Embed Size (px)
DESCRIPTION
Basics of ECG
Citation preview

BASICS OF ELECTROCARDIOGRAPH
Y
DR. MVN Suresh.AHA Instructor for BLS & ACLS

Introduction
• A recording of the electrical activity of the heart over time
• Gold standard for diagnosis of cardiac arrhythmias
• Helps detect electrolyte disturbances (hyper- & hypokalemia)
• Allows for detection of conduction abnormalities• Screening tool for ischemic heart disease during
stress tests• Helpful with non-cardiac diseases (e.g.
pulmonary embolism or hypothermia )

Recording of the ECG:
Leads used:• Limb leads are I, II, II. So called because at one
time subjects had to literally place arms and legs in buckets of salt water.
• Each of the leads are bipolar; i.e., it requires two sensors on the skin to make a lead.
• If one connects a line between two sensors, one has a vector.
• There will be a positive end at one electrode and negative at the other.
• The positioning for leads I, II, and III were first given by Einthoven, form the basis of Einthoven’s triangle

Important Precautions
Correct Lead placement and good contact Proper earth connection, avoid other
gadgets Deep inspiration record of L3, aVF Compare serial ECGs if available Relate the changes to Age, Sex, Clinical
history Consider the co-morbidities that may
effect ECG Make a xerox copy of the record for future
use Interpret systematically to avoid errors

ECG Bipolar Limb Leads
Bipolar leads record voltage between electrodes placed on wrists & legs (right leg is ground)
Lead I records between right arm & left arm
Lead II: right arm & left leg
Lead III: left arm & left leg

6
+
+ +
- - -
ECG Bipolar Limb Leads
R L
F
R
F
L

7
Standard ECG is recorded in 12 leads Six Limb leads – L1, L2, L3, aVR, aVL,
aVF Six Chest Leads – V1 V2 V3 V4 V5 and
V6 L1, L2 and L3 are called bipolar leads L1 between LA and RA L2 between LF and RA L3 between LF and LA
ECG Bipolar Limb Leads

8
8
ECG Chest Leads

9
Precardial (chest) Lead Position V1 Fourth ICS, right sternal border V2 Fourth ICS, left sternal border V3 Equidistant between V2 and V4 V4 Fifth ICS, left Mid clavicular Line V5 Fifth ICS Left anterior axillary line V6 Fifth ICS Left mid axillary line
ECG Chest Leads

10
The Six Chest Leads
TRANSVERSE PLANE

ECG Complex

12
ECG ComplexP wave
PR Interval
QRS complex
ST segment
T Wave
QT Interval
RR Interval

3 distinct waves are produced during cardiac cyc3 distinct waves are produced during cardiac cycleP wave caused by atrial depolarizationQRS complex caused by ventricular depolarizationT wave results from ventricular repolarizationle
ECG Complex

Cardiac Impulse
SA node -> atrial muscle -> AV node -> bundle of His -> Left and Right Bundle Branches -> Ventricular muscle

ECG ComplexElements of the ECG:• P wave: Depolarization of both atria;
• Relationship between P and QRS helps distinguish various cardiac arrhythmias
• Shape and duration of P may indicate Atrial enlargement
• PR interval: from onset of P wave to onset of QRS
• Normal duration = 0.12-2.0 sec (120-200 ms) (3-4 horizontal boxes)
• Represents atria to ventricular conduction time (through His bundle)
• Prolonged PR interval may indicate a 1st degree heart block
• QRS complex: Ventricular depolarization
• Larger than P wave because of greater muscle mass of ventricles
• Normal duration = 0.08-0.12 seconds
• Its duration, amplitude, and morphology are useful in diagnosing cardiac arrhythmias, ventricular hypertrophy, MI, electrolyte derangement, etc.
• Q wave greater than 1/3 the height of the R wave, greater than 0.04 sec are abnormal and may represent MI

ST segment:• Connects the QRS complex and T wave• Duration of 0.08-0.12 sec (80-120 msec
T wave: • Represents Repolarization or recovery of ventricles
• Interval from beginning of QRS to apex of T is referred to as the absolute refractory period
QT Interval:• Measured from beginning of QRS to the end of the T wave
• Normal QT is usually about 0.40 sec• QT interval varies based on heart rate
ECG Complex

