Embed Size (px)
Citation preview

Advance Care Planning:
Do we respect patient
choices at the end of life?
Assoc Prof W Silvester
Director, Respecting Patient Choices Program
Intensive Care Specialist



What is advance care planning?
… ‘a process, whereby a patient, in consultation with health care providers, family members and important others, makes decisions about his or her future health care, should he/she become incapable of participating in medical treatment decisions’.
P Singer et al 1996
Ethical principles - autonomy - informed consent
- dignity - prevent suffering
Case study of Patient AG
Patient Background
81yo man lives with wife, diagnosed with lung fibrosis in July 2004,
and treated with steroids and oxygen. Poor response to treatment
with increasing breathlessness, and increasing oxygen
requirements.
Respecting Patient Choices
RPC was introduced.
• At his initial contact in July 2004 he declined.
• In January 2005 he was approached again, and he was able to state
some of his wishes, including:
• Not for intubation
• Not for ICU and other aggressive management

AG Continued …..
• He discussed his wishes with his GP, and these were documented
on the discussion card, but he did not complete a MEPOA (was in
process of doing this) or SOC.
• He subsequently became acutely breathless at home and asked his
wife to ring GP, not ambulance (as he would have previously done).
• His GP attended him and provided comfort care at home and he
died.

RPC: building the evidence

Randomised controlled trial
• English speaking, competent patients aged ≥ 80YO,
admitted to hospital
• Intervention – ACP using the RPC model
• Primary outcome
• compliance with patients EOL wishes
• Wishes known & respected
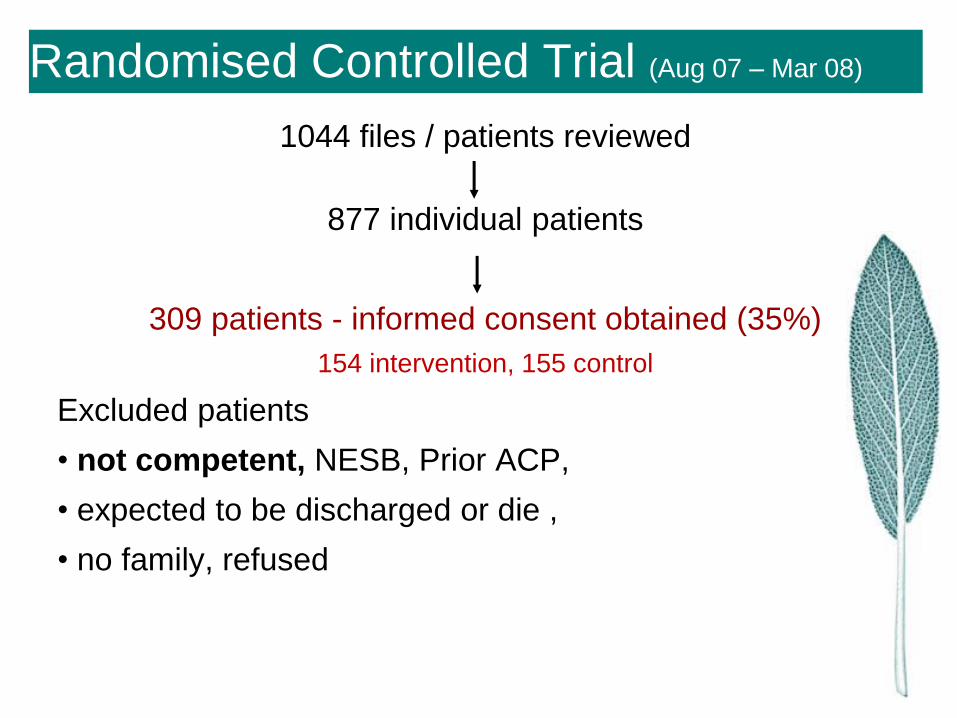
Randomised Controlled Trial (Aug 07 – Mar 08)
1044 files / patients reviewed
877 individual patients
309 patients - informed consent obtained (35%)
154 intervention, 155 control
Excluded patients
• not competent, NESB, Prior ACP,
• expected to be discharged or die ,
• no family, refused

Deceased patients
• 56 patients (18%) died within 6 months
• 29 intervention, 27 control patients
• Patient’s wishes known and respected
• Intervention 86%
• Control 30% p < 0.001
• No difference in mortality between groups

