Embed Size (px)
Citation preview
Manejo clínico del paciente con enfermedad mental y adicciones: El tratamiento de la comorbilidad.
Antoni Gual Unidad de Conductas Adic/vas ICN. Hospital Clínic. Barcelona
IDIBAPS. RTA [email protected]
Índice • Importancia de la comorbilidad • Abordaje motivacional del paciente dual • Tratamiento de la comorbilidad más
prevalente • Conclusiones
Importancia de la Patologia dual
• Tasas altas de comorbilidad • Peor pronóstico • Menor cumplimiento del tratamiento • Mayor tendencia al abandono del
tratamiento • Mayores tasas de suicidio • Menor soporte familiar y social
Estudios epidemiológicos en población general
• ECA • ESEMeD • NESARC
Metodología del ‘Epidemiological Catchment Area Study’ (ECA)
• Estudio de trastornos mentales, y por uso de alcohol y otras drogas. 20.291 habitantes.
• Instrumento: Diagnostic Interview Schedule (DIS) • Clínica psiquiátrica de los adictos sólo valorada en
ausencia de consumos • Regresión logística para controlar variables
confundidoras (edad, género, etnia, estado civil y estatus socioeconómico)
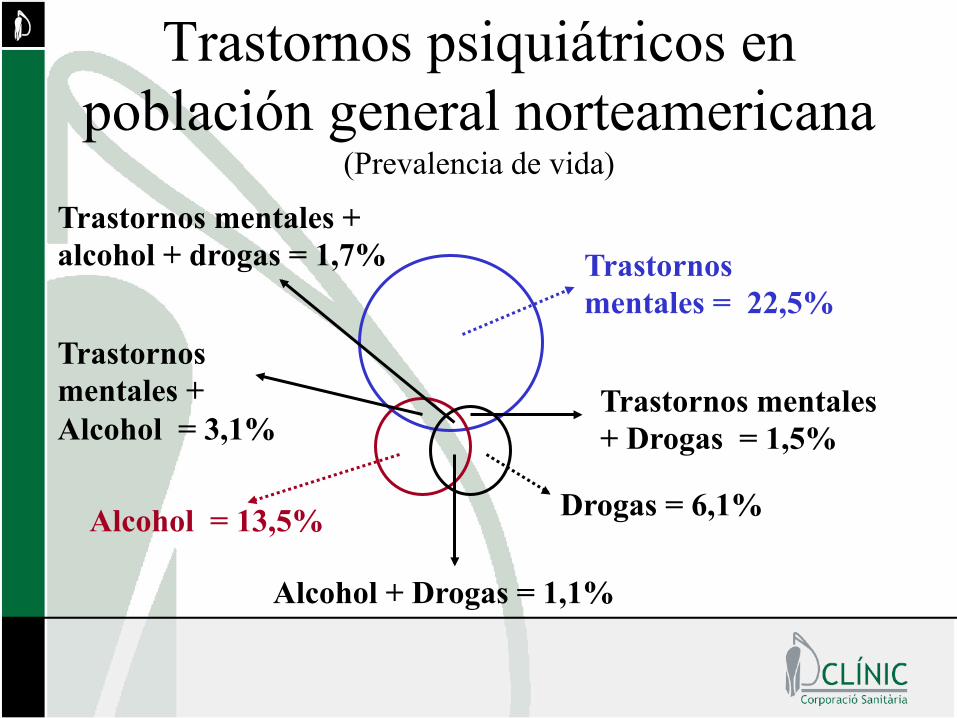
Trastornos psiquiátricos en población general norteamericana
(Prevalencia de vida)
Trastornos mentales = 22,5%
Trastornos mentales + alcohol + drogas = 1,7%
Alcohol = 13,5%
Alcohol + Drogas = 1,1%
Drogas = 6,1%
Trastornos mentales + Drogas = 1,5%
Trastornos mentales + Alcohol = 3,1%
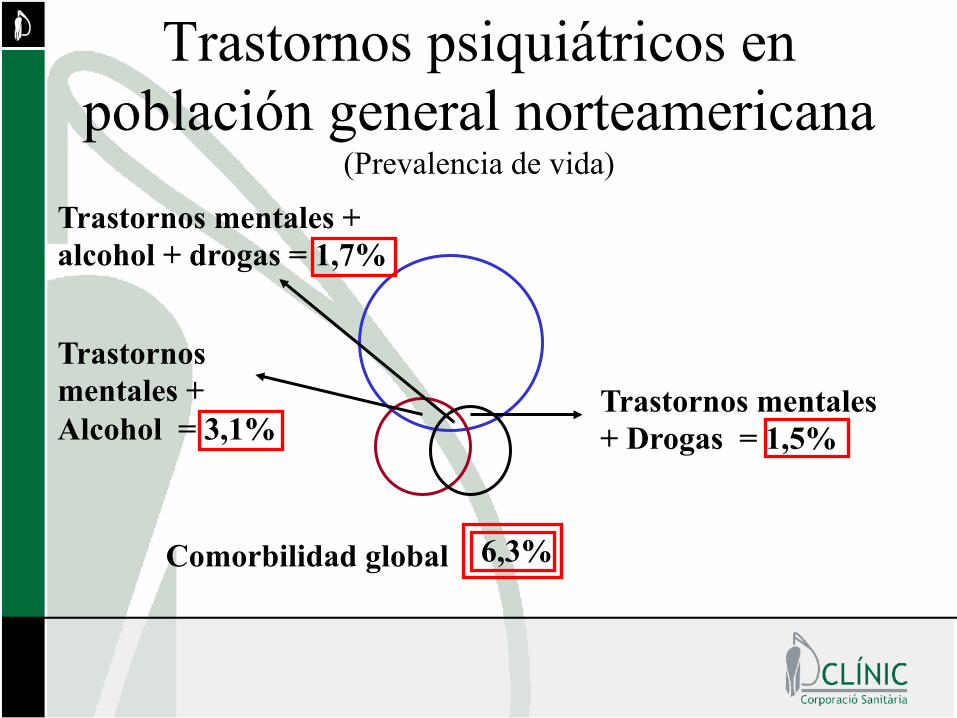
Trastornos psiquiátricos en población general norteamericana
(Prevalencia de vida)
Trastornos mentales + alcohol + drogas = 1,7%
Trastornos mentales + Drogas = 1,5%
Trastornos mentales + Alcohol = 3,1%
6,3% Comorbilidad global
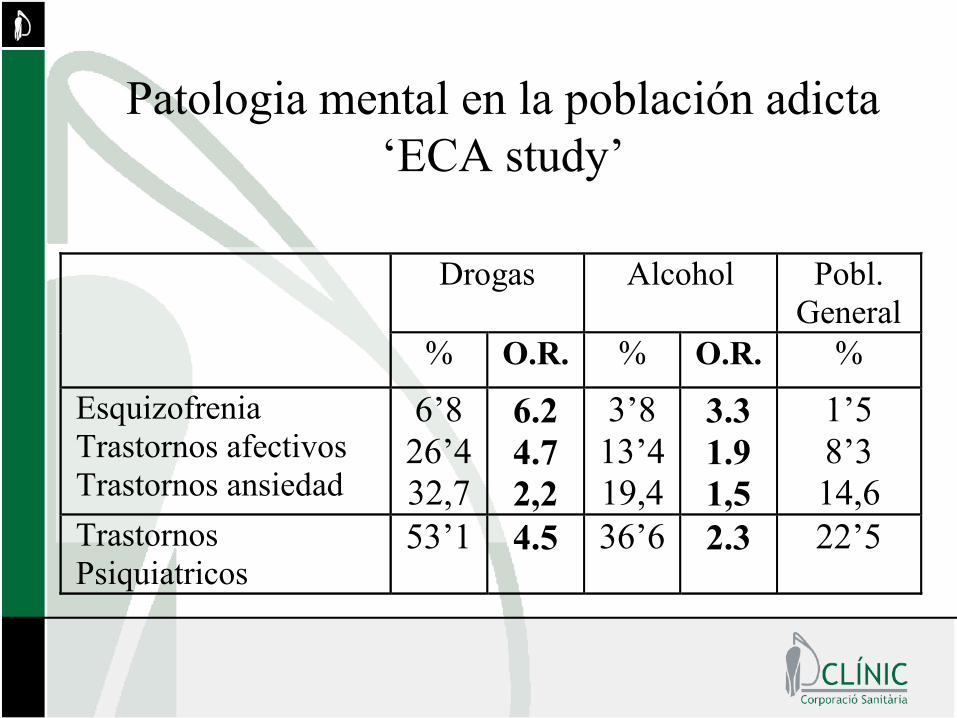
Patologia mental en la población adicta ‘ECA study’
Drogas Alcohol Pobl.
General
% O.R. % O.R. %
Esquizofrenia Trastornos afectivos Trastornos ansiedad
6’8 26’4 32,7
6.2 4.7 2,2
3’8 13’4 19,4
3.3 1.9 1,5
1’5 8’3 14,6
Trastornos Psiquiatricos
53’1 4.5 36’6 2.3 22’5
Estudio ESEMeD (European Study of the Epidemiology of Mental Disorders)
• Estudio de trastornos mentales, y por uso de alcohol y otras drogas. 21.425 habitantes.
• Alemania, Bélgica, España, Francia, Holanda e Italia
• Instrumento: Composite International Diagnostic Interview (WMH-CIDI)
• Se evalua prevalencia de vida y en los últimos 12 meses en población no institucionalizada
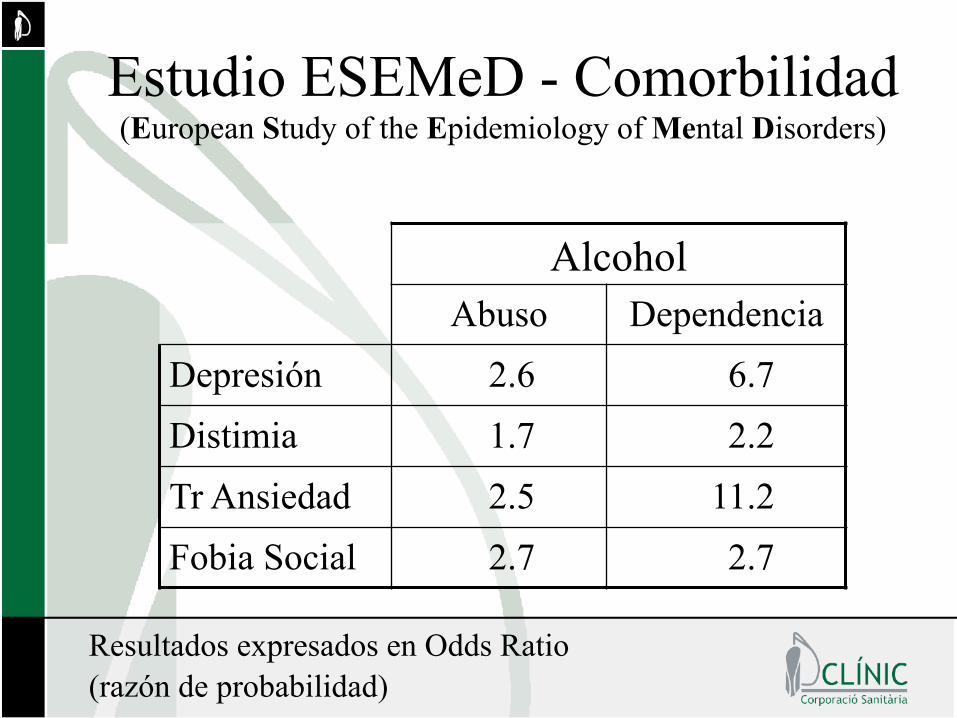
Estudio ESEMeD - Comorbilidad (European Study of the Epidemiology of Mental Disorders)
Alcohol Abuso Dependencia
Depresión 2.6 6.7 Distimia 1.7 2.2 Tr Ansiedad 2.5 11.2 Fobia Social 2.7 2.7
Resultados expresados en Odds Ratio (razón de probabilidad)
11
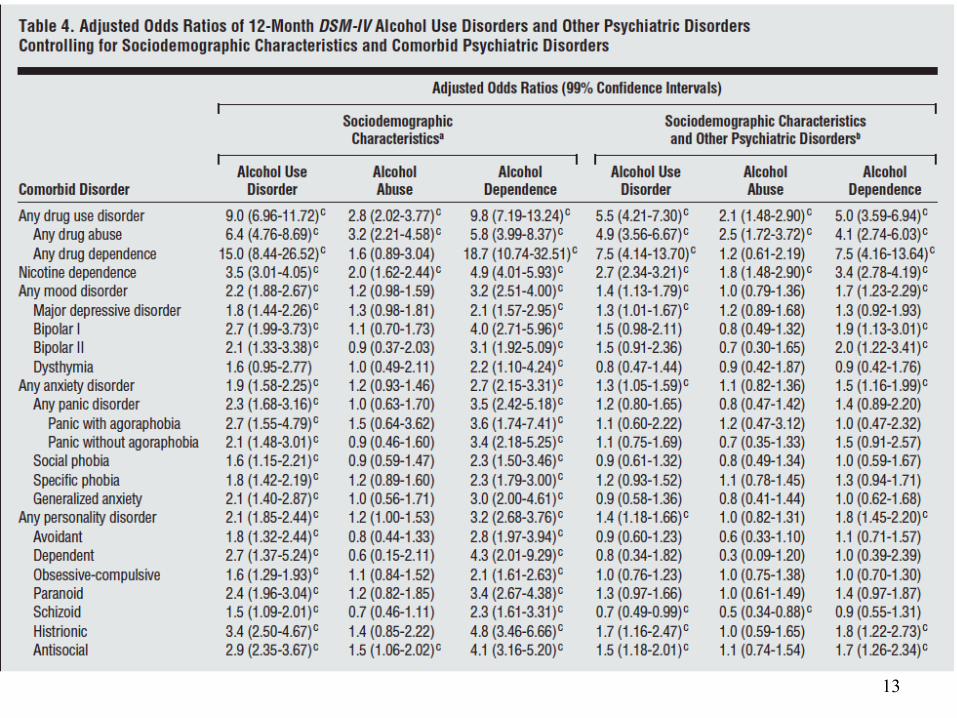
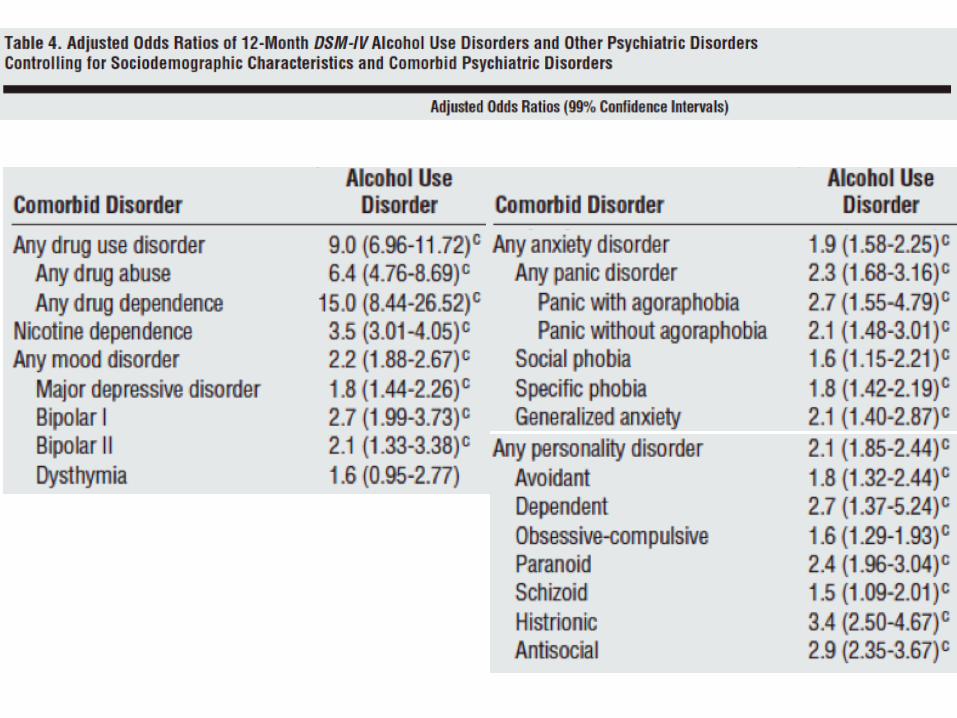
Estudio NESARC
Estudio NESARC
• Muestra representa/va nacional • Entrevistas cara a cara • Muestra entrevistada: 43093 personas, • Población mayor de 18 años • Ciudadanos no ins/tucionalizados residentes en USA
• 2001-‐2002
13

Resultados del estudio EDTA (Estado actual del Diagnóstico y
tratamiento de los Trastornos Adictivos en España)
Objetivos del estudio EDTA
Describir la situación actual de la patología dual en España y analizar la
carga asistencial y las características de dicha patología en función del ámbito
asistencial donde se atiende y de la formación especializada del profesional
que la atiende.
