Embed Size (px)
Citation preview

Le suivi du patient à haut risque CVPrise en charge de la dyslipémie
Dr Pierre TroisfontainesCardiologue
Dr Pierre Troisfontaines• Cardiologue au C.H.R. de la Citadelle (Liège)• Cardiologue au Centre Cardio-vasculaire Piercot
• Responsable du Centre de l’Insuffisance cardiaque du CHR
• Membre de la Société Belge de Cardiologie.
• Président du Belgian Working Group on Heart Failure and Cardiac Function.
• Membre de la Heart Failure Association (HFA-ESC).
• Vice-président de l’ASBL, « Mon Cœur Entre Parenthèses ».
MALADIES CARDIO-VASCULAIRES
1e cause de mortalité en Belgique et dans le monde
(OMS Europe).17,5 millions de morts en 2012
soit 31% de la mortalité mondiale totale,
Poste le plus important de consommation de soins et de
biens médicaux.
11,5 % des hospitalisations.
Augmentation de la prévalence en raison du vieillissement de
la population et des modifications des facteurs de
risque
Modification des facteurs de risque : augmentation de
l’incidence de l’obésité et du diabète et augmentation du
tabagisme féminin
INTRODUCTION


2016 European Guidelines on cardiovascular disease prevention in
clinical practiceThe Sixth Joint Task Force of the European Society of Cardiology and Other Societies on Cardiovascular Disease Prevention in Clinical Practice (constituted by representatives of 10 societies and by invited experts)Developed with the special contribution of the European Association for Cardiovascular Prevention & Rehabilitation (EACPR)
European Heart Journal. doi:10.1093/eurheartj/ehw106, online May 2016
European Society of Cardiology (ESC), European Association for Cardiovascular Prevention & Rehabilitation (EACPR), European Society of Hypertension (ESH), International Society of Behavioral Medicine (ISBM), European Heart Network (EHN), European Association for the Study of Diabetes (EASD), European Atherosclerosis Society (EAS), International Diabetes Federation Europe (IDF-Europe), European Society of General Practice/Family Medicine (ESGP/FMI/Wonca), European Stroke Initiative (EUSI), International Federation of Sports Medicine
Guidance for Cholesterol management

Risk categories
ACS, acute coronary syndrome; AMI, acute myocardial infarction; BP, blood pressure; CKD, chronic kidney disease; DM, diabetes mellitus; GFR, glomerular filtration rate; PAD, peripheral artery disease; SCORE, systematic coronary risk estimation; TIA, transient ischaemic attack.
European Heart Journal. doi:10.1093/eurheartj/ehw106, online May 2016

