Embed Size (px)
Citation preview
Dr. Salah Atta, MDDr. Salah Atta, MDConsultant Electrophysiolgist, SBCCConsultant Electrophysiolgist, SBCC
Professor of CardiologyProfessor of Cardiology,,Assiut UniversityAssiut University..
Electrophysiologic studyElectrophysiologic study
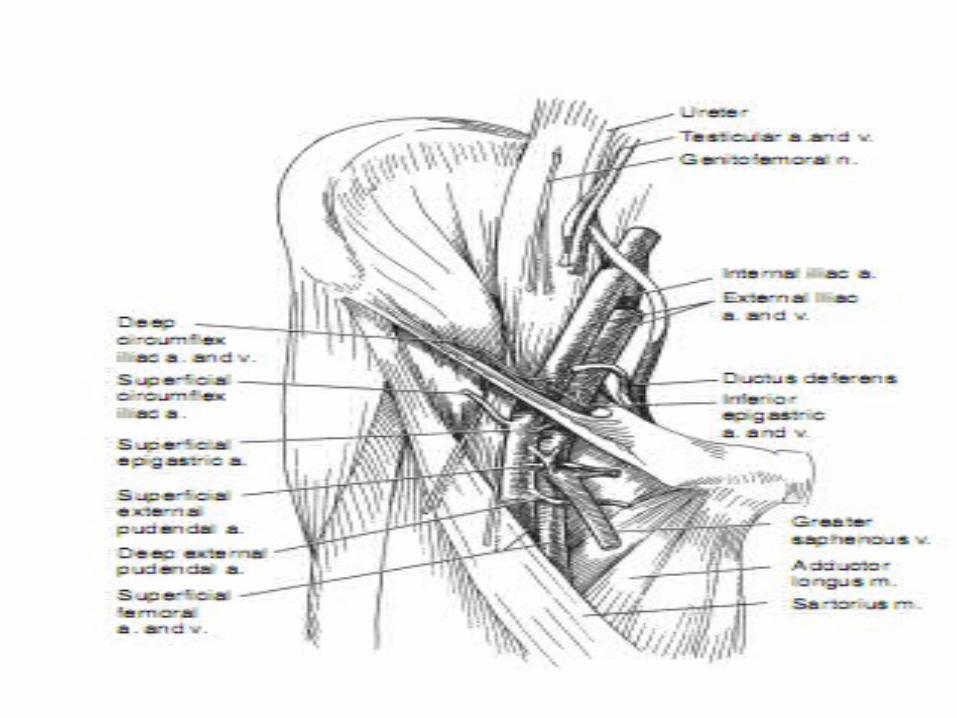
An electrophysiologic study (EPS) entails the An electrophysiologic study (EPS) entails the percutaneous introduction and positioning of percutaneous introduction and positioning of multiple special electrode catheters in strategic multiple special electrode catheters in strategic sites in the heart in order to:sites in the heart in order to:
1- 1- Record, explore intracardiac sequence of Record, explore intracardiac sequence of impulse formation and activation. impulse formation and activation.
2-2- Stimulate and evaluate automaticity, Stimulate and evaluate automaticity, conduction and refractoriness.conduction and refractoriness.
3-3- Initiate, terminate, diagnose and manage Initiate, terminate, diagnose and manage arrhythmias.arrhythmias.
Indications of EPS:Indications of EPS:
• Evaluation of bradycardias: Evaluation of bradycardias: sinus node sinus node
functions, level and severity AV blockfunctions, level and severity AV block
• Evaluation of tachycardias: Evaluation of tachycardias: Narrow and Narrow and
Wide QRS complex tachycardia for diagnostic and Wide QRS complex tachycardia for diagnostic and
therapeutic purposes.therapeutic purposes.
• Evaluation of unexplained syncope: Evaluation of unexplained syncope: recurrent unexplained syncope with –ve tilt test or recurrent unexplained syncope with –ve tilt test or
with structural heart disease and failure of non with structural heart disease and failure of non
invasive tests.invasive tests.
Electrophysiologic studyElectrophysiologic study
• Evaluation of cardiac arrest survivors: Evaluation of cardiac arrest survivors: with no with no
myocardial infarction (MI) or 48 hs after MI with no acute myocardial infarction (MI) or 48 hs after MI with no acute
ischaemia.ischaemia.
• Evaluation of palpitation:Evaluation of palpitation: specially palpitation specially palpitation
preceding syncope or with rapid pulse but no preceding syncope or with rapid pulse but no
ECG documentation.ECG documentation.
• Risk stratification in suspected Risk stratification in suspected
channelopathies, asymptomatic WPW.channelopathies, asymptomatic WPW.
Electrophysiologic studyElectrophysiologic study
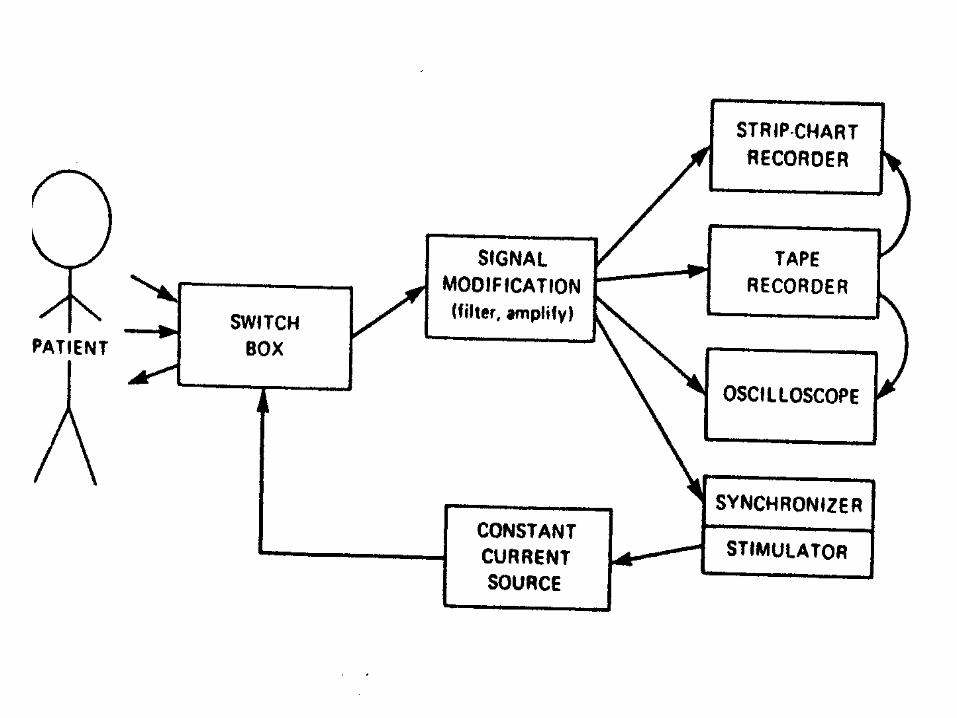
Requirements:Requirements:Well trained and knowledged Personnel.Well trained and knowledged Personnel.Cath Lab.Cath Lab.Electrode Catheters.Electrode Catheters.Stimulator.Stimulator.Displaying and recording system.Displaying and recording system.Junction Box.Junction Box.
What is needed ?!
