Embed Size (px)
Citation preview
EPILEPSY
August 10, 2013 SSG 1
August 10, 2013 SSG 2
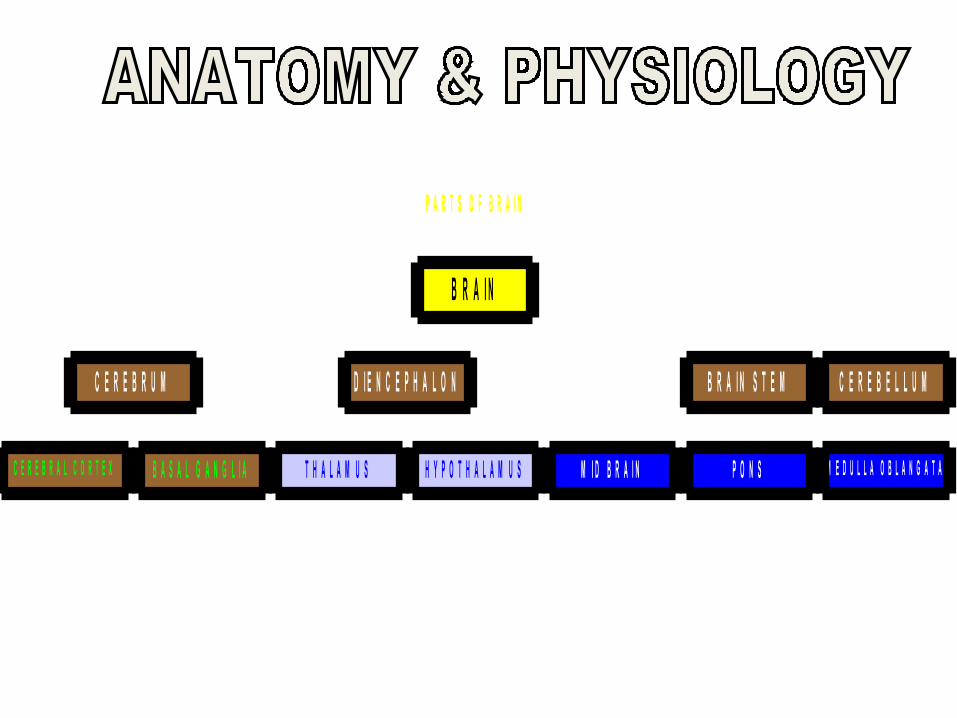
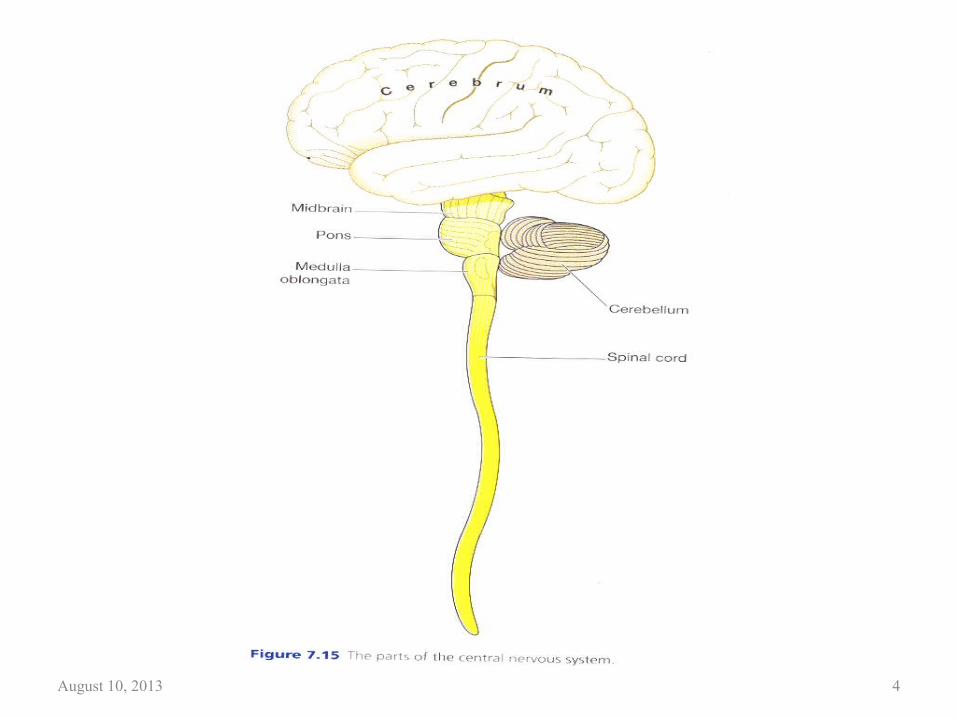
P A R T S O F B R A I N
C E R E B R A L C O R T E X B A S A L G A N G L I A
C E R E B R U M
T H A L A M U S H Y P O T H A L A M U S
D I E N C E P H A L O N
M I D B R A I N P O N S M E D U L L A O B L A N G A T A
B R A I N S T E M C E R E B E L L U M
B R A I N
August 10, 2013 CNE 3
August 10, 2013 CNE 4
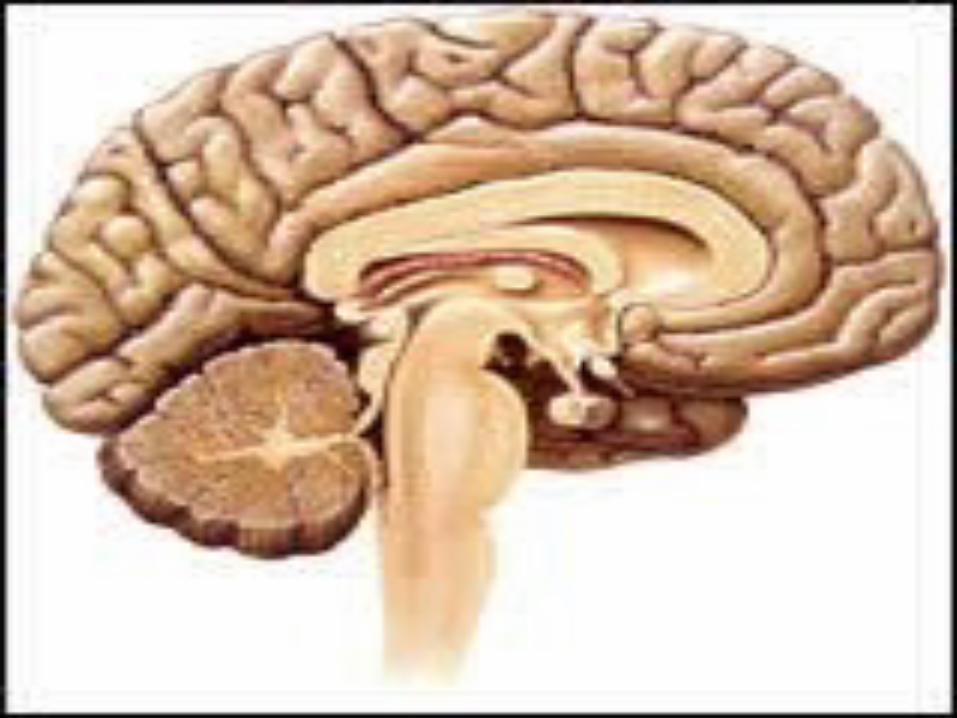
@ CEREBRUM (two hemisphere) A. FUNCTION
1. Highest level of functioning.
2. Governs all sensory and motor activity, thought and learning.
3. Analyzes, associates, integrates and stores information.
August 10, 2013 SSG 5
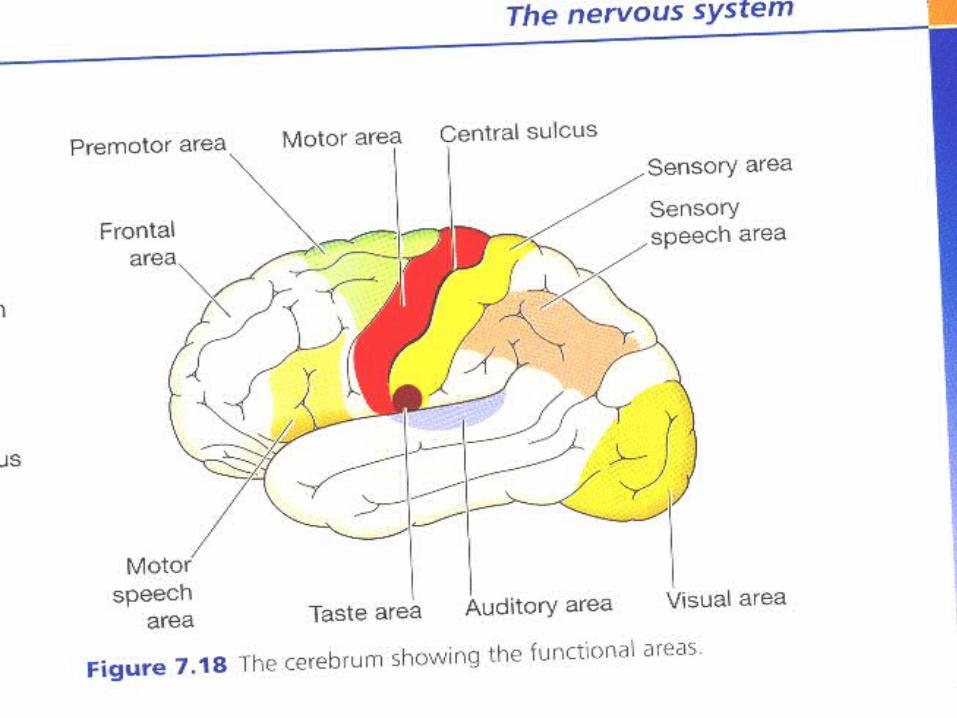
@ Cerebral Cortex (outer gray layer) divided into four major lobes:1. FRONTAL * Precentral gyrus-motor function * Broca s area –motor speech area * Prefrontal-controls