Risk factor goals and targets for important CV risk factors
European Heart Journal. doi:10.1093/eurheartj/ehw106, online May 2016
CV, cardiovascular; HDL-C, high density lipoprotein cholesterol; LDL-C, lowdensity lipoprotein cholesterol; PA, physical activity; BMI, body mass index;
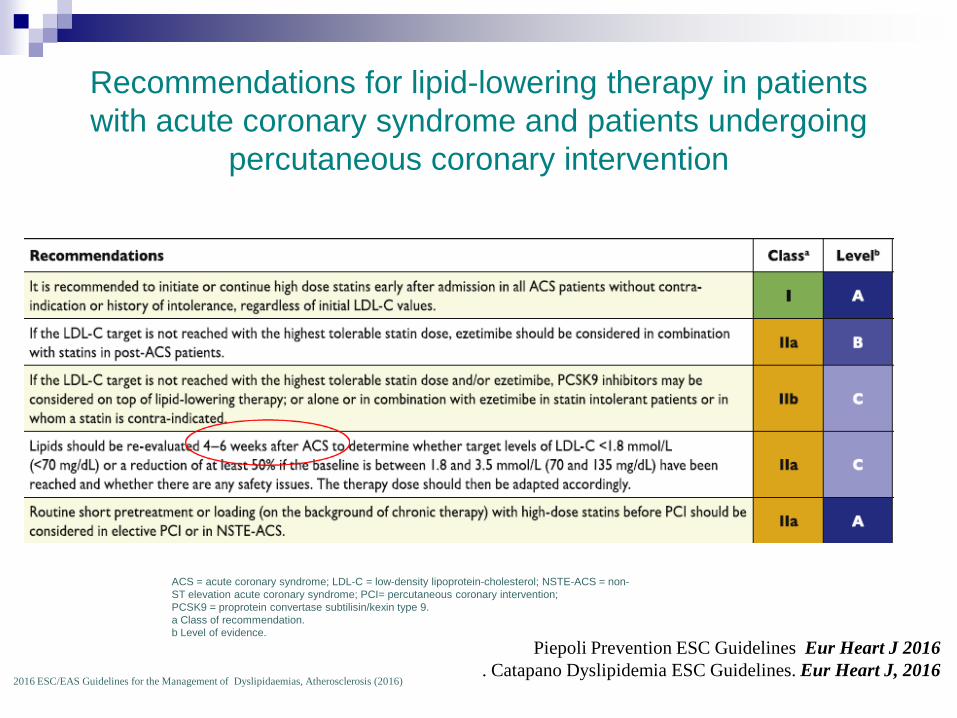
Recommendations for lipid-lowering therapy in patients with acute coronary syndrome and patients undergoing
percutaneous coronary intervention
ACS = acute coronary syndrome; LDL-C = low-density lipoprotein-cholesterol; NSTE-ACS = non-ST elevation acute coronary syndrome; PCI= percutaneous coronary intervention;PCSK9 = proprotein convertase subtilisin/kexin type 9.a Class of recommendation.b Level of evidence.