17
17
X-Axis represents time - Scale X-Axis – 1 mm = 0.04 sec Y-Axis represents voltage - Scale Y-Axis – 1 mm = 0.1
mV Runs at a paper speed of 25mm/sec One big square on X-Axis = 0.2 sec (big box) Two big squares on Y-Axis = 1 milli volt (mV) Each small square is 0.04 sec (1 mm in size at a speed
of 25mm/sec) Each big square on the ECG represents 5 small squares
= 0.04 x 5 = 0.2 seconds 5 such big squares = 0.2 x 5 = 1sec = 25 mm One second is 25 mm or 5 big squares One minute is 5 x 60 = 300 big squares
ECG Graph Paper

18
18
Next QRS
Rate Determination
QRS

19
No. of Big Boxes
R – R Interval Rate Cal.
Rate
One 0.2 sec 60 ÷ 0.2 300
Two 0.4 sec 60 ÷ 0.4 150
Three 0.6 sec 60 ÷ 0.6 100
Four 0.8 sec 60 ÷ 0.8 75
Five 1.0 sec 60 ÷ 1.0 60
Six 1.2 sec 60 ÷ 1.2 50
Seven 1.4 sec 60 ÷ 1.4 43
Eight 1.6 sec 60 ÷ 1.6 37
BRADY
T ACHY
NORMA L
Rate Determination

20
20
What is the Heart Rate ?
Answer on next slide

21
To find out the heart rate we need to know The R-R interval in terms of # of big
squares If the R-R intervals are constant
In this ECG the R-R intervals are constant
R-R are approximately 3 big squares apart
So the heart rate is 300 ÷ 3 = 100
What is the Heart Rate ?

22
22
What is the Heart Rate ?
Answer on next slide

23
To find out the heart rate we need to know The R-R interval in terms of # of big
squares If the R-R intervals are constant
In this ECG the R-R intervals are constant R-R are approximately 4.5 big squares apart So the heart rate is 300 ÷ 4.5 = 67
What is the Heart Rate ?

24
24
What is the Heart Rate ?
Answer on next slide

25
To find out the heart rate we need to know The R-R interval in terms of # of Big
Squares If the R-R intervals are constant
In this ECG the R-R intervals are not constant
R-R are varying from 2 boxes to 3 boxes It is an irregular rhythm – Sinus arrhythmia Heart rate is 300 ÷ 2 to 3 = 150 to 100
approx
What is the Heart Rate ?

26
26
QRS Axis
SE
NENW
SW

27
QRS Axis
The QRS electrical (vector) axis can have 4 directions
Normal Axis - when it is downward and to the left – southeast quadrant – from -30 to +90 degrees
Right Axis – when it is downward and to the right – southwest quadrant – from +90 to 180 degrees
Left Axis – when it is upward and to the left – Northeast quadrant –from -30 to -90 degrees
Indeterminate Axis – when it is upward & to the right – Northwest quadrant – from -90 to +180

28
28
Axis Determination
NORMAL RIGHT LEFT
MEET LEAVEALL UPRIGHT

29
Axis LI LIII aVF TIP
Normal Positive Positive Both Up
Right Negative Positive Meet
Left Positive Negative Leave
Indeterminae Negative Positive Meet
Axis Determination

30
30
LEAD 1
LEAD 2
LEAD 3
aVR
aVL
aVF
What is the Axis ?

31
ECG With Normal Axis
Note the QRS voltages are positive and upright in the leads - L1, L2, L3 and aVF
L2, L3 and aVF tell that it is downward
L1, aVL tell that it is to the left Downward and leftward is
Normal Axis Normal QRS axis

32
32
LEAD 1
LEAD 2
LEAD 3
aVR
aVL
aVF
What is the Axis ?