Método
• 427 médicos que atienden pacientes con conductas adictivas en el ámbito público aceptaron participar.
• Cada médico proporcionó de forma anónima información clínica sobre los primeros seis pacientes que atendió en un dia determinado.
Método (2)
• 2361 pacientes fueron entrevistados (92.1%)
• Se obtuvieron datos de las siguientes areas: – Área sociodemogáfica – Área Clínica – Diagnósticos – Tratamientos indicados
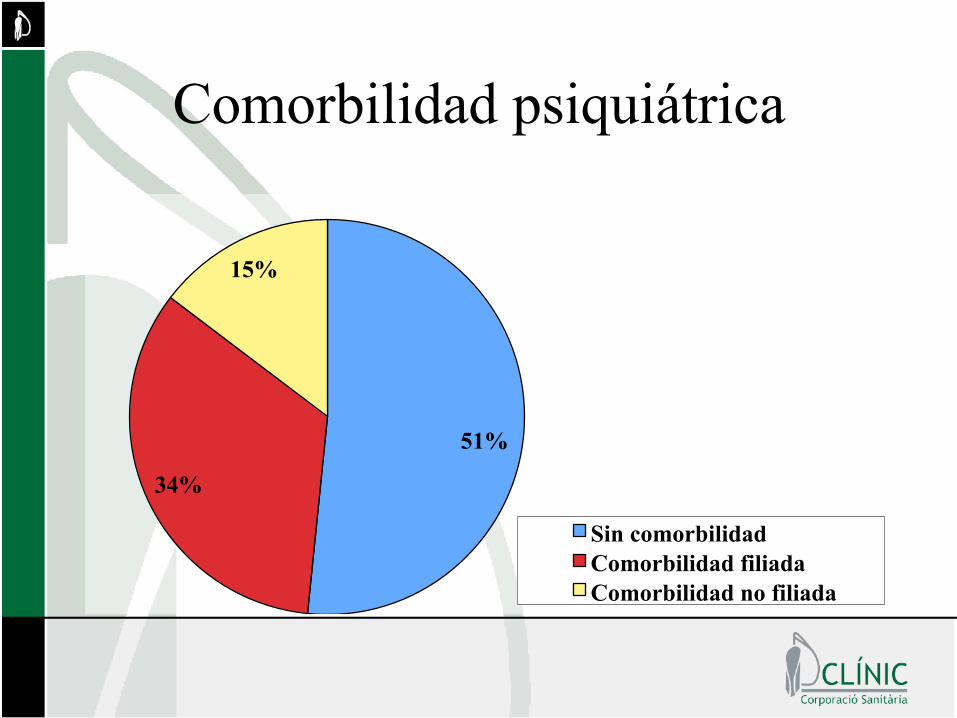
Comorbilidad psiquiátrica
51%
34%
15%
Sin comorbilidad Comorbilidad filiada Comorbilidad no filiada
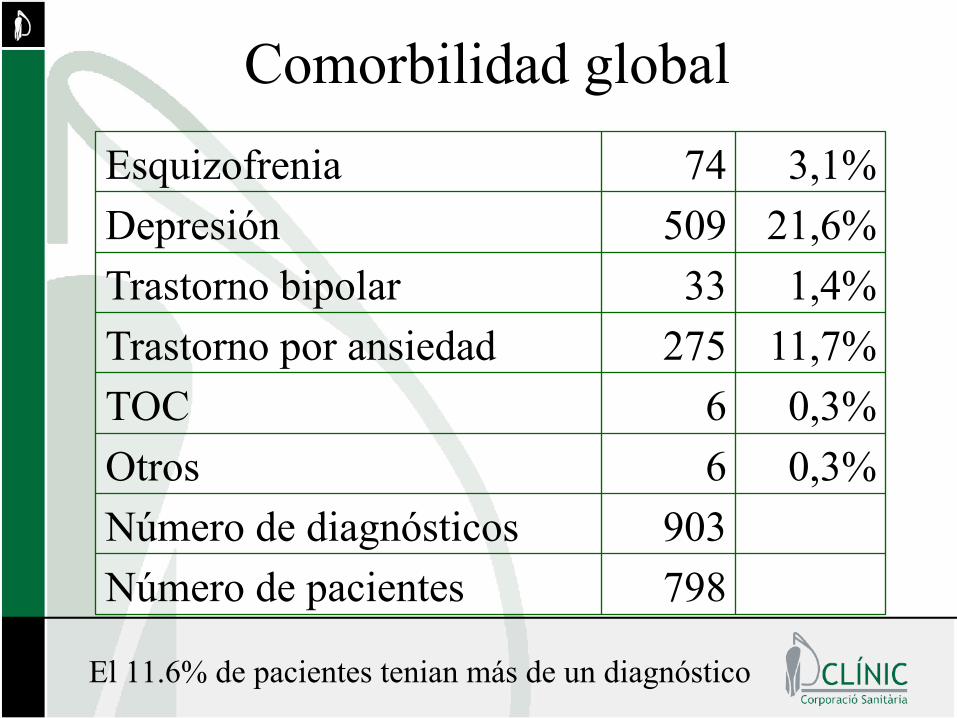
Comorbilidad global
798 Número de pacientes 903 Número de diagnósticos
0,3% 6 Otros 0,3% 6 TOC
11,7% 275 Trastorno por ansiedad 1,4% 33 Trastorno bipolar
21,6% 509 Depresión 3,1% 74 Esquizofrenia
El 11.6% de pacientes tenian más de un diagnóstico
Comorbilidad y edad
X (D)
• Con comorbilidad 40,5 (10,3)
• Sin comorbilidad 38,8 (10,5)
T-test; p<0,000
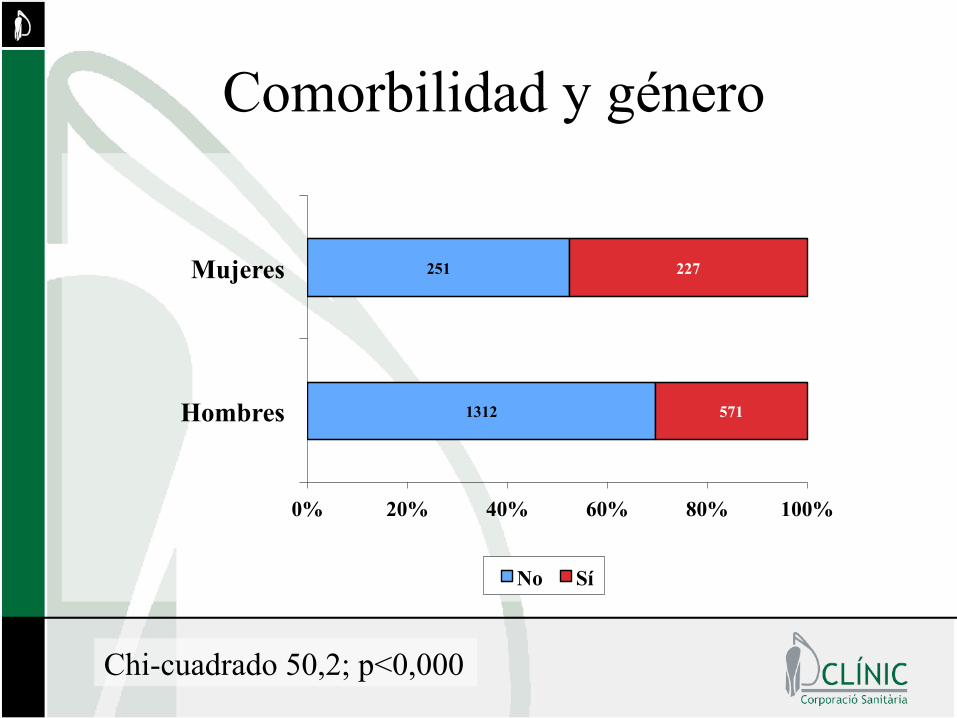
Comorbilidad y género
1312
251
571
227
0% 20% 40% 60% 80% 100%
Hombres
Mujeres
No Sí
Chi-cuadrado 50,2; p<0,000
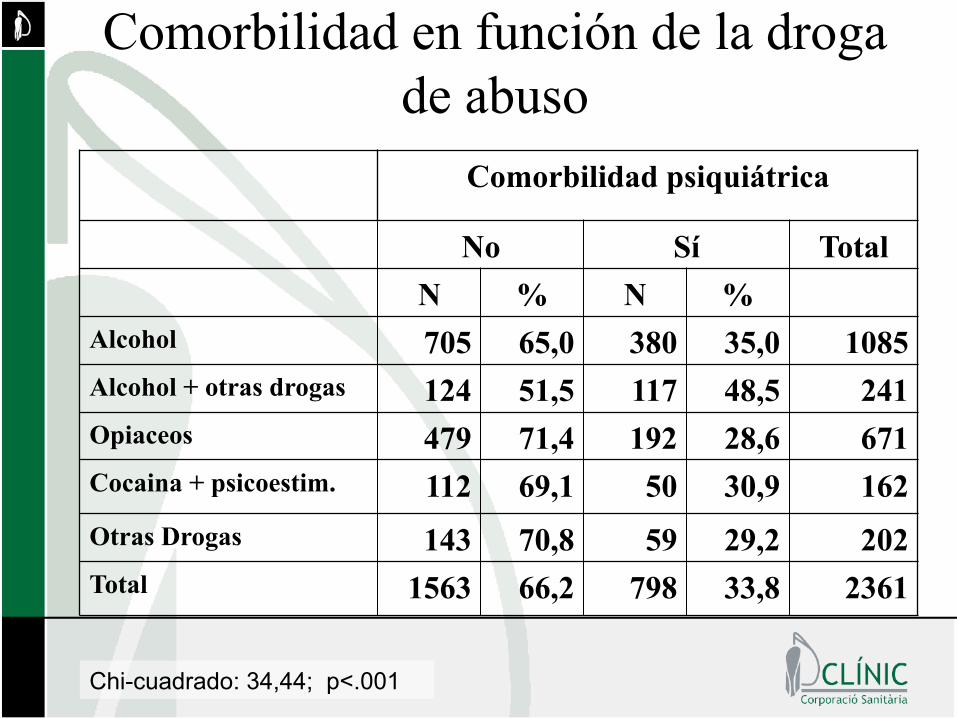
Comorbilidad en función de la droga de abuso
Comorbilidad psiquiátrica
No Sí Total N % N %
Alcohol 705 65,0 380 35,0 1085 Alcohol + otras drogas 124 51,5 117 48,5 241 Opiaceos 479 71,4 192 28,6 671 Cocaina + psicoestim. 112 69,1 50 30,9 162 Otras Drogas 143 70,8 59 29,2 202 Total 1563 66,2 798 33,8 2361
Chi-cuadrado: 34,44; p<.001
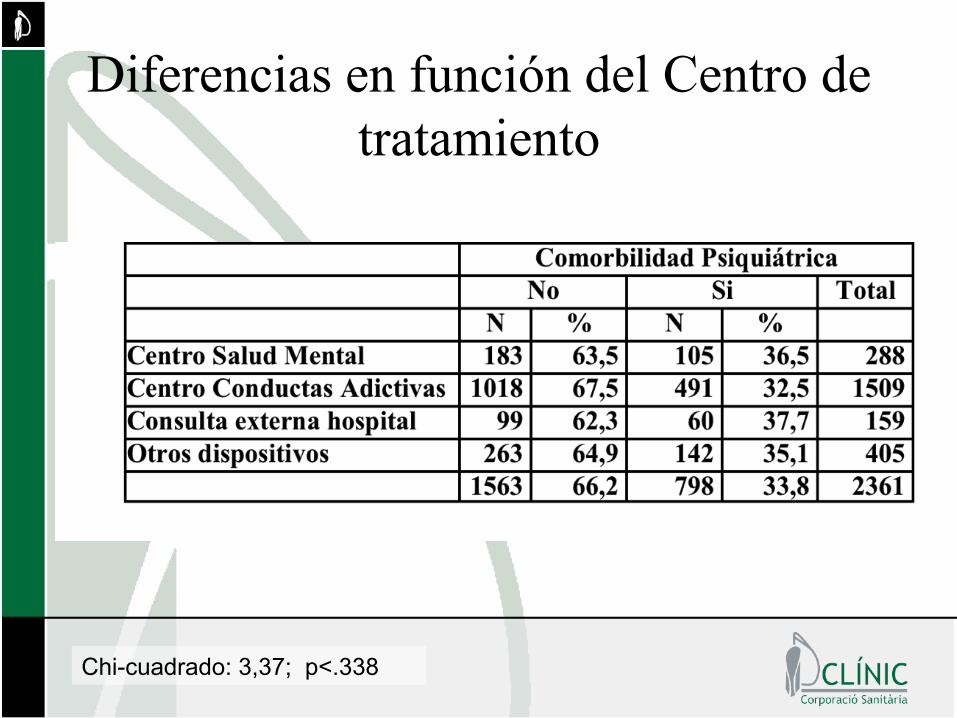
Diferencias en función del Centro de tratamiento
Chi-cuadrado: 3,37; p<.338
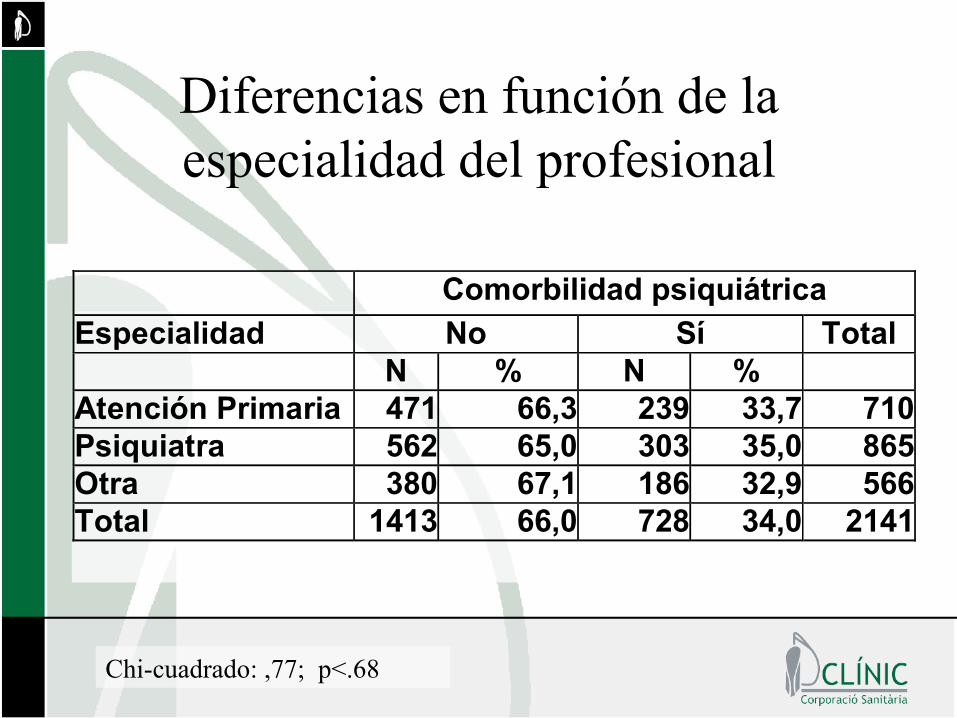
Diferencias en función de la especialidad del profesional
Chi-cuadrado: ,77; p<.68
Comorbilidad psiquiátrica Especialidad No Sí Total N % N % Atención Primaria 471 66,3 239 33,7 710 Psiquiatra 562 65,0 303 35,0 865 Otra 380 67,1 186 32,9 566 Total 1413 66,0 728 34,0 2141
Conclusiones • Trastornos afectivos y alcohol son la
principal asociación comórbida en pacientes duales
• Los factores que se asocian a la patología dual son: mujer, mayor edad, estar divorciado o viudo, estudios universitarios y policonsumos.
Índice • Importancia de la comorbilidad • Abordaje motivacional del paciente dual • Tratamiento de la comorbilidad más
prevalente • Conclusiones
MI is a higly recommended
component of a comprehensive
treatment approach for dually diagnosed
patients
Martino & Moyers, 2009
Rationale for using MI in DD patients
• Very severe population. Harm reduction strategies are accepted
• Classical confrontational style may be counterproductive and even exacerbate psychotic symptoms
• An MI style trying to elicit motivation for behaviour change and including harm reduction goals as first steps, is attractive.
• Mi is typically recommended as an evidence-based approach for DD patients (Bellack, 1999; Carey 1996; Drake 2001; Osher 1989)
Some modification of MI practice is necessary to address the complex needs of dually diagnosed patients
Martino & Moyers, 2009
Issues to be addressed in DD patients
• Need for integrated treatment • Cognitive impairment • Positive psychotic symptoms • Negative psychotic symptoms • Acute situations requiring intervention
