Embed Size (px)
Citation preview

CNS Fungal Infection
Prof. Mohamed Wael Samir
Prof. Of Neurosurgery
Ain Shams University

ILOs Enumerate the causative organism of the commonest mycotic infections of CNS. Describe the characteristics of those causative agents. Discuss the epidemiology of the commonest CNS fungal infection Describe the gross & histopathological features. Describe the radiological features. Describe the possible clinical presentationDiscuss diagnosis & differential diagnosis Discuss in details treatment of CNS mycosis


Life Treeالحياهالنطاالمملكقالشعبهأو ه الطائفهالصف
الرتبهأو فصيلهالجنعائله
سالنوع
• Growth• Reproduce• Energy…
Living subjec t= Organism
• Nothing
Non living subject =
Inanimate

Life Treeالحياهالنطاالمملكقالشعبهأو ه الطائفهالصف
الرتبهأو فصيلهالجنعائله
سالنوع

Life Treeالحياهالنطاالمملكقالشعبهأو ه الطائفهالصف
الرتبهأو فصيلهالجنعائله
سالنوع
Human Fungus
Organism
Eukarya
Animal Fungi
Cordate-Vertebrate
Mammals- Placetalia
Primate
Hominidae
Homo
H Sapiens

Difference between Fungi and Plants
mannoproteins
b1,6glucans
b1,3
chitin
ergosterol
b1,3 glucansynthase
Cellmembrane
Atlas of fungal Infections, Richard Diamond Ed. 1999Introduction to Medical Mycology. Merck and Co. 2001


1) Cell of origin & pathogenesis
2) Epidemiology
3) Macroscopic features
4) Microscopic features
5) Immunohistochemistry
6) Genetic features
7) Radiological features
8) Growth pattern & spread
9) Grading & behavior
10) Prognosis
Pathology

Types of fugi• Yeasts:
– Unicellular fungi, reproduce by budding– Include candida group.
• Filamentous Fungi (Molds ):– Multicellular filamentous, “fluffy” colonies
consisting of branching tubular structures called hyphae
– Include aspergillus

Types of fugi
Candida Yeast (GMS)
Aspegillus hyphae

Types of fugi• Dimorphic Fungi:
– Either yeast or hyphae form– At ambient environmental temperatures (e.g. 25° C)
grow as molds where they form reproductive spore structures.
– Inhaled spores grow as yeasts at body temperature (37° C) in the host

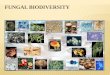
Fungal Habitats
• Most clinically relevant fungi reside in – Soil, – Bird feces, – Vegetation, – Skin and mucous membranes of mammals.

Pathogenesis of Mycotic infections of the central nervous system
• Direct spread:– Paranasal sinus
• Hematogenous spread: from extrtacranial fungal infection or opportunistic infection– Superficial mycosis: skin, hair, nails, mucous
membrane– Deep mycosis: Subcutaneous & deeper tissue– Systemic mycosis: pulmonary infection

Major Types of Opportunistic Mycosis
• Candidiasis: caused by Candida albicans
• Cryptococcosis: caused by Cryptococcus neoformans
• Aspergillosis: caused by Aspergillus sp.
• Others: Blastomycosis, coccidiomycosis, histoplasmosis,

1) Cell of origin & pathogenesis
2) Epidemiology
3) Macroscopic features
4) Microscopic features
5) Immunohistochemistry
6) Genetic features
7) Radiological features
8) Growth pattern & spread
9) Grading & behavior
10) Prognosis
Pathology

Epidemiology
• Incidence: ↑ ↑ ↑• Sex: More common in males (1 outdoor activities)
• Race: No predilection
• Age: More common in young and older individuals
• Risk factors: • Patients with impaired cell-mediated immunity (e.g. AIDS,
organ transplant) at heightened risk for severe disease.• Blastomycosis: Agricultural workers

1) Cell of origin & pathogenesis
2) Epidemiology
3) Macroscopic features
4) Microscopic features
5) Immunohistochemistry
6) Genetic features
7) Radiological features
8) Growth pattern & spread
9) Grading & behavior
10) Prognosis
Pathology

Macroscopic Features• Meningitis:
• Multible microabscesses:
• Granulomas (Micro or macro):
• Vascular invasions causing areas of:
– Hemorrahge
– Infarction
• Extensive brain necrosis
• Vertebral body or disc infection