33
ECG With Left Axis
Note the QRS voltages are positive and upright in leads L1and aVL
Negative in L2, L3 and aVF L1, aVL tell that it is leftward L2, L3, and aVF tell that it is not down ward
- instead it is upward Upward and Leftward is Left Axis See the Left - Leave criterion QRS in L1
and L3 leave each other Left Axis Deviation - LAD

34
34
Normal ECG

35
Normal ECG Standardization – 10 mm (2 boxes) = 1 mV Double and half standardization if required Sinus Rhythm – Each P followed by QRS, R-R constant P waves – always examine for in L2, V1, L1 QRS positive in L1, L2, L3, aVF and aVL. – Neg in aVR QRS is < 0.08 narrow, Q in V5, V6 < 0.04, < 3 mm R wave progression from V1 to V6, QT interval < 0.4 Axis normal – L1, L3, and aVF all will be positive ST Isoelectric, T waves ↑, Normal T↓ in aVR,V1, V2

36
36
Pediatric ECG

37
This is the ECG of a 6 year old child Heart rate is 100 – Normal for the
age See V1 + V5 R >> 35 – Not LVH –
Normal T↓ in V1, V2, V3 – Normal in child Base line disturbances in V5, V6 –
due to movement by child
Pediatric ECG

38
Juvenile ECG

39
39
Be aware of normal ECG Normal Resting ECG – cannot exclude disease Ischemia may be covert – supply / demand equation Changes of MI take some time to develop in ECG Mild Ventricular hypertrophy - not detectable in ECG Some of the ECG abnormalities are non specific Single ECG cannot give progress – Need serial ECGs ECG changes not always correlate with Angio results Paroxysmal events will be missed in single ECG

40
Normal Variations in ECG May have slight left axis due to rotation of
heart May have high voltage QRS – simulating LVH Mild slurring of QRS but duration < 0.09 J point depression, early repolarization T inversions in V2, V3 and V4 – Juvenile T ↓ Similarly in women also T↓ Low voltages in obese women and men Non cardiac causes of ECG changes may occur

Normal Variations in ECG

42
Early Repolarization
This ECG has all normal featuresThe ST-T (J) Junction point is elevated. T waves are tall, May be inverted in LIII, The ST segment initial portion is concave. This does not signify
Ischemia

43
43
Pseudo Normalization
Before Chest pain
During Chest pain
Chest pain Relieved
T↓
T↓
T↑

44
44
Atrial Waves

45
45
Left Atrial Enlargement

46
46
Left Atrial Enlargement
P wave duration is 4 boxes-0.04 x 4 = 0.16

47
Always examine V 1 and Lead 1 for LAE Biphasic P Waves, Prolonged P waves P wave 0.16 sec, ↑ Downward component Systemic Hypertension, MS and or MR Aortic Stenosis and Regurgitation Left ventricular hypertrophy with dysfunction Atrial Septal Defect with R to L shunt
Left Atrial Enlargement

48
48
Right Atrial Enlargement

49
49
Right Atrial Enlargement
P wave voltage is 4 boxes or 4 mm

50
Always examine Lead 2 for RAE Tall Peaked P Waves, Arrow head P
waves Amplitude is 4 mm ( 0.4 mV) -
abnormal Pulmonary Hypertension, Mitral
Stenosis Tricuspid Stenosis, Regurgitation Pulmonary Valvular Stenosis Pulmonary Embolism Atrial Septal Defect with L to R shunt
Right Atrial Enlargement

51
51
Ventricular Hypertrophy Ventricular Muscle
Hypertrophy QRS voltages in V1 and
V6, L 1 and aVL We may have to record
to ½ standardization T wave changes
opposite to QRS direction
Associated Axis shifts Associated Atrial
hypertrophy

52
52
Right Ventricular Hypertrophy

53
Tall R in V1 with R >> S, or R/S ratio > 1 Deep S waves in V4, V5 and V6 The DD is RVH, Posterior MI, Anti-clock
wise rotation of Heart Associated Right Axis Deviation, RAE Deep T inversions in V1, V2 and V3 Absence of Inferior MI
Right Ventricular Hypertrophy

54
54
Is there any hypertrophy ?