Preprocedure check list:Preprocedure check list:written consent, written consent, stop antiarrhythmics 5 half-lives before, stop antiarrhythmics 5 half-lives before, stop warfarin 3-5 days before and check stop warfarin 3-5 days before and check INR on the day, insure patient fasting, IV INR on the day, insure patient fasting, IV access, blood pressure monitoring, access, blood pressure monitoring, emergency equipment available, check emergency equipment available, check drugs available ( isoprenaline, atropine, drugs available ( isoprenaline, atropine, adenosine, sedatives and analgesics).adenosine, sedatives and analgesics).
What to do ?!
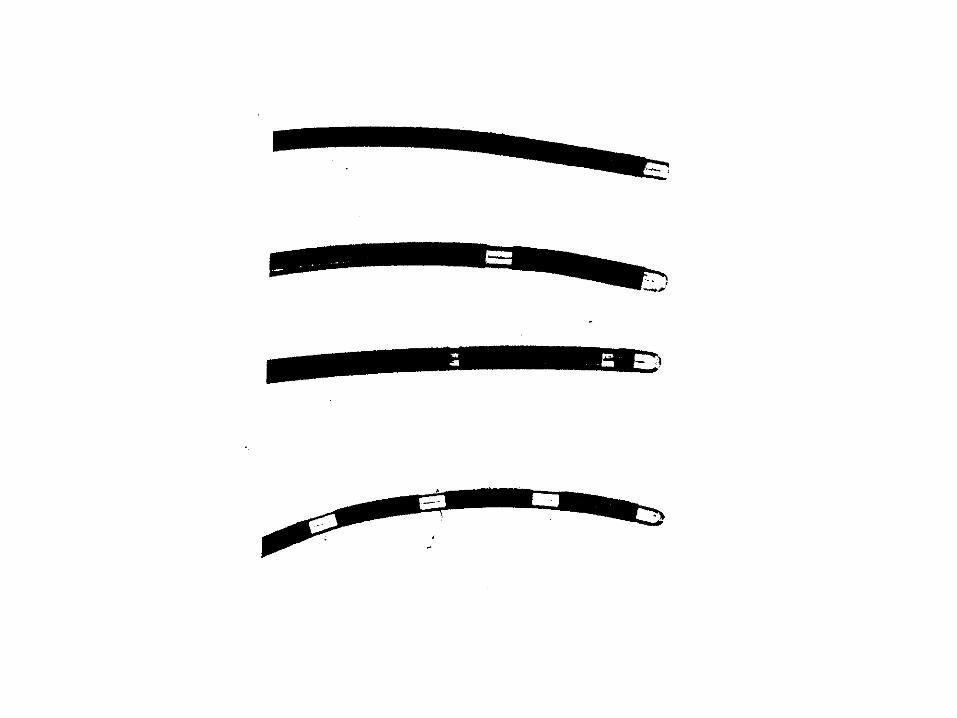



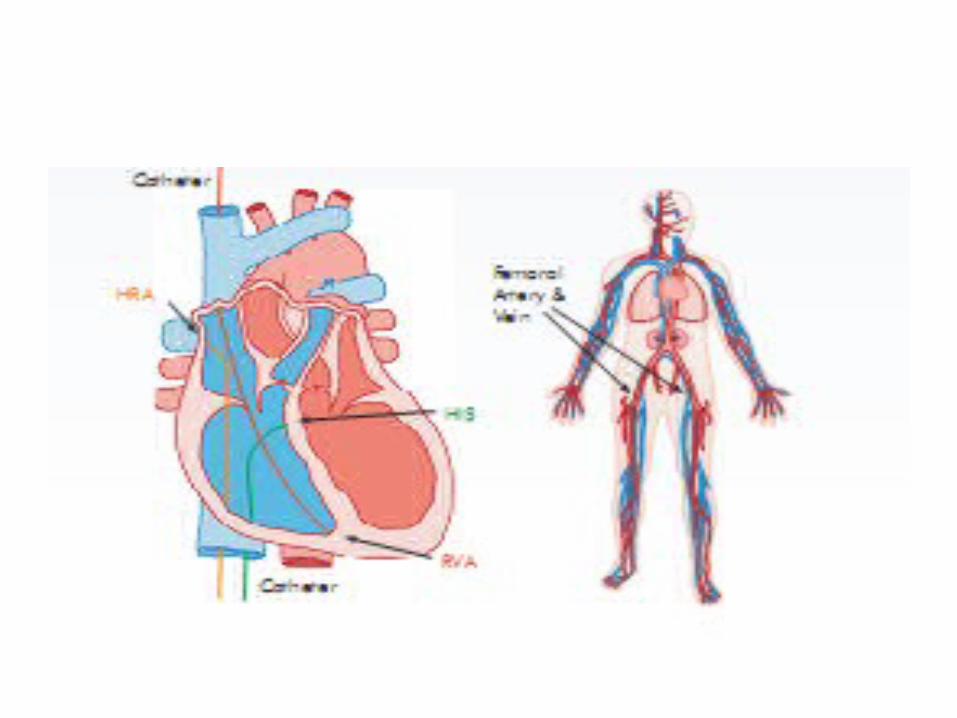
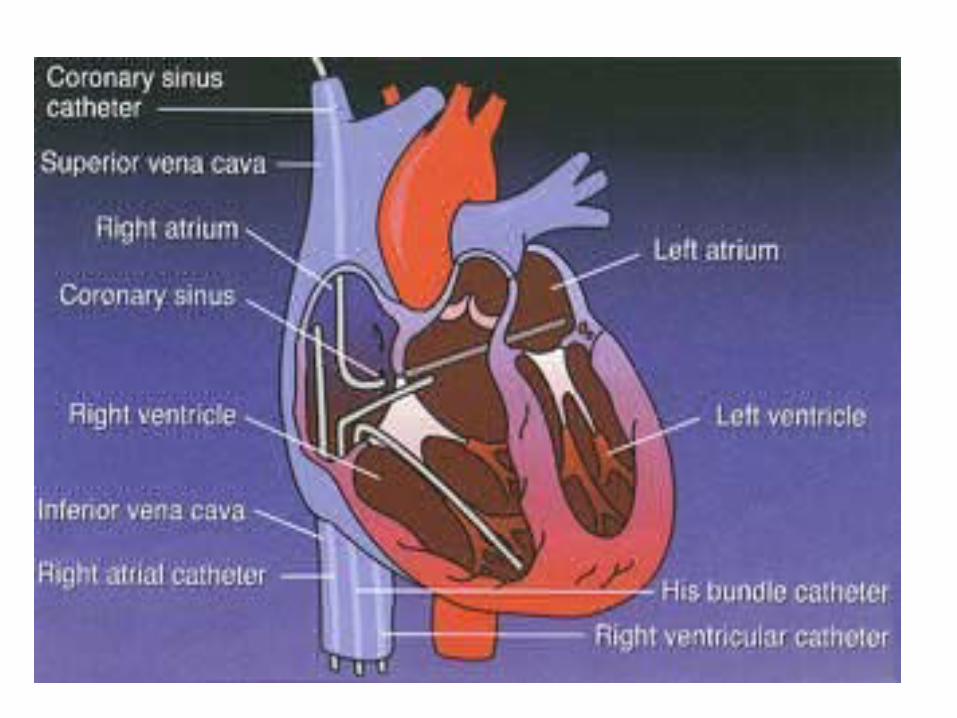
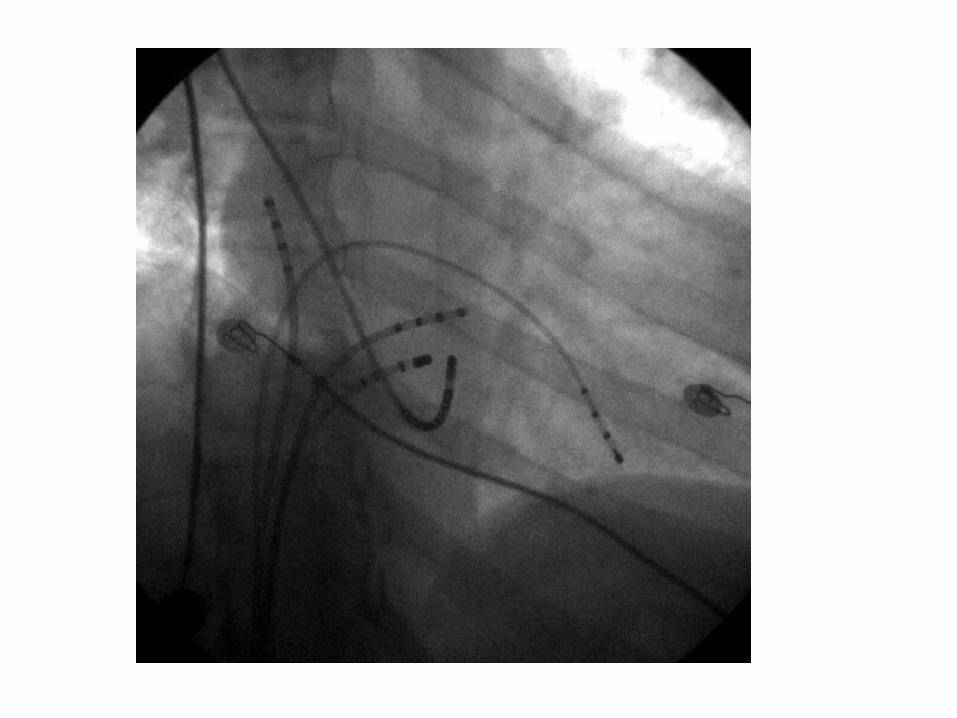
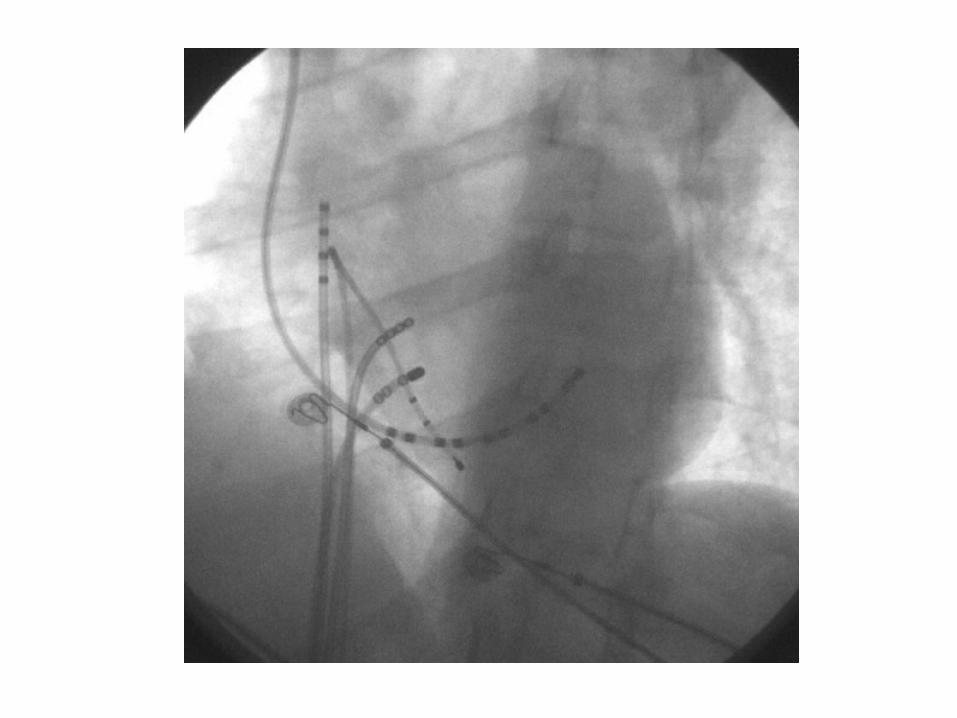
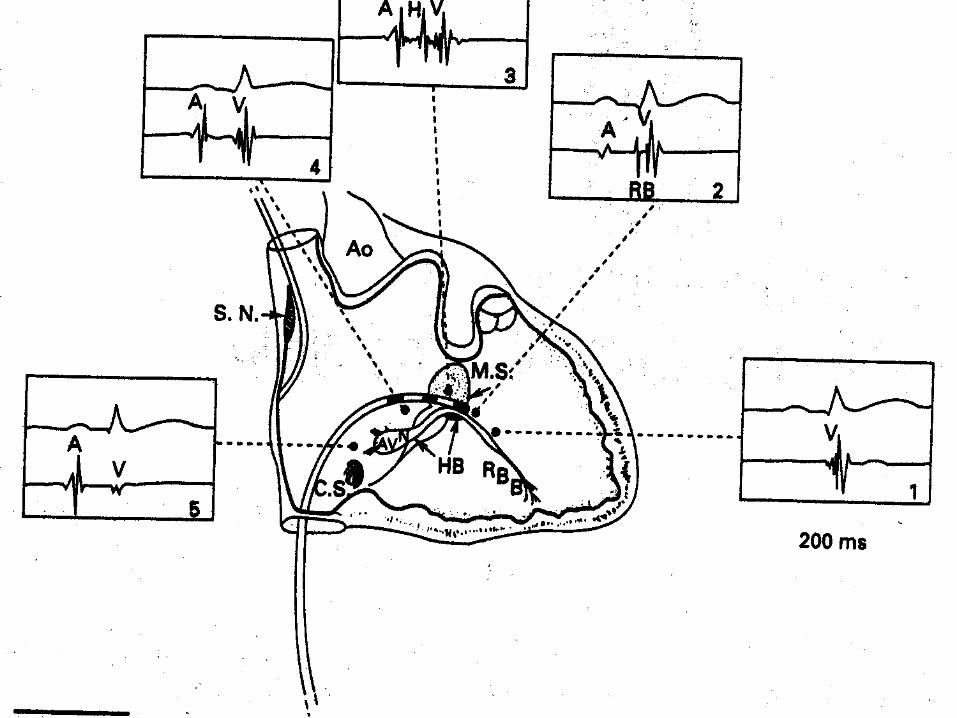
Basically, Catheters are placed Basically, Catheters are placed transvenously in four positions: transvenously in four positions:
• HRA (high right atrium).HRA (high right atrium).• RV (right ventricle).RV (right ventricle).• His : across the superior aspect of His : across the superior aspect of
the tricuspid ring.the tricuspid ring.• CS (coronary sinus)CS (coronary sinus)
Where to go ?!

Bipolar Recordings
• Cardiac electrograms are generated by the potential (voltage) differences recorded at two recording electrodes during the cardiac cycle. All clinical electrogram recordings are differential recordings from one source that is connected to the anodal (positive) input of the recording amplifier and a second source that is connected to the cathodal (negative) input.
Unipolar Recordings• Unipolar recordings are obtained by
positioning the exploring electrode in the heart and the second electrode (referred to as an indifferent electrode) distant (theoretically an infinite distance) from the heart such that it has little or no cardiac signal.