morals,values and judgments2. PARIETAL * Post central gyrus-integrates general sensation * Interprets pain,touch,temp. and pressure * Governs discriminations3. TEMPORAL * Auditory center * Wernicke”s area-sensory speech center4. OCCIPITAL –VISUAL AREA
August 10, 2013 SSG 6
@ BASAL GANGLIA * Collections of cell bodies in white
matter * Control motor movement * Part of extra pyramidal tract
August 10, 2013 SSG 7
@. DIENCEPHALON A.THALAMUS1. Screens and relays sensory impulses to cortex2. lowest level crude conscious awareness
B.HYPOTHALAMUS-
Regulates autonomic nervous system,stress response,sleep, appetite, body temp..fld bal. and emotions.
August 10, 2013 SSG 8
@. BRAIN STEM A. Midbrain-motor coordination
B. Pons-involuntary Resp. reflexes C. Medulla oblongata-vasomotor
center
August 10, 2013 SSG 9
@.CEREBELLUM Coordinates muscle movement,
posture and muscle tone.
August 10, 2013 SSG 10
August 10, 2013 CNE 11
HOW THE BRAIN WORKS? 1. Brain is made up of billions of cells,including a
networks of cell called NEURONS,this neurons branch out ,much like branches on a tree.This neural network enables communication with in the brain and bet. The brain and the rest of the body.
2. When a neuron “fires” it sends small electrical impulses along it’s branches toward surrounding cells. At the end of each branch is a small gap or synapse,which the impulse must overcome in order to continue it’s journey.
August 10, 2013 SSG 12

3. When an impulse reaches the end of a branch, chemicals called NEUROTRANSMITTER are released to fld. the synapse.
Some are excitatory, stimulating the neighboring cell to fire ,Others are inhibitory, making the next cells less likely to fire.
August 10, 2013 CNE 13

EPILEPSY A paroxysmal disturbance in a
consciousness with autonomic sensory and or motor dysfunction ;a manifestation of excessive neuronal discharges in the brain.
