Embed Size (px)
Citation preview

M.Khanlari .MD

Scheimpflug imgaginga wide depth of focus is achieved
Scheimpflug imgaging differs from conventional techniques in that the object plane, lens plane, and image plane are not parallel to each other,
but intersect in a common straight line.
The major advantage is that a wide depth of focus is achieved.

Dual Scheimpflug Imagingcaptures slit images from opposite sides of the illuminated slit
This type of imaging allows assessment of anterior and posterior corneal topography, anterior chamber depthanterior and posterior topography of the lens.
GALILEI captures slit images from opposite sides of the illuminated slit, and averages the elevation data
This Dual Scheimpflug Imaging technique improves the detection of the posterior corneal surface and provides for outstanding accuracy in pachymetry across the entire cornea, even when the camera is decentered due to eye movements

Dual Scheimpflug Imagingdeviation may generate errors in apparent thickness
Living human eyes are always in motion. In this situation, the projected slits impinge upon the anterior surface at different angles, resulting in two apparent slit images representing a different relative thickness.
1 mm of deviation may generate errors in apparent thickness of up to 30 um

Dual Scheimpflug ImagingSimple averaging of the reduces the decentration error
Simple averaging (green line) of the thicknesses in the two corresponding Scheimpflug views (red and blue lines) reduces the decentration error by a factor of 10

Dual Scheimpflug Imagingprincipal advantage
The dual Scheimpflug imaging principle is independent of inclined surfaces, and thus allows accurate pachymetry without knowledge of the actual decentration of the slit from the apex.

Dual Scheimpflug Imagingfaster single Scheimpflug techqniue
The Dual Scheimpflug technique is intrinsically faster than other devices, by requiring only 180° camera rotation instead of 360° rotation.
The short recording time makes the GALILEI easy on the patient, who is not forced to keep the eye open for a prolonged time.

Galilei also has a good eye tracker that detects and compensates for eye movements during image capture.
it singles out a unique patch on the iris and tracks its displacement throughout all of the images.This is done on the x, y, and z axes.
The Galilei may also add a second iris patch, located on the opposite side of the iris, to identify and correct cyclotorsional movement.
Dual Scheimpflug Imagingfaster single Scheimpflug techqniue C good eye-tracker system

Dual Scheimpflug Imaginghigh lateral resolution
lateral resolution is based on a pattern-matching algorithm
For most diagnostic examinations, the standard acquisition resolution is 15 scannings on 360º of the cornea and one Scheimpflug acquisition on each 24° of camera rotation.
With the Galilei, it is possible to increase this resolutions of between six and 60 acquisitions (ie, one acquisition from 60° to 6° of the camera’s rotation)
Therefore, the variety of resolutions provides us with more precise anterior and posterior elevation.

Galileioptical density
The Galilei also integrates a new diagnostic tool into its profile: optical densitometry.
this tool deciphers the patient’s degree of corneal opacity by calculating the intensity of the incident and transmitted rays.
The Galilei is the only tool to measure and control the optical density in two distinct manners, meaning it measures in a the x and y axes.
you can control each image by filtering its color . This function allows the surgeon to zoom in on corneal images, thus observing any changes in the corneal opacities

Galilei Placido Topography
Geometric analysis of the shape of
the reflected rings permits to calculate the steepness, or curvature, of any given point on the corneal surface, and hence to construct a curvature map.

The specific benefit of Placido topography is that it is capable of accurately determining central anterior corneal curvature; a task that is difficult for a Scheimpflug system
One major shortcoming of Placido topography is that it is measuring reflections on the surface of the cornea only. Therefore the method is not capable of detecting information about the thickness of the cornea.
Dual Scheimpflug ImagingPlacido Topography determining central anterior corneal curvature

Dual Scheimpflug Imagingmerging Placido and Scheimpflug data
GALILEI™ overcomes this limitation by merging Placido and Scheimpflug data, acquired simultaneously by the two techniques, into a comprehensive single data set. This is essential for obtaining highest accuracy for both elevation and curvature data across the entire cornea.
In comparison, the Orbscan has approximately 9,000 data points to the Galilei’s approximately 122,000 points.


Dual Scheimpflug Imagingunique features
GALILEI incorporates the following unique features:Merging of Placido and Scheimpflug Data○ Provides for high accuracy for both elevation &
curvature data over the entire corneal surface. Near/Far adjustable Fixation Target○ Allows examining the anterior chamber, crystalline
lens, and any implants under near and far accommodation.
Eye Motion Correction○ The motion of the eye is tracked based on iris pattern
recognition and corrected for to prevent motion artifacts.

