Embed Size (px)
Citation preview

ECHO IN AORTIC
STENOSIS AND
REGURGITATION
Dr V S R Bhupal

Normal Aortic valve Three cusps, crescent shaped
3 commissures 3 sinuses
supported by fibrous annulus
3.0 to 4.0 cm2
Node of arantius

2D Echo-Long axis view
Diastole Systole

2D Echo-Short axis viewDiastole Systole
Y or inverted Mercedes-Benz sign

2D - Apical five chamber view

2D – Suprasternal view

M Mode- Normal aortic valve

CAUSES AND
ANATOMIC
PRESENTATION

Aortic stenosis- Causes
Most common :-Bicuspid aortic valve with calcificationSenile or Degenerative calcific ASRheumatic AS
Less common:-CongenitalType 2 HyperlipoproteinemiaOchronosis

Combination of short and long axis images to identify
Number of leafletsDescribe leaf mobility, thickness, calcification
Combination of imaging and doppler allows the determination of the level of obstruction; subvalvular, valvular, or supravalvular.
Transesophageal echocardiography may be helpful when image quality is suboptimal.
Anatomic evaluation

Calcific Aortic Stenosis Nodular calcific masses on aortic side of cuspsNo commissural fusionFree edges of cusps are not involvedstellate-shaped systolic orifice

Calcific Aortic Stenosis
Parasternal long axis view showing echogenic and immobile aortic valve

Calcific Aortic Stenosis
Parasternal short-axis view showing calcified aortic valve leaflets. Immobility of the cusps results in only a slit like aortic valve orifice in systole

Bicuspid Aortic valve
Fusion of the right and left coronary cusps (80%) Fusion of the right and non-coronary cusps(20%)
Schaefer BM et al. Am J Cardiol 2007;99:686–90 Schaefer BM et al.Heart 2008;94:1634–
1638.

Two cusps are seen in systole with only two commissures framing an elliptical systolic orifice(the fish mouth appearance).
Diastolic images may mimic a tricuspid valve when a raphe is present.
Bicuspid Aortic valve

Bicuspid Aortic valve
Parasternal long-axis echocardiogram may show an asymmetric closure line systolic doming diastolic prolapse of the cusps
In children, valve may be stenotic without extensive calcification.
In adults, stenosis typically is due to calcific changes, which often obscures the number of cusps, making determination of bicuspid vs. tricuspid valve difficult

Calcific Aortic Stenosis
Calcification of a bicuspid or tricuspid valve, the severity can be graded semi-quantitatively as
0 1+ 2+ 3+ 4+ Schaefer BM et al.Heart 2008;94:1634–1638.
The degree of valve calcification is a predictor of clinical outcome. Rosenhek R et al. N Engl J Med 2000;343:611–7.

Aortic sclerosis
Thickened calcified cusps with preserved mobility
Typically associated with peak doppler velocity of less than 2.5 m/sec

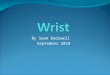
Rheumatic aortic stenosis
Characterized by Commissural fusionTriangular systolic orificethickening & calcification
Accompanied by rheumatic mitral valve changes.

Parasternal short axis view showing commissural fusion, leaflet thickening and calcification, small triangular systolic orifice
Rheumatic aortic stenosis

Subvalvular aortic stenosis(1) Thin discrete membrane consisting of
endocardial fold and fibrous tissue(2) A fibromuscular ridge (3) Diffuse tunnel-like narrowing of the LVOT(4) accessory or anomalous mitral valve tissue.

Supravalvular Aortic stenosis
Type I - Thick, fibrous ring above the aortic valve with less mobility and has the easily identifiable 'hourglass' appearance of the aorta.

Type II - Thin, discrete fibrous membranelocated above the aortic valve
The membrane usually mobile and may demonstrate doming during systole
Type III- Diffuse narrowing
Supravalvular Aortic stenosis

HOW TO ASSESS AORTIC STENOSIS

Doppler assessment of AS
The primary haemodynamic parameters recommended (EAE/ASE Recommendations for Clinical Practice 2008)
Peak transvalvular velocity
Mean transvalvular gradient
Valve area by continuity equation.