2016 ESC/EAS Guidelines for the Management of Dyslipidaemias, Atherosclerosis (2016)
Piepoli Prevention ESC Guidelines Eur Heart J 2016. Catapano Dyslipidemia ESC Guidelines. Eur Heart J, 2016
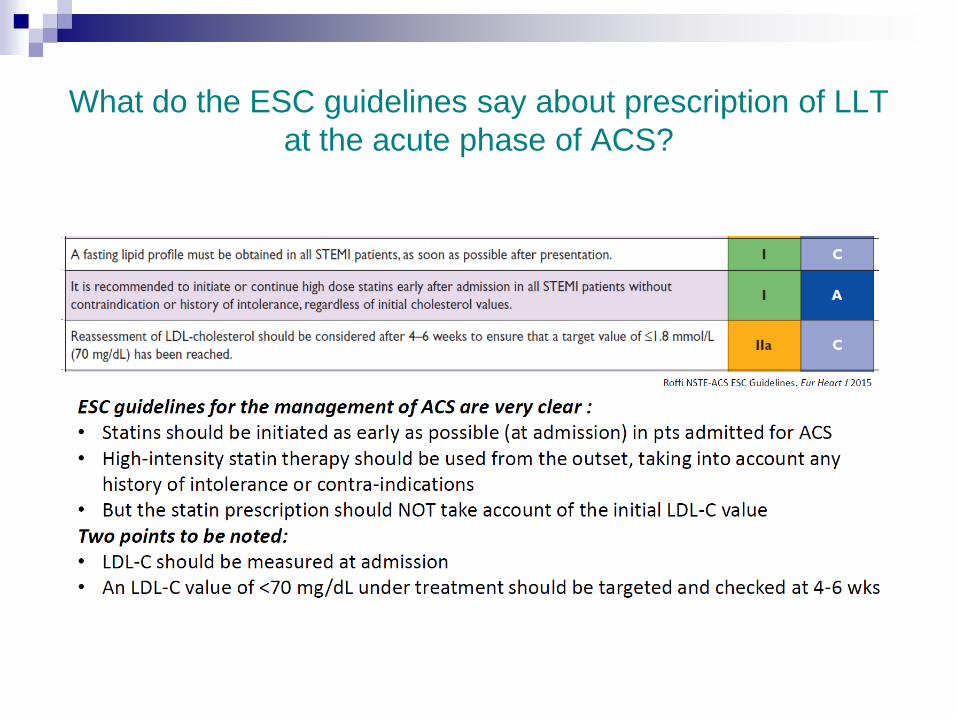
What do the ESC guidelines say about prescription of LLTat the acute phase of ACS?
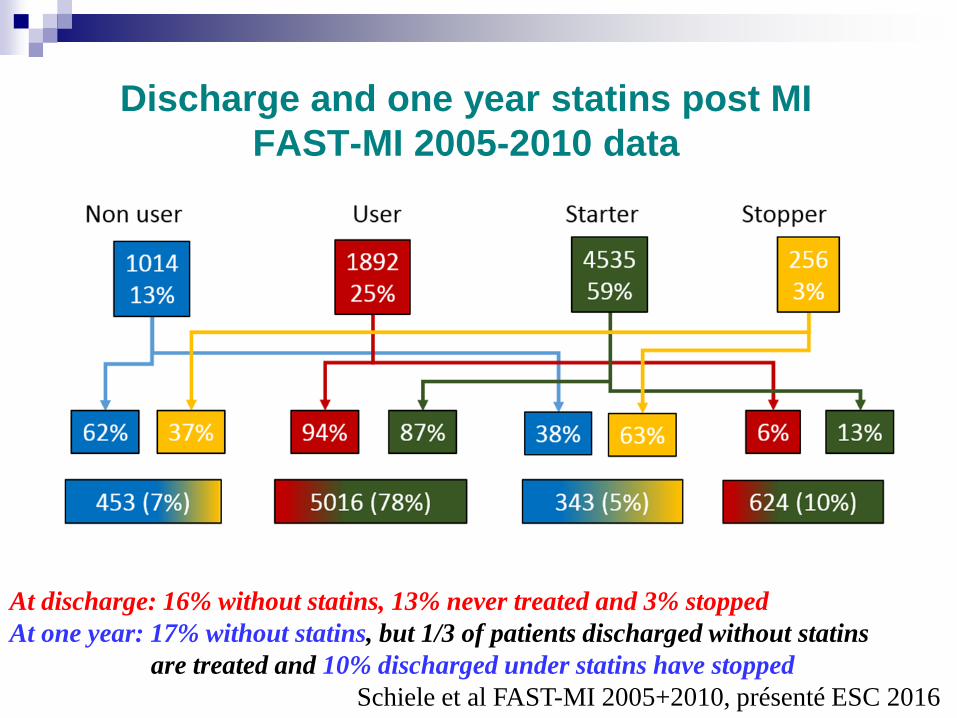
Discharge and one year statins post MIFAST-MI 2005-2010 data
At discharge: 16% without statins, 13% never treated and 3% stoppedAt one year: 17% without statins, but 1/3 of patients discharged without statins
are treated and 10% discharged under statins have stoppedSchiele et al FAST-MI 2005+2010, présenté ESC 2016
