• where targets and indicators get tied to deliverables and incentives
• key lever = all hospitals, CHCs and other providers sign Service Accountability Agreements with LHINs that govern flow of funds
• can build specific expectations and deliverables into those agreements
• will vary by community and provider -- but could include:• undertaking appropriate equity-focused planning to identify areas
where access to services is inequitable and developing plans to address barriers and gaps
• stratifying quality indicators by equity – e.g. reducing hospital readmission rates is common objective
→equity angle is to reduce any inequitable differences in readmission rates by language ability or neighbourhood
Embed Equity In Performance Management
23
© The Wellesley Institutewww.wellesleyinstitute.com
Precondition: Effective Equity Targets
• innovative work underway to develop equity indicators – but don’t need to wait
• build equity into existing targets:• reducing diabetes incidence is prov and LHIN priority → equity target = reduce differences in incidence, complications and rates of
hospitalization between populations or areas• a good service target has been proposed for diabetes = high/increasing % of people
who get best standard care → reduce differences by gender, income, ethno-cultural background
• need to drill down in specific areas that have high equity impact:→ ensuring access and use of primary health care does not vary inequitably by income
level, immigration status, neigbourhood, gender, race, etc. • many programs assess their services through client satisfaction surveys and
look for high and improving satisfaction → reduce any differences in satisfaction by gender, income, ethno-cultural background,
etc.
24
© The Wellesley Institutewww.wellesleyinstitute.com
• a promising direction several LHINs have taken up is to require providers to develop equity plans• hospitals in Toronto Central and Central LHINs – just refreshed 2nd generation in TC• and other providers in Central• CHCs are developing sector-wide plan in GTA
• these plans are designed to:• identify access barriers, disadvantaged populations, service gaps and opportunities in
their catchement areas and spheres• develop programs and services to address those gaps and better meet healthcare
needs of disadvantaged communities
• these provider plans have the potential to:• raise awareness of equity within the organizations• build equity into planning, resource allocation and routine delivery• pull their many existing initiatives together into a coherent overall equity strategy• build connections among providers for addressing common equity issues
Use Promising Tools/Levers: Equity Plans
25
© The Wellesley Institutewww.wellesleyinstitute.com
http://www.torontoevaluation.ca/tclhin/index.html
26
© The Wellesley Institutewww.wellesleyinstitute.com
• all this planning, monitoring indicators, and assessing progress against objectives and targets needs reliable data on:• ethno-cultural background, language, income, sexual orientation• service use and health outcomes, differentiated by these equity and
determinants of health variables• when hospitals in Toronto Central began working on their equity plans it became
very clear that they simply did not have the necessary data to do equity-driven planning• a workshop was held on what kinds of data on equity and diversity are available,
how the existing data sets can be effectively used, and what further types of data are needed
• three hospitals are collaborating on how to collect and incorporate equity data• but don’t wait for perfect data
• hospitals have been using postal code data as proxy for income• idea = no health research that doesn’t include SDoH data
Precondition: Equity-Relevant Data
27
© The Wellesley Institutewww.wellesleyinstitute.com
28
Target Investment for Equity Impact
• target services to:• those facing the harshest disparities – to raise the worst off fastest• or most in need of specific services• or the worst barriers to equitable access to high-quality services