Galilei Map Interpretation

Map interpretationRefractive report
The basic Refractive Report contains the four standard maps that are displayed by other tomographers. These maps include Anterior Axial Curvature, Pachymetry, Anterior Elevation and Posterior Elevation (BFS)

Map interpretationDefault and alternate profile
The Default Profile uses one default distribution of colors for all mapst that available in all GALILEI units in former versions
The Alternate Profile was optimized to use the best available scale for each magnitude and incorporates the universal meaning of traffic light colors for all maps
Although the same data are used to produce maps of both profiles, the map patterns and colors may look different due to the scales used.
Numerical values are shown only in the Alternate Profile and could be displayed on all maps.

The appearance of a yellow region indicates that the surface curvature is on the border-line of being abnormally steep and any orange region indicates that the surface has already an abnormally steep curvature.

Map interpretationThe Anterior Axial Curvature map The Default Profile is presented with the Default Type I 1.5 D color
scale The Alternate Profile with the Default CGA 1 D color scale and is
calculated with a keratometric refractive index of 1.3375 There are reasons why Anterior Axial maps with one diopter (D)
scale are recommended and easier to understand. First, it is faster and simpler to count color steps one-by-one in 1 D
increments Second, larger steps (1.5 D) may mask typical patterns of asymmetry and
astigmatism. Third, vertical or horizontal asymmetries larger than 1.4 D are usually
considered risk factors for refractive surgery. Since the GALILEI CGA 1 D color scale has 6 green steps ranging
from 41 D to 46 D, any asymmetry larger than 1 D will be evident. Yellow region indicates is on the border-line of being abnormally steep and any orange region indicates an abnormally steep curvature.

Map interpretationPachymetry map
The Default Profile use Default Type II 25 scale and ANSI Type III 10 µm but Alternate Profile use German CGA 20 µm scale that is much better
the thickness progression and distribution are more apparent when the yellow step is located in the middle of the color scale
The German style has 15 thicker steps of 20 µm each instead of only 11 steps as displayed with the Default style.

Map interpretationAnterior and Posterior BFS Elevation maps
Normal maximum peak ofAnterior Elevation BFS should be less than
10-12 µm and of the Posterior Elevation BFS should be less than
15-16 µm).. To facilitate map interpretation, the
Alternate profile provides 3 green steps show the normal ± 5 µm
values and 2 yellow steps to indicate border- line
values.

Map interpretationIndices displayed with the refractive repor
The indices are presented in mm and diopters The average SimK values, K Steep, K Flat and
steeper Astigmatism with angle are calculated and displayed at the top.
Anterior Instantaneous axial curvature (range: 41 D to 47 D)
Posterior axial curvature (range: -5.50 D to -6.8 D).
Eccentricity (€) value(corneal shape)○ Normal corneal surfaces vary from a sphere (€2
= 0) to a prolate toric ellipsoid asphere (+1 > €2 > 0).
○ The anterior surface (mean value €2 = +0.20 ± 0.16) is less prolate than the posterior surface (posterior €2 > anterior € 2)
○ it seems there are no normal untouched corneas with € 2 < 0 or € 2 ≥ +1

The mean Total Corneal Power (TCP) by ray tracing, TCP steep, TCP flat and steeper Astigmatism with angle
The Axial Anterior Curvature in diopters calculated with a 1.3375 refractive index
Corneal thickness averages ,the thinnest point thickness and location;
pupil size and location of pupil center, and the limbus-to-limbus distance from Superior-
Inferior and Temporal-Nasal.
Map interpretationIndices displayed with the refractive repor

The Refractive Report is the most commonly map used However may be insufficient for some cases because it
compares ante and post corneal surfaces using only BFS elevation map and the posterior surface curvature map is not shown in this popular report
For this reason suggest reviewing routine cases using two separate reports. A new customized report containing the curvature
and elevation topography of both anterior and posterior corneal surfaces
A second report using the Map x1 option and containing only the pachymetry map


Evaluation of refractive reportNormal Spherical Cornea
There is an anterior axial curvature map without a bow-tie pattern (0.22 D of astigmatism and €2 = 0.09) that tends to blue because the surface is uniformly flat (SimK Avg 41.09 D).
The thinnest thickness value is 560 µm and there is asymmetric thickening of the peripheral cornea well observed by the change of color from green to blue (more nasal blue steps than temporal).
There is an almost completely green anterior BFS map as should be expected when the surface uniformly fits the same radius of best fit sphere (±5 µm).
The normal green horizontal bridge pattern on the posterior BFS map suggests that the posterior surface is toric, prolate and elliptical (the indices report 0.25 D of astigmatism and €2 = 0.29).

