Embed Size (px)
Citation preview

Flexor Tendon Injuries
Dr Sanjibani Sudha

FLEXOR TENDON INJURIES
• Anatomy• Nutrition• Healing• Diagnosis• Techniques
• Zone I • Zone II injuries• Partial lacerations• Post op rehab• Reconstruction ladder

There are 12 flexor tendons in the hand and forearm regions, they include finger, thumb flexor and wrist flexor.
Finger flexor are FDS,FDP Thumb flexor FPL Wrist flexor FCR,FCU,PL

Anatomy
• Extrinsic flexors– Superficial group
• PT, FCR, FCU, PL
• Arise from medial
epicondyle, MCL,
coronoid process

Anatomy
• Extrinsic Flexors– Intermediate group
• FDS• Arises from medial
epicondyle, UCL, coronoid process
• Usually have independentmusculotendinous originsand act independantly

Anatomy• Extrinsic flexors
– Deep group• FPL – originates from
entire medial third of volar radius
• FDP – originates on proximal two thirds of the ulna, often has common musculotendinous origins

Anatomy
• Carpal tunnel– 9 tendons– Median
nerve
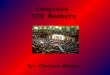
Anatomy• Flexor sheaths
From distal palm(neck of metacarple) to middle of distal phalynx

DIGITAL FLEXOR SHEATH
• Consist of SYNOVIAL SHEATH and PULLEYS(inter woven condensed fibrous bands
• SYNOVIAL sheath is thin layer of continous smooth paratenon, covering the inner surface of fibrous sheath.
• Provide smooth surface for tendon gliding• Provide nutrition to tendon• PULLEY SYSTEM is unique consists of annular pulley
and cruciate pulleys

• Cruciate pulleys are compressible , allowes digital flexion to occur with condensation of fibro osseous sheaths at inner part of flexed finger.
called as CONCERTINA effect


pulleys
• 5 annular pulleys and 3 cruciate pulleys
• Annular pulleys are heavier,condensed and rigid • A1 A3 A5 originates from palmar plate of MCP PIP DIP
joints. A2 A4 from proximal and middle phalynx• A2 is the broadest one,and encompasses the bifurcation
of fds• Maintain the anatomical path of tendons close to bone
and joints, optimising the mechanical efficiency of digital flexion


• Thumb has 3 pulleys ;A1, oblique and A2• A1 and oblique are fuctionaly imp• A1 pulley located palmar to MCP jnt, • Oblique pulley over proximal phalynx . • A2 near the site of incertion of FPL

Anatomy
• Camper’s Chiasma

• FDS lies superficial to FDP upto bifurcation of FDS at the level of MCP J. Then FDS tendon becomes 2 slips coursing laterally and then deeper to the FDP tendons .This FDS bifurcation is in the A2 pulleys area . this part of FDS also serves to constrain the FDS tendon.
• Deep to FDP tendon the FDS slips rejoin to form CAMPERS chiasm and distally inserted to proximal and middle part of middle phalynx