• The pre-cordial ECG leads are unipolar recordings that use an indifferent electrode (Wilson central terminal), created by connecting the arms and left leg electrodes through high impedance resistors.
• Most clinical recording systems have the option for selecting a unipolar recording mode that connects the negative input of the recording amplifier to the Wilson central terminal.
• We may use an alternative to the Wilson central terminal to reduce electrical noise. The amplifier is left in the bipolar configuration, but the negative input is connected to an intravascular electrode that is remote from the heart, in the inferior vena cava.
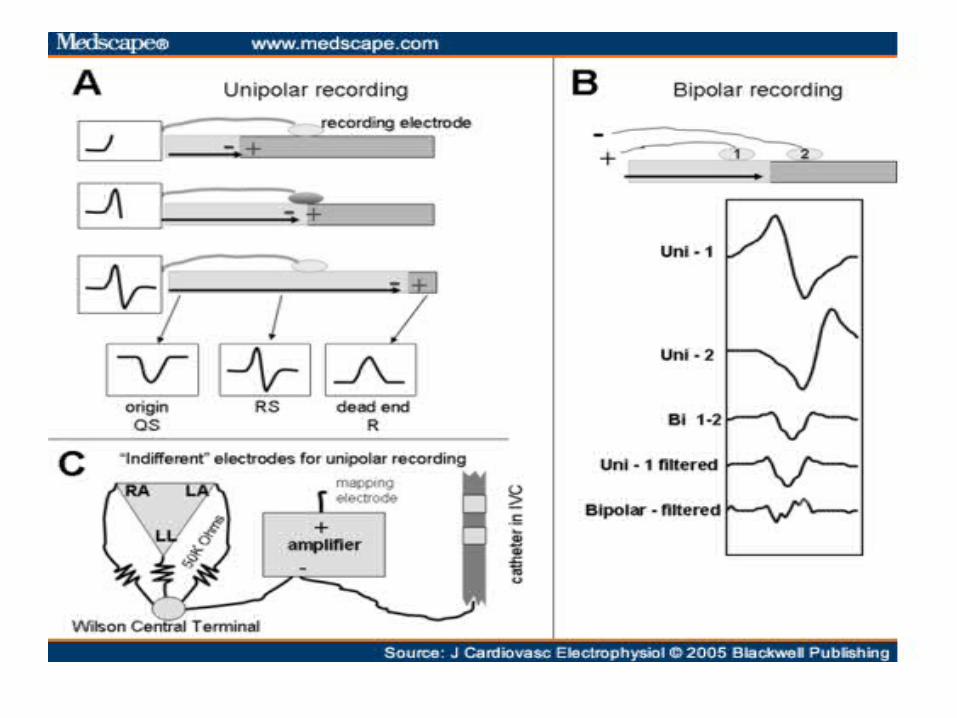
• By convention the exploring electrode that is in contact with the myocardium is connected to the positive input of the recording amplifier. In this configuration a wavefront of depolarization that is propagating toward the exploring electrode generates a positive deflection.
• As the wavefront reaches the electrode and propagates away, the deflection sweeps steeply negative. Thus an R/S complex is generated. In a sheet of uniformly conducting tissue, the maximum negative slope (–dV/dt) of the signal coincides with the arrival of the depolarization wavefront directly beneath the electrode.
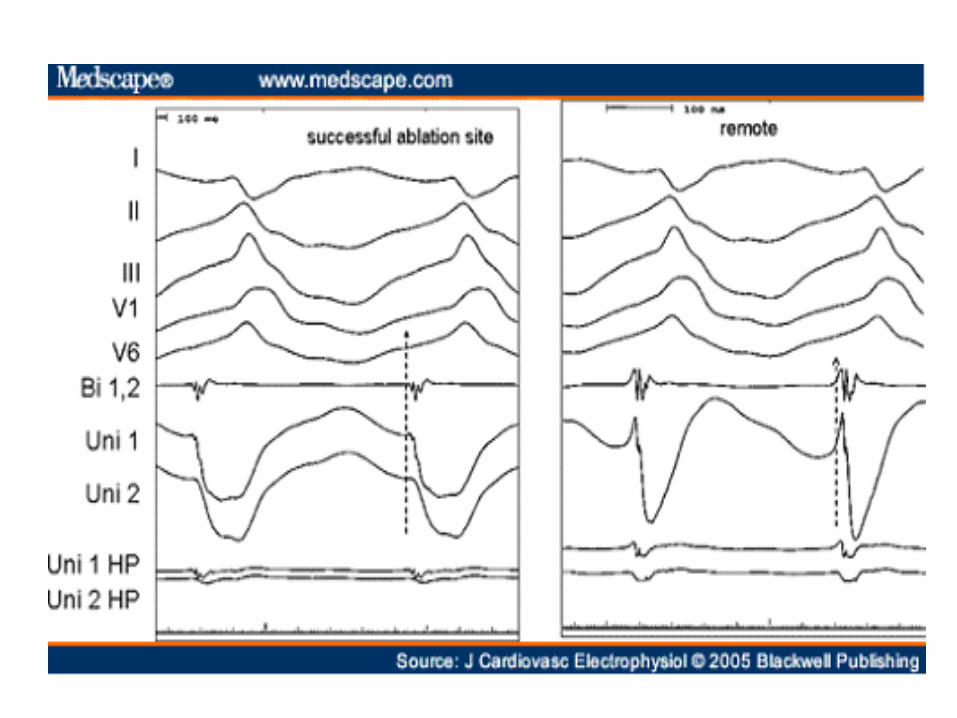
Unipolar Recordings for Identifying the Site of Earliest Activation
• The morphology of the unipolar recording indicates the direction of wave front propagation, provided that the corner frequency for the high pass filter is kept low; we usually use 0.5 Hz. When the exploring electrode is located at the site of initial activation depolarization produces a wavefront that spreads away from the electrode generating a monophasic QS-complex.