Evaluation of refractive reportnormal astigmatic cornea
A normal anterior prolate elliptical surface (€2 = 0.31) with a typical steeper vertical (warmer) bow-tie representing a 1.5 D with-the-rule astigmatism.
A completely green pachymetry map indicating a normal thickness distribution and there is a normal symmetric thickness progression (fewer than 10 steps of 20 µm per step).
A normal horizontal green bridge pattern is in the anterior BFS map
The posterior surface is also elliptical but more prolate (€2 = 0.72) than the anterior surface.
The posterior BFS map also shows a normal horizontal bridge pattern with a yellow “hot zone” at the temporal side.
When these hot zones are temporal or nasal, it usually announces an asymmetric bow-tie (irregular astigmatism) in the respective curvature maps When they are located at the center of the bridge, they may correlate with steeper curvatures

Evaluation of refractive reportKC with Irregular Astigmatism
an irregular with-the-rule astigmatism in both the ante and post surfaces
very asymmetric vertical bow-tie appearance
inferior steepening of more than 52 D and a superior flattening less than 40 D
Both anterior and posterior surfaces (€2 = 1.17 and €2 = 1.23, respectively) are prolate with an asymmetric hyperbolic shape (€2 > 1.0). e)
CCT is 471 µm and the thinnest point is 467 µm
The thinnest point is located 0.8 mm from the pupil centroid
an abnormal central hot zone in both BFS elevation maps achieving almost 20 µm in the anterior and 30 µm in the posterior surface.

Map interpretationkeratoconus report
Keratoconus Report inclueAnterior Instantaneous (tangential)
Curvature map.PachymetryAnterior Elevation mapPosterior Elevation (BFS)map

Map interpretationInstantaneous map of keratoconus report (Alternate and default )
In the Alternate Profile This Instantaneous map is calculated with the keratometric refractive index of 1.3375 and is displayed with the Default CGA 1.5 D scale.
In the Default Profile it is shown with the Default Type I 1.5 D scale.

Map interpretationInstantaneous map keratoconus indices
The numerical indices of axial curvature and indices,The Inferior-Superior (I-S) index (an I-S index >1.20 is considered a risk
factor The Standard Deviation of Corneal Power (SDP) are often increased in KC.The Keratoconus Prediction Index (KPI) is a compilation index that
simulates the percent probability of KC based on the anterior surface analysis○ KPI from 0 to 10% seems to correspond to normal or suspicious corneas; ○ KPI from 10 to 20% to suspicious or borderline keratoconic corneas; ○ KPI from 20 to 30 % to keratoconic or perhaps still suspicious corneas, and ○ KPI more than 30% should be considered pellucid marginal degeneration
(PMD) or KC The Keratoconus Probability (KProb) refers to a specificity and sensitivity
validation of the reported KPI value based on the statistical analysis of a series of normal corneas and corneas with KC

The keratoconus prediction index is a compilation index of DSI, OSI, CSI, SAI, SimK1, SimK2, IAI, and AA. \
The Keratoconus Probability (Kprob) is the probability that a keratoconic pattern was correctly detected, based on anterior surface axial curvature. Kprob was calculated based on GALILEI data from a unique database of clinically diagnosed normal and Keratoconus patients.
The Cone Location Magnitude Index (CLMI) is detected on the anterior axial curvature map using a 2 mm spot to search a total search zone of 8 mm diameter. To activate CLMI on the map, make a right-click on the anterior curvature map and tick “CLMI”. The CLMI location will appear as a circle directly on the map. The corresponding value is always displayed in the Keratoconus indices section as CLMI aa.
Percent Probability of Keratoconus (PPK) is defined as the optimal probability threshold for the detection of the disease, based on CLMI. The “suspect” range limits are 20% < PPK < 45%, where PPK > 45% has a high probability of Keratoconus.
Area Analyzed (AA) The simulated index is the ratio of the actual data area to the area circumscribed by a circle 4.0 mm in radius. It is a percentage value equaling 100% if the area is completely covered with measurementvalues.
Average Central Power (ACP) ACP is simulated as the average dioptric power of all points within the central 3 mm.
Central/Surround Index (CSI) The simulated center/surround index reports the difference between the average area-corrected power between the central area (3-mm diameter) and an annulus surrounding the central area (3–6 mm).
Differential Sector Index (DSI)The simulated differential sector index reports the greatest difference inaverage area-corrected power between any two 45° sect

