Embed Size (px)
Citation preview
GRAND ROUND
Dr. Yasir JameelClinical Fellow Orthopadic Trauma
• 80 year old male sustaind fall at home and presented with hip pain to A&E
• History
• Age, sex, occupation• Presenting complain• History of PC• Past medical history• Past surgical history • Drugs, Allergies• Social history
Investigations
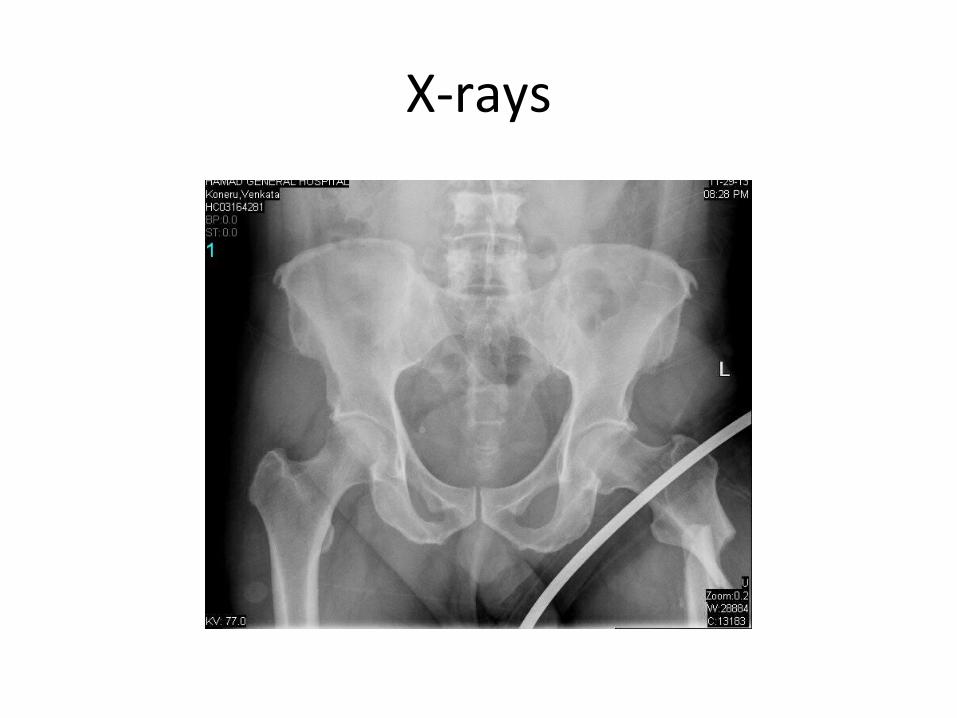
X-rays

X-rays

X-rays
Subtrochenteric femur fracture
• Subtrochanteric area typically defined as area from lesser trochanter to 5cm distal.
