Embed Size (px)
DESCRIPTION
GERD in children
Citation preview

GERDKhaled Saad

The passage of gastric contents into the esophagus (GER) is a normal physiologic process that occurs in healthy infants, children. Most episodes are brief and do not cause symptoms, esophageal injury, or result in other complications. In contrast, gastroesophageal reflux disease (GERD) occurs when the reflux episodes are associated with complications such as esophagitis or poor weight gain.

DEFINITIONS The term "uncomplicated” (GER) is used to
describe the normal physiologic process of frequent regurgitation in the absence of pathological consequences. The term, (GERD), is used when the reflux has pathological consequences, such as esophagitis, nutritional compromise, or respiratory complications.

Natural history: Gastroesophageal reflux (GER) is extremely common in healthy infants, in whom gastric fluids may reflux into the esophagus 30 or more times daily. The frequency of reflux decreases with increasing age, such that physiologic regurgitation or vomiting decreases toward the end of the first year of life, and is unusual in children older than 18 months old. Pediatrics 1991; 88:834.

Although the problem usually resolves by the end of infancy, there is a weak association with GERD later in life. As an example, frequent regurgitation during infancy and a history of GERD in the mother (but not the father) both predict the risk of reflux-related symptoms during childhood. Pediatrics 2002; 109:1061.

Prevalence
The prevalence of various symptoms suggestive of gastroesophageal reflux (GER) was 1.8 to 8.2 percent.
Arch Pediatr Adolesc Med 2000; 154:150.

CLINICAL MANIFESTATIONS
The most common symptoms of gastroesophageal reflux (GER) and gastroesophageal reflux disease (GERD) vary according to age, although overlap may exist:

Infants –Regurgitation is present in 50 to 70 percent of all infants, peaks at age four months, and typically resolves by one year.
A small minority of infants with GER develop other symptoms suggestive of GERD, including feeding refusal, irritability, hematemesis, anemia, respiratory symptoms, and failure to thrive.

Preschool age children with GERD may present with intermittent regurgitation. Less commonly, they may have respiratory complications including persistent wheezing. Decreased food intake or poor weight gain without any other complaints may be a symptom of esophagitis in young children. All of these symptoms are nonspecific and insufficient to make a definitive diagnosis of GERD.

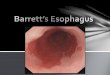
Older children and adolescents – The pattern of GERD in older children and adolescents resembles that seen in adults. The cardinal symptoms are chronic heartburn and/or regurgitation. Complications of GERD, including esophagitis, strictures, Barrett's esophagus, and hoarseness due to reflux laryngitis, also may be seen. Older children may complain of nausea, dysphagia and/or epigastric pain.

Surgery
Life Style
Dietary Management
Pharmacotherapy
Management Complications
Wise Approach GERDWise Approach GERD
5 Stages Management5 Stages Management
Life Style

Life Style ModificationLife Style ModificationPositions in infantsPositions in infants

Position in ChildrenPosition in Children
Daily activities modificationDaily activities modification•Exercise:? Exercise induced reflux•Overweight•No snaking close to bed time
•Exercise:? Exercise induced reflux•Overweight•No snaking close to bed time

Surgery
Life Style
Dietary Management
Pharmacotherapy
Management Complications
Wise Approach GERDWise Approach GERD
5 Stages Management5 Stages Management
Dietary Management

Dietetic ManagementDietetic Management
Regurge with normal weight gain and No Signs of GERD
1.Changing feeding schedule: burping, gently massage abdomen and avoid tight diapers
2.Use pacifiers: saliva and neutralize acid
3.Thickening feeds: precooked corn starch, one grain cereal, carob, gower gum, rice starch??
4.Using special AR formulas
5.Trying solid foods if weaned
1.Changing feeding schedule: burping, gently massage abdomen and avoid tight diapers
2.Use pacifiers: saliva and neutralize acid
3.Thickening feeds: precooked corn starch, one grain cereal, carob, gower gum, rice starch??
4.Using special AR formulas
5.Trying solid foods if weaned