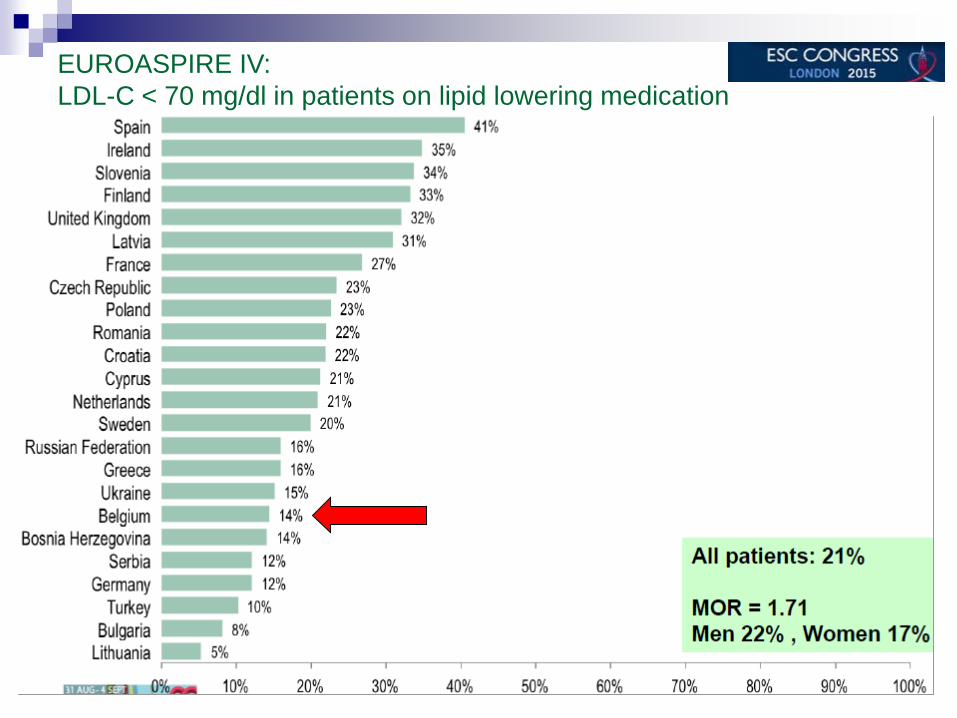
EUROASPIRE IV: LDL-C < 70 mg/dl in patients on lipid lowering medication
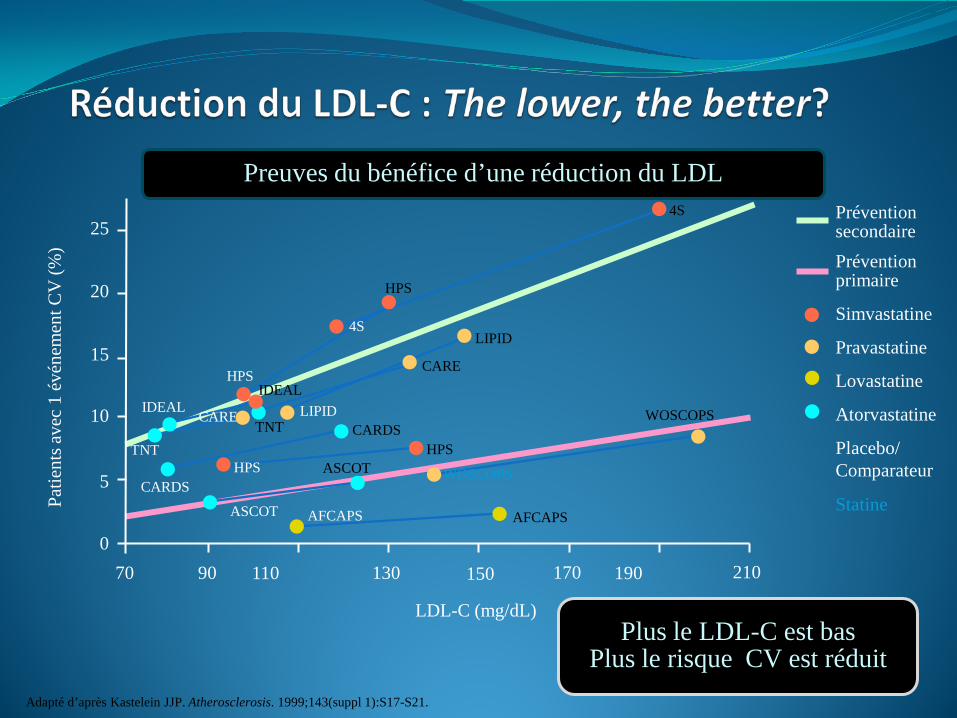
Adapté d’après Kastelein JJP. Atherosclerosis. 1999;143(suppl 1):S17-S21.
Pravastatine
PréventionsecondairePrévention primaire
Simvastatine
Lovastatine
Atorvastatine
0
5
10
15
20
25
Patie
nts a
vec
1 év
énem
entC
V (%
)
Preuves du bénéfice d’une réduction du LDL
StatineASCOT AFCAPS
WOSCOPS
CARE LIPID
4S
HPS
HPS
CARDS
TNT
IDEAL
Placebo/Comparateur
TNTWOSCOPS
LIPID
4S
CARE
AFCAPS
ASCOTHPS
HPS
CARDS
IDEAL
21070 110 130 150 170 19090
LDL-C (mg/dL)Plus le LDL-C est bas
Plus le risque CV est réduit