August 10, 2013 SSG 14
CAUSES It can be structural,chemical or physiological or
combined causes:1. Genetic factors2. Trauma-head-brain3. Brain tumor4. Circulatory disorder (stroke, arteriovenous
malformation)5. Metabolic disorder (hypoglycemia, hypocalcaemia, abnoxia)6. Toxicity (drugs and alcohol)7. CNS infection (encephalitis, meningitis, abscess)
August 10, 2013 SSG 15
CLASSIFICATIONS:
1. Symptomatic-secondary to probable cause.
2. Idiopathic-primary epilepsy without definite known cause.
August 10, 2013 SSG 16
SEIZURE: An excessive discharge of electrical activity
within the brain,which leads to a change in movement, sensation, experience or consciousness.
The effects they have on the body vary greatly depending on where in the brain the seizures starts and where it spreads.
August 10, 2013 SSG 17
PHASES:
1. AURA- An unusual sensation or peculiar feeling often felt prior to a more widespread seizure.can also be called a simple partial seizure.
2. ICTUS- The whole seizure including the aura
3. POST ICTUS- Time after seizure;may experience muscle weakness of deep sleep.
August 10, 2013 SSG 18
SEIZURE CAN CAUSE:1. A twitching muscle2. Convulsive movements3. A tingling sensation4. Sweating 5. The perception of an unusual smell or taste6. Hallucinations7. Fear or anxiety8. Changes in awareness9. Loss of consciousness
10. Other changesAugust 10, 2013 SSG 19
TYPES:
1. GENERALIZED SEIZURES: Affects both hemispheres of the brain at the same time.abnormal activity is not focused in one specific area and there generally is no aura at the start.
August 10, 2013 SSG 20
FORMS: 1. Typical absence seizure (Petit Mal)
-Result in brief episodes of impaired awareness. There also may be small motor movements, changes in muscle tone or automatic behaviors. Most common in children.
2. Atonic / Akinetic seizures -Associated with a sudden loss of muscle tone in a limb or throughout the entire body.The person having the seizures will drop things or fall to the ground.
August 10, 2013 SSG 21
3. Myoclonic -Sudden shock like jolt to one or more muscle which increases muscle tone and causes movement. These sudden jerks are like those that occur in healthy people as fall sleep.
4. Tonic-Clonic (Grand Mal) -Begin with simultaneous loss of consciousness and the tonic phase (stiffening of the body) the person falls to the ground and often emits a loud cry as the chest muscle stiffing.Next comes the clonic phase,during which the muscles rhythmically jerk.
August 10, 2013 SSG 22

2. PARTIAL SEIZURE
- It begin in a part of one brain hemisphere, generally in the temporal or frontal lobe.
August 10, 2013 SSG 23
TYPES:
1. SIMPLE PARTIAL (aura’s)
* Is focused in a specific area of the brain.* A person remains alert and afterward is
able to remember what happened. * An aura or simple partial seizure may
constitute the entire seizure or may precede a complex partial or generalized seizure.
August 10, 2013 SSG 24
SYMPTOMS VARY ON THE AREA OF THE BRAIN:
1. Motor seizures cause a change in muscle activity and may involve jerking or stiffening of a part of the body.2. Sensory seizures may cause abnormal functions in any of the five senses.3. Autonomic seizures affect involuntary functions
and may cause a rapid heart beat or breathing rate, sweating or an unpleasant sensation in
the abdomen,chest,throat or head.4. Psychic seizures may affect perception and memory or stimulate emotions such as fear
August 10, 2013 SSG 25
2.COMPLEX PARTIAL SEIZURES:
@ Seizure accompanied by impaired consciousness and recall. @ May also involve staring,automatic behavior such as smacking chewing ,picking ,walking, grunting, repetition of word or phrases or other symptoms and signs.
