Embed Size (px)
Citation preview

UJ Glaucoma

UJIntroduction
is a group of eye diseases traditionally characterized by elevated intraocular pressure (IOP).
However, glaucoma is more accurately defined as an optic neuropathy with optic neuropathy with characteristic visual field loss characteristic visual field loss than a disease of high pressure
UJBasic Physiology
The intra-ocular pressure depends on the balance between production and removal of aqueous humour.
Aqueous humour is produced from the ciliary processes by active secretion and ultra filtration Post chamber Through pupil Ant chamber Drained

UJ
Drainage:1) Conventional pathway Through the
trabecular meshwork, Schlemm’s canal and episcleral veins.
2) Uveoscleral pathway Across the ciliary body into the supra-choroidal space and into the venous circulation across the sclera.(4%)

UJ

UJ

UJ
Q) How does elevated ocular pressure cause damage to ocular nerve fibers?
1) Direct mechanical damage to optic nerve axons2) Ischemia of nerve axons due to reduction of the
blood flow.
Pathophysiology of glaucoma is multifactorial and both of these mechanisms play a role.

UJ

UJ Primary Glaucomas are classified according whether or not the
iris is:
1) Clear of the trabecular meshwork (Open angle).
2) Covering the meshwork (Closed Angle).

UJ
UJPrimary Open Angle Glaucoma
How can you see the irido-corneal angle?You use a Gonioscopy Lens during a slit lamp
examination.In open angle glaucoma, the structure of the
trabecular meshwork appears normal but functionally it offers increased resistance to flow due to:
1) Thickening of trabecular lamellae which reduce pore size
2) Reduction in the number of lining trabecular cells.3) Increased extra-cellular material in the trabecular
meshwork spaces.

UJ iridocorneal angle

UJ Gonioscopy Lens
UJ Open Angle GlaucomaAka: chronic simple glaucoma (CSGAka: chronic simple glaucoma (CSG))
and primary open angle glaucoma (POAGand primary open angle glaucoma (POAG))
Onset: 50+ years of ageOnset: 50+ years of age
SymptomsSymptoms Usually noneUsually none
May have loss of centralMay have loss of central and peripheral visionand peripheral vision
latelate
SignsSigns Elevated IOPElevated IOP
Visual field lossVisual field loss Glaucomatous disk changesGlaucomatous disk changes

UJ O_oNormal/low tension glaucoma: when the optic nerve head is susceptible to IO pressure, damage happens even when the IO is NL
Ocular HTN: IO pressure is raised but no optic disc damage

UJ
UJEpidemiology:
•Affects 1-200 of population over the age of 40 and the prevalence increases with age
•Males equally affected as females
•1st degree relatives of patients with chronic open angle glaucoma have a 16% chance of developing the disease themselves.Mode of Inheritance is complex

UJ History •Symptoms depends on the rate of IO pressure rises.
•Associated with slow rise in pressure and it’s symptomless until pt becomes aware of visual deficit.

UJ On examination:� Need full slit lamp exam to:
Measure the ocular pressure using the tonometer ranges between (11-21 mmHg) – In chronic open angle glaucoma: pressure 22-40
mmHg– In angle closure glaucoma >60 mmHg
To measure the thinkness of the cornea with a pachymeter, to adjust the value of IO pressure.

UJ
To examine the iridocorneal angle to confirm that an open angle is present
To exclude other ocular disease that may be 2ry cause for the glaucoma
Examine the optic disc and determine whether it is pathologically cupped

UJ
Disc cupping is normal up to a cup to disc ratio of 0.8
that the size of the cup is dependant on the size of the disc.
In chronic glaucoma the central cup expands and the rim of nerve fibres (neuroretinal rim) becomes thinner. The nerve head becomes atrophic. The cup to disc ratio in the vertical is greater than 0.4 and the cup deepens.