Tendon Morphology
• 70% collagen (Type I)• Extracellular components
– Elastin– Mucopolysaccharides (enhance water-binding
capability)
• Endotenon – around collagen bundles• Epitenon – covers surface of tendon• Paratenon – visceral/parietal adventitia
surrounding tendons in hand• Synovial like fluid environment
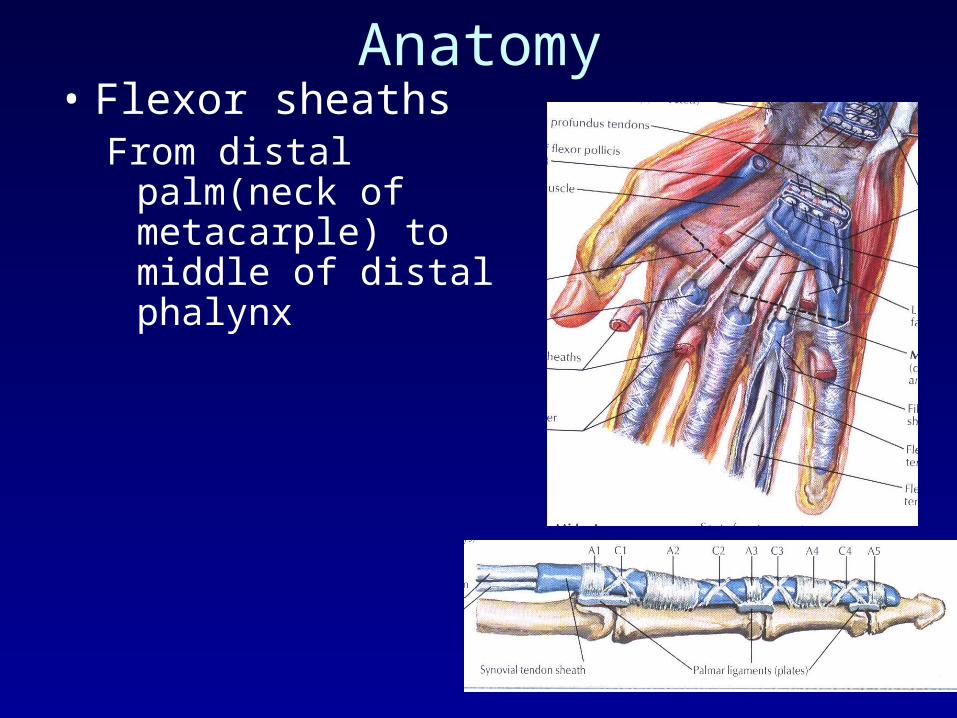
Tendon Nutrition
1. Synovial fluid :produced within tenosynovial
sheath2. Blood supply provide by vincular circulation
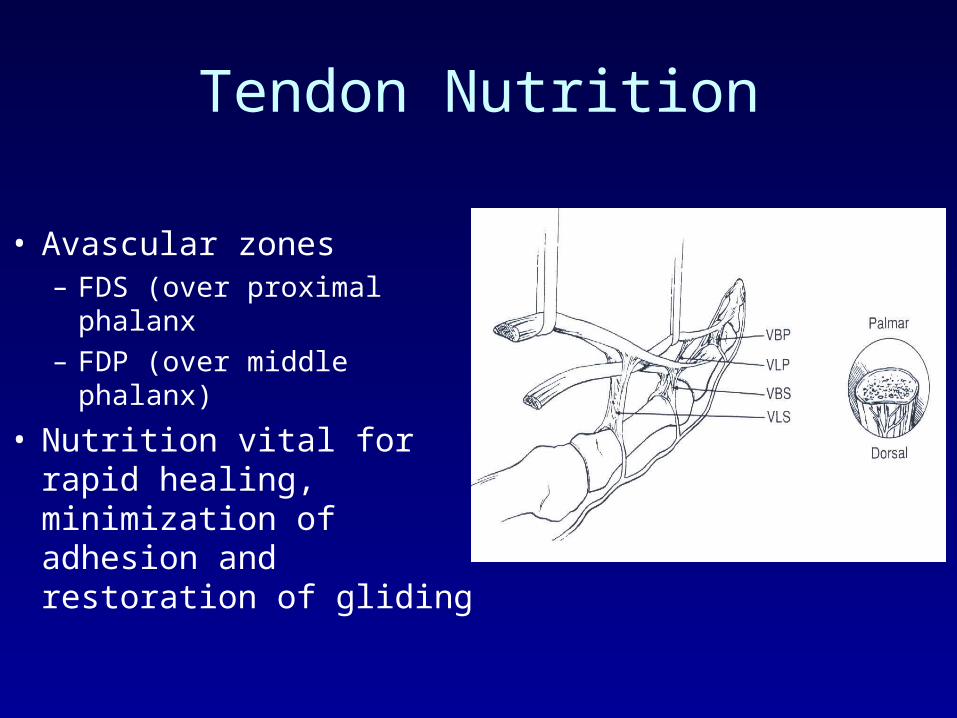
Vascular supply to flexor tendon

Tendon Nutrition
• Vascular– Longitudinal vessels
• Enter in palm• Enter at proximal synovial fold
– Segmental branches from digital arteries• Long and short vinculae
– Vessels at osseous insertions
• Synovial fluid diffusion– Imbibition (pumping mechanism)

Tendon Nutrition
• Avascular zones– FDS (over proximal
phalanx– FDP (over middle phalanx)
• Nutrition vital for rapid healing, minimization of adhesion and restoration of gliding