55
Criteria and Causes of RVH Criteria of RVH Tall R in V1 with R >> S, or R/S ratio > 1 Deep S waves in V4, V5 and V6 The DD is RVH, Posterior MI, Rotation Associated Right Axis Deviation, RAE Deep T inversion in V1, V2 and V3Cause of RVH Long standing Mitral Stenosis Pulmonary Hypertension of any cause VSD or ASD with initial L to R shunt Congenital heart with RV over load Tricuspid regurgitation, Pulmonary stenosis

56
56
What is in this ECG ?

57
ECG OF MS with RVH, RAE
Classical changes seen are Right ventricular hypertrophy Right axis deviation Right Bundle Branch Block P – Pulmonale - Right Atrial enlargement P – Mitrale – Left Atrial enlargement If Atrial Fibrillation develops – ‘P’
disappears

58
58
Left Ventricular Hypertrophy

59
High QRS voltages in limb leads R in Lead I + S in Lead III > 25 mm S in V1 + R in V5 > 35 mm R in aVL > 11 mm or S V3 + R aVL >
24 ♂, > 20 ♀ Deep symmetric T inversion in V4, V5
& V6 QRS duration > 0.09 sec Associated Left Axis Deviation, LAE Cornell Voltage criteria, Estes point
scoring
Left Ventricular Hypertrophy

60
60
What is in this ECG ?

61
Causes of LVH Pressure overload - Systemic Hypertension, Aortic
Stenosis Volume overload - AR or MR - dilated cardiomyopathy VSD - cause both right & left ventricular volume
overload Hypertrophic cardiomyopathy – No pressure or volume
overloadCriteria of LVH High QRS voltages in limb leads R in Lead I + S in Lead III > 25 mm or S in V1 + R in V5
> 35 mm R in aVL > 11 mm or S V3 + R aVL > 24 ♂, > 20 ♀ Deep symmetric T inversion in V4, V5 & V6 QRS duration > 0.09 sec, Associated Left Axis
Deviation, LAE
Causes and Criteria of LVH

62
62
Atrial EctopicsAPC
APCAPC
APC

63
Note the premature (ectopic) beats marked as
APC (Atrial Premature Contractions) These occurred before the next
expected QRS complex (premature) Each APC has a P wave preceding
the QRS of that beat – So impulse has originated in the atria
The QRS duration is normal < 0.08, not wide
Atrial Ectopics

66
66
Complete RBBB

67
67
Complete LBBB

68
Complete LBBB Complete LBBB has a QRS duration > 0.12 sec Prominent S waves in lead V1, R in L I, aVL, V6 Usually broad, Bizarre R waves are seen, M
pattern Poor R progression from V1 to V3 is common. The "normal" ST-T waves in LBBB should be
oriented opposite to the direction of the QRS Incomplete LBBB looks like LBBB but QRS
duration is 0.10 to 0.12 sec, with less ST-T change.
This is often a progression of LVH changes.

69
69
Blood Supply of Heart
LCA
RCA
LAD
LCX
RCA

70
Heart has four surfaces Anterior surface – LAD, Left Circumflex (LCx) Left lateral surface – LCx, partly LAD Inferior surface – RCA, LAD terminal portion Posterior surface – RCA, LCx branches Rt. and Lt. coronary arteries arise from aorta They are 2.5 mm at origin, 0.5 mm at the end Coronary arteries fill during diastole Flow - epicardium to endocardium –
poverty/plenty
Blood Supply of Heart

71
71
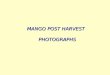
Ischemia, Injury & Infarction
Myocardial Ischemia
Myocardial Injury
Myocardial Infarction
1. Ischemia produces ST segment depression with or without T inversion
2. Injury causes ST segment elevation with or without loss of R wave voltage
3. Infarction causes deep Q waves with loss of R wave voltage.

