Embed Size (px)
Citation preview

Dr. John Mew Dr. María José Muñoz
Dr. Antonio Facal
Dr. Eduardo Padrós SerratDr. Javier Plaza
Dr. Barry RaphaelDr. Juan Font Dr. Sandra Kahn
Dr. José Luis Gandía
Universidad de Valencia


Showing off the castle
Papa John
150 mostly young orthodontists

John Sandra Me (awake)

The Tropic PremiseIf the teeth are lightly in contact with the lips sealed and the tongue on the palate for between 4-8 hours a day, the face will grow properly with room for 32 teeth.

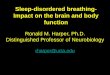
1)The Forehead2) The upper indicator line3) The lower indicator line4) The cheek line5) Muscle bulges
Orbicularis Oris: gets big by sucking on the teethMentalis: bulges and throws the lower lip forwardBuccinators : gets big by sucking on tongue
6) Nasal size and contour.7) The shape of the lips: They will regain size8) Lip posture at rest and seal9) Tongue posture: The main force that drives maxillary growth
Reading the Face

• Okay boys, it's happened... I was at a meeting this weekend with three dentists who were at the AARD meeting. One of them mentioned Mark and Kev and also Tom Colquitt who spoke about his own health/airway journey. Another one said he had "heard about this Raphael guy" who was in nj and they were thinking of having him speak to their small group. Another brought up a patient/friend who he thinks has an airway problem. They asked about Myo and appliances and the next step. So cool because the three of them are Kois trained dentists at the top of their field and they were clueless about airway and risk factors, BUT they were curious!
• I spent two days promoting the airway and the ALF programs. This is what we have hoped will happen - that practitioners start understanding the problem and are curious about how to solve it.
• BTW, the course I was at was a leadership conference (Kev - it was Fritz's group) and there was a lot of talk about creating a vision. Perhaps it would be worthwhile for us to craft a vision about what we hope for. Seems a bit hokey but it helps to define what we envision as the successful result of our endeavors. Maybe you already have a written vision and I'm just an interloper. But if not, perhaps as a group (get the tribal think tank in as well) we could talk about what our vision is? Perhaps this is the goal of of the white paper event at AAPMD?
Email from a friend…

• The anthropologic standard
• The modern environment is a stressor
• Our compensations create the symptoms
• Symptom management hides (ignores) these causes
The Four Premises

Basic Orthodoxies of Orthodontics
• Malocclusion is the Problem
• Genetics is THE etiology
• Shape of the face is a characteristic
• Our scope is the teeth and jaws

• Malocclusion is a symptom
• Soft Tissue as THE etiology
• Facial shape becomes a risk factor
• The Child attached to the teeth
My Paradigm Shift in Orthodontics

Setting up Research Protocols

Relationship between occlusal findings and orofacial myofunctional status in
primary and mixed dentition
Jana Seemann, Gunther Kunst, Franka Stahl de CastrillonDept of Orthodontics, U of Rostock, Germany
Part I: Prevalence of malocclusions
Part II: Prevalence of orofacial dysfunctions Part III: Interrelation between Malocclusions and orofacial dysfunctions
Part IV: Interrelation between space conditions and orofacial dysfunctions