Nutrition of tendon
Suspensory ligament of tendon
Stabilization of tendon
FDP has 2 vincula; a fan like short vinculum and a cord like long vinculum.
Short v is located at insertion of FDP tendon
Long v connects the FDP tendon through the short v of FDS tendon on the floor of palmar surface of phalynx

Flexor tendon healing• 2 forms:
– Intrinsic healing:– From prolifaration of tenocytes and extracellular
matrix from intrinsic cells. occurs without direct blood flow to the tendon
– Intrinsic healing is innately weaker then extrinsic healing
– If intrinsic capacity is disabled such as in excessive trauma, or in case of post surgical immobilisation extrinsic healing is favoured

• Extrinsic healing: occurs by proliferation of fibroblasts from the peripheral epitendon; adhesions occur because of extrinsic healing of the tendon and limit tendon gliding within fibrous synovial sheaths
Phases of Intrinsic healing1.Inflammatory (0-5 days) : strength of the
repair is reliant on the strength of the suture itself
2.Fibroblastic (5-28 days) : or so-called collagen-producing phase
3.Remodelling (>28 days)

Tendon Adhesion
• Increased adhesion formation with:– Traumatic/surgical injury
• Crush injuries
– Ischemia• Disruption of vinculae
– Immobilization– Gapping at repair site– Excision/injury to flexor sheath components
• Debate over benefit of sheath repair

Tendon Adhesion
• Experimental attempts to minimize adhesion formation– Oral: steroids, antihistamines, NSAIDS– Topical: beta-aminoproprionitrile,
hydrocyprolins, hyaluronic acid, collagen solutions, fibrin
– Physical: silicone/cellophane wrapping, polyethylene tubes, interposed sheath flaps
• Varying lab success but none proven definitively or adopted into clinical practice

Diagnosis
• History

Diagnosis
• Physical exam
• Abnormal resting posture
• Absent FDP / FDS function
• Associated digital nerve and digital vessel injury
• Discuss nature of injury and postoperative course with patient

I Distal to sublimis
II No man’sland
III Lumbricalorigin
IV carpaltunnel
V proximalto carpal tunnel
“No
Man’s
Land”
Bunnell

ZONES
• ZONE 1- distal to the insertion of superficialis
• ZONE 2- no mans land b/w the distal palmar crease and insertion of the sublimis
• ZONE 3- lumbrical region b/w distal palmar crease and the distal end of transverse carpal ligament
• ZONE 4- zone covered by the flexor retinaculum
• ZONE 5- proximal to the flexor retinaculum

Zones of Injury
FDS Insertion
Flexor Sheath(proximal)
TCL(distal edge) Carpal Tunnel

RULES OF REPAIR
• All flexor tendons when severed should be repaired irrespective of whatever is the zone.
• Ideally fix the fracture and repair the tendon and digital NV primarily.
• When delayed repair is done may need a tendon graft• Flexor tendon sheath should be repaired over the
tendon• A2 and A4 pulleys of the flexor sheaths should be
preserved to prevent bowstringing and flexion deformity
Timing of surgery• primary –within 24 hrs
• Delayed primary -1 to 10 days
• Secondary – upto 4 wks
• Late secondary beyond 4 wks
• If wound is clean, primary repair shd be done along with care of neurovascular injury and fracture.

Incisions
• Factors– Avoid crossing joints
at 90 deg.
– Existing lacerations

Repair Techniques
• Ideal– Gap resistant– Strong enough to tolerate forces generated by
early controlled active motion protocols• 10-50% decrease in repair strength from day 5-21
post repair in immobilized tendons• This is effect is minimized (possibly eliminated)
through application of early motion stress
– Uncomplicated– Minimal bulk– Minimal interference with tendon vascularity

• Core sutures• Epitenon sutures – reduce bulk and increase strength
• Core sutures – - careful handling and alignment of tendons - more dorsal suture placement better outcome - More sutures crossing the interaction site, more
strength - lacerations involving more than 60 % cross-section of
the tendon should be repaired - 4-0 braided sutures like polyester most commonly
used
Suture Configurations

Core Sutures
• Current literature supports several conclusions regarding core sutures– Strength proportional to number of strands– Locking loops increase strength but may collapse and
lead to gapping– Knots should be outside repair site– Increased suture callibre = increases strength– Braided 3-0 or 4-0 probably best suture material– Dorsally placed suture stronger and biomechanically
advantageous– Equal tension across all strands

