Embed Size (px)
Citation preview
ENDOMETRIOSIS
By Caroline Karunya Ponnarasi Kanagaraj
Group-IV
Introduction
one of the most common diseases but it is also one of the least understood
endo=within, metri= uterus (womb), osis=condition
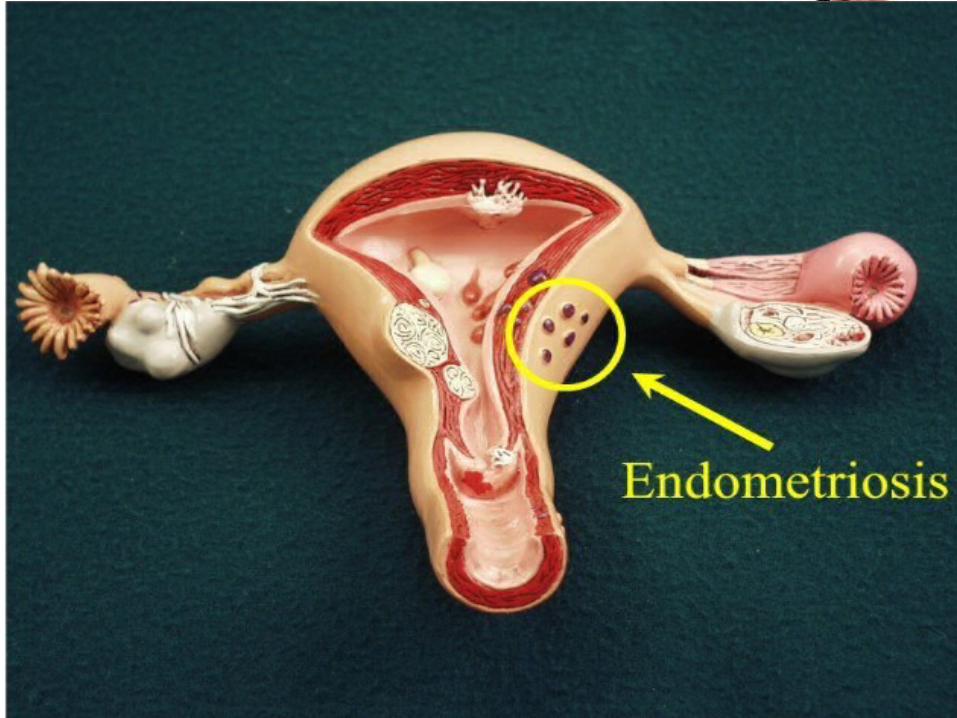
The presence of functioning endometrium(glands and stroma) in sites other
than uterine mucosa is called endometriosis.
These ectopic endometrial tissues may be found in the myometrium then it is
called endometriosis interna or adenomyosis.
More commonly these tissues are found at sites other than uterus then it is
called as endometriosis externa or generally referred to as endometriosis.
endometriosis is not cancer and there is no cure for it

PREVALANCE
found in 12-15 % of women (5 million women in the US).
21-47% of infertility cases
primarily found in women during their child-bearing years
common among adolescents
Severe disease may occur in families
More in women whose first degree relative have the disease
Exposure to ovarian hormones appears to be essential
No known racial or socioeconomic predilection
Often diagnosed incidentally
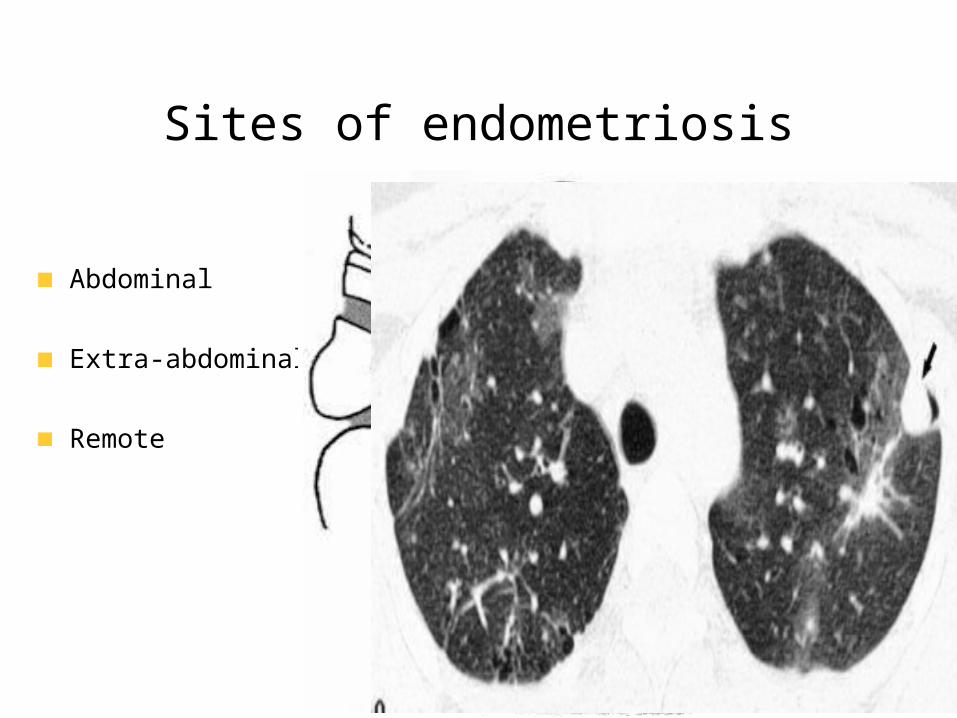
Sites of endometriosis
Abdominal
Extra-abdominal
Remote

PATHOGENESISSampson's theory:
Retrograde menses and peritoneal implantation
Most women retrograde menstruate
Meyer's theory:
Coelomic metaplasia
Low incidence of pleural disease
Halban's theory:
Hematogenous or lymphatic spread to distant tissues