Irregular Astigmatism Index (IAI) is simulated as the average summation of area-corrected dioptric variations along every semi-meridian for the entire analyzed surface and normalized by the averagecorneal power and number of all measured points. The mathematical description of the simulated IAI index is:
Inferior-Superior (I-S) is simulated as the difference between the inferior and superior average dioptric values approximately 3 mm peripheral to the corneal vertex as defined by the center of the map.
Opposite Sector Index (OSI) The simulated opposite sector index reports the greatest difference in average area-corrected power between opposite 45° sectors.
Surface Asymmetry Index (SAI) is simulated as the centrally weighted average of the summation of differences in corneal power between corresponding points 180° apart on all meridians.
Standard Deviation Powers (SDP) is simulated as the standard deviation of all measured powers present on the map.
Surface Regularity Index (SRI) index is simulated as a difference in power gradient between successive points on a hemi meridian that is assigned a positive value and added to the running sum. This sum is divided by the number of points that went into the sum and then scaled. The mathematical formula of the simulated SRI index is:

Evaluation of Keratoconus reportsNormal Spherical Cornea
I-S index is 0.61 D indicating a small asymmetry within normal range.
SDP is only 0.36 SRI is 0.41 D suggesting a
regular and spherical anterior surface.
ACP is 40.99 D confirming the tendency towards a flat surface.
The KPI is 0%.

Evaluation of Keratoconus reportsAstigmatic Cornea With Initial Posterior Surface Changes
A “D-shaped” pattern in the horizontal meridian that has been reported as a risk factor for ectasia
I-S index is 1.29 D also indicating some inferior-superior asymmetry.
The SDP index is 0.91 D, SRI is 0.93 D, ACP is 43.87 D and KPI is 0.9%

Evaluation of Keratoconus reportsKC with Irregular Astigmatism
more than 54 D of inferior steepening and less than 36 D of superior flattening (≈ 18 D of diop-tric difference).
The I-S index is 10.18 D The SDP index is 3.67 D, SRI is 1.81 D, ACP is 47 .62 D KPI is 100%

Galilei and IOL power calculationanterio and posterior corneal power measurment

Map interpretation The IOL Power report The IOL Power report include 4 map
Anterior Axial curvature map Total Corneal Power map Total Wavefront HOA map Placido ring pattern
This report shows all indices including SimK ,SimKavg , astigmatism Total Corneal Power RMS HOA SA (spherical aberation) ACD (from the corneal endothelium ) Anterior chamber volume Chamber angles in degrees at the superior, temporal, inferior and nasal
direction, Nasal-temporal (horizontal) and superior-inferior (vertical) limbus
diameter, Pupil diameter (approximately mesopic) and the Cartesian location of
the pupil centroid relative to the center of the map. The average anterior segment length (ASL) or distance to the posterior
lens requires measurement with a dilated pupil.


The most important value in this window is the 4-mm central average Total Corneal Power (TCP).
The TCP is calculated by ray tracing the refractive power of the cornea using the anterior surface, the pachymetry and the posterior surface
The equivalent power of the cornea (thick lens formula) is the addition of the anterior and posterior curvatures including the ratio thickness/ refractive index of the cornea
Map interpretation The IOL Power report ( Total corneal power )

Galilei and IOL power calculationanterio and posterior corneal power measurment
Anterior cornea power measurment precision The surgeon must remember two relationships:
0.1 mm of error in anterior curvature radius translates into 0.65 D of error in simulated keratometry (SimK), and
1.00 D of error in keratometry becomes 1.00 D of error in pseudophakic refraction
Posterior corneal power measurment precisioncan be calculated from the anterior radius using the value 1.3375,
or the standard index of refraction. Total corneal power measurment precision
keratometers and topographers calculate SimK, represents the average of total central power, just measuring the anterior surface.
It has been known for a long time that this number overestimates the true corneal power.