• fractures with an associated intertrochanteric component may be called intertrochanteric fracture with subtrochanteric extension or peritrochanteric fracture
Epidemiology
• Younger patients with a high-energy mechanism RTA
• may occur in elderly patients from a low-energy mechanism
• Pathologic or atypical femur fracture • Bisphosphonate use, particularly alendronate,
can be risk factor • Preveious neck fixation with screws placed
with entry below lesser trochenter
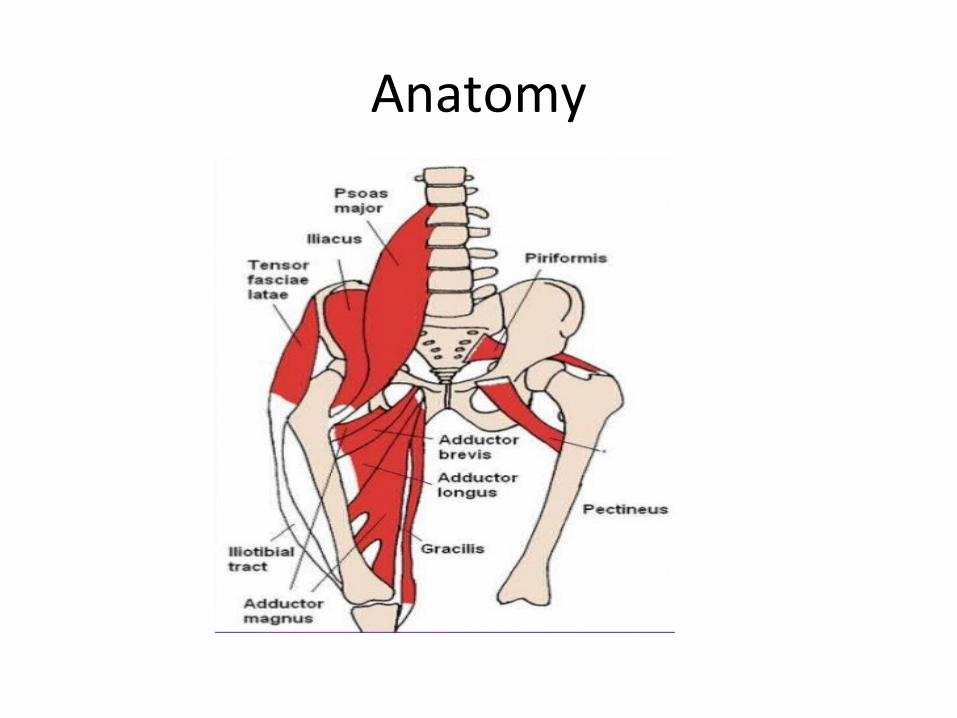
Anatomy
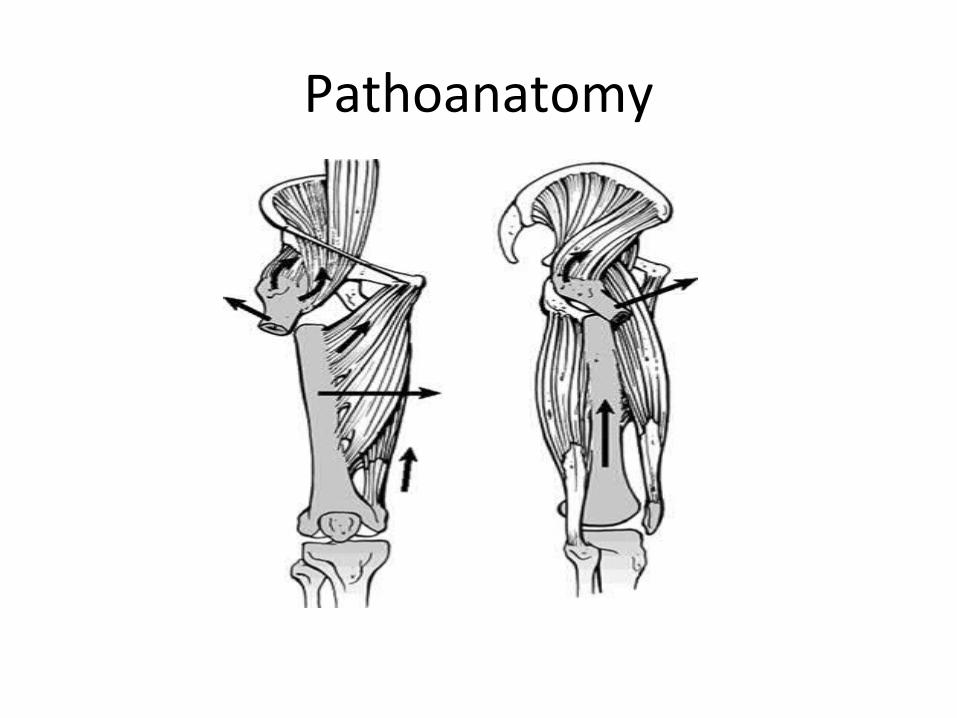