Treating comorbidity (Dual Diagnosis)
Three proposed strategies: • Sequential • In parallel • Integrated

Adressing multiple behaviour targets
• Attend to motivation for using drugs and its interaction with psychiatric comorbidity – Use open ended questions to elicit concerns on
those interactions • Target medication and treatment adherence
– Use feedback and decisional balance to discuss pros & cons of adherence
– Pay attention to side effects of medication
When does MI stop being appropriate?
• Patients who have become motivated for changing • Acute psychiatric exacerbations • No clear limit on psychotic functioning allows us
to stablish when MI can be used • The response of the patient to an MI intervention
is key: does he respond with increased symptoms or does he become more organized?
What does research teach us?
• Three different applications of MI in DD patients:
1. Referral engagement 2. Standard treatment suplement 3. Stand-alone intervention
Abstinencia al año
• Design Randomized trial • Population Schizophrenia or schizoaffective
+ substance use disorder • Nation US • N 36 adults (marijuana) • MI 5 sessions + 24 CBT sessions • Comparison 24 CBT sessions • Follow-up 1 year
Barrowclough et al, 2001; American Journal of Psychiatry, 158:1706-1713
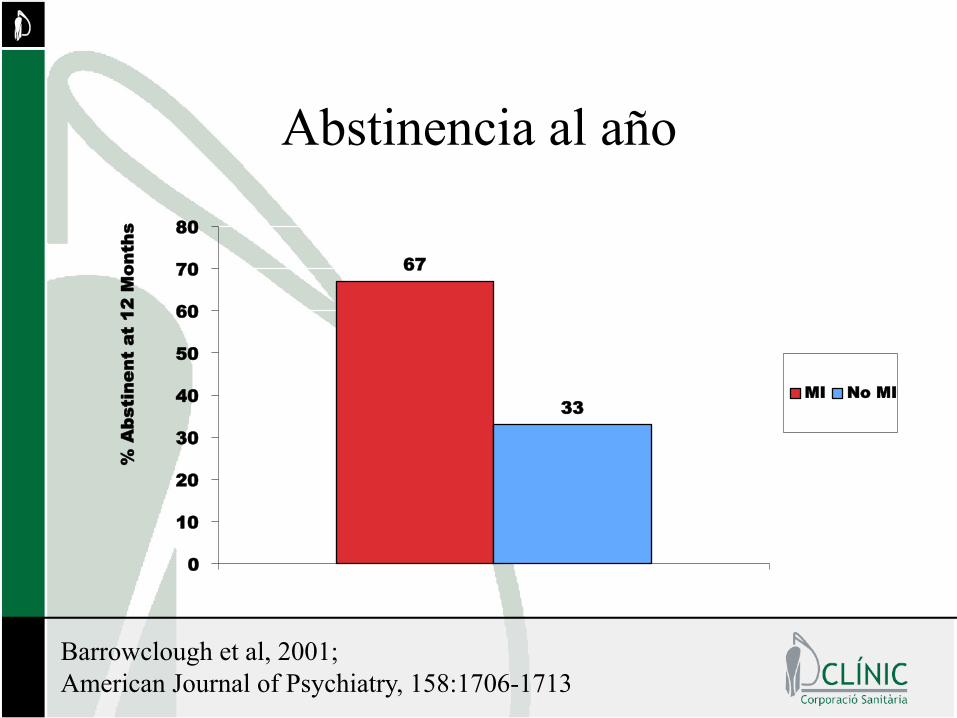
67
33
0
10
20
30
40
50
60
70
80
% A
bsti
nent
at
12 M
onth
s
MI No MI
Barrowclough et al, 2001; American Journal of Psychiatry, 158:1706-1713
Abstinencia al año
Cumplimiento y reingresos
• Design Consecutive assignment • Population Discharge from treatment • Nation US (Pittsburgh, PA) • N 23 adults (cocaine+depression) • MI 5 individual + 4 group sessions • Comparison TAU • Follow-up 1 year
Daley et al, 1998; American Journal of Psychiatry, 155:1611-1613
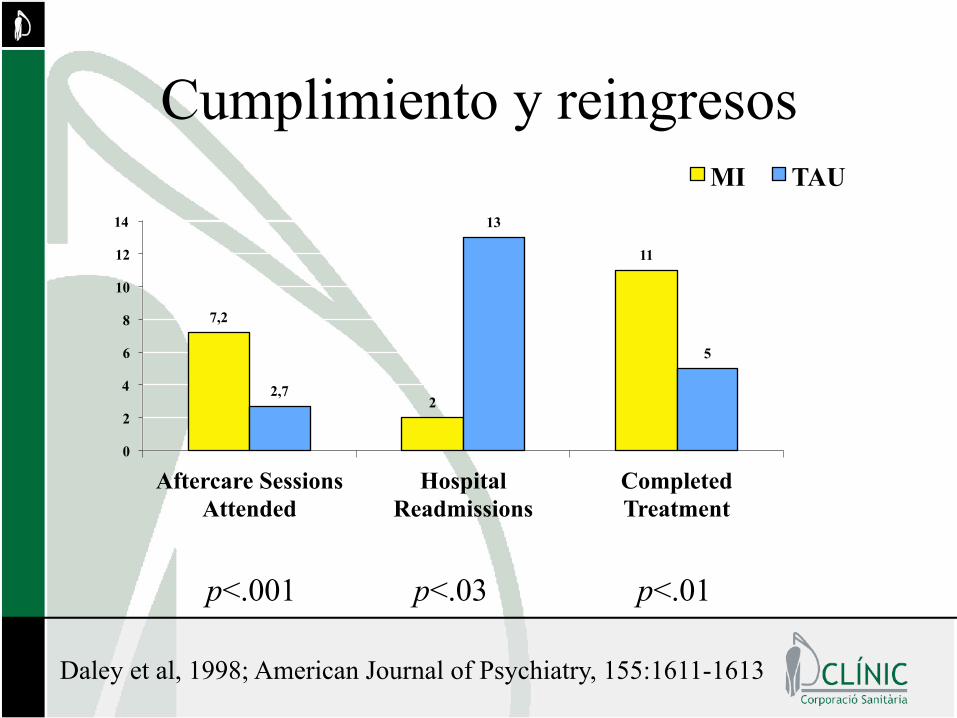
7,2
2
11
2,7
13
5
0
2
4
6
8
10
12
14
Aftercare Sessions Attended
Hospital Readmissions
Completed Treatment
MI TAU
p<.001 p<.03 p<.01
Cumplimiento y reingresos
Daley et al, 1998; American Journal of Psychiatry, 155:1611-1613
Daley & Zuckoff, 1998; Social Work, 43:470-473
• Design Consecutive cohorts • Population Dual diagnosis inpatients • Nation US (Pittsburgh, PA) • MI 1 pre-discharge session • Comparison TAU (no MI) • Follow-up Proximal
Asistencia a la primera visita post-alta
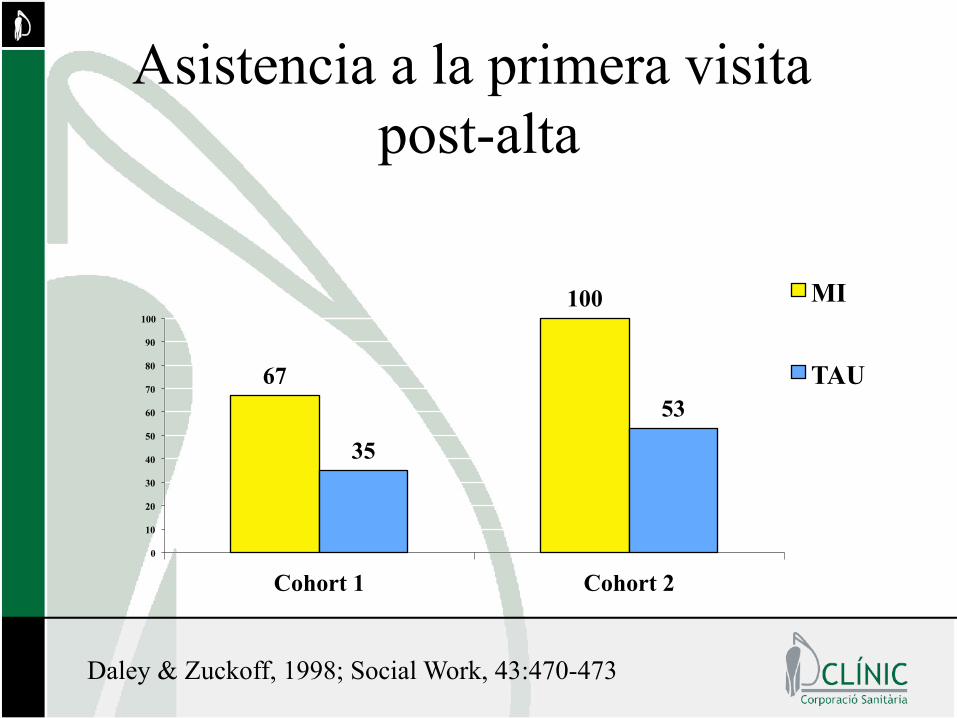
Asistencia a la primera visita post-alta
67
100
35
53
0
10
20
30
40
50
60
70
80
90
100
Cohort 1 Cohort 2
MI
TAU
Daley & Zuckoff, 1998; Social Work, 43:470-473
Martino et al., 2000; American Journal on Addictions, 9:88-91
• Design Randomized clinical trial • Population Partial hospital program • Nation US (New Haven, CT) • N 23 dual diagnosis patients • MI 1 session (45-60 min) • Comparison TAU • Follow-up End of treatment (12 wk)
Asistencia al Hospital de dia
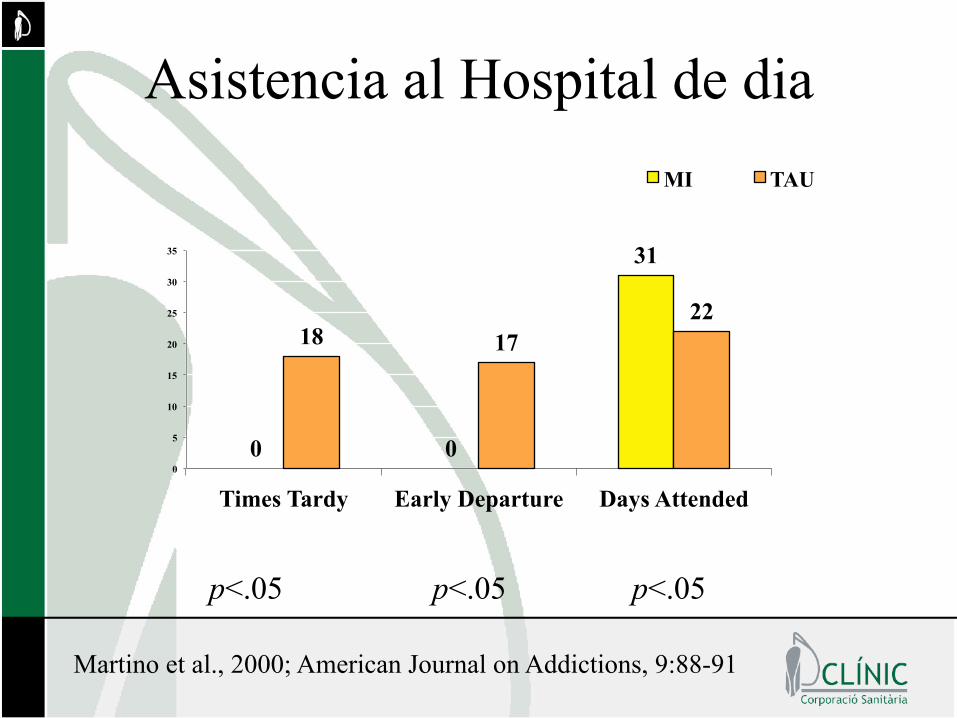
Asistencia al Hospital de dia
0 0
31
18 17 22
0
5
10
15
20
25
30
35
Times Tardy Early Departure Days Attended
MI TAU
p<.05 p<.05 p<.05
Martino et al., 2000; American Journal on Addictions, 9:88-91
Índice • Importancia de la comorbilidad • Abordaje mo/vacional del paciente dual • Tratamiento de la comorbilidad más prevalente
• Conclusiones

¿Cual es la comorbilidad más prevalente?