Macroscopic Features• Meningitis:
• Multible microabscesses:
• Granulomas (Micro or macro):
• Vascular invasions causing areas of:
– Hemorrahge
– Infarction
• Extensive brain necrosis
• Vertebral body or disc infection

Macroscopic Features• Meningitis:
• Multible microabscesses:
• Granulomas (Micro or macro):
• Vascular invasions causing areas of:
– Hemorrahge
– Infarction
• Extensive brain necrosis
• Vertebral body or disc infection

Macroscopic Features• Meningitis:
• Multible microabscesses:
• Granulomas (Micro or macro):
• Vascular invasions causing areas of:
– Hemorrahge
– Infarction
• Extensive brain necrosis
• Vertebral body or disc infection

Macroscopic Features• Meningitis:
• Multible microabscesses:
• Granulomas (Micro or macro):
• Vascular invasions causing areas of:
– Hemorrahge
– Infarction
• Extensive brain necrosis
• Vertebral body or disc infection

Macroscopic Features• Meningitis:
• Multible microabscesses:
• Granulomas (Micro or macro):
• Vascular invasions causing areas of:
– Hemorrahge
– Infarction
• Extensive brain necrosis
• Vertebral body or disc infection

1) Cell of origin & pathogenesis
2) Epidemiology
3) Macroscopic features
4) Microscopic features
5) Immunohistochemistry
6) Genetic features
7) Radiological features
8) Growth pattern & spread
9) Grading & behavior
10) Prognosis
Pathology

Microscopic Features
• Hematoxylin and Eosin (H&E)
• Gomori Methenamine Silver (GMS)
• Periodic acid-Schiff (PAS)
Hematoxylin and Eosin staining of Aspergillus.

Microscopic Features
• Hematoxylin and Eosin (H&E)
• Gomori Methenamine Silver (GMS)
• Periodic acid-Schiff (PAS)
GMS staining of Aspergillus

Microscopic Features
• Hematoxylin and Eosin (H&E)
• Gomori Methenamine Silver (GMS)
• Periodic acid-Schiff (PAS)
PAS staining of Cryptococcus

1) Cell of origin & pathogenesis
2) Epidemiology
3) Macroscopic features
4) Microscopic features
5) Immunohistochemistry
6) Genetic features
7) Radiological features
8) Growth pattern & spread
9) Grading & behavior
10) Prognosis
Pathology

1) Cell of origin & pathogenesis
2) Epidemiology
3) Macroscopic features
4) Microscopic features
5) Immunohistochemistry
6) Genetic features
7) Radiological features
8) Growth pattern & spread
9) Grading & behavior
10) Prognosis
Pathology

1) Cell of origin & pathogenesis
2) Epidemiology
3) Macroscopic features
4) Microscopic features
5) Immunohistochemistry
6) Genetic features
7) Radiological features
8) Growth pattern & spread
9) Grading & behavior
10) Prognosis
Pathology

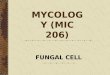
Radiological Features: CT

Radiological Features: MRI
Ill defined in flair
Ring enhancementGranuloma
Meningeal enhancement
small enhancing lesions (arrows) in the erivascular spaces along lenticulostriate
arteries in the basal ganglia.

1) Cell of origin & pathogenesis
2) Epidemiology
3) Macroscopic features
4) Microscopic features
5) Immunohistochemistry
6) Genetic features
7) Radiological features
8) Growth pattern & spread
9) Grading & behavior
10) Prognosis
Pathology

Growth pattern & Spread
• Spread from paranasal sinuses to brain– Through invasion of skull base or – Through vascular invasion
• Spread from contaminated scalp and skull traumatic wound to brain
• Spread generally from the environment to people with limited person-to-person spread.

1) Cell of origin & pathogenesis
2) Epidemiology
3) Macroscopic features
4) Microscopic features
5) Immunohistochemistry
6) Genetic features
7) Radiological features
8) Growth pattern & spread
9) Grading & behavior
10) Prognosis
Pathology

1) Cell of origin & pathogenesis
2) Epidemiology
3) Macroscopic features
4) Microscopic features
5) Immunohistochemistry
6) Genetic features
7) Radiological features
8) Growth pattern & spread
9) Grading & behavior
10) Prognosis
Pathology

Prognosis
• Disease’s factors:
– Localized (Abscess or granuloma) # diffuse
(meningoencephalitis)
• Patient’s factors:
– Immunocompromised # Immunocompetent
• Treatment’s factors:
– Early/Specific # Late/non specific


