Embed Size (px)
Citation preview

Dr Pradeep

LBW--<2500gm
Prev. 15.5%, 96.5% are born in developing world
Can be d/t preterm birth or small for gestational age
SGA- Wt. for gestation <10th centile
LBW babies are more prone to:◦ Malnutrition
◦ Recurrent infections
◦ Neurodevelopmental delay
LBW contributes 60-80% of neonatal deaths

classification group
Wt - 2000- 2500gm Term LBW
1500-2000gm Preterm (32-36 wks)
1000-1500gms Preterm <32 wks
<1000gms Preterm <28 wks

Birth asphyxia
Hypothermia
Feeding difficulties
Infections
Hyperbilirubinemia
• Respiratory distress
• Apneic spells
• Intraventricular hemorrhage
• Hypoglycemia
• Metabolic acidosis

Inadequate feeding skills
Prone to illness-prematurity
Higher fluid requirements--- higher feed volumes
Gut immaturity
Low body stores of micronutrients

Mothers own milk best for all LBW infants/Expressed breast milk
Donor breast milk
Infant formula
Animal milk
•Standard infant formula•Preterm formula < 1500 gms &
up to 2000 gms achieved

Behavior at breast Range of gestation Response when offered expressed breast milk
Occasional sucklingeffort
28-31 wks Opening mouth, tongue out of mouth, licking milk.Not able to co ordinatebreathing n swallowing
Root n attach to breast .Weak suckling attempts
32- 33 wks Opening mouth, tongue forward, licking milk,i.e -co-ordinate
Root n attach to breast 34-36 wks Able to suck at milk from cup

Is stable?
Fast breathing (RR>60/min)
Severe chest in-drawing
Apnea
Requirement for oxygen
Convulsions
Abnormal state of consciousness
Abdominal distension
Shock
If unstable, start intravenous (IV) fluids
Presence of any one of these signs = UNSTABLE

Initial feeding method in stable babies
Clinically stable
no
Start i.v fluid
yes
Birth wt > 1250 gms
Manage as sick babies guidelines
Able to breast feed effectively
Rot, attach and suckle effectively
no
yesInitiate BF
YES
NO
Able to accept feed by alternate methods-
•When offerd cup swallows without
coughing/spluttering•Adequate quantity to
satisffy needs
Give oral feeds by cup / spoon/paladay
INTRAGASTRIC FEED
yes
NO

Steps in progression feedingHow to decide the
initial feeding method

Progression of feeding low birth
wt


On exclusive breast feeding – iron has to be given 2mg /kg/day from 2- 23 months of age
Breast feed infants < 1500 gms =: when tolerating the feed -
calcium 80mg /kg /day Until 40 wks post menstrual age
phosphorous 15mg/kg/day do
Vitamin D 400 IU/Day do


Rec. fluid requirements & feed volumes
Day of life
Fluid ml/kg/d
Feed every 3 hrly (vol)
Fluid ml/kg/d
Feed every 3 hrly
Fluid ml/kg/d
Feed every 2 hrly
Day 1 60 17 60 12 60 6
Day 2 80 22 75 16 70 7
Day 3 100 27 90 20 80 8
Day 4 120 32 115 24 90 9
2000-2500gms 1500-2000gms 1000-1500gms

Rec. fluid requirements & feed volumes2000 - 2500 1500-2000 1000-1500gms
Day of life
Fluid ml/kg/d
Feed every 3 hrly (vol
Fluid ml/kg/d
Feed every 3 hrly
Fluid ml/kg/d
Feed every 2 hrly
Day 5 140 37 130 28 110 11
Day 6 150 40 145 32 130 13
Day 7 onwards
160+ 42 160 35 150 16

Breast milk should be given as trophic feed 5-10 ml / day if clinically stable

For breast feeding
•Observe•attachment/suckling/ti
redness of infants•Look for sore
nipple/engorgement
Ask mother •How many times in
24 hours feeds•Any problems
experienced by her