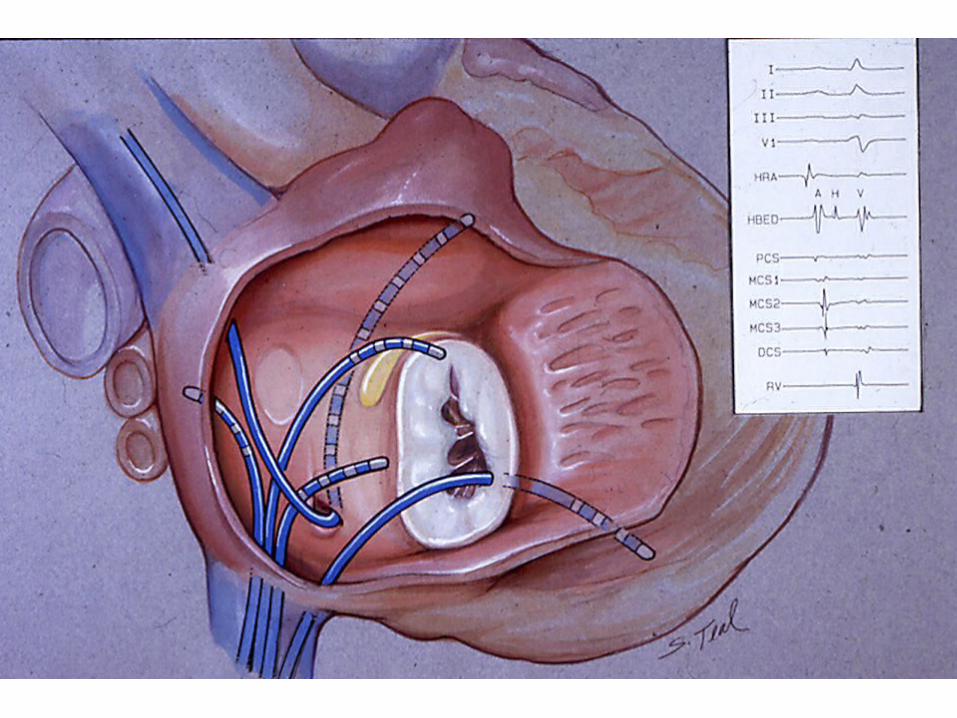
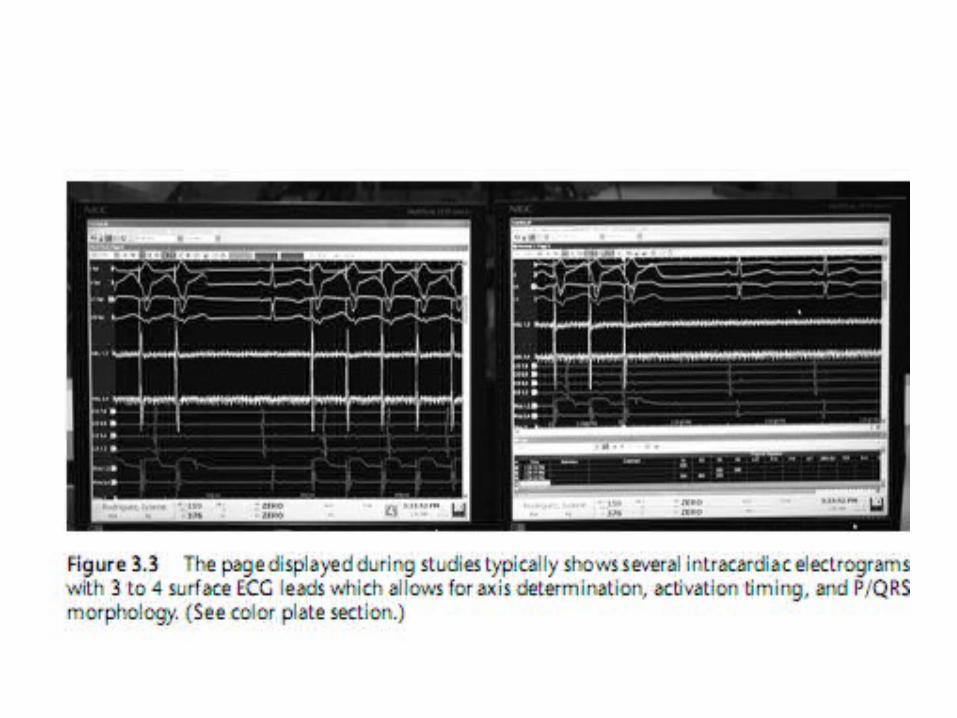
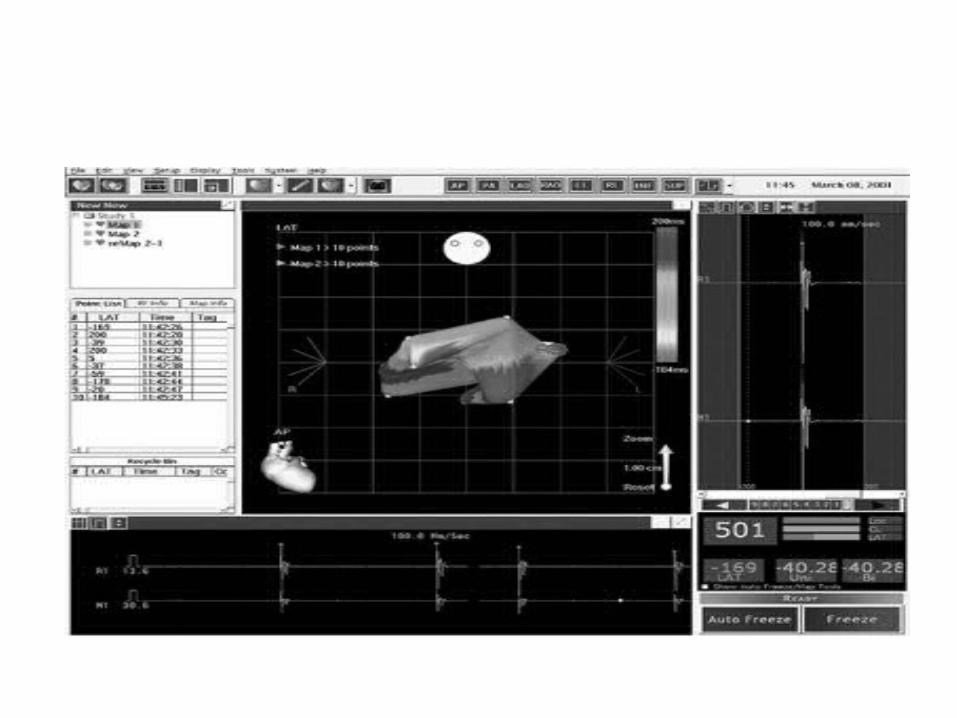
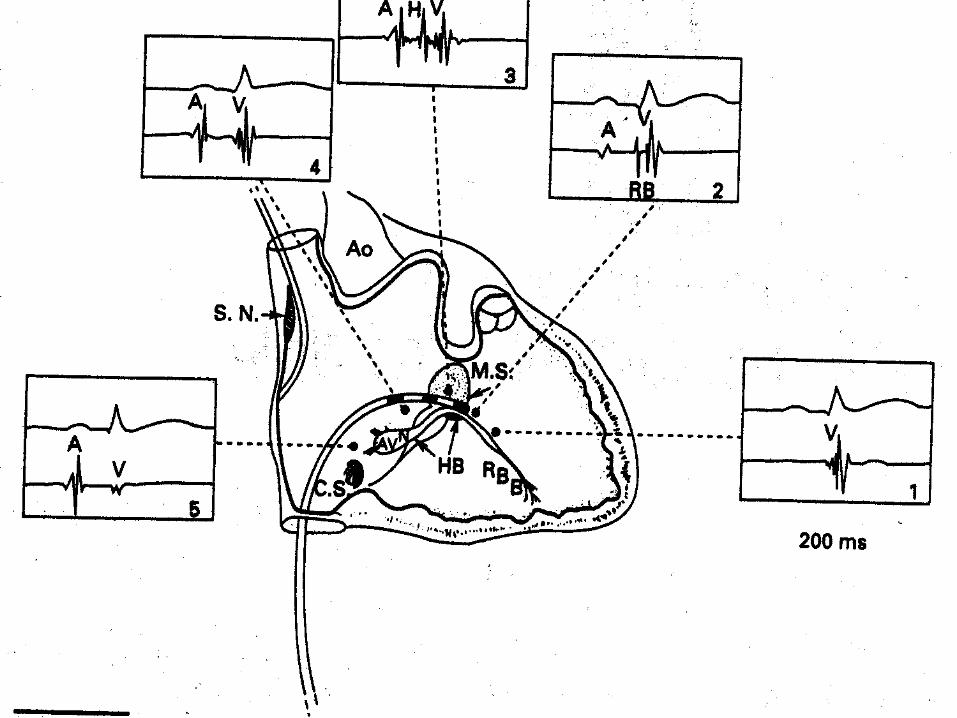
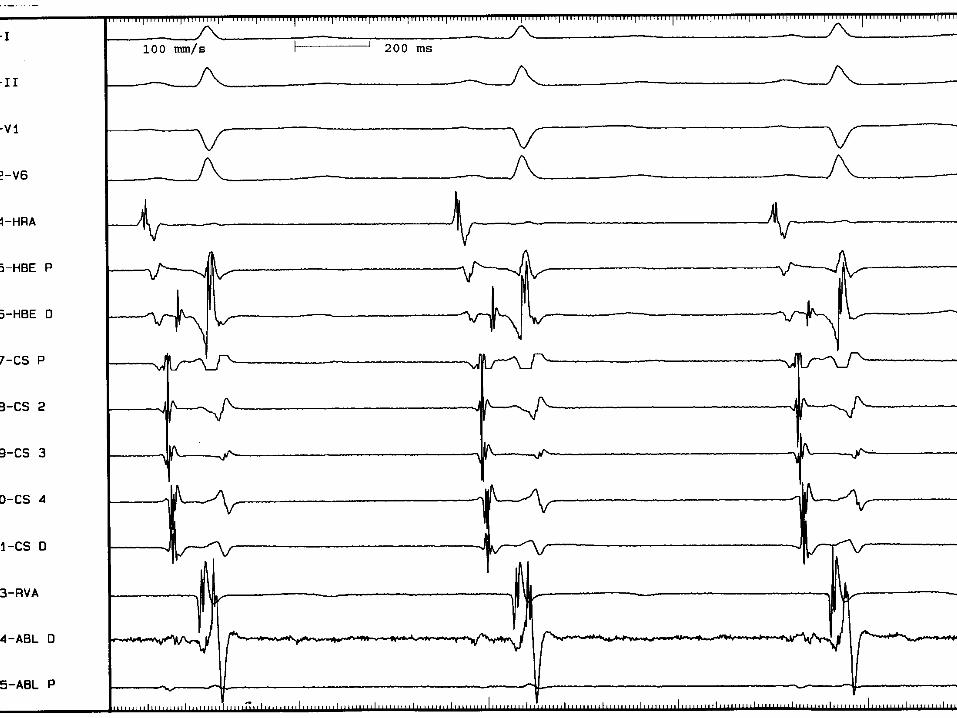
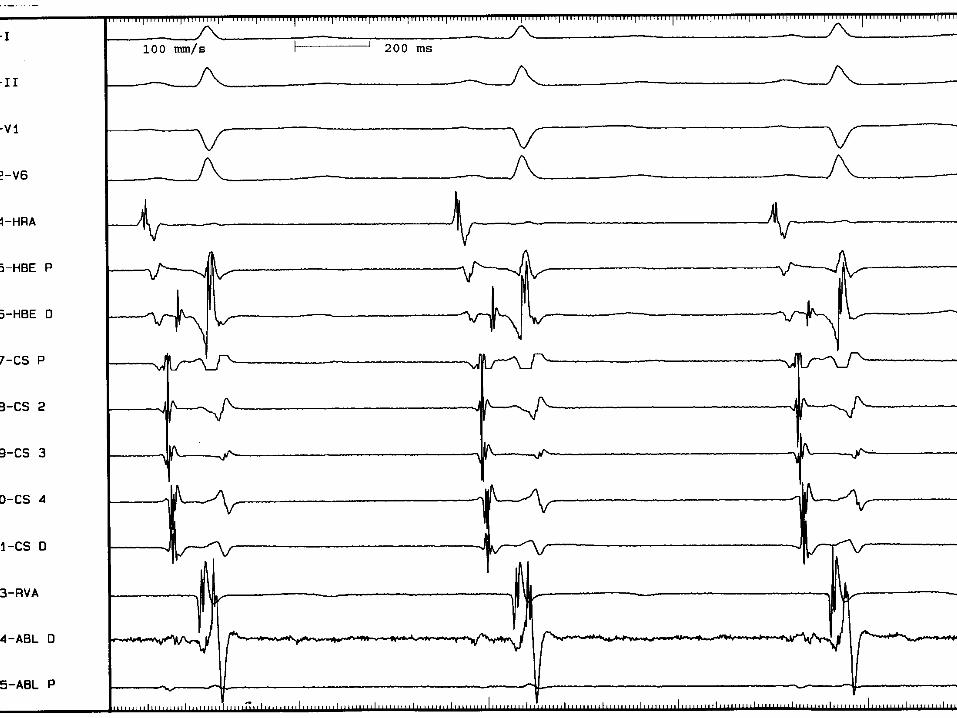
Reading An EP tracing:
(Identify the channels and correlate electrograms)
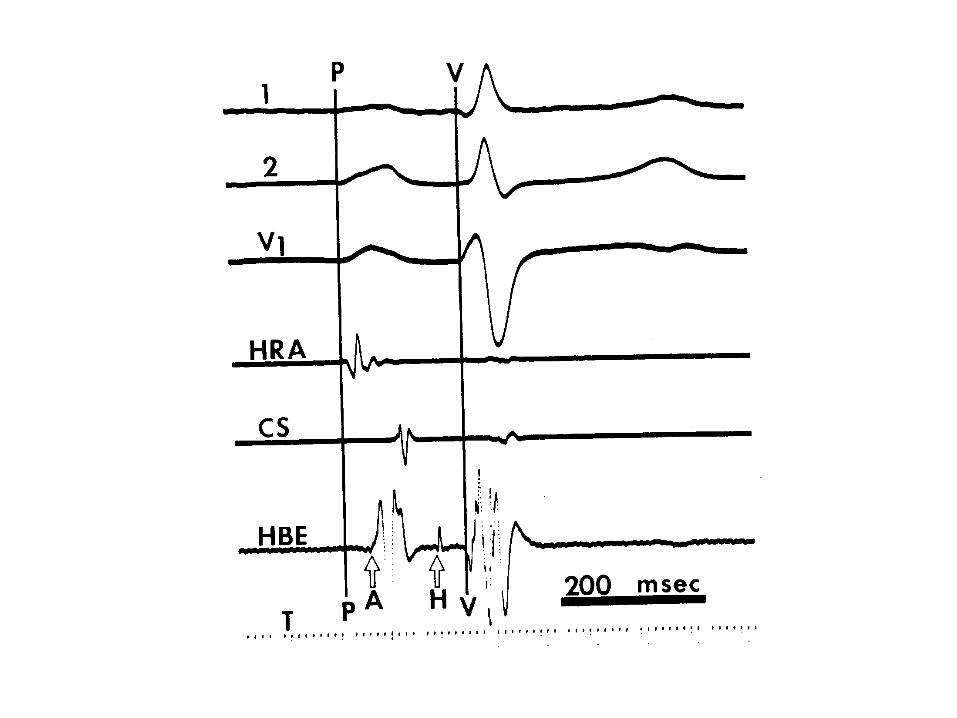
•Ist correlate the intracardiac electrogram with surface ECG: •Electrogram coincident with P wave represents atrial activity (A), •Electrogram coincident with QRS wave represents ventricular activity (V). •Electograms in between represent the conduction system: His, Bundle B, AP.
• Identify if any pacing stimulus, then from which channel is it done and in which manner.
• Can measure the intervals using the system or the tracing using the ruler and knowing the recording speed:
• the duration in ms = distance in mm x 1000/speed in mm
• e.g if speed is 100 mm/sec, then 100 mm =1000 msec and a distance of 20 mm= 20x1000/100=200 msec
The key to understanding an EP The key to understanding an EP tracing is the simple tracing is the simple understanding of the activation understanding of the activation sequence of the heart.sequence of the heart.