August 10, 2013 SSG 26
DRUGS COMMONLY USED IN EPILEPSY:
1. CARBAMAZEPINE2. PHENYTOIN3. PHENOBARBITAL4. VALPROATE
August 10, 2013 SSG 27
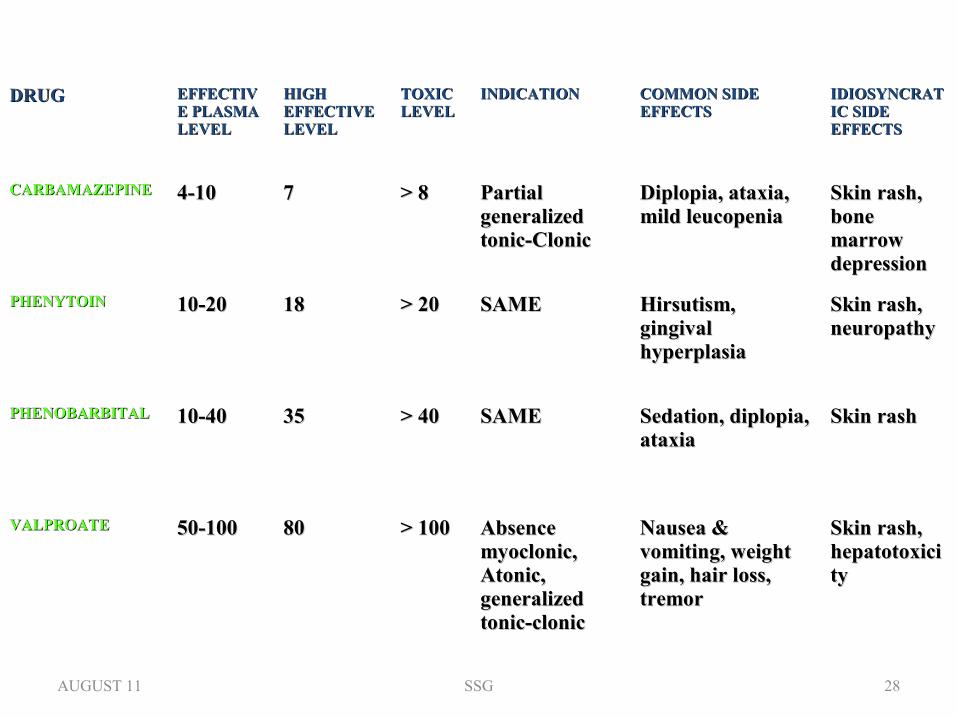
DRUGDRUG EFFECTIVEFFECTIVE PLASMA E PLASMA LEVELLEVEL
HIGH HIGH EFFECTIVE EFFECTIVE LEVELLEVEL
TOXIC TOXIC LEVELLEVEL
INDICATIONINDICATION COMMON SIDE COMMON SIDE EFFECTSEFFECTS
IDIOSYNCRATIDIOSYNCRATIC SIDE IC SIDE EFFECTSEFFECTS
CARBAMAZEPINECARBAMAZEPINE 4-104-10 77 > 8> 8 Partial Partial generalized generalized tonic-Clonictonic-Clonic
Diplopia, ataxia, Diplopia, ataxia, mild leucopeniamild leucopenia
Skin rash, Skin rash, bone bone marrow marrow depressiondepression
PHENYTOINPHENYTOIN 10-2010-20 1818 > 20> 20 SAMESAME Hirsutism, Hirsutism, gingival gingival hyperplasiahyperplasia
Skin rash, Skin rash, neuropathy neuropathy
PHENOBARBITALPHENOBARBITAL 10-4010-40 3535 > 40> 40 SAMESAME Sedation, diplopia, Sedation, diplopia, ataxiaataxia
Skin rashSkin rash
VALPROATEVALPROATE 50-10050-100 8080 > 100> 100 Absence Absence myoclonic, myoclonic, Atonic, Atonic, generalized generalized tonic-clonictonic-clonic
Nausea & Nausea & vomiting, weight vomiting, weight gain, hair loss, gain, hair loss, tremortremor
Skin rash, Skin rash, hepatotoxicihepatotoxicityty
AUGUST 11 SSG 28
DIAGNOSTIC TEST / PROCEDURE
1. ELECTRO ENCEPHALOGRAM (EEG) Involves attaching a series of metal disc called electrodes to the head of the patient to measure the brain’s electrical activity.