The importance of LDL-C lowering: CTT

1. Sever PS, et al. Lancet. 2003;361:1149-1158.2. IDEAL subanalysis. Pedersen, Olsson, Cater et al. Presented at World Congress of Cardiology 20063. LaRosa JC, et al. N Engl J Med. 2005;352:1425-1435.
LDL-C de base
LDL-C en fin d’étudemg/dL
SPARCL6
80 mgTNT5
80 mgCARDS4
10 mgTNT3
80 mgIDEAL2
80 mgASCOT-LLA1
10 mg
133 mg/dl160 mg/dl118 mg/dl98 mg/dl130 mg/dl133 mg/dl
77 mg/dl 73 mg/dl 82 mg/dl 77 mg/dl 80 mg/dl 90 mg/dl
4. Colhoun HM, et al. Lancet. 2004;364:685-696.5. Shepherd J et al. Diabetes Care. 2006;29:1220-1226.6. The SPARCL Investigators N Engl J Med. 2006;355:549-559.
Critère d’évaluation
primaire
Mortalitécoronarienne et
IM non fatal
- 36% - 25%
EvénementsCV majeurs
- 34% - 22% - 37%
Evénements CV majeurs
Evénements CV majeurs
AVC fatal ou non fatal
- 16%
Evénementscoronariens majeurs
Bénéfices substantiels sur un large spectre de patients avec différents risques CV traités par
atorvastatine
Hypertendus à haut risque CV sans antécédent
Patients en SCAPatients avec
maladies coronaires stables
Diabétiques sans antécédents CV
Diabétiques avec antécédents CV
Patients avec antécédentsd’AVC/AIT

15
1. Jones PH et al. Am J Cardiol. 2003;92:152–160. 2. SmPC Zocor (simvastatin), 06/2015
STELLAR: LDL-C Reductions With Statin Monotherapy1
A 6-week, parallel-group, open-label, randomized, multicenter study comparing LDL-reducing efficacy of rosuvastatin vs atorvastatin, simvastatin, and pravastatin across the dose ranges in adults with hypercholesterolemia (n=2,431; per dose group, n=156–167), after dietary lead-in.
Mea
n ch
ange
in L
DL-
Cfr
om u
ntre
ated
bas
elin
e, %
10 mg20 mg40 mg80 mg
–55–45–35–25–15–5
–28%–37%
–7%
–6%
–6%
–3%
–5%
–4%
–3%
Atorvastatin RosuvastatinbSimvastatina
–20%
–4%–6%
Pravastatin
–46%
–53
–37–42 –45
–54
-70
-60
-50
-40
-30
-20
-10
0
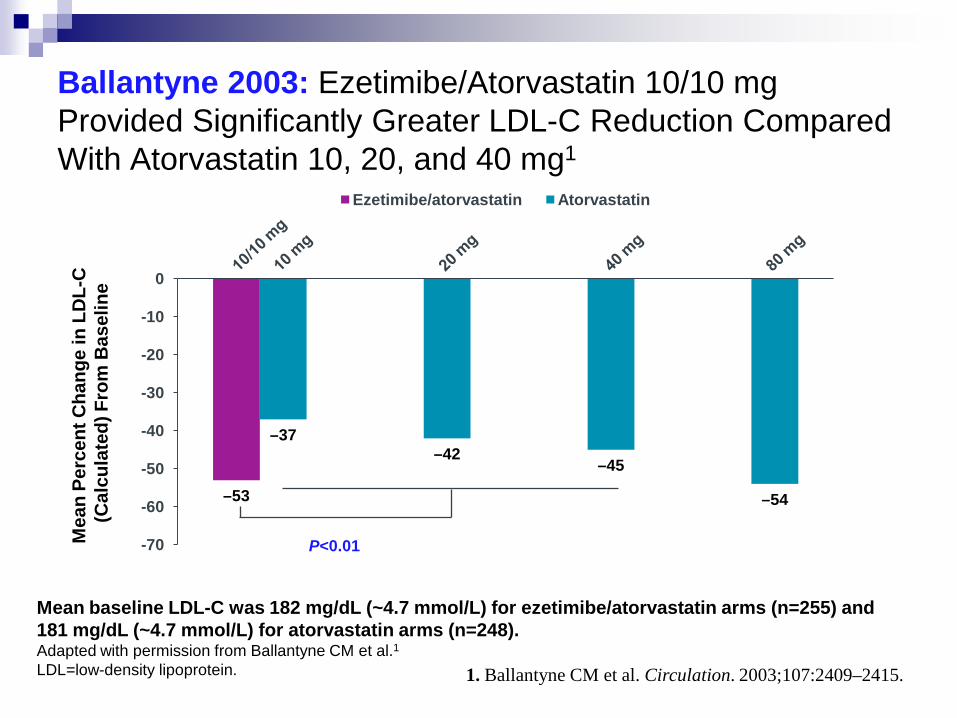
Ezetimibe/atorvastatin Atorvastatin
Ballantyne 2003: Ezetimibe/Atorvastatin 10/10 mg Provided Significantly Greater LDL-C Reduction Compared With Atorvastatin 10, 20, and 40 mg1
Mean baseline LDL-C was 182 mg/dL (~4.7 mmol/L) for ezetimibe/atorvastatin arms (n=255) and 181 mg/dL (~4.7 mmol/L) for atorvastatin arms (n=248).Adapted with permission from Ballantyne CM et al.1LDL=low-density lipoprotein.
Mea
n Pe
rcen
t Cha
nge
in L
DL-
C
(Cal
cula
ted)
Fro
m B
asel
ine
P<0.01
1. Ballantyne CM et al. Circulation. 2003;107:2409–2415.