• La comorbilidad médica • La comorbilidad psiquiátrica
– Tabaco, adicciones y psiquiatría – Alcohol, ansiedad y depresión – Adicción y suicidio – Trastornos de personalidad y adicción
45
¿Cual es la comorbilidad más prevalente?
• La comorbilidad médica • La comorbilidad psiquiátrica
– Tabaco, adicciones y psiquiatría – Alcohol, ansiedad y depresión – Adicción y suicidio – Trastornos de personalidad y adicción
46
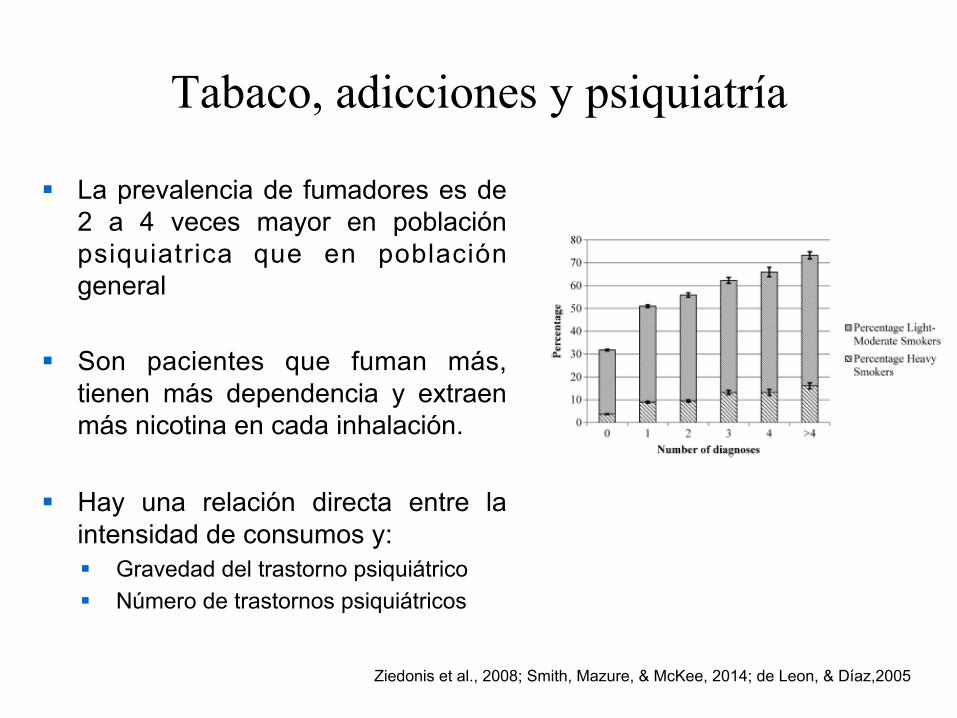
Tabaco, adicciones y psiquiatría
§ La prevalencia de fumadores es de 2 a 4 veces mayor en población psiquiatrica que en población general
§ Son pacientes que fuman más, tienen más dependencia y extraen más nicotina en cada inhalación.
§ Hay una relación directa entre la intensidad de consumos y: § Gravedad del trastorno psiquiátrico § Número de trastornos psiquiátricos
Ziedonis et al., 2008; Smith, Mazure, & McKee, 2014; de Leon, & Díaz,2005
Tabaco, adicciones y psiquiatría
• Una parte importante de pacientes psiquiátricos desean dejar de fumar
• Son pacientes más graves que precisan tratamientos más intensivos
• La clínica depresiva hace más diZcil la cesación, pero los antecedentes depresivos no son relevantes
• Los alcohólicos pueden dejar de fumar y beber simultáneamente
¿Cual es la comorbilidad más prevalente?
• La comorbilidad médica • La comorbilidad psiquiátrica
– Tabaco, adicciones y psiquiatría – Alcohol, ansiedad y depresión – Adicción y suicidio – Trastornos de personalidad y adicción