Clinical syndromes of CNS fungal infection
• Meningitis:• Brain abscess:• Brain Mass:• Stroke-like syndrome:
– Infarcts– Intracerebral hemorrhage– Mycotic aneurysms– Subarachnoid hemorrhage,
Meninges, brain, spinal cord, vertebral bodies or discs

Candidiasis• Candida albicans • Yeast• Opportunistic infection from skin, GIT, or genitalia• Most common mycotic parenchymal infection of
CNS• Multiple microabscesses ± microgranulomas

Cryptococcosis
• Cryptococcus neoformans • Yeast• From lung to brain.• Most common mycotic meningeal infection of CNS• Less commonly, cryptococcosis produces multiple
intraparenchymal pseudocysts• Causing acute or chronic insidious meningitis• Leading to hydrocephalus, dementia, focal
neurological deficits.

Aspergillosis
• Aspergillus fumigatus or Aspergillus flavus• Septated mold• From soil to lung then to brain• 2nd-3rd common mycotic infection of CNS• Foci of hemorrhagic cerebritis

Mucormycosis (Phycomycosis)
• Belong to the family Mucoraceae, including
Rhizopus, Mucor, and Absidia
• Aseptated molds
• From soil to sinus and lung then to brain
• Increasing mycotic infection of CNS
• Sinus mass


Diagnosis
• Imaging:• Testing for serum beta glucan:• fungal culture:
– Blood– CSF obtained by lumbar puncture – Tissue obtained by biopsy.
• CSF analysis:• Specific fungal antibody tests:

Imaging: Meningitis

Imaging: Fungal abscess

Imaging: Granulomas

Beta D Glucan Essay

Direct examination of specimens
• Gram stain:
• Common tissue stains as
– Periodic acid-Schiff (PAS) stain.
– Gomori methenamine-silver nitrate (GMS) stain.
• KOH preparation with calcofluor white:
• INDIA INK PREPARATION

Fungal culture
• Rapid-growing fungi appear in one to three days:• Intermediate growers take five to nine days:• Slow growers take up to four weeks to appear:


Differential Diagnosis
• locally invasive skull base neoplasm:• Multiple ring-enhancing parenchymal lesions in
immunocompetent patients:– Metastases - Multiple pyogenic abscesses– TB - Parasites (e.g., neurocysticercosis)– Fungal abscess (rare) - Septic emboli
• Multiple ring-enhancing parenchymal lesions in immunocompromised patients– Fungal abscesses (common)– TB - Toxoplasmosis - PCNSL

Differential Diagnosis
• locally invasive skull base neoplasm:• Multiple ring-enhancing parenchymal lesions in
immunocompetent patients:– Metastases - Multiple pyogenic abscesses– TB - Parasites (e.g., neurocysticercosis)– Fungal abscess (rare) - Septic emboli
• Multiple ring-enhancing parenchymal lesions in immunocompromised patients– Fungal abscesses (common)– TB - Toxoplasmosis - PCNSL

Differential Diagnosis
• locally invasive skull base neoplasm:• Multiple ring-enhancing parenchymal lesions in
immunocompetent patients:– Metastases - Multiple pyogenic abscesses– TB - Parasites (e.g., neurocysticercosis)– Fungal abscess (rare) - Septic emboli
• Multiple ring-enhancing parenchymal lesions in immunocompromised patients– Fungal abscesses (common)– TB - Toxoplasmosis - PCNSL


Chemotherapeutic Agents
• Antibiotics• Antifungals• Antivirals• Antihelmintics• Antiprotozoal• Anticancer drugs

What are the targets for antifungal therapy?
Cell membraneFungi use principally ergosterol instead of cholesterol
Cell WallUnlike mammalian cells, fungi have a cell wall
DNA SynthesisSome compounds may be selectively activated by fungi, arresting DNA synthesis.

Cell Membrane Active Antifungal
• Cell WALL• Echinocandins
• Inhibit B (1,3) glucan synthesis• No drug in CSF or urine• Used i.v.