UJ

UJ
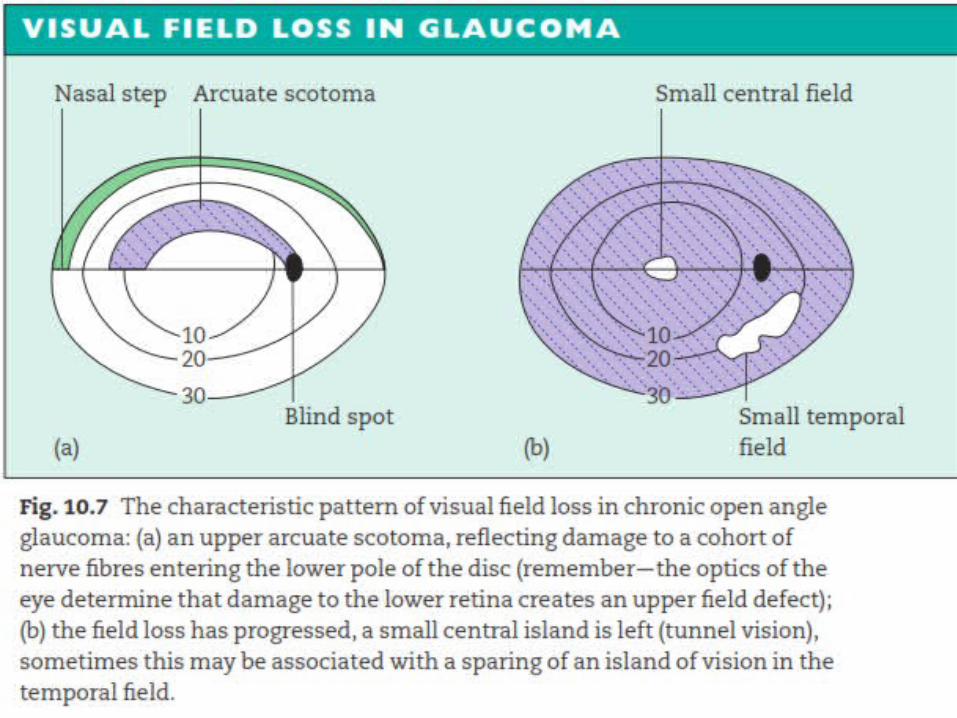
UJGLAUCOMA
Visual fields in glaucomaVisual fields in glaucoma
EarlyEarly LateLate

UJTreatment The main aim of treatment is reduction and
control of IOP at a level that prevents further glaucomatous damage to the eye.
This value of target pressure varies from one person to the other.
Modalities of treatment include:1) Medical2) Surgical3) Laser

UJ Medical Treatment
Topical Agents Example Action
Beta Blockers Timolol Decrease secretion
Parasympathomimetics Pilocarpine Increase outflow
Sympathomimetics Adrenaline Both DS & IO
Alpha-2 Agonists ApraclonidineIncrease Uveoscleral outflow & DS
Carbonic Anhydrase Inhibitors Dorzolamide DS
Prostaglandin Analogues LatanoprostIncrease Uveoscleral outflow
Systemic AgentsCarbonic Anhydrase Inhibitors Acetazolamide DS

UJ
In chronic open angle glaucoma, Prostaglandin analogues are becoming the 1st line treatment plus/minus Beta blockers.
Side effects of non selective beta blockers are exacerbation of asthma due to Beta 2 blockade and exacerbation of heart block due to Beta 1 blockade.
If after medical treatment the IOP is still high, the options are
1) adding a drug 2) Laser 3) Surgical

UJLaser Trabeculoplasty Involves placing a series of laser burns (50
microns) wide in the trabecular meshwork to improve outflow.
But in UK there’s increasing tendency towards early surgical procedures nowadays.

UJSurgical Treatment Trabeculectomy or drainage surgery is
creating a fistula between the anterior chamber and the subconjunctival space.
Very efficient in reducing the IOP dramatically.

UJ
Complications include:
1) Shallowing of the anterior chamber damaging the lens and cornea.
2) Intra-ocular infection.3) Increase in cataracts.4) Failure to reduce pressure adequately.5) An excessive low pressure (Hypotony) which
may cause macular edema.

