Embed Size (px)
Citation preview

Gastroparesis
Niccole CouseUniversity of South Florida
College of Nursing

Introduction (1)
• Gastroparesis is “delayed gastric emptying in the absence of a mechanical obstruction.”
• Commonly caused by autonomic neuropathy– Other causes are stress, infection, post-op
• Occurrence in “0.01%” of men and “0.04%” of women.– “36-49%” Idiopathic– “25-29%” Diabetes mellitus– “7-13%” Post surgical
• Prognosis depends on the cause

Pathophysiology (2)
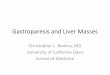
• Healthy
The interstitial cells of Cajal of the stomach are stimulated by the Vagus nerve to contract, which churns and digests food and stimulates peristalsis.

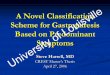
Pathophysiology (2)
• Disease stateIn gastroparesis the stomach does not
contract so food will sit in the stomach for longer than normal.
The main cause is usually neuropathy!– The stomach does not get the signal to
contract

Diagnosis (1)
• Gastroparesis can only be diagnosed after mechanical obstruction is ruled out– Endoscopic and radiologic techniques used.
• MRI, Ultrasound, EGG
– Scintigraphy is “gold standard” for diagnosis• Ingest “radiolabelled meal” and check for residue at
certain times• “Positive if more than 60% residual ingested meal
content is detected within the stomach after 2 h, or more than 10% residual content is detected at 4 h.”

Risk Factors (2)
• Diabetes– Diabetic neuropathy
• Female– Higher Progesterone• Reduces smooth muscle activity
• Viral infections– Certain viruses can lead to damage to
the stomach

Signs and Symptoms
• Persistent nausea and vomiting
• GERD• Constipation and
diarrhea• Abdominal pain• Bloating• Anorexia• Unintended weight loss • Inconsistent blood
glucose levels

Treatments (1)
• Dietary management– Dietary consult with patient– Evauate best tolerated foods– Reduce meal size and smaller pieces of
food– Low fat (liquid if needed)– No alcohol or carbonated beverages– Fiber consumption is debated
• Most agree that insoluble fiber should be avoided

Treatments
• Medications– Prokinetic drugs (1)
• Metoclopramide• Erythromycin• domperidone
– Botulinum toxin injections (Botox) (1)
• Relaxes smooth muscle• Injected into pyloric sphyncter allows for
easier passage of food into the duodenum

Treatments
• NG/NJ tube placement– If dietary changes and medications are
ineffective than an NG/NJ tube may be placed to provide nutrition
• Parenteral nutrition –May be considered –Weigh the risks of infection and
thrombosis

Treatments
• Surgery– PEG-J tubes (1)
• Allows food to skip the stomach• Relievs symptoms• Improves nutritional status in “83%” of patients
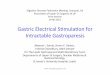
– Gastric pacemaker (3)
• Electrical stimulation of the stomach• High frequency stimulation is shown to reduce
nausea and vomiting• Low frequency stimulation is shown to increase
motility and peristalsis

Gastric Pacemaker

Prognosis (4)
• Many people with gastroparesis are able to live normally with long-term prokinetic therapy
• Patients with gastroparesis caused by diabetes often require a more serious intervention along with prokinetic therapy

Clinical Example
• Admission Dx: intractable vomiting• Other diagnoses: – Gastroparesis– Chronic gastritis– Barrett esophagitis– Fibromyalgia– hyperthyroidism

Clinical Example
• HPI:– 40y white female– Has been experiencing persistent nausea
and vomiting for the past six months• Throws up at least once a day
– Complains that she “can’t keep anything down”
– Patient states that the nausea is constant– Patient denies any aggravating factors– Patient smokes marijuana and cigarettes

Clinical Example
• Medications– 0.9%NaCl IV – Pregabalin – pain– Baclofen – pain/fibromyalgia– Omeprazole – healing of erosive esophagitis– Milnacipran – fibromyalgia management– Odansetron – nausea prevention– Lorazepam – anxiety
• Current therapies– Full liquid diet– Strict monitoring of I & O– Vitals Q6H– Glucose monitoring at meal time

Assessment
• Inspect– Swelling, abdominal distention, tenderness– Fluid output– Daily Weights
• Auscultate– Presence of bowel sounds
• Percuss– Tympany
• Palpate– Pain, tenderness, masses

Nursing Diagnosis
• Risk for deficient fluid volume
• Impaired nutrition: less than body requirements
• Risk for electrolyte imbalance

NCLEX style question
• A client with diabetes has been diagnosed with gastroparesis. The nurse realizes this is considereda) A long-term complication of diabetic
neuropathy.b) A symptom of microvascular diseasec) A precursor to long-term wound
infections.d) A precursor to renal failure

NCLEX style question
• A client with diabetes has been diagnosed with gastroparesis. The nurse realizes this is considereda) A LONG-TERM COMPLICATION OF
DIABETIC NEUROPATHY.b) A symptom of microvascular diseasec) A precursor to long-term wound
infections.d) A precursor to renal failure

NCLEX style question
• Which of the following treatments would NOT be appropriate for a client with gastroparesis?a) Botulinum Toxin injectionb) Bowel diversion surgeryc) NJ tube feedingsd) Gastric Electrical
Stimulation/Pacemaker

NCLEX style question
• Which of the following treatments would NOT be appropriate for a client with gastroparesis?a) Botulinum Toxin injectionb) BOWEL DIVERSION SURGERYc) NJ tube feedingsd) Gastric Electrical
Stimulation/Pacemaker

References(1) Athwal, V., Keld, R., Kinsley, L., & Lal,S. (2011). Pathogenesis, investigation and
dietary and medical management of gastroparesis. Journal of Human Nutrition and Dietetics, volume 24(issue5). DOI: 10.1111/j.1365-277X.2011.01190.x
(2) Buckle D.C. Treatment of Gastroparesis in the Age of the Gastric Pacemaker: Gastric Electrical Stimulation. Retrieved from
http://www.medscape.com/viewarticle/460632
(3) Lin,Z. Forester, J. Sarosiek, I. & McCallum, W. Treatment of Gastroparesis with Electrical Stimulation. Digestive Diseases and Disorders, volume 48(issue5). DOI DOI:
10.1023/A:1023099206939
(4) Rayner, C. & Horowitz, M. New Management Approaches for gastroparesis. Medscape. Retrieved from http://www.medscape.com/viewarticle/514206_8