Peak transvalvular velocity
Continuous-wave Doppler ultrasound
Multiple acoustic windows Apical and suprasternal or right parasternal
most frequently yield the highest velocity rarely subcostal or supraclavicular windows
may be required
Three or more beats are averaged in sinus rhythm, with irregular rhythms at least 5 consecutive beats

AS jet velocity is defined as the highest velocity signal obtained from any window after a careful examination
Any deviation from a parallel intercept angle results in velocity underestimation
The degree of underestimation is 5% or less if the intercept angle is within 15⁰ of parallel.
‘Angle correction’ should not be used because it is likely to introduce more error given the unpredictable jet direction.
Peak transvalvular velocity

The velocity scale adjusted so the spectral doppler signal fills on the vertical axis, and with a time scale on the x-axis of 100 mm/s
Wall filters are set at a high level and gain is decreased to optimize identification of the velocity curve.
Grey scale is used
A smooth velocity curve with a dense outer edge and clear maximum velocity should be recorded
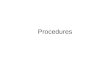
Peak transvalvular velocity

Peak transvalvular velocityThe shape of the CW Doppler velocity curve is helpful
in distinguishing the level and severity of obstruction.
With severe obstruction, maximum velocity occurs later in systole and the curve is more rounded in shape
With mild obstruction, the peak is in early systole with a triangular
shape of the velocity curve

The shape of the CWD velocity curve also can be helpful in determining whether the obstruction is fixed or dynamic
Dynamic sub aortic obstruction shows a characteristic late- peaking velocity curve, often with a concave upward curve in early systole
Peak transvalvular velocity

Mean transvalvular gradient
The difference in pressure between the left ventricle and aorta in systole
Gradients are calculated from velocity information
The relationship between peak and mean gradient depends on the shape of the velocity curve.

Bernoulli equations ΔP =4v²
The maximum gradient is calculated from maximum velocity
ΔP max =4v² max
The mean gradient is calculated by averaging the instantaneous gradients over the ejection period
Mean transvalvular gradient

The simplified Bernoulli equation assumes that the proximal velocity can be ignored
When the proximal velocity is over 1.5 m/s or the aortic velocity is ,3.0 m/s, the proximal velocity should be included in the Bernoulli equation ΔP max =4 (v² max- v2
proximal)
Mean transvalvular gradient

Sources of error for pressure gradient calculations
Malalignment of jet and ultrasound beam.Recording of MR jet

Neglect of an elevated proximal velocity.
Any underestimation of aortic velocity results in an even greater underestimation in gradients, due to the squared relationship between velocity and pressure difference
The accuracy of the Bernoulli equation to quantify AS pressure gradients is well established
Sources of error for pressure gradient calculations

The conversion of potential energy to kinetic energy across a narrowed valve results in a high velocity and a drop in pressure.
Distal to the orifice, flow decelerates again. Kinetic energy will be reconverted into potential energy with a corresponding increase in pressure, the so-called PR
Pressure recovery

Pressure recovery is greatest in stenosis with gradual distal widening
Aortic stenosis with its abrupt widening from the small orifice to the larger aorta has an unfavorable geometry for pressure recovery
PR= 4v²× 2EOA/AoA (1-EOA/AoA)
Pressure recovery

Comparing pressure gradients calculated fromdoppler velocities to pressures measured at
cardiac catheterization.