UJ

UJGLAUCOMA
Filtration blebsFiltration blebs

UJ
Sympathomimetics and drugs containing preservatives may decrease the success of surgery by causing post operative sub-conjunctival scarring resulting in a non-functional drainage channel.
To prevent this fibrosis from happening, anti-metabolite (5-FU, Mitomicin) may be used at the time of surgery.

UJ
Treatment of normal/low tension glaucoma may be difficult since target pressure is usually below 14mmHg,
Some patients appear to have non-progressive visual field defects and require no treatment.
In those with progressive field loss lowering intraocular pressure maybe beneficial.

UJClosed Angle Glaucoma The condition usually occurs in small eyes
(usually hypermetropic) with shallow anterior chambers.
Relative pupil block in normal eyes. In angle closure glaucoma, this resistance
may be increased due to blockage of the drainage system usually associated with pupil dilatation.
Pressure usually rises abruptly. Contact between the iris and cornea usually
leads to adhesions called peripheral anterior synechiae (PAS).

UJ
The severely reduced or stagnant circulation of aqueous deprives the whole cornea of nutrition and the posterior cornea of oxygen Giving rise to a massive corneal edema which is amplified by the raise IOP This results in a profound loss of vision.

UJ
A full blown case of acute angle closure glaucoma may be preceded by subacute attacks of angle closure resulting in transient rises of the IOP, headaches and corneal edema confined to the epithelium.
This continuous insult to the basal epithelial cells of the cornea by edema fluid, acting as a diffraction grating, is the basis to the key symptom of such prodromal attacks Coloured halos around bright lights.

UJEpidemiology Primary angle closure glaucoma affects 1 in
1000 people over 40 years of age. Patients are usually long sighted Small
eyes More crowded anterior chamber.
Female>males
Onset: 40+ years of ageOnset: 40+ years of age

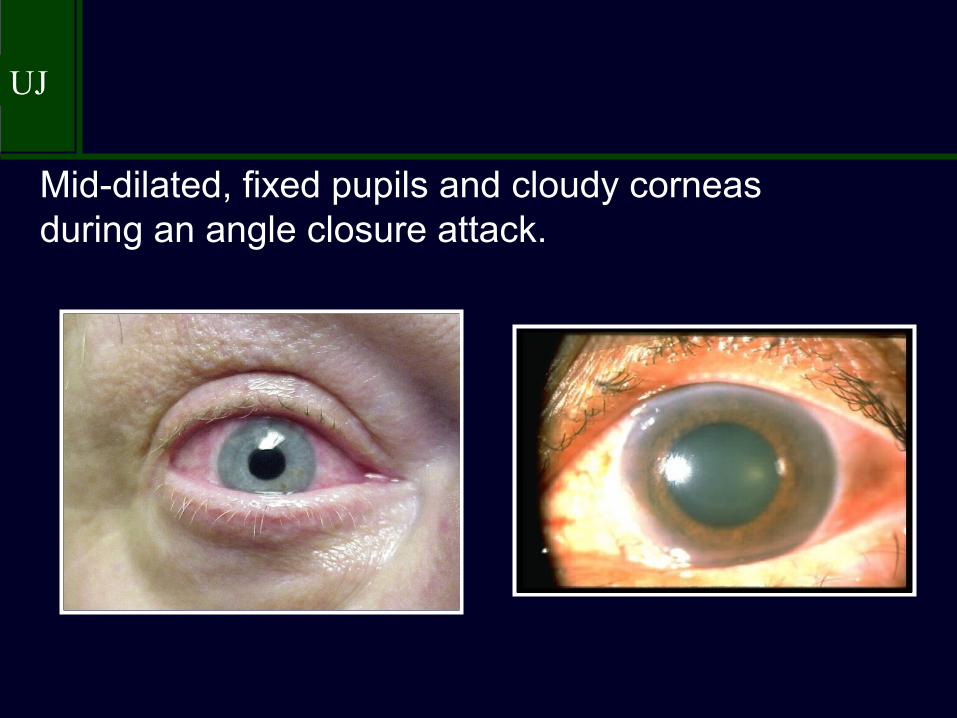
UJ Hx & P/E In acute angle closure glucoma, there is an
abrupt increase in pressure and the eye becomes photophobic…painful due to ischemia…watering of the eye…loss of vision..
Pt feels unwell…nausea…abdominal pain On exam.: red eye…visual acuity is
reduced…cloudy cornea…pupil is oval fixed and dialated
39
UJ
Mid-dilated, fixed pupils and cloudy corneas during an angle closure attack.
UJTreatment The abrupt increase in pressure must be
reduced dramatically in order to avoid permanent damage to the vision.
Acetazolamide is administered I.V and subsequently orally along with topical Pilocarpine and Beta Blockers.
Pilocarpine constricts the pupil, so removes the iris out of the angle, Acetazolamide and Beta Blockers reduce aqueous secretion and so the pressure is reduced.
UJ
The previous measures will probably treat an acute attack, but subsequent management requires that a small hole (Iridotomy, Iridectomy) be made in the peripheral iris to prevent subsequent attacks.
This hole will provide an alternative connection for the aqueous between the anterior and posterior chambers.
Its is usually done by YAG laser YAG laser or surgically.