Ezetimibe/atorvastatin 10/40 mg(n=277)
Atorvastatin 80 mg(n=279)
74%32%
Mean Statin-TreatedBaseline LDL-C: 89 mg/dL (~2.3 mmol/L)
Mean Statin-TreatedBaseline LDL-C: 90 mg/dL (~2.3 mmol/L)
P<0.001
The mean decrease in LDL-C from statin-treated baseline was 27% with ezetimibe/atorvastatin 10/40 mg compared with 11% with atorvastatin 80 mg; P<0.001.
LDL=low-density lipoprotein. 1. Leiter LA et al. Am J Cardiol. 2008;102:1495–1501.
EZ-PATH: More Than Twice as Many Patients Reached LDL-C <70 mg/dL With Ezetimibe/ Atorvastatin 10/40 mg vs Doubling
Atorvastatin Dose to 80 mg1
Patients Reaching LDL-C <70 mg/dL (~1.8 mmol/L) at 6 weeks, as a Result of Greater LDL-C Reduction

IMPROVE IT : IMProved Reduction of OutcomesVytorin Efficacy International Trial
AHA 2014 – D'après Cannon CP et al., abstract LB2, actualisé
Patients stables post SCA ≤ 10 jours :LDL-C 50–125*mg/dL (ou 50–100**mg/dL si traitement hypolipémiant antérieur)
Tt médical standard & Tt interventionnel
Ezetimibe / Simvastatine10 / 40 mg
Simvastatine40 mg
Visite de suivi à J30, puis tous les 4 mois
Durée : suivi minimum 2 ans ½ (au moins 5250 événements)
Critère principal :décès CV, IDM, hospitalisation pour angor instable,Revascularisation coronarienne (≥ 30 j après randomisation) ou AVC
n = 18 144Titrage jusqu’àSimva 80 mg
si LDL-C >79
*3,2 mM**2,6 mM
Puissance de 90 % pourDétecter une différence ~9 %
Cannon CP AHJ 2008;156:826-32; Califf RM NEJM 2009;361:712-7; Blazing MA AHJ 2014;168:205-12

Caractéristiques patients à l’inclusion
AHA 2014 – D'après Cannon CP et al., abstract LB2, actualisé
40
50
60
70
80
90
100
QE R 1 4 8 12 16 24 36 48 60 72 84 96
LDL-
C m
oyen
(mg/
dl)
Mois depuis la randomisation
Simvastatine(n = 9 077)[%]
EZ/Simva(n = 9 067)[%]
Age (années) 64 64Femmes 24 25Diabétiques 27 27ATCDd’IDM avant SCA index 21 21STEMI / NSTEMI / angor instable 29 / 47 / 24 29 / 47 / 24Délai post SCA –randomisation en jours (IQR) 5 (3, 8) 5 (3, 8)Cath / angioplastie pour SCA 88 / 70 88 / 70Traitement hypolipémiant antérieur (%) 35 36LDL-C (mg/dL) (IQR) 95 (79, 110) 95 (79,110)
Moyenneà 1 an LDL-C TC TG HDL CRP usSimva 69,9 145,1 137,1 48,1 3,8EZ/Simva 53,2 125,8 120,4 48,7 3,3Δ en mg/dl -16,7 -19,3 -16,7 +0,6 -0,5
Différence moyenne69,5 vs 53,7 mg/dl
SimvastatineEzetimibe/simvastatine
Évolution du LDL-C et du bilan lipidique