Does not explain gravity dependent disease sites
Immunogenic defect

PATHOLOGY
These ectopic foci respond to cyclic hormonal fluctuations in much the same way as intrauterine endometrium, with proliferation, secretory activity, and cyclic sloughing of menstrual material. The products of this metabolic activity, including the concentrated and cyclic release of cytokines and prostaglandins, lead to an altered inflammatory response characterized by neovascularization and fibrosis formation. Some investigators have been able to demonstrate abnormal T- and B-cell function, abnormal complement deposition, and altered interleukin (IL)-6 production in women with this disease.
PATHOLOGYIf it happens to occur on the pelvic peritoneum, it provides adhesions and puckering of the peritoneum
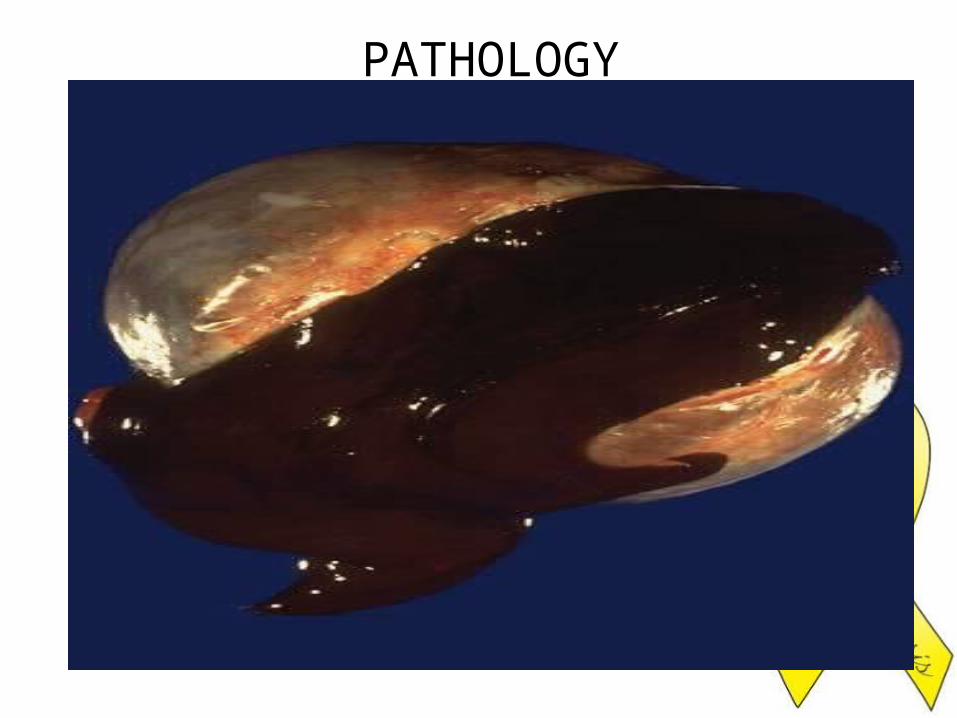
Endometriomao If encysted the cyst enlarges with cyclic bleeding and the content inside
becomes chocolate coloredo Contains blood, fluid & menstrual debriso Hence the cyst is called chocolate cyst which is commonly located in
the ovary.o Brown to black color due to Hemosiderino Chocolate cyst may also be due to hemorrhagic follicular or corpus
luteum cyst or bleeding in to a cyst adenoma. for this reason, the term endometrial cyst or endometrioma is preferred to chocolate cyst

PELVIC ENDOMETRIOSISTypically there are small black dots, the so called ‘power burns’
seen on the uterosacral ligaments and pouch of douglas.