• this requires resources• lever = certain % of LHIN budgets to be equity targeted
• this requires sophisticated analyses of the bases of disparities:• i.e. is the main problem language barriers, lack of coordination among
providers, sheer lack of services in particular neighbourhoods, etc.• which requires good local research and detailed information – speaks to great
potential of community-based research to provide rich local needs assessments and evaluation data
• involvement of local communities and stakeholders in planning and priority setting is critical to understanding the real local problems
© The Wellesley Institutewww.wellesleyinstitute.com
• vulnerable populations will vary:• poor neighbourhoods with high % of racialized population in many big cities• Aboriginal communities across the prov• isolated rural areas
• solid evidence that enhancing primary care is one of key ways to improve care of disadvantaged• lack of access to primary care has been identified as a key issue for Prov and LHINs→ concentrate new FHTs or other initiatives in particular regions or neighbourhoods, or
in particular populations such as refugees or uninsured• need to drill down with good research:
• South Asian immigrants had 3X and Caribbean and Latin American 2X risk of diabetes than immigrants from Western Europe or North America
• greater risk for women• risk increases with time since immigration
Creatore et al CMAJ Aril 19, 2010
Target Populations
29
© The Wellesley Institutewww.wellesleyinstitute.com
Target Barriers• one of critical equity challenges for many LHINs, hospitals and other providers in
diverse communities is language• LHINs need to specifically require hospitals to ensure interpretation is available
in languages of their community• need to fund centralized interpretation services to support smaller agencies
• in some other areas, distance and isolation are the critical determinants• in Toronto and other cities: people without health insurance – primarily
immigrants/refugees:• many community initiatives to provide access• Women’s College Hospital Network on Noninsured is forum for coordination• recently held research conference showing critical barriers to access and good
care and resulting adverse health outcomes for vulnerable people• equity is complex – ‘wicked’ policy problems• but not all of it = avoidable disparities and workable solution• eliminate the three month wait for OHIP for new immigrants
30
© The Wellesley Institutewww.wellesleyinstitute.com
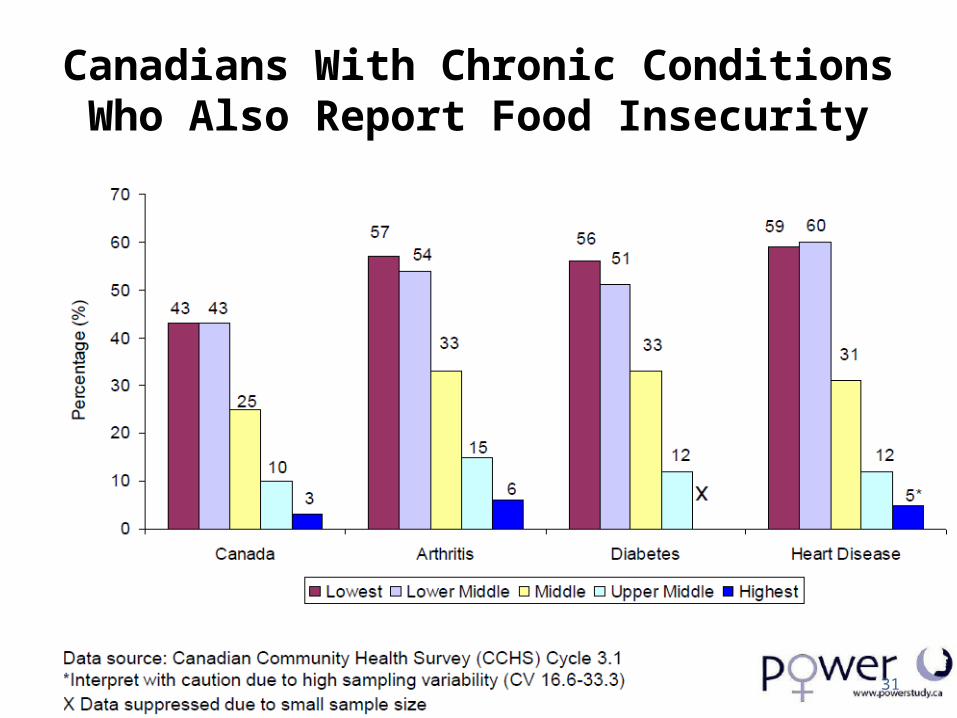
Canadians With Chronic Conditions Who Also Report Food Insecurity
31
© The Wellesley Institutewww.wellesleyinstitute.com
32
Up Stream Through an Equity Lens: Chronic Conditions
• investing in better chronic care prevention and management are vital for quality and health system sustainability
• up-stream initiatives need to be planned and implemented through an equity lens• very clear gradient in incidence – and impact – of chronic
conditions• some populations and communities have fewer resources
to prevent and manage chronic conditions• need to build this greater need for support into CDPM
planning and resource allocation• a very interesting primer has been developed by Health
Nexus, the Ontario Chronic Disease Prevention Alliance and other partners to help incorporate social determinants into chronic care management and support
© The Wellesley Institutewww.wellesleyinstitute.com
Up Stream Through an Equity Lens: Health Promotion
• more emphasis on health promotion is vital to long-term sustainability of system and individual health• consistent data on variations of risk factors along the social
gradient• anti-smoking, exercise and other health promotion
programmes need to explicitly foreground the particular social, cultural and economic factors that shape risky behaviour in poorer communities– not just the usual focus on individual behaviour and lifestyle