49
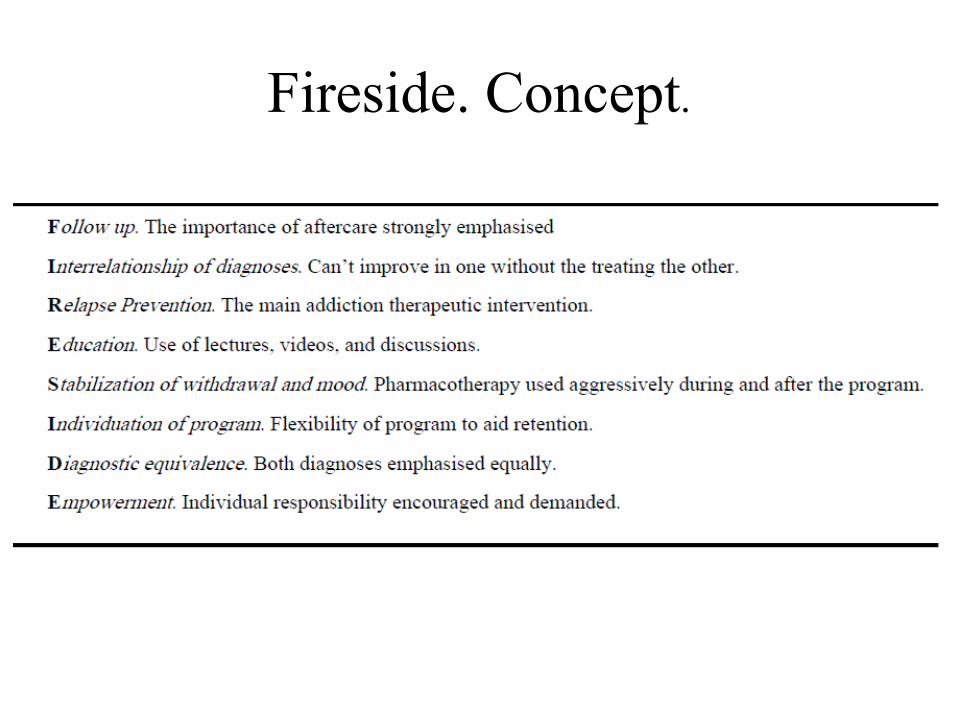
Fireside. Concept.
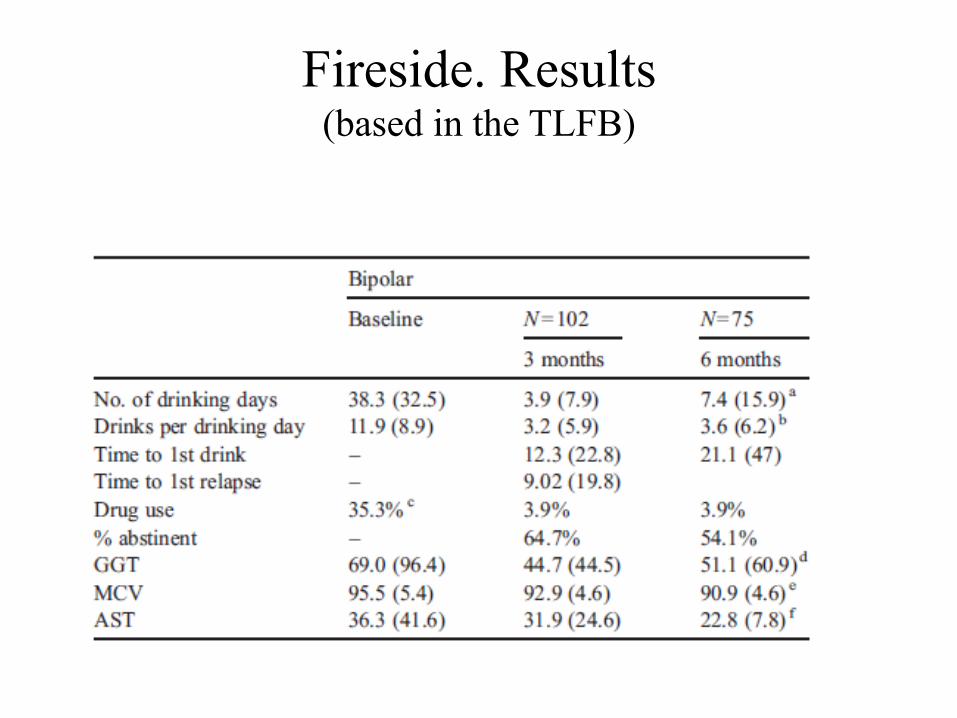
Fireside. Results (based in the TLFB)
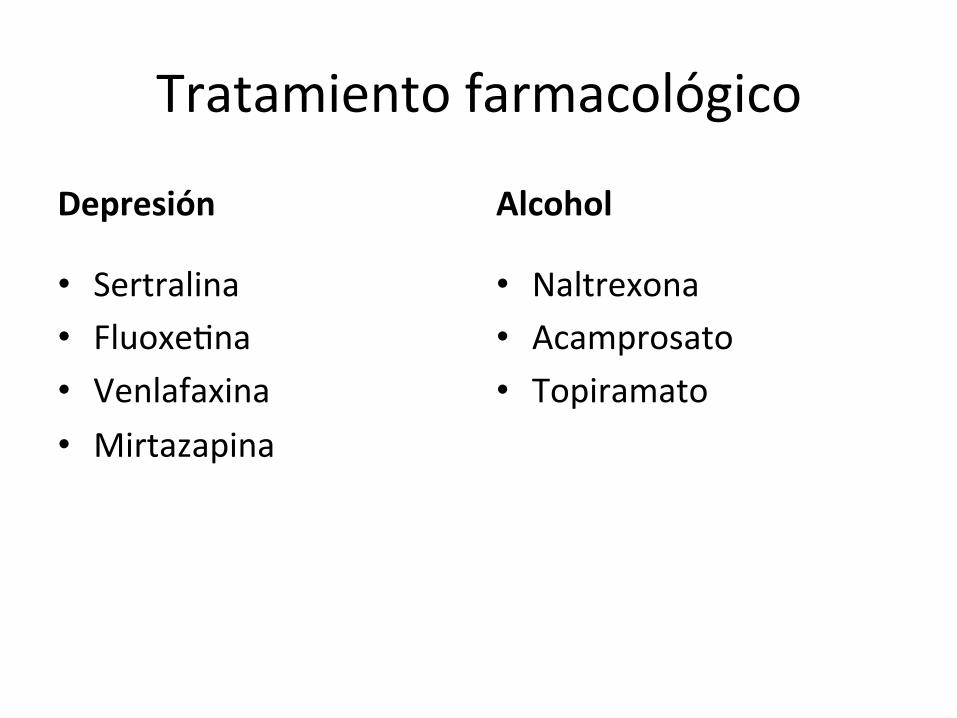
Tratamiento farmacológico
Depresión
• Sertralina • Fluoxe/na • Venlafaxina • Mirtazapina
Alcohol
• Naltrexona • Acamprosato • Topiramato
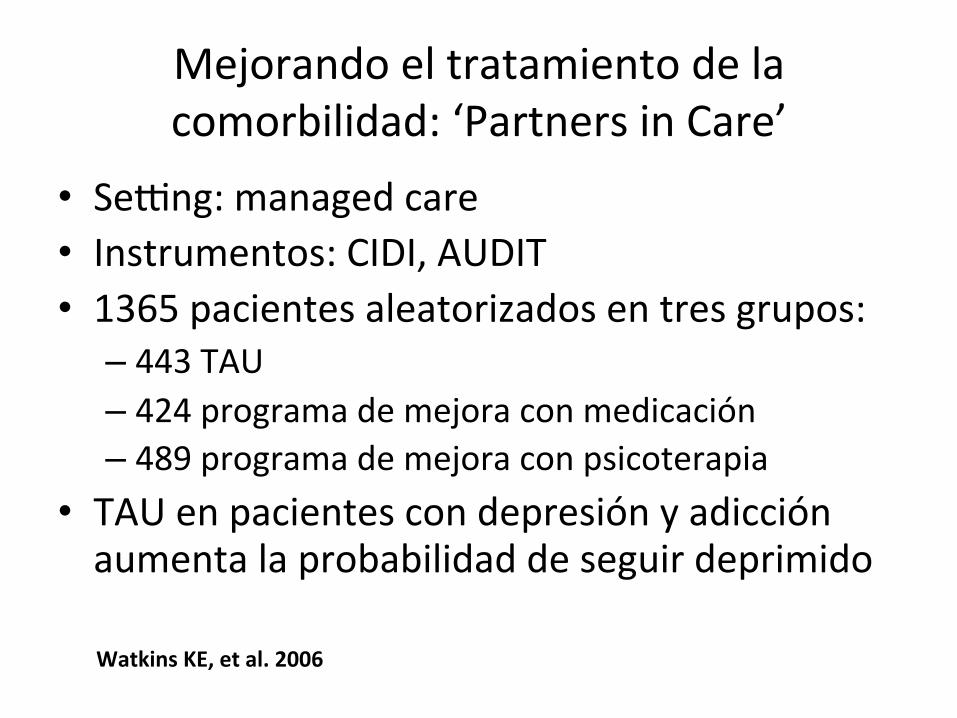
Mejorando el tratamiento de la comorbilidad: ‘Partners in Care’
• Se`ng: managed care • Instrumentos: CIDI, AUDIT • 1365 pacientes aleatorizados en tres grupos:
– 443 TAU – 424 programa de mejora con medicación – 489 programa de mejora con psicoterapia
• TAU en pacientes con depresión y adicción aumenta la probabilidad de seguir deprimido
Watkins KE, et al. 2006
‘Partners in Care’. Caracterís/cas del programa de mejora
• Compromiso ins/tucional (financiacion de recursos) • Equipo supervisor local de la cualidad de las intervenciones
• Formación específica de los profesionales • Enfermeras de soporte especializadas • Materiales orienta/vos • Acceso a enfermera para mo/var en la toma de la medicación
• Acceso a psicoterapia breve focal (4 sesiones)
Watkins KE, et al. 2006
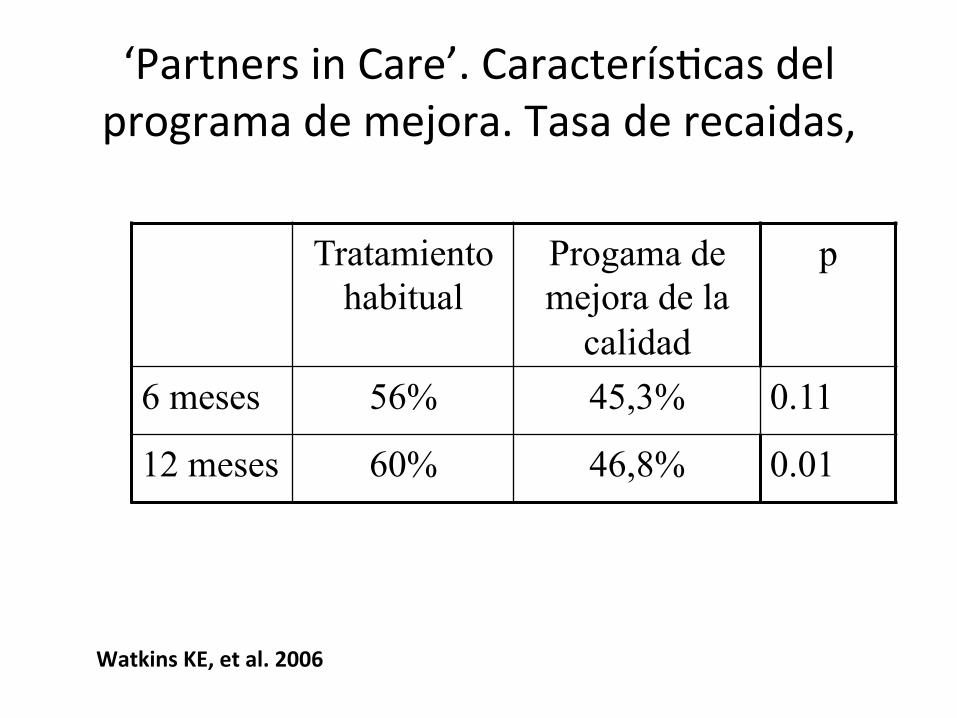
‘Partners in Care’. Caracterís/cas del programa de mejora. Tasa de recaidas,
Watkins KE, et al. 2006
Tratamiento habitual
Progama de mejora de la
calidad
p
6 meses 56% 45,3% 0.11
12 meses 60% 46,8% 0.01