Comparing pressure gradients calculated fromdoppler velocities to pressures measured at
cardiac catheterization.
Currie PJ et al. Circulation 1985;71:1162-1169

Aortic valve areaContinuity equation

Continuity equation concept that the stroke volume ejected through the LV outflow tract all passes through the stenotic orifice
AVA= CSA LVOT×VTILVOT / VTIAV
Calculation of continuity-equation valve area requires three measurements
AS jet velocity by CWD LVOT diameter for calculation of a circular CSA LVOT velocity recorded with pulsed Doppler.
Aortic valve areaAortic valve area

LVOT diameter and velocity should be measured at the same distance from the aortic valve.
When the PW sample volume is optimally positioned, the recording shows a smooth velocity curve with a well-defined peak.
Aortic valve areaContinuity equation

The VTI is measured by tracing the dense modal velocity throughout systole
LVOT diameter is measured from the inner edge to inner edge of the septal endocardium, and the anterior mitral leaflet in mid-systole
Aortic valve areaContinuity equation

Well validated - clinical & experimental studies. Zoghbi WA et al. Circulation 1986;73:452-
9.
Oh JK et al. J Am Coll Cardiol 1988;11:1227-34.
Measures the effective valve area, the weight of the evidence now supports the concept that effective, not anatomic, orifice area is the primary predictor of clinical outcome.
Baumgartner et al. J Am Society Echo 2009; 22,1 , 1-23.
Aortic valve area-Continuity equationLevel of Evidence

Limitations of continuity-equation valve area
Intra- and interobserver variability AS jet and LVOT velocity 3 to4%. LVOT diameter 5% to 8%.
When sub aortic flow velocities are abnormal SV calculation at this site are not accurate
Sample volume placement near to septum or anterior mitral leaflet

Observed changes in valve area with changes in flow rate
AS and normal LV function, the effects of flow rate are minimal
This effect may be significant in presence concurrent LV dysfunction.
Limitations of continuity-equation valve area

Left ventricular systolic dysfunction
Low-flow low-gradient AS includes the following conditions:
Effective orifice area < 1.0 Cm2
LV ejection fraction < 40% Mean pressure gradient < 30–40 mmHg
Severe AS and severely reduced LVEF represent 5% of AS patients
Vahanian A et al. Eur Heart J 2007;28:230–68.

Provides information on the changes in aortic velocity, mean gradient, and valve area as flow rate increases.
Measure of the contractile response to dobutamine
Helpful to differentiate two clinical situationsSevere AS causing LV systolic dysfunctionModerate AS with another cause of LV dysfunction
Dobutamine stress Echo

A low dose starting at 2.5 or 5 ủg/kg/min with an incremental increase in the infusion every 3–5 min to a maximum dose of 10–20 ủg/kg/min
The infusion should be stopped as soon asPositive result is obtained Heart rate begins to rise more than 10–20 bpm
over baseline or exceeds 100bpm
Dobutamine stress Echo

Role in decision-making in adults with AS is controversial and the findings recommend as reliable are
Stress findings of severe stenosis AVA<1cm² Jet velocity>4m/s Mean gradient>40mm of Hg
Nishimura RA et al. Circulation 2002;106:809-13.
Lack of contractile reserve- Failure of LVEF to ↑ by 20% is a poor prognostic sign
Monin JL et al. Circulation 2003;108:319-24..
Dobutamine stress Echo

Serial measurements
During follow-up any significant changes in results should be checked in detail:
Make sure that aortic jet velocity is recorded from the same window with the same quality (always report the window where highest velocities can be recorded).
when AVA changes, look for changes in the different components incorporated in the equation.
LVOT size rarely changes over time in adults.

Alternate measures of stenosis severity
(Level 2 EAE/ASE Recommendations )

Based on the concept that in native aortic valve stenosis the shape of the velocity curve in the outflow tract and aorta is similar so that the ratio of LVOT to aortic jet VTI is nearly identical to the ratio of the LVOT to aortic jet maximum velocity.
AVA= CSA LVOT×VLVOT / VAV
This method is less well accepted because results are more variable than using VTIs in the equation.
Simplified continuity equation.