Impact of death on surviving relatives
• Death of a relative can cause significant anxiety,
depression and post-traumatic stress
– Azoulay E, et al. Am J Resp CCM2005;171:987-94
– Lautrette A, et al. N Engl J Med 2007;356:469-78
– Wright AA, et al. JAMA 2008;300:1665-73.
• How do you quantify the impact?
– IES: Impact of Event Score
– HADS: Hospital Anxiety & Depression Score

Deceased patients (56 patients)
Intervention Control P value
IES score: median, IQR 5, 2-5.5 15, 5-21 <0.001
Number of people with IES > 30 0 4 0.03
HADS depression: median, IQR 0, 0-1.5 5, 0-9 <0.001
Number of people with HADS –
depression > 8 0 8 0.002
HADS anxiety: median, IQR 0, 0-3.5 3, 0-6 0.03
Number of people with HADS –
anxiety > 8 0 5 0.02
FM’s satisfaction with the quality
of death
Very satisfied: n, %
Satisfied: n, %
Not satisfied, n. %
24, 82.8%
2, 6.9%
3, 10.3%
13, 48.1%
8, 29.6%
6, 22.2%
0.02
FM’s perception of patient’s
satisfaction with the quality of
death
Very satisfied: n, %
Satisfied: n, %
Not satisfied, n. %
25, 86.2%
1, 3.4%
3, 10.3%
10, 37.0%
10, 37.0%
7, 25.9%
<0.001

Deceased patients (56 patients)
Intervention Control P value
IES score: median, IQR 5, 2-5.5 15, 5-21 <0.001
Number of people with IES > 30 0 4 0.03
HADS depression: median, IQR 0, 0-1.5 5, 0-9 <0.001
Number of people with HADS –
depression > 8 0 8 0.002
HADS anxiety: median, IQR 0, 0-3.5 3, 0-6 0.03
Number of people with HADS –
anxiety > 8 0 5 0.02
FM’s satisfaction with the quality
of death
Very satisfied: n, %
Satisfied: n, %
Not satisfied, n. %
24, 82.8%
2, 6.9%
3, 10.3%
13, 48.1%
8, 29.6%
6, 22.2%
0.02
FM’s perception of patient’s
satisfaction with the quality of
death
Very satisfied: n, %
Satisfied: n, %
Not satisfied, n. %
25, 86.2%
1, 3.4%
3, 10.3%
10, 37.0%
10, 37.0%
7, 25.9%
<0.001

Deceased patients (56 patients)
Intervention Control P value
IES score: median, IQR 5, 2-5.5 15, 5-21 <0.001
Number of people with IES > 30 0 4 0.03
HADS depression: median, IQR 0, 0-1.5 5, 0-9 <0.001
Number of people with HADS –
depression > 8 0 8 0.002
HADS anxiety: median, IQR 0, 0-3.5 3, 0-6 0.03
Number of people with HADS –
anxiety > 8 0 5 0.02
FM’s satisfaction with the quality
of death
Very satisfied: n, %
Satisfied: n, %
Not satisfied, n. %
24, 82.8%
2, 6.9%
3, 10.3%
13, 48.1%
8, 29.6%
6, 22.2%
0.02
FM’s perception of patient’s
satisfaction with the quality of
death
Very satisfied: n, %
Satisfied: n, %
Not satisfied, n. %
25, 86.2%
1, 3.4%
3, 10.3%
10, 37.0%
10, 37.0%
7, 25.9%
<0.001

Deceased patients (56 patients)
Intervention Control P value
IES score: median, IQR 5, 2-5.5 15, 5-21 <0.001
Number of people with IES > 30 0 4 0.03
HADS depression: median, IQR 0, 0-1.5 5, 0-9 <0.001
Number of people with HADS –
depression > 8 0 8 0.002
HADS anxiety: median, IQR 0, 0-3.5 3, 0-6 0.03
Number of people with HADS –
anxiety > 8 0 5 0.02
FM’s satisfaction with the quality
of death
Very satisfied: n, %
Satisfied: n, %
Not satisfied, n. %
24, 82.8%
2, 6.9%
3, 10.3%
13, 48.1%
8, 29.6%
6, 22.2%
0.02
FM’s perception of patient’s
satisfaction with the quality of
death
Very satisfied: n, %
Satisfied: n, %
Not satisfied, n. %
25, 86.2%
1, 3.4%
3, 10.3%
10, 37.0%
10, 37.0%
7, 25.9%
<0.001