Pathoanatomy• Deforming forces on the proximal fragment • Abduction gluteus medius and gluteus minimus • Flexion iliopsoas • External rotation short external rotators • deforming forces on distal fragment • Adduction hip adductors • Shortening quads and hamstrings
Pathoanatomy
Biomechanics
• Posteriomedial femur undergoes compressive forces
• Lateral femur undergoes tensile forces
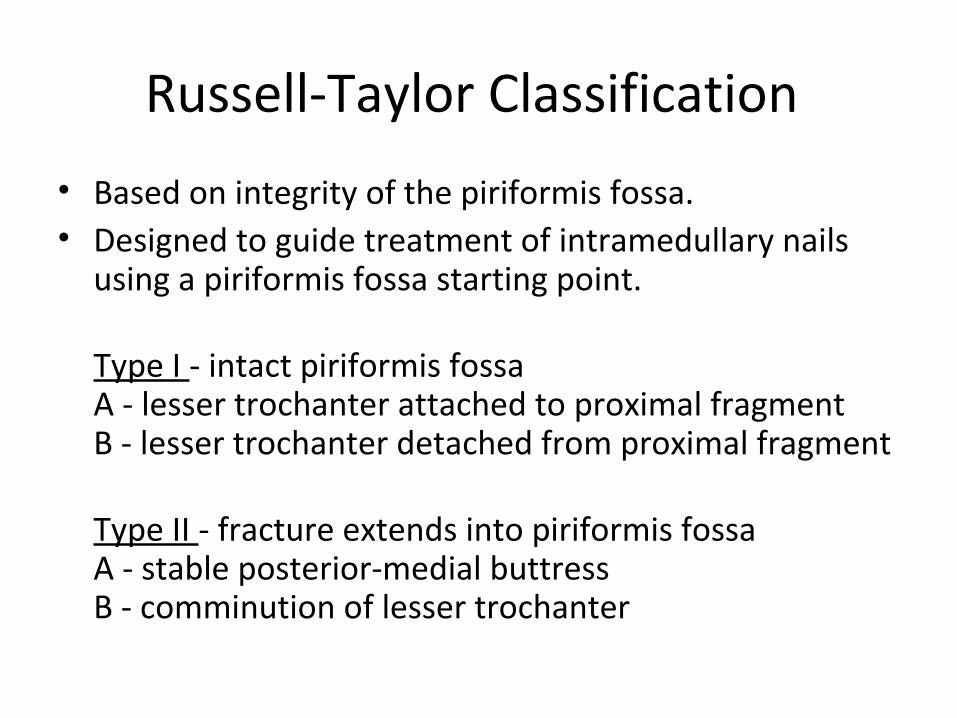
Russell-Taylor Classification
• Based on integrity of the piriformis fossa.• Designed to guide treatment of intramedullary nails
using a piriformis fossa starting point.