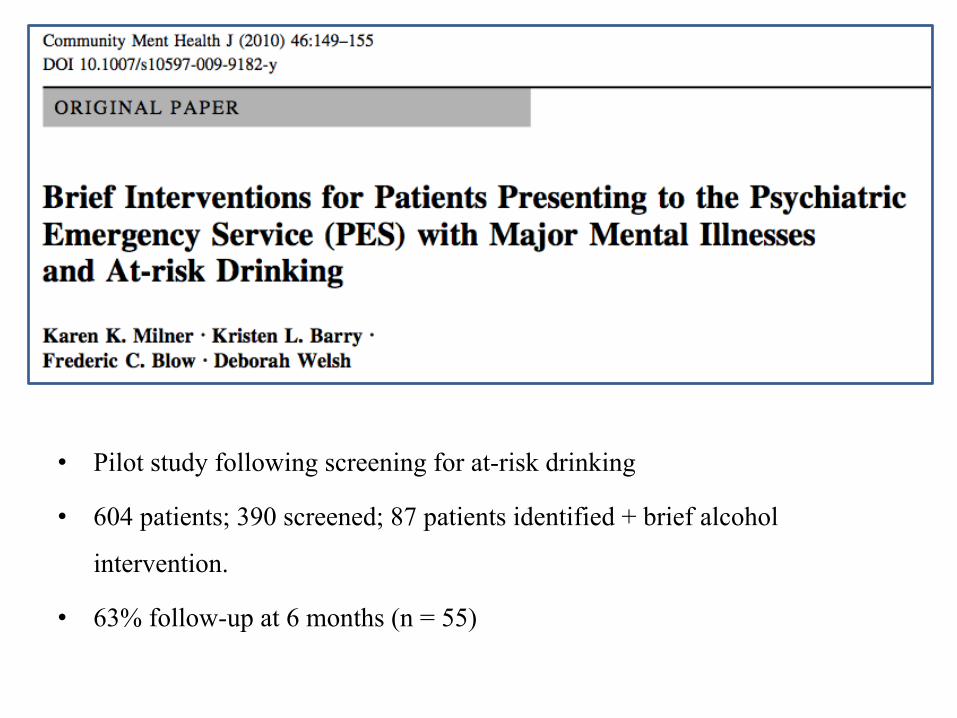
• Pilot study following screening for at-risk drinking
• 604 patients; 390 screened; 87 patients identified + brief alcohol
intervention.
• 63% follow-up at 6 months (n = 55)
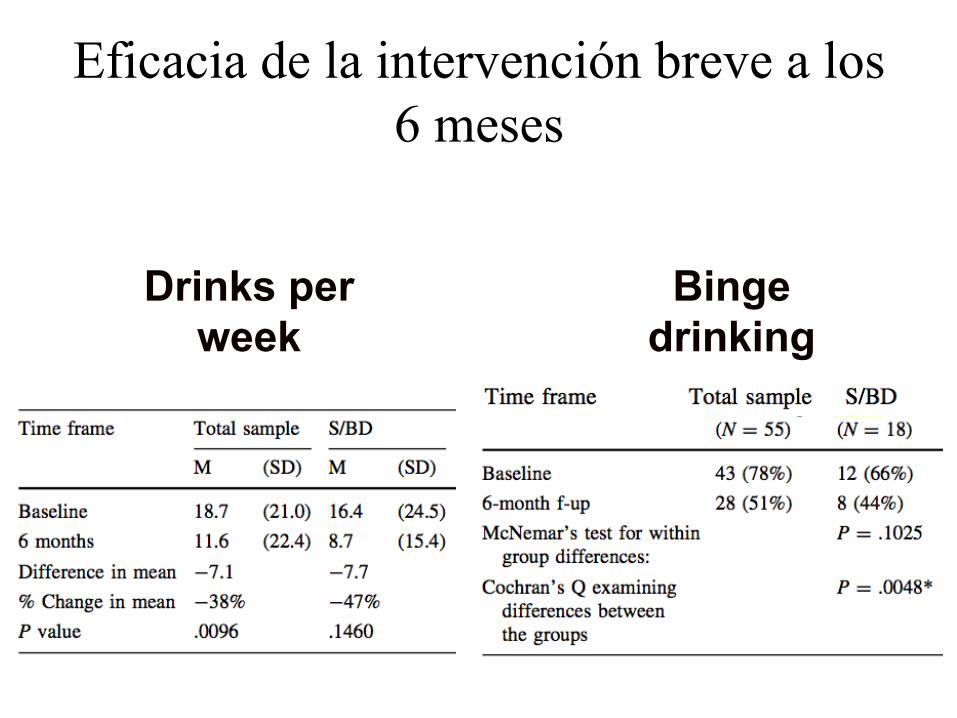
Eficacia de la intervención breve a los 6 meses
Drinks per week
Binge drinking
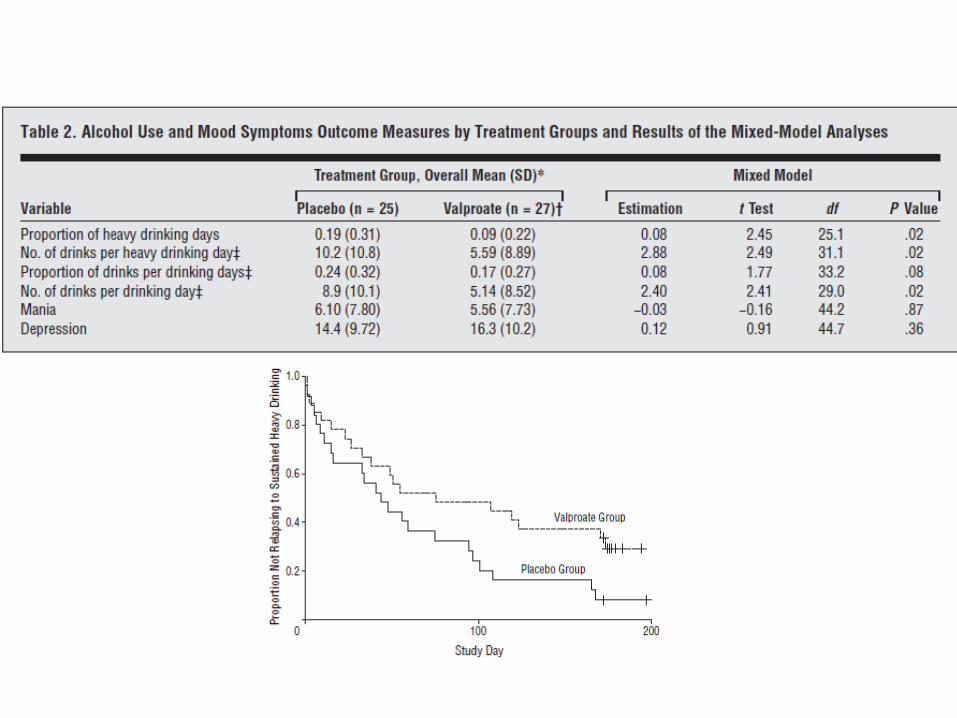
59 patients with BD and AUD in treatment with lithium
carbonate and psychosocial interventions were
randomized into two groups; placebo and valproate
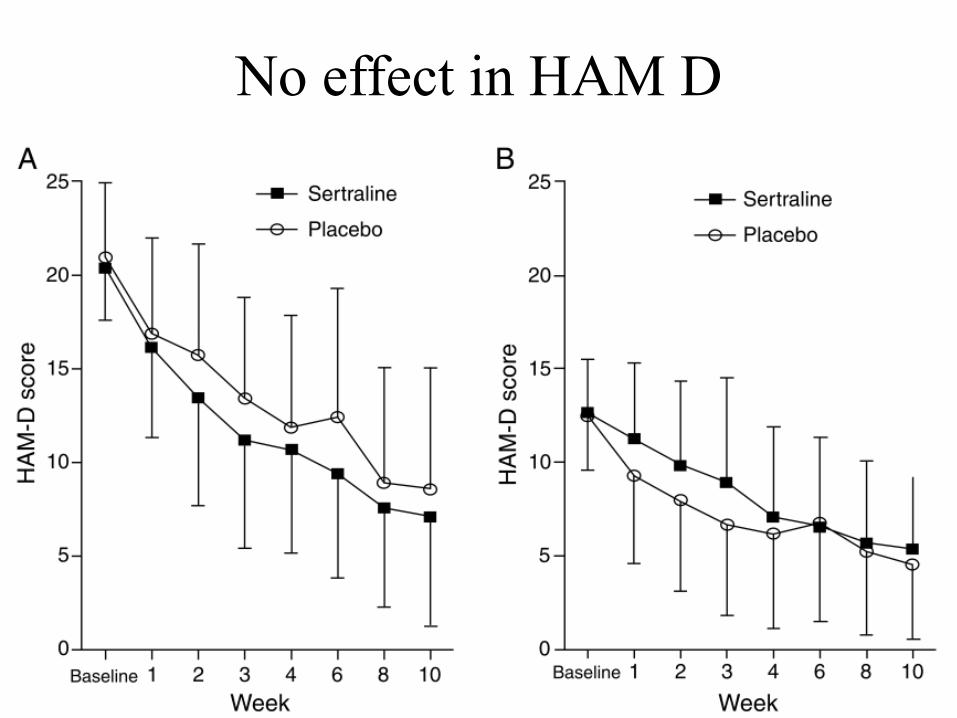
No effect in HAM D
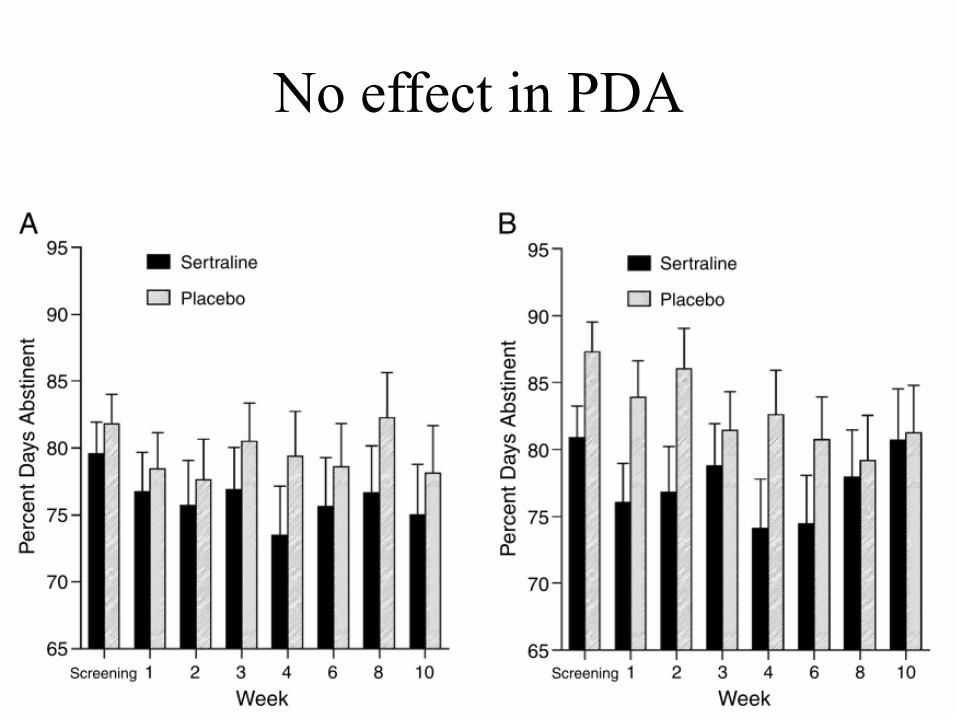
No effect in PDA
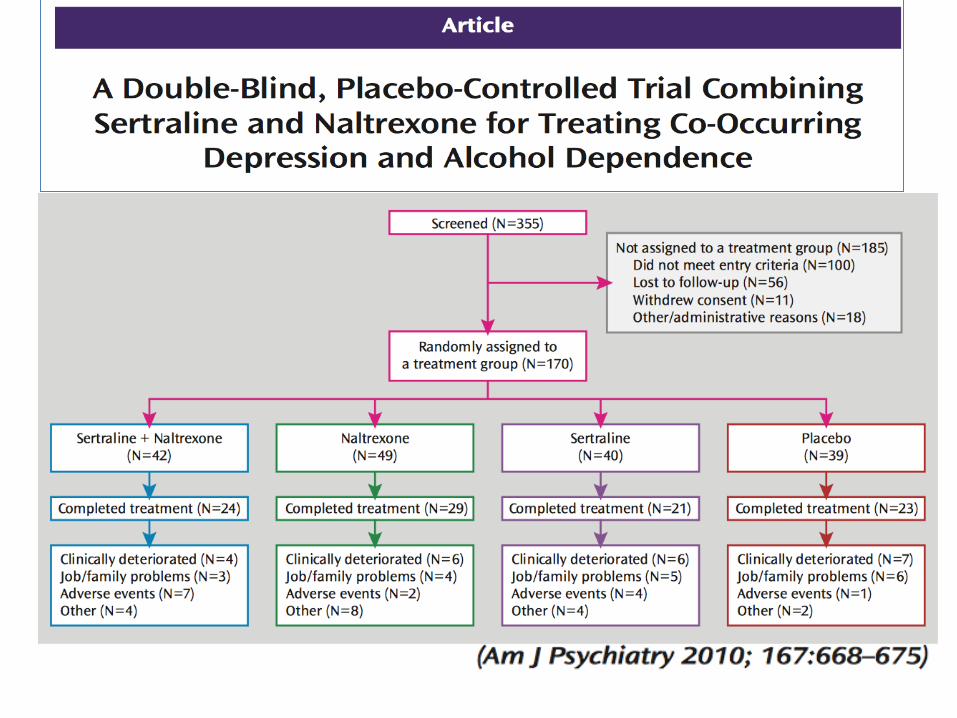
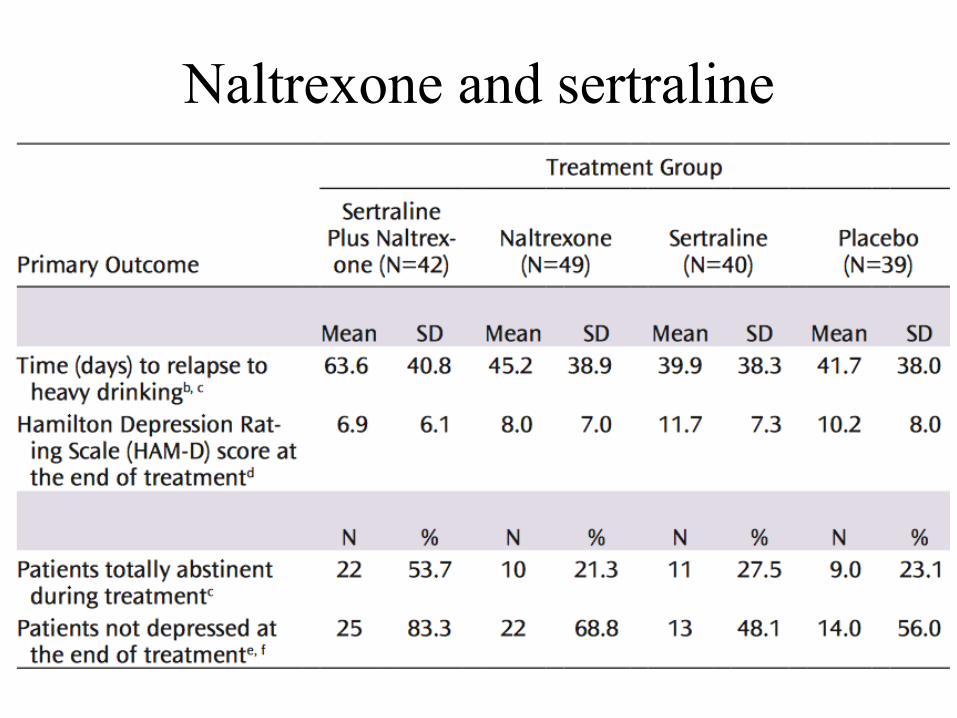
Naltrexone and sertraline
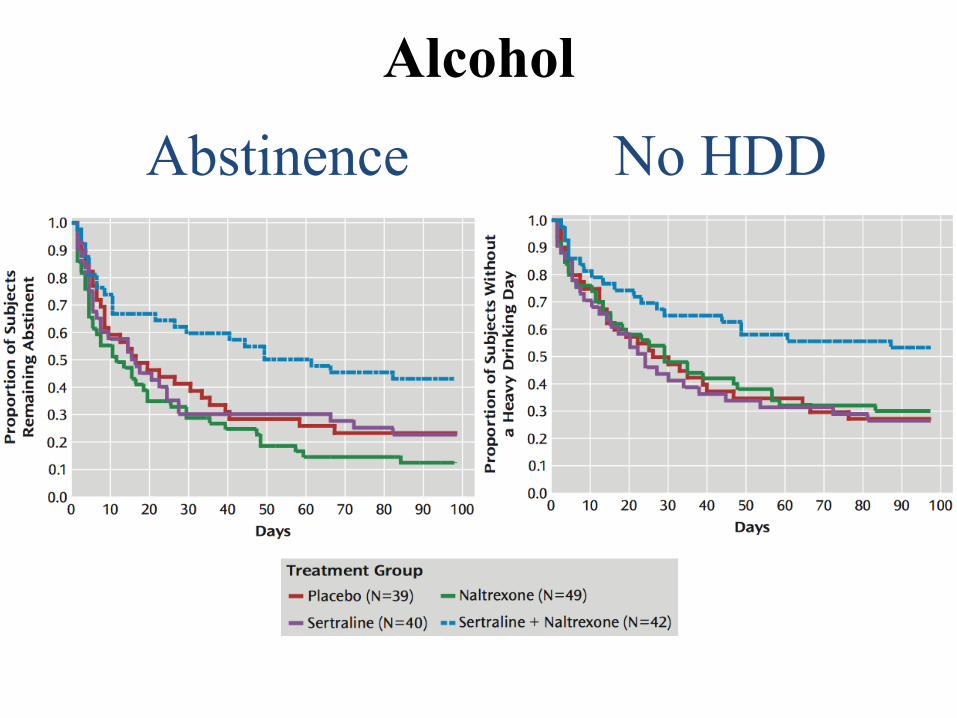
Alcohol
Abstinence No HDD
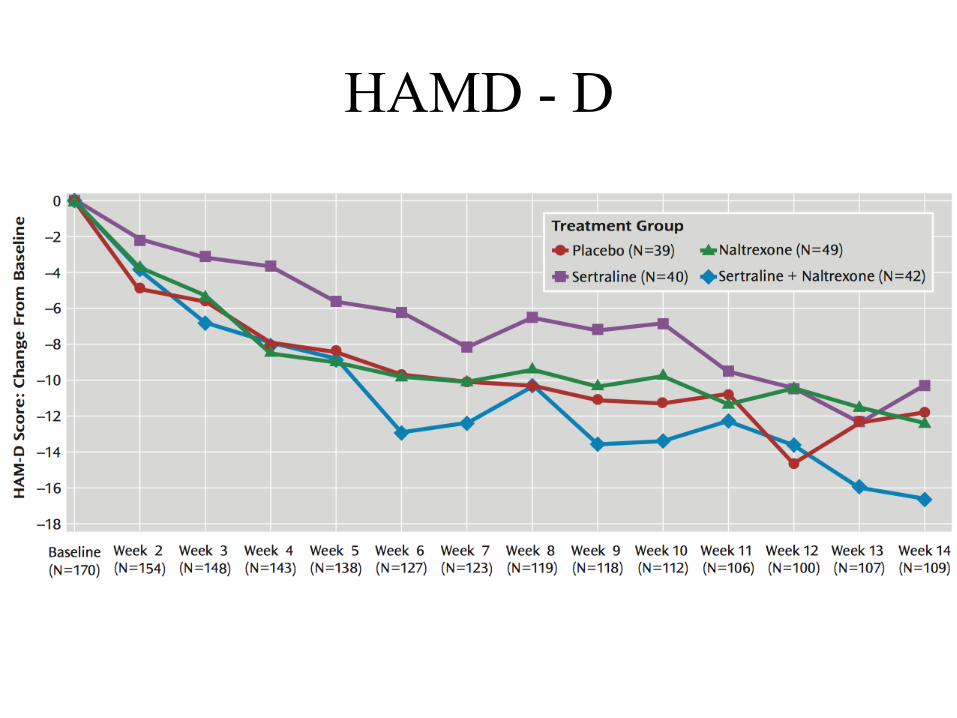
HAMD - D
Depression & Alcohol (Pettinati et al. 2013)
• A review of 8 RCTs of antidepressants (and counseling) for patients with a depressive disorder and alcohol dependence reported that 75% of the studies found a relationship between the medication and reductions in depressive symptoms and only 3 of the 8 studies (38%) found a reduction in drinking.
• Combining ATD with anticraving medication yields to better results.
• In the next future genetic factors that may affect medication treatment response will need to be taken into account.
¿Cual es la comorbilidad más prevalente?