Fibrosis and scarring in the peritoneum surrounding the implants is
also a typical finding
Other subtle apperances:
Red flame shaped areas
Red polypoid areas
Yellow brown patches
White peritoneal areas
Circular peritoneal defects.
Symptoms
According to siteNo relation between extent of the disease and severity of the symptomsFemale reproductive tract:o Dysmenorrheao Lower abdominal and pelvic paino Dyspareuniao Accident to endometriotic cysto Low back paino Infertilityo Menstrual irregularity .
Urinary tract:o Cyclical haematuria / dysuriao Ureteric obstruction
Gastrointestinal tract:o Dyscheziao Cyclical rectal bleedingo Intestinal obstruction
Lungso Cyclical hemoptysiso Blood stained Pleural effusionso Catamenial Pneumothorax

DiagonosisSerum CA 125
Sensitivity 28% & specificity 90% Not useful for screening, because of poor sensitivityCan be used to identify a sub-group of women who are likely to benefit from early laparoscopy & to follow the progress of disease after establishing the diagnosis
Ultrasound:Sensitivity for focal endometrial implants is poor
CT scanEndometriomas may appear solid, cystic or mixedBecause of poor specificity & high radiation, CT has been replaced by MRI
MRIRole is limited in visualizing small endometriotic implants and adhesionsMore useful for lesions in extraperitoneal locations & the contents of pelvic massMore frequently used in staging & treatment response monitoring
Direct visualization of the lesionLaparascopyLaparatomy
Histopathology to confirm the diagnosis
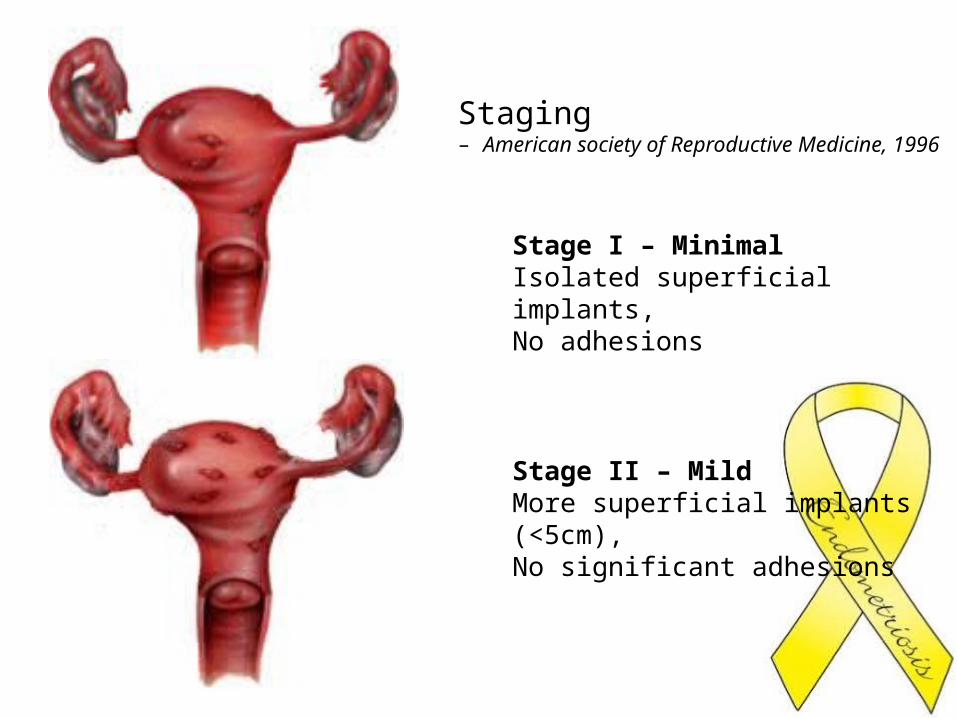
Staging – American society of Reproductive Medicine, 1996
Stage I – Minimal Isolated superficial implants,No adhesions
Stage II – MildMore superficial implants (<5cm), No significant adhesions
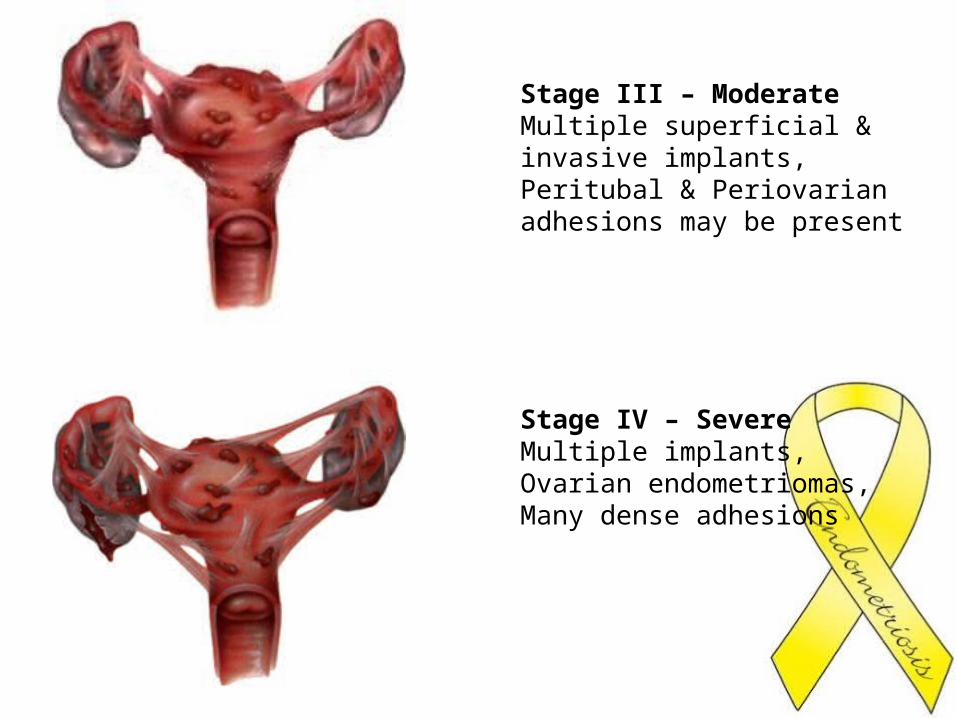
Stage III – ModerateMultiple superficial & invasive implants,Peritubal & Periovarian adhesions may be present
Stage IV – SevereMultiple implants,Ovarian endometriomas,Many dense adhesions

TreatmentConsider
AgeSymptomsStageInfertility
Recognize Goals: Pain ManagementPreservation / Restoration of Fertility
Discuss with Patient:Disease may be Chronic and Not CurableOptimal Treatment Unproven or Nonexistent
Lines of management
Expectant
Medical
Hormonal
Surgical
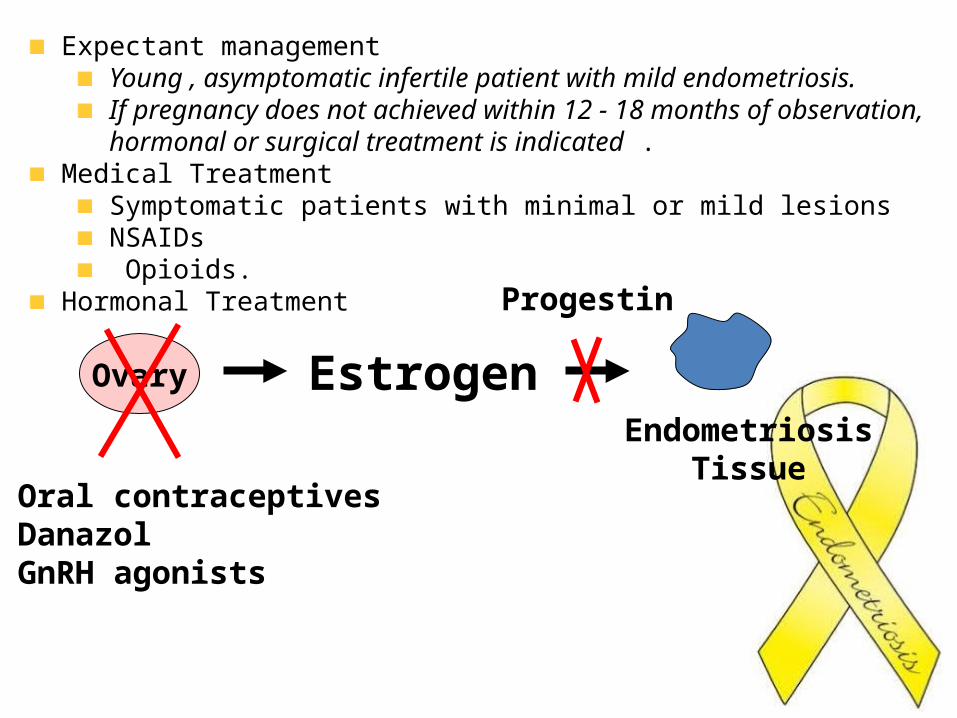
Expectant managementYoung , asymptomatic infertile patient with mild endometriosis.If pregnancy does not achieved within 12 - 18 months of observation, hormonal or surgical treatment is indicated .