• need to customize and concentrate health promotion programs especially for most disadvantaged
• if this isn’t done → can unintentionally widen disparities as better off take up programs more
33
© The Wellesley Institutewww.wellesleyinstitute.com 34
© The Wellesley Institutewww.wellesleyinstitute.com
Back to Service Delivery and Excellent Care: Take SDoH Into Account
• all of this equity planning loops back to quality• patient-centred care means taking the full range of people’s
specific needs into account• social context and living conditions are part of this
• when people face adverse social determinants of health → can increase risk of mental and physical health challenges and illness → fewer resources to cope (from supportive social networks, to good
food and being able to afford medication)
• providers and programs need to know this to customize and adapt care to needs and contexts
• more intensive case management, referral planning and post-discharge follow-up
35
© The Wellesley Institutewww.wellesleyinstitute.com
Not Just at Individual Level: Build Equity-Driven Service Models
• Community Health Centre model of care• explicitly geared to supporting people from marginalized communities • comprehensive multi-disciplinary services covering full range of needs
→ look beyond vulnerable individuals to the communities in which they live• have to take SDoH into account in program design
→ meeting full range of needs means moving beyond healthcare• focus on community development as part of mandate• providing and partnering to provide related services/support such as
settlement, language, child care, literacy, employment training, youth support, etc.
36
© The Wellesley Institutewww.wellesleyinstitute.com
Equity-Driven Innovation: Hub Models of Integrated Care
• hub-style multi-service centres in which a range of health and employment, child care, language, literacy, training and social services are provided out of single ‘one stop' locations• many countries have clinics that provide both health and wider social
services in one place• some new satellite CHCs are being developed in designated high-need
areas in Toronto will involve the CHCs delivering primary and preventive care and other agencies providing complementary social services out of the same location
• not just health -- idea of schools as service hubs is being developed • think back to earlier eras with public health nurses in schools • start by putting hubs in schools in most disadvantaged areas• concentrated and integrated services for most disadvantaged kids have
proven to be effective investment37
© The Wellesley Institutewww.wellesleyinstitute.com
Build SDoH Into Planning:Cross-Sectoral Planning Through an Equity Lens
• cross-sectoral coordination and planning are much emphasized in public health and health policy circles• but what sectors? for what purposes?
• addressing wider SDoH is the glue for collaboration into action• public health departments and LHINs are pulling together or
participating in cross-sectoral planning tables → Prov should make this an explicit expectation
• Local Immigration Partnerships , Social Planning Councils• the Ministry of Health Promotion and Sport is
developing a healthy communities strategic approach• cross-sectoral planning to ground health promotion • at best, this implies wider community development and capacity
building approaches
38
© The Wellesley Institutewww.wellesleyinstitute.com 39
Equity-Driven Collaboration and Coordination
• across Canada, leading Regional Health Authorities have developed operational and planning links with local social services or emphasized community capacity building:• Saskatoon is developing cross-sectoral action on health equity:
• began from local research documenting shocking disparities among neighbourhoods
• focusing interventions in the poorest neighbourhoods – locating services in schools, relying on First Nations elders to guide programming, etc.