• La comorbilidad médica • La comorbilidad psiquiátrica
– Tabaco, adicciones y psiquiatría – Alcohol, ansiedad y depresión – Adicción y suicidio – Trastornos de personalidad y adicción
75
76
Conceptual framework
Bagge CL, Sher KJ. Clinical Psychology Review 28 (2008) 1283–1296
77
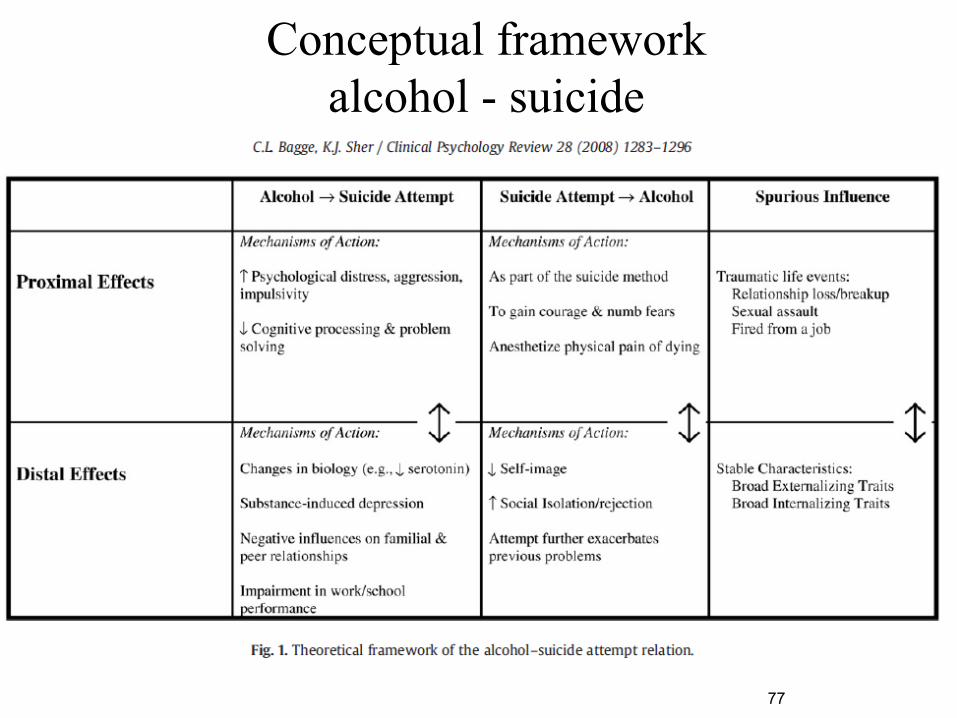
Conceptual framework alcohol - suicide
Efectos Alcohol Suicidio Suicidio Alcohol Proximales • Distrés psicológico
• Agresividad • Impulsividad • Deterioro cognitivo
• Como parte del plan suicida
• Para tener coraje • Para anestesiar el dolor
Distales • Cambios biológicos (serotonina)
• Depresión inducida • Deterioro relaciones • Deterioro profesional
• Deterioro autoestima • Rechazo y aislamiento
social • Agravamiento problemas
previos
Mecanismo de accción Bagge CL, Sher KJ Clinical Psychology Review 28 (2008) 1283–1296
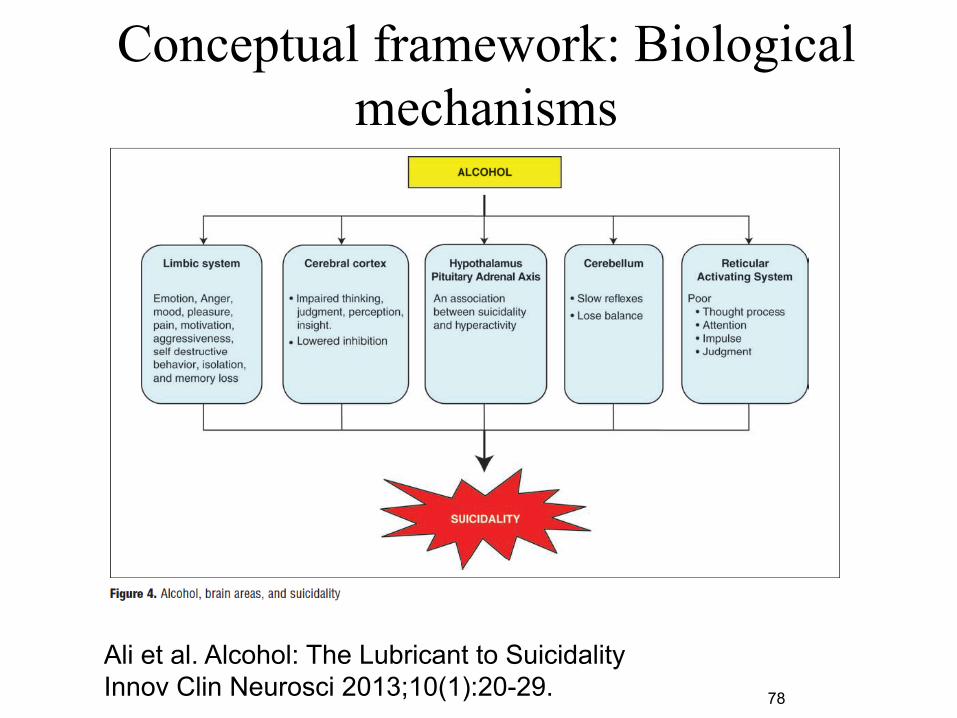
Conceptual framework: Biological mechanisms
78
Ali et al. Alcohol: The Lubricant to Suicidality Innov Clin Neurosci 2013;10(1):20-29.
79
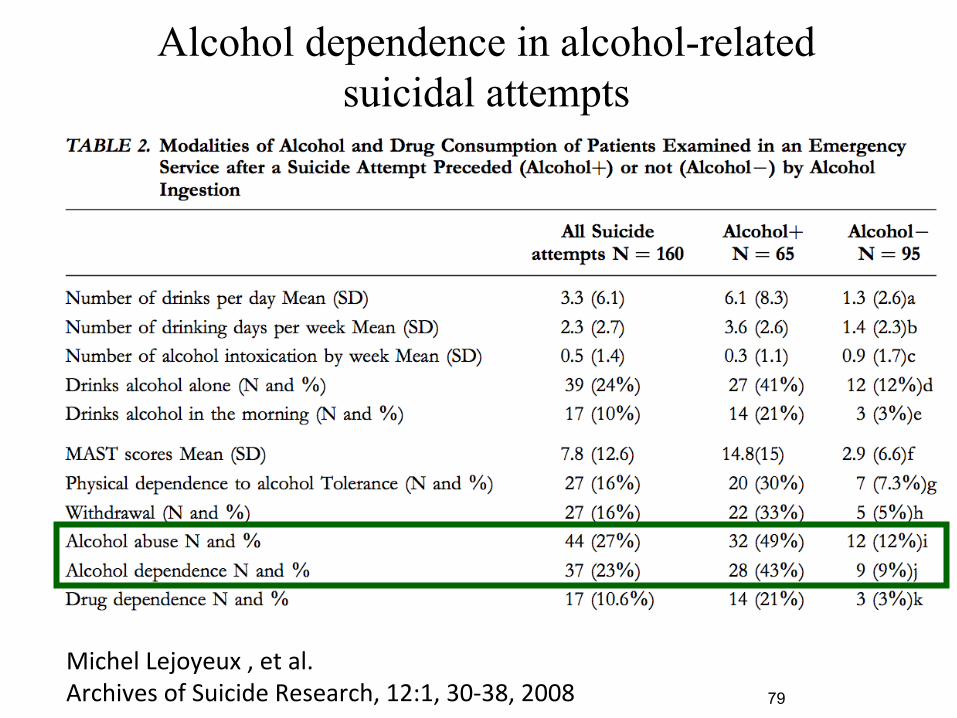
Michel Lejoyeux , et al. Archives of Suicide Research, 12:1, 30-‐38, 2008
Alcohol dependence in alcohol-related suicidal attempts
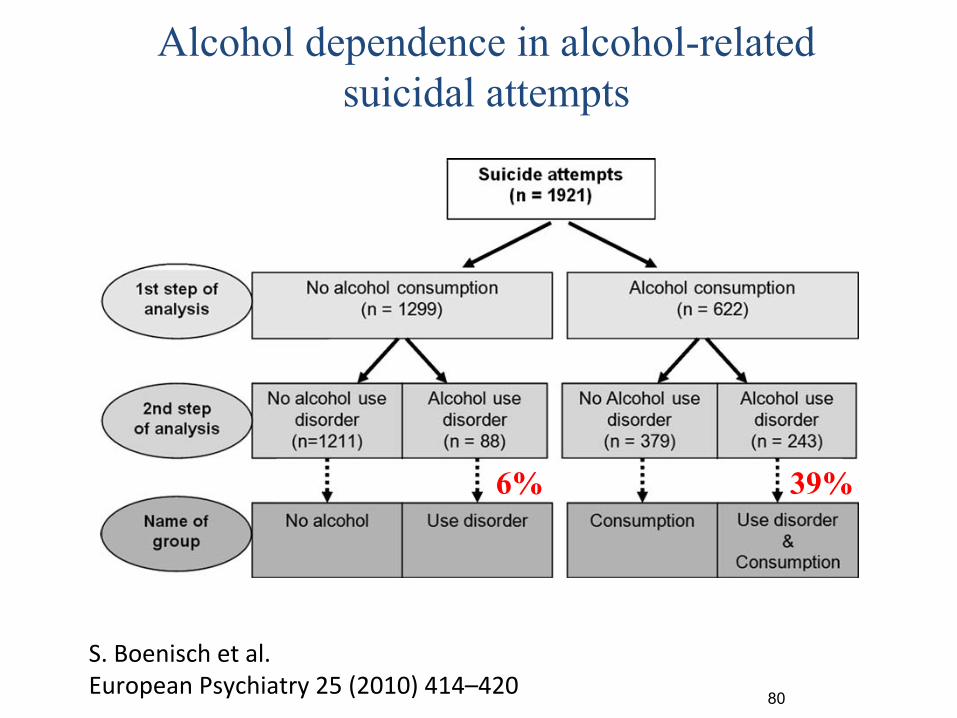
80
S. Boenisch et al. European Psychiatry 25 (2010) 414–420
examining the effects of alcohol use disorder separately from theeffects of alcohol consumption. To this end, the following researchquestions will be clarified:
! Are the characteristics of suicide attempts committed byindividuals with a diagnosis of an alcohol use disorder (malesex, older age range, history of prior suicide attempts) indepen-dent of alcohol consumption?! Is the choice of method of suicide attempt independent of
whether alcohol was consumed or not?
2. Methods
2.1. Study design
Data on suicide attempts was gathered during a 5-year period(2000–2004) in the city of Nuremberg, Germany (480,000 inhabi-tants). ‘‘Suicide attempts’’ defined according to the WHO definitionof parasuicide [4] were documented. In line with the WHOdefinition, habitual deliberate self-harm (e.g. associated with aknown borderline personality disorder) was, therefore, excludedfrom analysis.
Data was gathered at all major sites in Nuremberg wheremedical treatment is usually provided to suicide attempters. This ispredominately the Nuremberg General Hospital. Its department ofpsychiatry serves the entire population in the Nurembergcatchment area. Mental health specialists of the department ofpsychiatry serve as consultants to all other inpatient facilities inNuremberg. Consequently, those inpatient facilities could beincluded in the study. Furthermore, all outpatient crisis interven-tion centres, the local public health authority and a representativenumber of the 70 psychiatric practices in Nuremberg wereincluded in the study. However, the circa of 500 generalpractitioners and psychotherapists in Nuremberg were notincluded in the study. A major number of attempted suicide casescould not be expected among them.
Information was collected during presentation of those whohad attempted suicide. Information was documented by thetreating clinicians by means of an adapted version of themonitoring form of the WHO/EURO Multicentre Study on SuicidalBehaviour. Treating clinicians were physicians or clinical psychol-ogists who made first contact with the suicide attempter in thehospital or practice after the attempted suicide was reported. Theclinicians filled out the monitoring form according to theinformation they gathered during assessment. This includedsociodemographic data, information on current and possible prior
suicide attempts, alcohol use and psychiatric diagnosis accordingto ICD-10. All clinicians were trained in filling out the monitoringform and well versed in using ICD-10. A researcher of the studycentre visited the data-gathering institutions regularly to motivateand train clinicians to monitor suicide attempts and control thevalidity of the data gathered.
Data was pseudonomysed, allowing the identification ofrepeated suicide attempts by the same individuals.
The use of alcohol in connection with the suicide attempt wasdocumented in two ways:
! Diagnoses of alcohol-related disorders according to ICD-10 (F10.1 to 10.9) were clinically made by the treating physician/clinical psychologist and recorded accordingly (referred to asalcohol use disorder).! Consuming alcohol before and/or at the time of the suicide
attempt as well as using alcohol as part of the method(referred to as alcohol consumption) was documented in anopen section that dealt with the method of the suicide attemptin detail.
We distinguished between four groups of suicide attempts(Fig. 1):
! No alcohol: suicide attempts without any relation to alcohol, i.e.,without alcohol consumption at the time of suicide attempt andwithout a clinical diagnosis of alcohol use disorder;! Use disorder: suicide attempts committed by individuals with a
diagnosis of alcohol use disorder but without alcohol consump-tion at the time of the suicide attempt;! Consumption: suicide attempts by individuals consuming
alcohol in relation to the attempt but without a diagnosis ofalcohol use disorder.! Use disorder and consumption: suicide attempts by individuals
consuming alcohol in relation to the attempt and with adiagnosis of alcohol use disorder.
The study was approved by the ethics committee of the LudwigMaximilian University in Munich and was in line with theguidelines laid down in the current version of the Declaration ofHelsinki.
2.2. Data processing and statistical analysis
Age was summarised in ‘‘age groups’’. For ethical reasons theminimum age was 18 years. ‘‘Methods of suicide attempt’’ were
Fig. 1. Classification of suicide attempts depending on alcohol consumption at the time of suicide attempt and a diagnosis of alcohol use disorder.
S. Boenisch et al. / European Psychiatry 25 (2010) 414–420 415
6% 39%
Alcohol dependence in alcohol-related suicidal attempts
81 Suokas J, Lönnqvist J. Acta Psychiatr Scand. 1995 Jan;91(1):36-40
82
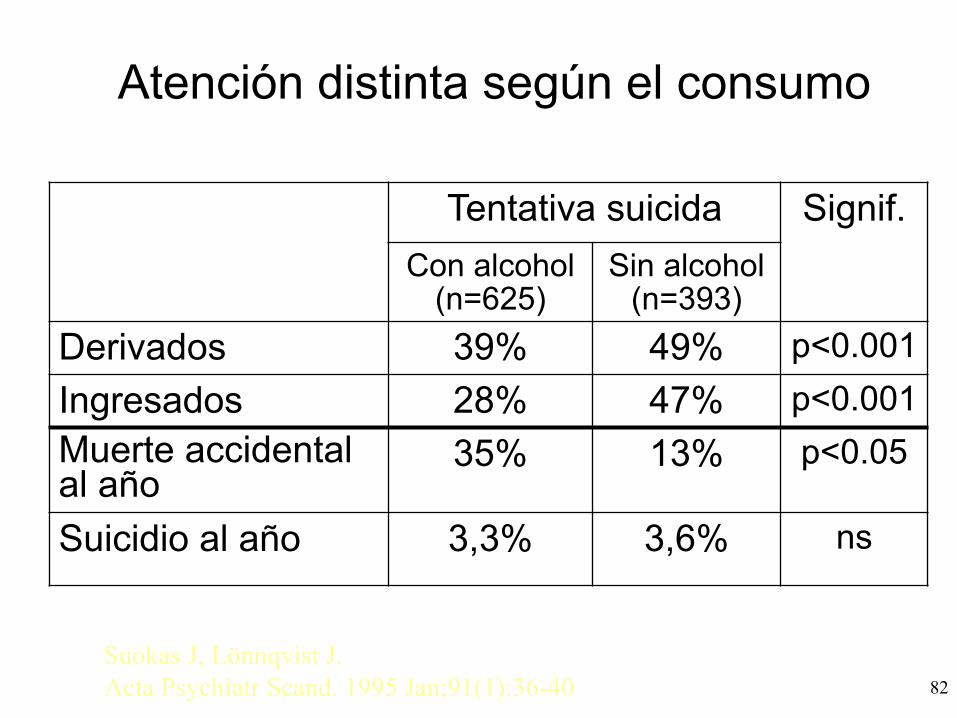
Atención distinta según el consumo
Tentativa suicida Signif. Con alcohol
(n=625) Sin alcohol
(n=393) Derivados 39% 49% p<0.001 Ingresados 28% 47% p<0.001 Muerte accidental al año
35% 13% p<0.05
Suicidio al año 3,3% 3,6% ns
Suokas J, Lönnqvist J. Acta Psychiatr Scand. 1995 Jan;91(1):36-40
¿Cual es la comorbilidad más prevalente?