Galilei and IOL power calculationmain biass: Anterior-to-posterior radii ratio is constant
More accurate SimK calculations may be obtained using other index of refraction values, such as 1.3315 or 1.333, both of which have been tried in the literature.
The 1.3375 value has worked well for contact lens adaptation and IOL power calculations because this inaccuracy, being systematic, can be corrected by compensating for the bias.
However, the Achilles heel of this calculation is that it is based upon one main assumption: Anterior-to-posterior radii ratio is constant
This means that the steepness of the posterior cornea is proportional to the anterior cornea, with a normal value of around 1.21. Any cornea with a different ratio will make the SimK calculation with an arbitrary index of refraction erroneous.

In the last couple of years, we have seen many corneas that have an abnormal ratio. After myopic LASIK or PRK, the anterior radius of curvature
becomes higher (flatter), and the posterior radius remains unchanged, thus increasing the anterior-to-posterior ratio value.
After radial kera-totomy, the ratio increases in a lower magnitude, because there is some posterior flattening as well.
After hyperopic corneal surgery, the change is opposite, and the ratio decreases.
In irregular corneas (eg, keratoconus, scars), the ratio can change as well.
Galilei and IOL power calculationmain biass: Anterior-to-posterior radii ratio is constant

Once both radii are known, ray tracing can be performed to determine the optical properties of that cornea. Paraxial calculations can give a simple central power value, and more complex exact calculations can display lower- and higher order aberrations of the total cornea.
The Galilei performs precise measurement of the posterior cornea, with a high repeatability index of 0.11 D using the Bland-Altman coefficient. It shows a similar value before and after corneal refractive surgery.
Moreover, the software calculates total central power by means of raytracing and algorithms that predict pseudophakic anterior chamber depth
Galilei and IOL power calculationGalilei performs precise measurement of the posterior cornea

Galilei and IOL power calculationThe Galilei predicts IOL power for normal patients as well as the IOLMaster do


The GALILEI G6 Lens ProfessionalThe Advantages of an All-in-One System

The GALILEI G6 Lens ProfessionalThe Advantages of an All-in-One System
The GALILEI G6 Lens Professional* (Ziemer Ophthalmic Systems AG) is advantageous to use for preoperative screening of cataract patients as well as refractive surgery candidates because it encompasses both corneal tomography and an optical biometer in a single devicConvenience. the patient no longer has to move between
several machines. Cost. Additional machines are no longer requiredPhysical space., freeing up space for other uses.Functionality. The GALILEI enables to perform corneal
tomography, wavefront analysis, pachymetry, and biometry for different purposes, including standard cataract surgery, cataract surgery with toric IOL implantation, planning limbal relaxing incisions (LRIs), and LASIK

The GALILEI G6 for Subclinical KeratoconusAutomated Detection Program

The GALILEI G6 for Subclinical KeratoconusAutomated Detection Program
an automated screening program based on artificial intelligence for improving the sensitivity of subclinical keratoconus detection.
One of the major advantages of this decision-tree classification method is its ease of interpretation and of understanding
Automated decision tree, generated to discriminate between normal corneas and those with forme fruste keratoconus. The discriminating rule includes the posterior asphericity asymmetry index (AAI) and the corneal volume.

The GALILEI G6 for Subclinica KeratoconusAutomated Detection Program
This index is calculated over the best-fit toric and aspheric (BFTA) reference surface, which was recently shown to improve the sensitivity of subclinical keratoconus detection when compared with the elevation analysis over the classical best fit sphere (BFS.)

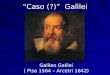
GALILEI image that shows the suspect anterior instantaneous curvature and posterior best sphere elevation map
GALILEI image that shows the abnormal posterior best fit toric asphere elevation map (AAI = 24 µm)
The GALILEI G6 for Subclinica KeratoconusAutomated Detection Program

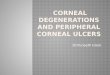
GALILEI images that show the clear keratoconus throughout the left eye (A, B) and especially when viewing the posterior best fit toric asphere elevation map (AAI = 100 µm).
The GALILEI G6 for Subclinica KeratoconusAutomated Detection Program