Type I - intact piriformis fossaA - lesser trochanter attached to proximal fragmentB - lesser trochanter detached from proximal fragment
Type II - fracture extends into piriformis fossaA - stable posterior-medial buttressB - comminution of lesser trochanter
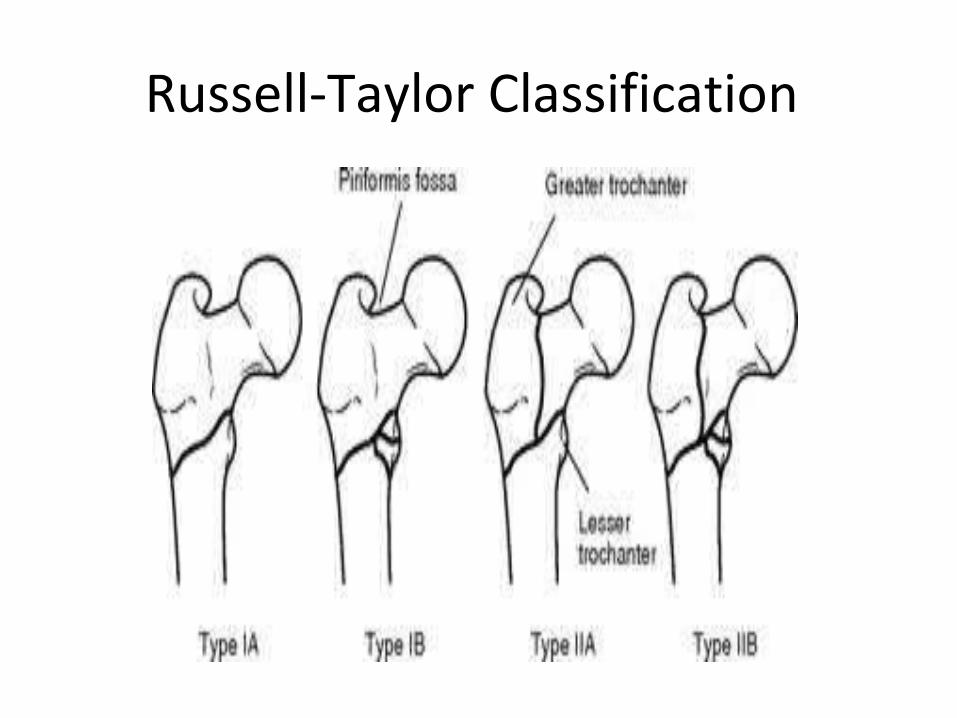
Russell-Taylor Classification
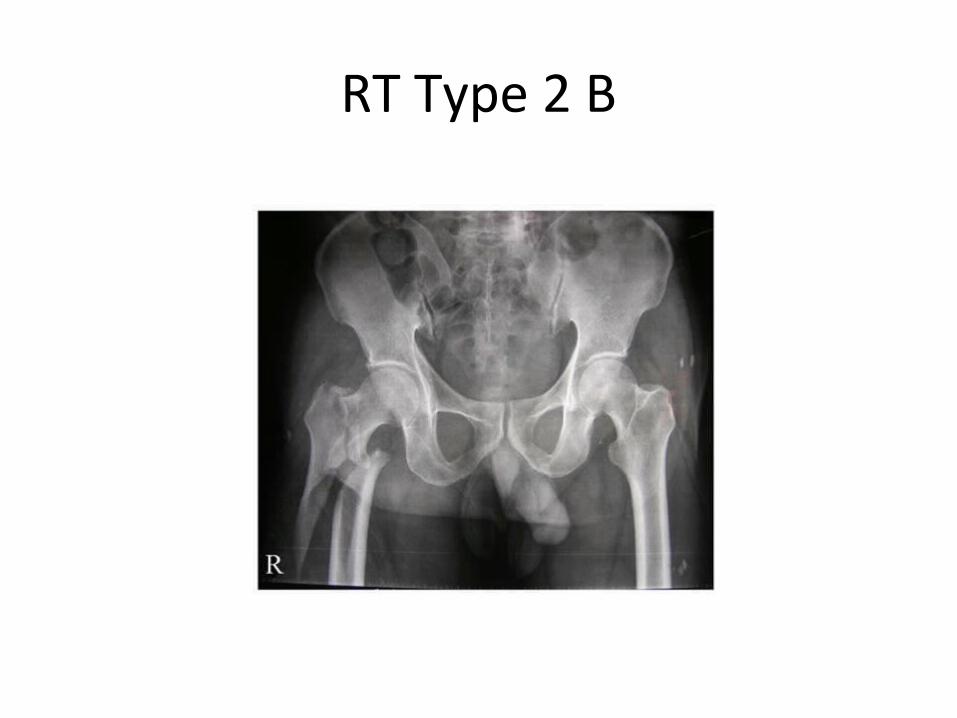
RT Type 2 B
Treatment
• Nonoperative – observation with pain management • indications
– non-ambulatory patients with medical co-morbidities not fit for surgery
– limited role due to strong muscular forces displacing fracture and inability to mobilize patients without surgical intervention
Treatment
• Operative – intramedullary nailing (usually cephalomedullary)
• indications – historically Russel-Taylor type I fractures– newer design of intramedullary nails has expanded indications– most subtrochanteric fractures treated with IM nail
– fixed angle plate • indications
– surgeon preference– associated femoral neck fracture– narrow medullary canal– pre-existing femoral shaft deformity
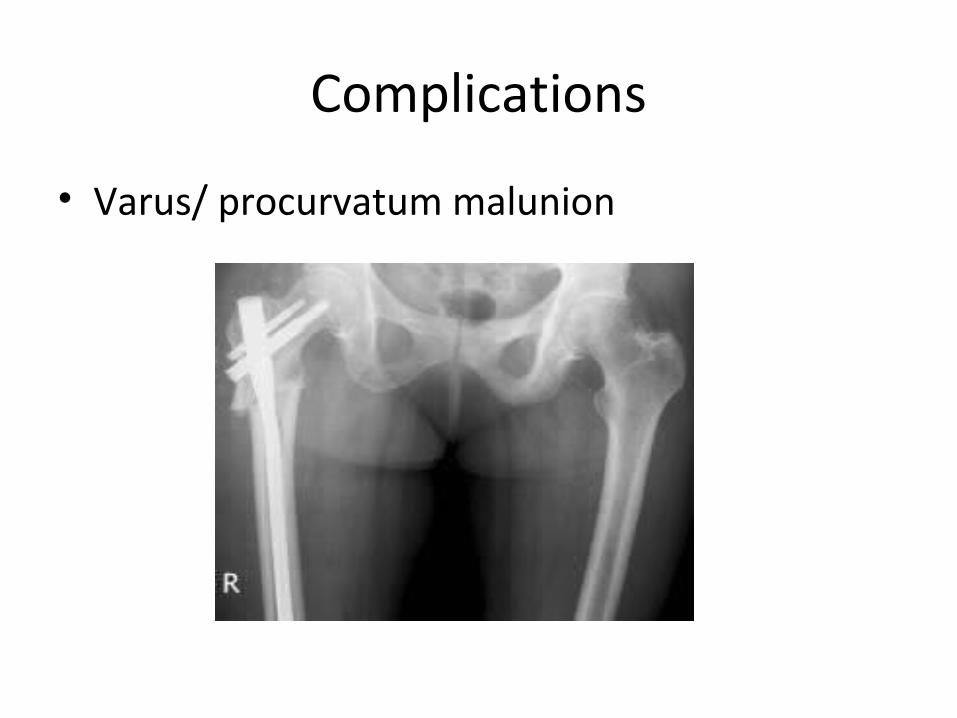
Complications
• Varus/ procurvatum malunion
Complications
• Nonunion
Incidence of 0-8% , continued inability to bear weight at 4-6 months and continued pain. Varus malreduction is an important predictor of nonunion accompanied by implant failure.
Complications
• Malunion: Coxa varus: Caused by uncorrected abduction
deformity, nail entry point that is too lateral, and migration of hardware proximally in the femoral head and neck
Shortening: Due to uncorrected shortening intraoperatively and premature dynamization.
Rotational deformity: Do to uncorrected external rotation of proximal fragment. This can be assessed intraoperatively with visualization of the lesser trochanter
Complications
• Fixation failure: Most common in osteoporotic bone. Screw cutout in the femoral head; backing out of locking screws.
• Failure of implant: Excessive motion at fracture site leads to implant fatigue
• Do you have any question??????????????????
THANK YOU



















![BIKHRAY MOTI [MAULANA TARIQ JAMEEL]](https://img.pdfslide.net/doc/110x75/623437e65f33c03043274db5/bikhray-moti-maulana-tariq-jameel.jpg)