• La comorbilidad médica • La comorbilidad psiquiátrica
– Tabaco, adicciones y psiquiatría – Alcohol, ansiedad y depresión – Adicción y suicidio – Trastornos de personalidad y adicción
83
TP y adicción
• Mayor complejidad • Patrón adic/vo irregular • Impacto nega/vo de la adicción en el TP • Necesidad de un abordaje integral
Psychiatr Serv. 2014 Dec 1;65(12):1406-‐8. doi: 10.1176/appi.ps.201400235. Epub 2014 Oct 31. Integrated care: tobacco use and mental illness: a wake-‐up call for psychiatrists. Williams JM1, Stroup TS, Bruneme MF, Raney LE. Author informaLon Abstract Tobacco use results in numerous consequences for individuals with mental illnesses and other substance use disorders, yet it is not adequately addressed by behavioral health professionals, including psychiatrists. This column describes current inac/on among behavioral health professionals and some possible reasons for it and recommends next steps. Psychiatrists should provide treatment for all pa/ents with a co-‐occurring tobacco use disorder and provide leadership to change policies and prac/ces in treatment centers. Psychiatrists can be vital leaders of the effort to reduce the toll of tobacco use among people with mental illnesses, addic/ons, or both. A na/onal movement for addressing tobacco use in the behavioral health field can be galvanized if more psychiatrists par/cipate.
• Muestra: Profesionales en la base de datos de la SEPD (> 2000) • Par/cipantes: 659 profesionales • Encuesta online
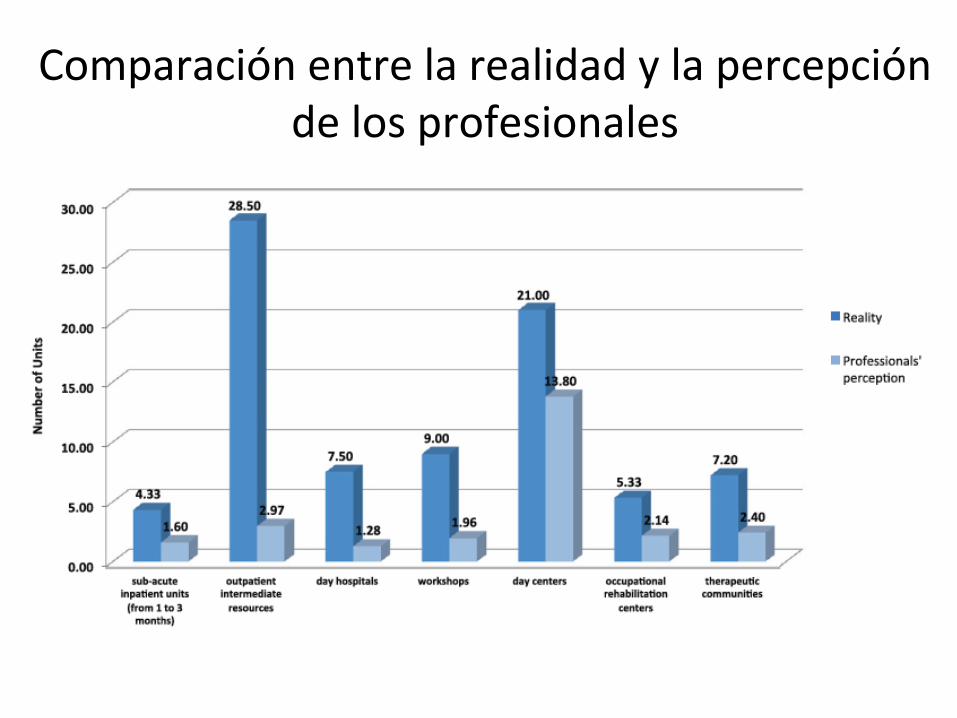
Comparación entre la realidad y la percepción de los profesionales
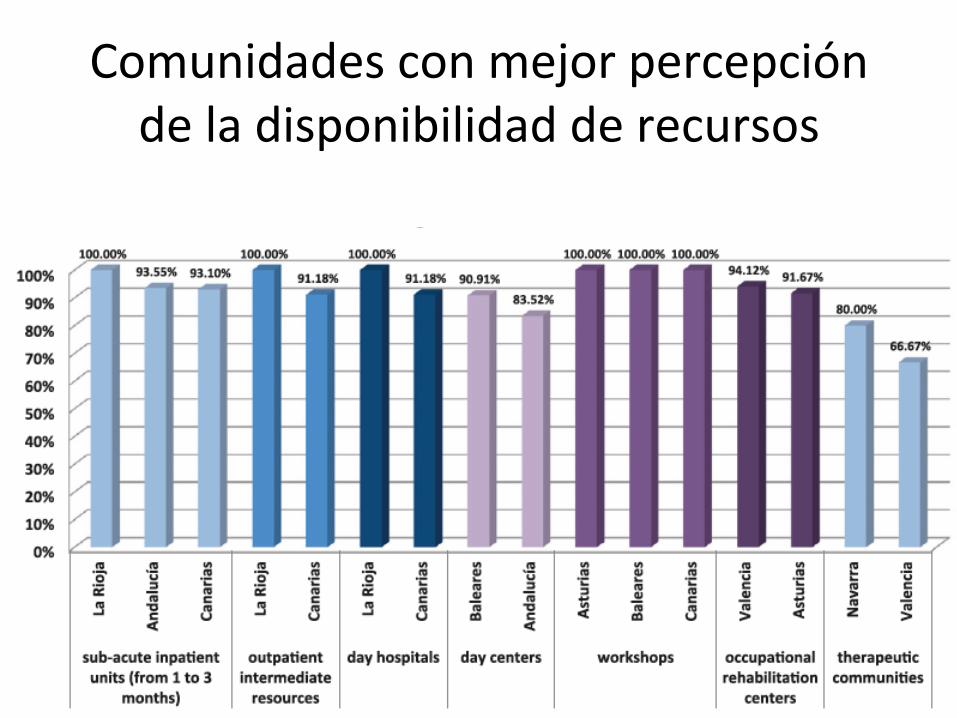
Comunidades con mejor percepción de la disponibilidad de recursos
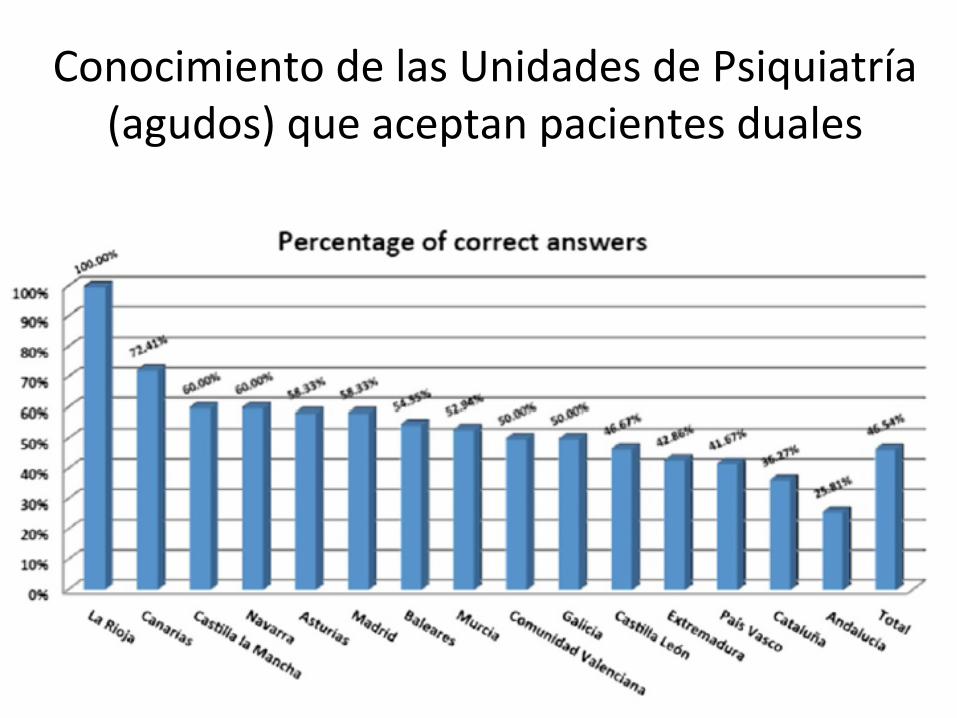
Conocimiento de las Unidades de Psiquiatría (agudos) que aceptan pacientes duales
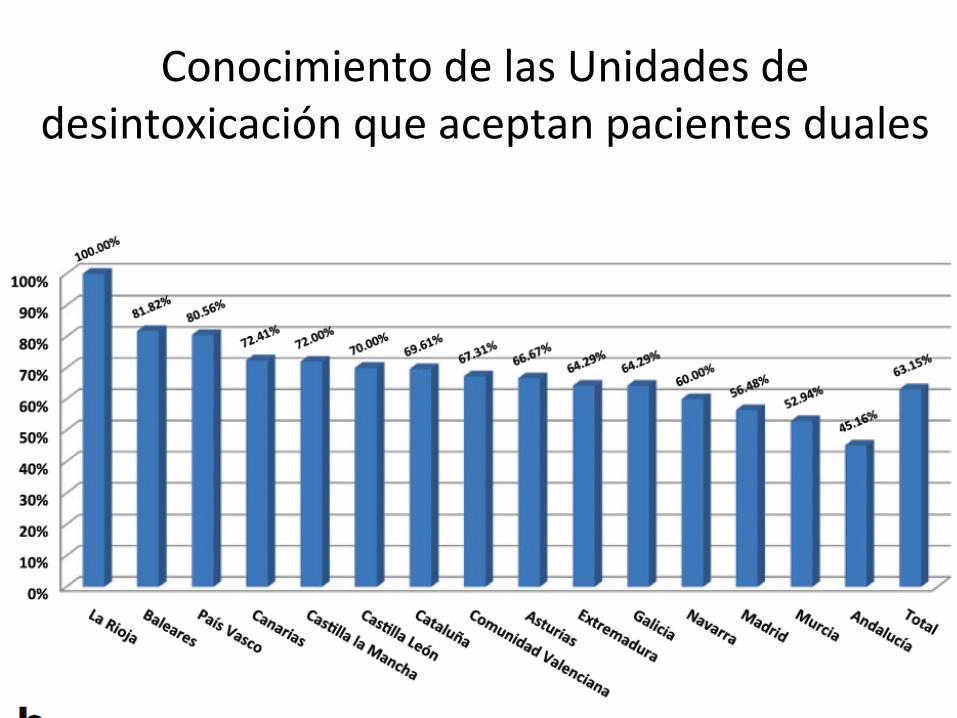
Conocimiento de las Unidades de desintoxicación que aceptan pacientes duales
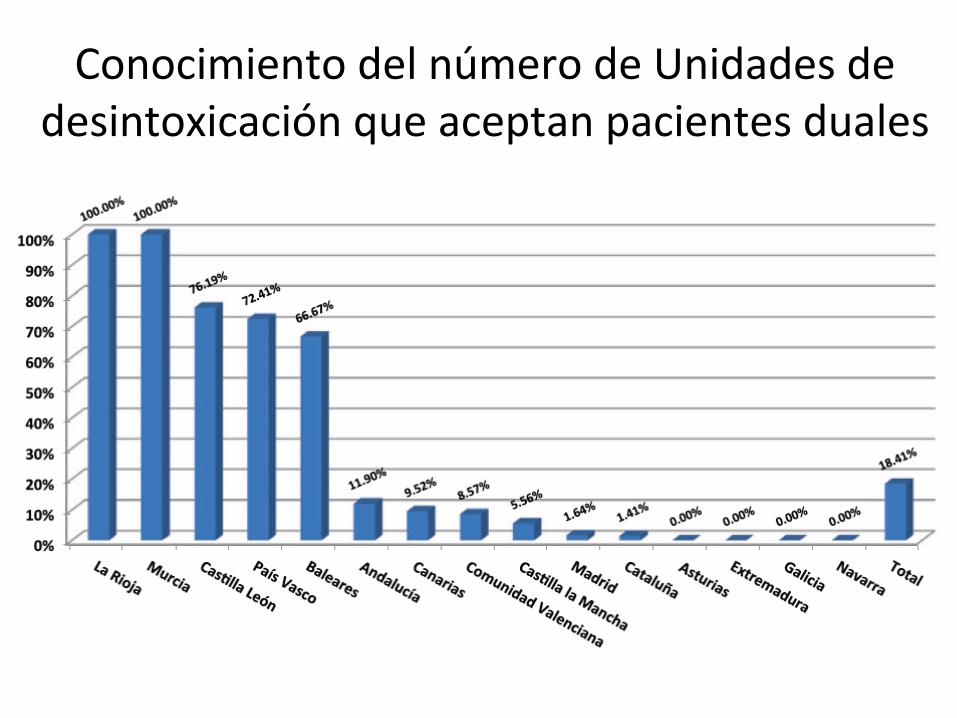
Conocimiento del número de Unidades de desintoxicación que aceptan pacientes duales
Conclusiones
• La patologia dual (y trial) es altamente prevalente
• Su abordaje debe ser mediante un modelo de atención integral y con un es/lo mo/vacional
• Ansiedad y depresión son las patologías comórbidas más prevalentes
• El conocimiento de los recursos asistenciales es todavía insuficiente
Manejo clínico del paciente con enfermedad mental y adicciones: El tratamiento de la comorbilidad.
Antoni Gual Unidad de Conductas Adic/vas ICN. Hospital Clínic. Barcelona
IDIBAPS. RTA [email protected]





