0
10
20
30
40
0 1 2 3 4 5 6 7
Even
t rat
e (%
)
Années depuis la randomisation
IMPROVE IT Critère principal – ITT
AHA 2014 – D'après Cannon CP et al., abstract LB2, actualisé
Simva – 34,7 % 2 742 événements
EZ/Simva – 32,7 % 2 572 événements
NNT = 50
HR = 0,936 ; IC95 : 0,887-0,988 ;p = 0,016
• Décès CV, IDM, réhospitalisation pour angor instable, revascularisation coronarienne (≥ 30 jours) ou AVC
Réduction du risque de 6,4 %

Total Primary Endpoint EventsTotal
N=9545
Sabina A. Murphy ACC 2015

Total Primary Endpoint Events#
Eve
nts
Ezetimibe Simvastatin
Simvastatin Alone
45624983
Total Events RR 0.91P=0.007
Additional EventsRR 0.88
(0.79-0.98)
1st Event HR 0.936P=0.016
-421
-251
-170
ACC 2015


Algorithme du traitement des dyslipidémies en prévention cardiovasculaire
O. S. Descamps; Louvain Medical


En conclusion: Evaluer le risque cardio-vasculaire global du patient. Impliquer le patient dans la démarche thérapeutique Définir la valeur cible du LDL-C et le pourcentage de
réduction nécessaire. Choisir la statine qui permettra cette réduction Augmenter les doses de statine jusqu’à obtention du
résultat (recommandation de classe IA) Si les statines sont insuffisantes, associer à d’autres
médicaments. (recommandation de classe IIb C ) De nouvelles molécules apparaissent également comme
les inhibiteurs des PCSK9.

Actualités:Controverses sur les Statines

Aujourd'hui, l'étude du professeur Nicholas Moore de l'Université de Bordeaux, spécialisé en cardiologie et en pharmacologie, avance que cet ouvrage aurait fait 10.000 morts en France, et 2000 morts en Belgique.
Les professeurs Philippe Even et Bernard Debré interdits d'exercer la médecine pendant un an. Chambre disciplinaire de l'ordre des médecins d'Ile-de-France
En 2011 et 2012, le taux d'arrêt de la statine était de 8,5% des patients traités avec ce médicament.
En 2013, de 11,9% soit 40% d'augmentation. Les auteurs de l'étude estiment à 13% la hausse de mortalité dans le groupe à risque intermédiaire, le plus nombreux.
De là, ils extrapolent à toute la population française pour arriver à une mortalité supplémentaire de 10 000.
RTBF – Le Soir Août 2016



Sune Fallgaard Nielsen SF, et al. Eur Heart J. 2016;37:908-916
Negative statin-related news stories decrease statin persistence and
increase myocardial infarction and cardiovascular mortality:
a nationwideprospective cohort study

Le Conseil supérieur de la santé veut interdired’urgence la levure de riz rouge Le Soir - Frédéric Soumois
• C’est aussi une statine ! • Ces produits s’apparentent donc à des médicaments avec le risque d’interaction,
d’effets indésirables (myalgie) et de mauvais usage (chez la femme enceinte, le très jeune enfant, en cas d’insuffisance hépatique ou rénale)
• Risque de cacher la véritable nature du produit (une statine), ce qui n’est pas éthique !• Manque de preuves solides que la levure de riz rouge est efficace et bien toléré à long
terme• Absence de standardisation entre les lots des préparations • Grande variabilité de composition parmi les centaines de produits distribués• Effets toxiques éventuels dus aux contaminants (dans certaines préparations) qui
apparaissent lors de la fermentation du riz et restent présents dans l’extrait, dont notamment des mycotoxines potentiellement dangereuses pour les reins.
• Prise multiple (1 à 4/jour) et coût important (> 20 euros par mois, non remboursé)
Polémique, intolérance, non adhérence et autres contrariétés autour de la prescription des statines ? Comment y faire face ?
Olivier S Descamps, Louvain med 2016; 135 (9): 600-608

Actualités:Contrôles et évaluation des ES

Incidence de Bénéfices 1000 cas en moins
d’évènement cardiovasculaire
(prévention secondaire)OU
500 des cas en moins d’évènement
cardiovasculaire(prévention primaire)
Incidence d’inconvénients 5 cas de myopathie (dont
un pourrait progresser vers la rhabdomyolyse),
50 à 100 cas de diabètes, 5 à 10 une AVC
hémorragique.
Prévalences estimées des bénéfices et inconvénients de la prise d’une statine (exemple atorvastatine 40 mg par jour)
par 10.000 patients pendant 5 ans
Collins R, et al. Lancet. 2016;388:2532-2561