Another approach to reducing error related to LVOT diameter measurements is removing CSA from the simplified continuity equation.
This dimensionless velocity ratio expresses the size of the valvular effective area as a proportion of the CSA of the LVOT.
Velocity ratio= VLVOT/VAV
In the absence of valve stenosis, the velocity ratio approaches 1, with smaller numbers indicating more severe stenosis.
Velocity ratio

Aortic valve area -Planimetry
Planimetry may be an acceptable alternative when Doppler estimation of flow velocities is unreliable
Planimetry may be inaccurate when valve calcification causes shadows or reverberations limiting identification of the orifice
Doppler-derived mean-valve area correlated better with maximal anatomic area than with mean-anatomic area.
Marie Arsenault, et al. J. Am. Coll. Cardiol. 1998;32;1931-1937

Aortic valve area - Planimetry

Experimental descriptors of stenosis
severity
(Level 3 EAE/ASE Recommendations -not recommended for routine
clinical use)

Valve resistance
Relatively flow-independent measure of stenosis severity
Depends on the ratio of mean pressure gradient and mean flow rate
Resistance = (ΔPmean /Qmean) × 1333
There is a close relationship between aortic valve resistance and valve area
The advantage over continuity equation not established

Left ventricular stroke work loss
Left ventricle expends work during systole to keep the aortic valve open and to eject blood into the aorta
SWL(%) = (100×ΔPmean)/ ΔPmean+SBP
A cutoff value more than 25% effectively discriminated between patients experiencing a good and poor outcome.
Kristian Wachtell. Euro Heart J.Suppl. (2008) 10 ( E), E16–E22

Energy loss index Damien Garcia.et al. Circulation. 2000;101:765-771.
Fluid energy loss across stenotic aortic valves is influenced by factors other than the valve effective orifice area .
An experimental model was designed to measure EOA and energy loss in 2 fixed stenoses and 7 bioprosthetic valves for different flow rates and 2 different aortic sizes (25 and 38 mm).
EOA and energy loss is influenced by both flow rate and AA and that the energy loss is systematically higher (15±2%) in the large aorta.
Damien Garcia.et al. Circulation. 2000;101:765-771.

Energy loss coefficient (EOA × AA)/(AA - EOA) accurately
predicted the energy loss in all situations .
It is more closely related to the increase in left ventricular workload than EOA.
To account for varying flow rates, the coefficient was indexed for body surface area in a retrospective study of 138 patients with moderate or severe aortic stenosis.
The energy loss index measured by Doppler echocardiography was superior to the EOA in predicting the end points
An energy loss index #0.52 cm2/m2 was the best predictor of diverse outcomes (positive predictive value of 67%).
Energy loss index Damien Garcia.et al. Circulation. 2000;101:765-771.

Classification of AS severity (a ESC & bAHA/ACC Guidelines)
Aortic Sclerosis Mild Moderate Severe
Aortic jet velocity (m/s) ≤ 2.5 m/s 2.6 -2.9 3.0 - 4 > 4
Mean gradient (mm Hg) < 20b(<30a) 20 – 40b (30 -50a) > 40
AVA (cm²) > 1.5 1.0 - 1.5 < 1.0
Indexed AVA (cm²/m²) > 0.85 0.60 – 0.85 < 0.6
Velocity ratio > 0.50 0.25 – 0.50 < 0.25

Effects of concurrent conditions on assessmentof severity

Effect of concurrent conditions ……
Left ventricular systolic dysfunction
Left ventricular hypertrophySmall ventricular cavity & small LV ejects a
small SV so that, even in severe AS the AS velocity and mean gradient may be lower than expected.
Continuity-equation valve area is accurate in this situation

Hypertension35–45% of patients primarily affect flow and gradients but less AVA
measurements Control of blood pressure is recommendedThe echocardiographic report should always
include a blood pressure measurement
Effect of concurrent conditions contd…

Aortic regurgitation
About 80% of adults with AS also have aortic regurgitation
High transaortic volume flow rate, maximum velocity, and mean gradient will be higher than expected for a given valve area
In this situation, reporting accurate quantitative data for the severity of both stenosis and regurgitation
Effect of concurrent conditions contd…

Mitral valve disease
With severe MR, transaortic flow rate may be low resulting in a low gradient .Valve area calculations remain accurate in this setting
A high-velocity MR jet may be mistaken for the AS jet. Timing of the signal is the most reliable way to distinguish
Effect of concurrent conditions contd…