72
72
Ischemia and Infarction
TRANSMURAL Injury ST Elevation

73
Ischemic Heart Disease (IHD)
Blood supply Sub-endocardial
Transmural
IschemiaTransient loss
StableAngina
Variant Angina
InfarctionPersistent loss
NSTEMIACS
STEMIACS
ST Segment Depressed Elevated

74
74
Interpret this ECG

75
NSTEMI
Non ST ↑ MI or NSTEMI, Non Q MI Or also called sub-endocardial Infarction Non transmural, restricted to the sub-
endocardial region - there will be no ST ↑ or Q waves
ST depressions in anterio-lateral & inferior leads
Prolonged chest pain, autonomic symptoms like nausea, vomiting, diaphoresis
Persistent ST-segment ↓even after resolution of pain

76
76
What are these ECGs

77
STEMI and QWMI
STEMI and QWMI ST ↑ signifies severe transmural myocardial
injury – This is early stage before death of the muscle tissue – the infarction
Q waves signify muscle death – They appear late in the sequence of MI and remain for a long time
Presence of either is an indication for thrombolysis

78
78
Evolution of Acute MI
A – Normal ST segment and T waves
B – ST mild ↑ and prominent T waves
C – Marked ST ↑ + merging upright T
D – ST elevation reduced, T↓,Q starts
E – Deep Q waves, ST segment returning to baseline, T wave is inverted
F – ST became normal, T Upright, Only Q+

79
79
Critical Narrowing of LAD

80
80
Normal Q waves
Notice the small
Normal Q in Lead I

81
81
Pathological Q wave
Notice the deep & wide
Infarction Q in Lead I

82
82
Very Striking

83
Hyper Acute MI
Note the hyper acute elevation of ST The R wave is continuing with ST and
the complexes are looking rectangular Some times tall and peaked T waves in
the precardial leads may be the only evidence of impending infarct
Sudden appearance LBBB indicates MI MI in Dextro-cardia – right sided leads
are to be recorded

84
Hyper Acute MI
Note the hyper acute elevation of ST The R wave is continuing with ST and
the complexes are looking rectangular
Some times tall and peaked T waves in the precardial leads may be the only evidence of impending infarct
Sudden appearance LBBB indicates MI
MI in Dextro-cardia – right sided leads are to be recorded

85
85
Severe Chest Pain – Why ?

86
Acute Anterio-lateral MI
Note the marked ST elevations in chest leads V2 to V5 and also ST↑ in L1 & aVL
T inversions have not appeared as yet
R wave voltages have dropped markedly in V3, V4, V5 and V6
Small R in L1 and aVL.

87
87
Which wall MI ?

88
88
Acute True Posterior MI

89
Due to occlusion of the distal Left circumflex artery or posterior descending or distal right coronary artery
Mirror image changes or reciprocal changes in the anterior precardial leads
Lead V1 shows unusually tall R wave (it is the mirror image of deep Q)
V1 R/S > 1, Differential Diagnosis - RVH
Acute True Posterior MI

Sinus Bradycardia
What is the rhythm?

Tachyarrhythmias
What is the rhythm?

Tachyarrhythmias
Ectopic rate nomenclature:
[150-250] Paroxysmal tachycardia
[250-350] Flutter
[350+] Fibrillation

AV Block
What is the rhythm?

AV Block

AV Block

Tachyarrhythmias
What is the rhythm?

Atrial Fibrillation

Monomorphic VT

V1
Polymorphic VT

“Torsade de Pointes”(Polymorphic VT Associated with Prolonged Repolarization)

Ventricular Fibrillation (VF)
• Totally chaotic rapid ventricular rhythm• Often precipitated by VT• Fatal unless promptly terminated (DC shock)

Sustained VT: Degeneration to VF

Atrial Fibrillation with Rapid Conduction ;Via Accessory Pathway: Degeneration to VF

Representation in culture:
• In TV medical dramas, an isoelectric ECG (no cardiac electrical activity, aka, flatline, is used as a symbol of death or extreme medical peril.
• Technically, this is known as asystole, a form of cardiac arrest, with a partcularly bad prognosis.
• Defibrillation, which can be used to correct arrythmias such as ventricular fibrillation and pulseless ventricular tachycardia, cannot correct asystole.
In common

SUMMARY Rate Rhythm Axis Intervals Hypertrophy Infarct
To summarize:1. Calculate RATE2. Determine RHYTHM3. Determine QRS AXIS4. Calculate INTERVALS5. Assess for HYPERTROPHY6. Look for evidence of INFARCTION