Assessment of feeding adequacy of alternating methods
Ask•Volume/freq in 24
hrs/spills/splutters of milkOr
•Baby take too long time to feed
ObserveSpluttering/spitting
the milkOr
Tiring of infants to take required amount

Sign of inadequate feeding
Breast feeding•<8 times in 24 hrs
•Poor attachment/ineffective suckling
•Baby tired/take him off before completion of feeds•Mother having engorged
/sore nipple
By alternative methods
•Feed vol less than indicated
•Less freq/excessive spilling
•Take long time top finish

Wt loss not more than 10% of birth wt
Start wt gaining after 2 wks
Average daily wt gain of LBW in initial 3 -4 mnths
Birth wt -<1500gms: 13.5 to 16 gm/kg/dIf > 1500gms – 10-
13 gm /kg/d

Weeks of life 2000-2500gms 1500-2000gms 1000-1500gms
Wks 3-4 100 100 -
Wks 5-6 100 100 100
Wks 7-11 200 150 100-150
Wks 12-13 250 200 150
Expected wt gain of LBW INFANTS till 3 months of agePer week

Causes of inadequate weight gain

Management of inadequate weight gain
Proper counselling of mothers and ensuring adequate support for breastfeeding their infants
Assessment of positioning/attachment, managing sore/flat nippleExplaining the frequency and timing of breastfeeding and spoon/ paladai feeds
Infrequent feeding is one of the commonest Mothers should be properly counselled regarding the frequency and the importance of night feed
A time-table where mother can fill the timing and amount of feeding
Giving EBM by spoon/paladai feeds after breastfeeding also helps in preterm infants who tire out easily while

Proper demonstration of the correct method of expression of milk and paladai feeding: observe how the mother gives paladai feeds; the technique and amount of spillage followed by a practical demonstration of the proper procedure.
Initiating fortification of breast milk when indicated
Management of the underlying conditions such as anemia, feed intolerance,etc.If these measures are not successful-
• Energy (calorie) content of milk by adding MCT oil, corn starch• Infants on formula feeds given concentrated feeds (by reconstituting 1 scoop in 25 mL of water)
ORb. Feed volume – to 200 mL/kg/day.

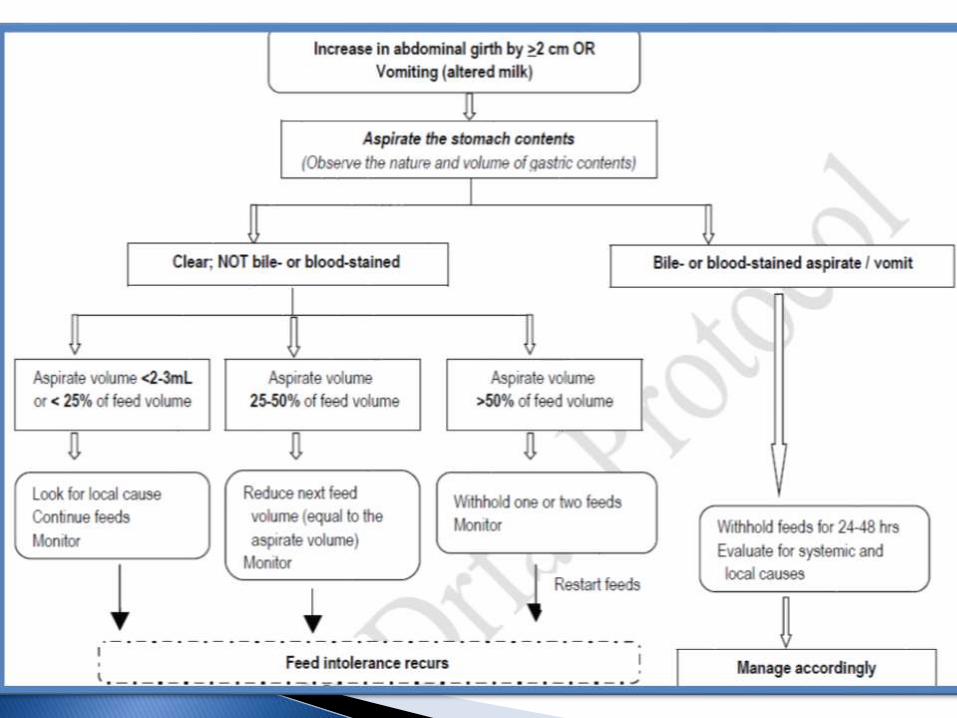
Symptoms:1. Vomiting (altered milk/bile or blood-stained)*2. Systemic features: lethargy, apnoeaSigns:1. Abdominal distension (with or without visible bowel loops)*2. Increased gastric residuals: >2mL/kg or any change from previous pattern
3. Abdominal tenderness
4. Reduced or absent bowel sounds
5. Systemic signs: cyanosis, bradycardia, etc.
Indicators of feed intolerance