Surveillance biologique des enzymes hépatiques et musculaires.
O. S. Descamps; Louvain Med. 2012; 131 (4): 166-176

Rhabdomyolysis and Statins• Very rare: 0.7 cases / 100,000 person-years• Can also occur in absence of statin therapy•Incidence for individual statins (AERS)
(1 reported case per number of prescriptions)• Lovastatin 5.2 million• Atorvastatin 23.4 million• Pravastatin 27.1 million• Simvastatin 8.3 million• Cerivastatin 320,000
FDA Adverse Reporting System• Rosuvastatin incidence similar to other statinsFDA Advisory 2005Statin dose-related incidence of rhabdomyolysis Compared to Atorvastatin 10mg:
• 40 mg HR 3.8 (95% CI 2.3-6.6)• 80mg HR 11.3 (95% CI 6.4-20.4)
Holbrook A et al. Can J Cardiol 2011; 27:146-51

CHECK-LIST for STATIN INTOLERANT PATIENT
Canadian Journal of Cardiology 2016


• Non-modifiable risk factors: >80 years, female, low BMI, Asian descent
• Excess physical activity, alcohol or grapefruit juice• Acute infection, hypothyroidism, impaired renal or hepaticfunction, organ transplant recipient, trauma, HIV, diabetes• Vitamin D deficiency• History of CK elevation or unexplained muscle/joint/tendonpain, myopathy while receiving another lipid-lowering therapy• Inflammatory or inherited metabolic, neuromuscular/muscledefects• Polymorphisms in CYP450 isoenzymes or drug transporters
Risk factors for statin-associated muscle symptoms (SAMS)
Stroes EK et al. EAS/ESC Eur Heart J. 2015;36:1012-22.

Risk Factors for Statin-Induced MyopathyStatin Dose and Pharmacodynamics
Statin dose– Muscle-related side effects not related to lipid lowering potency– Dose threshold generally above approved doses– High vs low statin dose• 7 RCT meta analysis N= 29,395• No increase in myopathyProperties of statin• Bioavailabity• Lipophilicity• Potential for drug interactions• CYP450 inhibitors• Inhibition of glucuronidation (eg. gemfibrozil)
Josan K et al. CMAJ 2008; 178:576-84


Risk Factors for Statin-Induced MyopathyDrug Interactions related to CYP Metabolism

• The only adverse events that have been reliably shown to becaused by statin therapy are myopathy (defined as musclepain or weakness combined with large increases in creatinekinase blood concentrations) and new-onsetdiabetes mellitus, along with a probable increase in strokesdue to bleeding (ie, haemorrhagic strokes).
• Typically, treatment of 10 000 patients for 5 years with astandard statin regimen (such as atorvastatin 40 mg daily)would be expected to cause about 5 cases of myopathy, 50–100 new cases of diabetes, and 5–10 haemorrhagic strokes.
Collins R, et al. Lancet. 2016;388:2532-2561
Recent review of statins’ benefit and safety

• Pre-treatment assessment• Assess risk (e.g. elderly, prior muscle pains, FH of myopathy, renaldisease, DM, hypothyroidism)• Consider exogenous factors (e.g. statin dose, alcohol use, drug-druginteractions, excessive grapefruit juice use)• Measure baseline CK, ALT, TSH, creatinine• Counseling• Inform that statins are very well tolerated in most people• Inform about muscular symptoms and when to discontinue• Monitoring• Check CK / ALT when monitoring lipid lowering efficacy• At 6-8 weeks after starting or with dose increase and then every6-12 m• Avoid severe exercise for several days prior to testing
Prevention of Statin Intolerance

• More common than clinical trials suggest• Probably more frequent at higher doses• Important cause of poor adherence to treatment• Prevent statin induced muscle adverse events• Manage adverse events• Use alternative statin• Reduce frequency of statin• Use non-statin agents as monotherapy or together with
reduced dose or frequency statin
ConclusionsAdverse Effects of Statin Treatment

Merci de votre attention
Yann Arthus-BertrandCOEUR DE VOH EN 1990, Nouvelle-Calédonie