)
The GALILEI G6 for Avoiding Visual Complaints With Premium IOLs

The GALILEI G6 for Avoiding Visual Complaints With Premium IOLs(Asheric IOL)
Spherical AberrationAverage corneal surfaces a Q factor (Є2) around 0.00 and spherical
aberration between 0.25 to 0.30 µm .The Є2 is an index of corneal surface shape and correlates well with the total corneal spherical aberration
In normal aspheric ellipsoid prolate cornea, - Q or + Є2 increase and the corneal spherical aberration becomes less positive (µm).
Ideally, aspheric corneas with anterior Є2 around 0.60 have 0.00 µm of spherical aberration;after laser refractive surgery ○ hyperprolate corneas with higher anterior Є2 have negative spherical
aberration.○ oblate cornea with lower Є2 have positive spherical aberration
After cataract surgery, the total spherical aberration is the sum of the corneal spherical aberration and the IOL’s spherical aberration. ○ Therefore, the preoperative total corneal spherical aberration can be
used to select the best spherical or aspheric IOL in accordance to what the practitioner decides is best for the eye after cataract surgery

The Kranemann-Arce Index is the quantitative index of asymmetry of corneal surface shape and may be assessed in the BFTA maps of the GALILEI.
The GALILEI G6 for Avoiding Visual Complaints With Premium IOLs(Asheric IOL)

Suggested decision tree for the selection of IOLs according to the corneal surface shape and the total corneal spherical aberration.
The GALILEI G6 for Avoiding Visual Complaints With Premium IOLs(Asheric IOL)

The GALILEI G6 for Avoiding Visual Complaints With Premium IOLs(multifocal and toric IOL)
Coma aberrationAn asymmetric corneal surface shape correlates well with the
total corneal coma , which is the induced starlike dispersion of light rays not focused at the optical axis causing a variation in magnification over the entrance pupil
Large kappa distance or misaligned aspheric IOLs tend to induce increased coma that may be clinically significant in patients who receive a multifocal IOL.
Increased K-A index and coma have been linked with visual complaints in patients with keratoconus and after implantation of toric, aspheric monofocal, or multifocal IOLs.

(Restor,Tecnis) should not be implanted in eyes with vertical or horizontal total corneal >than ±0.50
µm and kappa distance > 0.45 mm
(Rezoom) would be contraindicated in eyes with kappa distance > 0.75 mm
Better results with toric IOLs have been observed when coma is parallel or 90° from the steepest axis of astigmatism. Ideal eyes for toric IOL implantation are those with a symmetric corneal shape and little coma
The GALILEI G6 for Avoiding Visual Complaints With Premium IOLs(multifocal and toric IOL)

Trefoil, Quatrefoil, And Other HOIncreased abnormal trefoil and quatrefoil correspond well with
wavy shape of wavefrontthat commonly found in corneas that have previously undergone radial keratotomy, penetrating or lamellar keratoplasty; those with asymmetric keratoconus, pellucid marginal degeneration, or postoperative ectasia
presently recommend not to implant multifocal IOLs when a○ cornea has >+2.00 SD of HOAs.
In the presence of○ >±0.50 µm of coma,○ >±0.40 µm of trefoil,○ >±0.30 µm of quatrefoil, and ○ >±0.20 µm of fifth-order aberrations,
toric and multifocal IOLs should probably not be implanted
The GALILEI G6 for Avoiding Visual Complaints With Premium IOLs(multifocal and toric IOL)

The GALILEITotal Corneal Astigmatism for Toric IOLs
The posterior cornea, in almost every case, is steep vertically. Because the posterior cornea is a minus lens, that vertical
steepness creates refractive astigmatism that is against-the-rule, meaning the corneal power is greater along the horizontal meridian.
The GALILEI is designed to help surgeons more accurately select the toric IOL and prevent what is commonly occurring: over-correcting eyes that have with-the-rule astigmatism and under-correcting eyes that have against-the rule astigmatism
GALILEI will enable us to measure the posterior corneal curvaturebefore surgery and, in so doing, we will be able to get a comprehensive measurement of total corneal astigmatism.
This will allow us to select our toric IOL appropriately based solely on that have against-the-rule astigmatism

In this case, the SimK astigmatism (from the anterior cornea) was 2.88 D @ 85°, the posterior corneal astigmatism was -0.63 D@ 88°, and the total corneal astigmatism was 2.59 D @ 84°. Based on anterior corneal measurements only, one might select an IOL that corrects at least 2.50 D of astigmatism. Knowing that the posterior cornea contributed more than 0.50 D of an against-the-rule refractive effect, a toric IOL that corrected 2.00 D of astigmatism was implanted. At 3 weeks postoperatively, the manifest refraction was plano.
The GALILEITotal Corneal Astigmatism for Toric IOLs

THANK YOU