Masson-Allen Criss-cross
Modified kessler Tajima

Masson-Allen Criss-cross
Modified kessler Tajima

Sheath Repair
• Advantages– Barrier to extrinsic adhesion formation– More rapid return of synovial nutrition
• Disadvantages– Technically difficult– Increased foreign material at repair site– May narrow sheath and restrict glide
• Presently, no clearcut advantage to sheath repair has been established
Partial Lacerations
• Controversy in past as partial lacerations were felt to predispose to entrapment, triggering and rupture
• Repair if > 50%
• Some advocate repair of partial lacerations > 60%
ZONE 1
• Repair primarily• Tendon advancement and primary repair to
bone• Advance 1 cm• More than 1 cm; quadriga effect• Old cases: tendon grafting, arthrodesis,
tenodesis

Tendon Advancement
– Previously advocated for zone 1 repairs, as moving the repair site out of the sheath was felt to decrease adhesion formation
– Disadvantages• Shortening of flexor system• Contracture• Quadregia effect• Little excursion distally, therefore adhesions near
insertion less of an issue

FDP Avulsions
• Commonly male athletes
• Forced extension at DIP during maximal flexion (jersey finger)
• Often missed due to normal xray and intact flexion at MP and PIP– Opportunity for FDP reinsertion lost if
treatment delayed

FDP Avulsions
- Type 2: small bony fragment retracts to A3 level- Can fix up to 6 wks
post injury (less shortening)
- May convert to type 1 if tendon slips through A3 pulley and into palm
- Use same technique as for type 1

FDP Avulsions
Leddy and Packer

Pull out wire technique

ZONE 2
• Called bunnells zone or no mans land zone.
• Notorious for bad results, adhesions are a big problem. Area of pulleys
• Repair both tendons at the same time
• Tendons are sutured malrotated
• Suturing should be intratendonous configuration.

ZONE 3
• Lumbrical zone
• Primarily sutured
• Do not suture the belly of the lumbricals as it increases the tension of the muscles
• Lumbrical plus syndrome- paradoxical extension on attempted flexion
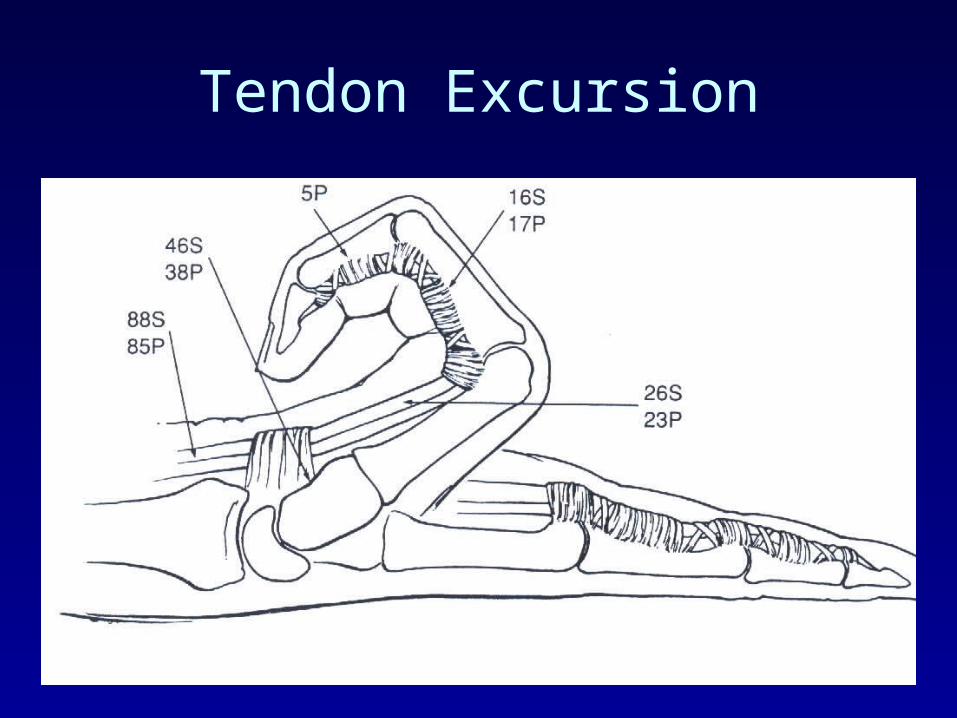
Tendon Excursion