Medical TreatmentSymptomatic patients with minimal or mild lesionsNSAIDs Opioids.
Hormonal Treatment
Ovary EstrogenEndometriosis
Tissue
Progestin
Oral contraceptivesDanazolGnRH agonists
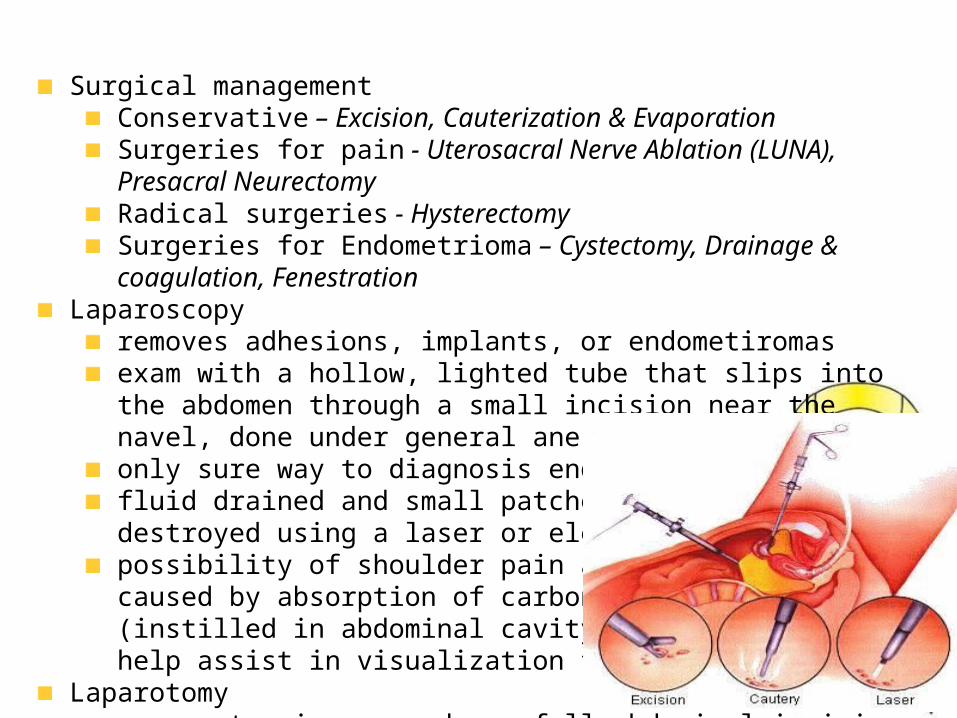
Surgical managementConservative – Excision, Cauterization & EvaporationSurgeries for pain - Uterosacral Nerve Ablation (LUNA), Presacral NeurectomyRadical surgeries - Hysterectomy Surgeries for Endometrioma – Cystectomy, Drainage & coagulation, Fenestration
Laparoscopyremoves adhesions, implants, or endometiromasexam with a hollow, lighted tube that slips into the abdomen through a small incision near the navel, done under general anesthesia only sure way to diagnosis endometriosisfluid drained and small patches of endometriosis destroyed using a laser or electrical currentpossibility of shoulder pain after operation, caused by absorption of carbon dioxide gas (instilled in abdominal cavity during surgery to help assist in visualization for the surgeon)
Laparotomymore extensive procedure, full abdominal incision, longer recovery period (4-6 weeks)purpose: perform delicate microscopic surgery
This March marks the 15th annual health awareness month recognition of Endometriosis Awareness Month.
Conclusion
• Endometriosis is a mystery tour as it requires decision making at every stage by the physician and the patient.
• Endometriosis still stand as one of the most-investigated disorders in gynecology. So is one of the highest priorities for research.