MTCT accounts for most cases of hiv in children…
Without any intervention risk during breastfeeding is 5-20 %
Major risk factors are-primary infection at time of breastfeeding(viraemia)-severe disease-poor local health( mastitis, fissures, oral thrush*)-mixed feeding-prolonged feeding

Exclusive breastfeeding for first 6 months of lifeunless replacement feeding is acceptable, feasible, affordable,sustainable and safe..
When replacement feeding is acceptable, feasible,affordable, sustainable and safe, avoidance of all breastfeeding by HIV-infected mothers is recommended.
All HIV-exposed infants should receive regular follow-up care and periodic re-assessment of infant feeding choices,
At 6 months, if adequate feeding from other sources
cannot be ensured, continue to breastfeed their infants and give complementary foods in addition,
. All breastfeeding should stop once an adequate diet without breast milk can be provided.

Process of feeding a child who is not breastfeeding with a diet that provides all the nutrients the child needs, until the child is fully fed on family food.
Could be formula based or heat treated breast milk.

Chronological age-from date of birth
Post –conception/post menstrual age-gestation at birth in wks + chronological age
Corrected age – chronological age in wks-no of wks the infant born early(40 wks)
Growth monitoring for infants up to 40 wks done by UK CHARTS. After that by WHO CHARTS


Steps of Paladai FeedingPlace the infant in up-right posture on mother’s laP
Keep a cotton napkin around the neck to mop the spillage
Take the required amount of expressed breast milk by using a clean syringe
Fill the paladai with milk little short of the brim
Hold the paladai from the sides; DO NOT put your finger
Place it at the lips of the baby in the corner of the mouth

Feed the infant slowly; he/she will actively swallow the milk
If the infant does not actively accept and swallow, try to arouse him/her with gentle stimulation
While estimating the milk intake, deduct the amount of milk left in the cup and the amount of estimated spillage
Wash the paladai with soap and water and then put in boiling water for 20 minutes to sterilize before next feed
Steps of Paladai Feeding
Steps of Intra-gastric Tube Feeding
1. Before starting a feed, check the position of the tube2. Remove the plunger the syringe (ideally a sterile syringe should be used)3. Connect the barrel of the syringe to the end of the gastric tube4. Pinch the tube and fill the barrel of the syringe with the required volume of milk5. Hold the tube with one hand, release the pinch and elevate the syringe barrel6. Let the milk run from the syringe through the gastric tube by gravity;DO NOT force milk through the gastric tube by using the plunger of the syringe7. Control the flow by altering the height of the syringe. Lowering the syringe slows the milk flow, raising the syringe makesthe milk flow faster

8. It should take about 10-15 minutes for the milk to flow into the infant’s stomach
9. Observe the infant during the entire gastric tube feed. Do not leave the infant unattended. Stop the tube feed if the infantshows any of the following signs: breathing difficulty, change in colour/ looks blue, becomes floppy, and vomiting
10. Cap the end of the gastric tube between feeds; if the infant is on CPAP, the tube is preferably left open after about half an Hour
11. Avoid flushing the tube with water or saline after giving feeds.
Steps of Intra-gastric Tube Feeding......





