2. COMPUTED TOMOGRAPHY(CT SCAN) or MRI For further exploration of the brain to detect the cause of seizure such as tumor,congenital malformation or other changes in the brain.
August 10, 2013 SSG 29
FOCUS CHARTING:FOCUS : SEIZURES
DATA- Seen patient having fits / seizures
ACTIONS:1. Protect client from injurya. Informed your colleague to call the doctorb. Stay with client during seizurec. Pad bed rails or put pillowsd. Make the bed flat,provide protectione. Provide an airway or mouth gag
August 10, 2013 SSG 30
*never restraints of if tongue is caught in teeth do not attempt to open it *
3. Observe and record seizures pattern4. Provide privacy during seizure5. Administer and monitor the effects of medications
RESPONSE- Free from injury and privacy provided and absence of seizure.
August 10, 2013 SSG 31
CASE HISTORY PATIENT NAME MR. X
SEX /AGE MALE / 19 Y.O.NATIONALITY SAUDICOMPANY ARAMCO-PCUR MR # 43-71-98CASE NO. 249877DATE OF ADMISSION 23/09/03DATE OF DISCHARGE STILL IN THE HOSPITALNAME OF DOCTOR; DR. M.D. MANIKALDEPARTMENT NEUROLOGY.
August 10, 2013 SSG 32
MEDICAL HISTORY. THIS 19 YAER OLD MALE WITH HISTORY OF SECONDARY EPILEPSY, POST MENINGITIS, MENTAL RETARDATION, ADMITTED ON SEPTEMBER 23,2003 WITH TWO DAYS HISTORY OF GENERALIZED SEIZURES OFF AND ON.
PATIENT WAS NOT TAKING HIS MEDICINES SINCE THE LAST TWO DAYS.
August 10, 2013 SSG 33

EXAMINATION.
PATIENT IS AWAKE, POST ICTAL STATE AND IRRITABLE.
PULSE: 105/MIN.BLD. PRESSURE: 120/80 mmHg, Afebrile, SPO2: 95%.
Other systemic examination unremarkable. A scar of old brain surgery long time ago on left side of scalp was noted.
August 10, 2013 SSG 34
LABORATORY INVESTIGATIONS;
S. Carbamazepine level 6.4 ug/mlS. Phenytoin level 4.2 ug/mlS. Depakine level 7.68 ug/ml
Other blood biochemistry was unremarkable.
August 10, 2013 SSG 35
TREATMENT Patient was admitted in ICU, given Valium 5mg IV stat then PRN basis. Started on IV flds, given IV Phenytoin 600mg IV stat then Phenytoin 200mg IV Tid for 24hrs. then Phenytoin 400mg PO x OD started his usual medicines.Tegretol CR 400mg PO TID, Lamictal 150mg PO BID, Caltrate 600mg PO x OD, One Alpha 0.25 ug PO BID. Patient has improved and transferred to floor on Sept. 25, 2003 in satisfactory condition.
August 10, 2013 SSG 36
This young man needs a constant caregiver attention to cater to his daily self care / hygiene activities as also to attend to regular medications and seizure precautions. Strict compliance to anti-epileptic medications is needed so that he does not present repeatedly with seizures as emergency to the hospital.He is being discharged and may attend follow up as required every month or two to the Neurology clinic.
August 10, 2013 SSG 37
His relatives however are reluctant to keep him at home on the basis that he has a chronic permanent illness. This young man is again readmitted with seizure recurrence.His S.Tegretol level is low , Epanutin level is high. Doses are being readjusted. He developed one episode of hematemesis and awaiting upper GI Endoscopy. He is likely to be a permanent neurological invalid due to his mental retardation and uncontrolled epilepsy,secondary to childhood meningitis.He should ideally be in Long-term care unit, So LTC was recommended and transferred to the ALTC ward.
August 10, 2013 SSG 38

August 10, 2013 SSG 39