Embed Size (px)
Citation preview

By
Magdy Abdelrahman Mohamed
2017

It is an incision of the perineum during labour.

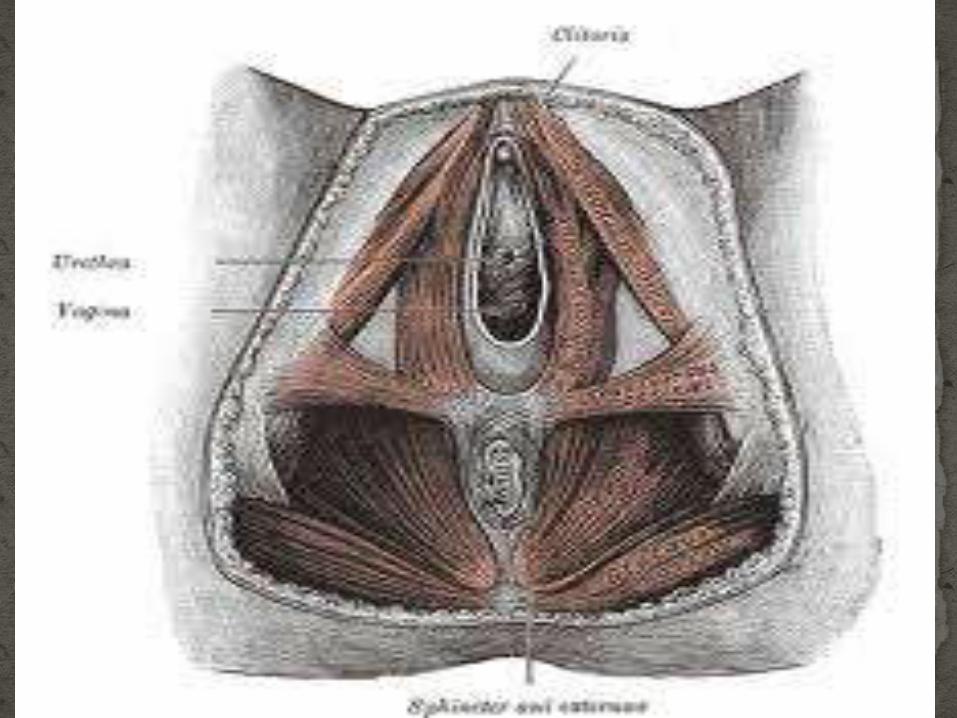
It is a pyramidal shaped area betweenthe lower vagina and the anal canal andthe lower end of the rectum.


Avoid irregular tears.
Avoid fetal intracranial hemorrhage.

Absolute:Preterm labour.
Breech presentation.
During forceps application.

Relative:
Primipara.
Scarred perineum
Rigid perineum.
Narrow subpubic angle.
Shoulder dystocia.
Malposition.