Patient / family feedback
• Discharge questionnaire
• Control patients- negative comments
• the doctors don’t listen
• I felt ignored and in the way
• They don’t want me as I am too old
• They wouldn’t speak to me, and kept discussing
things with my family

Survey of family of deceased patient
Intervention group
• He had a very peaceful death, just as it should have been, & I would like to thank all staff for this.
• Even though we already knew what he wanted it was great to be able to talk about it so openly.
_____________________________________________
Control group
• Mum didn’t want heroics. I was horrified to hear she received 45 minutes of CPR. She didn’t want it. All anyone had to do was ask.
• The doctors kept asking if dad should be resuscitated. I didn’t think they should keep asking, as they also told us it wouldn’t help him. It was obvious to us he was dying.

Benefits of ACP
• ACP improves EOL care and patient satisfaction
• Empowers the patient NOW, not just in the future
• ACP assists family to:
1. know patient wishes, be involved in ACP discussions
• More able to make decisions
• Less burdened
2. Have less risk of stress, anxiety and depression
3. Be more satisfied with quality of patient’s death

• Test the hypothesis that changing the terminology from
the negative “Do Not Resuscitate”
to the positive “Allow Natural Death”
• J Med Ethics 2008

Advance care planning
• Works with people with dementia
– “best interests” test
• Is not euthanasia
– Steers people away from euthanasia
• Is more about withholding future treatment than
withdrawing treatment now
• Aligned with Catholic Healthcare Code of Ethics

Is ACP nationally supported?
National Health and Hospitals Reform Commission, 2010 -
advance care planning should be an integral component of
planning for the care of older persons in Residential Aged Care
Facilities. (Recommendations 51 and 57).
Productivity Commission: Caring for Older Australians,
July 2011, - further impetus for inclusion of advance care
planning into normal practice in aged care (Recommendations
10.1 to 10.4).
Australian Human Rights Commission-
“Respect and Choice- A human rights approach for ageing and
health” - Section 3.2 Advance care planning
National Palliative Care Strategy.
National Primary Care Strategy

National Standards Standard 1: Governance
1.18.4 Patients and carers are supported to
document clear advance care directives and/
or treatment limiting orders
ACP information is available
for patients
• Austin Health specific patient information
brochures
• available English, Greek and Italian
• patient information packs
• included on the Austin Health intranet and
internet sites.

Education & training of staff in
ACP & EOLC
• in orientation programs- nurses and doctors
• e-learning modules are accessible via the intranet
• one day workshop
• postgraduate nursing courses
• Training to Allied Health
• at grand rounds and ward in-services
• to the community through a trained volunteer program,
• Junior doctors- principles & communication EOLC
• Fifth year medical students

Auditing practice
• Mortality & morbidity audit to ensure that treatment
received reflects patient’s wishes
• assess the quality and content of the Medical Enduring
Power of Attorney (MEPOA)
– As a result a form to document MEPOA for patients who
can’t sign.
• CALD patients who complete advance care plans.
– interpreters have been trained in ACP processes and
communication and a targeted strategy for CALD patients
– significant increase in number of CALD patients
• ACP activity, frequency of ACDs & RPs
• quality of the completion of ACPs

Standard 9: Recognising and
Responding to Acute Deterioration
9.8.1 A system is in place for preparing and-or
receiving advance care plans in partnership
with patients, families and carers.
9.8.2 Advance Care plans and other treatment –
limiting orders are documented in the patient
clinical record
Appropriate policies
• Life Prolonging Treatment Policy
• Advance Care Planning Policy
• both outline the framework for the process of
limiting treatment and advance care planning at
Austin Health.
• These policies include how patients, families
and their carers are involved in the processes.
Appropriate documentation
• To document medical treatment wishes
• doctor generated - the Resuscitation Plan
• patient generated documents
–Medical Enduring Power of Attorney
–Refusal of Treatment Certificate
–Advance Care Plans or Directives