Persistent regurge signs of poor weight gain esophagitis or respiratory symptoms
Consider cow milk with protein eliminationConsider cow milk with protein elimination
Re-evaluate (upper GI examination)Re-evaluate (upper GI examination)
Trial of medicationTrial of medication
N.B. - Probiotics-
Homeotherapy
N.B. - Probiotics-
Homeotherapy

Surgery
Life Style
Dietary Management
Pharmacotherapy
Management Complications
Wise Approach GERDWise Approach GERD
5 Stages Management5 Stages Management
Pharmacotherapy

PharmacotherapyPharmacotherapy
II) Second line drugsII) Second line drugs
- Acid blocking drugs (neutralise or stomach acidity)- Acid blocking drugs (neutralise or stomach acidity)
1- Histamine H2RA Ranitidine
2- Proton pump inhibitors PPI
Omeprazole
1- Histamine H2RA Ranitidine
2- Proton pump inhibitors PPI
Omeprazole
I) First line drugsI) First line drugs
- Mylicon
- Gaviscon
- Mylicon
- Gaviscon

Prokinetics (drugs that improve intestinal coordination)
1- Cisapride (propalsid) abnormal heart rate
2- Erythromycin side effect is an advantage
III)Third line drugsIII)Third line drugs

Approaches toAcid-Reducing Therapy
Begin treatment with PPI Maintain improvement with
PPI Switch to H2RA
Begin treatment with PPI Maintain improvement with
PPI Switch to H2RA
Begin treatment with H2RA Inadequate response PPI Inadequate response ↑ PPI
dose
Begin treatment with H2RA Inadequate response PPI Inadequate response ↑ PPI
dose
Step DownStep Down
Step UpStep Up

• Tachyphylaxis: tolerance with prolonged use inspite increasing dose
• Decreased absorption of Fe, Ca, Folic acid, B12
• Tachyphylaxis: tolerance with prolonged use inspite increasing dose
• Decreased absorption of Fe, Ca, Folic acid, B12
Side effects of antacids:Side effects of antacids:
• Stomach acid is a part of the body immune system Kills pathological bacteria in the gut
• Stomach acid is a part of the body immune system Kills pathological bacteria in the gut

Surgery
Life Style
Dietary Management
Pharmacotherapy
Management Complications
Wise Approach GERDWise Approach GERD
5 Stages Management5 Stages Management
Management Complications

Management of Supraesophageal Complications
Management of Supraesophageal Complications
Chronic sore throat & hoarsness
Dental erosions
OM & Sinusitis
Wheezing Asthma
Apnea Bradycardia
Chronic cough
ALTE

• ALTE = acute life threatening event
apnea, color change, chocking gaging
• 60% to 70% of infants with ALTE have recurrent regurge and abnormal esophageal pH
• Relationship between GER and obstructive or mixed apnea most convincing when infant was:
Awake, Supine, Fed within past hour
• ALTE = acute life threatening event
apnea, color change, chocking gaging
• 60% to 70% of infants with ALTE have recurrent regurge and abnormal esophageal pH
• Relationship between GER and obstructive or mixed apnea most convincing when infant was:
Awake, Supine, Fed within past hour
GER and ALTEGER and ALTE

Aspiration SyndromesAspiration Syndromes
• Aspiration pneumonia &pleural effusion
• Acid aspiration pneumonitis
• Interstitial lung disease & pulmonary fibrosis
• Aspiration pneumonia &pleural effusion
• Acid aspiration pneumonitis
• Interstitial lung disease & pulmonary fibrosis

• GER Asthma
• GER Asthma
• GER Asthma
• GER Asthma
• GER Asthma
• GER Asthma
• GER Asthma
• GER Asthma
Does GER Cause Asthma?Does GER Cause Asthma?


Surgery
Life Style
Dietary Management
Pharmacotherapy
Management Complications
Wise Approach GERDWise Approach GERD
5 Stages Management5 Stages Management
Surgery

Infants and Children:• Failure of medical therapy
• Dependence on aggressive or prolonged medical therapy
• Persistent asthma or recurrent pneumonia due to GERD
Infants and Children:• Failure of medical therapy
• Dependence on aggressive or prolonged medical therapy
• Persistent asthma or recurrent pneumonia due to GERD