Cell Membrane Active AntifungalCell membrane
1. Polyene antifungals - Amphotericin B2. Azole antifungals - Imidazoles (mostly topical) :
Ketoconazole-Triazoles: 1) Fluconazole (Diflucan®)2) Itraconazole (Sporanox ®)3) Voriconazole (Vfend ®)4) Posaconazole (Noxafil ®)
3. Allylamines class

Polyenes: Amphotericin B (Fungizone ®)
• Mechanism of action: • Antifungal Activity: Broad spectrum for both yeast & Molds• Indications: imperial treatment in serious illness• Rout of administration:
– IV (not well tolerated- chills, headaches, nausea) or – Intra-thecal for fungal meningitis
• Adverse effects: – Infusion-related toxicity:: – Cumulative toxicity: Renal impairment
• Dose:– Test dose: 1 mg + 20 mL of D5% over 20 - 30 minutes– Then: 0.25-1.0 mg/kg/d
• Duration: 2-3 gm

Fluconazole (Diflucan®)• Mechanism of action: • Antifungal Activity: Broad spectrum for yeast only• Rout of administration:
– Oral cap: 50 & 150 or syrup 50mg/5mL– Intravenous: 50 ml (2mg/ml)
• Adverse effects: – The most common adverse reaction is relatively minor gastrointestinal
upset– Drug interaction:
• (Diflucan®) ↑ serum level of phenytoin, oral hypoglycemic• (Diflucan®) serum level ↓ by cimetidin and Rifampin
• Dose:– Loading dose for one day: Double maintenance dose (up to 400mg)– Maintenance dose: 200-400mg/d on a single dose [Pediatric: 3-12 mg/kg/d
(max 400mg/d) ]• Duration: until infection resolved

Voriconazole (Vfend ®)• Mechanism of action: • Antifungal Activity: Broad spectrum for both yeast & Molds esp Aspergillus • Rout of administration:
– Oral Tablets: 50 & 200 mg or Powder for Oral Suspension: 200 mg/5ml– Intravenous: Powder for injection: 200 mg
• Adverse effects: – Infusion Related Reactions:– Arrhythmias and QT Prolongation– Visual disturbances:– Drug interaction:
• ((Vfend ®) ↑ serum level of phenytoin, oral Anticoagulants, NSAI, fentanyl, Calcium Blockers
• ((Vfend ®) serum level ↓ by phenytoin and Rifampin
• Dose:– Loading dose for one day: 6 mg/kg q12h – Maintenance dose: 4 mg/kg q12h IV or 200 mg q12h orally
• Duration:– until infection resolved

DNA & Protein Synthesis Active Antifungal
DNA synthesis1. Flucytosine2. Griseofulvin (Grisactin®, Fulvicin®) - Mainly for skin fungus

5’-Flucytosine (Ancobon ®)
• Mechanism of action: • Antifungal Activity: Candida, Cryptococcus and ?Aspergillosis • Rout of administration:
– Oral• Adverse effects:
– Hepatic– Bone marrow
• Dose:– A: PO: 50-150mg/kg/d in four divided doses. for 3 months– C:>50kg:PO: 50-150mg/kg/d in 4 divided doses.– C: < 50kg :PO: 1.5-4.5 g/m2 /d in four divided doses. – C: < 50: PO:1.5-4.5 g/m2 /d in four divided doses. – Neonate: PO: 50-100mg/kg/d in 1-2 divided doses.
• Duration:– until infection resolved ( ~ 3 months)

disease protocal dose duration
HIV neg. 1 Amphotericin 0.7MKD +flucytosine 100MKD +fluconazole 400mg/d
2 wk
10 wk2 Amphotericin 0.7MKD
+flucytosine 100MKD10 wk
HIV pos.induction
Amphotericin 0.7MKD +flucytosine 100MKD +fluconazole 400mg/d
2 wk
10 wkmaintanance Fluconazole 400 mg/d

Refrences
• Eileen P. Scully, Lindsey R. Baden and Joel T. Katz (2008): Fungal brain infections. Curr Opin Neurol 21:347–352
• Anne G. Osborn et al 2004: Infection and Demyelinating Disease. In: Diagnostic imaging Brain. First Edition. Amirsys Inc, Salt Lake City, Utah. part I/section 8/ pp 4- 82
• Srevenc. Bausermanandk. Gillnaul (2001). Bacterial, fungal, and parasitic diseases of the central nervous system. In: Principles and practice of neuropathology, 2nd ed (James S. Nelson, Hernando Mena, Joseph E. Parisi and Sydney S. Schochet) Oxford University Press, Inc. pp.45-77
• Critical Steps for Diagnosing Brain Infections: Slideshow. http://reference.medscape.com/features/slideshow/brain-infections. WebMD LLC. Reviewed 03/26/12