• wide collaboration among public health, municipality, business, community, Aboriginal and other leaders
• in Ontario public health are key players in addressing health disparities on the ground• a number of public health units have been pioneering social determinants
approaches -- Sudbury, Waterloo, Toronto, Peterborough • generally through broad community collaborations
© The Wellesley Institutewww.wellesleyinstitute.com 40
Extend That → Build on/from Local and Regional Initiatives
• there is always much to be learned from policies, programs and initiatives in other jurisdictions
• health equity strategies in European and other leading jurisdictions combine:• national level macro strategies to reduce social health
inequalities• with local or regional implementation and adaptation• British example: Health Action Zones and other models were
designed to combine community economic development with targeted healthcare and social service improvements
• that is the potential of LHINs and RHAs→ build equity into regional planning and coordination
© The Wellesley Institutewww.wellesleyinstitute.com
Extend That Further→ Build on/from Community-Driven Action
• comprehensive community initiatives:• broad partnerships of local residents, community organizations,
governments, business, labour and other stakeholders• coming together to address deep-rooted local problems – poverty,
neighbourhood deterioration• collaborative cross-sectoral efforts – for poverty reduction,
community development, health disparities• Vibrant Communities – 14 communities across the country to build
individual and community capacities to reduce poverty• Wellesley review of evidence = these initiatives have the
potential to build:• individual opportunities• awareness of structural nature of poverty• local mobilization → into policy advocacy
41
© The Wellesley Institutewww.wellesleyinstitute.com
Back Up to High-Level Strategy: It’s All About Inequality
• increasing international and high-level attention:• WHO Commission on Social Determinants of Health• European Union, with its Closing the Gap and other projects to tackle health
disparities • a number of countries have made lessening health disparities a top national
priority and have developed cross-sectoral policy frameworks and/or action plans:• England, Scotland, Australia, New Zealand• many European countries, with Nordic ‘welfare’ states leading
• all about reducing structured inequality• focus on inclusive labour market, anti-discrimination, childcare, affordable
housing, social security and other policies• equitable access to improved health care was seen to be just one part of this
broader package• emphasized partnerships with community service providers and organizations
– in both policy development and service delivery
© The Wellesley Institutewww.wellesleyinstitute.com
42
© The Wellesley Institutewww.wellesleyinstitute.com
Which Means Policy Change
• reducing overall social and economic inequality → requires a significant commitment and re-orientation of social and economic policy
• need to build health equity into all macro social and economic policy:• not just as one factor among many to be balanced, but as core priority• some jurisdictions have built equity consideration into their policy
processes – e.g. a change in tax policy or new environmental policy would be assessed for its health equity impacts
• and implementation:• e.g. Ministries, LHINs and other public bodies always considering SDoH
in strategic and program planning -- from where to locate primary care to how to design health promotion
• and more ‘joined-up’ policy processes:• cross-Ministry collaboration and incentives• led from central authorities• Saskatchewan, Quebec
43
© The Wellesley Institutewww.wellesleyinstitute.com
Back to Community: Building on Potential of Community-Based Service Initiatives and Innovation
• huge number of community and front-line initiatives already addressing equity across province• Community Health Centres, community mental health, community
organizations based out of specific ethno-cultural communities• e.g. many community providers have established ‘peer health ambassadors’ to
provide system navigation, outreach and health promotion services to particular communities
• for homeless people:• CAISI database so records are accessible from many providers• travelling psychiatrists, nurses and other providers• my Baby and Me passport• Street Health report as community-based research into action
• this progressive service delivery = beacon of inspiration for other sectors + constant living demonstration that action is possible
• but not being systemically shared or built upon ….