Decision Making Framework for Resuscitation Plan
LPT OFFERED
Doctor determines that it is medically
indicated to offer treatment
Is proposed life prolonging
treatment (LPT) medically indicated? 1
LPT NOT OFFERED
Doctor determines that treatment is
not medically indicated
Patient is
competent
Inform patient
of decision2
(and family4 as
appropriate)
7
Patient is
competent3 Patient is not competent
Able to consult with family4
regarding previous
expressed wishes &
family’s views?7 Complete Resuscitation Plan
reflecting medical decisions
The patient has an
advance care plan
or MEPOA
Seek Further Advice5
The patient has no
advance care plan
and no MEPOA
NO YES
Patient is not
competent
Inform family4
of the decision2
7
Complete Resuscitation Plan
reflecting patient’s wishes
YES NO
Discuss6 with
MEPOA / family4 7
Discuss with
patient 7

Where are the documents held?
• filed in the legal (front) section of the inpatient
history
• stored within the legal section of the Scanned
Medical Record (SMR).

Electronic Alerts?
An alert is placed within Cerner.
• prompts staff to the presence of ACP or RP
• easy to see urgently if required
• when patient presents to ED
• automatically printed out on the daily ward lists
• alerts ACP clinicians- targeted service provision

Resuscitation Status Order
Ordered, Modified, Ceased on the same Order
Profile screen as Path, Imaging, etc

Order Profile View
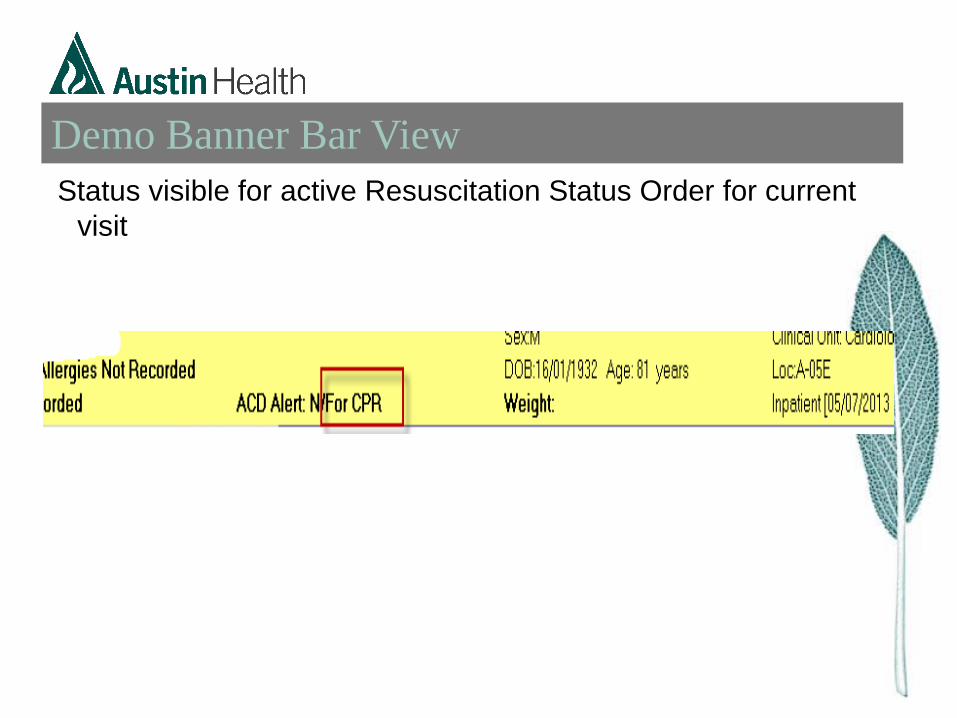
Demo Banner Bar View
Status visible for active Resuscitation Status Order for current
visit

Policy + electronic alerts catalyse
change in medical practice
A doctor must complete a RP in any patient who:
• is > 75 yrs
• has advanced cancer or advanced dementia
• advanced cardiac or respiratory disease
• is dialysis dependent + septic or vascular co-morbidities
• has requested Not For Resuscitation on their ACP
• has a previous RP or a Refusal of Treatment Certificate

What has auditing shown?
Electronic alerts have avoided:
• inappropriate resuscitation in multiple patients
who either requested NFR or were not
appropriate for CPR
• significantly reduced inappropriate MET calls.