Embed Size (px)
Citation preview

Epidemiology and Vaccines
BR SinghHead Division of Epidemiology
Indian Veterinary Research Institute, Izatnagar

Disease control?
• Can we control/ prevent/ eradicate a disease?
• How can we achieve this goal:
– Epidemiological interventions-Modulation of Host, agent and environmental determinants
– Vaccine

Vaccine
• Epidemiological parameters to think about vaccine use:
– Aetiology
– σ
– Herd immunity-
• Vaccine type,
• Vaccine efficacy
• Vaccine administration
• Duration of immunity conferred etc.

Aetiology
• Infectious/non infectious
• Physiological/ non-physiological
• Nature of infectious agent
• Antigenic structure

σ /R0 Values
The average number of secondary cases arising from an average primary case in an entirely
susceptible population.In epidemiology, the basic reproduction
number (sometimes called basic reproductive rate, basic reproductive ratio and denoted R0, r
nought) of an infection is the number of cases one case generates on average over the course of its
infectious periodHigher the r0 more difficult is to control the
disease.

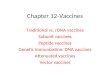
Infectious disease Host R0Measles Humans (UK) 16-18Pertussis (whooping cough) Humans (UK) 16-18Chickenpox (varicella) Humans (UK) 10-12Rubella Humans (UK) 6-7Smallpox Humans 3.5-6Feline immunodeficiency virus
(FIV) Domestic cats 1.1-1.5Rabies Dogs (Kenya) 2.44Phocine distemper Seals 2-3Tuberculosis Cattle 2.6Influenza Humans 3-4Foot-and-mouth disease Livestock farms (UK) 3.5-4.5Mumps Humans 12Poliomyelitis (polio) Humans 5HIV Male homosexuals UK 4HIV Female prostitutes in Kenya 11Malaria Humans ≈ 100
Source: Keeling and Rohani (2008)

Ro is affected by infectiousness of agent,
latent period (period during which hosts are infected but not yet infectious) and
infectious period
Infectious disease Incubation period Latent period Infectious periodMeasles 8-13 6-9 6-7Mumps 12-26 12-18 4-8Pertussis 6-10 21-23 7-10Rubella 14-21 7-14 11-12Diphtheria 2-5 14-21 2-5Chickenpox 13-17 8-12 10-11Hepatitis B 30-80 13-17 19-22Poliomyelitis 7-12 1-3 14-20Influenza 1-3 1-3 1-3Smallpox 10-15 8-11 2-3Scarlet fever 2-3 1-2 14-21

FACTORS AFFECTING R0
It can be explained by the epidemiological triad• Host Factor: Mixed Population, different age group of
animals, difference in nutritional status, inbredpopulation, parasitic load and mobility of host.
• Environment Factor: Seasonal Variation e.gFMD(autumn and spring) and Malaria(hot and humidclimate).
• Agent Factor: The agent may not spread at the samerate in all the countries. Genetic changes in the hostfactors like Genetic drift and genetic shift. Differentstrains of Ebola (Zaire, Sudan, and Ivory Coast Ebola virus,Reston Ebola virus) and different strains of HIV, Influenzaviruses, Different serovars of E. coli and Salmonella.

HOW TO REDUCE R0 VALUE
It can be done at any point in the transmission cycle by the following methods:
Reducing or eliminating the shedding of the agent bythe infected host. e.g by antibiotics and segregationand quarantine.
Reducing the duration of environmental survival ofthe agent. e.g sunlight.
Reducing or eliminating vehicle contamination andfomite transmission.
Controlling the Vector Population for biologicaltransmission.
Reducing the exposure of susceptible host. E.gdensity reduction.
Increasing the resistance of susceptible host byvaccination.

R0 and Vaccination
• R0= β/ γ
• β=transmission rate (Number contacts by infective case in defined time, contact rate)
• γ= 1/ average infectious period
• 1- 1/R0 is the fraction of the population to be vaccinated for getting herd immunity.

Disease Elimination and R0
• If the herd effect reduces the risk of infectionamong the uninfected sufficiently then theinfection may no longer be sustainable within thepopulation and the infection may be eliminated.
• The “effective reproduction number” (R) has tobe reduced below 1.
• If a proportion P of the population are immunethen R = (1- P) R0
So, to get R down to about 1, P must be up to1-1/ R0
Thus if R0 = 5 then vaccine coverage will have to bein excess of 80%

Heard Immunity
Herd Immunity can be defined as follows:
1. The resistance of a group for attack by a diseasebecause of the immunity of a large proportion of themembers and the consequent lessening of thelikelihood of an affected individual coming intocontact with a susceptible individual.
2. The prevalence of immunity in a population abovewhich it becomes difficult for the organism to circulateand reach new susceptible is called herd immunity.
3. It is well known that not everyone in a populationneeds to be immunised to eliminate disease.

Types of Herd Immunity
• Innate (Inherent) Herd Immunity: It isgenetically determined physiological changeswith respect to antibody production or otherdefence mechanism in a herd. It does notdepend on the previous exposure of herdwith infection or it may arise in a herdthrough prolonged exposure to an infectionor natural selection. Similar to emergence ofMDR pathogens.

• Some population of domestic fowl haveinnate resistance to pullorum disease due toan inherited difference in lymphocytenumbers immediately after hatching.(Robert& Card,1926)
• Inheritance of resistance to influenza virus inmice is probably due to a single dominantautosomal allele. (Lindermann, 1964)
• Cameroon et al., have shown that resistanceto brucellosis in swine may be geneticallydetermined.

• Acquired Herd Immunity: It is a type ofherd immunity where a sufficient numberof its members have actually beenexposed naturally or artificially toinfectious agents during their lifespan.
• This kind of exposure may be made veryearly in life.
• Vaccination


Advantages of Herd ImmunityBeneficial effects
Potential for infection elimination.
Reduced risk of infection for those refusingvaccination (“free riders”).
Reduced risk of infection for those for whomvaccination is contraindicated (e.g. immune-suppressed) or who cannot be vaccinated e.gcancer patients, too young animals andpregnant animals.

LimitationsHerd immunity generally applies only to
diseases that are contagious. It does not apply to diseases such as tetanus, botulism food borne infections and intoxications.
Raise the average age of infection amongthose who are infectedParticular problem for those infectionswhere the severity of infection increaseswith age (e.g. polio, rubella, varicella,measles, hepatitis A)

Reasons of vaccination failure
• Non-understanding epidemiology of the disease in the vaccinationation area leading to poor planning (host factors, carriers, multiplier hosts, intermediate hosts etc., agent factors viz., strains, virulence, contagiousness etc.).
• Non-implementation or poor implementation of the programme.
• Vaccine quality• Infection load• Hygiene and veterinary care.• Environmental, social and economic factors

Conclusions
• Even before thinking of developing a vaccine one should understand epidemiology of the Disease.
• While developing the vaccine one should test it on the principles of Epidemiology.
• Vaccination programmes should be formulated by trained epidemiologists.