During EPS the activation During EPS the activation sequence is examined in sequence is examined in several settings. several settings.
How to know ?!
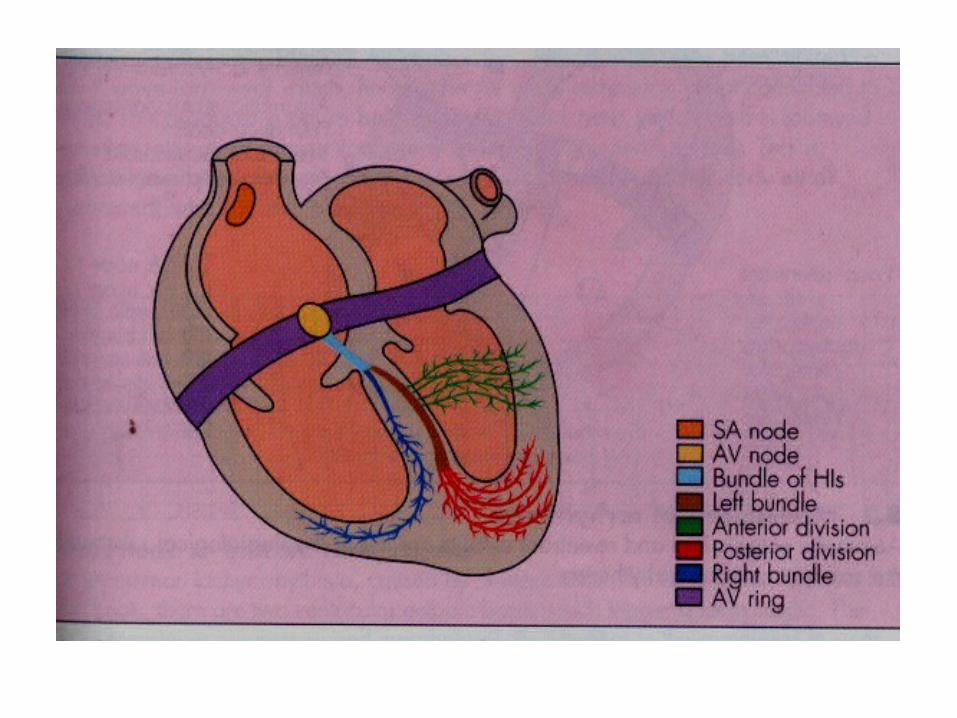
During normal sinus rhythm:During normal sinus rhythm:
Normal sequence of activation in Normal sequence of activation in the atrium and in the ventricles.the atrium and in the ventricles.
How to know ?!
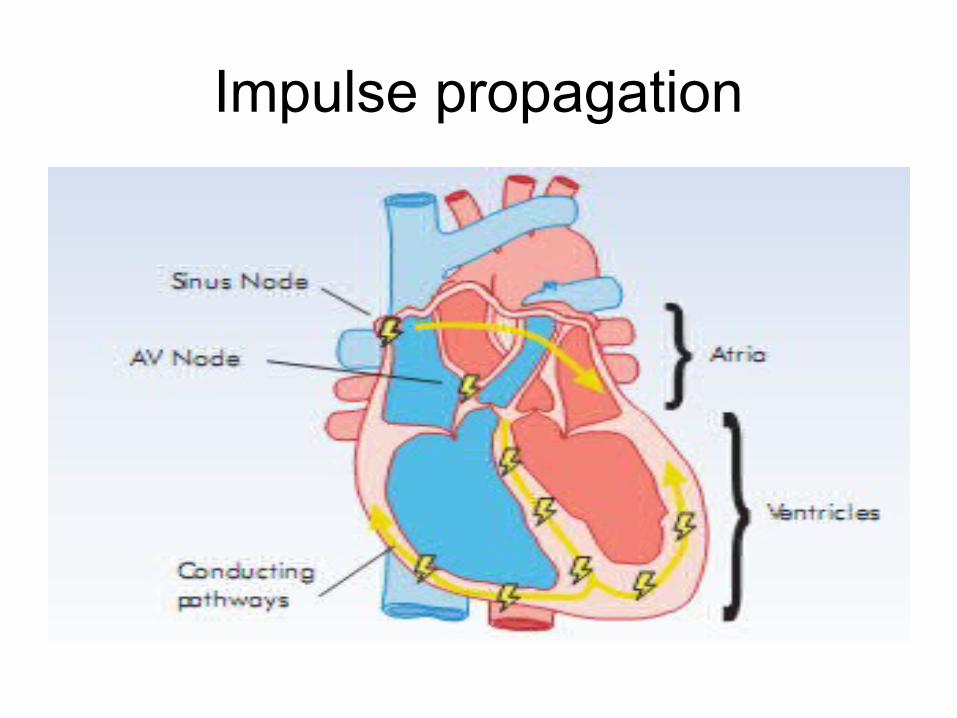
Impulse propagation
Sequence of Activation
• Determination of the sequence of antegrade and retrograde atrial and ventricular activation during spontaneous rhythms, atrial pacing, ventricular pacing, and induced rhythms is essential in differentiating ventricular tachycardia from supraventricular tachycardia and in defning the reentrant circuit in supraventricular tachycardia.
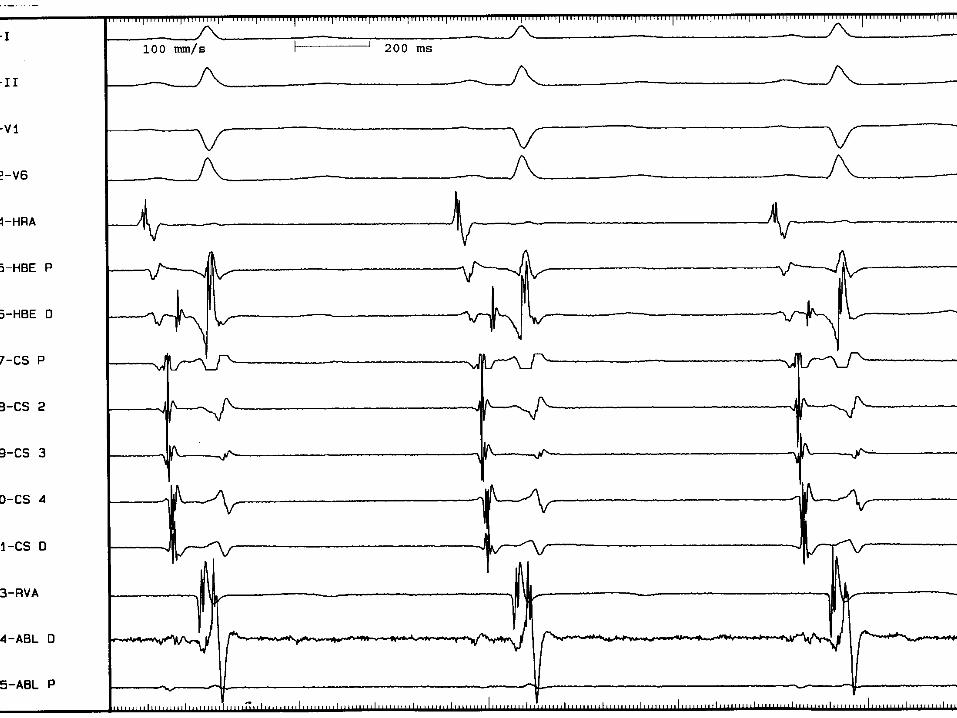