High cardiac outputRelatively high gradients in the presence of
mild or moderate AS The shape of the CWD spectrum with a very
early peak may help to quantify the severity correctly
Ascending aortaAortic root dilationCoarctation of aorta
Effect of concurrent conditions contd…

Maximal aortic cusp separation (MACS) Vertical distance between right CC and non CC
during systole
M Mode- Aortic Stenosis
Aortic valve area MACS Measurement Predictive value
Normal AVA >2Cm2 Normal MACS >15mm 100%
AVA>1.0 > 12mm 96%
AVA< 0.75 < 8mm 97%
Gray area 8-12 mm …..
DeMaria A N et al. Circulation.Suppl II. 58:232,1978

M Mode- Aortic Stenosis

Limitations Single dimension Asymmetrical AV involvement Calcification / thickness ↓ LV systolic function ↓ CO status
M Mode- Aortic Stenosis

Valve anatomy, etiology
Exclude other LVOTO
Stenosis severity – jet velocity
mean pressure gradient
AVA – continuity equation
LV – dimensions/hypertrophy/EF/diastolic fn
Aorta- aortic diameter/ assess COA
AR – quantification if more than mild
MR- mechanism & severity
Pulmonary pressure
Approach

ECHOCARDIOGRAPHIC ASSESSMENT OF AORTIC REGURGITATION

SEVERITY• 1. Regurgitant jet width/LVOT diameter ratio greater than or equal to 60
percent • 2. Vena contracta greater than 6 mm • 3. Regurgitant jet area/LVOT area ratio greater than or equal to 60
percent
• 4. Aortic regurgitation pressure half-time less than or equal to 250 ms • 5. Holodiastolic flow reversal in the descending thoracic or abdominal
aorta • 6. Regurgitant volume greater than or equal to 60 mL • 7. Regurgitant fraction greater than or equal to 50 percent • 8. Effective regurgitant orifice greater than or equal to 0.30cm2 • 9. Restrictive mitral flow pattern (usually in acute setting)

• Regurgitant jet height measured as maximal diameter of regurgitant jet just below AV,PLAX view
• LVOT diameter in end diastole

Regurgitant jet width/LVOT diameter ratio greater than or equal to 60 percent

Vena contracta greater than 6 mm

• Regurgitant jet area measured from PSAX view at level of LVOT
• LVOA measured at end diastole at same site• Ratio calculated



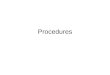
• Regurgitant doppler signal is a function of pressure gradient between aorta and LV
• Mild AR –small increase in LVEDP-gradual decline and flat deceleration slope
• Severe AR –LVEDP rises rapidly-rapid decline



• Suprasternal window-descending aortic flow profile
• Short period of low velocity flow reversal-normal
• Pan diastolic flow reversal with end diastolic velocity>20cm/s



Calculation of R.Volume and R.fraction
• SV=CSAxVTI• R.Volume=SV[lvot]-SV[mv]• RF=R.Volume/SV[lvot]• ERO=R.Volume/VTI[ARjet]• R.V>60ml,RF>50%,ERO>0.3cm² indicate severe
AR





MILD MODERATE
SEVERE
Jet width/LVOT diameter
<25% >/=65%
Vena contracta
<3mm >/=6mm
Jet area/LVOT area
<5% >60%
PHT >500 ms </= 250ms
Holodiastolic flow reversal
present

MILD MODERATE SEVERE
Reg vol < 30 ml >/= 60 ml
Reg fraction < 30 % >/= 50%
ERO < 0.1 cm2 >/= 0.3 cm2
Mitral inflow restriction
Present

Extent of jet

Signal intensity

ACUTE VS CHRONIC
• Shape of the envelope CW doppler• Rate of deceleration of flow• Premature mitral valve closure • Endocarditis,dissection• Normal lv dimensions


• LV chamber dimensions• LV systolic function• Aortic root dilatation


THANK YOU