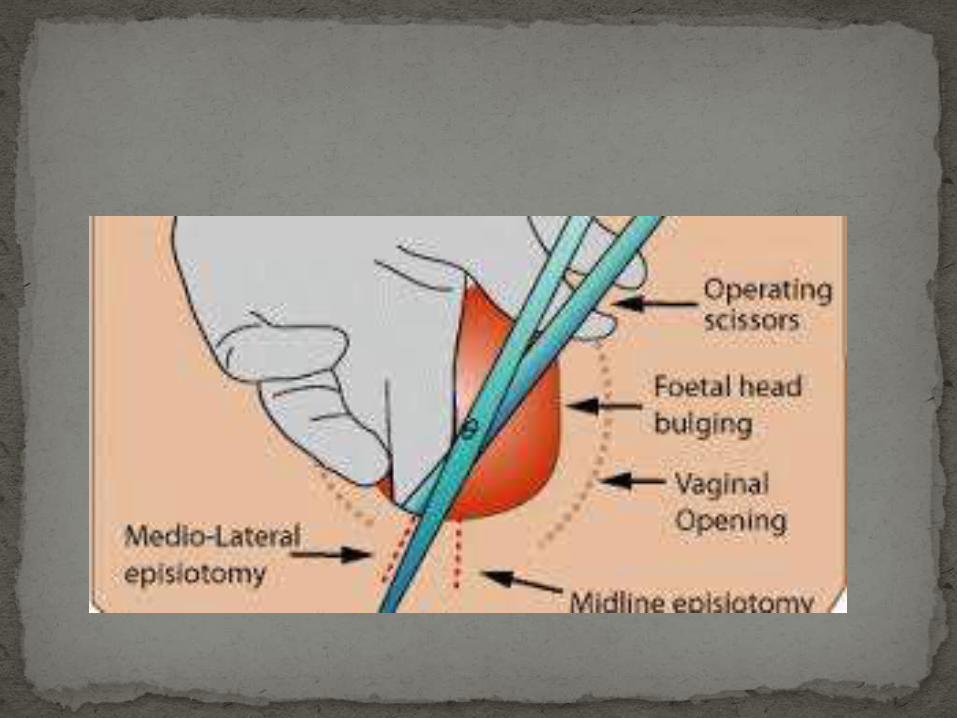
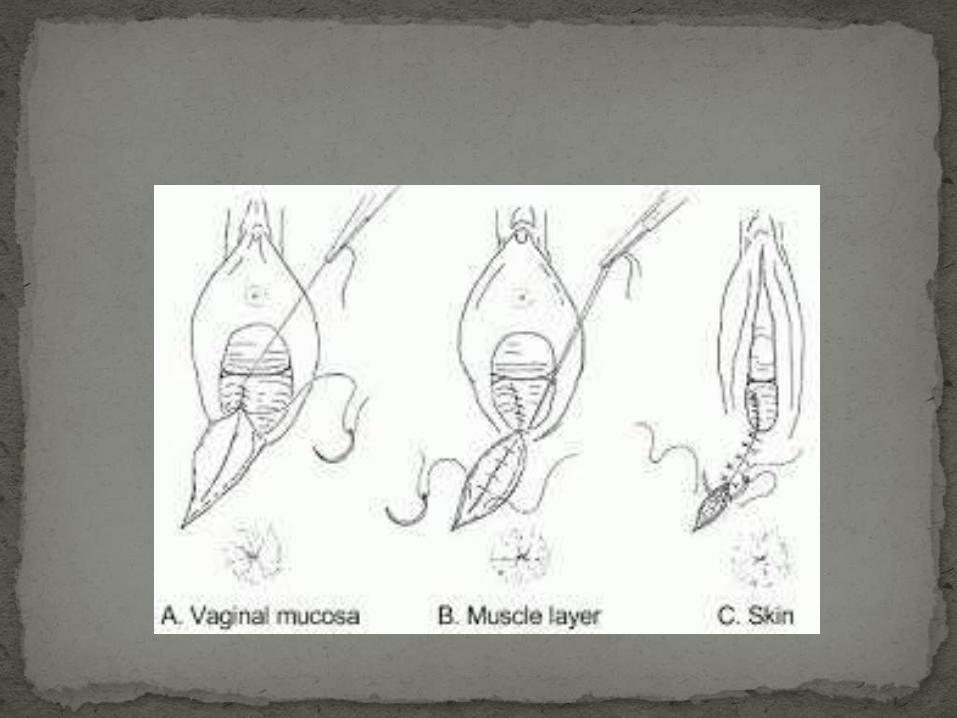
Median ( midline) episiotomy:
Mediolateral episiotomy:
J shaped episiotomy:

Timing.
Local anesthesia.
Repair.

Hematoma.
Abscess formation.
Infection and gapped wound.


It is replacement the presenting part by anotherone.
If the aim is to make the head the presenting partit is called cephalic version and if the breech willbe the presenting part it is podalic version.
External cephalic version.
Internal podalic version.

Indications
* Breech presentation.
* Transverse or oblique lie.

Timing:
Preferred after 36w till onset of labour.

Prerequisites :
1. Facilities for monitoring. US: FHR visualisation
CTG: before & after procedure
2. Facilities for immediate delivery .
3. Anti-D immunoglobulin to rhesus-negative.
4. Informed consent.

Contraindications:
CS is indicated.
Antepartum haemorrhage within the last 7days.
Abnormal CTG.
Major uterine anomaly.
Ruptured membranes.
Multiple pregnancy.

Technique:
No anaesthesia as the pain is a safe guard againstrough manipulations.
The patient evacuates her bladder.
She lies in a Trendelenburg position with exposedvulva to detect any vaginal bleeding.
The fetal position is determined and FHS isauscultated.

Technique:
One hand is applied externally to the fetalhead and the other on its buttock.
The two poles are approximated to flex thefetus and rotation is done by the two handssimultaneously to bring the head lowerdown.

If neither vaginal bleeding nor fetal distressresults, an abdominal binder is applied to fix thenew position and re-examined twice weekly.
If the original presentation returned again, theprocedure of version can be repeated.
Some doctors prefer to induce labour immediatelyafter successful version.

Complications:
Placental separation.
Rupture of membrane.
Fetal distress.
Indications:
Retained second twin in a transverse lie.

Pre-requisites:
General anaesthesia.
Evacuation of the bladder.
Complete aseptic conditions.
Cervix is fully dilated.
No previous uterine scar.
Adequate amniotic fluid.


Complications:
Neurogenic shock
Rupture uterus.
Puerperal sepsis.

HISTORICAL

Craniotomy.
Decapitation.
Evisceration.
Cleidotomy: division one or both calvicle