UJ
Peripheral IridotomyPeripheral Iridotomy

UJ
If the pressure has been raised for some days, the iris becomes adherent to the peripheral cornea (PAS), the iridocorneal angle is damaged and additional medical or surgical measures may be required to lower the IOP.
In some patients with cataract, lens extraction with IOL may help open the iridocorneal angle.
UJ Secondary Glaucoma IOP rises in secondary glaucoma due to
trabecular meshwork blockage by:1) Blood (hyphaema) following a blunt trauma2) Inflammatory cells (uveitis)3) Pigment from the iris (Pigment dispersion
syndrome)4) Deposition in the trabecular meshwork of
material produced by the epithelium of the lens, iris and ciliary body (Pseudoexfoliative glaucoma)
5) Drugs increasing trabecular meshwork resistance (Steroids)

UJ
Angle closure also accounts for some cases of secondary glaucoma:
1) Rubeosis Iridis due to diabetic retinopathy or central retinal vein occlusion.
2) Large choroidal melanoma pushing the iris forward.
3) Cataract may swell, also pushing the iris forward.
4) Uveitis may cause the iris to adhere to the trabecular meshwork.

UJ
Secondary glaucoma are much rarer than primary glaucomas.
Again, symptoms and signs depend on the rate at which the IOP rises.
most are symptomless. Treatment generally is the same as primary
glaucoma, PLUS treating the underlying cause
Difficult cases may be selected for selective ciliary ablation surgery to reduce aqueous production, usually by laser or cryoprobe.

UJCongenital Glaucoma The cause remains uncertain. The iridocorneal angle may be
developmentally abnormal and covered with a membrane which increases outflow resistance.

UJCongenital Glaucoma
Onset: antenatally to 2 years old
Signs and Symptoms:
Excessive tearingIncreased corneal diameter (buphthalmos)Cloudy corneaSplit’s in Descemet’s membrane

UJCongenital Glaucoma
Buphthalmos and cloudy corneasBuphthalmos and cloudy corneas
The right eye in each patient has congenital glaucoma.
UJ
It is usually treated surgically. An incision is made into the trabecular
meshwork (Goniotomy) to increase aqueous drainage, or a direct passage between schlemm’s canal and the anterior chamber is created (Trabeculotomy).

UJPrognosis of Glaucomas
The goal of treatment in glaucoma is to stop or reduce the rate of visual damage.
Currently, the mainstay of treatment is control of IOP, neuro-protective drugs and the issue of optic nerve head ischaemia is being addressed.
Even though some patients continue to experience progressive visual loss despite control of their IOPs, this control greatly reduces the rate of progression.

UJ
If the diagnosis is made late, the eye will most probably become blind despite treatment. :(
If IOP remains controlled following acute treatment of angle closure glaucoma, progressive visual damage is unlikely.

UJ

UJ
جزاكمريخ اريخ خيرا





