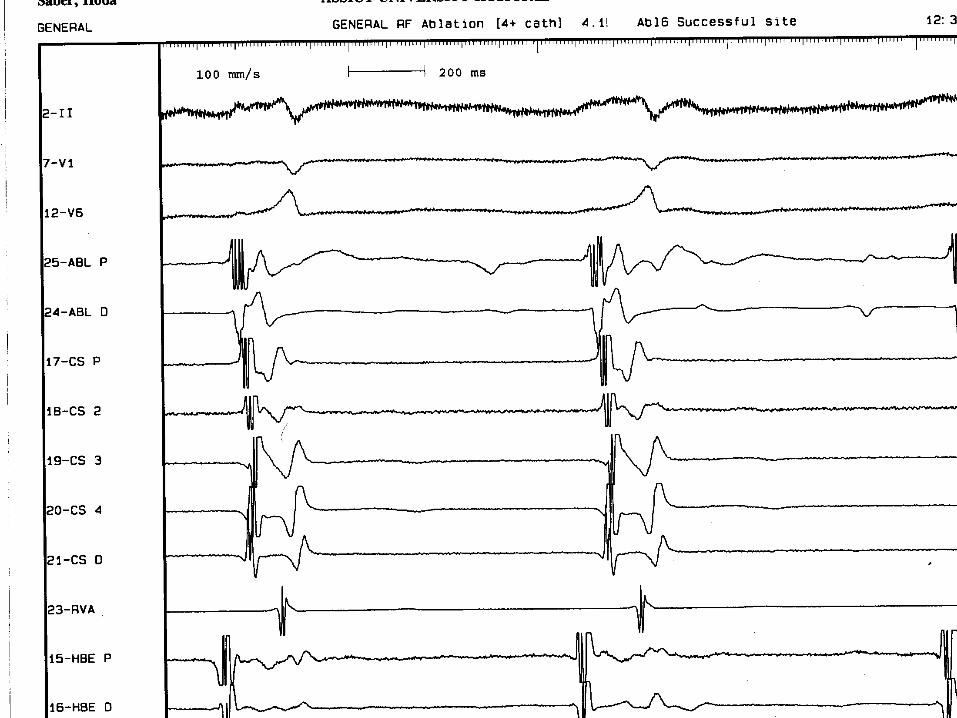
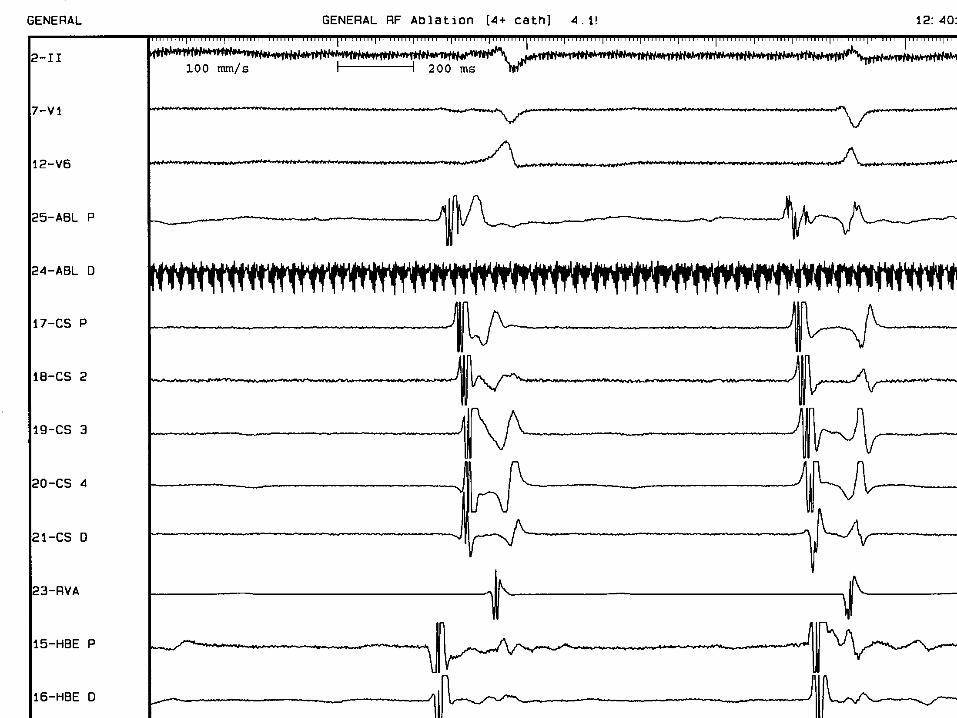
Sequence of Antegrade Activation
• The atrial activation normally begins in the high right atrium and spreads to the low right atrium and His bundle, with left atrial activation recorded from the coronary sinus catheter occurring signifcantly later.
Sequence of Retrograde Activation
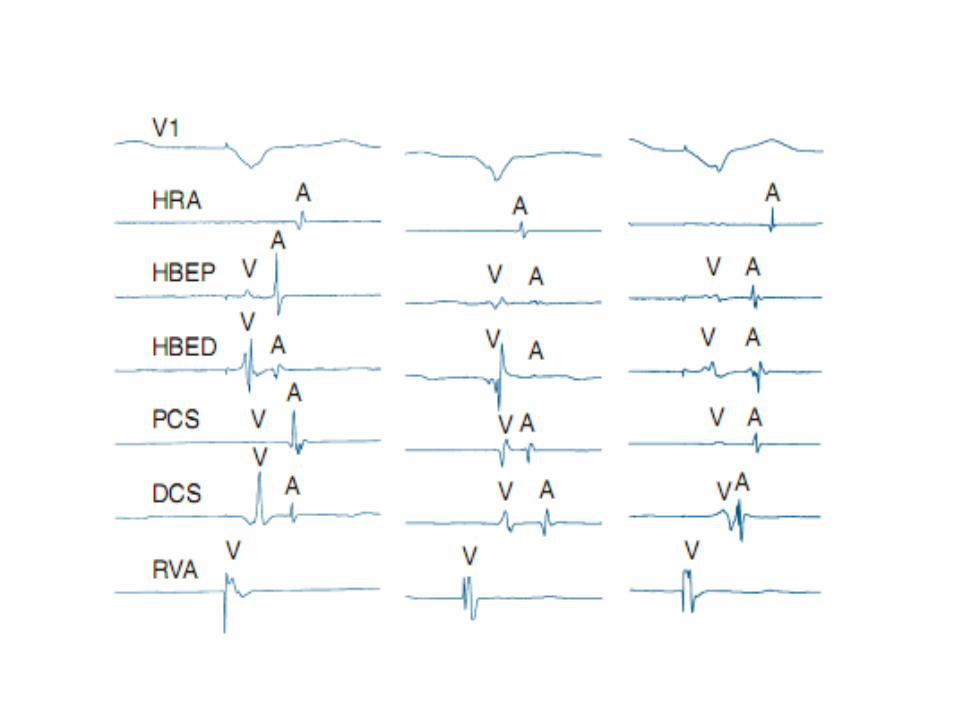
When ventriculoatrial conduction is present during ventricular pacing, the earliest retrograde atrial activity is recorded in the His bundle electrogram followed by the RA and coronary sinus recordings.
Abnormal or eccentric sequences of retrograde atrial activation occur in the presence of AV accessory pathways. This is discussed in more detail in subsequent sections dealing with supraventricular tachycardia and catheter ablation.
Till next time InshaALLAH
Thank you