Summary
• Strong gap resistant repair• 4 strand, locking epitendinous (or
equivalent), 3-0 suture needed for early active motion– 4-0 suture, modified Kessler, running
epitendinous suture adequate for more conservative protocols
• No sheath repair• Large grasping/locking loops

FDP Avulsions
- Type 1: zig-zag exposure- Tendon delivered through
pulley system with catheter passed retrograde
- Fixed to base of phalanx with monofilament suture through distal phalanx and nail plate and tied over button
- Fix within 7-10 days before tendon degeneration and myostatic shortening occurs

FDP Avulsions
- Type 3: large bony fragment retracts to A4 level- Bony reduction and
fixation of fragment

Children
• Usually not able to reliably participate in rehabilitation programs
• No benefit to early mobilization in patients under 16 years
• Immobilization > 4 wks may lead to poorer outcomes

Reconstruction

Ladder of tendon reconstruction
• Tenolysis
• Tendon transfer
• Primary tendon graft
• Two stage tendon graft

Tenolysis• Indication
tendon adhesion
• Preop evaluation
discripency exists between passive and active range of motion after hand therapy has platued
• Timing– 3-6 mos. Post repair (minimum)– Plateau with physiotherapy
• Anesthesia– Local with sedation
• Allows patient participation• Motivates patient

Tenolysis
• Technique– Zig zag incisions– Adhesions divided maintaining non-limiting
adhesions– Pulleys reconstructed as needed
• If extensive or not possible convert to staged reconstruction
– On post op- active range of motion should begin immediately
Single Stage Tendon GraftingZone 2
Indications injuries resulting in segmental tendon loss. Delay in repair that obviates primary repair, such as
laceration that have been neglacted for 3 to 6 weeks and show tendon degenerations
Zone 2 injury where large section of tendon have been damaged and surgeon belives delayed grafting is better option
Delay presentation of FDP avulsion injury associated with significant tendon retraction Supple joints with adequate passive ROM

Principles include
• Place only one graft in each finger• Never sacrifice intact FDS• Use a graft of smaller caliber• Perform the junctions outside the tndon sheath• Ensure adequate graft tension
• Before sx wound should be well healed with no extensive scarring
• Joint should be free of contracture and maximum passive range of motion shd have been attained
• Circulation is satisfactory• At least one digital nerve in affected digit is intact
• Pts with joint contacture shd undergo hand therapy regimen to achive maximum possible passive range of motion
• In case of extensive scarring,pulley incompitance,joint contacture single stage grafting is contraindicated.
Single Stage Tendon Grafting Zone 2
• Technique– 1 cm distal FDP stump left intact– 1 cm of FDS insertion left intact (decreased
adhesion formation vs granulating insertion site)
– Tenodesis of FDS tail to flexor sheath (10-20 deg of flexion) optional
• Hyperextension at PIP in absence of FDS tendon occurs occasionally

Single Stage Tendon Grafting Zone 2
• Technique– Graft donors
• Palmaris longus• Plantaris• Long toe extensors• (EIP)• (EDM)

Single Stage Tendon Grafting Zone 2
• Technique– Graft passed through pulley system
• Atraumatic technique
– Distal fixation with tension set proximally or proximal fixation first
– Multiple methods for fixation of graft ends

DISTAL JUNCTURE
• No gliding motion occures at distal juncture,making it as paramount concern there shd be a durable and firm union between the tendon and FDPstump or volar base of distal phalynx
• If enough FDP stump is available graft can be sutured to stump or woven through the stump
• If sufficient stump is not available BUNNEL TENDON TO BONE PULL OUT technique is used
• Place a transverse drill hole across the base of distal phalynx and the graft is threaded through the hole and sutured to itself.in this case graft must be thin enough to pass through bony tunnel

Single Stage Tendon Grafting Zone 2
• Technique– Distal
juncture

PROXIMAL JUNCTURE
• Is made into FDP tendon just distal to lumbrical origin• Motor tendon is slit at its end and graft is threaded into
the slit• pts graft length is estimated in an anesthetized pts by
relaxed position of finger with the wrist in neutral position• Here each finger shd fall into semiflexion, slightly less
flexed then its ulnar neighbour.