44
© The Wellesley Institutewww.wellesleyinstitute.com
Enabling Equity-Driven Innovation
• to drive equity-focused innovation and effective interventions, we need to be able to:• collate and analyze all the useful intelligence gained from equity-focused
planning• capture and share information on local initiatives, and build on local front-line
insights• share the resulting knowledge across regions – and beyond • assess the most promising initiatives or directions rigorously• scale up promising initiatives across the province where appropriate
• need to create forums and infrastructure for this innovation knowledge management
• and need to build equity-focused innovation into incentives and drivers -- cascading from Prov to LHINs to providers• expectation that X% of budget will be devoted to equity-orientated innovation• ear-marked funds for equity innovation
45
© The Wellesley Institutewww.wellesleyinstitute.comApril 15, 2023
Back to Community Again: Build Momentum and Mobilization
• sophisticated strategy, solid equity-focused research, planning and innovation, and well-targeted investments and services are key
• but in the long run, also need fundamental changes in over-arching state social policy and underlying structures of economic and social inequality
• these kinds of huge changes come about not because of good analysis but through widespread community mobilization and public pressure
• key to equity-driven reform will also be empowering communities to imagine their own alternative vision of different health futures and to organize to achieve them
• we need to find ways that governments, providers, community groups, unions, and others can support each others’ campaigns and coalesce around a few ‘big ideas’
46
© The Wellesley Institutewww.wellesleyinstitute.comApril 15, 2023
Health Equity
could be one of those ‘big’ unifying ideas..• if we see opportunities for good health and wellbeing as a basic right of
all• if we see these pervasive health disparities as not only incredibly
damaging to so many, but also as an indictment of an unequal society• if we recognize that coming together to address the social determinants
that underlie health inequalities will benefit many other spheres – from better early child development to building a non-racist society
• if we see that addressing the roots of so many of our social problems requires broad collaboration and mobilization
• thinking of what needs to be done to create health equity is a way of imagining and forging a powerful vision of a progressive future
• and showing that we can get there from here
47

© The Wellesley Institutewww.wellesleyinstitute.com
Key Messages• health disparities are pervasive and deep-seated – but can’t let that paralyze
us• do need a comprehensive and coherent health equity strategy – but don’t
wait for perfect strategy• think big and think strategically – but get going• there is a solid base of evidence, provider experience, commitment and
community connections to build on
• have set out a roadmap – of strategies, principles and tools -- to drive equity into action through policy change and community mobilization
• many within the health system and beyond have long experience and strong commitment to equity → build on this to drive coordinated and coherent system-wide equity agenda into action
• work in partnerships and collaborations well beyond the health care system to address the underlying determinants of health inequalities
48
© The Wellesley Institutewww.wellesleyinstitute.com
• these speaking notes and further resources on policy directions to enhance health equity, health reform and the social determinants of health are available on our site at http://wellesleyinstitute.com
• my email is [email protected]• I would be interested in any comments on the
ideas in this presentation and any information or analysis on initiatives or experience that address health equity
Following Up
49
© The Wellesley Institutewww.wellesleyinstitute.com
Wellesley Roadmap for Action on the Social Determinants of Health
1. look widely for ideas and inspiration from jurisdictions with comprehensive health equity policies, and adapt flexibly to Canadian, provincial and local needs and opportunities;
2. address the fundamental social determinants of health inequality – macro policy is crucial, reducing overall social and economic inequality and enhancing social mobility are the pre-conditions for reducing health disparities over the long-term;
3. develop a coherent overall strategy, but split it into actionable and manageable components that can be moved on;
4. act across silos – inter-sectoral and cross-government collaboration and coordination are vital;
5. set and monitor targets and incentives – cascading through all levels of government and programme action;
50
© The Wellesley Institutewww.wellesleyinstitute.com
Wellesley Roadmap II6 rigorously evaluate the outcomes and potential of programme initiatives and
investments – to build on successes and scale up what is working; 7 act on equity within the health system:
• making equity a core objective and driver of health system reform – every bit as important as quality and sustainability;
• eliminating unfair and inefficient barriers to access to the care people need;• targeting interventions and enhanced services to the most health
disadvantaged populations;8 invest in those levers and spheres that have the most impact on health
disparities such as:• enhanced primary care for the most under-served or disadvantaged
populations;• integrated health, child development, language, settlement, employment, and
other community-based social services;
51
© The Wellesley Institutewww.wellesleyinstitute.com
Wellesley Roadmap III9 act locally – through well-focussed regional, local or neighbourhood cross-
sectoral collaborations and integrated initiatives;10 invest up-stream through an equity lens – in health promotion, chronic care
prevention and management, and tackling the roots of health disparities;11 build on the enormous amount of local imagination and innovation going on
among service providers and communities across the country;12 pull all this innovation, experience and learning together into a continually
evolving repertoire of effective programme and policy instruments, and into a coherent and coordinated overall strategy for health equity.
52
The Wellesley Institute advances urban health through rigorous research, pragmatic policy solutions, social innovation, and community action.
© The Wellesley Institutewww.wellesleyinstitute.com
© The Wellesley Institutewww.wellesleyinstitute.com 53