Single Stage Tendon Grafting Zone 2
• Technique– proximal
juncture
Pulvertaft weave creates a stronger repair vs end to endtechniques, and allows for greater ease when setting tension

Post op care
Early motion exercise have been used Protected passive range of motion can be instituted after
2 to 3 days of sx if the juncture are strong enough to withstand the tesile strength
Post op splint- static dorsal bloking splint with wrist positioned in neutral,MP in 45 degree flexion, Ipin neutral. And worn for 6 weeks after sx

Secondary Reconstruction Zone 1
• Zone 1 (functioning FDS)– Eg. Late presentation of FDP avulsion– DIP fusion– Tendon graft
• Risks damaging FDS function through injury/adhesions in a very functional finger
• ? Young patients, supple joints, need for active DIP flexion

Secondary Reconstruction Zones 3, 4 and 5
• Usually associated with 3 – 5 cm gap– Interposition graft– FDS to FDP transfer– End to side profundus juncture

Two Stage Reconstruction
• Primary grafting likely to give poor result, but salvage of functioning finger still desirable
• Sub-optimal conditions– Extensive soft tissue scarring
• Crush injuries• Associated fractures, nerve injuries
– Loss of significant portion of pulley system
Two Stage Reconstruction
• Patient selection– Motivated– Absence of neurovascular injury– Good passive joint motion
• Balance benefits of two additional procedures in an already traumatized digit with amputation/arthrodesis

Two Stage Reconstruction
• Stage 1– Excision of tendon remnants
• Distal 1 cm of FDP left intact, remainder excised to lumbrical level
• FDS tail preserved for potential pulley reconstruction
– Incision proximal to wrist• FDS removed/excised• Hunter rod then placed through pulley system and
fixed distally (suture or plate and screw – depending on implant)

Tenolysis
– Release of nongliding adhesions for salvage in poorly functioning digits with previous tendon injury
– Avoid in marginal digits• May not tolerate additional vascular/neurologic
injury
– May need concomitant collateral ligament release, capsulotomy
– Prepare patient for possible staged reconstruction

Two Stage Reconstruction
• Stage 1– Rod extends proximally to distal forearm in
plane between FDS and FDP– Test glide– Reconstruct pulleys as needed if implant
bowstrings

Two Stage Reconstruction
• Stage 1– Postop
• Start passive motion at 7 days• Continue x 3mos to allow pseodosheath to form
around implant• Before stage 2 joints should be supple, and
wounds soft

Two Stage Reconstruction
• Stage 2 – implant removal and tendon graft insertion– Distal and proximal incisions opened– Implant located proximally and motor selected
(FDP middle/ring/small, FDP index)– Graft harvested, sutured to proximal implant
and delivered distally• Fixed to distal phalanx with pull out wire over
button

Two Stage Reconstruction
• Stage 2 – implant removal and tendon graft insertion– Proximally sutured to motor with pulvertaft
weave
• FDS transfer from adjacent digit described• Obviates need for graft• Difficulty with length/tension
• Postop• Early controlled motion x 3 wks, then slow
progression to active motion

Pulley Reconstruction
• Pulley loss– Bowstringing = tendon taking shortest
distance between remaining pulleys– Biomechanical disadvantage
• Excursion translates into less joint motion
– Adhesions/rupture at remaining pulleys due to increased stress
– A2 and A4 needed (minimum) • Most biomechanically important• Some authors advocate reconstructing a 3 or 4
pulley system for optimal results

Pulley Reconstruction
• Most done in conjunction with a two stage tendon reconstruction
• Can be done with single stage tendon graft
• generally if extensive pulley reconstruction is required it is better to do a two stage procedure

Pulley Reconstruction
• Methods– Superficialis tendon
• Insertion left intact• Remnant sutured to original pulley rim, to
periosteum, or to bone through drill holes
– Tendon graft• Sutured as above• Passed through hole drilled in phalanx (risk of
fracture)• Wrapped around phalanx (requires 6-8 cm of graft)

Pulley Reconstruction

Pulley Reconstruction
• Methods– Extensor retinaculum
• Excellent gliding surface• Difficult to harvest the 8-6 cm required for fixation
around phalanx
– Artificial materials• Dacron, PTFE, nylon silicone• Due to abundant atogenous material and
disadvantages of artificial materials, this has not become common clinical practice
• May be stronger in long term vs autogenous